 Dan Cao1
Dan Cao1 Zongxin Zhang2*
Zongxin Zhang2*- 1Department of Hematology, Huzhou Central Hospital, Affiliated Central Hospital of Huzhou University, Huzhou, Zhejiang, China
- 2Clinical Laboratory, Huzhou Central Hospital, Affiliated Central Hospital of Huzhou University, Huzhou, Zhejiang, China
Background: Previous studies have explored the relationship between the geriatric nutritional risk index (GNRI) and survival outcomes of diffuse large B-cell lymphoma (DLBCL) cases, but the results were inconsistent. Consequently, the present meta-analysis was conducted to investigate how GNRI affects DLBCL and its function in terms of prognosis.
Methods: The Web of Science, PubMed, Embase, and Cochrane Library databases were thoroughly searched until January 18, 2023. We calculated combined hazard ratios (HRs) and 95% confidence intervals (CIs) to estimate the relationship between the GNRI and survival outcomes of patients with DLBCL.
Results: This meta-analysis included seven articles involving 2,353 cases. A lower level of GNRI predicted dismal overall survival (HR=1.40, 95% CI=1.25–1.56, p<0.001) and inferior progression-free survival (HR=1.46, 95% CI=1.19-1.80, p<0.001) of DLBCL patients. Moreover, a low GNRI was significantly related to Eastern Cooperative Oncology Group Performance Status ≥2 (odds ratio [OR]=4.55, 95% CI=2.75–7.54, p<0.001), Ann Arbor stage III–IV (OR=2.91, 95% CI=2.38–3.57, p<0.001), B symptoms (OR=3.51, 95% CI=2.34–5.29, p<0.001), and extranodal disease (OR=2.90, 95% CI=2.32–3.63, p<0.001).
Conclusion: A lower GNRI level predicted poorer short- and long-term prognosis in patients with DLBCL. A low GNRI was correlated with clinical factors of disease progression in DLBCL patients.
Introduction
Among non-Hodgkin lymphoid (NHL) malignancies, diffuse large B-cell lymphoma (DLBCL) accounts for the highest proportion (30–40% of NHL cases) (1). Approximately 60% of the DLBCL cases can be treated using standard therapeutic regimens (such as rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) (2). However, 45–50% of the cases relapse or become refractory after a complete response (3). The prognosis for patients experiencing relapse is poor because 80% of them ultimately die from DLBCL, even after treatment with subsequent regimens (4). The poor survival outcomes of DLBCL patients are partially due to the lack of effective prognostic markers. Therefore, identifying novel and readily available biomarkers is important for the prognosis of DLBCL.
Growing evidence has shown that nutritional status and immune responses play essential roles in tumor initiation, development, and metastasis (5, 6). Many parameters derived from laboratory examinations have drawn considerable attention because of their prognostic value. Recently, numerous studies reported the relationship between a series of serum-based parameters and the prognosis of DLBCL (7–10). These indexes include the lymphocyte-to-monocyte ratio (7), neutrophil-to-lymphocyte ratio (NLR) (8), C-reactive protein (9), and platelet-to-lymphocyte ratio (PLR) (10). The geriatric nutritional risk index (GNRI) is a nutritional marker that includes patient’s body weight (BW), height, and serum albumin content. It is calculated by the formula: GNRI = 1.487 × serum albumin (g/L) + 41.7 × present/optimal BW (kg) (11). In clinical settings, the GNRI is used as a simple nutrition evaluation approach, and a low GNRI indicates poor nutritional status of patients (12, 13). In recent years, numerous studies have analyzed the role of GNRI in predicting the prognosis of DLBCL cases (14–20), but their findings remain controversial. For example, in some studies, low GNRI significantly predicted poor survival in DLBCL patients (14, 16, 19). However, other researchers have reported that the GNRI is not related to DLBCL survival (15). Previous studies that adopted different cut-off values of the GNRI could also contribute to the conflicting results. Therefore, we searched recent literatures and carried out a meta-analysis to identify whether the GNRI predicted DLBCL prognosis accurately.
Materials and methods
Study guideline
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (21).
Literature search
Studies were identified in the Web of Science, PubMed, Embase, and Cochrane Library databases. The search strategies were as follows: (geriatric nutritional risk index or GNRI) and (diffuse large B-cell lymphoma or DLBCL or lymphoma). Detailed search strategies for each database are provided in Supplementary File 1. Retrieval timeline was from inception until January 18, 2023. Only publications published in the English language were considered. Relevant documents in references of the identified studies were also searched.
Eligibility criteria
Studies conforming to the following criteria were included (1): cases with a pathological diagnosis of DLBCL; (2) GNRI determined prior to anticancer therapy; (3) studies mentioning the function of GNRI in predicting prognosis, such as overall survival (OS), progression-free survival (PFS), recurrence-free survival (RFS), and cancer-specific survival (CSS); (4) studies with available hazard ratios (HRs) together with associated 95% confidence intervals (CIs) regarding patient outcomes; (5) studies with a threshold to classify high/low GNRI; and (6) articles written in the English language. Studies conforming to the following standards were excluded: (1) reviews, case reports, meeting abstracts, letters, and correspondences; (2) articles that included overlapping patients; and (3) animal studies.
Data collection and quality evaluation
Two independent reviewers (D.C. and Z.Z.) were responsible for data collection from qualified articles. Any disagreement between the reviewers was resolved through mutual negotiation until a consensus was reached. The following data were collected: name of first author, country, publication year, sample size, age, sex, study duration, follow-up, threshold GNRI, threshold measurement approach, study center, survival analysis, survival endpoints, treatment, and HRs with 95% CIs. The methodological quality of the eligible articles was evaluated using the Newcastle–Ottawa scale (NOS) (22). Articles with NOS scores of ≥6 were regarded as high-quality articles.
Statistical analysis
Combined HRs and 95% CIs were determined to estimate the relationship between the GNRI and survival outcomes in the DLBCL cases. Heterogeneity among the enrolled articles was analyzed using I2 statistics and the Cochran’s Q test. An I2 statistics of ≥50% and/or p<0.10 on the Cochran Q test indicated obvious heterogeneity, and the random-effects model was used; otherwise, the fixed-effects model was adopted. Diverse factor-stratified subgroup analyses were carried out to detect sources of heterogeneity. Correlations of GNRI with clinicopathological features in DLBCL were explored by combining odds ratios (ORs) and associated 95% CIs. The Begg’s test was used for publication bias, while an asymmetry assessment was performed using a funnel plot. All statistical analyses were carried out using Stata software (version 12.0; Stata Corporation, College Station, TX, USA). Statistical significance was set at p<0.05 (two-sided), which represented statistical significance.
Ethnics statement
The need for ethical approval was waived from this work, and no informed consent was obtained because no patient information was involved.
