
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 12 July 2023
Sec. Pediatric Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1192806
This article is part of the Research Topic Critical Complications In Pediatric Oncology and Hematopoietic Cell Transplant, volume II View all 22 articles
 Marijn Soeteman1
Marijn Soeteman1 Marta F. Fiocco1,2Joppe Nijman3
Marta F. Fiocco1,2Joppe Nijman3 Casper W. Bollen3
Casper W. Bollen3 Maartje M. Marcelis1Ellen Kilsdonk1
Maartje M. Marcelis1Ellen Kilsdonk1 Edward E. S. Nieuwenhuis4Teus H. Kappen5Wim J. E. Tissing1,6
Edward E. S. Nieuwenhuis4Teus H. Kappen5Wim J. E. Tissing1,6 Roelie M. Wösten-van Asperen3*
Roelie M. Wösten-van Asperen3*Background: Pediatric oncology patients who require admission to the pediatric intensive care unit (PICU) have worse outcomes compared to their non-cancer peers. Although multi-organ dysfunction (MOD) plays a pivotal role in PICU mortality and morbidity, risk factors for MOD have not yet been identified. We aimed to identify risk factors at PICU admission for new or progressive MOD (NPMOD) during the first week of PICU stay.
Methods: This retrospective cohort study included all pediatric oncology patients aged 0 to 18 years admitted to the PICU between June 2018 and June 2021. We used the recently published PODIUM criteria for defining multi-organ dysfunction and estimated the association between covariates at PICU baseline and the outcome NPMOD using a multivariable logistic regression model, with PICU admission as unit of study. To study the predictive performance, the model was internally validated by using bootstrap.
Results: A total of 761 PICU admissions of 571 patients were included. NPMOD was present in 154 PICU admissions (20%). Patients with NPMOD had a high mortality compared to patients without NPMOD, 14% and 1.0% respectively. Hemato-oncological diagnosis, number of failing organs and unplanned admission were independent risk factors for NPMOD. The prognostic model had an overall good discrimination and calibration.
Conclusion: The risk factors at PICU admission for NPMOD may help to identify patients who may benefit from closer monitoring and early interventions. When applying the PODIUM criteria, we found some opportunities for fine-tuning these criteria for pediatric oncology patients, that need to be validated in future studies.
The simultaneous dysfunction of multiple organ systems plays a pivotal role in the mortality of children admitted to the pediatric intensive care unit (PICU) (1). Multiple organ dysfunction (MOD) is defined as two or more concurrent organ dysfunctions (1–3). While the term multiple organ dysfunction syndrome (MODS) has traditionally been used, it was recently posited that this term should be selectively applied to patients with a shared underlying mechanism that affects multiple organ systems simultaneously (4). MOD can be categorized in new MOD, defined as MOD in patients who have single or no organ dysfunction on PICU admission, and progressive MOD, defined as additional dysfunctional organ systems in patients who already meet MOD criteria at admission (5).
In children, the risk factors for developing MOD include sepsis, major trauma, severe hypoxemia, and young age (e.g., infancy) (6, 7). The number of dysfunctional organ systems is associated with mortality, with each additional failing organ system increasing the risk of death (7–10). Pediatric oncology patients are particular at high risk for MOD due to the aggressive cancer pathophysiology and intensive treatment regimens, that may lead to organ infiltration, systemic toxicity, and immunosuppression (11). Similarly to general pediatric patients, MOD plays a significant role in the high morbidity and mortality of these patients (12). Early recognition and intervention in organ dysfunction may provide the potential to modify its course and prevent further deterioration (13–16). In adult oncology patients, it was shown that early interventions in deteriorating patients improved both short- and long-term outcomes (14, 15). Therefore, identifying risk factors for MOD at start of the PICU admission could provide opportunities for intensified monitoring and early interventions, which may ultimately reduce morbidity and mortality in critically ill pediatric oncology patients (12, 16, 17). Despite the important role of MOD in PICU morbidity and mortality, risk factors for MOD in pediatric oncology patients have not yet been identified.
In this study, we aimed to identify risk factors at PICU admission for MOD during the first week of PICU stay in pediatric oncology patients. Recently, the Pediatric Organ Dysfunction Information Update Mandate (PODIUM) evidence-based pediatric organ dysfunction criteria were published (12); this is the first study in pediatric oncology patients using these criteria. In addition, fine-tuning of these criteria for pediatric oncology patients may be needed, as they frequently experience organ dysfunction as a result of their oncological treatment. This dysfunction may not necessarily indicate MOD. Therefore, the second objective of this study was to assess whether adjusting the PODIUM criteria for pediatric oncology patients would reveal different risk factors for MOD.
We performed a retrospective cohort study between June 1, 2018 and June 1, 2021, at an 18-bed PICU of the Wilhelmina Children’s Hospital, that is shared with the adjacent Princess Máxima Center, an 80-bed national referral center for pediatric oncology. All pediatric oncology patients with International Classification of Diseases in Oncology (ICD-O) diagnosis of pediatric malignancy (morphology code 1, 2 or 3) aged 0 to 18 years admitted to the PICU were eligible for inclusion. Patients without consent for the use of clinical data were excluded. The study was approved by the ethical review board of our hospital (IRB protocol number 16-572/C).
We classified organ dysfunction based on the PODIUM criteria (18) (Table 1 and Supplementary Table 1). Clinical data were extracted from the electronic health records and comprised patient characteristics, organ dysfunction in the 24 hours preceding PICU admission, and clinical time series with a frequency of 1 measurement per minute (vital signs and mechanical ventilator data), laboratory results, observations (e.g. Glasgow Coma scores), vasoactive medication, and fluid balance data. Additional data for organ dysfunction, e.g., cardiopulmonary resuscitation, encephalopathy and gastro-intestinal perforation, were acquired from free text fields in clinical or imaging reports through text-mining. In applying the PODIUM criteria, we made assumptions based on clinical expertise to get from a high frequency dataset to the classification of (concurrent) organ dysfunction, including handling measurement errors and missing data. Detailed information on the assessment of the PODIUM criteria is provided in the Supplementary Material. Single organ dysfunction was classified based on the PODIUM criteria within 1-hour windows, and the number of concurrent organ dysfunctions was classified within each 24-hour window.
