 Li Liu
Li Liu Aihua Zhang4†
Aihua Zhang4† Mingzhu Su
Mingzhu Su Xiaojie Sun
Xiaojie Sun
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 21 April 2023
Sec. Cancer Epidemiology and Prevention
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1151465
This article is part of the Research TopicFinancial Anxiety in Cancer Prevention and Cancer ControlView all 10 articles
Background: Financial hardship has been described as a patient’s economic experiencefollowing cancer-related treatment. Standardized patient-reported outcome measures(PROM) to assess this distress has not been well-studied, especially among older cancer survivors.
Objective: The aim of this study was to develop and validate PROM for assessing the financial hardship of older cancer survivors in China.
Methods: Items were generated using qualitative interviews and literature review. Items were screened based on Delphi expert consultation and patients’ opinions. Item response theory (IRT) and classical test theory (CTT) were used to help reduce items. Retained items formed a pilot instrument that was subjected to psychometric testing. A cut-off score for the new instrument for predicting poor quality of life was identified by receiver operating characteristic (ROC) analysis.
Results: Qualitative interviews and literature review generated 135 items, which were reduced to 60 items because of redundancy. Following Delphi expert consultation and patients’ evaluation, 24 items with high importance were extracted. Sixteen items were selected due to satisfactory statistical analysis based on CTT and IRT. Ten items were retained and comprised 2 domains after loadings in exploratory factor analysis (EFA). Internal consistency was satisfactory (α = 0.838). Test-retest reliability was good (intraclass correlation, 0.909). The ROC analysis suggested that the cut-off of 18.5 yielded an acceptable sensitivity and specificity.
Conclusions: The PROM for Hardship and Recovery with Distress Survey (HARDS) consists of 10 items that specifically reflect the experiences of financial hardship among older Chinese cancer survivors, and it also showed good reliability and validity in clinical settings.
Financial hardship is defined as patients often being confronted with negative financial consequences of cancer treatment, which include material hardships (e.g., significant out-of-pocket, loss of income), psychological response measures (e.g., distress, stress due to paying medical bills), and coping behavioral measures (e.g., delaying cancer treatment, skipping medications) (1, 2). Financial hardship has a negative effect on cancer patients’ health-related quality of life (HRQoL) and clinical outcomes. Patients with financial hardship were likely to show cancer-related medication nonadherence; worse overall physical, emotional, and social functioning; and decreased well-being (3, 4). Cancer survivors experienced severe and persistent financial hardship long after a cancer diagnosis and regarded it as one of their prime unmet survivorship demands (5).
Although the near-universal population coverage offered by social insurance in China has reduced the proportion of out-of-pocket spending, cancer therapies may still require substantial expenditures even among those with medical insurance. There are two basic health insurance schemes with different reimbursement proportions covering more than 95% of Chinese people, Urban Employee Basic Medical Insurance (UEBMI) and Urban-Rural Resident Basic Medical Insurance (URRBMI) (6). Generally speaking, UEBMI has a better benefits package and lower out-of-pocket costs than URRBMI (7, 8). However, approximately two-thirds of older adults [more than 60 years or older (9, 10)] participate in URRBMI. Patients covered by URRBMI had lower health care utilization and direct medical costs than those covered by UEBMI but paid higher out-of-pocket costs. Therefore, the URRBMI only provides a low level of medical security for members (11). Compared to the experiences of older patients in Western countries, the financial hardship of Chinese patients has been found to be worse (12, 13). Some older cancer survivors borrowed money because of cancer (12). In the context of Chinese culture, the tradition of filial piety is still prominent, meaning that adult children are expected to provide love, respect, material provisions, and physical care to their parents (14). A prior study found that a majority of older patients had to depend on their children to pay for cancer costs; thus, cancer-related financial hardship extended into children’s families (15). Therefore, cancer-related financial hardship among older adults is an important challenge for the healthcare system and patients’ extended families.
