
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 03 May 2023
Sec. Cancer Genetics
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1161048
This article is part of the Research TopicNew Therapeutic Approaches in Microsatellite Stable Colorectal Cancer Patients.View all 7 articles
 Annalice Gandini1
Annalice Gandini1 Silvia Puglisi1
Silvia Puglisi1 Chiara Pirrone1
Chiara Pirrone1 Valentino Martelli1
Valentino Martelli1 Fabio Catalano1
Fabio Catalano1 Simone Nardin1
Simone Nardin1 Andreas Seeber2
Andreas Seeber2 Alberto Puccini1,3†Stefania Sciallero1†*
Alberto Puccini1,3†Stefania Sciallero1†*Colorectal cancer (CRC) is the third leading cause of cancer-related deaths worldwide, despite several advances has been achieved in last decades. Few prognostic and predictive biomarkers guide therapeutic choice in metastatic CRC (mCRC), among which DNA mismatch repair deficiency and/or microsatellite instability (dMMR/MSI) holds a crucial role. Tumors characterized by dMMR/MSI benefit from immune checkpoint inhibitors. However, most of the mCRC patients (around 95%) are microsatellite stable (MSS), thereby intrinsically resistant to immunotherapy. This represents a clear unmet need for more effective treatments in this population of patients. In this review, we aim to analyze immune-resistance mechanisms and therapeutic strategies to overcome them, such as combinations of immunotherapy and chemotherapy, radiotherapy or target therapies specifically in MSS mCRC. We also explored both available and potential biomarkers that may better select MSS mCRC patients for immunotherapy. Lastly, we provide a brief overview on future perspectives in this field, such as the gut microbiome and its potential role as immunomodulator.
Colorectal cancer (CRC) is the third leading cause of cancer-related deaths in men and in women, and its global incidence is continuously increasing (1). During the last two decades, a tremendous improvement in outcome has been achieved in metastatic CRC (mCRC), mainly due to the introduction of novel drugs and biomarker-driven patient selection.
However, to date, only a few biomarkers have sufficient actionable and clinical implications to guide treatment choice, such as RAS and BRAF mutations and DNA mismatch repair deficiency and/or microsatellite instability (dMMR/MSI). Indeed, CRC patients harboring dMMR/MSI tumor showed outstanding and practice-changing results with immune checkpoints inhibitors, doubling progression free survival (PFS) and maintaining durable response (2). Unfortunately, only 15% of early stages CRC and 5% of mCRC are dMMR/MSI (3), thus the vast majority of mCRC patients do not benefit from this treatment approach. Because of this, scientific community is focusing on better understanding mechanisms behind the intrinsic resistance to immunotherapy in order to overcome them. This field is a big unmet need in CRC, and many trials have been carried on: in this review we would like to walk through the available data on immunotherapy, alone or in combination, in pMMR/MSS metastatic CRCs to better understand how far along we are and what the main gaps are.
CRC carcinogenesis and immunity are a complex system that derives from interactions on different levels. The majority (85%) of CRC presents a chromosomal instability and are typically MSS (4), while 15% have genetic instability, resulting in high MSI status. Finally, epigenetic is driven by hypermethylation or hypomethylation and modulates the expression of certain genes without any genetic alterations (5). About microsatellite instability, it is related to defects in the mismatch repair system which lead to mutations across the genome and, consequently, cause the release of many mutation-associated neoantigens (MANA) that enhance the immunity response: this is why dMMR/MSI tumors are highly responsive to immunotherapeutic agents (6). Indeed, tumor mutational burden (TMB) is directly proportional to the production of neoantigens and, consequently, can induce a pro-inflammatory tumor microenvironment (TME) (5, 7). Since CRCs with a proficient mismatch-repair pathway do not accumulate mutations, TMB is low and TME is not pro-inflammatory, defining them as “cold” tumors. Due to that, several studies were conducted to find a way to enhance the production of neoantigens, although therapeutic implications of this approach are still under investigation (7).
In addition to the primarily low involvement of the immune system, immunity cells may be selected to limit their efficiency according to the so called “immune exclusion” phenomenon (8). Indeed, preclinical experiments demonstrated different T-cell populations inside deficient (dMMR) and proficient-MMR (pMMR) tumors, in terms of both cell quantity and heterogeneity (9): it seems that in pMMR/MSS tumors immunity cells react against the tumor, but their presence is localized all around it, without reaching the core; thus compromising efficacy of immunotherapy. In this regard, preclinical models investigated the role of transforming growth factor-beta (TGF-b), which prevents T cell tumor infiltration through induction of fibrosis (10). Moreover, the up-regulation of oncogenic pathways, like WNT/beta-catenin signaling pathway and MAP-kinase pathway, has shown to contribute to immune-exclusion trough silencing the activation of T-cells (11). In particular, about 60% of MSS CRCs have an up-regulation of the MAP-kinase pathway, which leads to a reduction of Major Histocompatibility Complex (MHC) class I molecules’ expression and a decrease of the number of CD8-positive T cells in the tumor core (12). Also, some immunosuppressive patterns seem to be involved in poor responses to immunotherapy. PIK3CA mutations, that can be found in about 13% of CRCs regardless the MMR status (13) and can be secondary to a loss of Phosphatase and tensin homolog (PTEN) (14), are associated with Programmed Death-Ligand 1 (PDL-1) expression and immunosuppressive effect.
In addition, both intensity and quality of the TME can influence response to immunotherapy (15): a high prevalence of FOXP3 positive regulatory T cells (Treg) or myeloid derived suppressor cells (MDSC) is associated with poor prognosis in several neoplasms, although their role in CRCs is more complex and under further investigation (6, 16).
Furthermore, it is important to underline the role of the Vascular Endothelial Growth Factor (VEGF), that can induce endothelial cell proliferation, thus promoting neo-angiogenesis in the tumor mass (17). Along with the mechanisms whereby the tumor cells evade immunity system, the adaptation to a hypoxic environment represents a powerful stimulus for up-regulating genes involved in proliferation, glycolysis and angiogenesis, often related to aggressive and metastatic tumor behavior (18). VEGF is also a mediator of immunosuppression by promoting the accumulation of MDSCs and Tregs (19) thus enhancing its potential involvement in immune exclusion.
Such complex mechanisms contribute to create a “cold” tumor environment and could represent potential targets for novel therapeutic strategies to overcome resistance to immunotherapy, even if specific targets and biomarkers need further investigation.
To overcome resistance and enhance an effective immune response against tumor cells, several trials are investigating immunotherapy-based combination strategies to synergistically stimulate the tumor microenvironment in order to promote immune cell recruitment in MSS mCRC (20).
Based on the rational that chemotherapy may interrupt mechanisms of immune tolerance and, consequently, enhance cancer cells’ immunogenicity (21), several trials were designed to study the association of chemotherapy and immunotherapy (Table 1).
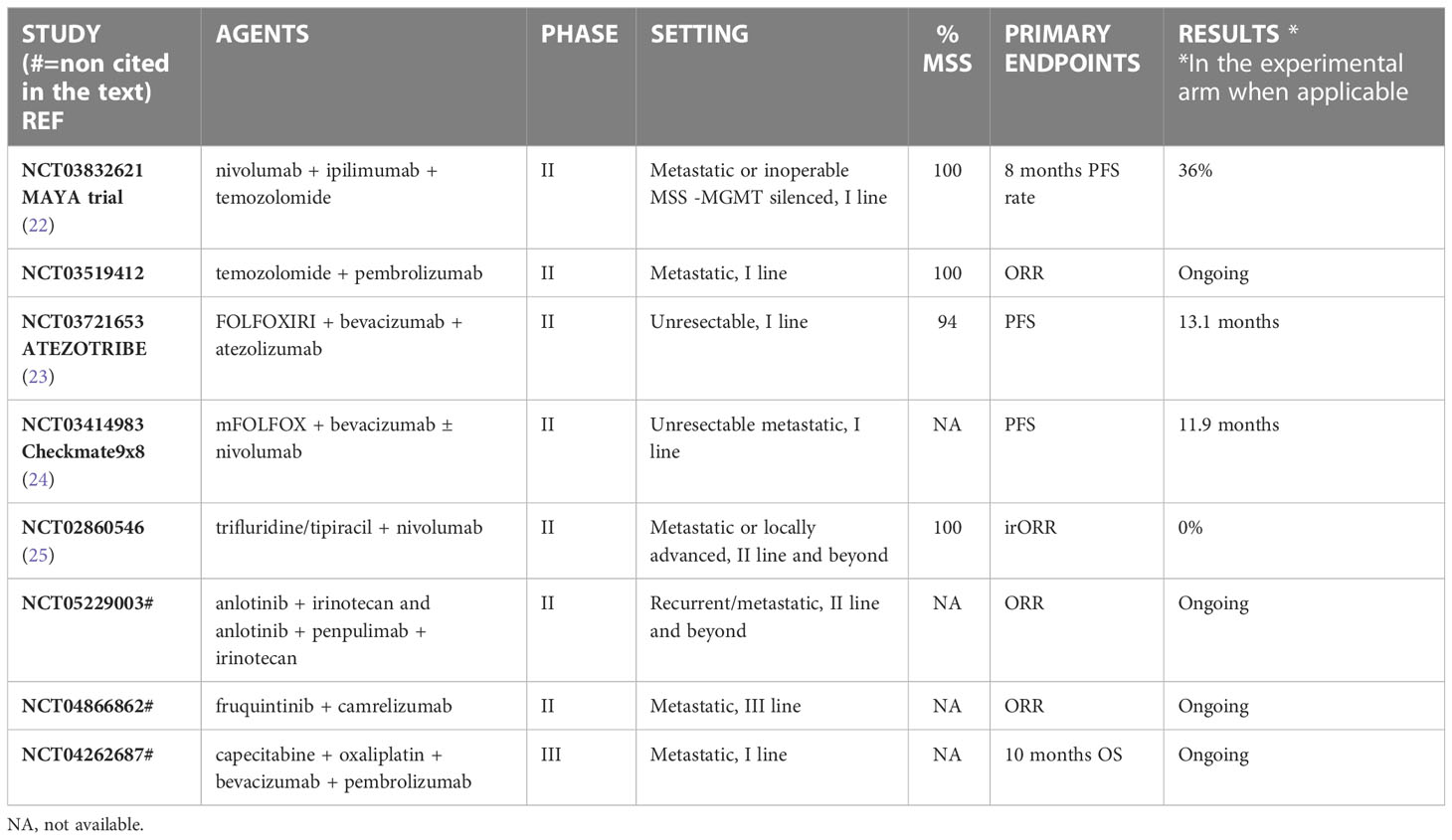
Table 1 Immunotherapy plus Chemotherapy.