Results
Study selection process
As shown in Figure 1, the original study selection detected 60 studies, and after removal of the duplicates, 32 records remained. Subsequently, titles and abstracts were scanned, and 21 articles were discarded because of their irrelevance. By reading the full texts of 11 articles, 4 articles were then eliminated due to no cut-off value of GNRI (n=3) and inclusion of overlapping patients (n=1). Finally, seven articles, involving 2,353 cases (14–20), were included in the present study (Figure 1; Table 1).
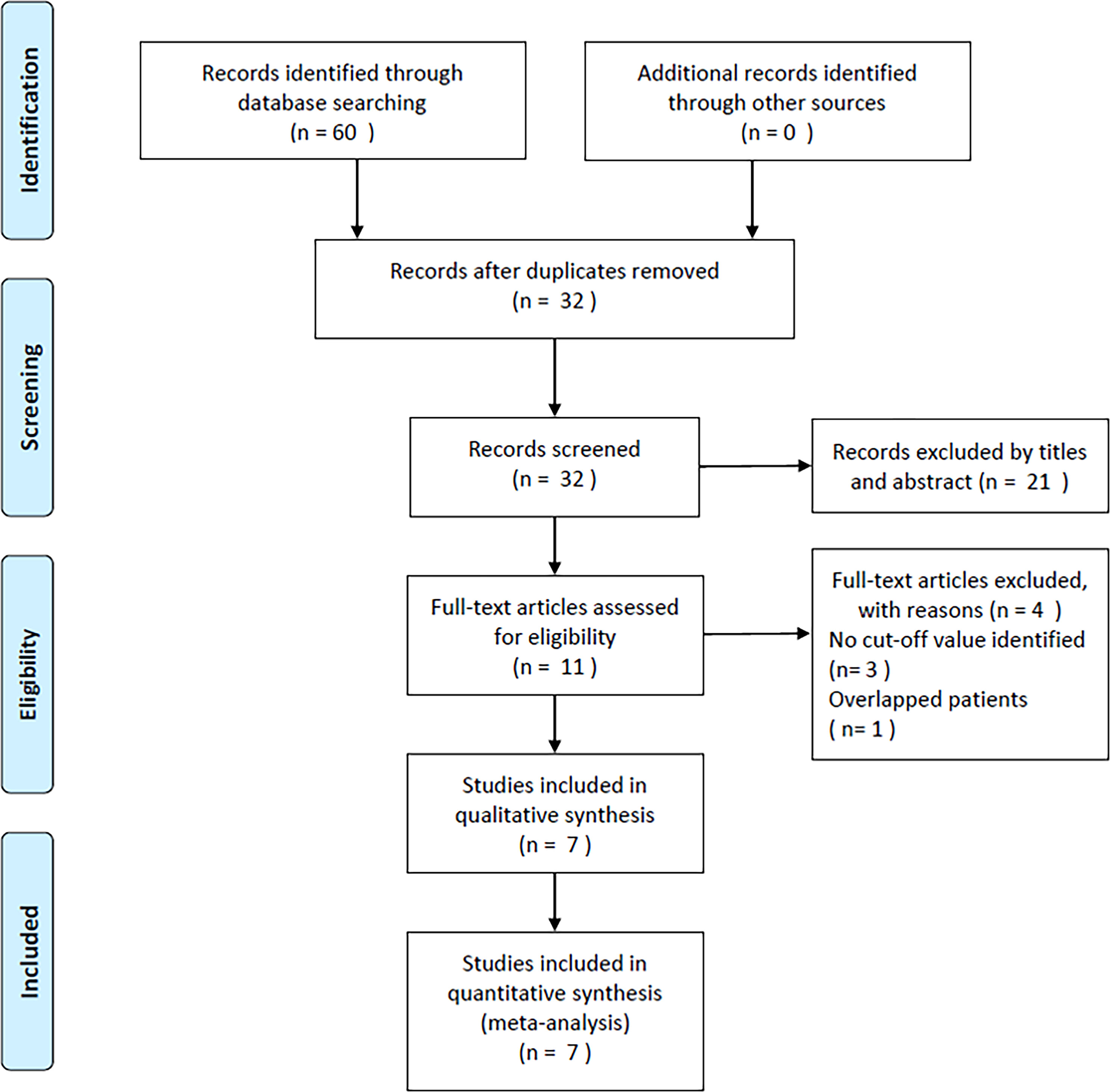
Figure 1 PRISMA flow diagram of the study selection process.
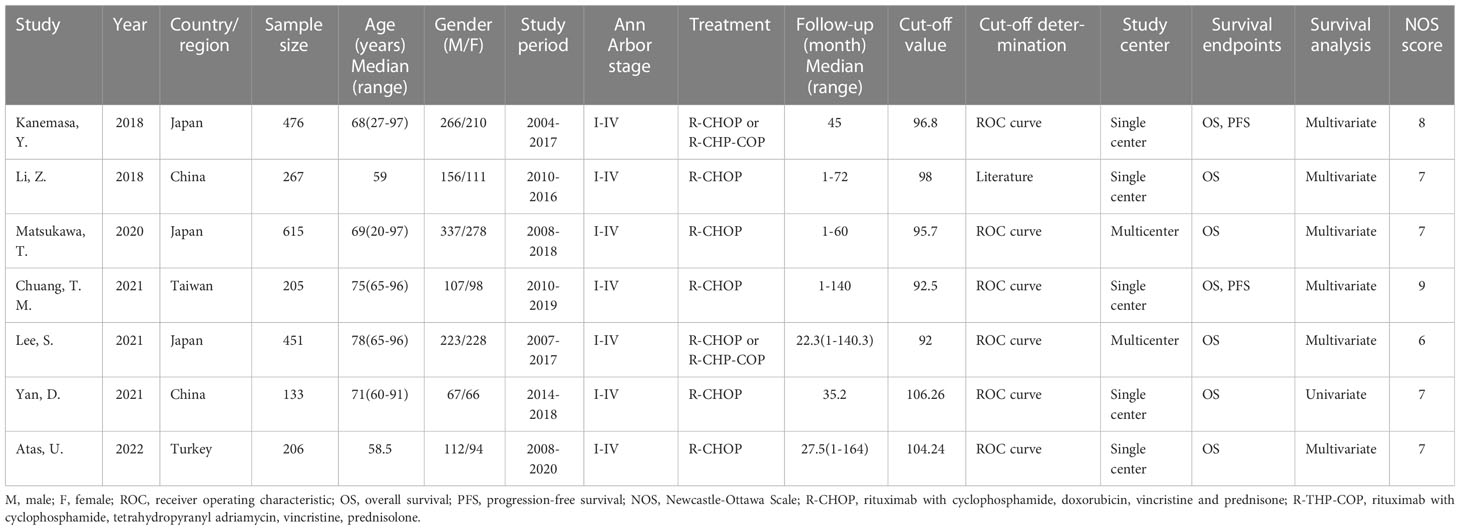
Table 1 Baseline characteristics of included studies in this meta-analysis.
