 Ying’e Gao
Ying’e Gao Jingjing Lin
Jingjing Lin Yuzhuo Zhou
Yuzhuo Zhou Rongjin Lin
Rongjin Lin
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 11 August 2023
Sec. Cancer Imaging and Image-directed Interventions
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1213045
Breast cancer, the most prevalent malignant tumor among women, poses a significant threat to patients’ physical and mental well-being. Recent advances in early screening technology have facilitated the early detection of an increasing number of breast cancers, resulting in a substantial improvement in patients’ overall survival rates. The primary techniques used for early breast cancer diagnosis include mammography, breast ultrasound, breast MRI, and pathological examination. However, the clinical interpretation and analysis of the images produced by these technologies often involve significant labor costs and rely heavily on the expertise of clinicians, leading to inherent deviations. Consequently, artificial intelligence(AI) has emerged as a valuable technology in breast cancer diagnosis. Artificial intelligence includes Machine Learning(ML) and Deep Learning(DL). By simulating human behavior to learn from and process data, ML and DL aid in lesion localization reduce misdiagnosis rates, and improve accuracy. This narrative review provides a comprehensive review of the current research status of mammography using traditional ML and DL algorithms. It particularly highlights the latest advancements in DL methods for mammogram image analysis and offers insights into future development directions.
Golobocan’s latest cancer report (1) states that in 2020, approximately 19.3 million newly diagnosed cancer cases were reported worldwide, resulting in 10 million cancer-related deaths. Among these cases, female breast cancer accounted for about 2.3 million new cases, representing 11.7% of all cancer cases and surpassing lung cancer as the most prevalent malignant tumor. Breast cancer has emerged as a leading malignancy among women, significantly endangering their physical and mental well-being. The mortality rate of breast cancer patients has been decreasing due to advancements in medical technology and early detection. From 1975 to 1989, breast cancer mortality experienced a yearly increase of 0.4 percent but has steadily declined since reaching its peak in 1989. Between 1989 and 2020, there was a remarkable 43 percent decrease in mortality, resulting in a reduction of 460,000 breast cancer-related deaths (2). The decrease in breast cancer mortality can be attributed to improved and more targeted treatment methods, as well as early screening practices. Consequently, early diagnosis and treatment play pivotal roles in enhancing the prognosis of these patients.
Currently, the primary techniques used for the early diagnosis of breast cancer include mammography, magnetic resonance imaging (MRI), ultrasonography (US), computed tomography (CT), and pathological examination (3). Mammograms, among these methods, are relatively inexpensive, straightforward, and rapid. They enable the detection of even minor breast changes that may go unnoticed during manual examination, thereby enhancing diagnostic accuracy (4). Hence, despite the emergence of new technologies for breast cancer diagnosis, mammography remains the simplest and most frequently employed tool for early breast cancer screening (5). However, following mammography imaging, the clinical interpretation and analysis of images necessitate significant time and labor costs, relying heavily on the expertise of clinicians for film interpretation. Diagnosis by doctors is subjective, and their individual experience levels vary. Even experts find it challenging to make immediate and accurate judgments when faced with diverse breast abnormalities, leading to the potential for missed diagnoses and misdiagnoses. Furthermore, training experienced clinicians requires substantial investments of time and effort, posing challenges for professions facing a shortage of technical expertise. Therefore, the development of new technologies is necessary to address these aforementioned challenges. The advancement and widespread adoption of computer technology have facilitated the availability of sufficient computational power for medical image analysis and processing. This, in turn, mitigates the reliance on the expertise level of doctors to some extent, with ML methods proving particularly suitable under these circumstances.
ML is a subfield of artificial intelligence (AI) that emerged in the 1980s (Figure 1) (6). By training and learning, the machine extracts the most relevant features from the dataset and constructs a model to handle unfamiliar data (7). ML comprises three main categories: supervised learning, unsupervised learning, and reinforcement learning. In supervised learning, well-labeled data is used to train a model, which then generates predictions or classification outcomes based on the provided data (8); In unsupervised learning, computers address pattern recognition problems using unlabeled training samples. For instance, unsupervised DL algorithms can identify distinguishing features between benign and malignant nodules, classifying them into respective categories (8); Conversely, reinforcement learning relies on reward feedback to maximize returns or accomplish specific objectives (9). The most frequently employed supervised learning methods include Artificial Neural Networks (ANN), Support Vector Machine (SVM) (10), and Random Forest (RF) (11, 12). Clustering algorithms, such as K-Means (13), Principal Component Analysis (PCA), and Singular Value Decomposition, are the most common types of unsupervised algorithms. Currently, computers are far from matching human learning abilities; however, in certain practical applications, ML has demonstrated impressive outcomes, even surpassing human capabilities. Within clinical settings, ML technology can aid in lesion localization to a certain extent, leading to a reduction in misdiagnosis rates and an improvement in accuracy. Its application in early breast cancer screening has yielded significant results, particularly when combined with mammography X-ray, ultrasound, breast MRI, and pathological diagnosis, alongside other auxiliary examinations.
Figure 1 Relation between AI、ML and DL.
DL, as a subset of ML, is capable of automatically extracting meaningful features from big data (14), including the development of image recognition in three stages: text recognition, digital image recognition, and object The basic structure of DL comprises the input layer, hidden layer, and convolutional layer. The hidden layer further consists of the convolutional layer, pooling layer, and fully connected layer (15). The input layer primarily handles data input into the convolutional layer for consolidation purposes, such as feature scaling and data enhancement (16). The primary function of the convolutional layer is to perform feature extraction and calculate the convolution results of data feature mapping using trainable convolutional filters and bias parameters (17). The pooling layer filters and consolidates the features, which are then fed into the fully connected layer for non-linear combination and output (18). The fully connected layer is a structure where every neuron in two adjacent layers is interconnected. Following this layer, the output layer produces the classification result or probability. DL models have extensive applications, encompassing various architectures such as deep neural networks (DNNs), autoencoders (AEs), deep belief networks (DBNs), deep convolutional neural networks (CNNs), recurrent neural networks (RNNs), and generative adversarial networks (GANs).CNN is one of the most representative algorithms in DL, known for its ability to extract high-level information from similar features located at different spatial positions within the input signal (19). Consequently, CNN has achieved significant success in visual recognition and speech recognition tasks (19, 20), particularly excelling in visual recognition due to its high-performance advantages in image processing.
This narrative review provides a comprehensive review of the progress and challenges in the field of ML and DL for mammography, aiming to facilitate researchers’ understanding of the latest advancements. Several published review papers have been presented in the last few years. However, all of them have only been addressed one side focusing on one application or topic, such as Sechopoulos et al. (21) for breast cancer detection with mammography, Gastounioti et al. (22) for breast cancer risk prediction with mammography, Computer-aided breast cancer detection and classification in mammography (23), DL for breast cancer diagnosis (18), DL for Classification of Breast Microcalcifications (24), and etc. This review paper has a distinctive focus compared to previous articles for the following reasons. Firstly, we aim to present an up-to-date examination of the advancements in ML and DL techniques applied to mammography for breast diagnosis. This review serves as a valuable reference for the development of new diagnostic methods. Secondly, we comprehensively discuss the utilization of ML and DL in various stages of mammography image processing, including preprocessing, detection of masses and microcalcifications, as well as segmentation and classification. Furthermore, we address the existing challenges associated with ML and DL approaches, such as limited training data, high implementation costs, and suboptimal accuracy in lesion recognition. Lastly, based on our thorough review, we have derived several significant conclusions that can greatly benefit future research endeavors in the field of medical imaging for breast cancer.
Several databases were searched, including PubMed, Web of Science, and CNKI.The search was limited to studies published between January 2018 and March 2023. Exclusion criteria were applied, which encompassed studies lacking conventional performance metrics such as sensitivity, specificity, area under the receiver operating characteristic curve, and others. Additionally, studies consisting solely of guidelines, review articles, abstracts, animal studies, or with a sample size smaller than 10 were excluded. Following the removal of duplicate studies and those containing redundant or non-novel information, these libraries offer a large number of candidate papers for this study (Figure 2).