In preclinical models, acquired resistance to the clinical agent temozolomide (TMZ) could inactivate the MMR system and, therefore, increase the mutational burden and trigger immune surveillance (26). Based on this result, the MAYA trial evaluated the efficacy and safety of an immune-sensitizing strategy through an induction therapy with temozolomide followed by a combination of low-dose ipilimumab and nivolumab in patients with MSS and MGMT-silenced mCRCs. Median progression free survival (mPFS) was 7 months and median overall survival (mOS) 18.4 months, with objective response rate (ORR) of 45%. These data provide a “proof of concept” that induction therapy with temozolomide followed by immunotherapy could induce sustained clinical benefit with a good tolerability (22). The applicability in the clinical practice needs further investigations since the selection of patients could represent an important limit: among the 716 patients prescreened, only 135 started the first part of the treatment and, among these, only 24% of patients could start the second part. Similar results are expected by the ARETHUSA trial, which selects patients based on MMR status, MGMT expression for the induction with TMZ and, at the end, TMB for treatment with pembrolizumab: this trial is still recruiting and data are immature [NCT03519412].
In first line, positive results came from the ATEZOTRIBE trial, where patients with previously untreated pMMR/MSS mCRC were randomized to receive mFOLFOXIRI (5fluoro-uracil, leucovorin, oxaliplatin and irinotecan) plus bevacizumab with or without atezolizumab. After 19.9 months of follow-up, median PFS was 13.1 months in the atezolizumab group and 11.5 months in the control group (hazard ratio HR=0·69 p=0·012), suggesting that this strategy could give a benefit in this setting, although the benefit was probably restricted to the subgroup of MSI mCRC patients included in the trial (23).
At the American Society of Clinical Oncology (ASCO) Gastrointestinal Cancers Symposium in 2022, Lenz et al. reported the results of Checkmate 9x8, a phase II study which assessed the role of nivolumab added to the standard first line therapy (mFOLFOX plus bevacizumab) in mCRC, regardless of the MMR status. Primary endpoint was PFS and in both arms mPFS was 11.9 months with HR of 0.81, which did not meet the prespecified threshold for statistical significance. However, nivolumab plus standard of care (SOC) showed higher PFS rates at 15 months (45% VS 21.5%) with no difference between MSS and MSI patients, a higher objective response rate (60% vs 46%), and more durable responses (12.9 months vs 9.3 months), with acceptable safety (24).
Moving to the maintenance setting, unsatisfactory results came from the umbrella trial MODUL in which patients were treated with fluoropyrimidine plus bevacizumab alone or with an experimental biomarker-driven treatment based on histopathological characteristics (5FU/LV plus cetuximab and vemurafenib in BRAFV600E mutated, capecitabine plus trastuzumab and pertuzumab in HER2 positive, fluoropyrimidine plus bevacizumab and atezolizumab or cobimetinib plus atezolizumab in wild-type patients). At the moment, only results on cohort 2 have been published: endpoints of efficacy were not reached in the experimental arm with atezolizumab in MSS mCRC (27, 28).
Several combination trials were performed also in further lines.
Patel at al., in a phase II trial investigated the combination of trifluridine–tipiracil plus nivolumab in heavily pretreated MSS mCRC. The trial was negative with no clinical benefit: none of the patient enrolled achieved objective response and the trial was interrupted (25).
To date, combining immunotherapy and chemotherapy in MSS mCRC patients did not obtain clinically meaningful results thus this strategy is not currently available in clinical practice.
In preclinical models, the combination of immunotherapy and tyrosine kinase inhibitors (TKI) in pMMR/MSS CRC cells seems to increase the production of neoantigens and, consequently, to induce immune-mediated cell death (29). Therefore, Fukuoka et al. developed the REGONIVO trial [EPOC1603], a phase I trial assessing efficacy of nivolumab plus regorafenib in CRC and gastric cancer. Only one out of the 25 CRC patients was dMMR/MSI. In the results presented, the cohort of patients with CRC showed a median PFS of 7.8 months with one-year PFS rate of 41.7% and one-year OS rate of 68%. Interestingly, patients with lung metastases had higher objective response rates when compared with those with liver metastases (30).
The phase II evaluating the combination regorafenib and nivolumab has just been published (31) and confirms the lack of effect of this combination in patients with liver metastases (mPFS 11.9 months in patients without liver involvement, versus 1.8 months in those with hepatic disease).
Kim et al. evaluated the same combination in a phase I/Ib trial and reached a mPFS of 4.3 months and mOS of 11.1 months (32). Similar results were found with regorafenib in association with pembrolizumab that obtained a median PFS of 2.0 (1.8 -3.5) months and median OS of 10.9 (5.3-not reached) months (33) in heavily pre-treated mCRC patients.
The association of regorafenib with avelumab was evaluated in the single-arm phase II trial REGOMUNE, but it did not show objective response rates, with stable disease as best response in 53.5% of the 48 patients enrolled. Median PFS and median OS were 3.6 and 10.8 months, respectively (34).
Lenvatinib in combination with immunotherapy has demonstrated great efficacy in other malignancies, such as endometrial cancer. LEAP-005 is a phase 2 study assessing ORR and safety of the combination in previously treated solid tumors, including pMMR/MSS CRC. In particular, this subgroup of patients was treated in third line and reached an objective response rate of 22% and a mPFS of 2.3 months, with manageable toxicities (35). The phase III randomized trial is ongoing to investigate this combination in larger cohorts [LEAP-017 NCT04776148].
Slightly better results were obtained from the CAMILLA trial, were pMMR mCRC patients who progressed after 2 or more lines of therapy were treated with durvalumab plus cabozantinib. The trial followed preclinical results in which cabozantinib with anti-PD1 showed to slow tumor’s growth and increase expression of the CD4+ T cell ligand HLA-DR on the tumor cells themselves (36). Despite the different immunotherapeutic agent used, CAMILLA’s efficacy analyses revealed an ORR of almost 30% and a disease control rate of 86.2% (25/29), with a median PFS of 4.4 months and a median OS of 9.1 months (37).
The BEACON trial in 2019 (38) set a new therapeutic paradigm for BRAFV600E mutated mCRC and preclinical data demonstrated that the combination of BRAF inhibitor plus epidermal growth factor receptor (EGFR) inhibitor could induce a transient MSI phenotype. On this background, Van Morris and Colleagues designed a phase I/II trial with the triplet encorafenib, cetuximab and nivolumab in BRAFV600E pretreated MSS mCRC. The results presented at ASCO Gastrointestinal Cancers Symposium in 2022 are promising, reaching an ORR of 50%, a median PFS of 7.4 months (vs 4.2 in the BEACON) and a median OS of 15.1 months (vs 9.3 months in the BEACON trial) (39). The randomized phase II trial [NCT05308446] is actually ongoing to confirm these preliminary results.
Several preclinical models and different studies have suggested that MEK inhibition can lead to up-regulation of MHC I and increase the infiltration of CD8+ into the tumors (40, 41).
Therefore, different trials investigating the synergic role of immunotherapy plus MEK inhibitors were developed.
In 2016 Bendell et al. presented the results of a phase Ib trial which assessed the clinical activity of atezolizumab plus cobimetinib in 24 patients with pretreated mCRC. The ORR was 17% and, among responders, three patients with major response were MSS (42). The same combination has been evaluated by Hellman and Colleagues in a cohort of 84 CCRs of which 74% were MSS. They reported a response rate in seven patients (8% of the cohort), of whom six patients had microsatellite stable status (43). IMblaze370 is a multicenter, open-label, phase 3, randomized, controlled trial, that was opened in 73 academic medical centers among 11 countries, whose results were published in 2019 on Lancet Oncology. The 363 patients with pre-treated unresectable or metastatic CRC, mostly with microsatellite stability, were randomized to receive atezolizumab alone or in combination with cobimetinib or SOC (regorafenib). Unfortunately, this trial did not met its primary endpoint of improving overall survival (OS) in the experimental arm compared to SOC, registering a mOS of 8.9 months in the combination arm, 2.1 months in the atezolizumab alone arm and 8.5 months in the regorafenib arm: these results demonstrated lack of benefit using immunotherapy, with or without the combination of a MEK inhibitor, in patients with low levels of inflammation (44). Despite the unsatisfactory results, few more trials are ongoing evaluating cobimetinib in association with nivolumab and ipilimumab [NCT02060188] or atezolizumab and bevacizumab [NCT02876224] in pretreated MSS mCRC.
To date, most of the clinical trials investigating the combination of immunotherapy and TKI in MSS mCRC failed to show clinically significant results, that may be partly explained with poor selection of heavily refractory mCRC MSS patients. In Table 2 are summarized the main trials available and ongoing. These negative results highlight the strong need for a better understanding of underlying mechanisms of immune-resistance and synergistic effects between different drugs.
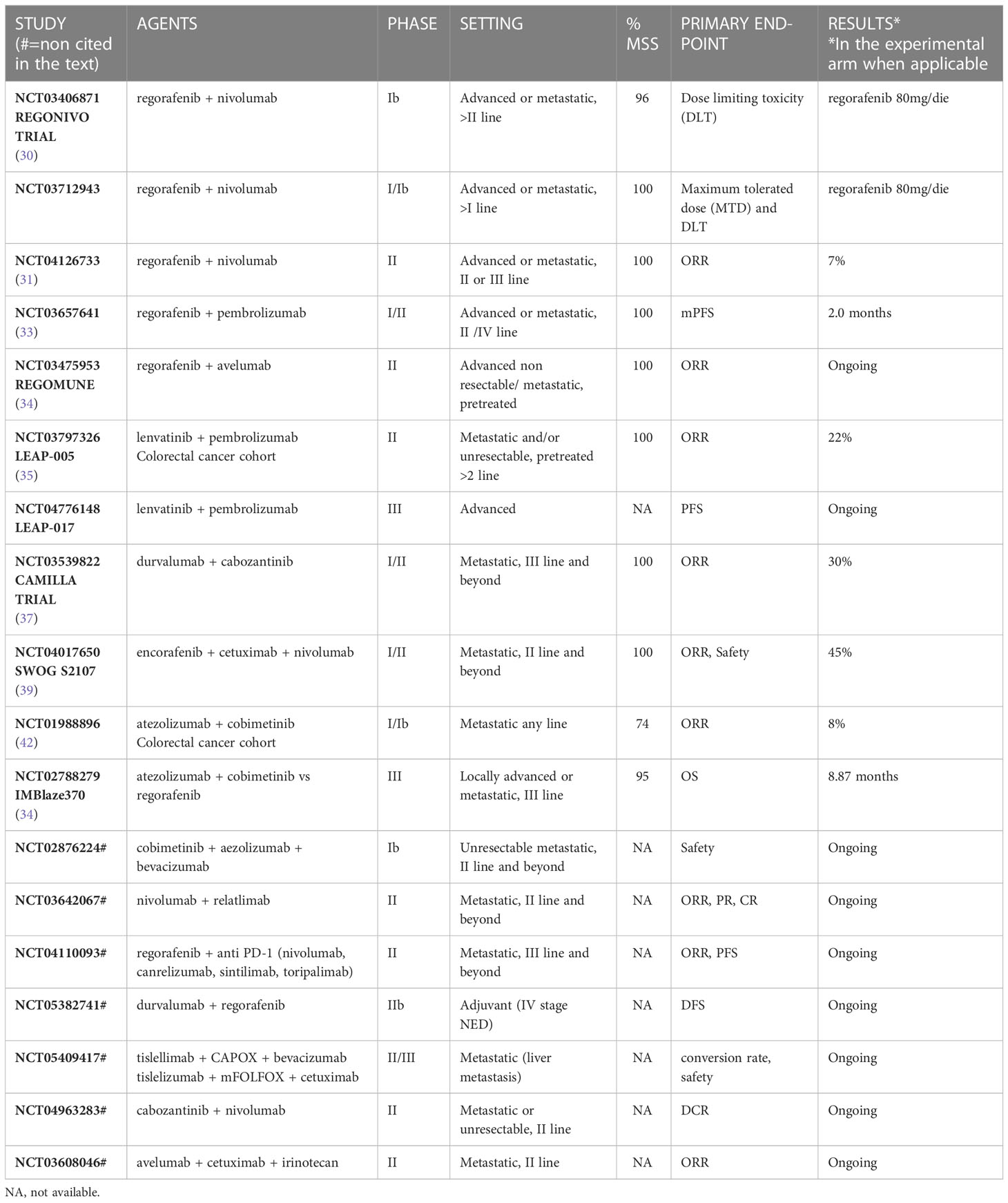
Table 2 Immunotherapy plus target therapy and Tyrosine kinase inhibitors.