The need for specific instruments to estimate financial hardship has been acknowledged in previous research. In the USA, the Comprehensive Score for financial Toxicity (COST) was developed based on patient-reported outcome measures (PROM), which were validated for measuring financial hardship in cancer patients with advanced cancer and undergoing chemotherapy (16). The Financial Index of Toxicity (FIT) was developed and validated to measure financial hardship for patients with head and neck cancer in Canada (17). The Patient Reported Outcome for Fighting Financial Toxicity of cancer (PROFFIT) was designed for patients undergoing cancer treatment in Italy (18). All of these current instruments were created in relatively wealthy, developed countries in the west (19). In fact, they are not always appropriate for use in China, due to social, economic, and cultural differences between developed and developing countries (20). In particular, older cancer patients have a high risk of occurrence of comorbidities, geriatric syndromes, and disability, which significantly reduced the HRQoL of patients and caused catastrophic expenses (21). In order to alleviate medical economics burdens for older adults with cancer in China, it is essential to gain a thorough understanding of cancer-related financial hardship and its effects.
However, there is no a special instrument to describe the effects of cancer-related financial hardship among older adults in China. This theoretical framework was based on a typology of three broad domains of financial hardship. These three domains cover the following aspects: (i) the material conditions that arise from increased direct and indirect costs, (ii) the psychological response as a result of efforts necessary to cope with the increased costs and(iii) the coping behaviors itself that patients adopt to manage their medical care while experiencing increased expenses (22). The aim of this study was to develop a PROM for assessment of financial hardship among older adults with cancer that captures and integrates the relevant domains of subjective financial distress. The following specific aims guided our study: (1) develop a new measure of financial hardship for older cancer survivors in China; (2) evaluate the reliability and validity of the instrument; (3) validate this new instrument in clinical settings.
The approval for this study was provided by the Ethics Committee of the Centre for Health Management and Policy Research at Shandong University (ECSHCMSDU20200901). Participants who understood the research purposes and provided written informed consent were included. The development and validation of the instrument were performed in accordance with the Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) (23). The size and criteria of the sample was shown in the Supplemental Table 1.
The original item pool was constructed through qualitative interviews and literature reviews. We interviewed 21 older cancer survivors, 20 family caregivers, 6 oncologists, and 8 nurses using purposive sampling to explore the experiences of cancer-related financial hardship among cancer survivors, and ensure adequate representation of the conceptual domain. The early qualitative findings of the project were published (24, 25). A literature review was performed through PubMed, Web of Science, and Cochrane using selected keywords such as “financial hardship”, “financial toxicity”, “financial burden”, “financial stress/distress”, “cancer survivor”, “cost of cancer care” and “patient-reported outcome (PRO)” to extract published items related to measuring financial hardship after cancer treatment. First, the items the research team members jointly analyzed, while checking for redundancy, overlapping content, and ambiguous language. Second, the items were discussed with anyone with a different view until consensus was reached through consolidation, reflection, and theoretical thinking. Finally, if discrepancies could not be resolved, all team members held weekly online meetings to discuss the pending items and further voting produced the final result.
A Delphi method was used to evaluate the feasibility and importance of the items in the pool. A questionnaire was emailed to 23 experts representing diverse expertise in oncology-related fields (e.g., oncology, nursing, psychology, health economics). Experts were asked to rate each item in the initial pool according to (a) rationality and specificity; (b) feasibility and representativeness of implementation into clinical practice (26). Each rating was made on a 0 (low) to 10 (high) scale. To reinforce the understanding of the link between financial hardship and item content, we also invited 40 patients for the importance of the items and cognitive test. We collapsed the options to “important (assign it the value of 1)” and “not important (assign it the value of 0)” to define whether items were important and the mean values of importance scores were calculated. Finally, the items with mean value ≥0.6 (i.e., support rate ≥ 60%) were retained (16).
Older survivors who had received any cancer treatment for at least one consecutive month were included in this step. The item analysis based on Classical Test Theory (CTT) mainly included: critical ratio (CR), reliability analysis, option selection rate analysis, and correlation coefficient. Item Response Theory (IRT) was used to explore the ability and response at every level among the participants. Specifically, two-parametric logistic regression model analysis were used for dichotomous variables and five-point Likert items were analyzed by the Graded Response Model (GRM). We also performed each item’s discriminability and difficulty, item characteristic curve (ICC), item information function (IIF), and scale information function (SIF) to assess internal validity of the instrument. We deleted items with unsatisfactory indicators after group meeting. In Exploratory Factor Analysis (EFA), the factor structure used principal axis factoring analysis. Factors with eigenvalues greater than 1.0 were retained using the Kaiser–Guttman principle. We used a scree plot and parallel analysis to examine the retained factors. Factor loadings over 0.5 showed theoretical and practical significance.