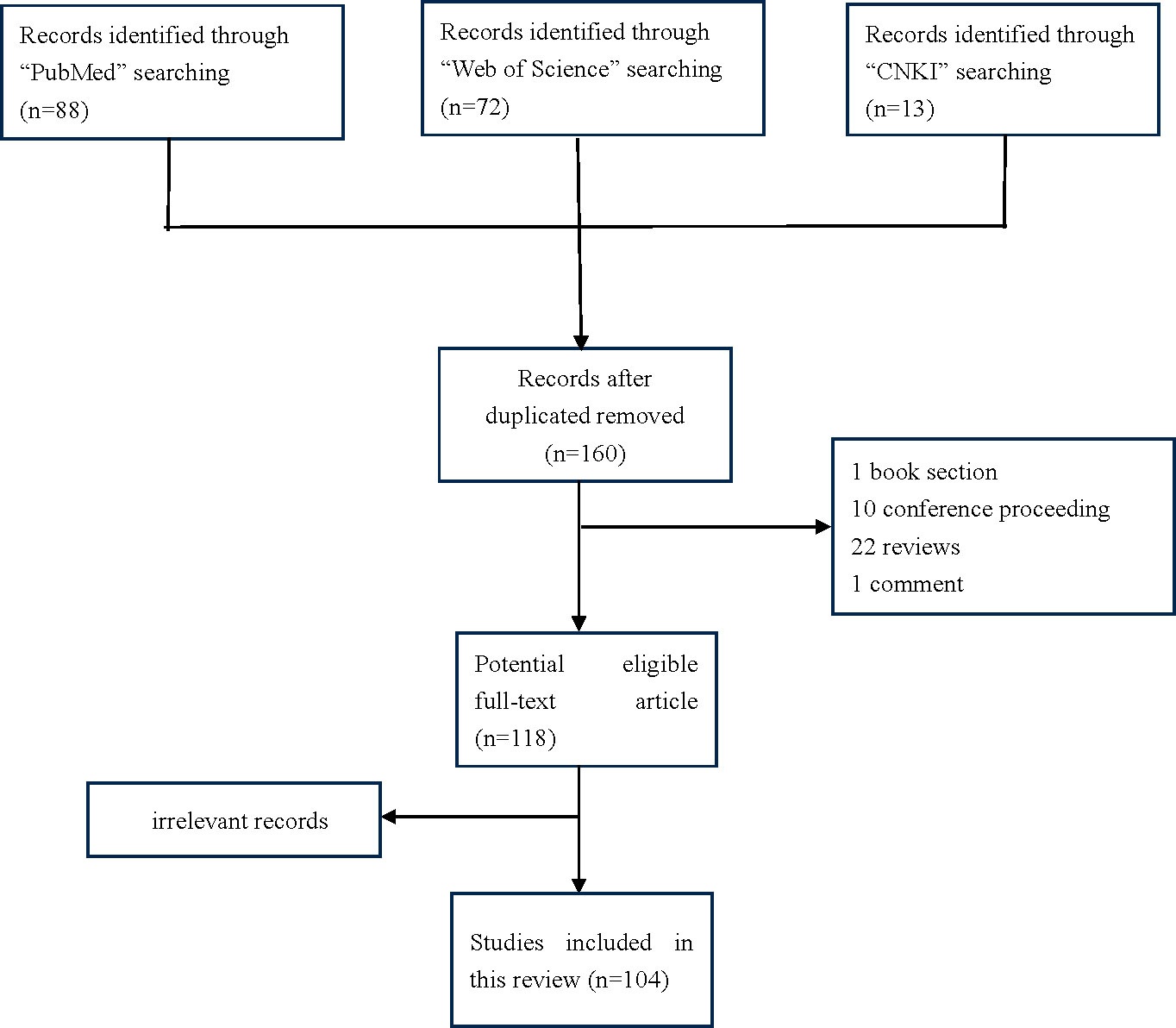
Figure 2 Flow diagram of identification of researches included in the review.
As the cause of breast cancer remains unclear, the focus of breast cancer prevention primarily lies in secondary prevention strategies Mammography imaging is a preferred method for clinical breast disease examination due to its simplicity and high recognition rate for early microcalcifications However, mammography has limitations in cases of dense mammary glands, resulting in reduced accuracy (25). ML-based mammograms overcome this limitation by employing ML algorithms to perform tasks such as lesion detection, segmentation, feature extraction, and benign and malignant classification, eliminating the reliance on visual recognition (26) (Figure 3).

Figure 3 Workflow of computer-aided diagnosis of mammographic images.
Image preprocessing is essential due to the challenges encountered in diagnosing mammography images of early breast cancer, including small and irregular calcification points, diverse morphological distribution, poor contrast, and the presence of residual lesion tissues in dense breast tissue. High resolution is often necessary to overcome these challenges, which may require extensive processing time if performed directly on the original images. Common mammography preprocessing methods encompass the removal of background and muscle tissue artifacts, noise reduction, image enhancement, and image resizing. Various algorithms can be applied during the preprocessing stage to improve image quality, including adaptive median filtering, histogram equalization (HE), dynamic thresholding, morphological operations, wavelet transform, Wiener filtering, and contrast-limited adaptive histogram equalization (27). The objective of mammogram preconditioning is to enhance contrast effectively and remove unwanted details within the breast, including the background and pectoral muscles visible in the Medial and Lateral Oblique (MLO) position view, while preserving areas that may hold diagnostic significance (23). Hazarika and Mahant (28)utilized a combination of threshold-based segmentation and morphological manipulation, achieving 98.7% accuracy in identifying breast boundaries and removing the background from the image. Bora et al. (29)employed Hough line transforms and “texture gradient” and “Euclid distance regression” for approximating the chest edge and segmenting muscles from mammograms. Their method successfully removed pectoral muscles from 96.75% of the images. Mammography images often contain speckle noise, which adversely affects image contrast and resolution. Thus, filtering techniques are necessary to remove noise and improve image quality (30). Kavitha et al. (31) proposed the OMLTS-DLCN model, which incorporates adaptive fuzzy median filtering (AFF) as a pretreatment step to remove noise from mammogram images. Arora et al. (32) employed the histogram equalization (HE) method to enhance contrast effectively and improve the image’s edge by expanding its dynamic range as part of the image preprocessing stage.
Mammography image preprocessing primarily aims to remove irrelevant information and noise, while retaining relevant and useful information (33). Continuous advancements in mammography technology have led to significant improvements in picture quality, resulting in reduced noise levels. Due to the similarity between noise and early calcification points, there is a risk of misjudgment during the noise removal process, leading to instances where the noise is not completely eliminated. Given the similarity in grayscale between pectoral muscles and masses, it becomes necessary to normalize the image or enhance contrast to mitigate disturbances caused by the presence of pectoral muscles. Hence, pretreatment plays a vital role in accentuating features, enhancing feature contrast, and improving the reliability of subsequent processing steps.
Breast cancer originates from the aberrant proliferation of cells in breast tissue, resulting in the development of diverse lesion types, such as asymmetry between the left and right breasts, tissue structure distortion, and the presence of microcalcifications (MCs) and lumps in varying sizes and shapes (34). Breast masses and microcalcifications are prevalent types of lesions encountered in clinical practice. MCs are small calcium deposits commonly found in the breast, appearing as bright spots on mammograms (35). While individual MCs are not highly indicative of breast cancer detection, the formation of microcalcification clusters through the aggregation of microcalcifications serves as an important early sign of breast cancer. Microcalcification clusters, consisting of three or more calcification points per centimeter, can lead to a preliminary diagnosis of early breast cancer. Thus, the detection of microcalcification clusters holds significant value in the early examination of breast cancer. Lumps typically manifest as relatively dense areas (off-white areas) on mammograms. Benign lumps exhibit a round, smooth, and well-circumscribed appearance, while suspicious lumps display irregular, rough, and blurred borders (35).
Duarte et al. (36) demonstrated a technique for segmenting microcalcifications by combining geodesic active profiles with anisotropic texture filtering. The images undergo preprocessing through Alternating Sequential Filtering, and contrast enhancement is achieved using Adaptive Histogram Equalization (CLAHE) technology. The image set utilized in the system is extracted from the DDSM database. This technique achieved an average area overlap measurement of 0.52 ± 0.20, encompassing 87.4% of malignant cases and 86.4% of benign cases. Guo (37) et al. described a system for detecting microcalcified clusters present in digital mammogram images. The zone growth method was employed to eliminate artifacts in mammal X images. The top hat transform and grayscale adjustment methods are utilized for contrast enhancement. The contourlet transform is employed to identify suspicious regions in the breast X image. Calcified clusters are detected using unlinked pulse-coupled neural networks. The proposed system achieved a good accuracy of 95.8%, sensitivity of 96.3%, and specificity of 94.7% when tested on the MIAS and JSMIT databases, respectively. In the (38) study, the researchers proposed a CAD system for mammography microcalcification detection based on a new feature set. They employed statistical observations of classical features (such as higher-order statistics, discrete wavelet transform, and wavelet decomposition) for preprocessing, used the t-test method for evaluation and feature reduction, and achieved good results in sensitivity. Fadil et al. (39) proposed a computer-based automated method for segmenting and classifying breast microcalcifications in mammograms. They utilized discrete wavelet transforms and random forests (DWT-RF) and tested the method on 966 images (322 benign, 322 malignant, and 322 normal). The results showed that DWT-RF achieved a sensitivity of 93%, specificity of 97%, a false positive rate of 3%, and an accuracy of 95%. Moreover, the area under the ROC curve was 0.92, which is comparable to the latest methods and other existing classifiers. Suhail et al. (40) developed a novel method for classifying benign and malignant microcalcifications. They utilized the improved Fisher linear discriminant analysis (LDA) method to perform a linear transformation of segmented microcalcified data and employed junction SVM variants to classify between the two classes. The results demonstrated an average accuracy of 96%.