Qualified article characteristics
Table 1 shows the basic characteristics of the qualified articles. All the eligible articles were published between 2018–2022 (14–20). Three studies were conducted in Japan (14, 16, 18), two in China (15, 19), and one each in Taiwan (17) and Turkey (20). The sample size was 133–615 (median, 267). All the included studies had a retrospective design and enrolled DLBCL patients with Ann Arbor stage I–IV (14–20). The threshold GNRI was 92–106.26 (median, 96.8). Six studies analyzed thresholds with receiver operating characteristic (ROC) curves (14, 16–20), while one study selected cut-off values according to the literature (15). Five studies were carried out in a single center (14, 15, 17, 19, 20), and two were multicenter trials (16, 18). All seven articles mentioned the role of GNRI in predicting OS (14–20), and two studies reported an association between the GNRI and PFS (14, 17) in DLBCL. Six articles mentioned the HRs and 95% CIs through multivariate regression (14–18, 20), and one study adopted a univariate analysis (19). The NOS scores were 6–9 (median, 7), indicating high quality.
Prognostic value of GNRI for OS and PFS
Seven articles with 2,353 patients (14–20) reported GNRI values for predicting OS in DLBCL. No obvious heterogeneity (I2 = 48.8%, p=0.069) was detected; therefore, we selected a fixed-effects model. According to Table 2 and Figure 2, the combined results were: HR=1.40, 95% CI=1.25–1.56, p<0.001, demonstrating that low GNRI was markedly associated with poor OS in DLBCL. Subgroup analysis by various factors was conducted (Table 2), which showed that the reduced GNRI significantly predicted poor OS, regardless of the study center, sample size, treatment, or survival analysis type. Furthermore, a lower GNRI markedly predicted poor OS when using a cut-off value of <98 when the patients’ median age was ≥60 years, and cut-off values were determined using the ROC curve (Table 2). Two studies involving 681 patients reported an association between the GNRI and PFS in DLBCL (14, 17). Based on the combined data, a lower GNRI significantly predicted dismal PFS in DLBCL cases (HR=1.46, 95% CI=1.19–1.80, p<0.001; Figure 3 and Table 2).
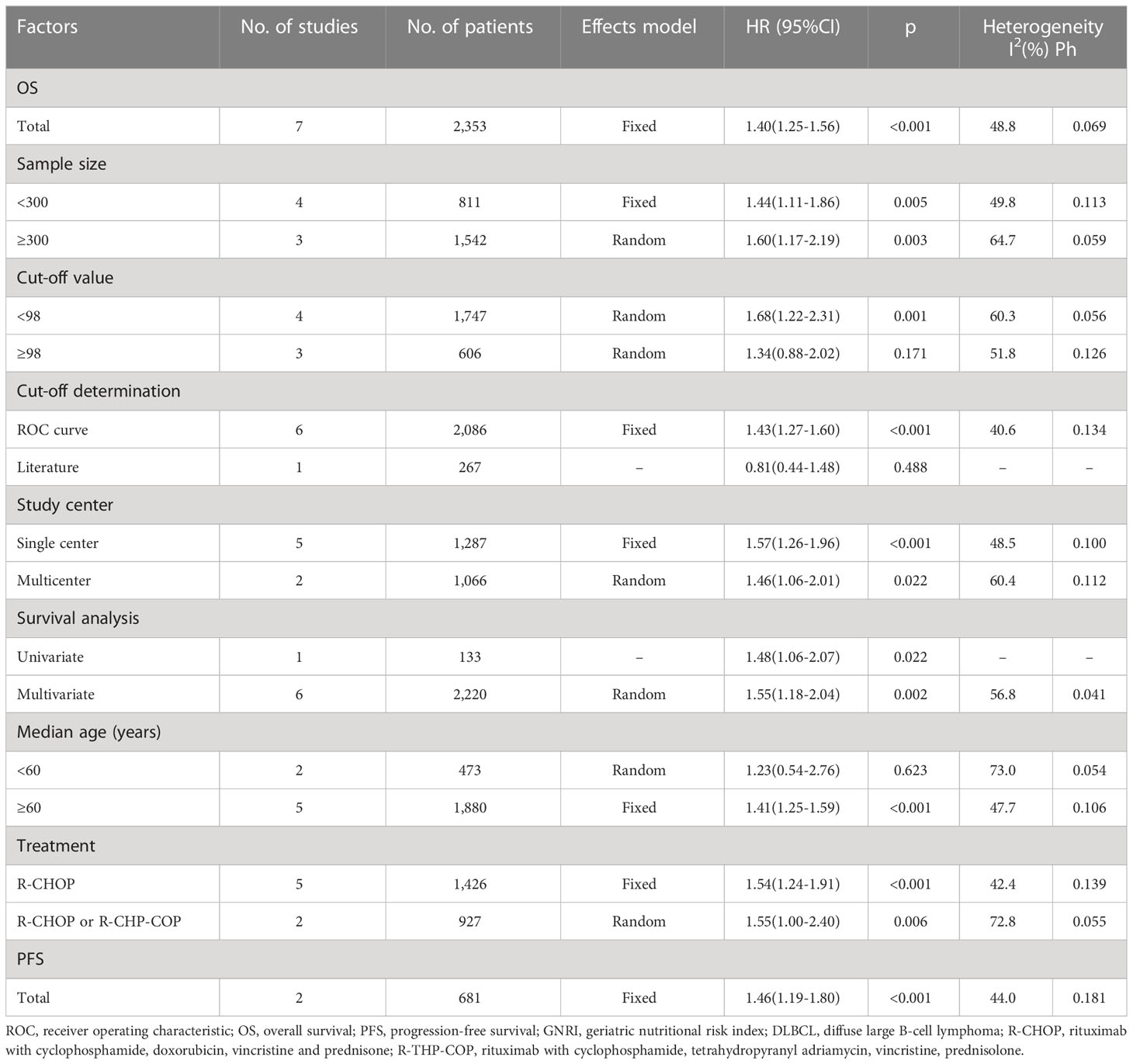
Table 2 Subgroup analysis of the prognostic value of GNRI for OS and PFS in patients with DLBCL.