The anti-angiogenic bevacizumab seems to potentiate dendritic cells’ functions, to facilitate CD8+ lymphocytes infiltration into tumor and to decrease Tregs functions, important studies such as the MODUL trial, cited above, and the BACCI trial (capecitabine in association with bevacizumab and atezolizumab in refractory mCRC) (45) were then developed, but both reported negative results in all the subgroups. Other studies which aim to assess the role of bevacizumab in association with immunotherapy [NCT03396926, NCT02848443] are reported in Table 3, but results are still unknown. Moreover, in a humanized mice model, the association of cobimetinib, bevacizumab and pembrolizumab was not able to act on tumor growth. However, an immune modulation in TILs was observed, suggesting that the combination could potentially enhance immune susceptibility in MSS CRC (36). The use of dual therapy with VEGF inhibitors and immunotherapy has been widely evaluated in many different malignancies, although no thrilling results were obtained in CRCs (24, 45, 49, 50).
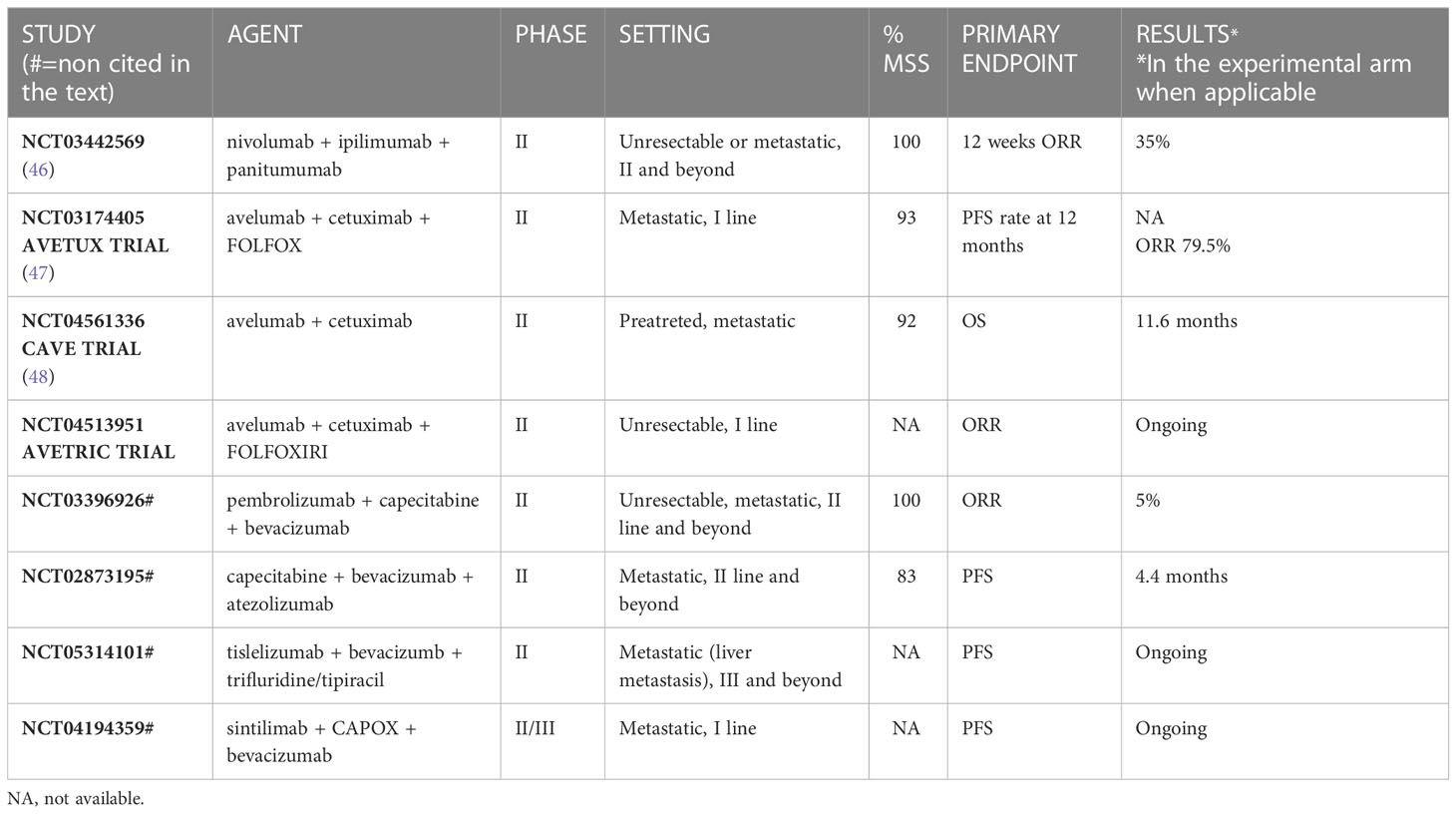
Table 3 Immunotherapy plus antiangiogenetic.
Preclinical data showed that anti-EGFR therapy can contribute to activate a tumor-specific adaptive immune response and immunogenic apoptosis, often associated with an increased expression of CTLA-4 and PD-L1, during the development of treatment resistance (51). Therefore, several attempts have been made to evaluate association of anti-EGFR and immunotherapy (Table 3).
Preliminary results of a trial evaluating if the addition of ipilimumab and nivolumab to panitumumab would increase response rate in patients with RAS/BRAF wild-type MSS mCRC were published last year. Among 49 enrolled patients, the 12-week response rate was 35% with median PFS of 5.7 months, meeting the prespecified primary endpoint (46).
Afterwards, Stein and colleagues developed the AVETUX trial, a single arm trial that combined in first line mFOLFOX6 and avelumab with cetuximab in RAS/BRAF wild-type mCRC patients. The primary endpoint of 12 months PFS rate was not reached, but high tumor responses were observed, especially in terms of depth of response (47).
On the same basis, Martinelli et al. reported results from the randomized phase II CAVE trial to evaluate the efficacy of rechallenge with cetuximab in association with avelumab in the third-line in RAS wild-type mCRC with no selection regarding microsatellite status: the trial showed a promising median OS of 11.6 months (48), suggesting potential synergism between immune checkpoint inhibitors and anti-EGFR drugs.
Moreover, cetuximab and avelumab were also evaluated in first line in association with mFOLFOXIRI in the AVETRIC trial: it has just closed the enrolment and results are not available yet [NCT04513951].
Combined blockade with immunotherapy strategies has been explored to overcome immune resistance (Table 4).
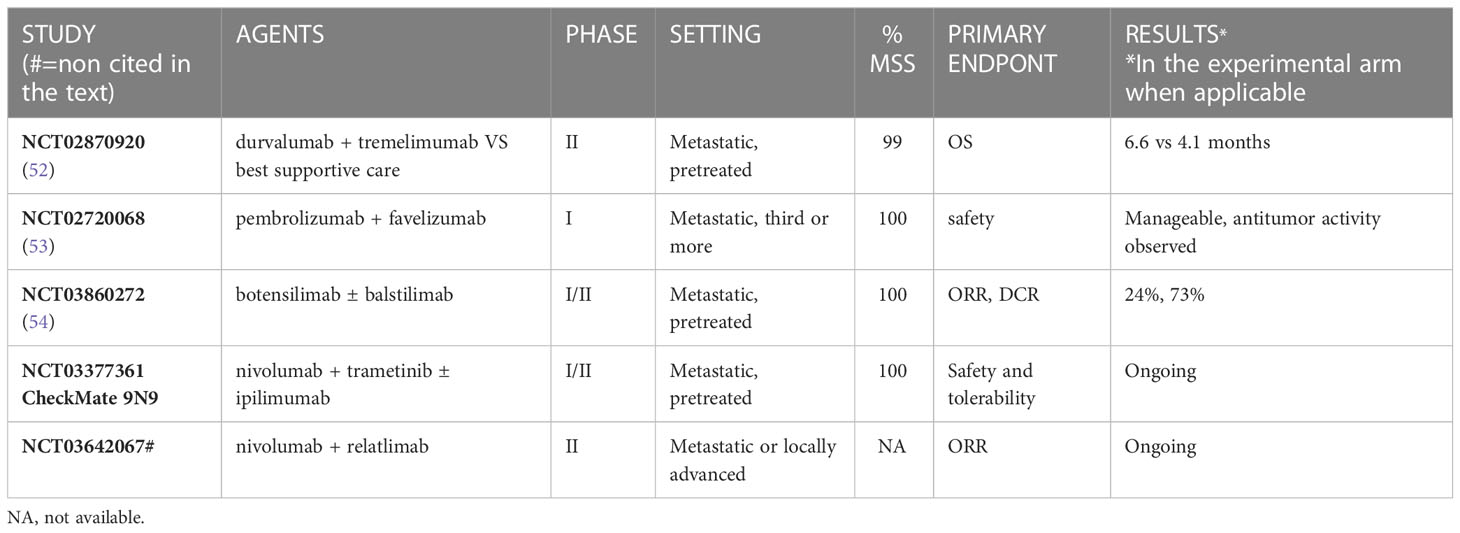
Table 4 Combination of immune checkpoint inhibitors.
The NCT02870920 study evaluated the combination of durvalumab (anti PDL1) and tremelimumab (anti- Cytotoxic T-Lymphocyte Antigen 4 CTLA-4) versus best supportive care for refractory mCRC. Disease control rate (DCR) was of 22.6% and 6.6%, median PFS was not prolonged (1.8 months vs. 1.9 months), but median OS was longer in the experimental group (6.6 months vs 4.1 months). It is important to notice that patients with a TMB > 28 MTs/MB benefited more from dual immunotherapy, whereas high TMB in the best supportive care group was associated with a poor prognosis, enhancing the relative benefit (52).