Recently, the detection of microcalcification points in mammography has gained significant attention as a challenging research area. Despite numerous methods proposed for detecting microcalcification points. However, due to the complex structure of mammography X-ray images, uneven background, and the presence of noise similar to microcalcifications, the detection of microcalcification points still poses certain challenges. Current methods have not yielded satisfactory results, with routine examinations missing 10-30% of cases (41). Hence, researchers should prioritize the development of new technologies to enhance the efficiency and accuracy of detecting microcalcification points in the breast. Additionally, most studies continue to rely on breast image databases from Europe and North America, resulting in a limited number of studies focused on dense mammary X-ray images. Furthermore, there is currently no standardized breast image database suitable for Asian women researchers. Therefore, establishing a standardized breast image database specifically tailored for Asia is an urgent concern.
Huang et al. (42) conducted a retrospective analysis of mammography images, encompassing 124 benign breast masses and 139 malignant breast masses. They extracted the texture features of mammography images and trained four models, namely, linear discriminant analysis (LDA), logistic regression, RF, and SVM, using the training set data. The performance of these models was then verified using the validation set. The RF model exhibited a higher compliance rate, Kappa coefficient, and AUC value in both the training and validation sets. These results highlight the advantages of ML models based on the texture features of mammary X-ray images in distinguishing between benign and malignant breast masses. Tourassi et al. (43) extracted the masses from mammography images and created a region of interest (ROI) database based on the ROI label information of the breast masses in the DDSM database. They employed mutual information as a similarity measure between the template image and the image block to be matched. By calculating the similarity between all suspected mass areas and the template image, they sorted the similarity values and selected the area with the highest matching degree as the detected breast mass. Yu et al. (44) combined median filtering, morphology, and Sobel edge detection to acquire the initial rough edge of the mass. They subsequently employed gradient vector flow snake (GVF-Snake) and gradient map adjustment to perform the final mass segmentation.
Traditional methods for lesion area segmentation can be categorized into region-based, threshold-based, edge-based, feature-based, and theory-based approaches. However, due to the irregular shape of lesions, irregular boundaries, and the presence of grayscale heterogeneity within lesions, relying solely on a single segmentation method often fails to achieve optimal results. Thus, the current trend in research is to synthesize different methods to enhance segmentation accuracy. Additionally, lesion detection methods are frequently combined with segmentation algorithms to simultaneously segment the lesion area and determine the presence of lesions, thereby improving the effectiveness of computer-aided diagnosis.
Accurate segmentation of the breast lesion area is fundamental to mammography-assisted diagnosis technology as it serves as the basis for subsequent feature extraction and classification of breast lesions. Generally, the irregularity of a lump’s shape correlates with its malignancy level (45). Traditional methods for breast lump segmentation typically involve area-based algorithms (46), contour-based algorithms (14), threshold segmentation (47), edge detection (Table 1). Li et al. (48) developed SAP-cGAN, a mammography mass segmentation model based on an enhanced conditional generative adversarial network (cGAN). The model incorporates a superpixel averaging pool layer in the cGAN decoder, utilizing superpixels to enhance boundary segmentation. Additionally, a multi-scale input strategy is employed to enable the network to learn scale-invariant features and improve robustness. The study demonstrated significant qualitative and quantitative improvements of SAP-cGAN over baseline cGAN and other methods in mammogram mass segmentation using CBIS-DDSM and INbreast datasets. However, the SAP-cGAN model has limitations when applied to mass segmentation involving complex tissue structures. Kozegar et al. (49)propose a two-stage segmentation method that incorporates shape information from training samples. In the first stage, they utilize a novel adaptive region growth algorithm to estimate the mass boundary roughly. Based on the volume and roundness of the training samples, a Gaussian mixture model is employed to determine the algorithm’s similarity threshold. In the second stage, they introduce a novel deformable model based on geometric edges, using the results from the first stage as the initial profile. The study demonstrates the effectiveness of the proposed supervised method in achieving accurate mass segmentation results measured by the Dice coefficient. Alam et al. (50) proposed a novel technique for segmenting microcalcification (MC) clusters by employing a series of morphological operations. The method aims to enhance the accuracy of MC cluster segmentation by selecting the most significant features from the segmented image. These selected features facilitate the generation of the final output in the CADx pipeline. Jen et al. (51)proposed an anomalous feature detection method for mammography based on a novel abnormality detection classification approach. The method utilizes the gray value quantification method to extract five features for detecting the region of interest in the segmented mammogram image. Principal Component Analysis (PCA) is then employed to determine the weight. Experimental results demonstrate that the sensitivity of the method, combined with feature weight adjustment, reaches 88% and 86% on the MIAS dataset and DDSM dataset, respectively. Shi et al. (52) propose an automated image processing pipeline that primarily relies on pixel clustering without training to estimate breast boundaries and simultaneously characterize breast tissue. This pipeline includes skin boundary estimation, breast segmentation, and calcification detection.
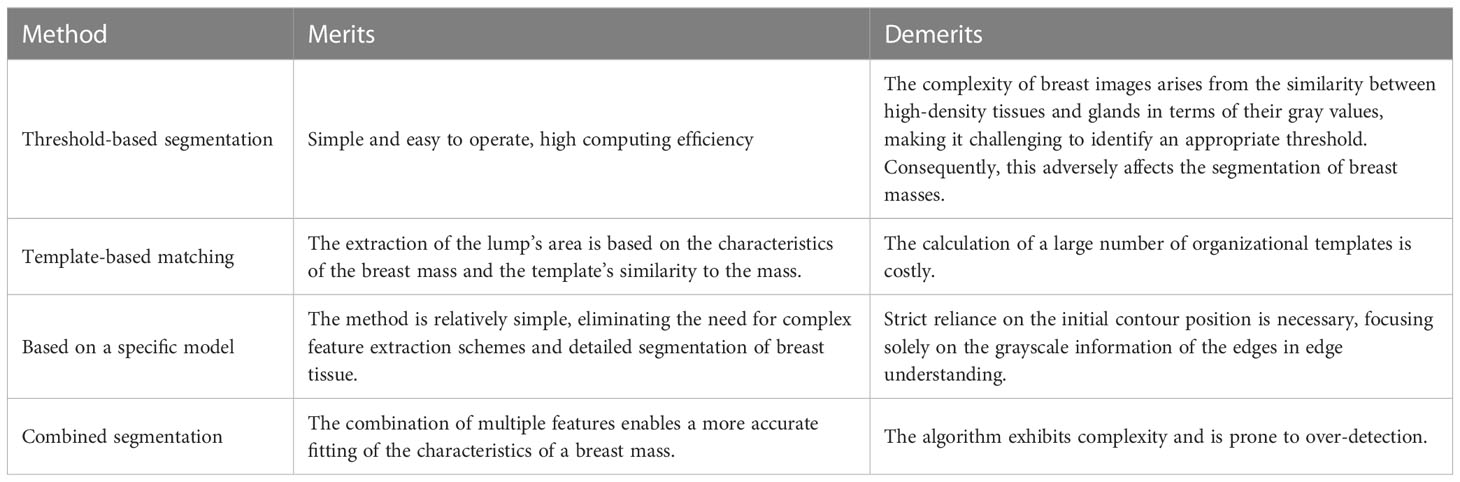
Table 1 Introduction to lesion segmentation.
Lesion segmentation poses significant challenges due to the highly irregular edges of malignant mass lesions, making it difficult to achieve accurate resultsusing a single segmentation method. Additionally, the presence of high-density breast tissue can lead to erroneous segmentation of the dense area as a breast mass. Therefore, addressing these issues necessitates the adoption of a comprehensive range of methods to enhance segmentation accuracy in the future.