Internal reliability of the multi-item instrument was assessed by analyzing inter-item correlations and using Cronbach’s α coefficient adjusted by the number of items. An estimate of Cronbach’s α >0.70 was considered to indicate acceptability (17). To analyze the test-retest reliability, the intraclass correlation coefficient (ICC) was estimated by repeating the questionnaire between the patients’ first survey and approximately 2 weeks later, with an ideal level of ICC ≥0.7 (27). Confirmatory factor analysis (CFA) was used to evaluate the overall structural validity of the instrument with criteria for a good model fit identified as: Root Mean Square Error of Approximation (RMSEA) ≤0.080, a value of ≥0.960 for Comparative Fit Index (CFI), and Tucker–Lewis Index (TLI), Goodness of Fit Index (GFI)≥0.900 (27). Convergent validity was evaluated by using the average variance extracted (AVE) and composite reliability (CR). Discriminant validity and criterion validity of the new instrument was also determined.
Cut-off scores were determined using receiver operating characteristic (ROC) analyses, which produce a comprehensive assessment of diagnostic values for sensitivity and specificity. Since the ROC curve plots the relationship between the true positive rate (sensitivity) and the false positive rate (1-specificity), it can help in selecting a value with the best predictive power. We assessed the accuracy of this prediction by the area under the ROC curve (AUC). If a value of closer to 1.0 indicates more perfect accuracy, a value ≤ 0.5 shows lower accuracy. The cut-off score of the new instrument was determined by ROC analysis based on its discriminatory ability to predict the first quartile of the PROM 10-item Global Health Scale in measuring for HRQoL (28). With poor quality of life as the health outcome, the financial hardship score was divided into higher and lower financial hardship. Finally, a multivariable logistic regression model was used to examine the relationship between cancer survivors’ characteristics and higher financial hardship. Independent variables included sociodemographic and cancer characteristics.
IRT analysis was performed using R programs to select items. The CTT analyses and EFA were conducted in SPSS 21.0. A parallel analysis was performed in MonteCarlo PCA to determine the most appropriate number of factors to extract. The data was submitted for further CFA using AMOS 24.0 with the maximum likelihood method. The characteristics of the participants such as frequency, percentage, means, and standard deviation were analyzed using descriptive statistics. Independent variables with a P value <0.05 on univariate analysis were entered into a multivariate logistic regression model analysis by adopting the stepwise method. All tests were 2-sided, and a P value < 0.05 was considered statistically significant. ROC and Logistic regression analyses were performed using SAS 9.4. All analyses were performed in 2021.
Literature review yielded 80 candidate items. An additional 43 candidate items were generated by interviews with 21 survivors and 20 family caregivers, while an additional 12 items were generated from feedback from 6 oncologists and 8 nurses. These 135 items were reduced to 60 by the investigators because of redundancy and overlapping content (see Figure 1).