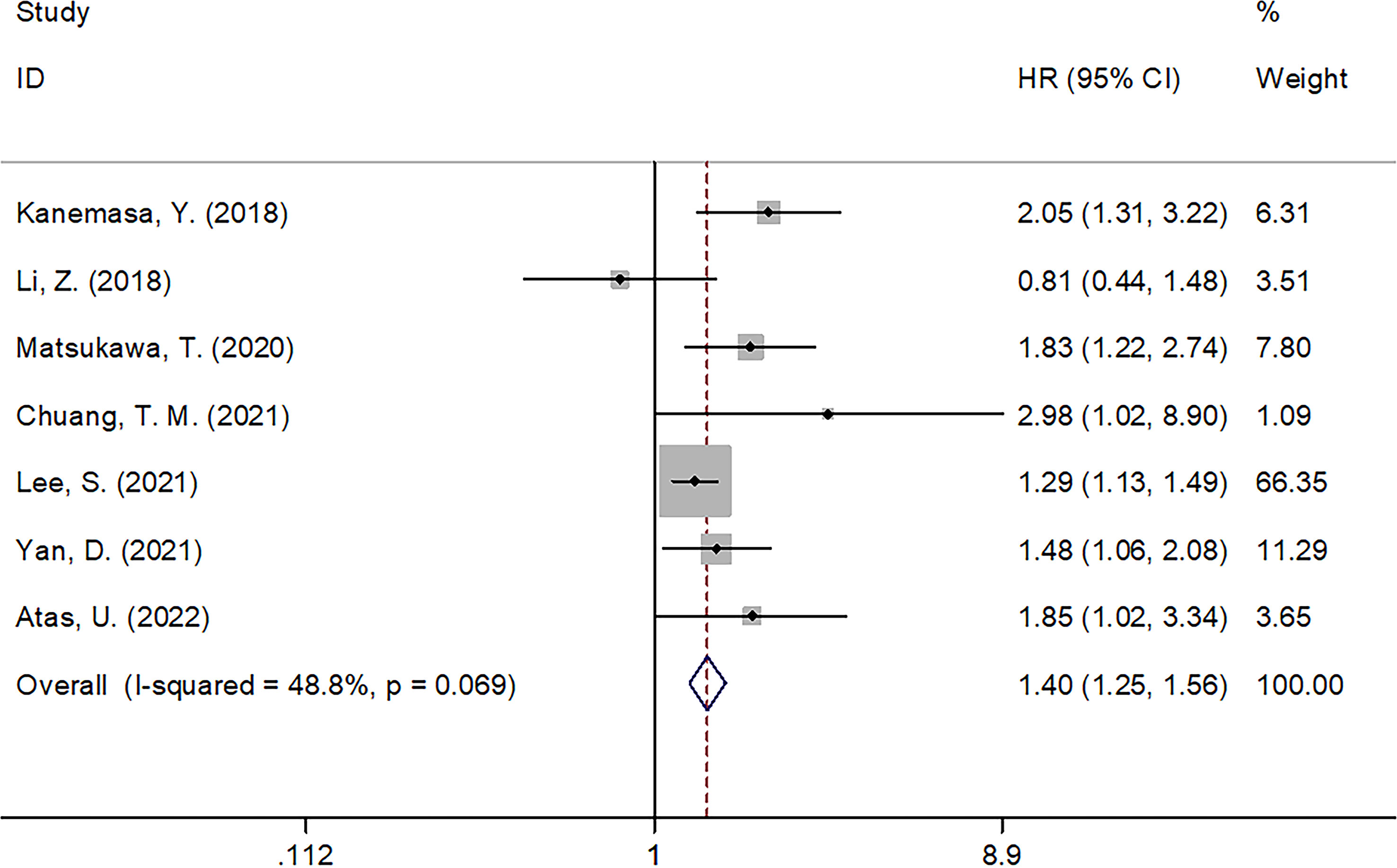
Figure 2 Forest plot of the association of GNRI with OS in patients with DLBCL.
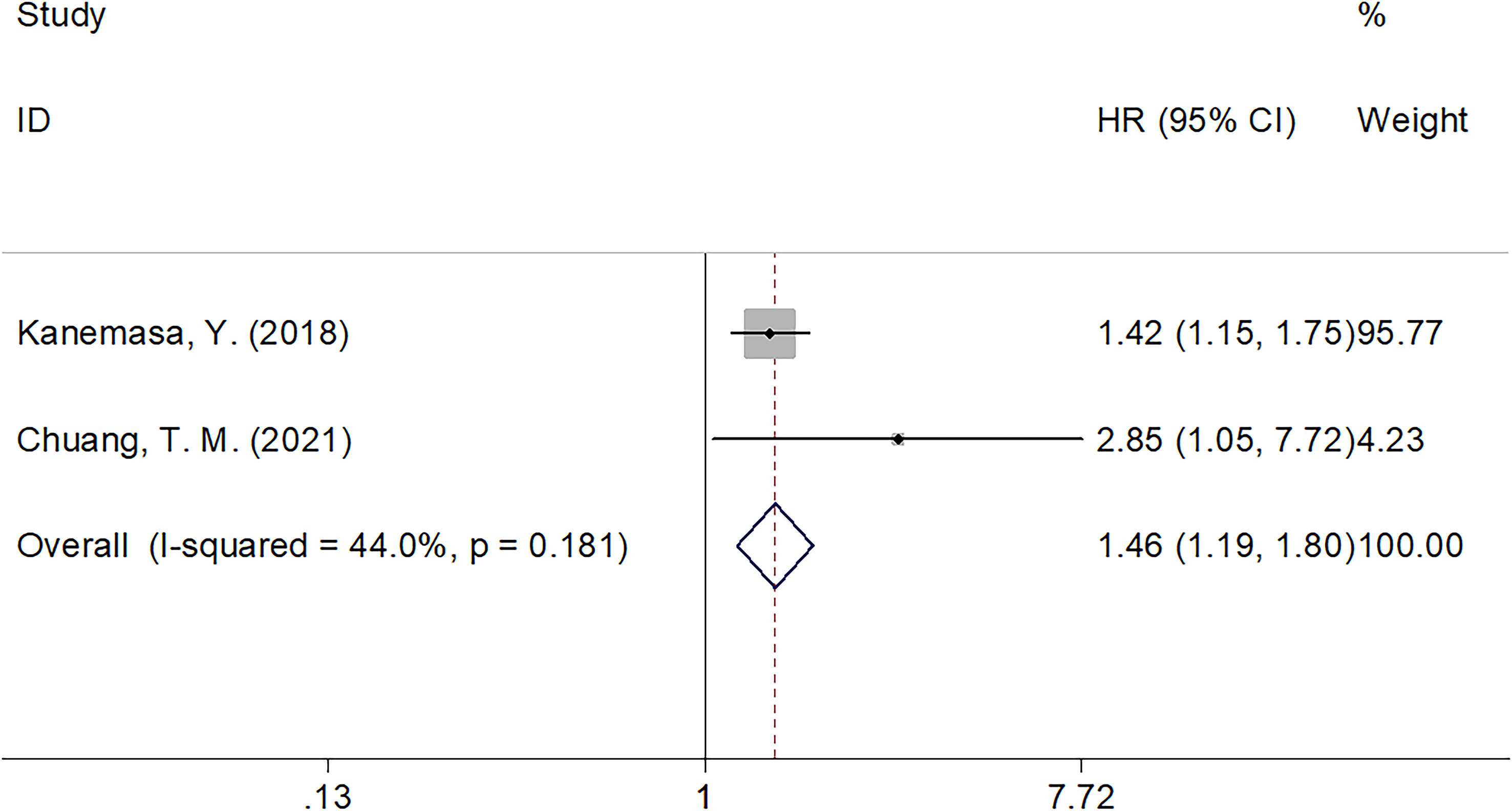
Figure 3 Forest plot of the association of GNRI with PFS in patients with DLBCL.