Following pretreatment and accurate segmentation of regions of interest (ROIs) in mammograms, various features can be extracted to classify ROIs as normal, benign, suspect, or malignant microcalcifications (MCs). Common feature extraction methods employed in the extraction stage of mammary lesion features include grayscale co-occurrence matrix (GLCM), multidimensional co-occurrence matrix, independent component analysis, genetic algorithm, two-dimensional PCA, wavelet and curvature methods, and PCA. These methods are utilized to extract features like entropy, skewness, variance, and kurtosis (27).In 2017, Khan et al. (53) employed Gabor filters to extract features from textured micropatterns at various scales and orientations. They utilized Linear Discriminant Analysis (LDA) and Principal Component Analysis (PCA) for dimensionality reduction and employed a weighted SVM based on successive reinforcement learning for classification. The method achieved an average accuracy range of 68% to 100%.Ghazouani et al. (54) propose a fully automated breast cancer diagnostic method that utilizes small training datasets. The method extracts features from mammography images using a genetically programmed descriptor that leverages statistics of local binary pattern-like local distributions defined at each pixel. This approach yields promising results for both content-based retrieval and classification problems. Additionally, The authors (55) present a computer-aided diagnosis (CAD) system for classifying breast masses within mammogram ROIs as malignant or benign. The system employs 13 features based on GLCM to characterize textures. These extracted features are inputted into a SVM classifier, achieving an accuracy of 94%.Vijayarajeswari et al. (56) employed the Canny edge detector, followed by the Hough transform, to extract local texture features. They extracted four types of intensity-based features (mean, entropy, standard deviation, and variance) and utilized them as input for training classifiers. This method achieved an accuracy of 94% in distinguishing normal and abnormal breast tissue. In a study by (57), Haralick’s features were extracted from ROI images, followed by nuclear principal component analysis to reduce the dimensionality of the feature vectors. Subsequently, a wrapper-based parameter optimization kernel extreme learning machine was employed to identify the most significant features from the simplified feature vector.Finally, a wrapper-based parameter optimization kernel extreme learning machine is utilized to select the most prominent features from the simplified feature vector. The multi-level classification accuracy reached 92.61% in the digital breast screening database. Omondiagbe (58)presents a hybrid approach for breast cancer diagnosis that employs Linear Discriminant Analysis (LDA) to reduce the high dimensionality of features and subsequently applies a new dimensionality reduction feature dataset to Support Vector Machines (SVMs). The method achieved an accuracy of 98.82%, sensitivity of 98.41%, specificity of 99.07%, and an area under the receiver operating characteristic curve of 0.9994. SINGH et al. (59) initially enhanced the region of interest using morphological operations. They then extracted cluster shape features and cluster texture features and employed SVM for classification. The feature set was augmented with a set of shape features obtained using the recursive subsampling method, resulting in improved classification accuracy, with an achieved accuracy of 94.25%. Experiments demonstrated that the proposed classification system effectively reduces classification errors and enhances the efficiency of accurate diagnosis. Fanizzi et al. (60) propose an automated binary model for tissue classification in digital mammograms. The model utilizes statistical features obtained through multiscale decomposition of images based on Haar wavelet transforms, as well as points of interest and corners detected using the Speeded Up Robust Feature and Minimum Eigenvalue Algorithm. State-of-the-art machine learning classifiers, such as RF, are trained with these features to address binary discrimination tasks. The proposed model’s performance is evaluated through cross-validation on 260 regions of interest (ROIs). Experimental results demonstrate the model’s excellent prediction performance, with median Area Under the Curve (AUC) values of 98.16% and 92.08% for normal/abnormal and benign/malignant problems, respectively, along with accuracies of 97.31% and 88.46%.Ghasemzadeh et al. (61) extracted feature vectors from mammogram images using the Gabor wavelet transform. They conducted tenfold cross-validation through multiple experiments to analyze the data complexity in each fold. The achieved results showed an average accuracy above 0.939, average sensitivity up to 0.951, and average specificity greater than 0.92. Naseem et al. (62) present an automatic detection system for breast cancer diagnosis and prognosis based on a classifier ensemble. They compare various ensemble models and ML-based test models with and without upsampling techniques on two benchmark datasets. They also investigate the impact of using balanced class weights on prediction datasets and compare the performance with other methods. The results demonstrate the superiority of the ensemble method, achieving an accuracy rate of 98.83%. Dhahbi et al. (63) proposed a grayscale structural analysis method to characterize the region of interest in mammography. They studied the utilization of research methods such as GLCM, fractal analysis, Hilbert image representation, Kolmogorov-Smirnov distance, and maximum subregion descriptors. By extracting features directly from the entire region of interest, the proposed method not only avoids the challenging problem of breast mass segmentation but also considers the texture surrounding the lesion, which significantly aids in breast cancer diagnosis. Additionally, several classifiers including RF, SVM, and decision trees were employed to differentiate between normal tissues and masses. Empirical evaluation using a large database of challenging suspicious regions extracted from the DDSM database demonstrated the effectiveness of the proposed method in reducing false positives in mammography mass detection.
In the clinical diagnosis of breast cancer, it is essential to consider multiple types of lesions, including masses and microcalcifications. Simultaneous classification of benign and malignant lesions across different types is required. Currently, there is a scarcity of research on classification methods for multi-class lesions, and the achieved classification results are also subpar. Addressing this gap in research is a crucial direction for future studies.
The continuous development and optimization of DL models and algorithms have significantly expanded the application of DL in mammography image analysis (56). Table 2 presents a compilation of state-of-the-art mammography imaging methods that employ DL techniques
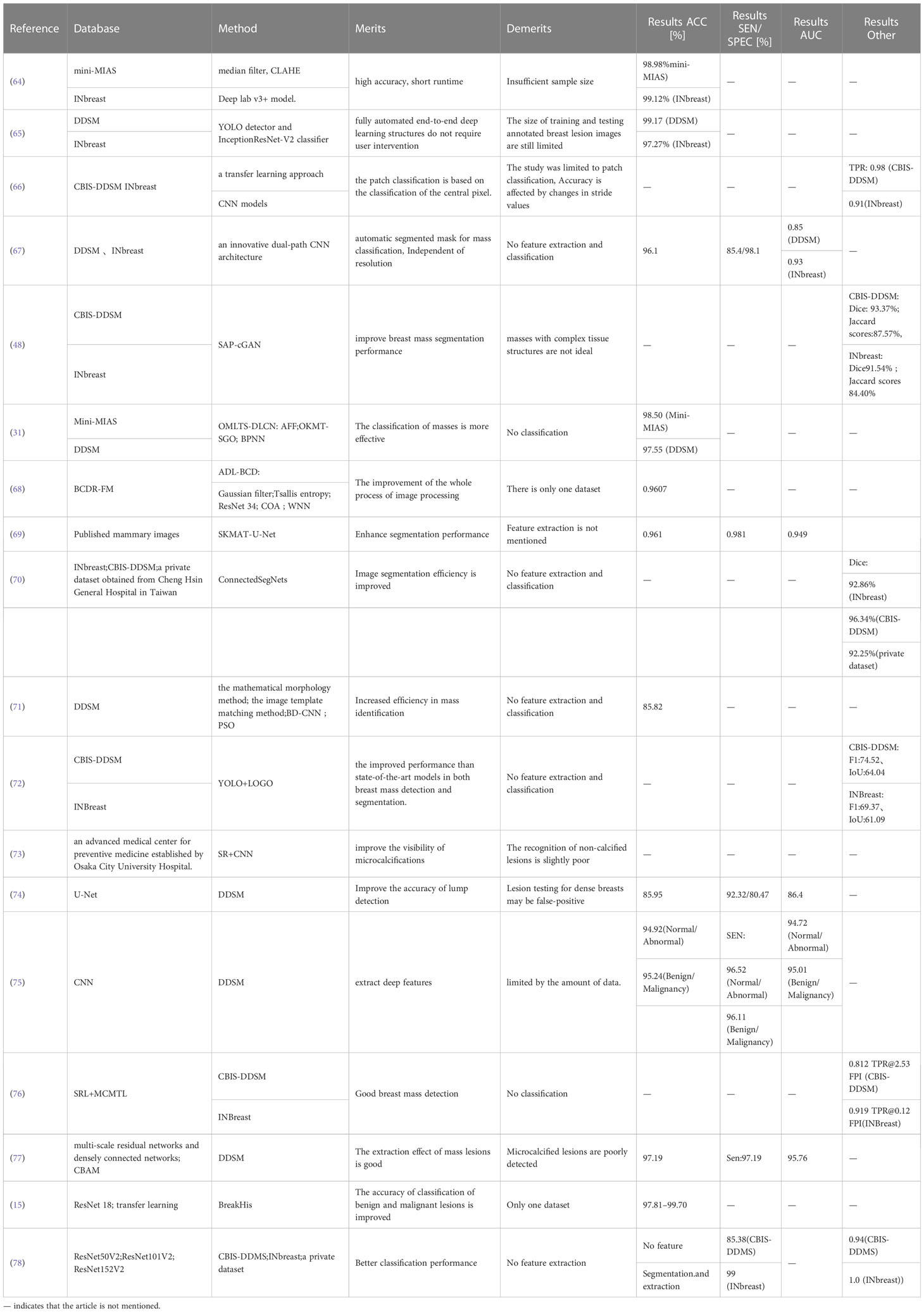
Table 2 Literature comparison of different studies on breast cancer.
Leong et al. (79) proposed an adaptive transfer learning deep convolutional neural network for segmenting mammogram images with calcified cases, aiming to assist in early breast cancer diagnosis and intervention. Honjo et al. (73) p proposed a deep-learning-based super-resolution (SR) model based on DL for identifying microcalcifications (MCs) in mammography images. Researchers conducted visual and quantitative comparisons between pre-processed and post-processed images, demonstrating the model’s potential in detecting and diagnosing microcalcifications. Zeiser et al. (74) introduced a U-Net-based model for diagnosing CAD systems in digitized mammograms, enabling lesion monitoring over time. The proposed methodology involves (1): Preprocessing, including removal of irrelevant information, contrast enhancement, and area of interest extraction (2); Data enrichment through horizontal mirroring, scaling, and resizing of images (3); Training based on a six-membered U-Net model with diverse characteristics. The results indicated that the best model achieved a sensitivity of 92.32%, specificity of 80.47%, accuracy of 85.95%, Dice index of 79.39%, and AUC of 86.40%.Al-atari et al. (65) presented an integrated CAD system for breast lesion detection and classification using DL. They first utilized the YOLO detector based on DL to evaluate breast lesion detection in the DDSM and INBREAM mammogram databases, achieving overall detection rates of 99.17% and 97.27%, respectively. Using the detected breast lesions, the average overall accuracy of the CNN, ResNet-50, and InceptionResNet-V2 classification models for the DDSM and INbreasts datasets was reported as 94.50%, 95.83%, 97.50%, and 88.74%, 92.55%, 95.32%, respectively. The DL-based YOLO detector improves lesion detection accuracy in mammography X-rays, thereby enhancing the classification model’s diagnostic performance for breast lesions. Sun et al. (71) proposed a novel breast mass detection method that integrates mathematical morphology, image template matching, CNN-based breast mass detection, and a breast mass bounding box regression model using the particle swarm algorithm. The proposed method’s detection performance was experimentally evaluated on the mammography image dataset DDSM and compared with the state-of-the-art breast mass detection method. Niu et al. (77) utilized a convolutional neural network method to classify benign and malignant masses in mammography films. They employed a multi-scale residual network and a dense connectivity network as the backbone network to extract features from global and local image patches. Additionally, they employed the Convolutional Block Attention Module to enhance the feature expression ability of the network. Finally, the characteristics of multi-scale image patches were fused to achieve the classification of benign and malignant breast masses.
