
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol., 24 October 2023
Sec. Cancer Immunity and Immunotherapy
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1210297
This article is part of the Research TopicSex Differences in Cancer Incidence, Mortality, and Survival: Methodological PerspectivesView all 15 articles
 Vianey Rodriguez-Lara1*
Vianey Rodriguez-Lara1* Giovanny Soca-Chafre2
Giovanny Soca-Chafre2 Maria Rosa Avila-Costa3
Maria Rosa Avila-Costa3 Juan Jose Juarez-Vignon Whaley4
Juan Jose Juarez-Vignon Whaley4 Jeronimo Rafael Rodriguez-Cid4
Jeronimo Rafael Rodriguez-Cid4 José Luis Ordoñez-Librado3
José Luis Ordoñez-Librado3 Emma Rodriguez-Maldonado5Nallely A. Heredia-Jara1
Emma Rodriguez-Maldonado5Nallely A. Heredia-Jara1Currently, immunotherapy based on PD-1/PD-L1 pathway blockade has improved survival of non-small cell lung cancer (NSCLC) patients. However, differential responses have been observed by sex, where men appear to respond better than women. Additionally, adverse effects of immunotherapy are mainly observed in women. Studies in some types of hormone-dependent cancer have revealed a role of sex hormones in anti-tumor response, tumor microenvironment and immune evasion. Estrogens mainly promote immune tolerance regulating T-cell function and modifying tumor microenvironment, while androgens attenuate anti-tumor immune responses. The precise mechanism by which sex and sex hormones may modulate immune response to tumor, modify PD-L1 expression in cancer cells and promote immune escape in NSCLC is still unclear, but current data show how sexual differences affect immune therapy response and prognosis. This review provides update information regarding anti-PD-1/PD-L immunotherapeutic efficacy in NSCLC by sex, analyzing potential roles for sex hormones on PD-L1 expression, and discussing a plausible of sex and sex hormones as predictive response factors to immunotherapy.
Lung cancer (LC) holds the highest cancer-related incidence and mortality worldwide and is expected to reach 3.2 million deaths globally in 2050 (1). The LC prognosis after diagnosis remains poor, and the 5-year survival rate is less than 20% (2). LC is classified into small (SCLC, 15%) and non-small types (NSCLC, 85%) (3–5). NSCLC exhibits several differences by sex; since women are frequently non-smoker, diagnosed at younger age, and present adenocarcinoma with EGFR mutations. Women also respond better to chemotherapy and men to immunotherapy, whereas outcomes and survival are significantly better in women (4, 6–8). Furthermore, NSCLC is influenced by sex hormones, mainly estrogens (4, 9).
Targeted and immune therapies have increased LC patients’ survival (10). Median overall survival (OS) for chemotherapy is less than a year, while combined with immunotherapy, OS almost doubles (11). PD-1/PD-L1 based immunotherapy improves NSCLC survival, however sex-derived differences have been reported, suggesting sex as a potential predictor for immunotherapy response (12–14). Sex hormones regulate immune response modifying PD-L1 expression, however in LC this relation is still being explored. This article focuses on PD-1/PD-L1 NSCLC immunotherapy, discussing sex differences in response to PD-L1 blockade, as well as sex-related effects and sex hormones impact on the PD-1/PD-L1 pathway and therapeutic responses implications.
PD-1 is a transmembrane protein from the CD28/CTLA-4 immunoglobulin family expressed on different immune cells. PD-1 controls immune responses and T-cell activation, proliferation, and effector activity by binding PD-L1/2. Cancer cells inactivate T-cells and accomplish immune evasion through PD-L1 expression (15, 16). Intrinsic PD-L1 regulation includes genetic (transcriptional regulation through KRAS, EGFR, ALK pathways) and epigenetic factors (DNMT1, HDAC, miR-135). Conversely, cytokines (INF-γ), growth factors (EGF, VEGF), hypoxia, post-translational modifications (phosphorylation, glycosylation, palmitoylation, ubiquitination), and even treatments including chemotherapy, radiotherapy, and tyrosine kinase inhibitors, extrinsically modify PD-L1 expression (16, 17).
Among several immune evasion mechanisms, tumor PD-L1 expression alone induces immune escape, inactivating cytotoxic T-cells (18). Therefore, this pathway is an important therapeutic target for multiple cancers including NSCLC, since PD-1/PD-L1 blockade restores immune response increasing patient survival. To date, six PD-1/PD-L1 inhibitors have been approved including nivolumab, pembrolizumab, cemiplimab (anti-PD-1), atezolizumab, durvalumab, and avelumab (anti-PD-L1) (19).
LC diagnosis and treatment has developed substantially over the last decade, improving OS, progression-free survival (PFS), treatment response, and quality of life. NSCLC patients undergo EGFR, KRAS and ALK genes mutation. Unfortunately, not all patients are targeted therapies candidates, and may appear mutations resistance and recurrence. In this context, immune PD-1/PD-L1 inhibitors, have completely changed NSCLC management.
Baseline PD-L1 levels stratifies patients with a potentially better response. A higher PD-L1 tumor proportion score (TPS) correlates with improved outcomes. Among NSCLC patients with PD-L1 ≥ 50% treated with pembrolizumab, those with 90-100% PD-L1 TPS show better response (20).
For patients with elevated PD-L1 (≥50%), treatment includes immunotherapy as monotherapy, chemoimmunotherapy, or dual immunotherapy. Those with PD-L1 ≥ 50% without EGFR/ALK mutations who received pembrolizumab had greater OS compared with chemotherapy (30 vs 14.2 months) (21). Pembrolizumab also resulted in longer OS compared to other PD1-/PD-L1 inhibitors (26.3 vs. ≤14 months). Additionally, pembrolizumab improved OS combined with chemotherapy and radiotherapy (22, 23). Dual immunotherapy has exhibited durable benefits in OS and PFS regardless of PD-L1 expression compared to chemotherapy (24, 25). Combined immunotherapy or dual immunotherapy might also increase adverse effects (AE) (26).
Moreover, PD-L1 blockade has improved OS and PFS regardless of PD-L1 levels. Low PD-L1 (1-49%) cases are treated with immunotherapy + chemotherapy or dual immunotherapy (25, 27). More patients reached 12-months OS in pembrolizumab plus chemotherapy compared to the placebo (69.2% vs. 49.9%) irrespective of PD-L1 levels (28). Similarly, the IMpower 150 showed atezolizumab + chemotherapy increased OS and PFS independently of PD-L1 levels (29).
Finally, patients with negative (<1%) PD-L1 are still candidates for combined immunotherapy with chemotherapy or targeted therapy and dual immunotherapy (25, 30, 31). PD-L1 blockade has significantly improved clinical outcomes mainly in patients with higher PD-L1 levels. However, PD-L1inhibitors are considered the choice treatment even in those without PD-L1 expression, making these agents the LC new gold standard therapy.
Although PD-1/PD-L1 blockade improved survival compared to chemotherapy and targeted therapy, sex-related differences have been reported (13, 14, 32). A systematic review (11,351 patients; 67% men and 37% women) showed different ICI efficacy by sex in melanoma and NSCLC. The pooled OS hazard ratio (HR) of ICI treatment was higher for women (12). Moreover, 4 NSCLC trials (1,672 patients; 73.2% men and 26.8 women) evaluated pooled OS-HR of PD1/PD-L1 ICI vs chemotherapy, resulting higher risk for females (13) Women also experience more immunotherapy AE (33).This data suggests a significant benefit of ICIs in males. Conversely, women with advanced NSCLC responded better to chemotherapy+PD-1/PD-L1-immunotherapy than men who benefited from PD-L1 blockade monotherapy (14).
A systematic review of trials and observational studies reported improved survival for male patients after pembrolizumab/nivolumab as monotherapy. Otherwise, women experienced increased survival rates, in chemoimmunotherapy (34). Additionally, the pooled HRs comparing ICIs vs chemotherapy were 0.74 (95% CI0.67-0.81) for men and 0.83 (95% CI 0.73-0.95) for women (35). Better PFS was also observed in advanced NSCLC male patients treated with ICI (5 months vs 4). Nivolumab exhibited significantly higher PFS in males vs. females also disease control rate was higher in male (55.7 vs 45.7%) and their disease progression was lower (44.3 vs 54.3%) (36). All above, supports the increased benefit of ICIs monotherapy for males and ICIs+chemotherapy for female patients.