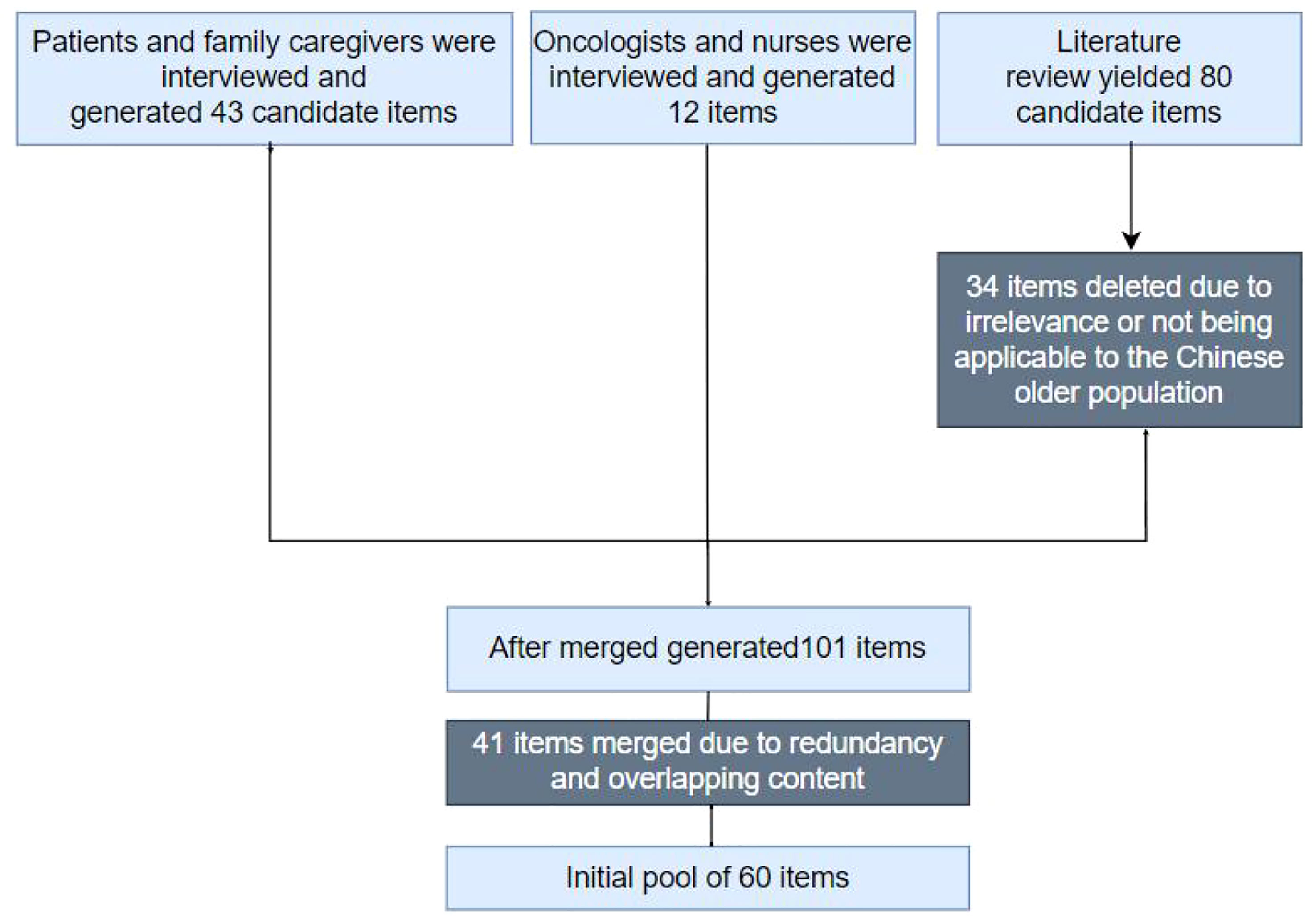
Figure 1 Initial items pool.
Two Delphi rounds were conducted. The response rate of the questionnaire was 82.6% (19/23) in round 1, and 89.5% (17/19) in round 2. In the 2-round Delphi methods, the experts’ authority coefficients were more than 0.700; they were 0.800 in round 1 and 0.897 in round 2. Finally, 36 items were deleted and 5 items were added by experts. In total, 29 items were retained. Subsequently, the important support rate of items from the 40 patients ranged from 17.5% to 100%. 5 items were excluded by an important support rate of <60%; finally, 24 items were retained (see the Supplemental Table 2).
The IRT-based item analysis showed good parameter of discrimination and difficulty among majority of items; ICC, IIF, and SIF were well distributed. The CTT based analysis item CR suggested that the majority of items had good discrimination. The correlation coefficient method indicated that most items had a good correlation with the total score, and some items had a strong correlation (≥0.70, P<0.01). Cronbach’s α coefficient indicated that the correlation coefficients of a few items (item 6, item 7, and item 8) were all less than 0.350 after correction, and the Cronbach’s alpha if item deleted (CAID) values increased. Finally, 8 items were removed from the items pool following the criteria mentioned in the methods section above (see Table 1).