Su et al. (72) eveloped a deep-learning model architecture for detecting and segmenting breast cancer masses using mammography. The model combines YOLO (You Only Look Once) and LOGO (Local-Global) architectures for quality inspection and segmentation. Firstly, YoloV5L6 was employed to locate and crop the breast lump in the mammogram. Secondly, to achieve a balance between training efficiency and segmentation performance, the researchers modified the LOGO training strategy by training the entire image and cropping the image on the global and local Transformer model branches, respectively. These two branches are then merged to make the final split decision. The results demonstrate that the proposed YOLO-LOGO model exhibits higher efficiency, improved performance, reduced computing requirements, and enhanced versatility and accuracy in computer-assisted breast cancer diagnosis. Zhou et al. (64) present a novel DL-based method for extracting breast regions that combines various pretreatment techniques, including noise suppression using median filters, contrast enhancement using CLAHE, and semantic segmentation using Deep lab v3+ models. The method is trained and evaluated on the mini-MIAS dataset and also evaluated on the INbreasts dataset. The results surpass those of recent studies, highlighting the model’s capability to maintain accuracy and runtime advantages across different databases with varying image resolutions.Li et al. (67) propose a novel DL framework for processing mammogram images that involves mass segmentation and simultaneous prediction of diagnostic outcomes. Firstly, they construct a quality and context texture learner, known as the Locality Preserving Learner, using a stack of convolutional blocks to map regions of interest to class labels at a relatively large scale. Secondly, they employ the Conditional Graph Learner, which combines graph and CNN, to learn correlations in relatively small-scale ROIs and utilize the extracted segmentation features to enhance the final quality classification performance. The DUAL CORENET framework achieves optimal mammogram segmentation and classification, exhibiting superior segmentation performance at both low and high resolutions. Li et al. (48) propose a novel network architecture for segmenting massive images in digital mammograms. The architecture combines two modules within the main basic cGAN framework: a superpixel average pooling layer and a multiscale input module. These modules provide prior boundary information and scale-invariant features. The model’s performance is evaluated on large-scale images from two commonly used datasets, CBIS-DDSM and INBREST. The model achieves impressive results in terms of Dice and Jaccard scores, accuracy, specificity, and sensitivity. For the CBIS-DDSM dataset, the Dice and Jaccard scores are 93.37% and 87.57%, respectively. For the INBREASTS dataset, the Dice and Jaccard scores are 91.54% and 84.40%, respectively. These findings indicate that the proposed model outperforms current state-of-the-art breast mass segmentation methods. Chakravarthy et al. (69) introduce an enhanced version of U-Net called SKMAT-U-Net. This model incorporates a selective kernel with an attention mechanism to adaptively adjust the network’s receptive fields. It combines feature maps extracted through extended and standard convolution operations. The researchers then integrate four attention loss functions based on the traditional cross-entropy loss function to form a U-Net using the Mixed Attention Loss Function. The proposed model effectively segments lesions in ultrasound images of the mammary glands. Alkhaleefah et al. (70) developed a DL model called Connected SegNets for segmenting breast tumors from X-ray images. In the proposed model, two SegNet architectures are connected by skip-the-loop connections between their layers. To enhance the model’s robustness to noise during training, the original SegNet’s cross-entropy loss function is replaced by the intersection-over-union (IoU) loss function. Contrast Limited Adaptive Histogram Equalization (CLAHE) is applied to all datasets to enhance the compressed area and smooth pixel distribution. Additionally, two image enhancements, rotation and anti-warping, are employed to augment the training data and mitigate overfitting. Experimental results demonstrate the superiority of the proposed connected segmented network model over existing methods, as evidenced by higher Dice score and IoU score. Rodriguez-Ruiz et al. (80) proposed an automatic pectoral muscle segmentation model based on the U-Net DL architecture. The model was trained using 136 DBT images acquired by a single system. It was then evaluated on 125 images of three different types: Digital breast tomosynthesis (DBT), synthetic mammographic image (SM), and digital mammography (DM). The obtained Dice Similarity Coefficients (DSCs) ranged from 0.947 to 0.970, a visually determined range ensuring adequate segmentation.
Zhang et al. (75) proposed a multi-view feature fusion network model for classifying mammograms using a multi-scale attention-dense network as the backbone network for feature extraction. The model incorporates two CNN branches to extract features from mammography images captured from different perspectives, enabling the network to leverage a broader range of spatial information. Additionally, a multi-scale convolution module is introduced to extract features at various scales within the images. Experimental results demonstrate the model’s strong performance in both classification tasks. The model achieves an accuracy of 94.92% and 95.24%, sensitivity of 96.52% and 96.11%, and AUC values of 94.72% and 95.03% for classifying normal and abnormal mammograms, and benign and malignant mammograms, respectively. Shen et al. (76) propose a novel DL framework composed of two primary stages: Suspicious Region Localization (SRL) and Multicontext Multitask Learning (MCMTL). In the first stage, SRL is responsible for generating the region of interest (ROI) and extracting multi-sized patches from these suspicious regions. In the second stage, the MCMTL network combines the features of the multi-sized patches from the suspicious areas to perform simultaneous classification and segmentation. The proposed method demonstrates performance that is on par with the most advanced methods reported in the literature. Aljuaid et al. (15) propose a computer-aided diagnostic method for breast cancer image classification utilizing deep neural networks (ResNet 18, ShuffleNet, and Inception-V3Net) and transfer learning. The method leverages BrakeHis’ publicly available breast cancer images and considers various image magnification factors and data augmentation techniques to enhance the classification process. Three deep neural networks were employed to classify the breast cancer images using an image-based approach. The results indicate that the average accuracy for binary and multiclass classification ranged from 97.81% to 99.70%. The researchers concluded that ResNet was the most accurate and efficient classifier among the three models. Baccouche et al. (78) developed a stacked ensemble of ResNet models (ResNet50V2, ResNet101V2, and ResNet152V2) to classify breast masses as malignant or benign and assess their BI-RADS category on a scale of 2 to 6, considering their shape (oval, round, lobulated, or irregular). The results of the proposed method demonstrate improved classification performance compared to individual models and other methods applied to existing benchmark datasets. Agarwal et al. (66) propose a patch-based CNN method for automatic detection of breast lesions in full-field digital mammograms (FFDM). They employ transfer learning by training CNNs on a large public database of digitized mammograms (CBIS-DDSM dataset) and transferring the model to a smaller digital mammogram database (INbreast dataset) for evaluation. VGG16, ResNet50, and InceptionV3 are used as depth feature extractors, and the InceptionV3-based model achieves the best detection results with a true positivity rate (TPR) of 98%. LKavitha et al. (31) proposed the Optimal Multi-Level Thresholding-based Segmentation with DL enabled Capsule Network (OMLTS-DLCN), a breast cancer diagnostic model based on digital mammograms. The model incorporates Adaptive Fourier Filtering (AFF) as a pretreatment step to remove noise from mammogram images. It employs the Optimal Kapur’s based Multilevel Thresholding with Shell Game Optimization (OKMT-SGO) algorithm for segmentation and lesion detection in mammogram images. Additionally, the model utilizes a Capsule Network-based feature extraction method and a Back-Propagation (BP) neural network for breast cancer detection. The diagnostic performance of the OMLTS-DLCN model was evaluated using the benchmark Mini-MIAS dataset and DDSM dataset, achieving high accuracy rates of 98.50% and 97.55%, respectively. Escorcia-Gutierrez (68) proposes an automated DL-based breast cancer diagnosis method called ADL-BCD technology, which employs digital mammograms for the detection of breast cancer. ADL-BCD technology encompasses GF-based preprocessing, Tsallis entropy-based segmentation, ResNet34-based feature extraction, chimp optimization algorithm (COA)-based parameter tuning, and wavelet neural network-based classification. The use of COA-based hyperparameter optimization significantly enhances diagnostic efficiency. The ADL-BCD method was evaluated using a benchmark dataset, and the simulation results demonstrate its superior performance compared to existing methods across various evaluation measures.