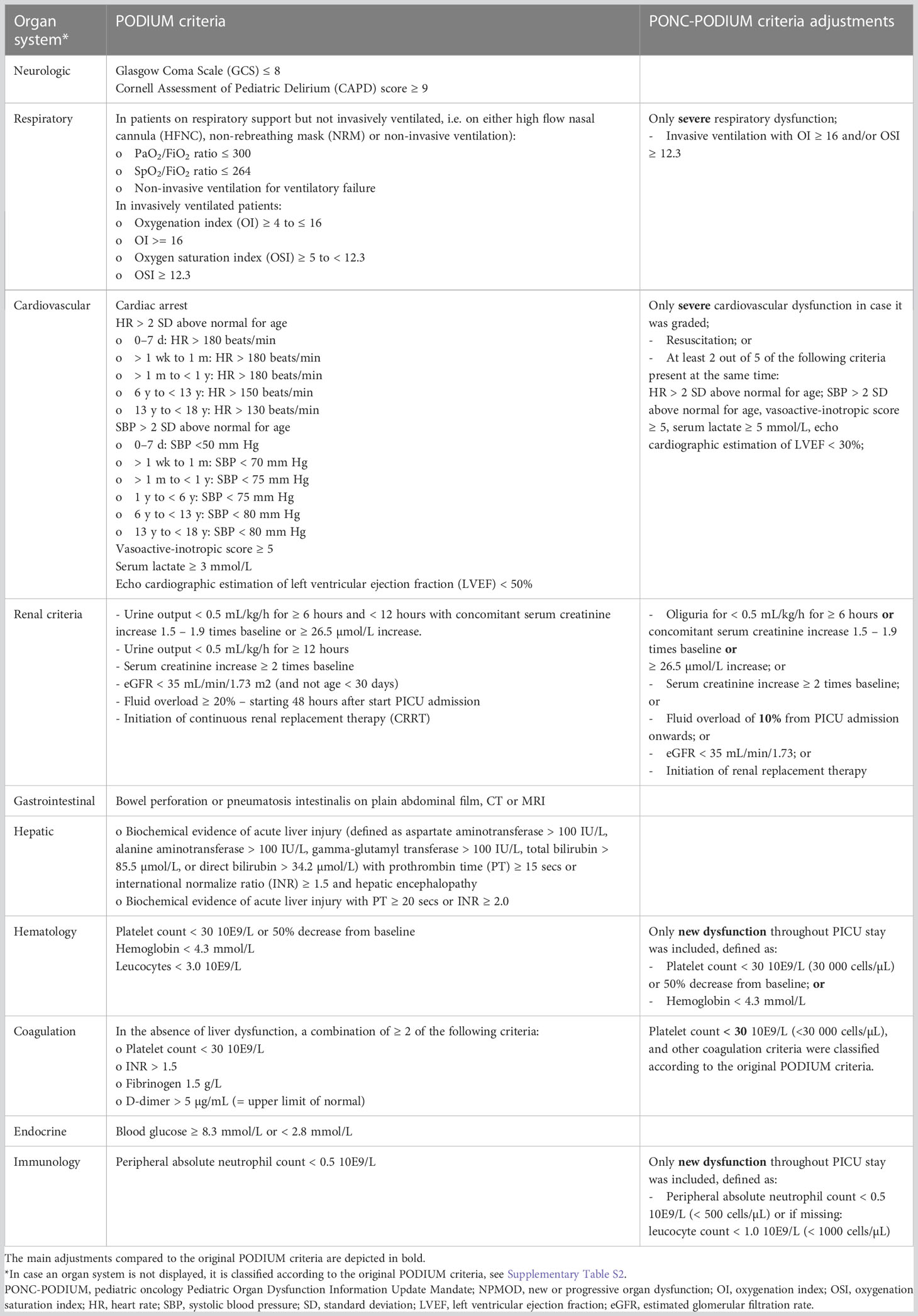
Table 1 Assessment of the PODIUM and PONC-PODIUM criteria.
We assessed presence of organ dysfunction at PICU admission (baseline) by evaluating all relevant laboratory values and free text data in the 24 hours prior to and the first three hours of PICU admission. Missing data were classified as no organ dysfunction at PICU baseline. For further details on assessment of the organ dysfunction criteria, see Supplementary Table 2.
Although some specific criteria for oncology patients are included in the PODIUM criteria, we proposed additional considerations for these patients since some laboratory variables may reflect side-effects of the cancer treatment instead of organ dysfunction in the context of MOD. We therefore adjusted some criteria for this specific patient population: the pediatric oncology (PONC) PODIUM criteria (Table 1).
Invasive ventilation and the use of vasoactive medication are associated with increased PICU mortality in pediatric oncology patients (19). Therefore, we used the thresholds of severe respiratory dysfunction, i.e., invasive ventilation and an oxygenation index of ≥ 16 or an oxygenation saturation index of ≥ 12.3. For cardiovascular dysfunction, we used the severe threshold for lactate and left ventricular ejection fraction (LVEF).
Considering the renal criteria, it was shown that patients with a fluid overload greater than 10% were 6 times more likely to die during PICU admission than those with less than or equal to 10% fluid overload (20). Moreover, oliguria is often not present in pediatric oncology patients with acute kidney injury (AKI) (20). We therefore adjusted the criteria for renal dysfunction: oliguria was not required and a fluid overload > 10%, instead of 20%, was used directly from the start of PICU admission onwards (as opposed to starting 48 hours after admission).
Since hematological and immunological dysfunction at baseline are less relevant due to the idiopathic nature of these in oncology patients and likely does not represent dysfunction due to critical illness, we excluded the leukocyte criterion from hematological dysfunction and only included hematological or immunological dysfunction that was newly developed during PICU stay for the classification of NPMOD. In classifying coagulation dysfunction, we used the platelet count threshold for pediatric oncology patients (i.e., < 30 10E9/L or < 30 000 cells/µL).
The primary outcome was new or progressive MOD (NPMOD). New MOD was defined as no MOD at baseline and the concurrent dysfunction of at least 2 organs. Progressive MOD was defined as MOD (i.e., concurrent dysfunction of at least 2 organ systems) at baseline, and the development of one or more additional concurrent organ dysfunction(s).
A multivariable logistic regression model was used to estimate the association between covariates and the outcome. Covariates at baseline of PICU admission were selected based on literature and expert opinion. The included covariates encompassed diagnosis category (i.e., hemato-oncological, solid tumor or neuro-oncological); hematopoietic stem cell transplantation; neutropenia at baseline; a composite covariate of sepsis and/or infection (bacterial or fungal (21)); high-flow oxygen therapy preceding PICU admission; the number of organ dysfunctions at baseline (categorized into 0, 1 or ≥ 2), unplanned PICU admission, and previous relevant PICU admission (i.e., a previous PICU admission that was either unplanned or had a protracted course). See Supplementary Material for a detailed description of the covariates.
We analyzed the first week of PICU admission, or up to discharge within seven days, whichever event first occurred. We assessed the outcome NPMOD based on both the original and our PONC-PODIUM criteria, to determine whether adjustments of the organ dysfunction criteria for pediatric oncology population yielded different significant risk factors. In addition, we performed a subgroup analysis of only unplanned PICU admissions to identify possible different significant risk factors for NPMOD. A multivariable logistic regression model was used to estimate the association between covariates and the outcome, including the same covariates as before except for unplanned PICU admission. The outcome NPMOD within one week based on both original PODIUM criteria and PONC-PODIUM criteria was assessed.
To study the predictive performance of the model, internal validation was performed by using Efron’s bootstrap (i.e. resampling the dataset 500 times) (22). Statistical analyses were performed using R-statistical software (23), version 4.2.1 (2022–06–23)., see Supplementary Material for associated packages.
A total of 761 PICU admissions of 571 patients were included. Table 2 reports the clinical characteristics of the PICU admissions. The median age [interquartile range] at PICU admission was 6.0 [2.7 – 12.8] years. The cohort included 25% hemato-oncological patients, 35% solid tumor patients, 40% neuro-oncology patients, and 2% had a hematopoietic stem cell transplantation (HSCT) in the year preceding PICU admission. Among the 761 PICU admissions, 288 (38%) were unplanned admissions. Neuro-oncology and solid tumor patients most often had planned postoperative PICU admissions (89% and 67% respectively), whereas hemato-oncology patients largely required unplanned PICU admissions (93%). Data of at least 2 organ systems were available at baseline in 744 of 761 PICU admissions (98%) for the classification of MOD at baseline.