Contradictory results have also emerged, showing no sex differences in response to immunotherapy as monotherapy or combined. A study involving advanced NSCLC patients treated with ICI monotherapy and ICI+chemotherapy observed no differences in PFS by sex, although differences in prognostic factors were noticed (37). Additionally, no sex-related differences were observed in squamous cell NSCLC patients treated with chemotherapy+PD-L1-inhibitors, although different AE were observed by sex (38).
A higher response to chemotherapy has been reported in women than in men (39, 40). Differences in DNA repair capacity between sexes (41) could explain women’s higher sensitivity to chemotherapy (42). Additionally, chemotherapy might improve immunotherapy by enhancing anti-tumor immune response, recruiting, and activating cytotoxic T-cells, inducing immunogenic cell death, releasing tumor antigens and damage-associated molecular patterns, activating dendritic cells, and reducing T regulatory cells (Treg). But chemotherapy enhancing effects to immunotherapy are produced when administered locally since systemic chemotherapy produces high non-specific toxicity (43, 44). These facts could explain the higher chemotherapy response plus immunotherapy observed in women. Higher sensitivity to immunotherapy as monotherapy in men could be explained by disparities in PD-L1 expression.
Some confounding variables including previous treatments, tumor mutational burden (TMB), and smoking habit could explain the controversial response to ICI by sex. Since, there is a sex bias in NSCLC features, it is critical to elucidate sex effects on immunotherapy responses to improve future therapies.
Sex determines diverse conditions, including lifestyle and toxicant exposure, as well as genetic, and immune features that modify cancer biomarker expression, promoting significant differences in treatment response, including PD-L1 inhibitors. Ye et al., found differences by sex in immune characteristics impacting NSCLC immunotherapy (45).
Several studies show sex differences in PD-L1 levels, which might explain LC immunotherapy response disparities (46–49). A high percentage of PD-L1 positive NSCLC tumors correspond to men, who exhibit higher PD-L1 TPS than females (48–51). Fu et al., reported 18.3% of women with NSCLC vs 26% of men with PD-L1 TPS of 1-49%, and only 5.5% of women vs 17% of men with PD-L1 TPS ≥ 50% (49). Lin et al., reported 13.6% of men with high PD-L1 TPS (≥50%) vs. only 3.8% in females NSCLC patients (52). These findings have been supported by several studies summarized in Table 1 (47–55). Conversely, no association between PD-L1 expression and sex has also been reported (56). Despite the discrepancies, accumulating evidence discloses differences by sex in PD-L1 status in NSCLC (40, 42, 44–49).
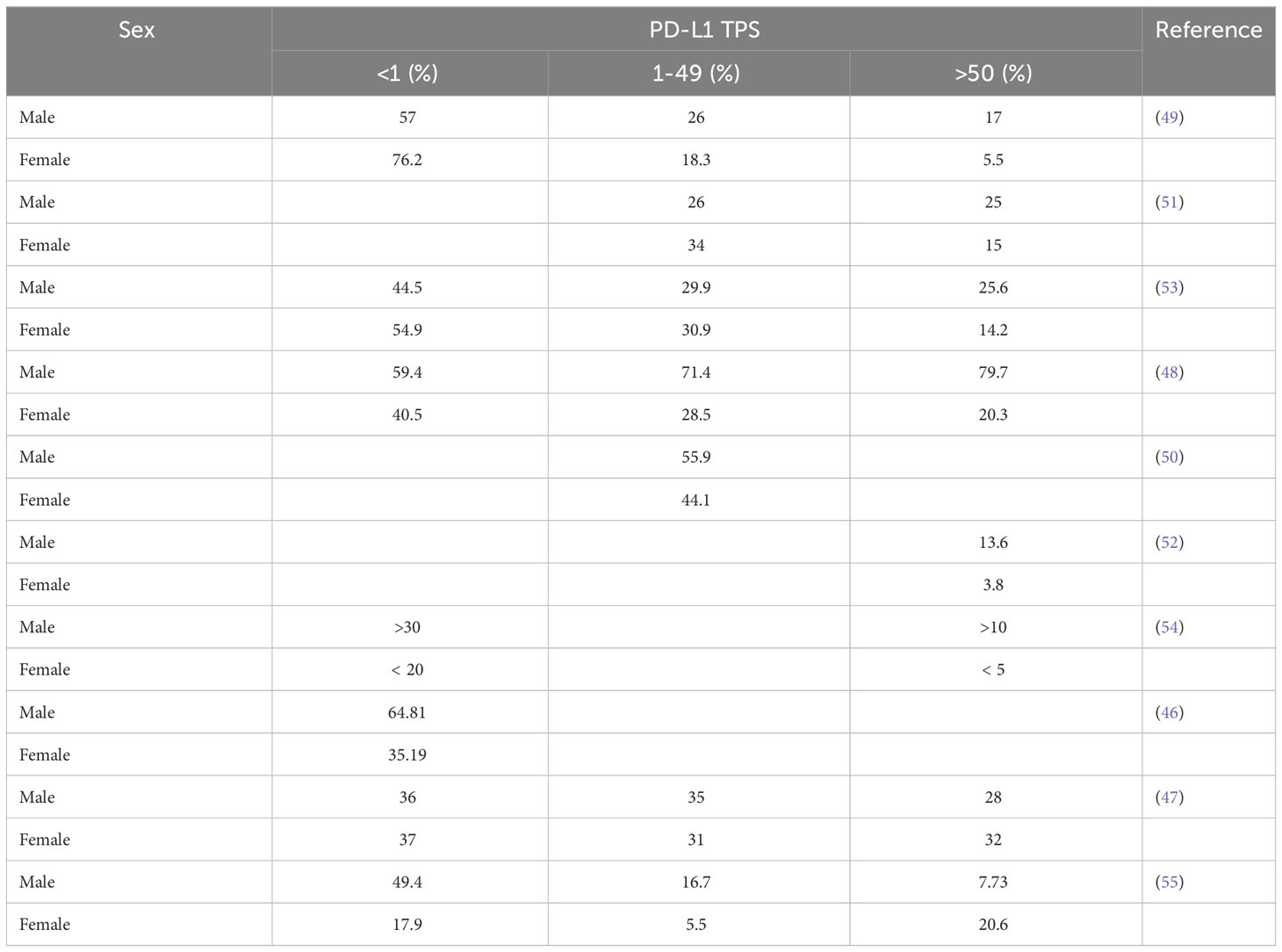
Table 1 Differences in PD-L1 expression by sex in NSCLC patients.
Some intrinsic and extrinsic sex factors might drive differences in PD-L1 levels. Smoking status, generally associated with LC male patients, has been related to PD-L1 expression. High PD-L1 TPS was correlated with smoking history and better immunotherapy response. Smoking patients presented higher and prolonged OS and PFS in ICI vs. chemotherapy (57–62). KRAS mutation and squamous histology associate with PD-L1 expression, and tobacco smoking could partially explain differences in PD-L1 levels in NSCLC patients by sex (63). Further studies are needed to confirm sex differences in PD-L1 levels and factors affecting its expression. More women must be integrated into studies, being generally underrepresented. Also, TMB, histology, smoking status, and hormonal factors should be considered.
Steroids sex hormones participate in several carcinogenic pathways in LC and could probably play a role in sex PD-L1 disparities (64, 65). Although many LC patients exhibit low sex hormone levels (mainly estrogen) due to age and menopause, lung tumors produce sex hormones locally through aromatase (ARO) overexpression (66–69). ARO and hormone receptors could modify PD-L1 expression regardless of sex and hormonal status.
The estrogen pathway has taken relevance in NSCLC given its role in lung carcinogenesis. Estrogen receptor (ER)-β, the most common LC isoform and ARO expression, correlate with poor prognosis and survival (68). ERβ is overexpressed in 60-80% of male and female NSCLC patients. Estrogen (E2), through its nuclear receptors (ERα/ERβ) and G-protein-coupled estrogen receptor (GPER), promotes LC progression by cell proliferation, apoptosis resistance, angiogenesis, epithelial mesenchymal transition (EMT), cell migration and metastases (4, 9, 70, 71). Moreover, an important role for estrogen related receptor alpha (ERRα) has been reported in NSCLC, which stimulates proliferation and EMT (72, 73).