The rapid development of DL and the significant improvement in computer performance have made DL a prominent research area for analyzing and processing medical images to aid in lesion diagnosis. Traditional computer-aided diagnosis (CAD) systems lack deep networks and can only extract shallow features, resulting in poor system performance. DL, on the other hand, can automatically extract informative features from medical images, including those that may not be easily visible to the naked eye. This capability greatly enhances the diagnostic accuracy and efficiency, particularly in the context of breast lesion diagnosis. Recent studies have demonstrated that DL applied to breast cancer screening is approaching the diagnostic proficiency of experienced radiologists (81).. However, the challenge of relying on ROI annotation in DL techniques has yet to be effectively addressed. Therefore, further research should be conducted to explore DL techniques that reduce the dependency on ROI annotation. However, the challenge of relying on ROI annotation in DL techniques has yet to be effectively addressed. Therefore, further research should be conducted to explore DL techniques that reduce the dependency on ROI annotation. Some researchers (82, 83) have employed various DL techniques to detect and classify suspicious areas in mammography images, resulting in improved model performance to some extent. Moreover, considering that DL training and validation sets require extensive data, the creation of a large publicly available dataset with high accuracy, resolution, and diversity becomes necessary. This dataset will facilitate the training of CAD models with superior performance. Consequently, the integration of DL into mammography CAD systems represents a promising direction for advancing computer-aided diagnosis technology for mammography images.
Mammography is a widely used method for early diagnosis of breast cancer. It offers high-resolution X-ray images that enable the visualization of different layers of breast tissue. This technique is effective in detecting breast hyperplasia, benign and malignant tumors, as well as disorders in breast tissue structure (84). Additionally, mammography provides clear images that facilitate before-and-after comparisons, making it highly significant for early detection, diagnosis, and treatment. This narrative review provides an analysis and discussion on the current state of computed breast diagnosis technology, encompassing both traditional ML methods and DL. Firstly, the paper introduces the definition and fundamental theoretical knowledge of ML and DL. It then explores the research on the application of traditional ML techniques in mammography, including preprocessing, feature extraction, lesion segmentation, and benign and malignant classification. Subsequently, the paper delves into the application of DL in mammography, covering lesion detection, segmentation, and classification, while briefly outlining the advantages and disadvantages of DL. Despite the deepening of research on computer diagnosis of breast cancer, there are still many challenges:
(1) The available sample data for glandular structure distortion and asymmetric dense shadow is limited and lacks standardization. Currently, most research focuses on mass and microcalcification detection, neglecting the investigation of glandular structure distortion and asymmetric dense effects. Therefore, it is crucial for researchers to prioritize the development of models for detecting multiple lesions and creating automated tools for identifying glandular structure distortion and asymmetric dense effects.
(2) The variability in shapes and edges of suspicious lesions, along with the blurred boundary between the lesion and the surrounding tissues, results in unstable lesion depiction and increases the risk of misdiagnosis. Although ML-assisted breast diagnosis has significantly improved accuracy, establishing a stable lesion identification system and implementing it on a large scale remain challenging research areas. Therefore, there is a need for further improvements in techniques for automated detection and segmentation of breast lesions in mammograms.
(3) Despite the increasing research on DL, its application still faces limitations. Firstly, training a new DL system requires a large amount of raw data. Secondly, the lack of a unified standard in datasets due to technological, equipment, and operator limitations hinders the reproducibility of research findings across different datasets. Moreover, DL technology is costly to learn, and its internal workings are highly complex (85). Furthermore, DL models typically provide output results without easy-to-understand explanations.
(4) There is a lack of data with complete annotations, and the existing database is small. Both traditional ML and DL require a significant amount of labeled data for training. However, obtaining such data is challenging due to the highly specialized and fragmented nature of medical data. Consequently, in future research, it is imperative to expand the dataset and explore the utilization of DL and other approaches to enhance data availability.
(5) Exploring the integration of artificially defined features with deep features to enhance the performance of DL models is a pertinent research question. The conventional approach of feature extraction faces challenges, such as low efficiency, and the high data processing cost associated with DL.
Breast cancer poses a significant threat to women’s health and mortality, emphasizing the importance of early detection and treatment. Mammograms serve as a highly effective and reliable tool for timely identification and diagnosis of breast cancer (86). CAD systems built on mammography have aided doctors in decision-making and reduced diagnostic errors to some extent, traditional ML-based CAD systems encounter challenges in terms of limited generalization ability, inadequate automation, continued reliance on manual intervention, and a high demand for operators possessing specialized domain knowledge and engineering skills. However, with the advancement of DL research, DL-based CAD systems emerge as a viable solution to address these issues effectively, significantly enhancing the efficiency of breast cancer diagnosis.
YG: Data analysis and writing original draft, writing. JL and YZ review and editing. RL funding acquisition, methodology, project administration, resources, supervision. All authors contributed to the article and approved the submitted version.
This study was supported by the Natural Science Foundation of Fujian Province (Grant No. 2019J01444).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
2. Giaquinto AN, Sung H, Miller KD, Kramer JL, Newman LA, Minihan A, et al. Breast cancer statistics, 2022. CA Cancer J Clin (2022) 72:524–41. doi: 10.3322/caac.21754
3. Cronin KA, Lake AJ, Scott S, Sherman RL, Noone A-M, Howlader N, et al. Annual Report to the Nation on the Status of Cancer, part I: National cancer statistics: Annual Report National Cancer Statistics. Cancer (2018) 124:2785–800. doi: 10.1002/cncr.31551
4. Li H, Zhang S, Wang Q, Zhu R. Clinical value of mammography in diagnosis and identification of breast mass. Pak J Med Sci (2016) 32:1020–5. doi: 10.12669/pjms.324.9384
5. Wang Y, Li J, Gao X. Latent feature mining of spatial and marginal characteristics for mammographic mass classification. Neurocomputing (2014) 144:107–18. doi: 10.1016/j.neucom.2013.11.050
6. Rahmani AM, Yousefpoor E, Yousefpoor MS, Mehmood Z, Haider A, Hosseinzadeh M, et al. Machine learning (ML) in medicine: review, applications, and challenges. Mathematics (2021) 9:2970. doi: 10.3390/math9222970
7. MacEachern SJ, Forkert ND. Machine learning for precision medicine. Genome (2021) 64:416–25. doi: 10.1139/gen-2020-0131
8. McBee MP, Awan OA, Colucci AT, Ghobadi CW, Kadom N, Kansagra AP, et al. Deep learning in radiology. Acad Radiol (2018) 25:1472–80. doi: 10.1016/j.acra.2018.02.018
9. Senders JT, Arnaout O, Karhade AV, Dasenbrock HH, Gormley WB, Broekman ML, et al. Natural and artificial intelligence in neurosurgery: A systematic review. NEUROSURGERY (2018) 83:181–92. doi: 10.1093/neuros/nyx384
10. Asymmetric least squares support vector machine classifiers-Web of Science 核心合集 . Available at: https://www.webofscience.com/wos/woscc/full-record/WOS:000328306800029 (Accessed June 8, 2023).