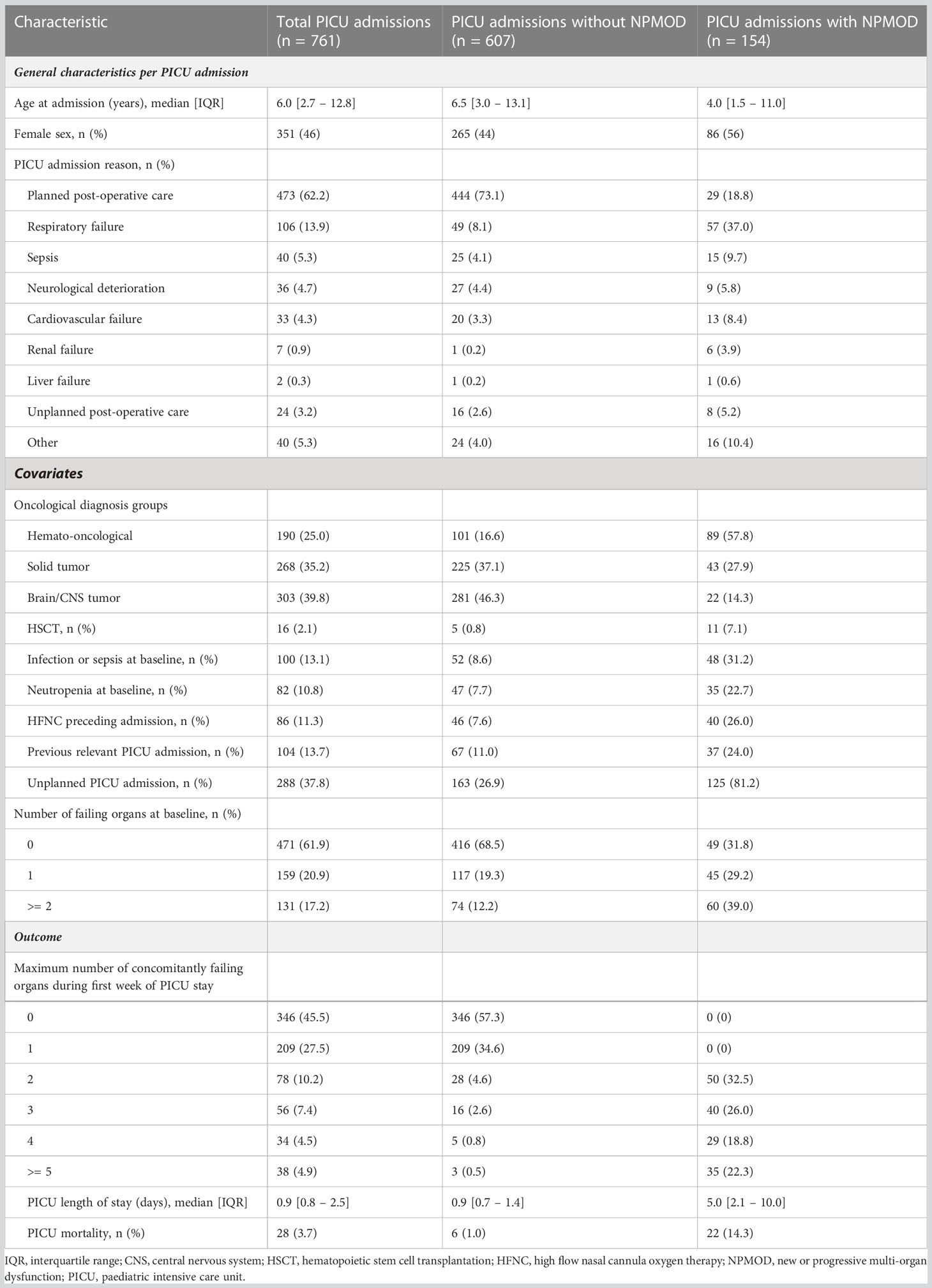
Table 2 Clinical and demographic characteristics of PICU admissions overall and by occurrence of NPMOD (defined according to PODIUM criteria).
NPMOD was present in 154 PICU admissions (20%). The PICU mortality was 4% in all PICU admissions, 1% in the group without NPMOD, and 14% in the group with NPMOD. In the PICU admissions where patients developed NPMOD, the three most frequently failing organ systems at PICU baseline included hematological (41%), immunological (23%) and respiratory (20%) dysfunction (see Figure 1A).
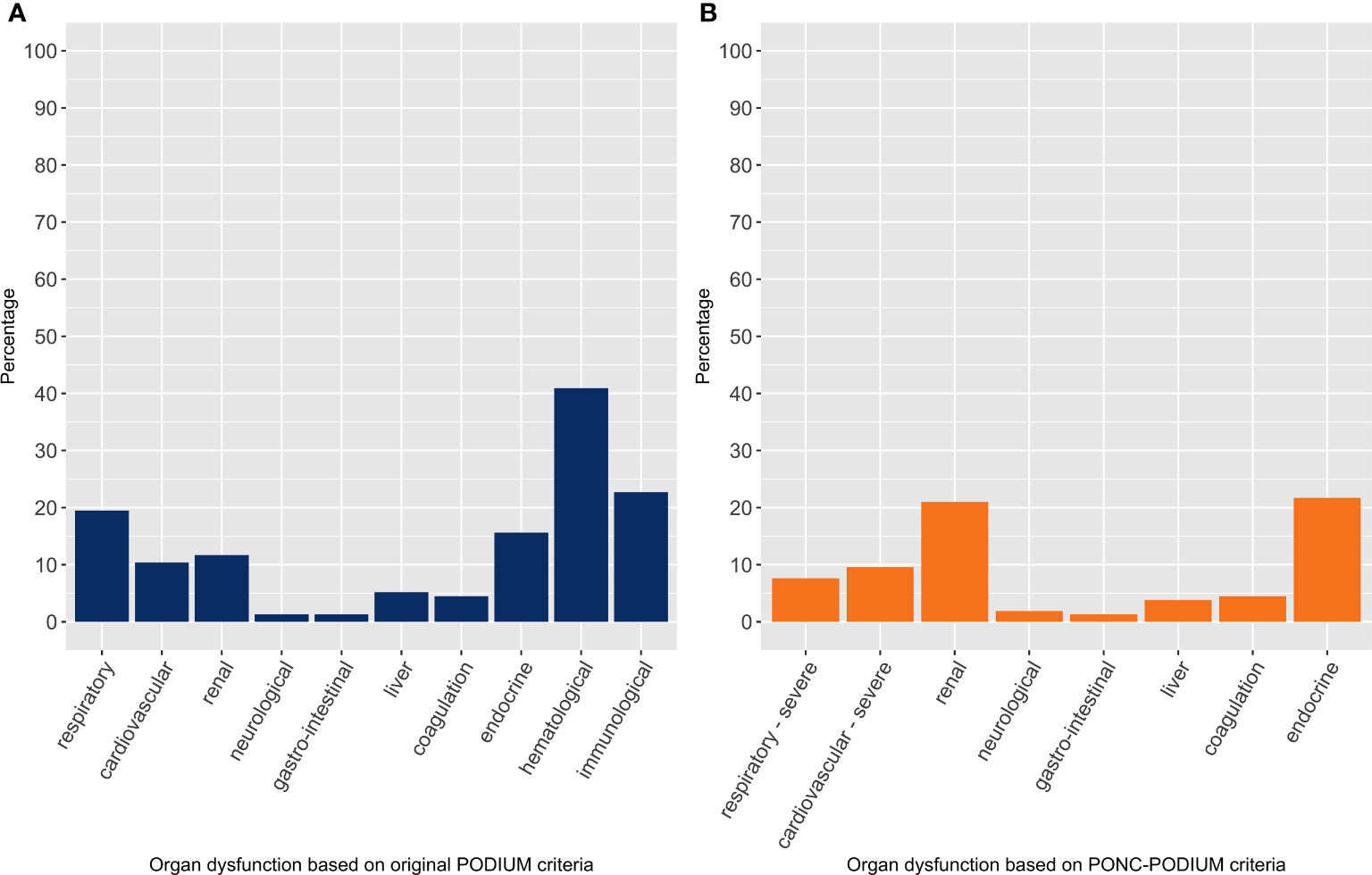
Figure 1 Organ dysfunction at PICU baseline in all PICU admissions with new or progressive multi-organ dysfunction, per organ system with percentage of failing organ system. The left panel (A) considers organ dysfunction based on the original PODIUM criteria, whereas the right panel (B) considers organ dysfunction based on the PONC-PODIUM criteria, thus adjusted for pediatric oncology patients.