Relationship of GNRI with clinicopathological factors
Five studies, involving 1,769 cases, mentioned the correlation between the GNRI and clinicopathological characteristics of DLBCL (14–17, 20). As shown in Table 3 and Figure 4, the combined results revealed a marked relation between the lower GNRI and Eastern Cooperative Oncology Group Performance Status (ECOG-PS) ≥2 (OR=4.55, 95% CI=2.75–7.54, p<0.001), Ann Arbor stage III–IV (OR=2.91, 95% CI=2.38–3.57, p<0.001), B symptoms (OR=3.51, 95% CI=2.34–5.29, p<0.001), and extranodal disease (OR=2.90, 95% CI=2.32–3.63, p<0.001). Nonetheless, the GNRI was not significantly related to sex in DLBCL (OR=0.93, 95% CI=0.77–1.12, p=0.436; Table 3; Figure 4).
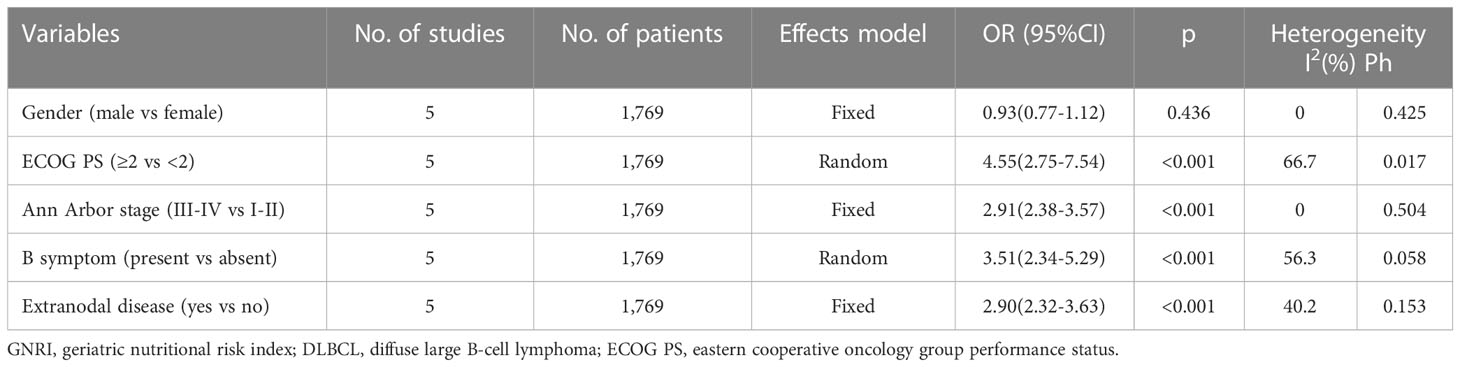
Table 3 The association between GNRI and clinicopathological features in patients with DLBCL.
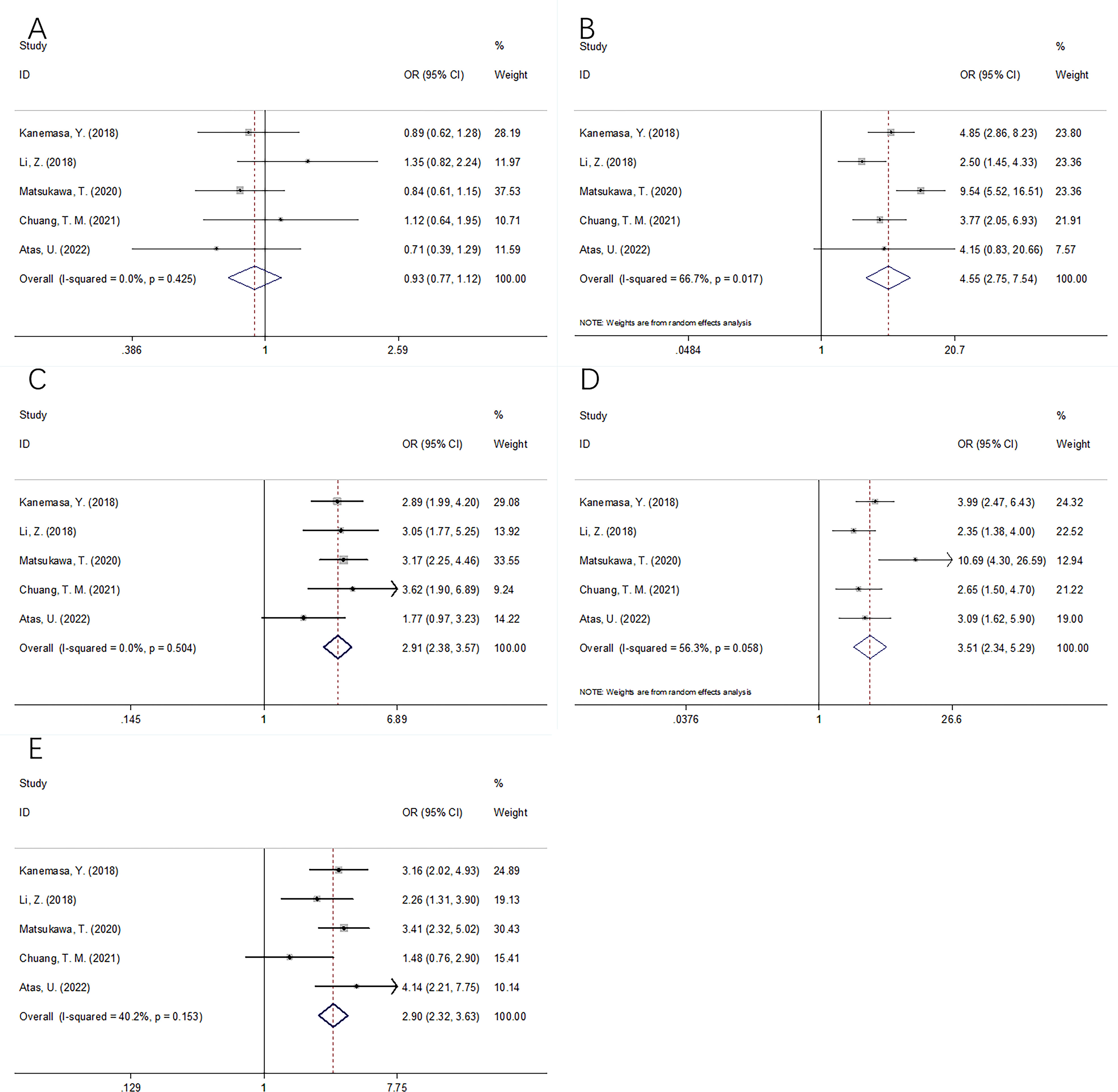
Figure 4 Forest plots of the correlation between GNRI and clinicopathological features in DLBCL patients. (A) Gender (male vs female); (B) ECOG PS (≥2 vs <2); (C) Ann Arbor stage (III-IV vs I-II); (D) B symptom (present vs absent); and (E) Extranodal disease (yes vs no).