11. Pal M. Random forest classifier for remote sensing classification. Int J Remote Sens (2005) 26:217–22. doi: 10.1080/01431160412331269698
12. Fusco R, Sansone M, Filice S, Carone G, Amato DM, Sansone C, et al. Pattern recognition approaches for breast cancer DCE-MRI classification: A systematic review. J Med Biol Eng (2016) 36:449–59. doi: 10.1007/s40846-016-0163-7
13. Kramer O. “K-Nearest Neighbors.,” Dimensionality Reduction with Unsupervised Nearest Neighbors. Intelligent Systems Reference Library. Berlin, Heidelberg: Springer Berlin Heidelberg (2013). doi: 10.1007/978-3-642-38652-7_2
14. Chen D-R, Chang R-F, Kuo W-J, Chen M-C. Diagnosis of breast tumors with sonographic texture analysis using wavelet transform and neural networks. Ultrasound Med Biol (2002) 28:1301–10. doi: 10.1016/S0301-5629(02)00620-8
15. Aljuaid H, Alturki N, Alsubaie N, Cavallaro L, Liotta A. Computer-aided diagnosis for breast cancer classification using deep neural networks and transfer learning. Comput Methods Programs BioMed (2022) 223:106951. doi: 10.1016/j.cmpb.2022.106951
16. Hamidinekoo A, Suhail Z, Qaiser T, Zwiggelaar R. Investigating the Effect of Various Augmentations on the Input Data Fed to a Convolutional Neural Network for the Task of Mammographic Mass Classification. In: Valdés Hernández M, González-Castro V, editors. Medical Image Understanding and Analysis. Communications in Computer and Information Science. Cham: Springer International Publishing (2017). p. 398–409. doi: 10.1007/978-3-319-60964-5_35
17. Schmidhuber J. Deep learning in neural networks: An overview. Neural Networks (2015) 61:85–117. doi: 10.1016/j.neunet.2014.09.003
18. Arun Kumar S, Sasikala S. Review on deep learning-based CAD systems for breast cancer diagnosis. Technol Cancer Res Treat (2023) 22:15330338231177976. doi: 10.1177/15330338231177977
19. Yao G, Lei T, Zhong J. A review of Convolutional-Neural-Network-based action recognition. Pattern Recognition Lett (2019) 118:14–22. doi: 10.1016/j.patrec.2018.05.018
20. Dhillon A, Verma GK. Convolutional neural network: a review of models, methodologies and applications to object detection. Prog Artif Intell (2020) 9:85–112. doi: 10.1007/s13748-019-00203-0
21. Sechopoulos I, Teuwen J, Mann R. Artificial intelligence for breast cancer detection in mammography and digital breast tomosynthesis: State of the art. Semin Cancer Biol (2021) 72:214–25. doi: 10.1016/j.semcancer.2020.06.002
22. Gastounioti A, Desai S, Ahluwalia VS, Conant EF, Kontos D. Artificial intelligence in mammographic phenotyping of breast cancer risk: a narrative review. Breast Cancer Res (2022) 24:14. doi: 10.1186/s13058-022-01509-z
23. Loizidou K, Elia R, Pitris C. Computer-aided breast cancer detection and classification in mammography: A comprehensive review. Comput Biol Med (2023) 153:106554. doi: 10.1016/j.compbiomed.2023.106554
24. Schönenberger C, Hejduk P, Ciritsis A, Marcon M, Rossi C, Boss A. Classification of mammographic breast microcalcifications using a deep convolutional neural network: A BI-RADS-based approach. Invest Radiol (2021) 56:224–31. doi: 10.1097/RLI.0000000000000729
25. Howard M, Agarwal G, Lytwyn A. Accuracy of self-reports of Pap and mammography screening compared to medical record: a meta-analysis. Cancer Causes Control (2009) 20:1–13. doi: 10.1007/s10552-008-9228-4
26. Liberman L, Abramson AF, Squires FB, Glassman JR, Morris EA, Dershaw DD. The breast imaging reporting and data system: positive predictive value of mammographic features and final assessment categories. Am J Roentgenology (1998) 171:35–40. doi: 10.2214/ajr.171.1.9648759
27. Zahoor S, Lali IU, Khan MA, Javed K, Mehmood W. Breast cancer detection and classification using traditional computer vision techniques: A comprehensive review. Curr Med Imaging (2020) 16:1187–200. doi: 10.2174/1573405616666200406110547
28. Hazarika M, Mahanta LB. A new breast border extraction and contrast enhancement technique with digital mammogram images for improved detection of breast cancer. Asian Pac J Cancer Prev (2018) 19:2141–8. doi: 10.22034/APJCP.2018.19.8.2141
29. Bora VB, Kothari AG, Keskar AG. Robust automatic pectoral muscle segmentation from mammograms using texture gradient and euclidean distance regression. J Digit Imaging (2016) 29:115–25. doi: 10.1007/s10278-015-9813-5
30. CHEN Z, Gao H, pan Y, Xing F. Review of computer aided diagnosis technology in mammography. Comput Eng Appl (2022) 58:1–21. doi: 10.3778/j.issn.1002-8331.2108-0205
31. Kavitha T, Mathai PP, Karthikeyan C, Ashok M, Kohar R, Avanija J, et al. Deep learning based capsule neural network model for breast cancer diagnosis using mammogram images. Interdiscip Sci (2022) 14:113–29. doi: 10.1007/s12539-021-00467-y
32. Arora R, Rai PK, Raman B. Deep feature-based automatic classification of mammograms. Med Biol Eng Comput (2020) 58:1199–211. doi: 10.1007/s11517-020-02150-8
33. Arevalo J, González FA, Ramos-Pollán R, Oliveira JL, Guevara Lopez MA. Representation learning for mammography mass lesion classification with convolutional neural networks. Comput Methods Programs BioMed (2016) 127:248–57. doi: 10.1016/j.cmpb.2015.12.014
34. Spak DA, Plaxco JS, Santiago L, Dryden MJ, Dogan BE. BI-RADS ® fifth edition: A summary of changes. Diagn Interventional Imaging (2017) 98:179–90. doi: 10.1016/j.diii.2017.01.001
35. Rangayyan RM, Ayres FJ, Desautels JE. A review of computer-aided diagnosis of breast cancer: Toward the detection of subtle signs. J Franklin Institute (2007) 344:312–48. doi: 10.1016/j.jfranklin.2006.09.003
36. Duarte MA, Alvarenga AV, Azevedo CM, Calas MJG, Infantosi AFC, Pereira WCA. Evaluating geodesic active contours in microcalcifications segmentation on mammograms. Comput Methods Programs BioMed (2015) 122:304–15. doi: 10.1016/j.cmpb.2015.08.016
37. Guo Y, Dong M, Yang Z, Gao X, Wang K, Luo C, et al. A new method of detecting micro-calcification clusters in mammograms using contourlet transform and non-linking simplified PCNN. Comput Methods Programs BioMed (2016) 130:31–45. doi: 10.1016/j.cmpb.2016.02.019
38. Khalaf AF, Yassine IA. Novel features for microcalcification detection in digital mammogram images based on wavelet and statistical analysis. 2015 IEEE Int Conf Image Process (ICIP) (2015), 1825–9. doi: 10.1109/ICIP.2015.7351116
39. Fadil R, Jackson A, El Majd BA, El Ghazi H, Kaabouch N. Classification of microcalcifications in mammograms using 2D discrete wavelet transform and random forest. 2020 IEEE Int Conf Electro Inf Technol (EIT) (2020), 353–9. doi: 10.1109/EIT48999.2020.9208290
40. Suhail Z, Denton ERE, Zwiggelaar R. Classification of micro-calcification in mammograms using scalable linear Fisher discriminant analysis. Med Biol Eng Comput (2018) 56:1475–85. doi: 10.1007/s11517-017-1774-z
41. Kumar A, Sheshadri HS. Analysis of classifiers performance for classification of potential microcalcification. Fifth Int Conf Digital Image Process (ICDIP 2013). SPIE (2013) 8878:613–8. doi: 10.1117/12.2031479
42. Huang L, Gao X, You C. Based on the texture features of mammography images, a machine learning model was established to identify benign and Malignant breast masses. Radiologic Pract (2021) 36:480–3. doi: 10.13609/j.cnki.1000-0313.2021.04.012
43. Tourassi GD, Vargas-Voracek R, Catarious DM, Floyd CE. Computer-assisted detection of mammographic masses: a template matching scheme based on mutual information. Med Phys (2003) 30:2123–30. doi: 10.1118/1.1589494
44. Yu S-S, Tsai C-Y, Liu C-C. A breast region extraction scheme for digital mammograms using gradient vector flow Snake. 4th Int Conf New Trends Inf Sci Service Science. (2010), 715–20.