E2 also modifies tumor microenvironment through pro-inflammatory cytokines and recruiting Tregs promoting immune evasion (74). Additionally, E2 up-regulates chemokine receptor CXCR4, contributing to immune evasion and metastases in NSCLC (75, 76). Currently the role of E2 in immune evasion and PD-L1 control in LC is being explored.
Estrogens downregulate PD-L1 expression in endometrial and breast cancer (BC) and correlates with ER-negative status in BC (77, 78). In MCF-7 cells, E2 negatively regulated PD-L1 transcription (79). Moreover, antiestrogens increased PD-L1 expression in ER+ BC (80). E2 probably decreases PD-L1 expression through IL-17 signaling (77). Also, E2/GPER pathway downregulated PD-L1 through COP9-signalosome subunit 5 degradation, as reported in melanoma and pancreatic ductal adenocarcinoma (81, 82).
Paradoxically, PD-L1 expression correlated with ER+, PR+, and Ki67+ in BC (83). E2/ERα increased PD-L1 but not PD-L2 expression in endometrial and BC. PD-L1 expression may be controlled through the PI3K/AKT pathway and post-transcriptional PD-L1-mRNA stabilization in BC (84). In metastatic renal cell carcinoma nivolumab increased E2 levels in male patients (85). Decreased PD-L1 levels by nivolumab increase IL-6 in melanoma animal models, consequently, increasing E2 synthesis and promoting immune evasion (85–87).
In melanoma and prostate cancer (PC), estrogen receptor modulators (SERMs) have been suggested to improve immunotherapy (88, 89). Besides, SERMs and degraders (SERDs) significantly improved immunotherapy efficacy in BC, suggesting an E2 role in up-regulated PD-L1 (90).
Estrogen mechanisms modifying PD-L1 seem to be complex and may depend on several factors such as cancer type, histology, TMB, ER isoforms, ARO expression, estrogen levels, and microenvironmental features (Figure 1). This relationship needs to be explored since E2 pathway blocking could improve immunotherapy in some cancers, including NSCLC.
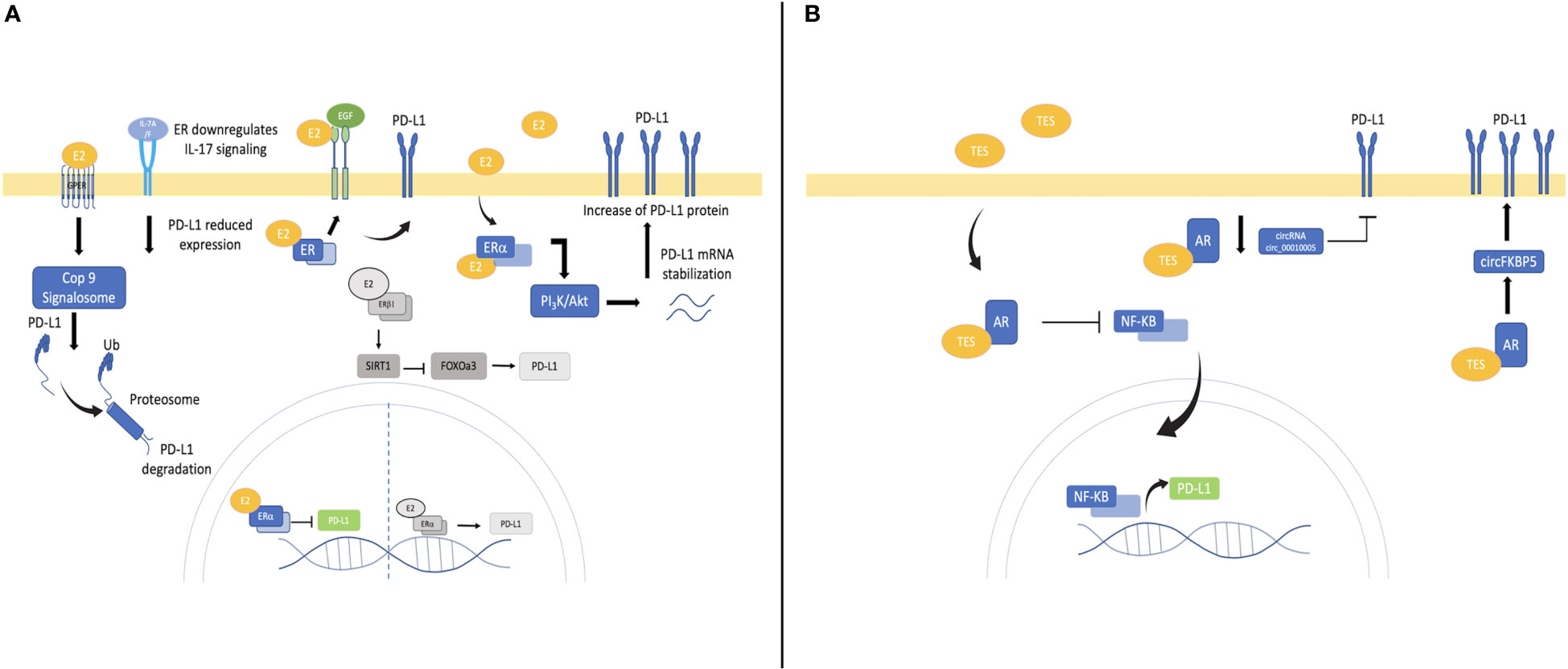
Figure 1 Mechanisms involved in PD-L1 control by estrogen and androgen in cancer and NSCLC. (A) Estrogen pathway downregulates PD-L1 by repressing its transcription, promoting its proteosomal degradation and IL-17 downregulation. E2/ER also activates the PI3k/Akt pathway promoting RNA stabilization and increasing PD-L1 protein as observed in breast cancer. E2/ER through EGFR/EGF pathway might stimulate PD-L1 increase in lung cancer. Emerging mechanisms by E2 pathway might up-regulates PD-L1 in NSCLC are represented in gray. E2/ERα increases PD-L1 transcription. Moreover, E2/ERβ activates SIRT1 promoting FOXOa3 degradation and consequently PD-L1 increases (B) Androgen pathway downregulates PD-L1 transcriptionally, mainly by inhibiting NF-kB translocation and decreasing promoter activation. AR regulates PD-L1 expression post-transcriptionally by modifying circRNAs.
The E2 role in NSCLC immune evasion has been scarcely investigated, and its PD-L1 relationship is emerging. For instance, E2 reduced cytotoxic lymphocyte activity by inducing ERβ1/5. Also, E2 up-regulated PD-L1 by increasing ERβ/SIRT1, Snail transcriptional factor while reducing FOXO3a (91). ERβ could be a critical target to improve immunotherapy given its higher expression in male and female NSCLC patients.
E2/ERα increased PD-L1 transcription was recently reported in vitro. Additionally, in vivo, letrozole (ARO inhibitor) improved pembrolizumab efficacy, while in NSCLC patients, ERα was a predictive response factor to pembrolizumab, even stronger than sex and PD-L1 levels (92). This could be explained by high ER expression independently of sex in NSCLC (9). Thus, ER could become a biomarker to predict to immunotherapy response in NSCLC.
Decreased levels of the receptor for advanced glycation end products (RAGE) associate with lung carcinogenesis and metastasis regulating PI3K/AKT and KRAS-RAF1 signaling. RAGE participates in redox regulation, and its polymorphisms are linked to LC incidence and progression (93). Thus, RAGE is an important axis in LC development. Recently it was reported that HMGB-RAGE promotes PD-L1 expression in BC (94). Also, E2 treatment up-regulated RAGE in human microvascular endothelial cells (94). The association between E2, RAGE and PD-L1 in NSCLC has not been elucidated; however, it could represent a key mechanism underlying carcinogenesis and immune evasion.
Besides, estrogens could modify PD-L1 in NSCLC through the EGFR pathway. EGFR/EGF activation increases E2 through ARO up-regulation (9, 67, 95). Since EGF enhancing PD-L1 in NSCLC (96), E2 could stimulates PD-L1 through the EGF/EGFR pathway; however, this hypothesis needs to be tested.