Publication bias
We adopted the Begg’s test and funnel plot to examine possible publication bias. As shown in Figure 5, symmetry was observed in the funnel plot, and the Begg’s test (p=0.368 and 0.317 for OS and PFS, respectively) revealed no evidence of obvious publication bias.
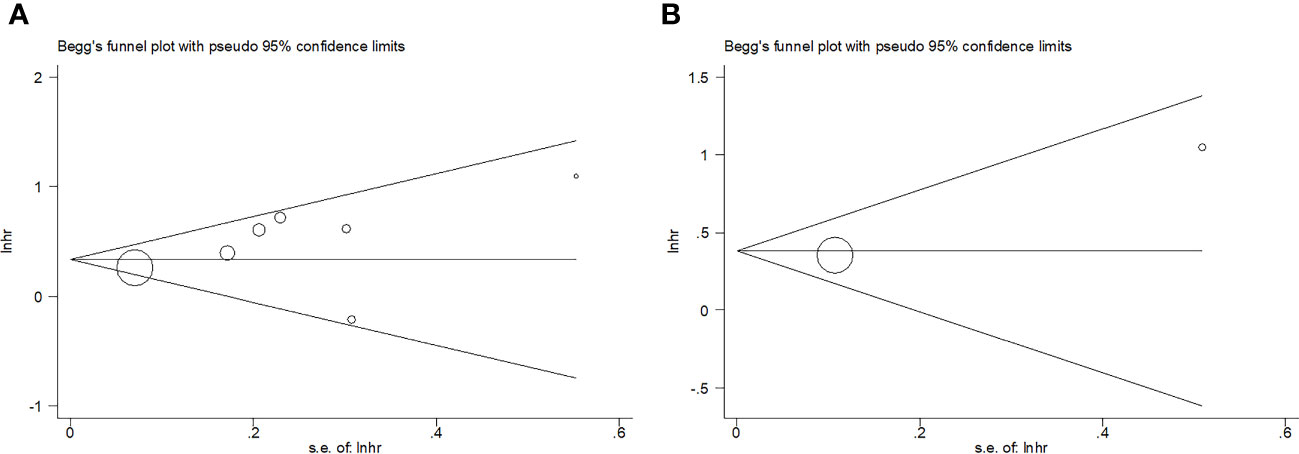
Figure 5 Publication bias. (A) OS, Begg’s test, p=0.368; (B) PFS, Begg’s test, p=0.317.
Discussion
The role of GNRI in predicting prognosis in patients with DLBCL is controversial based on prior articles. We obtained data from seven articles, comprising 2,353 cases and showed that a lower GNRI markedly predicted worse OS and PFS in DLBCL patients. Based on subgroup analysis, the GNRI reliably predicted OS, especially when the cut-off value was <92. This meta-analysis also revealed that decreased GNRI was significantly associated with clinical factors representing aggressive biological behavior, i.e., ECOG-PS ≥2, Ann Arbor stage III–IV, B symptoms, and extranodal disorder. These factors are well known high-risk factors for disease progression and dismal outcomes in DLBCL cases. Taken together, low GNRI significantly predicted poor OS and PFS in DLBCL patients. To the best of our knowledge, this is the first meta-analysis to analyze the role of GNRI in predicting DLBCL prognosis.
The GNRI is a beneficial tool for assessing nutritional status in clinical practice. There are several cancers for which the GNRI comprises serum albumin levels, BW, and height, which are identified as efficient prognostic factors (13, 23, 24). The correlation mechanism between the GNRI and DLBCL prognosis was interpreted based on components of the GNRI for cancer cases. Approximately 90% of the serum proteins are derived from albumin, which is produced by the liver. Albumin is essential to the human body (25). In addition to reflecting the nutritional status of the human body, serum albumin is a measure of inflammation (26). Albumin has a key effect in maintaining blood colloid osmotic pressure and delivering pharmaceuticals, hormones, cations, and fatty acids (27). Capillary permeability is increased by cancer-related inflammation, which allows serum albumin to escape into the interstitium. Second, >10% BW loss indicates protein-energy malnutrition (28). In comparison with normal-weight cases, underweight DLBCL cases have worse OS and PFS, according to a meta-analysis involving 8,753 participants (29). Patient outcomes have been shown to be significantly affected by weight, as a modifiable factor, and weight management should be aggressive during treatment (30). Finally, low GNRI, possibly caused by weight loss and decreased serum albumin content, is a reasonable and cost-effective prognostic marker for patients with DLBCL.
Notably, previous studies have also explored the prognostic value of several inflammatory parameters, such as the Glasgow prognostic score (GPS) (31), NLR (32), and PLR (33). These studies demonstrated that high GPS and elevated NLR and PLR remained effective prognostic indices for patients with DLBCL (31–33). The GNRI has several advantages and disadvantages compared with GPS, NLR, and PLR. The GNRI is a tool used for nutritional assessment. The nutritional status of patients could be directly reflected by the GNRI, but the GPS, NLR, and PLR have no such function. Second, the GNRI is a novel index that has drawn considerable attention in recent years. The clinical application of the GNRI is much more promising than that of the GPS, NLR, and PLR. However, disadvantages of the GNRI should also be acknowledged. Calculation of the GNRI is more complex than that of the GPS, NLR, and PLR.
We performed a subgroup analysis according to the median age and treatment regimens. As shown in Table 2, the results indicated that the GNRI remained a prognostic factor for OS in patients with a median age ≥60 years, and the prognostic role was not influenced by treatment strategies. Therefore, the GNRI could be a reliable prognostic indicator for DLBCL patients aged ≥60 years, whether they received the rituximab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate (Oncovin), and prednisone (R-CHOP) or R-CHOP-like regimens. The association between the GNRI and clinicopathological factors was analyzed, and the results are shown in Figure 4 and Table 3. We do not think that these associations are causal because the sample size was relatively sufficient (five studies with 1,769 participants). Moreover, the p-value was <0.001 in these groups, indicating a positive relationship.