NCT03860272 is the first trial of botensilimab, a novel innate/adaptive immune activator against CTLA-4, in association with the anti PD1 balstilimab in patients with advanced cancer. Patients were heavily pretreated, including 14/34 treated with prior immunotherapy, and received botensilimab at 1 or 2 mg/kg every 6 weeks plus balstilimab 3 mg/kg every 2 weeks. The ORR was 24% (10/41), with a DCR of 73% (30/41) (54).
The combination of nivolumab and trametinib with or without ipilimumab in previously treated cancer of the colon or rectum is being tested in an ongoing phase I/II trial [CheckMate 9N9-NCT03377361].
Interesting results, even if still immature, came from the use of antibodies against the lymphocyte activation gene-3 (LAG3). LAG-3 is a surface molecule expressed by immunity cells that plays a role in the regulation of lymphocytes and dendritic cells’ activity (55). It showed a potential role in cancer treatment in both preclinical and clinical studies, since its inhibition could potentially trigger an inflammatory phenotype (56).
The combination of pembrolizumab and the anti-LAG3 antibody favezelimab in previously treated MSS mCRC patients [NCT02720068], showed a median OS of 8.3 months and a median PFS of 2.1 months in a phase I study. Of 89 patients receiving the combined blockade, 4 patients achieved a partial response and 1 showed a complete response. Median duration of response was 10.6 months (range 5.6–12.7) (53).
Although the association of immune-checkpoint inhibitors blockade has not shown to be as effective as in dMMR/MSI counterpart, novel combinations demonstrated promising activity also in MSS mCRC, particularly among well-selected patients without liver metastases. Thus large phase III trials are ongoing and results are eagerly awaited.
Radiotherapy induces tumor-cell death and increases the expression of MHC class I on cell membrane, improving antigen presentation by dendritic cells with a strong immune activation (57). Some evidence showed, moreover, that it can also induce the so-called “abscopal effect”, a rare phenomenon that consists of tumor regression in a site distant from the field of irradiation due to the activation of immune system against cancer cells. Therefore, it was suggested that combining radiotherapy with immunotherapy could represent a good strategy for enhancing the immune system reaction (58). By now, the combination of RT plus immunotherapy has been studied especially in non-small cell lung cancer (NSCLC) and melanoma, because of their different background in tumor immunogenic biology (59). Unfortunately, in CRC, and especially in MSS CRC, only a few data are available (Table 5). A recent phase 2 trial [NCT03104439] has evaluated the combination of fractioned radiotherapy (8 Gy in three fractions to a single metastatic lesion) with ipilimumab and nivolumab in 40 patients with MSS metastatic colorectal and pancreatic cancer. Disease control rate in the intention to treat population was 25% with ORR of 10%; median PFS was 2.4 months, and median OS 7.1 months. However, 13 out of 40 patients did not receive radiotherapy: among the 27 patients treated with the protocol-defined radiotherapy, responses were higher, with a DCR of 37% and an ORR of 15%. The median duration of disease control was more than 15 months. It is important to notice, though, that half of the patients had grade 3-4 adverse events (60). Segal’s phase II trial failed at its primary endpoint of ORR in non-irradiated lesions but in rare instances a systemic immune augmentation and a regression at these sites was observed, supporting abscopal response with a manageable safety profile (61).
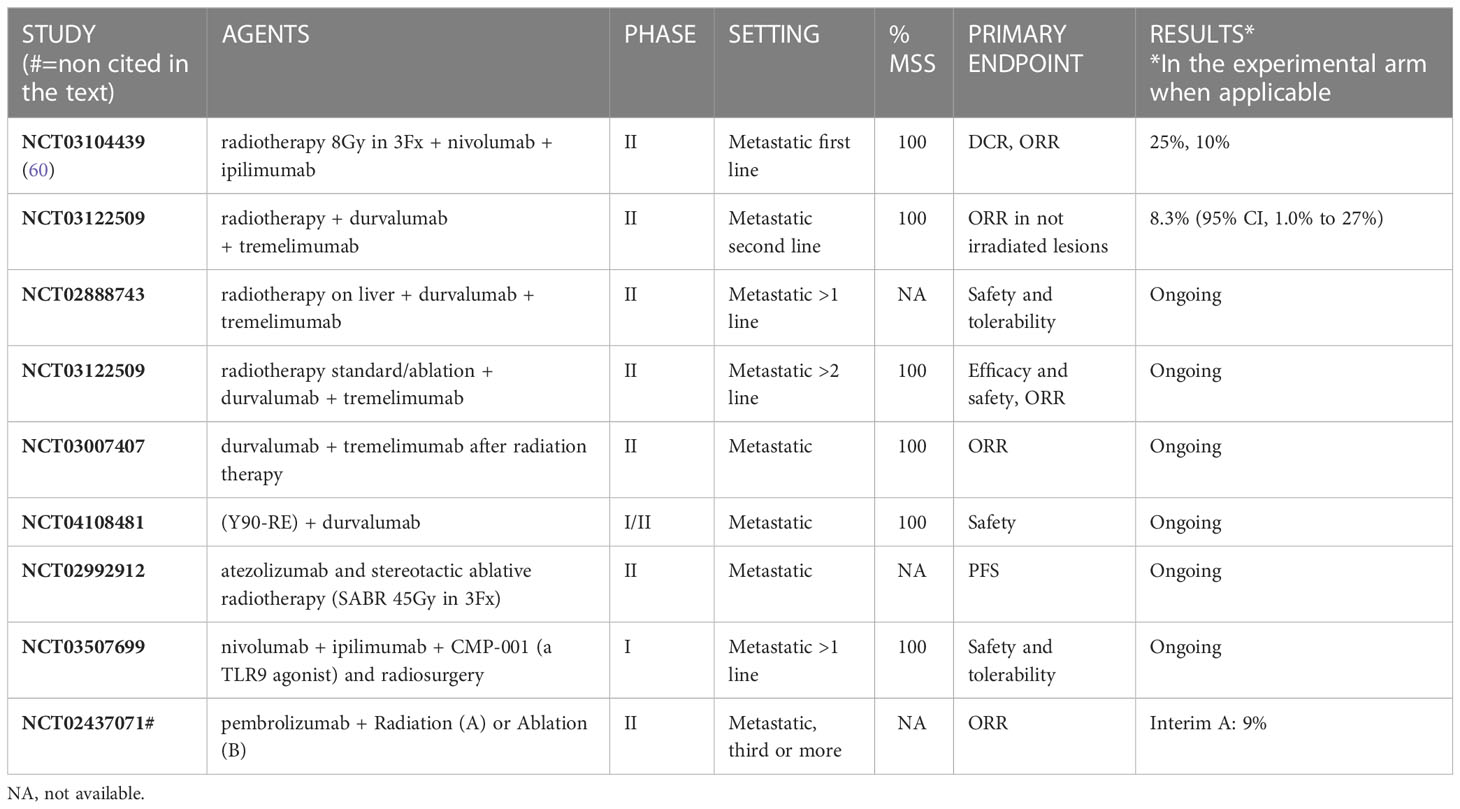
Table 5 Combination of immunotherapy plus radiotherapy.
Moreover, several trials on the combination of durvalumab and tremelimumab plus radiotherapy are ongoing and no data are available. Here we report few examples to underline the interest of the scientific community in this promising field:
-NCT02888743 is a randomized phase II trial designed to investigate the safety of durvalumab and tremelimumab with or without high or low-dose radiation therapy in patients with metastatic colorectal or non-small cell lung cancer.
-NCT03122509 is evaluating the efficacy and safety of durvalumab and tremelimumab plus radiotherapy in metastatic CRC patients who are undergoing to radiotherapy as standard therapy or plus ablation.
-NCT03007407 evaluates the safety and response to the combination of durvalumab plus tremelimumab when given after radiation therapy for patients with MSS mCRC.
-NCT04108481 is a single-centre, open-label, Phase I/II trial that evaluates the feasibility and safety of Yttrium-90 radioembolization (Y90-RE) in combination with durvalumab 750 mg in subjects with liver-predominant MSS mCRC.
About other immune checkpoint inhibitors, the results of a phase II study with a combination of atezolizumab and radiotherapy in pretreated MSS mCRC [NCT02992912] and of a combination study with nivolumab, ipilimumab, CMP-001 (a TLR9 agonist) and radiosurgery (21Gy in 3 fractions) in patients with mCRC and liver metastases [NCT03507699], are still not available.
The majority of efforts in pMMR/MSS mCRCs treated with immune checkpoint inhibitors have been focused on predictive factors of response to such therapies: several biomarkers have been evaluated in the last years, investigating the tumoral micro-environment, the mutational landscape, the immune system, and the clinical characteristics of the patients.
Despite all these attempts, it is not possible to draw clear conclusions in favour of one biomarker or another. In this part of the review, we will summarize the most promising results and the still existing areas of uncertainty.
The PD-1 receptor and its ligand PD-L1 expression are two well-known biomarkers; however the actual prevalence of PD-L1 expression in mCRC is not completely clear. Moreover, the few available data on these are limited to dMMR/MSI CRC, and they did not show strong positive results (62–64).
High TMB levels can be detected in about 3% of MSS mCRC. Therefore, the prevalence of TMB-high could be more significant than expected in the mCRC population (65), implying the necessity of testing it on a large scale (66). However, it is difficult to define when a tumor is TMB-high and when it is low, since several methods of analysis and ways to express the results are available (67). Moreover, the optimal threshold is far from being clearly assessed: Schrock et al. reported a cut-off of 37-41 mut/Mb (68), in the REGONIVO trial the cut-off was 22.5 mut/Mb [REGONIVO JCO], while in CCTG CO.26 trial it was 28 mut/Mb (52). The basket trial TAPUR evaluated the efficacy of already available target agents in metastatic solid tumors showing specific somatic genomic variants (69). For the TMB-high pMMR/MSS mCRC cohort, the a priori cut-off was > 9 mut/Mb, and the patients were allocated to receive different immune checkpoint inhibitors. Overall, 27 patients have been enrolled in the pembrolizumab subgroup: 7 showed benefit from the treatment for six months or more, and two out of the three patients treated for at least one year showed a TMB > 40 mut/Mb. The mPFS was 9.3 weeks, the mOS 51.9 weeks, and the 1-year OS rate 45.6%; moreover, the DCR was 28% and the ORR was 11% (70).
In the nivolumab plus ipilimumab arm, the median TMB was 13, ranging from 9 to 233 mut/Mb. This subgroup showed lower DC rate (10%) and mOS (42.9 weeks) and a higher toxicity. Given these results, the Authors concluded that the regimen should not be further investigated in TMB-high pMMR/MSS mCRC population, preferring to focus on other treatment strategies (71).