Differences in serum PD-1 (sPD-1) by sex were reported in NSCLC patients, where females exhibited higher sPD-1 and PD-1 on CD4+ T cells. Increased testosterone levels were also reported (97) suggesting sex hormones could control PD-1.
All these data support E2 contribution to immune evasion up-regulating PD-L1 through diverse mechanisms involving both ERα/ERβ in NSCLC (Figure 1). Antiestrogens could improve immunotherapy even in low PD-L1 conditions due to high ER expression in NSCLC. This is a new approach showing how estrogen pathway promotes lung carcinogenesis and how antiestrogens could improve immunotherapy as well as targeted therapy. However further studies are warranted to explore these mechanisms and their potential therapeutic impact.
LC androgen participation is still poorly explored and contradictory. Androgen receptor (AR) is downregulated in NSCLC tissues and cell lines, without differences by sex and staining. Higher AR levels associate to better survival rates. miR-224-5p is up-regulated in NSCLC promoting proliferation, decreased apoptosis, migration, and metastasis by, downregulating AR (98). Furthermore, AR+ status relate to favorable OS in NSCLC metastatic disease (99), not in early stages (100).
On the other hand, AR was overexpressed mainly in NSCLC male patients (101). AR was detected in 20% of LC patients; higher levels were in advanced LC stages associated with progression and metastasis (102). Moreover, targeting androgen pathway in NSCLC patients resulted in better survival (103), and reduced risk to second primary LC for PC patients (104). Androgen deprivation therapy (ADT) for PC, improved survival in NSCLC after diagnosis, particularly in Caucasians (105). In vitro, androgen up-regulated gene expression involved in DNA repair, oxygen transport, apoptosis, and hemoglobin synthesis while downregulated CYP1A1 (106). Also, AR promotes proliferation through cyclin D1 regulation, stimulate migration and invasion and regulates OCT-4 protein supporting stemness (101, 107, 108). Finally, KRAS mutational profiles are linked to AR levels in NSCLC (109). Despite controversial data, androgen pathway apparently plays an important role in lung carcinogenesis highlighting its therapeutic potential.
Although men appear to respond better to immunotherapy in NSCLC, androgen activity on immune response, evasion mechanisms and PD-L1 expression in LC has not been elucidated. However, AR down-regulates PD-L1 across different malignances.
Inverse correlation between AR and PD-L1 levels has been reported in muscle invasive or metastatic urothelial (110), thyroid (111) and hepatocellular carcinomas (112), suggesting PD-L1 downregulation through the AR pathway. In thyroid cancer, dihydrotestosterone reduced PD-L1 in a time- and dose-dependent manner, while flutamide (AR antagonist) restored PD-L1 expression. AR could decrease PD-L1 expression inhibiting NF-kB nuclear translocation and reducing PD-L1 promoter activation (111). In hepatocellular carcinoma AR downregulates PD-L1 acting as PD-L1 transcriptional repressor (112). In contrast, in bladder cancer targeting AR enhances NK activity decreasing PD-L1 expression; both anti-androgen treatment and knockdown significantly reduced PD-L1 expression and stimulated NK cell-mediated bladder cancer cell death by downregulating circRNA circ_0001005 (113). Also, Tang and coworkers (114) demonstrated how dihydrotestosterone/AR higher dose increased PD-L1 expression and suppressed NK cells immunotherapy efficacy in castration- resistant PC cells (CRPC) (Figure 1). AR-blockade improved sex-bias BRAF/MEK-targeted therapy response in melanoma (115), and enhanced CD8/T-cells activity in CRPC improving PD-1/PD-L1-inhibitors response (116), suggesting that AR promote targeted and immunotherapy resistance, and shows sex impact in treatment.
Although androgen immunosuppressive effects have been documented, and ADT improves PC immunotherapy (117), its relationship with PD-L1 in clinical and experimental conditions remains contradictory. Future studies are necessary to clarify androgen´s impact on PD-L1control in NSCLC, since PD-L1 is a key target in immunotherapy, to which men appear to respond better.
NSCLC is a significantly different disease between women and men, influenced by sex hormones. The estrogen and androgen roles in NSCLC immune response is not completely understood. Currently, data remain contradictory on differential response to PD-L1-based immunotherapy sex-related. Nevertheless, several studies show higher benefit in male NSCLC patients which could be explained by higher PD-L1 levels. Sex could be a predictive response factor to NSCLC immunotherapy; however, sex-derived differences must be validated as well as consistency across different populations, equilibrated groups by sex, histological subtypes, mutational profiles, and smoking status. Additionally, women should be stratified by hormonal status and serum hormonal levels could be measured to clarify the sex and sex hormones impact on PD-L1 control and immunotherapy responses.
Some factors sex-associated as TMB and tobacco smoking modify PD-L1 which partially explains immunotherapy differential responses. Hormones, mainly estrogen also affect the PD-L1 pathway in NSCLC. Although PD-L1 control by E2 remains controversial in different cancers; in NSCLC emerging data shows E2/ER up-regulates PD-L1 suggesting that SERDs might enhance NSCLC immunotherapy response. Studies on sex and sex hormones effects in immune evasion are critical, since antihormonal therapy might be easily extrapolated to NSCLC treatment, but a wide gap still exists in this field. Androgen effect on immune evasion mechanisms through PD-1/PD-L1 in NSCLC remains to be elucidated.
Finally, all this data shows the sex and sex hormones relevance in LC progression and its impact on PD-L1 based immunotherapy response. However, it is essential to strength research on sex-related differences to understand LC behavior, identify biomarkers, predict immunotherapy response, and establish better therapeutic guidelines according to sex and hormonal status.
VR-L designed, wrote, review, edited the manuscript, made the final version and coordinated teamwork. All authors contributed to the article by writing or final editing of the manuscript. All authors contributed to the article and approved the submitted version.
VR-L thanks to PAPIIT-DGAPA UNAM IN212021grant, and DIVISION DE INVESTIGACIÓN, FACULTAD DE MEDICINA, UNAM.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sharma R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int J Clin Oncol (2022) 27(4):665–75. doi: 10.1007/s10147-021-02108-2
2. Tsai CH, Kung PT, Kuo WY, Tsai WC. Effect of time interval from diagnosis to treatment for non-small cell lung cancer on survival: a national cohort study in Taiwan. BMJ Open (2020) 10(4):e034351. doi: 10.1136/bmjopen-2019-034351
3. Barta JA, Powell CA, Wisnivesky JP. Global epidemiology of lung cancer. Ann Glob Health (2019) 85(1):8. doi: 10.5334/aogh.2419
4. Rodriguez-Lara V, Avila-Costa MR. An overview of lung cancer in women and the impact of estrogen in lung carcinogenesis and lung cancer treatment. Front Med (Lausanne) (2021) 8:600121. doi: 10.3389/fmed.2021.600121
5. Ganti AK, Klein AB, Cotarla I, Seal B, Chou E. Update of incidence, prevalence, survival, and initial treatment in patients with non–small cell lung cancer in the US. JAMA Oncol (2021) 7(12):1824–32. doi: 10.1001/jamaoncol.2021.4932
6. Mederos N, Friedlaender A, Peters S, Addeo A. Gender-specific aspects of epidemiology, molecular genetics and outcome: lung cancer. ESMO Open (2020) 5(Suppl 4):e000796. doi: 10.1136/esmoopen-2020-000796
7. Stabellini N, Bruno DS, Dmukauskas M, Barda AJ, Cao L, Shanahan J, et al. Sex differences in lung cancer treatment and outcomes at a large hybrid academic-community practice. JTO Clin Res Rep (2022) 3(4):100307. doi: 10.1016/j.jtocrr.2022.100307
8. Rodriguez-Lara V, Ramirez-Tirado LA, Barron F, Zatarain-Barron ZL, Flores-Estrada D, Arrieta O. Characteristics of non-small cell lung cancer: differences by sex and hormonal status in a Mexican population. Salud Publica Mex (2019) 61(3):265–75. doi: 10.21149/10094
9. Rodriguez-Lara V, Hernandez-Martinez JM, Arrieta O. Influence of estrogen in non-small cell lung cancer and its clinical implications. J Thorac Dis (2018) 10(1):482–97. doi: 10.21037/jtd.2017.12.61
10. Punekar SR, Shum E, Grello CM, Lau SC, Velcheti V. Immunotherapy in non-small cell lung cancer: Past, present, and future directions. Front Oncol (2022) 12:877594. doi: 10.3389/fonc.2022.877594
11. Shokoohi A, Al-Hashami Z, Moore S, Pender A, Wong SK, Wang Y, et al. Effect of targeted therapy and immunotherapy on advanced nonsmall-cell lung cancer outcomes in the real world. Cancer Med (2022) 11(1):86–93. doi: 10.1002/cam4.4427
12. Conforti F, Pala L, Bagnardi V, de Pas T, Martinetti M, Viale G, et al. Cancer immunotherapy efficacy and patients’ sex: a systematic review and meta-analysis. Lancet Oncol (2018) 19(6):737–46. doi: 10.1016/S1470-2045(18)30261-4
13. Conforti F, Pala L, Pagan E, Corti C, Bagnardi V, Queirolo P, et al. Sex-based differences in response to anti-PD-1 or PD-L1 treatment in patients with non-small-cell lung cancer expressing high PD-L1 levels. A systematic review and meta-analysis of randomized clinical trials. ESMO Open (2021) 6(5):100251. doi: 10.1016/j.esmoop.2021.100251
14. Conforti F, Pala L, Bagnardi V, Viale G, de Pas T, Pagan E, et al. Sex-based heterogeneity in response to lung cancer immunotherapy: A systematic review and meta-analysis. JNCI J Natl Cancer Inst (2019) 111(8):772. doi: 10.1093/jnci/djz094
15. Patsoukis N, Wang Q, Strauss L, Boussiotis VA. Revisiting the PD-1 pathway. Sci Adv (2020) 6(38):eabd2712. doi: 10.1126/sciadv.abd2712
16. Lamberti G, Sisi M, Andrini E, Palladini A, Giunchi F, Lollini PL, et al. The mechanisms of PD-L1 regulation in non-small-cell lung cancer (NSCLC): which are the involved players? Cancers (Basel) (2020) 12(11):1–21. doi: 10.3390/cancers12113129