The results of the univariate and multivariable model are displayed in Table 3. Hemato-oncological diagnosis, number of failing organs at baseline and unplanned PICU admissions were significantly associated with NPMOD in the multivariable model. Internal validation of the model yielded a c-index of 0.81, indicating a reasonable discriminative ability. The calibration plot showed an overall good calibration, with an index-corrected slope of 0.93.
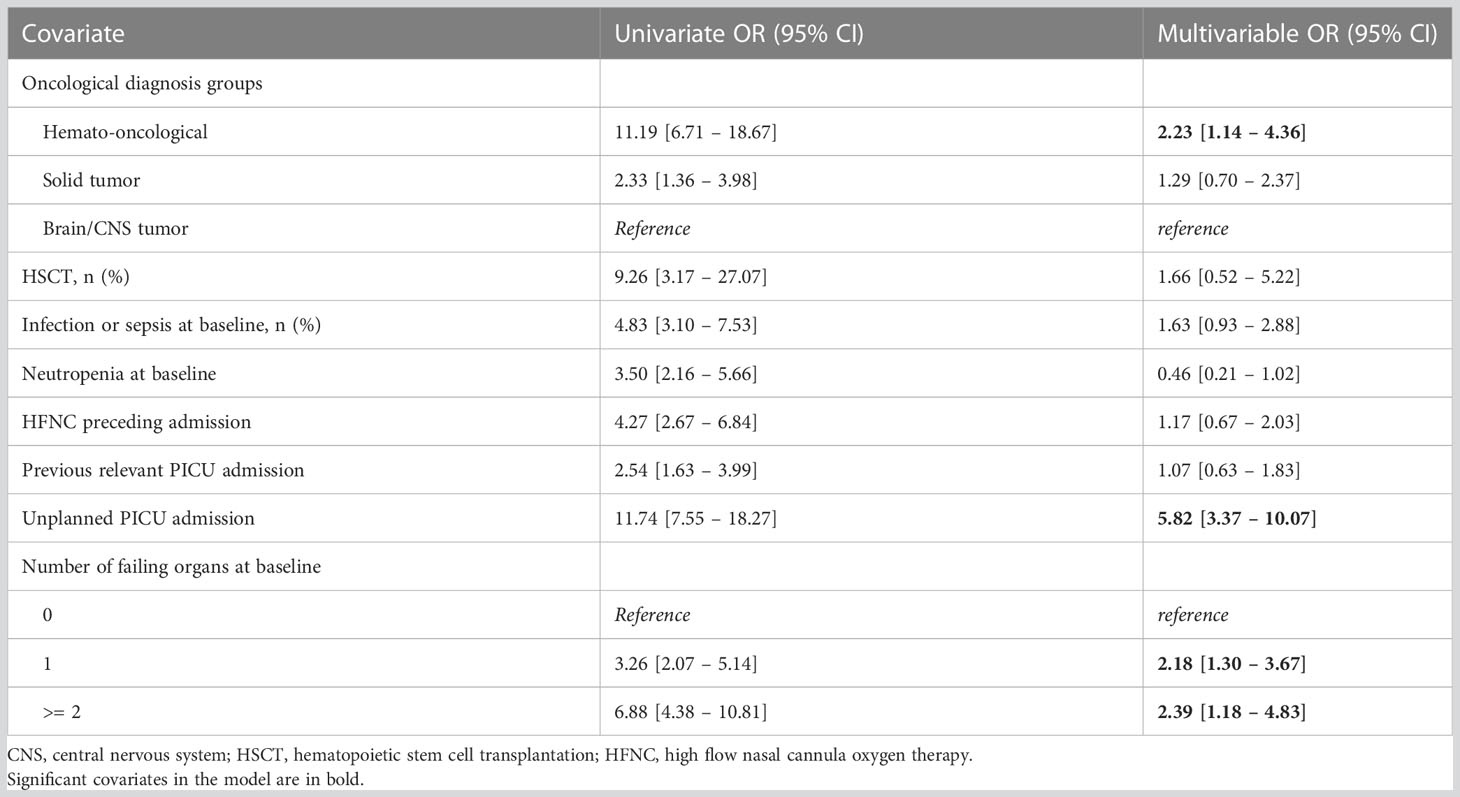
Table 3 Results of the univariate and multivariable logistic regression model, with estimated odds ratio (OR) along with the 95% confidence interval (CI), for outcome of new or progressive multi organ dysfunction (NPMOD) - defined according to the PODIUM criteria.
Using the PONC-PODIUM criteria, NPMOD was present in 157 PICU admissions (21%), see Supplementary Table S3. Applying these adjusted criteria revealed a different top three of frequently failing organ systems at PICU baseline, namely endocrine (22%), renal (21%), and severe cardiovascular dysfunction (10%) (Figure 1B). In the multivariable model, we found the same significant risk factors for NPMOD including hemato-oncological diagnosis, number of failing organs at baseline and unplanned PICU admission (Supplementary Table S4).
We performed a subgroup analysis including only the unplanned admissions (Table 4). NPMOD according to the original PODIUM criteria was present in 125 unplanned PICU admissions (43%). Respiratory failure, sepsis and neurological deterioration were the three major PICU admission reasons for unplanned PICU admission. PICU mortality rate was slightly higher compared to the total cohort, 4% in the patients without NPMOD and 17% in patients with NPMOD. The most frequently failing organ systems at admissions were similar to what was found in the total cohort, including hematological dysfunction (47%), immunological dysfunction (27%), and respiratory dysfunction (23%) (Figure 2A). In the multivariable logistic regression model, the number of failing organs at PICU baseline was significantly associated with NPMOD (Table 5).