Despite these not-so-encouraging results, there still may be a place for high TMB as a predictive biomarker with immune double blockage regimens, as shown in the CCTG CO.26 trial. Here, heavily pre-treated mCRC patients received durvalumab plus tremelimumab versus the best supportive care: the greatest OS benefit was found for the pMMR/MSS mCRC with plasma TMB higher than 28 mut/Mb (HR 0.34; 90% CI, 0.18 – 0.63; P = .004) (52).
According to the Cancer Genome Atlas results, one-quarter of hypermutated CRC presents DNA Polymerase Exonuclease Domain (POLE/POLD1) mutations (72), that are typically linked to a high TMB. In the pMMR/MSS population, POLE mutations have been identified in about 3% of the cases (73).
Wang et al. analysed a data set of different solid tumors treated with immune checkpoint inhibitors: the frequencies of POLE and POLD1 mutations were 2.79% and 1.37%, respectively, with a high prevalence in CRC (circa 7%); in the overall population, 74% of the POLE/POLD1 mutated patients also had a pMMR/MSS phenotype. In this work, mutations of POLE and POLD1 were demonstrated to be positive predictive factors of response to immunotherapy since the OS was 34 months, more than doubled when compared with the non-mutated counterpart (74). This positive result has also been confirmed by the multivariable Cox regression analysis, which showed POLE/POLD1 as an independent biomarker for ICI response.
This higher response rate is probably linked to the high presence of cytotoxic T cells (especially CD8+ lymphocytes) and effector cytokines in the tumor microenvironment (75). Nevertheless, more robust preclinical and clinical evidence is needed to assess the predictive role of POLE/POLD1 mutations in MSS mCRC (76).
Understanding the biology underlying MSS colorectal tumors will lead to improved clinical trial design and to the identification of clinical biomarkers relevant to this population. Because of this, efforts were made in the last years to organize the heterogeneous molecular landscapes of CRC, leading to the Consensus Molecular Subtypes (CMS) classification by the Colorectal Cancer Subtyping Consortium (77). This categorization consists of four different subgroups of tumors: the CMS1 (“immune subtype”, about 14% of all cases) characterized by dMMR/MSI phenotype, hypermutated status, BRAFV600E mutation; the CMS2 (“canonical”, about 37%) with chromosomal instability, MYC, Wnt and EGFR pathway activation; the CMS3 (“metabolic”, 13%), showing epithelial features and mutations in MAPK pathway; the CMS4 (“mesenchymal”, 23%) with constitutively activated VEGFR pathway. The remaining 13% of the patients shows mixed features, defining a transition phenotype.
The CMS1 and CMS4 subgroups are characterized by strong immune infiltration in their microenvironment, defining them as “hot” tumors with intense immune activation. However, the molecular features and cellular subpopulations differ: CMS1 shows an immunoreactive environment, with T-helper 1, CTLA4, and IDO1 overexpression. In contrast, CMS4 shows an immunosuppressive landscape, mainly characterized by M2 macrophages, Th17 cells, and TGF-b overexpression (78).
Above all, TGF-b raised interest in the last years as a potential target of specific drugs. Recently, a phase II trial evaluated the anti-PD-L1 antibody/TGF-b trap bintrafusp alfa combined with radiation therapy of metastatic lesions in CMS4 mCRC: unfortunately, no patients had any benefit in terms of disease response (ORR 0%) or survival (mPFS 1.6 months; mOS 5 months) (79); therefore, further efforts have to be done in this population.
Lenz et al. first evaluated CMS predictive role on a large population in the CHECKMATE 9X8 trial (24), which randomized MSS mCRC patients to receive nivolumab or placebo in combination with first-line FOLFOX plus bevacizumab. The trial was negative; however, in the exploratory analyses, the anti-PD-1 regimen showed a clinical benefit in CMS1 and CMS3 subgroups, where almost one patient out of three was free from progression at 20 months. This finding supports the idea of the possible usefulness of CMS as a predictive biomarker for immune checkpoint inhibitors.
As previously described, the majority of CRCs are characterized by microsatellites stability and so, due to the clinical relevance, several attempts of “immunizing” cold tumors have been made. Unfortunately, it is still unclear what the best strategy might be, and we would like to underline through this review which ones seem to be more promising and deserve to be carried on.
Unfortunately, among all the combination strategies, some of them have shown unacceptable toxicities or absence of response (durvalumab plus tremelimumab) (80).
On the other hand, the association of regorafenib with nivolumab probably leads to the development of a synergic effect that enhances the response and allow to overcome resistance to ICI (30). Despite several limits, such as the absence of synergic effect in presence of liver metastasis, the modest survival benefit and the absence of predictive biomarkers, this treatment could represent a valid therapeutic option for patients affected by CRC without liver metastasis (ORR 22% vs 0%) (81).
In addition, data of the combination of the novel second-generation CTLA4-inhibitor botensilimab plus the PD-1 inhibitor balstilimab give a hint of enhanced efficacy, due to the DCR of 96% in patients without liver metastasis, and no severe toxicity (54).
Finally, the association of pembrolizumab and the anti-LAG3 favezelimab in pretreated MSS mCRC seems promising, and data from the ongoing phase III trial are expected.
Research is also active on developing cancer vaccines, based on cancer-specific neoepitopes bounded by T-cells in order to enhance immunological response (82). In the last few years, different type of vaccines has been developed from cancer cell or vector-based, but with progress on next generation sequencing techniques, nano-vaccines and neoantigen vaccines are lastly prevailing (83). Nowadays they are considered a possible strategy to overcome the resistance of MSS mCRC to immunotherapy. Several trials are ongoing (Table 6) but data are still immature.
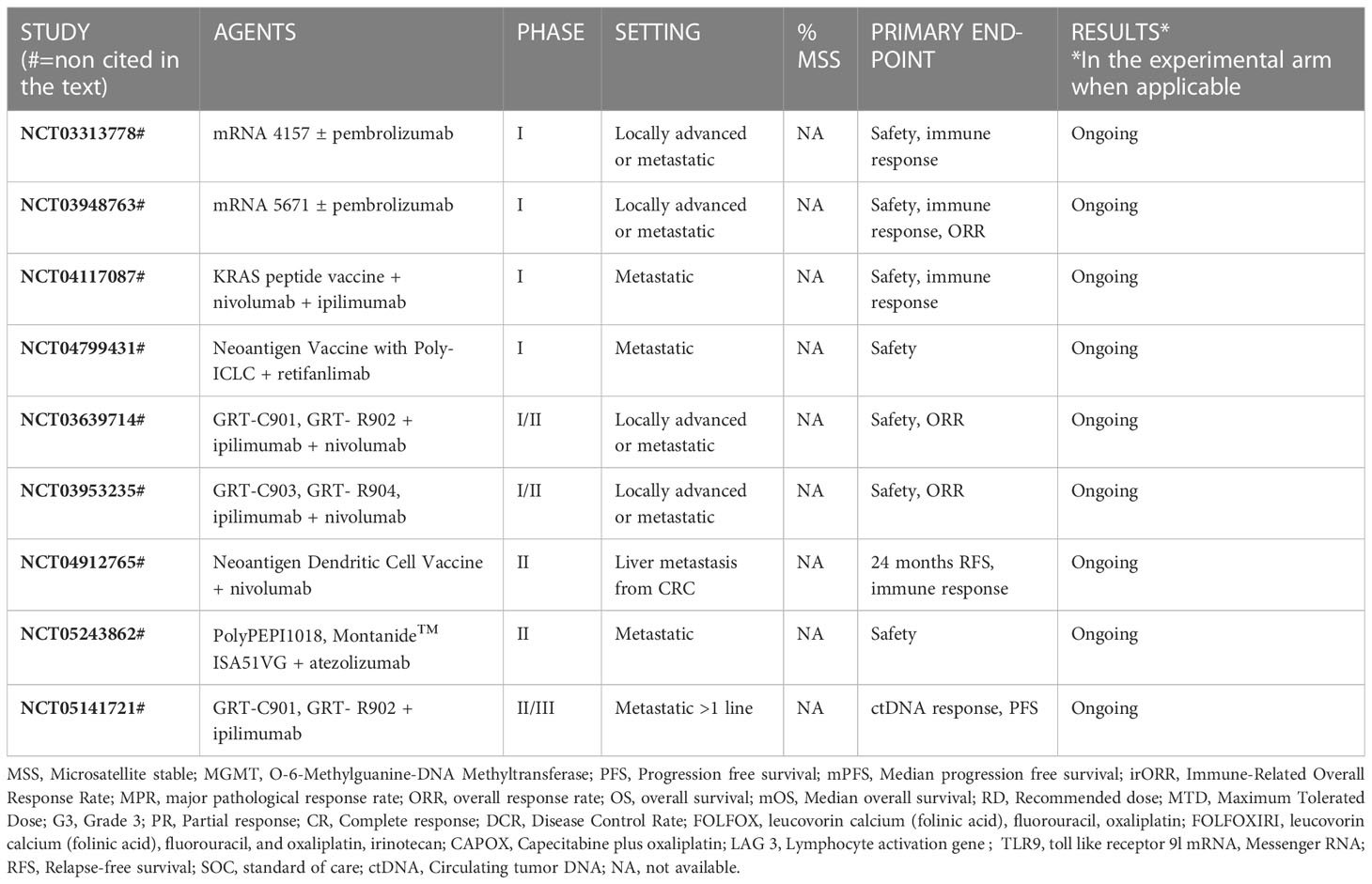
Table 6 Cancer vaccine.
Regarding biomarkers, the significant predictive value of response to ICI of harbouring a pathogenic variant of POLE/POLD (84) needs to be deepened since it is still unclear which POLE mutations must be determined. A promising possibility seems to be combining POLE mutation and TMB, in order to identify patients that could benefit most from immunotherapy.
Moreover, the clinical presentation of pMMR/MSS mCRC is becoming relevant as a reliable predictive factor and in particular the presence of liver metastases, as shown in the REGONIVO trial (30). Indeed, In the mCRC subgroup (25 patients), ORR was 33.3% with significant differences according to metastatic sites. Indeed, the ORR was 63.3% in the patients with lung or nodal metastatic disease and 8.3% in the patients with liver involvement. These results are consistent with those observed in other advanced tumors (85) and suggest that the liver micro-environment may show immunosuppressive features (86), with low tumor control by immune checkpoint inhibitors (87).
As a new avenue, recent evidence uncovered the central role that intestinal microbiome could play.
The human gut contains a huge variety of species and metabolites that can interact with other tissues, modulating their functioning (88). Moreover, it has been demonstrated that the prevalence of different bacteria species could also modify the risk of developing cancer, especially through the activation of inflammatory pathways including NF-kB, IL-6, TNF and other cytokines (89). For example, E. Coli, C. Jejuni and F. nucleatum produce metabolites that can induce oncogenic changes (89). Based on this knowledge, lot of studies have been made in order to evaluate if microbiota could be used to modulate prevention and therapy. Indeed, previously studies have demonstrated that some of the gut microbioma’s species can contribute not only to prevent or enhance the risk of CRC, but, furthermore, to modulate efficacy and toxicity of some chemotherapeutic drugs (89, 90).