45. Li S, Dong M, Du G, Mu X. Attention dense-U-net for automatic breast mass segmentation in digital mammogram. IEEE Access (2019) 7:59037–47. doi: 10.1109/ACCESS.2019.2914873
46. Guliato D, Rangayyan RM, Carnielli WA, Zuffo JA, Desautels JEL. Segmentation of breast tumors in mammograms using fuzzy sets. JEI (2003) 12:369–78. doi: 10.1117/1.1579017
47. Meenalosini S, Janet J, Kannan E. A novel approach in Malignancy detection of computer aided diagnosis. Am J Appl Sci (2012) 9:1020. doi: 10.3844/ajassp.2012.1020.1029
48. Li Y, Zhao G, Zhang Q, Lin Y, Wang M. SAP-cGAN: Adversarial learning for breast mass segmentation in digital mammogram based on superpixel average pooling. Med Phys (2021) 48:1157–67. doi: 10.1002/mp.14671
49. Kozegar E, Soryani M, Behnam H, Salamati M, Tan T. Mass segmentation in automated 3-D breast ultrasound using adaptive region growing and supervised edge-based deformable model. IEEE Trans Med Imaging (2018) 37:918–28. doi: 10.1109/TMI.2017.2787685
50. Alam N, Oliver A, Denton ERE, Zwiggelaar R. Automatic Segmentation of Microcalcification Clusters. In: Nixon M, Mahmoodi S, Zwiggelaar R, editors. Medical Image Understanding and Analysis. Communications in Computer and Information Science. Cham: Springer International Publishing (2018). p. 251–61. doi: 10.1007/978-3-319-95921-4_24
51. Jen C-C, Yu S-S. Automatic detection of abnormal mammograms in mammographic images. Expert Syst Appl (2015) 42:3048–55. doi: 10.1016/j.eswa.2014.11.061
52. Shi P, Zhong J, Rampun A, Wang H. A hierarchical pipeline for breast boundary segmentation and calcification detection in mammograms. Comput Biol Med (2018) 96:178–88. doi: 10.1016/j.compbiomed.2018.03.011
53. Khan S, Hussain M, Aboalsamh H, Bebis G. A comparison of different Gabor feature extraction approaches for mass classification in mammography. Multimed Tools Appl (2017) 76:33–57. doi: 10.1007/s11042-015-3017-3
54. Ghazouani H, Barhoumi W. Towards non-data-hungry and fully-automated diagnosis of breast cancer from mammographic images. Comput Biol Med (2021) 139:105011. doi: 10.1016/j.compbiomed.2021.105011
55. Htay TT, Maung SS. Early Stage Breast Cancer Detection System using GLCM feature extraction and K-Nearest Neighbor (k-NN) on Mammography image. 2018 18th Int Symposium Commun Inf Technol (ISCIT). (2018), 171–5. doi: 10.1109/ISCIT.2018.8587920
56. Vijayarajeswari R, Parthasarathy P, Vivekanandan S, Basha AA. Classification of mammogram for early detection of breast cancer using SVM classifier and Hough transform. Measurement (2019) 146:800–5. doi: 10.1016/j.measurement.2019.05.083
57. Mohanty F, Rup S, Dash B. Automated diagnosis of breast cancer using parameter optimized kernel extreme learning machine. Biomed Signal Process Control (2020) 62:102108. doi: 10.1016/j.bspc.2020.102108
58. Omondiagbe DA, Veeramani S, Sidhu AS. Machine learning classification techniques for breast cancer diagnosis. IOP Conf Ser: Mater Sci Eng (2019) 495:12033. doi: 10.1088/1757-899X/495/1/012033
59. Singh B, Kaur M. An approach for classification of Malignant and benign microcalcification clusters. Sādhanā (2018) 43:39. doi: 10.1007/s12046-018-0805-2
60. Fanizzi A, Basile TMA, Losurdo L, Bellotti R, Bottigli U, Dentamaro R, et al. A machine learning approach on multiscale texture analysis for breast microcalcification diagnosis. BMC Bioinf (2020) 21:91. doi: 10.1186/s12859-020-3358-4
61. Ghasemzadeh A, Sarbazi Azad S, Esmaeili E. Breast cancer detection based on Gabor-wavelet transform and machine learning methods. Int J Mach Learn Cyber (2019) 10:1603–12. doi: 10.1007/s13042-018-0837-2
62. Naseem U, Rashid J, Ali L, Kim J, Ul Haq QE, Awan MJ, et al. An automatic detection of breast cancer diagnosis and prognosis based on machine learning using ensemble of classifiers. IEEE Access (2022) 10:78242–52. doi: 10.1109/access.2022.3174599
63. Dhahbi S, Barhoumi W, Kurek J, Swiderski B, Kruk M, Zagrouba E. False-positive reduction in computer-aided mass detection using mammographic texture analysis and classification. Comput Methods Programs BioMed (2018) 160:75–83. doi: 10.1016/j.cmpb.2018.03.026
64. Zhou K, Li W, Zhao D. Deep learning-based breast region extraction of mammographic images combining pre-processing methods and semantic segmentation supported by Deeplab v3. Technol Health Care (2022) 30:173–90. doi: 10.3233/THC-228017
65. Al-Antari MA, Han SM, Kim TS. Evaluation of deep learning detection and classification towards computer-aided diagnosis of breast lesions in digital X-ray mammograms. Comput Methods Programs BioMed (2020) 196:105584. doi: 10.1016/j.cmpb.2020.105584
66. Agarwal R, Diaz O, Lladó X, Yap MH, Martí R. Automatic mass detection in mammograms using deep convolutional neural networks. JMI (2019) 6:31409. doi: 10.1117/1.JMI.6.3.031409
67. Li HY, Chen DD, Nailon WH, Davies ME, Laurenson DI. Dual convolutional neural networks for breast mass segmentation and diagnosis in mammography. IEEE Trans Med Imaging (2022) 41:3–13. doi: 10.1109/tmi.2021.3102622
68. Escorcia-Gutierrez J, Mansour RF, Beleno K, Jimenez-Cabas J, Perez M, Madera N, et al. Automated deep learning empowered breast cancer diagnosis using biomedical mammogram images. Cmc-Computers Materials Continua (2022) 71:4221–35. doi: 10.32604/cmc.2022.022322
69. Chakravarthy SRS, Rajaguru H. SKMAT-U-Net architecture for breast mass segmentation. International Journal of Imaging Systems and Technology (2022) 32:1880–8. doi: 10.1002/ima.22781
70. Alkhaleefah M, Tan TH, Chang CH, Wang TC, Ma SC, Chang L, et al. Connected-segNets: A deep learning model for breast tumor segmentation from X-ray images. Cancers (2022) 14:4030. doi: 10.3390/cancers14164030
71. Sun LL, Sun HJ, Wang JQ, Wu S, Zhao Y, Xu Y. Breast mass detection in mammography based on image template matching and CNN. Sensors (2021) 21:2855. doi: 10.3390/s21082855
72. Su YY, Liu Q, Xie WT, Hu PZ. YOLO-LOGO: A transformer-based YOLO segmentation model for breast mass detection and segmentation in digital mammograms. Comput Methods Programs Biomedicine (2022) 221:106903. doi: 10.1016/j.cmpb.2022.106903
73. Honjo T, Ueda D, Katayama Y, Shimazaki A, Jogo A, Kageyama K, et al. Visual and quantitative evaluation of microcalcifications in mammograms with deep learning-based super-resolution. Eur J Radiol (2022) 154:110433. doi: 10.1016/j.ejrad.2022.110433
74. Zeiser FA, da Costa CA, Zonta T, Marques NMC, Roehe AV, Moreno M, et al. Segmentation of masses on mammograms using data augmentation and deep learning. J Digit Imaging (2020) 33:858–68. doi: 10.1007/s10278-020-00330-4
75. Zhang C, Zhao J, Niu J, Li D. New convolutional neural network model for screening and diagnosis of mammograms. PloS One (2020) 15:e0237674. doi: 10.1371/journal.pone.0237674
76. Shen R, Zhou K, Yan K, Tian K, Zhang J. Multicontext multitask learning networks for mass detection in mammogram. Med Phys (2020) 47:1566–78. doi: 10.1002/mp.13945
77. Niu J, Li H, Zhang C, Li D. Multi-scale attention-based convolutional neural network for classification of breast masses in mammograms. Med Phys (2021) 48:3878–92. doi: 10.1002/mp.14942
78. Baccouche A, Garcia-Zapirain B, Elmaghraby AS. An integrated framework for breast mass classification and diagnosis using stacked ensemble of residual neural networks. Sci Rep (2022) 12:12259. doi: 10.1038/s41598-022-15632-6
79. Leong YS, Hasikin K, Lai KW, Mohd Zain N, Azizan MM. Microcalcification discrimination in mammography using deep convolutional neural network: towards rapid and early breast cancer diagnosis. Front Public Health (2022) 10:875305. doi: 10.3389/fpubh.2022.875305
80. Rodriguez-Ruiz A, Teuwen J, Chung K, Karssemeijer N, Chevalier M, Gubern-Merida A, et al. Pectoral muscle segmentation in breast tomosynthesis with deep learning. In: Medical Imaging 2018: Computer-Aided Diagnosis. SPIE (2018). p. 564–70. doi: 10.1117/12.2292920
81. Kooi T, Gubern-Merida A, Mordang J-J, Mann R, Pijnappel R, Schuur K, et al. A comparison between a deep convolutional neural network and radiologists for classifying regions of interest in mammography. Breast Imaging: 13th Int Workshop IWDM 2016 Malmö Sweden June 19-22 2016 Proc 13. Springer (2016), 51–6. doi: 10.1007/978-3-319-41546-8_7
82. Dhungel N, Carneiro G, Bradley AP. Automated mass detection in mammograms using cascaded deep learning and random forests. 2015 Int Conf Digital Image Computing: Techniques Appl (DICTA) (2015), 1–8. doi: 10.1109/DICTA.2015.7371234
83. Zhu W, Lou Q, Vang YS, Xie X. Deep Multi-instance Networks with Sparse Label Assignment for Whole Mammogram Classification. In: Descoteaux M, Maier-Hein L, Franz A, Jannin P, Collins DL, Duchesne S, editors. Medical Image Computing and Computer Assisted Intervention – MICCAI 2017. Lecture Notes in Computer Science. Cham: Springer International Publishing (2017). p. 603–11. doi: 10.1007/978-3-319-66179-7_69
84. Jg E, Ck W, Ch L, Dh H, Ar F. Variability in radiologists’ interpretations of mammograms. New Engl J Med (1994) 331:1493–1499. doi: 10.1056/NEJM199412013312206
85. Esteva A, Robicquet A, Ramsundar B, Kuleshov V, DePristo M, Chou K, et al. Dean J. A guide to deep Learn healthcare. Nat Med (2019) 25:24–9. doi: 10.1038/s41591-018-0316-z
Keywords: breast cancer, machine learning, mammogram image, deep learning, diagnose
Citation: Gao Y, Lin J, Zhou Y and Lin R (2023) The application of traditional machine learning and deep learning techniques in mammography: a review. Front. Oncol. 13:1213045. doi: 10.3389/fonc.2023.1213045
Received: 28 April 2023; Accepted: 25 July 2023;
Published: 11 August 2023.
Edited by:
Quing Zhu, Washington University in St. Louis, United StatesReviewed by:
Aimilia Gastounioti, Washington University in St. Louis, United StatesCopyright © 2023 Gao, Lin, Zhou and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rongjin Lin, cm9uZ2psaW5AZmptdS5lZHUuY24=
†These authors contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.