17. Han Y, Liu D, Li L. PD-1/PD-L1 pathway: current researches in cancer. Am J Cancer Res (2020) 10(3):727–42.
18. Juneja VR, McGuire KA, Manguso RT, LaFleur MW, Collins N, Nicholas Haining W, et al. PD-L1 on tumor cells is sufficient for immune evasion in immunogenic tumors and inhibits CD8 T cell cytotoxicity. J Exp Med (2017) 214(4):895. doi: 10.1084/jem.20160801
19. Vaddepally RK, Kharel P, Pandey R, Garje R, Chandra AB. Review of indications of FDA-approved immune checkpoint inhibitors per NCCN guidelines with the level of evidence. Cancers (Basel) (2020) 12(3):1–19. doi: 10.3390/cancers12030738
20. Aguilar EJ, Ricciuti B, Gainor JF, Kehl KL, Kravets S, Dahlberg S, et al. Outcomes to first-line pembrolizumab in patients with non-small-cell lung cancer and very high PD-L1 expression. Ann Oncol (2019) 30(10):1653–9. doi: 10.1093/annonc/mdz288
21. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fülöp A, et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol (2019) 37(7):537–46. doi: 10.1200/JCO.18.00149
22. Tang S, Qin C, Hu H, Liu T, He Y, Guo H, et al. Immune checkpoint inhibitors in non-small cell lung cancer: progress, challenges, and prospects. Cells (2022) 11(3):320. doi: 10.3390/cells11030320
23. Reck M, Rodríguez-Abreu; D, Robinson AG, Hui R, Csoszi T, Fülöp A, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ‡ 50%. J Clin Oncol (2021) 39:2339–49. doi: 10.1200/JCO.21.00174
24. Alifu M, Tao M, Chen X, Chen J, Tang K, Tang Y. Checkpoint inhibitors as dual immunotherapy in advanced non-small cell lung cancer: a meta-analysis. Front Oncol (2023) 13:1146905. doi: 10.3389/fonc.2023.1146905
25. Paz-Ares LG, Ramalingam SS, Ciuleanu TE, Lee JS, Urban L, Bernabe Caro R, et al. First-line nivolumab plus ipilimumab in advanced NSCLC: 4-year outcomes from the randomized, open-label, phase 3 checkMate 227 part 1 trial. J Thorac Oncol (2022) 17(2):289–308. doi: 10.1016/j.jtho.2021.09.010
26. Shen X, Huang S, Xiao H, Zeng S, Liu J, Ran Z, et al. Efficacy and safety of PD-1/PD-L1 plus CTLA-4 antibodies ± other therapies in lung cancer: a systematic review and meta-analysis. Eur J Hosp Pharm (2023) 30(1):3–8. doi: 10.1136/ejhpharm-2021-002803
27. Li X, Yan S, Yang J, Wang Y, Lv C, Li S, et al. Efficacy and safety of PD-1/PD-L1 inhibitors plus chemotherapy versus PD-1/PD-L1 inhibitors in advanced non-small cell lung cancer: A network analysis of randomized controlled trials. Front Oncol (2021) 10:574752. doi: 10.3389/fonc.2020.574752
28. Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. New Engl J Med (2018) 378(22):2078–92. doi: 10.1056/NEJMoa1801005
29. Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. New Engl J Med (2018) 378(24):2288–301. doi: 10.1056/NEJMoa1716948
30. Peng L, Liang WH, Mu DG, Xu S, Hong SD, Stebbing J, et al. First-line treatment options for PD-L1–negative non-small cell lung cancer: A bayesian network meta-analysis. Front Oncol (2021) 11:657545. doi: 10.3389/fonc.2021.657545
31. Ando K, Kishino Y, Homma T, Kusumoto S, Yamaoka T, Tanaka A, et al. Nivolumab plus Ipilimumab versus Existing Immunotherapies in Patients with PD-L1-Positive Advanced Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Cancers (2020) 12(7):1905. doi: 10.3390/cancers12071905
32. Pinto JA, Vallejos CS, Raez LE, Mas LA, Ruiz R, Torres-Roman JS, et al. Gender and outcomes in non-small cell lung cancer: an old prognostic variable comes back for targeted therapy and immunotherapy? ESMO Open (2018) 3(3):e000344. doi: 10.1136/esmoopen-2018-000344
33. Unger JM, Vaidya R, Albain KS, Leblanc M, Minasian LM, Gotay CC, et al. Sex differences in risk of severe adverse events in patients receiving immunotherapy, targeted therapy, or chemotherapy in cancer clinical trials. J Clin Oncol (2022) 40(13):1474–86. doi: 10.1200/JCO.21.02377
34. Patel K, Alpert N, Tuminello S, Taioli E. Association of personal characteristics and effectiveness of immunotherapy in late-stage non-small cell lung cancer: A systematic review. JNCI Cancer Spectr (2022) 6(2):pkac015. doi: 10.1093/jncics/pkac015
35. Liang J, Hong J, Tang X, Qiu X, Zhu K, Zhou L, et al. Sex difference in response to non-small cell lung cancer immunotherapy: an updated meta-analysis. Ann Med (2022) 54(1):2606–16. doi: 10.1080/07853890.2022.2124449
36. Caliman E, Petrella MC, Rossi V, Mazzoni F, Grosso AM, Fancelli S, et al. Gender matters. Sex-related differences in immunotherapy outcome in patients with non-small cell lung cancer. Curr Cancer Drug Targets (2022). Epub ahead of print. doi: 10.2174/1568009622666220831142452
37. Lang D, Brauner A, Huemer F, Rinnerthaler G, Horner A, Wass R, et al. Sex-based clinical outcome in advanced NSCLC patients undergoing PD-1/PD-L1 inhibitor therapy-A retrospective bi-centric cohort study. Cancers (Basel) (2021) 14(1):93. doi: 10.3390/cancers14010093
38. Tsiouda T, Sardeli C, Porpodis K, Pilikidou M, Apostolidis G, Kyrka K, et al. Sex differences and adverse effects between chemotherapy and immunotherapy for non-small cell lung cancer. J Cancer (2020) 11(11):3407–15. doi: 10.7150/jca.40196
39. Barrera-Rodriguez R, Morales-Fuentes J. Lung cancer in women. Lung Cancer: Targets Ther (2012) 3:79–89. doi: 10.2147/LCTT.S37319