A study conducted on patients affected by gastrointestinal cancers, for whom faecal samplings before and after chemotherapy were collected, showed, a modification of the pattern of microbiome bacteria, that may be related to efficacy: for example, R. faecis was more likely to decline after treatment in non-responder oesophageal cancer patients, while increased in good responders. The monitoring of the variation of specific bacteria could be an alternative in evaluating response to treatments, since the faecal microbiota test is non-invasive and easy to be performed. However, these aspects need further investigations (90).
Recent research suggests that the interaction between host and gut microbiome could also affect the responsiveness to immunotherapies, likely due to a systemic activation of CD8+ Tcell stimulated by the release from gut bacteria of immunomodulatory molecules and metabolites. However, the mechanism is still unclear and under investigation (91). In particular, an important role of Bacteroides species in immunostimulatory modulation of CTLA-4 blockade has been identified, while Akkermansia, Faecalibacterium, Clostridiale and Bifidobacterium spp seem to be associated with PD-L1 inhibitors (88). Since resistance to immunotherapy is difficult to overcome, manipulating the gut microbiota could represent a promising strategy (92).
Based on this evidence, an emerging method for altering microbiota is the faecal microbiota transplantation (FMT), already used in some gastrointestinal disease as Inflammatory Bowel Disease (IBD), that allows to transplant stool information from healthy donors to patients (88). In a recent published clinical trial, long responder melanoma patients were used as donors of faecal stool for patient with a diagnosis of melanoma primarily resistant to immune checkpoint inhibitors: 6 patients out of 15 showed a radiological response, including objective response and stable disease. These data suggest that FMT could represent a method to overcome resistance to ICIs in melanoma (93).
For CRC, data are still immature. A pre-clinical trial on mice with MSS CRC showed that changes in the gut microbiome, due to the use of different antibiotics, affect the glycerophospholipid metabolic pathway and, consequently, the expression of immune-related cytokines: this results in a regulation of the therapeutic effect of immunotherapy in this subset of tumors, widely known for been resistant to ICIs (94).
In conclusion, data on the therapeutic aspects of microbiome are still immature and need further investigations, but, based on the important role that it plays in the regulation of the immune system, it seems to be a promising option for modulating response to immunotherapy.
All authors made substantial contributions to this manuscript. AG, AP, SS contributed to the manuscript revision. AP and SS supervised the final version. All authors contributed to the article and approved the submitted version.
SS declares speaker fees from AMGEN, SERVIER, MERCK, MSD, travel/accomodation and expenses from NOVARTIS, IPSEN, AMGEN, TRIPLA-A, PFIZER, CELLGENE, and they’re a member of a roundtable for ASTRAZENECA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin january (2022) 72(1):7–33. doi: 10.3322/caac.21708
2. Diaz LA, Shiu KK, Kim TW, Jensen BV, Jensen LH, Punt C, et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, phase 3 study. Lancet Oncol (2022) 23(5):659–70. doi: 10.1016/S1470-2045(22)00197-8
3. Boland CR, Goel A. Microsatellite instability in colorectal cancer. Gastroenterology (2010) 138(6):2073–2087.e3. doi: 10.1053/j.gastro.2009.12.064
4. Sullivan BA, Noujaim M, Roper J. Cause, epidemiology, and histology of polyps and pathways to colorectal cancer. Gastrointest Endosc Clin N Am (2022) 32(2):177–94. doi: 10.1016/j.giec.2021.12.001
5. Huyghe N, Benidovskaya E, Stevens P, Van den Eynde M. Biomarkers of response and resistance to immunotherapy in microsatellite stable colorectal cancer: toward a new personalized medicine. Cancers (2022) 14(9):2241. doi: 10.3390/cancers14092241
6. Ghiringhelli F, Fumet JD. Is there a place for immunotherapy for metastatic microsatellite stable colorectal cancer? Front Immunol (2019) 10:1816. doi: 10.3389/fimmu.2019.01816
7. Siena S, Sartore-Bianchi A, Personeni N, Pietrantonio F, Germano G, Amatu A, et al. Pembrolizumab in MMR-proficient metastatic colorectal cancer pharmacologically primed to trigger dynamic hypermutation status: the ARETHUSA trial. J Clin Oncol (2019) 37(15_suppl):TPS2659–TPS2659. doi: 10.1200/JCO.2019.37.15_suppl.TPS2659
8. Pietrobon V, Marincola FM. Hypoxia and the phenomenon of immune exclusion. J Transl Med (2021) 19(1):9. doi: 10.1186/s12967-020-02667-4
9. Yoon HH, Shi Q, Heying EN, Muranyi A, Bredno J, Ough F, et al. Intertumoral heterogeneity of CD3+ and CD8+ T-cell densities in the microenvironment of DNA mismatch-Repair-Deficient colon cancers: implications for prognosis. Clin Cancer Res Off J Am Assoc Cancer Res (2019) 25(1):125–33. doi: 10.1158/1078-0432.CCR-18-1984
10. Owyang SY, Zhang M, Walkup GA, Chen GE, Grasberger H, El-Zaatari M, et al. The effect of CT26 tumor-derived TGF-β on the balance of tumor growth and immunity. Immunol Lett (2017) 191:47–54. doi: 10.1016/j.imlet.2017.08.024
11. Spranger S, Bao R, Gajewski TF. Melanoma-intrinsic β-catenin signalling prevents anti-tumour immunity. Nature (2015) 523(7559):231–5. doi: 10.1038/nature14404
12. Loi S, Dushyanthen S, Beavis PA, Salgado R, Denkert C, Savas P, et al. RAS/MAPK activation is associated with reduced tumor-infiltrating lymphocytes in triple-negative breast cancer: therapeutic cooperation between MEK and PD-1/PD-L1 immune checkpoint inhibitors. Clin Cancer Res (2016) 22(6):1499–509. doi: 10.1158/1078-0432.CCR-15-1125
13. Velho S, Oliveira C, Ferreira A, Ferreira AC, Suriano G, Schwartz S, et al. The prevalence of PIK3CA mutations in gastric and colon cancer. Eur J Cancer Oxf Engl 1990 (2005) 41(11):1649–54. doi: 10.1016/j.ejca.2005.04.022
14. Vidotto T, Melo CM, Castelli E, Koti M, dos Reis RB, Squire JA. Emerging role of PTEN loss in evasion of the immune response to tumours. Br J Cancer (2020) 122(12):1732–43. doi: 10.1038/s41416-020-0834-6
15. Saito T, Nishikawa H, Wada H, Nagano Y, Sugiyama D, Atarashi K, et al. Two FOXP3+CD4+ T cell subpopulations distinctly control the prognosis of colorectal cancers. Nat Med (2016) 22(6):679–84. doi: 10.1038/nm.4086
16. Nishikawa H, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Curr Opin Immunol (2014) 27:1–7. doi: 10.1016/j.coi.2013.12.005
17. Takahashi Y, Kitadai Y, Bucana CD, Cleary KR, Ellis LM. Expression of vascular endothelial growth factor and its receptor, KDR, correlates with vascularity, metastasis, and proliferation of human colon cancer. Cancer Res (1995) 55(18):3964–8.
18. Noman MZ, Buart S, Van Pelt J, Richon C, Hasmim M, Leleu N, et al. The cooperative induction of hypoxia-inducible factor-1α and STAT3 during hypoxia induced an impairment of tumor susceptibility to CTL-mediated cell lysis. J Immunol (2009) 182(6):3510–21. doi: 10.4049/jimmunol.0800854
19. Gabrilovich D, Ishida T, Oyama T, Ran S, Kravtsov V, Nadaf S, et al. Vascular endothelial growth factor inhibits the development of dendritic cells and dramatically affects the differentiation of multiple hematopoietic lineages in vivo. Blood (1998) 92(11):4150–66. doi: 10.1182/blood.V92.11.4150
20. Galbraith NJ, Wood C, Steele CW. Targeting metastatic colorectal cancer with immune oncological therapies. Cancers (2021) 13(14):3566. doi: 10.3390/cancers13143566
21. Emens LA, Middleton G. The interplay of immunotherapy and chemotherapy: harnessing potential synergies. Cancer Immunol Res (2015) 3(5):436–43. doi: 10.1158/2326-6066.CIR-15-0064
22. Morano F, Raimondi A, Pagani F, Lonardi S, Salvatore L, Cremolini C, et al. Temozolomide followed by combination with low-dose ipilimumab and nivolumab in patients with microsatellite-stable, O6-Methylguanine-DNA methyltransferase-silenced metastatic colorectal cancer: the MAYA trial. J Clin Oncol Off J Am Soc Clin Oncol (2022) 40(14):1562–73. doi: 10.1200/JCO.21.02583
23. Antoniotti C, Borelli B, Rossini D, Pietrantonio F, Morano F, Salvatore L, et al. AtezoTRIBE: a randomised phase II study of FOLFOXIRI plus bevacizumab alone or in combination with atezolizumab as initial therapy for patients with unresectable metastatic colorectal cancer. BMC Cancer (2020) 20(1):683. doi: 10.1186/s12885-020-07169-6
24. Lenz HJ, Parikh AR, Spigel DR, Cohn AL, Yoshino T, Kochenderfer MD, et al. Nivolumab (NIVO) + 5-fluorouracil/leucovorin/oxaliplatin (mFOLFOX6)/bevacizumab (BEV) versus mFOLFOX6/BEV for first-line (1L) treatment of metastatic colorectal cancer (mCRC): phase 2 results from CheckMate 9X8. J Clin Oncol (2022) 40(4_suppl):8–8. doi: 10.1200/JCO.2022.40.4_suppl.008
25. Patel MR, Falchook GS, Hamada K, Makris L, Bendell JC. A phase 2 trial of trifluridine/tipiracil plus nivolumab in patients with heavily pretreated microsatellite-stable metastatic colorectal cancer. Cancer Med (2021) 10(4):1183–90. doi: 10.1002/cam4.3630
26. Germano G, Lamba S, Rospo G, Barault L, Magrì A, Maione F, et al. Inactivation of DNA repair triggers neoantigen generation and impairs tumour growth. Nature (2017) 552(7683):116–20. doi: 10.1038/nature24673