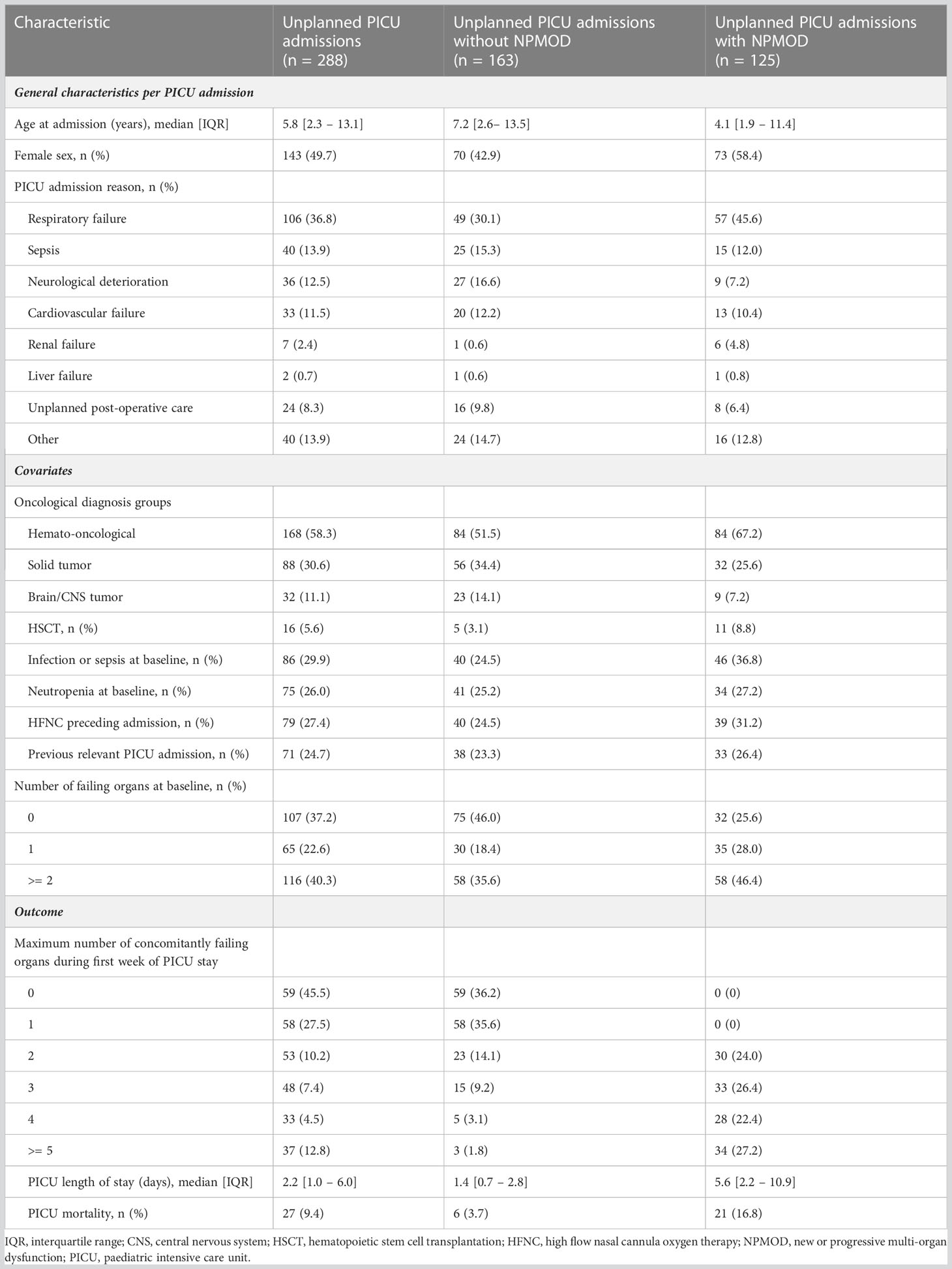
Table 4 Clinical and demographic characteristics of unplanned PICU admissions, by occurrence of new or progressive multi organ dysfunction (defined according to PODIUM criteria).
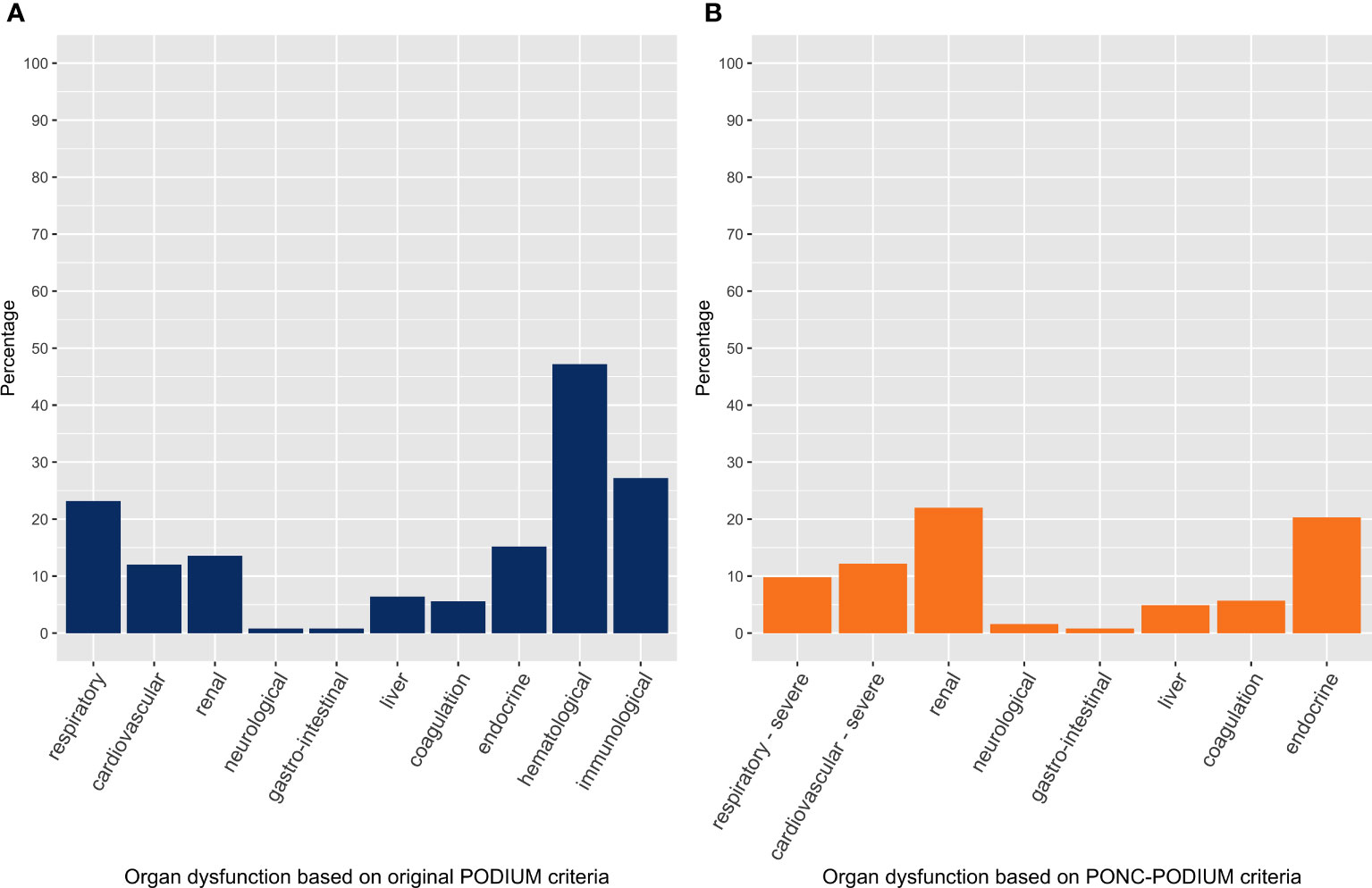
Figure 2 Organ dysfunction at PICU baseline in unplanned PICU admissions with new or progressive multi-organ dysfunction. The left panel (A) considers organ dysfunction based on the original PODIUM criteria, whereas the right panel (B) considers organ dysfunction based on the PONC-PODIUM criteria.