40. Wheatley-Price P, Blackhall F, Lee SM, Ma C, Ashcroft L, Jitlal M, et al. The influence of sex and histology on outcomes in non-small-cell lung cancer: a pooled analysis of five randomized trials. Ann Oncol (2010) 21(10):2023–8. doi: 10.1093/annonc/mdq067
41. Kirsch-Volders M, Bonassi S, Herceg Z, Hirvonen A, Moller L, Phillips DH. Gender-related differences in response to mutagens and carcinogens. Mutagenesis (2010) 25(3):213–21. doi: 10.1093/mutage/geq008
42. Su C, Zhou S, Zhang L, Ren S, Xu J, Lv M, et al. ERCC1, RRM1 and BRCA1 mRNA expression levels and clinical outcome of advanced non-small cell lung cancer. Med Oncol (2011) 28(4):1411–7. doi: 10.1007/s12032-010-9553-9
43. Li X, Yan S, Yang J, Wang Y, Lv C, Li S, et al. Efficacy and safety of PD-1/PD-L1 inhibitors plus chemotherapy versus PD-1/PD-L1 inhibitors in advanced non-small cell lung cancer: A network analysis of randomized controlled trials. Front Oncol (2021) 10. doi: 10.3389/fonc.2020.574752
44. Wu M, Huang Q, Xie Y, Wu X, Ma H, Zhang Y, et al. Improvement of the anticancer efficacy of PD-1/PD-L1 blockade via combination therapy and PD-L1 regulation. J Hematol Oncol (2022) 15(1):1–58. doi: 10.1186/s13045-022-01242-2
45. Ye Y, Jing Y, Li L, Mills GB, Diao L, Liu H, et al. Sex-associated molecular differences for cancer immunotherapy. Nat Commun (2020) 11(1):1–8. doi: 10.1038/s41467-020-15679-x
46. Zhao X, Zhao Y, Zhang J, Zhang Z, Liu L, Zhao X. Predicting PD-L1 expression status in patients with non-small cell lung cancer using [18F]FDG PET/CT radiomics. EJNMMI Res (2023) 13(1):1–10. doi: 10.1186/s13550-023-00956-9
47. Skov BG, Rørvig SB, Jensen THL, Skov T. The prevalence of programmed death ligand-1 (PD-L1) expression in non-small cell lung cancer in an unselected, consecutive population. Modern Pathol (2020) 33(1):109–17. doi: 10.1038/s41379-019-0339-0
48. Li J, Ge S, Sang S, Hu C, Deng S. Evaluation of PD-L1 expression level in patients with non-small cell lung cancer by 18F-FDG PET/CT radiomics and clinicopathological characteristics. Front Oncol (2021) 11:5396. doi: 10.3389/fonc.2021.789014
49. Fu F, Deng C, Sun W, Zheng Q, Jin Y, Li Y, et al. Distribution and concordance of PD-L1 expression by routine 22C3 assays in East-Asian patients with non-small cell lung cancer. Respir Res (2022) 23(1):1–10. doi: 10.1186/s12931-022-02201-8
50. Liu Y, Wu A, Li X, Wang S, Fang S, Mo Y. A retrospective analysis of eleven gene mutations, PD-L1 expression and clinicopathological characteristics in non-small cell lung cancer patients. Asian J Surg (2022) 45(1):367–75. doi: 10.1016/j.asjsur.2021.06.030
51. Ji M, Liu Y, Li Q, Li X, Ning Z, Zhao W, et al. PD-1/PD-L1 expression in non-small-cell lung cancer and its correlation with EGFR/KRAS mutations. Cancer Biol Ther (2016) 17(4):407–13. doi: 10.1080/15384047.2016.1156256
52. Lin G, Fan X, Zhu W, Huang C, Zhuang W, Xu H, et al. Prognostic significance of PD-L1 expression and tumor infiltrating lymphocyte in surgically resectable non-small cell lung cancer. Oncotarget (2017) 8(48):83986. doi: 10.18632/oncotarget.20233
53. Pawelczyk K, Piotrowska A, Ciesielska U, Jablonska K, Gletzel-Plucinska N, Grzegrzolka J, et al. Role of pd-l1 expression in non-small cell lung cancer and their prognostic significance according to clinicopathological factors and diagnostic markers. Int J Mol Sci (2019) 20(4):824. doi: 10.3390/ijms20040824
54. Yang X, Jiang L, Jin Y, Li P, Hou Y, Yun J, et al. PD-L1 Expression in chinese patients with advanced non-small cell lung cancer (nsclc): a multi-center retrospective observational study. J Cancer (2021) 12(24):7390–8. doi: 10.7150/jca.63003
55. Chen Q, Fu YY, Yue QN, Wu Q, Tang Y, Wang WY, et al. Distribution of PD-L1 expression and its relationship with clinicopathological variables: an audit from 1071 cases of surgically resected non-small cell lung cancer. Int J Clin Exp Pathol (2019) 12(3):774–86.
56. Li Y, Li C, Jiang Y, Han X, Liu S, Xu X, et al. Correlation of PD-L1 expression with clinicopathological and genomic features in chinese non-small-cell lung cancer. J Oncol (2022) 2022:1763778. doi: 10.1155/2022/1763778
57. Li B, Huang X, Fu L. OncoTargets and Therapy Dovepress Impact of smoking on efficacy of PD-1/PD-L1 inhibitors in non-small cell lung cancer patients: a meta-analysis. Onco Targets Ther (2018) 11:3691–6. doi: 10.2147/OTT.S156421
58. Norum J, Nieder C. Tobacco smoking and cessation and PD-L1 inhibitors in non-small cell lung cancer (NSCLC): a review of the literature. ESMO Open (2018) 3(6):e000406. doi: 10.1136/esmoopen-2018-000406
59. Li JJN, Karim K, Sung M, Le LW, Lau SCM, Sacher A, et al. Tobacco exposure and immunotherapy response in PD-L1 positive lung cancer patients. Lung Cancer (2020) 150:159–63. doi: 10.1016/j.lungcan.2020.10.023
60. Dai L, Jin B, Liu T, Chen J, Li G, Dang J. The effect of smoking status on efficacy of immune checkpoint inhibitors in metastatic non-small cell lung cancer: A systematic review and meta-analysis-NC-ND license (2021). Available at: http://creativecommons.org/licenses/by-nc-nd/4.0/.