27. Schmoll HJ, Arnold D, de Gramont A, Ducreux M, Grothey A, O’Dwyer PJ, et al. MODUL-a multicenter randomized clinical trial of biomarker-driven maintenance therapy following first-line standard induction treatment of metastatic colorectal cancer: an adaptable signal-seeking approach. J Cancer Res Clin Oncol (2018) 144(6):1197–204. doi: 10.1007/s00432-018-2632-6
28. Tabernero J, Grothey A, Arnold D, de Gramont A, Ducreux M, O’Dwyer P, et al. MODUL cohort 2: an adaptable, randomized, signal-seeking trial of fluoropyrimidine plus bevacizumab with or without atezolizumab maintenance therapy for BRAF metastatic colorectal cancer. ESMO Open (2022) 7(5):100559. doi: 10.1016/j.esmoop.2022.100559
29. Hoff S, Grünewald S, Röse L, Zopf D. Immunomodulation by regorafenib alone and in combination with anti PD1 antibody on murine models of colorectal cancer. Ann Oncol (2017) 28:v423. doi: 10.1093/annonc/mdx376.060
30. Fukuoka S, Hara H, Takahashi N, Kojima T, Kawazoe A, Asayama M, et al. Regorafenib plus nivolumab in patients with advanced gastric or colorectal cancer: an open-label, dose-escalation, and dose-expansion phase ib trial (REGONIVO, EPOC1603). J Clin Oncol Off J Am Soc Clin Oncol (2020) 38(18):2053–61. doi: 10.1200/JCO.19.03296
31. Fakih M, Raghav KPS, Chang DZ, Larson T, Cohn AL, Huyck TK, et al. Regorafenib plus nivolumab in patients with mismatch repair-proficient/microsatellite stable metastatic colorectal cancer: a single-arm, open-label, multicentre phase 2 study. eClinicalMedicine (2023) 58:101917. doi: 10.1016/j.eclinm.2023.101917
32. Kim RD, Kovari BP, Martinez M, Xie H, Sahin IH, Mehta R, et al. A phase I/Ib study of regorafenib and nivolumab in mismatch repair proficient advanced refractory colorectal cancer. Eur J Cancer Oxf Engl 1990 (2022) 169:93–102. doi: 10.1016/j.ejca.2022.03.026
33. Barzi A, Azad NS, Yang Y, Tsao-Wei D, Rehman R, Fakih M, et al. Phase I/II study of regorafenib (rego) and pembrolizumab (pembro) in refractory microsatellite stable colorectal cancer (MSSCRC). J Clin Oncol (2022) 40(4_suppl):15–5. doi: 10.1200/JCO.2022.40.4_suppl.015
34. Cousin S, Cantarel C, Guegan JP, Gomez-Roca C, Metges JP, Adenis A, et al. Regorafenib-avelumab combination in patients with microsatellite stable colorectal cancer (REGOMUNE): a single-arm, open-label, phase II trial. Clin Cancer Res Off J Am Assoc Cancer Res (2021) 27(8):2139–47. doi: 10.1158/1078-0432.CCR-20-3416
35. Gomez-Roca C, Yanez E, Im SA, Castanon Alvarez E, Senellart H, Doherty M, et al. LEAP-005: a phase II multicohort study of lenvatinib plus pembrolizumab in patients with previously treated selected solid tumors–results from the colorectal cancer cohort. J Clin Oncol (2021) 39(3_suppl):94–4. doi: 10.1200/JCO.2021.39.3_suppl.94
36. Lang J, Leal AD, Marín-Jiménez JA, Hartman SJ, Shulman J, Navarro NM, et al. Cabozantinib sensitizes microsatellite stable colorectal cancer to immune checkpoint blockade by immune modulation in human immune system mouse models. Front Oncol (2022) 12:877635. doi: 10.3389/fonc.2022.877635
37. Saeed A, Phadnis M, Park R, Sun W, Al-Rajabi RMT, Baranda JC, et al. Cabozantinib (cabo) combined with durvalumab (durva) in gastroesophageal (GE) cancer and other gastrointestinal (GI) malignancies: preliminary phase ib CAMILLA study results. J Clin Oncol (2020) 38(15_suppl):4563–3. doi: 10.1200/JCO.2020.38.15_suppl.4563
38. Kopetz S, Grothey A, Yaeger R, Van Cutsem E, Desai J, Yoshino T, et al. Encorafenib, binimetinib, and cetuximab in BRAF V600E-mutated colorectal cancer. N Engl J Med (2019) 381(17):1632–43. doi: 10.1056/NEJMoa1908075
39. Morris VK, Parseghian CM, Escano M, Johnson B, Raghav KPS, Dasari A, et al. Phase I/II trial of encorafenib, cetuximab, and nivolumab in patients with microsatellite stable, BRAFV600E metastatic colorectal cancer. J Clin Oncol (2022) 40(4_suppl):12–2. doi: 10.1200/JCO.2022.40.4_suppl.012
40. Ebert PJR, Cheung J, Yang Y, McNamara E, Hong R, Moskalenko M, et al. MAP kinase inhibition promotes T cell and anti-tumor activity in combination with PD-L1 checkpoint blockade. Immunity (2016) 44(3):609–21. doi: 10.1016/j.immuni.2016.01.024
41. Ciardiello D, Vitiello PP, Cardone C, Martini G, Troiani T, Martinelli E, et al. Immunotherapy of colorectal cancer: challenges for therapeutic efficacy. Cancer Treat Rev (2019) 76:22–32. doi: 10.1016/j.ctrv.2019.04.003
42. Bendell JC, Kim TW, Goh BC, Wallin J, Oh DY, Han SW, et al. Clinical activity and safety of cobimetinib (cobi) and atezolizumab in colorectal cancer (CRC). J Clin Oncol (2016) 34(15_suppl):3502–2. doi: 10.1200/JCO.2016.34.15_suppl.3502
43. Hellmann MD, Kim TW, Lee CB, Goh BC, Miller WH, Oh DY, et al. Phase ib study of atezolizumab combined with cobimetinib in patients with solid tumors. Ann Oncol Off J Eur Soc Med Oncol (2019) 30(7):1134–42. doi: 10.1093/annonc/mdz113
44. Eng C, Kim TW, Bendell J, Argilés G, Tebbutt NC, Di Bartolomeo M, et al. Atezolizumab with or without cobimetinib versus regorafenib in previously treated metastatic colorectal cancer (IMblaze370): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol (2019) 20(6):849–61. doi: 10.1016/S1470-2045(19)30027-0
45. Mettu NB, Ou FS, Zemla TJ, Halfdanarson TR, Lenz HJ, Breakstone RA, et al. Assessment of capecitabine and bevacizumab with or without atezolizumab for the treatment of refractory metastatic colorectal cancer: a randomized clinical trial. JAMA Netw Open (2022) 5(2):e2149040. doi: 10.1001/jamanetworkopen.2021.49040
46. Lee MS, Loehrer PJ, Imanirad I, Cohen S, Ciombor KK, Moore DT, et al. Phase II study of ipilimumab, nivolumab, and panitumumab in patients with KRAS/NRAS/BRAF wild-type (WT) microsatellite stable (MSS) metastatic colorectal cancer (mCRC). J Clin Oncol (2021) 39(3_suppl):7–7. doi: 10.1200/JCO.2021.39.3_suppl.7
47. Stein A, Binder M, Goekkurt E, Lorenzen S, Riera-Knorrenschild J, Depenbusch R, et al. Avelumab and cetuximab in combination with FOLFOX in patients with previously untreated metastatic colorectal cancer (MCRC): final results of the phase II AVETUX trial (AIO-KRK-0216). J Clin Oncol (2020) 38(4_suppl):96–6. doi: 10.1200/JCO.2020.38.4_suppl.96
48. Martinelli E, Martini G, Famiglietti V, Troiani T, Napolitano S, Pietrantonio F, et al. Cetuximab rechallenge plus avelumab in pretreated patients with RAS wild-type metastatic colorectal cancer: the phase 2 single-arm clinical CAVE trial. JAMA Oncol (2021) 7(10):1529–35. doi: 10.1001/jamaoncol.2021.2915
49. Bocobo AG, Wang R, Behr S, Carnevale JC, Cinar P, Collisson EA, et al. Phase II study of pembrolizumab plus capecitabine and bevacizumab in microsatellite stable (MSS) metastatic colorectal cancer (mCRC): interim analysis. J Clin Oncol (2021) 39(3_suppl):77–7. doi: 10.1200/JCO.2021.39.3_suppl.77
50. Chen DS, Hurwitz H. Combinations of bevacizumab with cancer immunotherapy. Cancer J (2018) 24(4):193–204. doi: 10.1097/PPO.0000000000000327
51. Woolston A, Khan K, Spain G, Barber LJ, Griffiths B, Gonzalez-Exposito R, et al. Genomic and transcriptomic determinants of therapy resistance and immune landscape evolution during anti-EGFR treatment in colorectal cancer. Cancer Cell (2019) 36(1):35–50.e9. doi: 10.1016/j.ccell.2019.05.013
52. Chen EX, Jonker DJ, Loree JM, Kennecke HF, Berry SR, Couture F, et al. Effect of combined immune checkpoint inhibition vs best supportive care alone in patients with advanced colorectal cancer: the Canadian cancer trials group CO.26 study. JAMA Oncol (2020) 6(6):831–8. doi: 10.1001/jamaoncol.2020.0910
53. Garralda E, Sukari A, Lakhani NJ, Patnaik A, Lou Y, Im SA, et al. A phase 1 first-in-human study of the anti-LAG-3 antibody MK4280 (favezelimab) plus pembrolizumab in previously treated, advanced microsatellite stable colorectal cancer. J Clin Oncol (2021) 39(15_suppl):3584–4. doi: 10.1200/JCO.2021.39.15_suppl.3584
54. Bullock A, Grossman J, Fakih M, Lenz H, Gordon M, Margolin K, et al. LBA O-9 botensilimab, a novel innate/adaptive immune activator, plus balstilimab (anti-PD-1) for metastatic heavily pretreated microsatellite stable colorectal cancer. Ann Oncol (2022) 33:S376. doi: 10.1016/j.annonc.2022.04.453
55. Goldberg MV, Drake CG. LAG-3 in cancer immunotherapy. Curr Top Microbiol Immunol (2011) 344:269–78. doi: 10.1007/82_2010_114
56. Natoli M, Hatje K, Gulati P, Junker F, Herzig P, Jiang Z, et al. Deciphering molecular and cellular ex vivo responses to bispecific antibodies PD1-TIM3 and PD1-LAG3 in human tumors. J Immunother Cancer (2022) 10(11):e005548. doi: 10.1136/jitc-2022-005548
57. Abuodeh Y, Venkat P, Kim S. Systematic review of case reports on the abscopal effect. Curr Probl Cancer (2016) 40(1):25–37. doi: 10.1016/j.currproblcancer.2015.10.001
58. Rodriguez-Ruiz ME, Rodriguez I, Barbes B, Mayorga L, Sanchez-Paulete AR, Ponz-Sarvise M, et al. Brachytherapy attains abscopal effects when combined with immunostimulatory monoclonal antibodies. Brachyther (2017) 16(6):1246–51. doi: 10.1016/j.brachy.2017.06.012
59. Zhang Z, Liu X, Chen D, Yu J. Radiotherapy combined with immunotherapy: the dawn of cancer treatment. Signal Transduct Target Ther (2022) 7(1):258. doi: 10.1038/s41392-022-01102-y