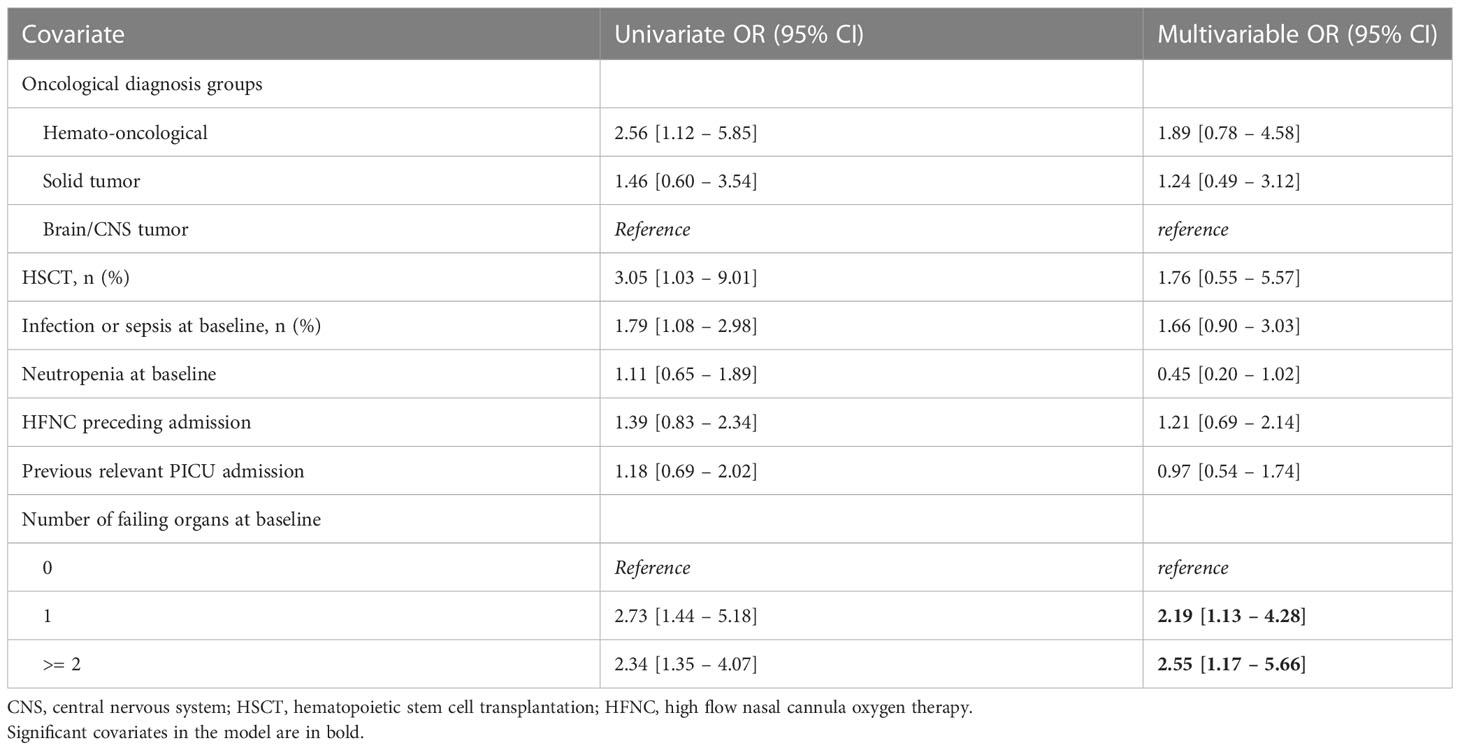
Table 5 Results of the univariate and multivariable logistic regression model, with estimated odds ratio (OR) along with the 95% confidence interval (CI), for outcome of new or progressive multi organ dysfunction in unplanned PICU admissions (defined according to the PODIUM criteria).
Using our PONC-PODIUM criteria in the cohort of unplanned admissions, NPMOD was present in 123 unplanned PICU admissions (43%) (Supplementary Table S5). In the unplanned admissions with NPMOD, the most frequent failing organ systems at admission included renal dysfunction (22%), endocrine dysfunction (20%), and severe cardiovascular dysfunction (12%) (Figure 2B). Consistent with the application of the original PODIUM criteria, the multivariable model showed that the number of failing organs was a significant risk factor associated with the occurrence of NPMOD (Supplementary Table S6).
This is the first study using the recently published PODIUM criteria for organ dysfunction (18) in pediatric oncology patients to identify risk factors for new or progressive multi-organ failure during the first week of PICU admission. Considering all PICU admissions, we found that hemato-oncological diagnosis, unplanned PICU admission and number of failing organs at PICU baseline were independent risk factors. In the subgroup of the unplanned PICU admissions, we found that the number of failing organs at PICU baseline was independently associated with NPMOD.
Our finding that hemato-oncological diagnosis is a significant risk factor for developing NPMOD is in line with other studies showing that hemato-oncological patients have greater illness severity at PICU admission, experience multi-organ failure more often, require more PICU resources and have a higher PICU mortality compared to solid tumor patients (11, 12, 24, 25). The high risk for organ dysfunction may be attributed to the combination of generally more dose-intense chemotherapy and glucocorticoids, that may result in increased toxic side-effects and profound and prolonged myelosuppression (11, 12, 26). Yet, upon analysis in only unplanned PICU admissions, we found that although a hemato-oncological diagnosis was associated with NPMOD in the univariate analysis, it was not a significant risk factor for NPMOD in the multivariable analysis.
Surprisingly, neutropenia was not a significant risk factor both in the total cohort and cohort of unplanned admissions. Some other studies in adult and pediatric oncology patients also failed to demonstrate an association of neutropenia with worse outcomes, in a multivariable analysis (27–29). Advances in the diagnosis and treatment of infections, the prescription of prophylactic antibiotics and antifungals, and antibiotic stewardship may have limited the role of neutropenia in worse outcome in critically ill oncology patients. A recent study including only pediatric hemato-oncology patients with unplanned PICU admissions showed that neutropenia was an independent risk factor for PICU mortality (30). Our study differs in that we also included patients with a solid or a brain or central nervous system tumor. The degree of multi-organ dysfunction during PICU admission is a significant prognostic factor for PICU mortality in pediatric oncology patients (12). We found that the presence of MOD already at PICU admission is an independent risk factor for progressive MOD, in both the total cohort as in the subgroup including only unplanned PICU admissions. These findings are in line with a study in general pediatric patients, showing that the presence of MOD on day 1 of PICU admission was associated with death or poor neurologic outcome (8). Our finding that PICU mortality in patients with NPMOD in the unplanned admissions was only slightly higher compared to the total cohort including also planned post-operative patients, emphasizes the pivotal role of MOD in the outcome of these patients. Early recognition of deteriorating organ functions before PICU admission followed by early initiation of appropriate treatment may be important to reduce morbidity and mortality in critically ill pediatric oncology patients (12, 16, 31, 32).
In the present study, we tailored the PODIUM criteria to pediatric oncology patients. The adjustments in renal criteria can be valuable to prevent missing AKI, as it was shown that AKI, even stage 1, is significantly associated with short- and long-term complications in critically ill children (33). Second, according to PODIUM, neutropenia is a classifier for dysfunction of two different organ systems (hematologic and immunologic), where we included dysfunction that is more likely to be part of a shared underlying pathway for MOD (e.g. in sepsis) instead of chemotherapeutic treatment. Furthermore, we found a high percentage of endocrine dysfunction. The threshold for glucose ≥ 8.3 mmol/L (150 mg/dL) might be a threshold at which particularly hemato-oncology patients are easily flagged, due to steroid-induced adrenal insufficiency or hyperglycemia (34). This threshold could be considered to be fine-tuned and validated in future studies.
Using our PONC-PODIUM criteria, we found different organ systems that frequently failed at PICU admissions. Endocrine, renal and severe cardiovascular dysfunction emerged as the most frequently failing organ systems in patients who develop NPMOD. This finding may merely have implications for early surveillance at the inpatient ward, prior to PICU admission. Particularly renal and cardiovascular dysfunction can be recognized in an early phase, and timely, appropriate interventions may potentially halt progression to irreversible organ damage. For example, the development of acute kidney injury (AKI) can be monitored at the ward, and substitution or adjustments of nephrotoxic medication and prevention of fluid overload can be easily implemented (35). This may lead to decreased AKI rates and better outcomes (33, 35). In addition, closely monitoring the fluid balance and prevention of fluid overload in patients with cardiovascular failure could provide an opportunity to prevent further deterioration.