61. Mo J, Hu X, Gu L, Chen B, Khadaroo PA, Shen Z, et al. Smokers or non-smokers: Who benefits more from immune checkpoint inhibitors in treatment of Malignancies? An up-to-date meta-analysis. World J Surg Oncol (2020) 18(1):1–12. doi: 10.1186/s12957-020-1792-4
62. Liam CK, Yew CY, Pang YK, Wong CK, Poh ME, Tan JL, et al. Common driver mutations and programmed death-ligand 1 expression in advanced non-small cell lung cancer in smokers and never smokers. BMC Cancer (2023) 23(1):659. doi: 10.1186/s12885-023-11156-y
63. Chen N, Fang W, Lin Z, Peng P, Wang J, Zhan J, et al. KRAS mutation-induced upregulation of PD-L1 mediates immune escape in human lung adenocarcinoma. Cancer Immunol Immunother (2017) 66(9):1175–87. doi: 10.1007/s00262-017-2005-z
64. Schafer JM, Xiao T, Kwon H, Collier K, Chang Y, Abdel-Hafiz H, et al. Sex-biased adaptive immune regulation in cancer development and therapy. iScience (2022) 25(8):104717. doi: 10.1016/j.isci.2022.104717
65. Özdemir BC, Dotto GP. Sex hormones and anticancer immunity. Clin Cancer Res (2019) 25(15):4603–10. doi: 10.1158/1078-0432.CCR-19-0137
66. Weinberg OK, Marquez-Garban DC, Fishbein MC, Goodglick L, Garban HJ, Dubinett SM, et al. Aromatase inhibitors in human lung cancer therapy. Cancer Res (2005) 65(24):11287–91. doi: 10.1158/0008-5472.CAN-05-2737
67. Márquez-Garbán DC, Chen HW, Goodglick L, Fishbein MC, Pietras RJ. Targeting aromatase and estrogen signaling in human non-small cell lung cancer. Ann N Y Acad Sci (2009) 1155:194. doi: 10.1111/j.1749-6632.2009.04116.x
68. Mah V, Marquez D, Alavi M, Maresh EL, Zhang L, Yoon N, et al. Expression levels of estrogen receptor beta in conjunction with aromatase predict survival in non-small cell lung cancer. Lung Cancer (2011) 74(2):318. doi: 10.1016/j.lungcan.2011.03.009
69. Niikawa H, Suzuki T, Miki Y, Suzuki S, Nagasaki S, Akahira J, et al. Intratumoral estrogens and estrogen receptors in human non-small cell lung carcinoma. Clin Cancer Res (2008) 14(14):4417–26. doi: 10.1158/1078-0432.CCR-07-1950
70. Siegfried JM, Hershberger PA, Stabile LP. Estrogen receptor signaling in lung cancer. Semin Oncol (2009) 36(6):524–31. doi: 10.1053/j.seminoncol.2009.10.004
71. Hershberger PA, Stabile LP, Kanterewicz B, Rothstein ME, Gubish CT, Land S, et al. Estrogen receptor beta (ERβ) subtype-specific ligands increase transcription, p44/p42 mitogen activated protein kinase (MAPK) activation and growth in human non-small cell lung cancer cells. J Steroid Biochem Mol Biol (2009) 116(1–2):102–9. doi: 10.1016/j.jsbmb.2009.05.004
72. Maitra R, Malik P, Mukherjee TK. Targeting estrogens and various estrogen-related receptors against non-small cell lung cancers: A perspective. Cancers (Basel) (2022) 14(1):80. doi: 10.3390/cancers14010080
73. Mukherjee TK, Malik P, Hoidal JR. The emerging role of estrogen related receptorα in complications of non-small cell lung cancers. Oncol Lett (2021) 21(4):258. doi: 10.3892/ol.2021.12519
74. Smida T, Bruno TC, Stabile LP. Influence of estrogen on the NSCLC microenvironment: A comprehensive picture and clinical implications. Front Oncol (2020) 10:137. doi: 10.3389/fonc.2020.00137
75. Rodriguez-Lara V, Ignacio GS, Cerbon Cervantes MA. Estrogen induces CXCR4 overexpression and CXCR4/CXL12 pathway activation in lung adenocarcinoma cells in vitro. Endocr Res (2017) 42(3):219–31. doi: 10.1080/07435800.2017.1292526
76. Rodriguez-Lara V, Peña-Mirabal E, Baez-Saldaña R, Esparza-Silva AL, García-Zepeda E, Cerbon Cervantes MA, et al. Estrogen receptor beta and CXCR4/CXCL12 expression: Differences by sex and hormonal status in lung adenocarcinoma. Arch Med Res (2014) 45(2):158–69. doi: 10.1016/j.arcmed.2014.01.001
77. Shuai C, Yang X, Pan H, Han W. Estrogen receptor downregulates expression of PD-1/PD-L1 and infiltration of CD8+ T cells by inhibiting IL-17 signaling transduction in breast cancer. Front Oncol (2020) 10:582863. doi: 10.3389/fonc.2020.582863
78. O’Meara T, Marczyk M, Qing T, Yaghoobi V, Blenman K, Cole K, et al. Immunological differences between immune-rich estrogen receptor-positive and immune-rich triple-negative breast cancers. JCO Precis Oncol (2020) 4(4):767–79. doi: 10.1200/PO.19.00350
79. Liu L, Shen Y, Zhu X, Lv R, Li S, Zhang Z, et al. ERα is a negative regulator of PD-L1 gene transcription in breast cancer. Biochem Biophys Res Commun (2018) 505(1):157–61. doi: 10.1016/j.bbrc.2018.09.005
80. Hühn D, Martí-Rodrigo P, Mouron S, Hansel C, Tschapalda K, Porebski B, et al. Prolonged estrogen deprivation triggers a broad immunosuppressive phenotype in breast cancer cells. Mol Oncol (2022) 16(1):148–65. doi: 10.1002/1878-0261.13083
81. Wang T, Jin J, Qian C, Lou J, Lin J, Xu A, et al. Estrogen/ER in anti-tumor immunity regulation to tumor cell and tumor microenvironment. Cancer Cell Int (2021) 21(1):1–13. doi: 10.1186/s12935-021-02003-w
82. Lim SO, Li CW, Xia W, Cha JH, Chan LC, Wu Y, et al. Deubiquitination and stabilization of PD-L1 by CSN5. Cancer Cell (2016) 30(6):925–39. doi: 10.1016/j.ccell.2016.10.010
83. Zhou T, Xu D, Tang B, Ren Y, Han Y, Liang G, et al. Expression of programmed death ligand-1 and programmed death-1 in samples of invasive ductal carcinoma of the breast and its correlation with prognosis. Anticancer Drugs (2018) 29(9):904. doi: 10.1097/CAD.0000000000000683
84. Yang L, Huang F, Mei J, Wang X, Zhang Q, Wang H, et al. Post-transcriptional control of PD-L1 expression by 17β-estradiol via PI3K/Akt signaling pathway in ERα-positive cancer cell lines. Int J Gynecol Cancer (2017) 27(2):196–205. doi: 10.1097/IGC.0000000000000875
85. Tulchiner G, Pichler R, Ulmer H, Staudacher N, Lindner AK, Brunner A, et al. Sex-specific hormone changes during immunotherapy and its influence on survival in metastatic renal cell carcinoma. Cancer Immunol Immunother (2021) 70(10):2805–17. doi: 10.1007/s00262-021-02882-y
86. Tsukamoto H, Fujieda K, Miyashita A, Fukushima S, Ikeda T, Kubo Y, et al. Combined blockade of IL6 and PD-1/PD-L1 signaling abrogates mutual regulation of their immunosuppressive effects in the tumor microenvironment. Cancer Res (2018) 78(17):5011–22. doi: 10.1158/0008-5472.CAN-18-0118
87. Purohit A, Newman SP, Reed MJ. The role of cytokines in regulating estrogen synthesis: implications for the etiology of breast cancer. Breast Cancer Res (2002) 4(2):65. doi: 10.1186/bcr425
88. Tong D. Selective estrogen receptor modulators contribute to prostate cancer treatment by regulating the tumor immune microenvironment. J Immunother Cancer (2022) 10(4):2944. doi: 10.1136/jitc-2021-002944
89. Chakraborty B, Byemerwa J, Shepherd J, Haines CN, Baldi R, Gong W, et al. Inhibition of estrogen signaling in myeloid cells increases tumor immunity in melanoma. J Clin Invest (2021) 131(23):e151347. doi: 10.1172/JCI151347
90. Márquez-Garbán DC, Deng G, Comin-Anduix B, Garcia AJ, Xing Y, Chen HW, et al. Antiestrogens in combination with immune checkpoint inhibitors in breast cancer immunotherapy. J Steroid Biochem Mol Biol (2019) 193:105415. doi: 10.1016/j.jsbmb.2019.105415
91. Song S, Tang H, Quan W, Shang A, Ling C. Estradiol initiates the immune escape of non-small cell lung cancer cells via ERβ/SIRT1/FOXO3a/PD-L1 axis. Int Immunopharmacol (2022) 107:1567–5769. doi: 10.1016/j.intimp.2022.108629