60. Parikh AR, Szabolcs A, Allen JN, Clark JW, Wo JY, Raabe M, et al. Radiation therapy enhances immunotherapy response in microsatellite stable colorectal and pancreatic adenocarcinoma in a phase II trial. Nat Cancer (2021) 2(11):1124–35. doi: 10.1038/s43018-021-00269-7
61. Segal NH, Cercek A, Ku G, Wu AJ, Rimner A, Khalil DN, et al. Phase II single-arm study of durvalumab and tremelimumab with concurrent radiotherapy in patients with mismatch repair-proficient metastatic colorectal cancer. Clin Cancer Res Off J Am Assoc Cancer Res (2021) 27(8):2200–8. doi: 10.1158/1078-0432.CCR-20-2474
62. Morse MA, Hochster H, Benson A. Perspectives on treatment of metastatic colorectal cancer with immune checkpoint inhibitor therapy. Oncologist (2020) 25(1):33–45. doi: 10.1634/theoncologist.2019-0176
63. André T, Overman M, Lonardi S, Aglietta M, McDermott R, Wong KYM, et al. Analysis of tumor PD-L1 expression and biomarkers in relation to clinical activity in patients (pts) with deficient DNA mismatch repair (dMMR)/high microsatellite instability (MSI-h) metastatic colorectal cancer (mCRC) treated with nivolumab (NIVO) + ipilimumab (IPI): CheckMate 142. Ann Oncol (2017) 28:v163. doi: 10.1093/annonc/mdx393.011
64. Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol (2017) 18(9):1182–91. doi: 10.1016/S1470-2045(17)30422-9
65. Fabrizio DA, George TJ Jr., Dunne RF, Frampton G, Sun J, Gowen K, et al. Beyond microsatellite testing: assessment of tumor mutational burden identifies subsets of colorectal cancer who may respond to immune checkpoint inhibition. J Gastrointest Oncol (2018) 9(4):610–7. doi: 10.21037/jgo.2018.05.06
66. Goodman AM, Sokol ES, Frampton GM, Lippman SM, Kurzrock R. Microsatellite-stable tumors with high mutational burden benefit from immunotherapy. Cancer Immunol Res (2019) 7(10):1570–3. doi: 10.1158/2326-6066.CIR-19-0149
67. Salem ME, Bodor JN, Puccini A, Xiu J, Goldberg RM, Grothey A, et al. Relationship between MLH1, PMS2, MSH2 and MSH6 gene-specific alterations and tumor mutational burden in 1057 microsatellite instability-high solid tumors. Int J Cancer (2020) 147(10):2948–56. doi: 10.1002/ijc.33115
68. Schrock AB, Ouyang C, Sandhu J, Sokol E, Jin D, Ross JS, et al. Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann Oncol (2019) 30(7):1096–103. doi: 10.1093/annonc/mdz134
69. Mangat PK, Halabi S, Bruinooge SS, Garrett-Mayer E, Alva A, Janeway KA, et al. Rationale and design of the targeted agent and profiling utilization registry study. JCO Precis Oncol (2018) 2):1–14. doi: 10.1200/PO.18.00122
70. Meiri E, Garrett-Mayer E, Halabi S, Mangat PK, Shrestha S, Ahn ER, et al. Pembrolizumab (P) in patients (Pts) with colorectal cancer (CRC) with high tumor mutational burden (HTMB): results from the targeted agent and profiling utilization registry (TAPUR) study. J Clin Oncol (2020) 38(4_suppl):133–3. doi: 10.1200/JCO.2020.38.4_suppl.133
71. Vaccaro GM, Rothe M, Mangat PK, Garrett-Mayer E, Hwang JJ, Alese OB, et al. Nivolumab plus ipilimumab (N+I) in patients (pts) with colorectal cancer (CRC) with high tumor mutational burden (hTMB): results from the targeted agent and profiling utilization registry (TAPUR) study. J Clin Oncol (2022) 40(4_suppl):107–7. doi: 10.1200/JCO.2022.40.4_suppl.107
72. The Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature (2012) 487(7407):330–7. doi: 10.1038/nature11252
73. The CORGI Consortium, The WGS500 Consortium, Palles C, Cazier JB, Howarth KM, Domingo E, et al. Germline mutations affecting the proofreading domains of POLE and POLD1 predispose to colorectal adenomas and carcinomas. Nat Genet (2013) 45(2):136–44. doi: 10.1038/ng.2503
74. Wang F, Zhao Q, Wang YN, Jin Y, He MM, Liu ZX, et al. Evaluation of POLE and POLD1 mutations as biomarkers for immunotherapy outcomes across multiple cancer types. JAMA Oncol (2019) 5(10):1504. doi: 10.1001/jamaoncol.2019.2963
75. Domingo E, Freeman-Mills L, Rayner E, Glaire M, Briggs S, Vermeulen L, et al. Somatic POLE proofreading domain mutation, immune response, and prognosis in colorectal cancer: a retrospective, pooled biomarker study. Lancet Gastroenterol Hepatol (2016) 1(3):207–16. doi: 10.1016/S2468-1253(16)30014-0
76. Baraibar I, Mirallas O, Saoudi N, Ros J, Salvà F, Tabernero J, et al. Combined treatment with immunotherapy-based strategies for MSS metastatic colorectal cancer. Cancers (2021) 13(24):6311. doi: 10.3390/cancers13246311
77. Jung G, Hernández-Illán E, Moreira L, Balaguer F, Goel A. Epigenetics of colorectal cancer: biomarker and therapeutic potential. Nat Rev Gastroenterol Hepatol february (2020) 17(2):111–30. doi: 10.1038/s41575-019-0230-y
78. Guinney J, Dienstmann R, Wang X, de Reyniès A, Schlicker A, Soneson C, et al. The consensus molecular subtypes of colorectal cancer. Nat Med november (2015) 21(11):1350–6. doi: 10.1038/nm.3967
79. Mehrvarz Sarshekeh A, Lam M, Zorrilla IR, Holliday EB, Das P, Kee BK, et al. Consensus molecular subtype (CMS) as a novel integral biomarker in colorectal cancer: a phase II trial of bintrafusp alfa in CMS4 metastatic CRC. J Clin Oncol (2020) 38(15_suppl):4084–4. doi: 10.1200/JCO.2020.38.15_suppl.4084
80. Loree JM, Topham JT, Kennecke HF, Feilotter H, Lee YS, Virk S, et al. Impact of consensus molecular subtyping (CMS) on survival in the CO.26 trial of durvalumab plus tremelimumab versus best supportive care (BSC) in metastatic colorectal cancer (mCRC). J Clin Oncol (2022) 40(16_suppl):3551–1. doi: 10.1200/JCO.2022.40.16_suppl.3551
81. Fakih M, Raghav KPS, Chang DZ, Bendell JC, Larson T, Cohn AL, et al. Single-arm, phase 2 study of regorafenib plus nivolumab in patients with mismatch repair-proficient (pMMR)/microsatellite stable (MSS) colorectal cancer (CRC). J Clin Oncol (2021) 39(15_suppl):3560–0. doi: 10.1200/JCO.2021.39.15_suppl.3560
82. Sahin U, Türeci Ö. Personalized vaccines for cancer immunotherapy. Science (2018) 359(6382):1355–60. doi: 10.1126/science.aar7112
83. Peng M, Mo Y, Wang Y, Wu P, Zhang Y, Xiong F, et al. Neoantigen vaccine: an emerging tumor immunotherapy. Mol Cancer (2019) 18(1):128. doi: 10.1186/s12943-019-1055-6
84. Wen L, Chen Z, Ji X, Fong WP, Shao Q, Ren C, et al. Pathological complete response to immune checkpoint inhibitor in patients with colorectal cancer liver metastases harboring POLE exonuclease domain mutation. J Immunother Cancer (2022) 10(7):e004487. doi: 10.1136/jitc-2022-004487
85. Yu J, Green MD, Li S, Sun Y, Journey SN, Choi JE, et al. Liver metastasis restrains immunotherapy efficacy via macrophage-mediated T cell elimination. Nat Med (2021) 27(1):152–64. doi: 10.1038/s41591-020-1131-x
86. Zeng X, Ward SE, Zhou J, Cheng ASL. Liver immune microenvironment and metastasis from colorectal cancer-pathogenesis and therapeutic perspectives. Cancers (2021) 13(10):2418. doi: 10.3390/cancers13102418
87. Gholami S, Grothey A, Lenz HJ. Microsatellite stable colorectal liver metastases–understanding the mechanisms of immune resistance. JAMA Netw Open (2021) 4(8):e2119025. doi: 10.1001/jamanetworkopen.2021.19025
88. Son YM, Kim J. The microbiome-immune axis therapeutic effects in cancer treatments. J Microbiol Biotechnol (2022) 32(9):1086–97. doi: 10.4014/jmb.2208.08002
89. Lu L, Dong J, Liu Y, Qian Y, Zhang G, Zhou W, et al. New insights into natural products that target the gut microbiota: effects on the prevention and treatment of colorectal cancer. Front Pharmacol (2022) 13:964793. doi: 10.3389/fphar.2022.964793
90. Li N, Bai C, Zhao L, Sun Z, Ge Y, Li X. The relationship between gut microbiome features and chemotherapy response in gastrointestinal cancer. Front Oncol (2021) 11:781697. doi: 10.3389/fonc.2021.781697
91. Azimi M, Keshavarz Shahbaz S, Mansourabadi AH, Mohamed Khosroshahi L, Pourkalhor S, Rezakhani M, et al. Intestinal microbiota: novel personalized cancer immunotherapy in colorectal cancer. Int Arch Allergy Immunol (2022) 183(11):1147–65. doi: 10.1159/000525695
92. Koustas E, Trifylli EM, Sarantis P, Papadopoulos N, Aloizos G, Tsagarakis A, et al. Implication of gut microbiome in immunotherapy for colorectal cancer. World J Gastrointest Oncol (2022) 14(9):1665–74. doi: 10.4251/wjgo.v14.i9.1665
93. Davar D, Dzutsev AK, McCulloch JA, Rodrigues RR, Chauvin JM, Morrison RM, et al. Fecal microbiota transplant overcomes resistance to anti-PD-1 therapy in melanoma patients. Science (2021) 371(6529):595–602. doi: 10.1126/science.abf3363
Keywords: microsatellite stable, MSS, colorectal cancer, immunotherapy, checkpoint inhibitors, combination strategy, immunomodulation, microbiome
Citation: Gandini A, Puglisi S, Pirrone C, Martelli V, Catalano F, Nardin S, Seeber A, Puccini A and Sciallero S (2023) The role of immunotherapy in microsatellites stable metastatic colorectal cancer: state of the art and future perspectives. Front. Oncol. 13:1161048. doi: 10.3389/fonc.2023.1161048
Received: 07 February 2023; Accepted: 21 April 2023;
Published: 03 May 2023.
Edited by:
Yu Sunakawa, St. Marianna University School of Medicine, JapanReviewed by:
Titto Augustine, Purdue University Indianapolis, United StatesCopyright © 2023 Gandini, Puglisi, Pirrone, Martelli, Catalano, Nardin, Seeber, Puccini and Sciallero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefania Sciallero, c3RlZmFuaWEuc2NpYWxsZXJvQGhzYW5tYXJ0aW5vLml0
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.