Recent meta-analyses have reported that the GNRI significantly predicts cancer prognosis (34–38). Zhang et al. conducted a meta-analysis of 5,593 patients and showed that the GNRI performed well in predicting long-term survival, as well as complications among surgical gastric cancer cases (34). Zhou et al. reported that a low GNRI estimated dismal OS and CSS in esophageal cancer cases in a meta-analysis of 11 studies (39). A recent meta-analysis involving 3,440 participants showed that a lower GNRI before treatment predicted poorer OS and disease-free survival of colorectal cancer cases (40). Another meta-analysis enrolling 6,792 patients indicated that a lower GNRI strongly estimated dismal OS, RFS/PFS, and CSS in urological cancers (38). According to Wang et al., a low GNRI predicted dismal OS, RFS, and CSS in lung cancer cases (41).
Some limitations of the present study should be noted. First, the enrolled articles were retrospective studies, which are not as convincing as randomized controlled trials. Second, all the eligible studies were conducted in Asia. Therefore, the role of GNRI in predicting the prognosis of DLBCL in non-Asian populations should be verified. Third, an optimum cut-off value of the GNRI was not determined in the included studies, which might have caused selection bias. Therefore, large-scale trials in multicenter regions should be conducted for further verification.
Conclusions
In summary, a low GNRI predicts poorer short- and long-term DLBCL prognosis. A low GNRI was correlated with clinical factors of disease progression in DLBCL.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
DC and ZZ designed and conceived the study. DC and ZZ collected the data. DC analyze the data and performed the statistical analysis. ZZ gave the important guidance for statistical analysis and methodology. DC and ZZ provided critical intellectual contributions. DC drafted the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1169749/full#supplementary-material
Abbreviations
GNRI, geriatric nutritional risk index; DLBCL, diffuse large B-cell lymphoma; HR, hazard ratio; CI, confidence interval; OS, overall survival; PFS, progression-free survival; ECOG-PS, eastern cooperative oncology group performance status; NHL, non-Hodgkin lymphoid; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; CRP, C-reactive protein; PLR, platelet-to-lymphocyte ratio; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; NOS, Newcastle-Ottawa Scale; OR, odds ratio; ROC, receiver operating characteristic.
References
1. Susanibar-Adaniya S, Barta SK. 2021 Update on diffuse large b cell lymphoma: A review of current data and potential applications on risk stratification and management. Am J Hematol (2021) 96(5):617–29. doi: 10.1002/ajh.26151
2. Cheson BD, Nowakowski G, Salles G. Diffuse large b-cell lymphoma: New targets and novel therapies. Blood Cancer J (2021) 11(4):68. doi: 10.1038/s41408-021-00456-w
3. Crump M, Neelapu SS, Farooq U, Van Den Neste E, Kuruvilla J, Westin J, et al. Outcomes in refractory diffuse large b-cell lymphoma: Results from the international SCHOLAR-1 study. Blood (2017) 130(16):1800–8. doi: 10.1182/blood-2017-03-769620
4. He MY, Kridel R. Treatment resistance in diffuse large b-cell lymphoma. Leukemia (2021) 35(8):2151–65. doi: 10.1038/s41375-021-01285-3
5. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell (2010) 140(6):883–99. doi: 10.1016/j.cell.2010.01.025
6. Hanahan D, Weinberg RA. Hallmarks of cancer: The next generation. Cell (2011) 144(5):646–74. doi: 10.1016/j.cell.2011.02.013
7. Li YL, Pan YY, Jiao Y, Ning J, Fan YG, Zhai ZM. Peripheral blood lymphocyte/monocyte ratio predicts outcome for patients with diffuse large b cell lymphoma after standard first-line regimens. Ann Hematol (2014) 93(4):617–26. doi: 10.1007/s00277-013-1916-9
8. Wang J, Zhou M, Xu JY, Yang YG, Zhang QG, Zhou RF, et al. Prognostic role of pretreatment neutrophil-lymphocyte ratio in patients with diffuse large b-cell lymphoma treated with RCHOP. Med (Baltimore) (2016) 95(38):e4893. doi: 10.1097/md.0000000000004893
9. Hong JY, Ryu KJ, Lee JY, Park C, Ko YH, Kim WS, et al. Serum level of CXCL10 is associated with inflammatory prognostic biomarkers in patients with diffuse large b-cell lymphoma. Hematological Oncol (2017) 35(4):480–6. doi: 10.1002/hon.2374
10. Wang S, Ma Y, Sun L, Shi Y, Jiang S, Yu K, et al. Prognostic significance of pretreatment Neutrophil/Lymphocyte ratio and Platelet/Lymphocyte ratio in patients with diffuse Large b-cell lymphoma. BioMed Res Int (2018) 2018:9651254. doi: 10.1155/2018/9651254
11. Buzby GP, Knox LS, Crosby LO, Eisenberg JM, Haakenson CM, McNeal GE, et al. Study protocol: A randomized clinical trial of total parenteral nutrition in malnourished surgical patients. Am J Clin Nutr (1988) 47(2 Suppl):366–81. doi: 10.1093/ajcn/47.2.366
12. Ito Y, Abe A, Hayashi H, Momokita M, Furuta H. Prognostic impact of preoperative geriatric nutritional risk index in oral squamous cell carcinoma. Oral Dis (2022). doi: 10.1111/odi.14255
13. Pan Y, Zhong X, Liu J. The prognostic significance of geriatric nutritional risk index in elderly patients with bladder cancer after radical cystectomy. Asian J Surg (2022). doi: 10.1016/j.asjsur.2022.11.082
14. Kanemasa Y, Shimoyama T, Sasaki Y, Hishima T, Omuro Y. Geriatric nutritional risk index as a prognostic factor in patients with diffuse large b cell lymphoma. Ann Hematol (2018) 97(6):999–1007. doi: 10.1007/s00277-018-3273-1
15. Li Z, Guo Q, Wei J, Jin J, Wang J. Geriatric nutritional risk index is not an independent predictor in patients with diffuse large b-cell lymphoma. Cancer Biomarkers (2018) 21(4):813–20. doi: 10.3233/cbm-170754
16. Matsukawa T, Suto K, Kanaya M, Izumiyama K, Minauchi K, Yoshida S, et al. Validation and comparison of prognostic values of GNRI, PNI, and CONUT in newly diagnosed diffuse large b cell lymphoma. Ann Hematol (2020) 99(12):2859–68. doi: 10.1007/s00277-020-04262-5