Our study revealed several challenges in applying predefined criteria for organ dysfunction to a dataset with continuous data at a frequency of 1 minute and interval data. We accounted for measurement errors and missing data. We thereupon defined age-based limits for artefacts in vital signs, carried last observations forward for a limited time defined per variable and classified organ dysfunction within 1-hour timeframes, to minimize that a single value could immediately flag organ dysfunction. Last observation carried forward to deal with missing data was similarly used in a retrospective study on the early prediction of organ dysfunction in children (36). We used the 24 hours preceding PICU admission to classify organ dysfunction at PICU admission. As PODIUM criteria did not incorporate a specific time period required to fulfil the criteria for organ dysfunction, we classified the concurrent number of failing organ systems within 24-hour windows. Yet, for future studies, a validated time period required to fulfil the criteria especially for respiratory and cardiovascular dysfunction may further optimize defining (concurrent) organ dysfunction.
This is the first study including all organ systems of the PODIUM criteria, as we extracted free text field data using an automatized process of text mining with standardized search terms to, for example, identify gastro-intestinal dysfunction. In addition, our study evaluated a PICU cohort that encompasses all subgroups of pediatric oncology patients, including HSCT patients, from a national referral center where oncology care has been nationally centralized.
Our study has several limitations. First, the data retrieved from patients’ medical records were primarily captured for clinical care. Consequently, selective measurements, such as laboratory values only assessed upon clinical suspicion of organ dysfunction, may bias the timing of onset of (multiple) organ dysfunction. Therefore, we summarized to NPMOD within 24-hour-time frames. Second, our study is a single-center study. Consequently, our findings may not be generalizable due to international differences in PICU policies regarding admission and care. Third, we did not have data on morbidity following prior PICU admissions. We therefore defined a relevant prior PICU admission as any prior unplanned admission, or a prior planned admission with a protracted course. For future studies, to assess the effect of a prior PICU admission on the risk of developing NPMOD in a current PICU admission, it would be beneficial to include data on relevant comorbidity following a prior admission. Last, in this retrospective study, we could not differentiate between underlying mechanisms of organ dysfunction and could thus not define MOD syndrome (MODS). The identification of a common underlying pathobiology, such as in MODS, may be helpful to evolve from isolated organ specific to more holistic strategies that target a common pathobiology (4).
This study shows that hemato-oncological diagnosis, number of failing organs and an unplanned admission are significant risk factors at PICU admission for the development of NPMOD in pediatric oncology patients. For future perspectives, we see opportunities to further refine the PODIUM criteria for pediatric oncology patients. Currently, the PODIUM criteria have been validated in general pediatric patients (5), and are yet to be validated in pediatric oncology patients. We provided a first step towards further refinement of these criteria for pediatric oncology patients. Yet, the criteria introduced in this study need to be validated, preferably in a large multi-center cohort incorporating all subgroups of pediatric oncology patients. The results of the present study may help to guide both intensivists and oncologists in risk stratification for critically ill pediatric oncology patients and to identify patients who may benefit from closer monitoring and early interventions at the ward prior to PICU admission.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by IRB protocol number 16-572/C. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
MS, WT and RW-vA designed the project. MS, JN, CB, MM and EK collected the data. MS, MF, and TK conducted the data analyses. MS, MF, JN, EN, TK, WT, and RW-vA drafted the manuscript. MS prepared the tables and figures. MS, MF, TK, WT, and RW-vA had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the analysis. All authors contributed to the article and approved the submitted version.
This work was supported by KiKa (a Dutch research charity foundation for pediatric oncology patients), grant number KiKa 287. The funders had no role in the design, conduct and submission of the study nor in the decision to submit the manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1192806/full#supplementary-material
1. Proulx F, Joyal JS, Mariscalco MM, Leteurtre S, Leclerc F, Lacroix J. The pediatric multiple organ dysfunction syndrome. Pediatr Crit Care Med (2009) 10(1):12–22. doi: 10.1097/PCC.0b013e31819370a9
2. Goldstein B, Giroir B, Randolph A. International consensus conference on pediatric sepsis. international pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med (2005) 6(1):2–8. doi: 10.1097/01.PCC.0000149131.72248.E6
3. Wilkinson JD, Pollack MM, Ruttimann UE, Glass NL, Yeh TS. Outcome of pediatric patients with multiple organ system failure. Crit Care Med (1986) 14(4):271–4. doi: 10.1097/00003246-198604000-00002
4. Weiss SL, Carcillo JA, Leclerc F, Leteurtre S, Schlapbach LJ, Tissieres P, et al. Refining the pediatric multiple organ dysfunction syndrome. Pediatrics (2022) 149(1 Suppl 1):S13–22. doi: 10.1542/peds.2021-052888C
5. Sanchez-Pinto LN, Bembea MM, Farris RW, Hartman ME, Odetola FO, Spaeder MC, et al. Patterns of organ dysfunction in critically ill children based on PODIUM criteria. Pediatrics (2022) 149(1 Suppl 1):S103–S10. doi: 10.1542/peds.2021-052888P
6. Upperman JS, Lacroix J, Curley MA, Checchia PA, Lee DW, Cooke KR, et al. Specific etiologies associated with the multiple organ dysfunction syndrome in children: part 1. Pediatr Crit Care Med (2017) 18(3_suppl Suppl 1):S50–S7. doi: 10.1097/PCC.0000000000001048
7. Leclerc F, Leteurtre S, Duhamel A, Grandbastien B, Proulx F, Martinot A, et al. Cumulative influence of organ dysfunctions and septic state on mortality of critically ill children. Am J Respir Crit Care Med (2005) 171(4):348–53. doi: 10.1164/rccm.200405-630OC
8. Typpo K, Watson RS, Bennett TD, Farris RWD, Spaeder MC, Petersen NJ, et al. Outcomes of day 1 multiple organ dysfunction syndrome in the PICU. Pediatr Crit Care Med (2019) 20(10):914–22. doi: 10.1097/PCC.0000000000002044
9. Leteurtre S, Duhamel A, Salleron J, Grandbastien B, Lacroix J, Leclerc F, et al. PELOD-2: an update of the pediatric logistic organ dysfunction score. Crit Care Med (2013) 41(7):1761–73. doi: 10.1097/CCM.0b013e31828a2bbd
10. Leteurtre S, Martinot A, Duhamel A, Proulx F, Grandbastien B, Cotting J, et al. Validation of the paediatric logistic organ dysfunction (PELOD) score: prospective, observational, multicentre study. Lancet (2003) 362(9379):192–7. doi: 10.1016/S0140-6736(03)13908-6
11. Zinter MS, DuBois SG, Spicer A, Matthay K, Sapru A. Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit. Intensive Care Med (2014) 40(10):1536–44. doi: 10.1007/s00134-014-3389-2