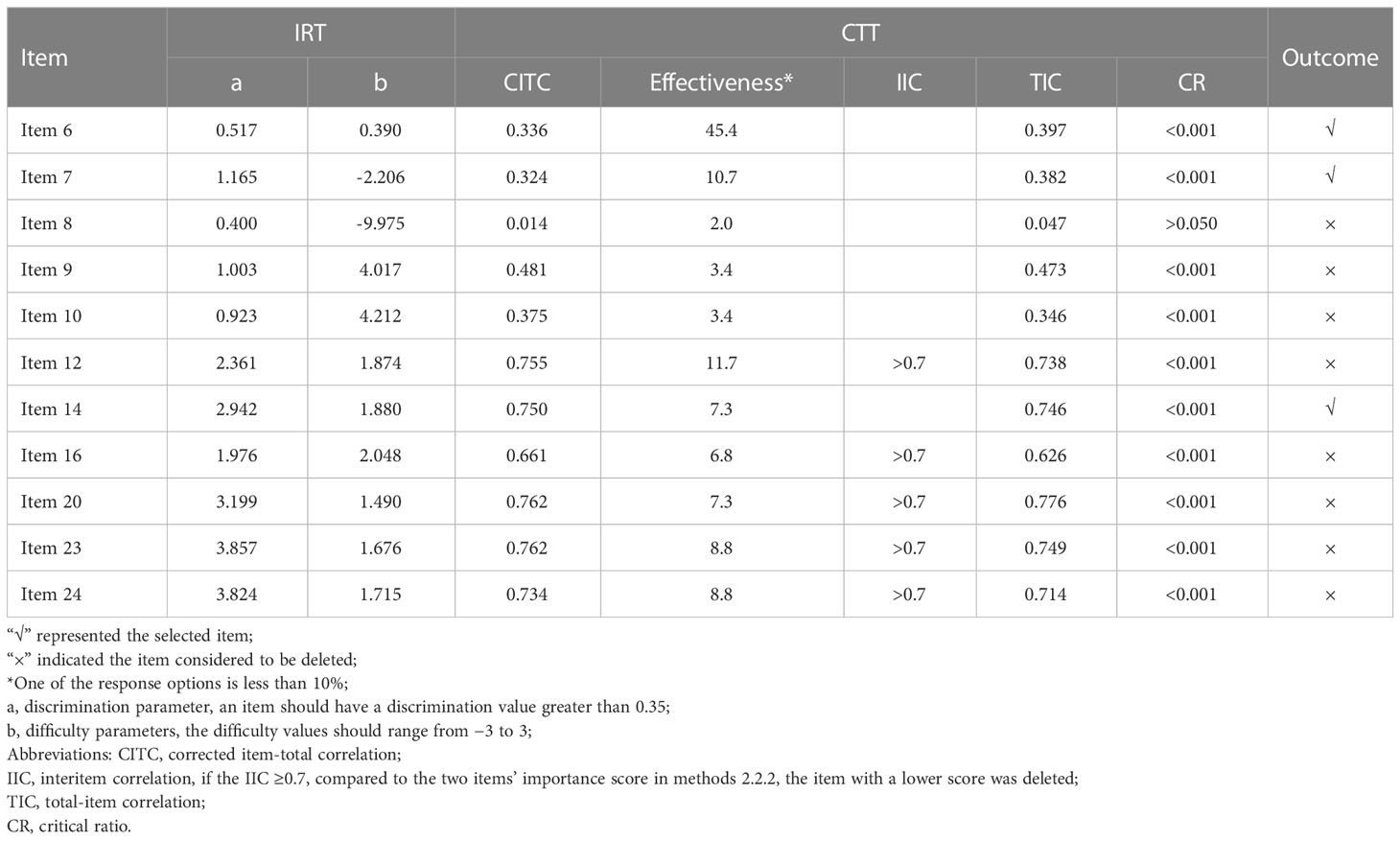
Table 1 Item reduction results using the IRT and CTT.