17. Chuang TM, Liu YC, Hsiao HH, Wang HC, Du JS, Yeh TJ, et al. Low geriatric nutritional risk index is associated with poorer prognosis in elderly diffuse Large b-cell lymphoma patients unfit for intensive anthracycline-containing therapy: A real-world study. Nutrients (2021) 13(9):3243. doi: 10.3390/nu13093243
18. Lee S, Fujita K, Morishita T, Negoro E, Oiwa K, Tsukasaki H, et al. Prognostic utility of a geriatric nutritional risk index in combination with a comorbidity index in elderly patients with diffuse large b cell lymphoma. Br J Haematol (2021) 192(1):100–9. doi: 10.1111/bjh.16743
19. Yan D, Shen Z, Zhang S, Hu L, Sun Q, Xu K, et al. Prognostic values of geriatric nutritional risk index (GNRI) and prognostic nutritional index (PNI) in elderly patients with diffuse Large b-cell lymphoma. J Cancer (2021) 12(23):7010–7. doi: 10.7150/jca.62340
20. Atas U, Sozel H, Iltar U, Yucel OK, Salim O, Undar L. The prognostic impact of pretreatment geriatric nutritional risk index in patients with diffuse Large b-cell lymphoma. Nutr Cancer (2022) 75(2):591–8. doi: 10.1080/01635581.2022.2142248
21. Moher D, Liberati A, Tetzlaff J, Altman DG, Grp P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
22. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
23. Riveros C, Chalfant V, Bazargani S, Bandyk M, Balaji KC. The geriatric nutritional risk index predicts complications after nephrectomy for renal cancer. Int Braz J urol (2023) 49(1):97–109. doi: 10.1590/s1677-5538.Ibju.2022.0380
24. Grinstead C, George T, Han B, Yoon SL. Associations of overall survival with geriatric nutritional risk index in patients with advanced pancreatic cancer. Nutrients (2022) 14(18):3800. doi: 10.3390/nu14183800
25. Artigas A, Wernerman J, Arroyo V, Vincent JL, Levy M. Role of albumin in diseases associated with severe systemic inflammation: Pathophysiologic and clinical evidence in sepsis and in decompensated cirrhosis. J Crit Care (2016) 33:62–70. doi: 10.1016/j.jcrc.2015.12.019
26. Duran AO, Inanc M, Karaca H, Dogan I, Berk V, Bozkurt O, et al. Albumin-globulin ratio for prediction of long-term mortality in lung adenocarcinoma patients. Asian Pacific J Cancer Prev (2014) 15(15):6449–53. doi: 10.7314/apjcp.2014.15.15.6449
27. He J, Pan H, Liang W, Xiao D, Chen X, Guo M, et al. Prognostic effect of albumin-to-Globulin ratio in patients with solid tumors: A systematic review and meta-analysis. J Cancer (2017) 8(19):4002–10. doi: 10.7150/jca.21141
28. Collins N. Protein-energy malnutrition and involuntary weight loss: Nutritional and pharmacological strategies to enhance wound healing. Expert Opin pharmacotherapy (2003) 4(7):1121–40. doi: 10.1517/14656566.4.7.1121
29. Wang Z, Luo S, Zhao X. The prognostic impact of body mass index in patients with diffuse Large b-cell lymphoma: A meta-analysis. Nutr Cancer (2021) 73(11-12):2336–46. doi: 10.1080/01635581.2020.1823437
30. Duconseil P, Garnier J, Weets V, Ewald J, Marchese U, Gilabert M, et al. Effect of clinical status on survival in patients with borderline or locally advanced pancreatic adenocarcinoma. World J Surg Oncol (2019) 17(1):95. doi: 10.1186/s12957-019-1637-1
31. Hao X, Wei Y, Wei X, Zhou L, Wei Q, Zhang Y, et al. Glasgow Prognostic score is superior to other inflammation-based scores in predicting survival of diffuse large b-cell lymphoma. Oncotarget (2017) 8(44):76740–8. doi: 10.18632/oncotarget.20832
32. Mu S, Ai L, Fan F, Qin Y, Sun C, Hu Y. Prognostic role of neutrophil-to-lymphocyte ratio in diffuse large b cell lymphoma patients: an updated dose-response meta-analysis. Cancer Cell Int (2018) 18:119. doi: 10.1186/s12935-018-0609-9
33. Chen Y, Zhang Z, Fang Q, Jian H. Prognostic impact of platelet-to-lymphocyte ratio on diffuse large b-cell lymphoma: a meta-analysis. Cancer Cell Int (2019) 19:245. doi: 10.1186/s12935-019-0962-3
34. Zhang Q, Zhang L, Jin Q, He Y, Wu M, Peng H, et al. The prognostic value of the GNRI in patients with stomach cancer undergoing surgery. J Pers Med (2023) 13(1):155. doi: 10.3390/jpm13010155
35. Xu J, Sun Y, Gong D, Fan Y. Predictive value of geriatric nutritional risk index in patients with colorectal cancer: A meta-analysis. Nutr Cancer (2023) 75(1):24–32. doi: 10.1080/01635581.2022.2115521
36. Yu J, Zhang W, Wang C, Hu Y. The prognostic value of pretreatment geriatric nutritional risk index in esophageal cancer: A meta-analysis. Nutr Cancer (2022) 74(9):3202–10. doi: 10.1080/01635581.2022.2069273
37. Yang M, Liu Z, Li G, Li B, Li C, Xiao L, et al. Geriatric nutritional risk index as a prognostic factor of patients with non-small cell lung cancer: A meta-analysis. Horm Metab Res (2022) 54(9):604–12. doi: 10.1055/a-1903-1943
38. Wu Q, Ye F. Prognostic impact of geriatric nutritional risk index on patients with urological cancers: A meta-analysis. Front Oncol (2022) 12:1077792. doi: 10.3389/fonc.2022.1077792
39. Zhou J, Fang P, Li X, Luan S, Xiao X, Gu Y, et al. Prognostic value of geriatric nutritional risk index in esophageal carcinoma: A systematic review and meta-analysis. Front Nutr (2022) 9:831283. doi: 10.3389/fnut.2022.831283
40. Yuan F, Yuan Q, Hu J, An J. Prognostic role of pretreatment geriatric nutritional risk index in colorectal cancer patients: A meta-analysis. Nutr Cancer (2023) 75(1):276–85. doi: 10.1080/01635581.2022.2109692
Keywords: geriatric nutritional risk index, meta-analysis, diffuse large B-cell lymphoma, prognosis, clinical practice
Citation: Cao D and Zhang Z (2023) Prognostic and clinicopathological role of geriatric nutritional risk index in patients with diffuse large B-cell lymphoma: A meta-analysis. Front. Oncol. 13:1169749. doi: 10.3389/fonc.2023.1169749
Received: 20 February 2023; Accepted: 20 March 2023;
Published: 30 March 2023.
Edited by:
Niklas Gebauer, University Medical Center Schleswig-Holstein, GermanyReviewed by:
Hanno Maximilian Witte, Bundeswehrkrankenhaus, GermanyPanpan Liu, Sun Yat-sen University Cancer Center (SYSUCC), China
Copyright © 2023 Cao and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zongxin Zhang, emhvbmd4aW4xMDA2QDEyNi5jb20=