12. Barking CTMM, Masjosthusmann K, Rellensmann G, Ehlert K, Zollner S, Jocham S, et al. Treatment of children with cancer and/or hematopoietic stem cell transplantation in the intensive care unit: experience at a large European pediatric cancer center. J Pediatr Hematol Oncol (2020) 42(7):e583–e8. doi: 10.1097/MPH.0000000000001718
13. Inwald DP, Tasker RC, Peters MJ, Nadel S, Paediatric Intensive Care Society Study Group (PICS-SG). Emergency management of children with severe sepsis in the united kingdom: the results of the paediatric intensive care society sepsis audit. Arch Dis Child (2009) 94(5):348–53. doi: 10.1136/adc.2008.153064
14. Lee DS, Suh GY, Ryu JA, Chung CR, Yang JH, Park CM, et al. Effect of early intervention on long-term outcomes of critically ill cancer patients admitted to ICUs. Crit Care Med (2015) 43(7):1439–48. doi: 10.1097/CCM.0000000000002314
15. Song JU, Suh GY, Park HY, Lim SY, Han SG, Kang YR, et al. Early intervention on the outcomes in critically ill cancer patients admitted to intensive care units. Intensive Care Med (2012) 38(9):1505–13. doi: 10.1007/s00134-012-2594-0
16. Fausser JL, Tavenard A, Rialland F, Le Moine P, Minckes O, Jourdain A, et al. Should we pay attention to the delay before admission to a pediatric intensive care unit for children with cancer? impact on 1-month mortality. a report from the French children's oncology study group, GOCE. J Pediatr Hematol Oncol (2017) 39(5):e244–48. doi: 10.1097/MPH.0000000000000816
17. Pillon M, Amigoni A, Contin A, Cattelan M, Carraro E, Campagnano E, et al. Risk factors and outcomes related to pediatric intensive care unit admission after hematopoietic stem cell transplantation: a single-center experience. Biol Blood Marrow Transplant (2017) 23(8):1335–41. doi: 10.1016/j.bbmt.2017.04.016
18. Bembea MM, Agus M, Akcan-Arikan A, Alexander P, Basu R, Bennett TD, et al. Pediatric organ dysfunction information update mandate (PODIUM) contemporary organ dysfunction criteria: executive summary. Pediatrics (2022) 149(1 Suppl 1):S1–S12. doi: 10.1542/peds.2021-052888B
19. Wösten-van Asperen RM, van Gestel JPJ, van Grotel M, Tschiedel E, Dohna-Schwake C, Valla FV, et al. PICU mortality of children with cancer admitted to pediatric intensive care unit a systematic review and meta-analysis. Crit Rev Oncol Hematol (2019) 142:153–63. doi: 10.1016/j.critrevonc.2019.07.014
20. Raymakers-Janssen PAMA, Lilien MR, Tibboel D, Kneyber MCJ, Dijkstra S, van Woensel JBM, et al. Epidemiology and outcome of critically ill pediatric cancer and hematopoietic stem cell transplant patients requiring continuous renal replacement therapy: a retrospective nationwide cohort study. Crit Care Med (2019) 47(11):e893–901. doi: 10.1097/CCM.0000000000003973
21. Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis (2020) 71(6):1367–76. doi: 10.1093/cid/ciz1008
22. DiCiccio TJ, Efron B. Bootstrap confidence intervals. Stat Sci (1996) 11(3):189–228. doi: 10.1214/ss/1032280214
23. Team RC. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2019).
24. Heying R, Schneider DT, Korholz D, Stannigel H, Lemburg P, Gobel U. Efficacy and outcome of intensive care in pediatric oncologic patients. Crit Care Med (2001) 29(12):2276–80. doi: 10.1097/00003246-200112000-00007
25. Owens C, Mannion D, O'Marcaigh A, Waldron M, Butler K, O'Meara A. Indications for admission, treatment and improved outcome of paediatric haematology/oncology patients admitted to a tertiary paediatric ICU. Ir J Med Sci (2011) 180(1):85–9. doi: 10.1007/s11845-010-0634-8
26. Loeffen EAH, Knops RRG, Boerhof J, Feijen E, Merks JHM, Reedijk AMJ, et al. Treatment-related mortality in children with cancer: prevalence and risk factors. Eur J Cancer (2019) 121:113–22. doi: 10.1016/j.ejca.2019.08.008
27. Bouteloup M, Perinel S, Bourmaud A, Azoulay E, Mokart D, Darmon M, et al. Outcomes in adult critically ill cancer patients with and without neutropenia: a systematic review and meta-analysis of the groupe de recherche en reanimation respiratoire du patient d'Onco-hematologie (GRRR-OH). Oncotarget (2017) 8(1):1860–70. doi: 10.18632/oncotarget.12165
28. Dursun O, Hazar V, Karasu GT, Uygun V, Tosun O, Yesilipek A. Prognostic factors in pediatric cancer patients admitted to the pediatric intensive care unit. J Pediatr Hematol Oncol (2009) 31(7):481–4. doi: 10.1097/MPH.0b013e3181a330ef
29. Zaidman I, Mohamad H, Shalom L, Ben Arush M, Even-Or E, Averbuch D, et al. Survival of pediatric patients requiring admission in the intensive care unit post hematopoietic stem cell transplantation: prognostic factors associated with mortality. Pediatr Blood Cancer (2022) 69(3):e29549. doi: 10.1002/pbc.29549
30. Pechlaner A, Kropshofer G, Crazzolara R, Hetzer B, Pechlaner R, Cortina G. Mortality of hemato-oncologic patients admitted to a pediatric intensive care unit: a single-center experience. Front Pediatr (2022) 10:795158. doi: 10.3389/fped.2022.795158
31. Piastra M, Fognani G, Franceschi A, Oncology IINFICIP. Pediatric intensive care unit admission criteria for haemato-oncological patients: a basis for clinical guidelines implementation. Pediatr Rep (2011) 3(2):e13. doi: 10.4081/pr.2011.e13
32. Lindell RB, Gertz SJ, Rowan CM, McArthur J, Beske F, Plunkett A, et al. High levels of morbidity and mortality among pediatric hematopoietic cell transplant recipients with severe sepsis: insights from the sepsis PRevalence, OUtcomes, and therapies international point prevalence study. Pediatr Crit Care Med (2017) 18(12):1114–25. doi: 10.1097/PCC.0000000000001338
33. Sanchez-Pinto LN, Goldstein SL, Schneider JB, Khemani RG. Association between progression and improvement of acute kidney injury and mortality in critically ill children. Pediatr Crit Care Med (2015) 16(8):703–10. doi: 10.1097/PCC.0000000000000461
34. Lowas SR, Marks D, Malempati S. Prevalence of transient hyperglycemia during induction chemotherapy for pediatric acute lymphoblastic leukemia. Pediatr Blood Cancer (2009) 52(7):814–8. doi: 10.1002/pbc.21980
35. Goldstein SL, Dahale D, Kirkendall ES, Mottes T, Kaplan H, Muething S, et al. A prospective multi-center quality improvement initiative (NINJA) indicates a reduction in nephrotoxic acute kidney injury in hospitalized children. Kidney Int (2020) 97(3):580–8. doi: 10.1016/j.kint.2019.10.015
Keywords: pediatric oncology, intensive care unit, multi-organ dysfunction, critical care, prognosis
Citation: Soeteman M, Fiocco MF, Nijman J, Bollen CW, Marcelis MM, Kilsdonk E, Nieuwenhuis EES, Kappen TH, Tissing WJE and Wösten-van Asperen RM (2023) Prognostic factors for multi-organ dysfunction in pediatric oncology patients admitted to the pediatric intensive care unit. Front. Oncol. 13:1192806. doi: 10.3389/fonc.2023.1192806
Received: 23 March 2023; Accepted: 26 June 2023;
Published: 12 July 2023.
Edited by:
Jennifer Ann McArthur, St. Jude Children’s Research Hospital, United StatesReviewed by:
Shira Jolene Gertz, Cooperman Barnabas Medical Center, United StatesCopyright © 2023 Soeteman, Fiocco, Nijman, Bollen, Marcelis, Kilsdonk, Nieuwenhuis, Kappen, Tissing and Wösten-van Asperen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roelie M. Wösten-van Asperen, ci5tLnZhbmFzcGVyZW5AdW1jdXRyZWNodC5ubA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.