92. Anobile DP, Salaroglio IC, Tabbò F, La Vecchia S, Akman M, Napoli F, et al. Autocrine 17-β-estradiol/estrogen receptor-α loop determines the response to immune-checkpoint inhibitors in non-small cell lung cancer. Clin Cancer Res (2023) 29(19):3958–73. doi: 10.1158/1078-0432.CCR-22-3949
93. Mukherjee TK, Malik P, Hoidal JR. Receptor for advanced glycation end products (RAGE) and its polymorphic variants as predictive diagnostic and prognostic markers of NSCLCs: a perspective. Curr Oncol Rep (2021) 23(1):1–12. doi: 10.1007/s11912-020-00992-x
94. Amornsupak K, Thongchot S, Thinyakul C, Box C, Hedayat S, Thuwajit P, et al. HMGB1 mediates invasion and PD-L1 expression through RAGE-PI3K/AKT signaling pathway in MDA-MB-231 breast cancer cells. BMC Cancer (2022) 22(1):578. doi: 10.1186/s12885-022-09675-1
95. Stabile LP, Lyker JS, Gubish CT, Zhang W, Grandis JR, Siegfried JM. Combined targeting of the estrogen receptor and the epidermal growth factor receptor in non-small cell lung cancer shows enhanced antiproliferative effects. Cancer Res (2005) 65(4):1459–70. doi: 10.1158/0008-5472.CAN-04-1872
96. Chen N, Fang W, Zhan J, Hong S, Tang Y, Kang S, et al. Upregulation of PD-L1 by EGFR activation mediates the immune escape in EGFR-driven NSCLC: implication for optional immune targeted therapy for NSCLC patients with EGFR mutation. J Thorac Oncol (2015) 10(6):910–23. doi: 10.1097/JTO.0000000000000500
97. Gu Y, Tang YY, Wan JX, Zou JY, Lu CG, Zhu HS, et al. Sex difference in the expression of PD-1 of non-small cell lung cancer. Front Immunol (2022) 13:6167. doi: 10.3389/fimmu.2022.1026214
98. Zhou J, Wang H, Sun Q, Liu X, Wu Z, Wang X, et al. miR-224-5p-enriched exosomes promote tumorigenesis by directly targeting androgen receptor in non-small cell lung cancer. Mol Ther Nucleic Acids (2021) 23:1217. doi: 10.1016/j.omtn.2021.01.028
99. Berardi R, Morgese F, Santinelli A, Onofri A, Biscotti T, Brunelli A, et al. Hormonal receptors in lung adenocarcinoma: expression and difference in outcome by sex. Oncotarget (2016) 7(50):82648–57. doi: 10.18632/oncotarget.12244
100. Grant L, Banerji S, Murphy L, Dawe DE, Harlos C, Myal Y, et al. Androgen receptor and ki67 expression and survival outcomes in non-small cell lung cancer. Horm Cancer (2018) 9(4):288–94. doi: 10.1007/s12672-018-0336-7
101. Lu HH, Yeh SD, Chou YT, Tsai YT, Chang C, Wu CW. Abstract 2126: Androgen receptor regulates lung cancer progress through modulation of OCT-4 expression. Cancer Res (2011) 71(8_Supplement):2126–6. doi: 10.1158/1538-7445.AM2011-2126
102. Yan M, Chen X, Wang S, Li Y. [Expression of ER and AR in lung cancer]. Zhongguo Fei Ai Za Zhi (2008) 11(1):126–9. Chinese. doi: 10.3779/j.issn.1009-3419.2008.01.027
103. Harlos C, Musto G, Lambert P, Ahmed R, Pitz MW. Androgen pathway manipulation and survival in patients with lung cancer. Horm Cancer (2015) 6(2–3):120–7. doi: 10.1007/s12672-015-0218-1
104. Jung K, Park JC, Kang H, Brandes JC. Androgen deprivation therapy is associated with decreased second primary lung cancer risk in the United States veterans with prostate cancer. Epidemiol Health (2018) 40:e2018040. doi: 10.4178/epih.e2018040
105. Nazha B, Zhang C, Chen Z, Ragin C, Owonikoko TK. Concurrent androgen deprivation therapy for prostate cancer improves survival for synchronous or metachronous non-small cell lung cancer: A SEER–medicare database analysis. Cancers (Basel) (2022) 14(13):3206. doi: 10.3390/cancers14133206
106. Mikkonen L, Pihlajamaa P, Sahu B, Zhang FP, Janne OA. Androgen receptor and androgen-dependent gene expression in lung. Mol Cell Endocrinol (2010) 317(1–2):14–24. doi: 10.1016/j.mce.2009.12.022
107. Lanzino M, Sisci D, Morelli C, Garofalo C, Catalano S, Casaburi I, et al. Inhibition of cyclin D1 expression by androgen receptor in breast cancer cells–identification of a novel androgen response element. Nucleic Acids Res (2010) 38(16):5351–65. doi: 10.1093/nar/gkq278
108. Chang C, Lee SO, Yeh S, Chang TM. Androgen receptor (AR) differential roles in hormone-related tumors including prostate, bladder, kidney, lung, breast and liver. Oncogene (2014) 33(25):3225–34. doi: 10.1038/onc.2013.274
109. Wang AR, Beyer H, Brennan S, Stiles S, Wiese D, Buehler D, et al. Abstract 3946: Androgen receptor drives differential gene expression in KRAS-mediated non-small cell lung cancer. Cancer Res (2018) 78(13_Supplement):3946–6. doi: 10.1158/1538-7445.AM2018-3946
110. Necchi A, Lo Vullo S, Giannatempo P, Raggi D, Perrone F, Nicolai N, et al. Association of androgen receptor expression on tumor cells and PD-L1 expression in muscle-invasive and metastatic urothelial carcinoma: insights for clinical research. Clin Genitourin Cancer (2018) 16(2):e403–10. doi: 10.1016/j.clgc.2017.09.016
111. O’Connell TJ, Dadafarin S, Jones M, Rodríguez T, Gupta A, Shin E, et al. Androgen activity is associated with PD-L1 downregulation in thyroid cancer. Front Cell Dev Biol (2021) 9. doi: 10.3389/fcell.2021.663130
112. Jiang G, Shi L, Zheng X, Zhang X, Wu K, Liu B, et al. Androgen receptor affects the response to immune checkpoint therapy by suppressing PD-L1 in hepatocellular carcinoma. Aging (Albany NY) (2020) 12(12):11466. doi: 10.18632/aging.103231
113. Liu Q, You B, Meng J, Huang CP, Dong G, Wang R, et al. Targeting the androgen receptor to enhance NK cell killing efficacy in bladder cancer by modulating ADAR2/circ_0001005/PD-L1 signaling. Cancer Gene Ther (2022) 29(12):1988–2000. doi: 10.1038/s41417-022-00506-w
114. Tang M, Sun Y, Huang CP, Chen L, Liu B, You B, et al. High dose androgen suppresses natural killer cytotoxicity of castration-resistant prostate cancer cells via altering AR/circFKBP5/miRNA-513a-5p/PD-L1 signals. Cell Death Dis (2022) 13(8):746. doi: 10.1038/s41419-022-04956-w
115. Vellano CP, White MG, Andrews MC, Chelvanambi M, Witt RG, Daniele JR, et al. Androgen receptor blockade promotes response to BRAF/MEK-targeted therapy. Nature (2022) 606(7915):797–803. doi: 10.1038/s41586-022-04833-8
116. Guan X, Polesso F, Wang C, Sehrawat A, Hawkins RM, Murray SE, et al. Androgen receptor activity in T cells limits checkpoint blockade efficacy. Nature (2022) 606(7915):791–6. doi: 10.1038/s41586-022-04522-6
Keywords: NSCLC, PD-1/PD-L1 pathway, immunotherapy, estrogen, androgen
Citation: Rodriguez-Lara V, Soca-Chafre G, Avila-Costa MR, Whaley JJJ-V, Rodriguez-Cid JR, Ordoñez-Librado JL, Rodriguez-Maldonado E and Heredia-Jara NA (2023) Role of sex and sex hormones in PD-L1 expression in NSCLC: clinical and therapeutic implications. Front. Oncol. 13:1210297. doi: 10.3389/fonc.2023.1210297
Received: 24 April 2023; Accepted: 28 September 2023;
Published: 24 October 2023.
Edited by:
Syed Ahsan Raza, University of Pittsburgh, United StatesReviewed by:
Amy E. Moran, Oregon Health and Science University, United States; Parth Malik, Ministry of Science and Technology, IndiaCopyright © 2023 Rodriguez-Lara, Soca-Chafre, Avila-Costa, Whaley, Rodriguez-Cid, Ordoñez-Librado, Rodriguez-Maldonado and Heredia-Jara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vianey Rodriguez-Lara, dmlhbmV5cmxAZmFjbWVkLnVuYW0ubXg=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.