The parallel analysis and scree plot results show two factors would be extracted. Six items were deleted because they did not load on either of the extracted factors. The EFA was then conducted again on the remaining ten items. The Kaiser-Meyer-Oklin value was 0.842, and Bartlett’s spherical test P< 0.5. Two factors explained 56% of the variance and were named “subjective financial distress” (items 14,15, 18, 19, and 22) and “objective medical burden” (items 1, 2, 3, 4, and 5) (see Table 2). This new 10-item version was then developed, which was named the “Hardship And Recovery with Distress Survey” (HARDS) (see Supplemental Table 4). The total score range was from 10 (highest financial hardship) to 50 (lowest financial hardship). Figure 2 summarizes the adopted stepwise approach.
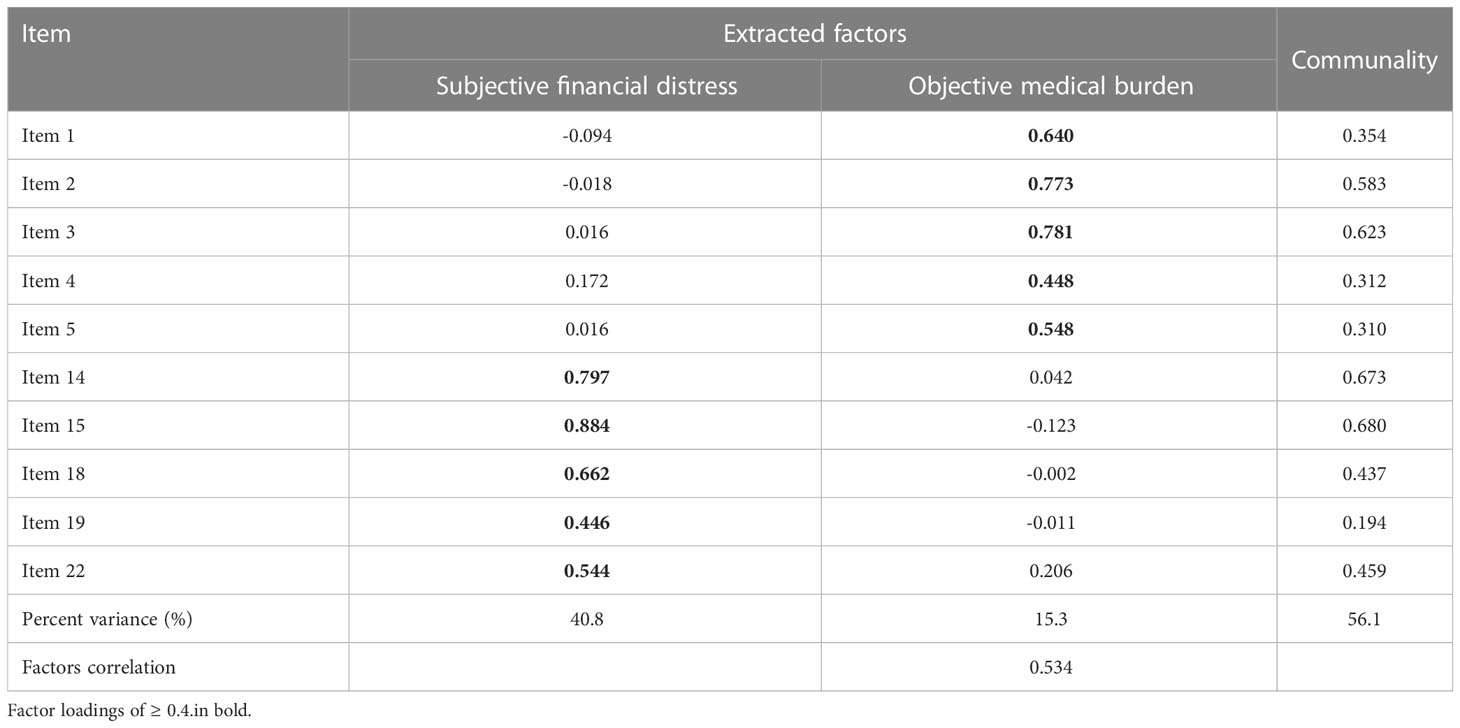
Table 2 Factor loadings of the remaining 10-item HARD using EFA.
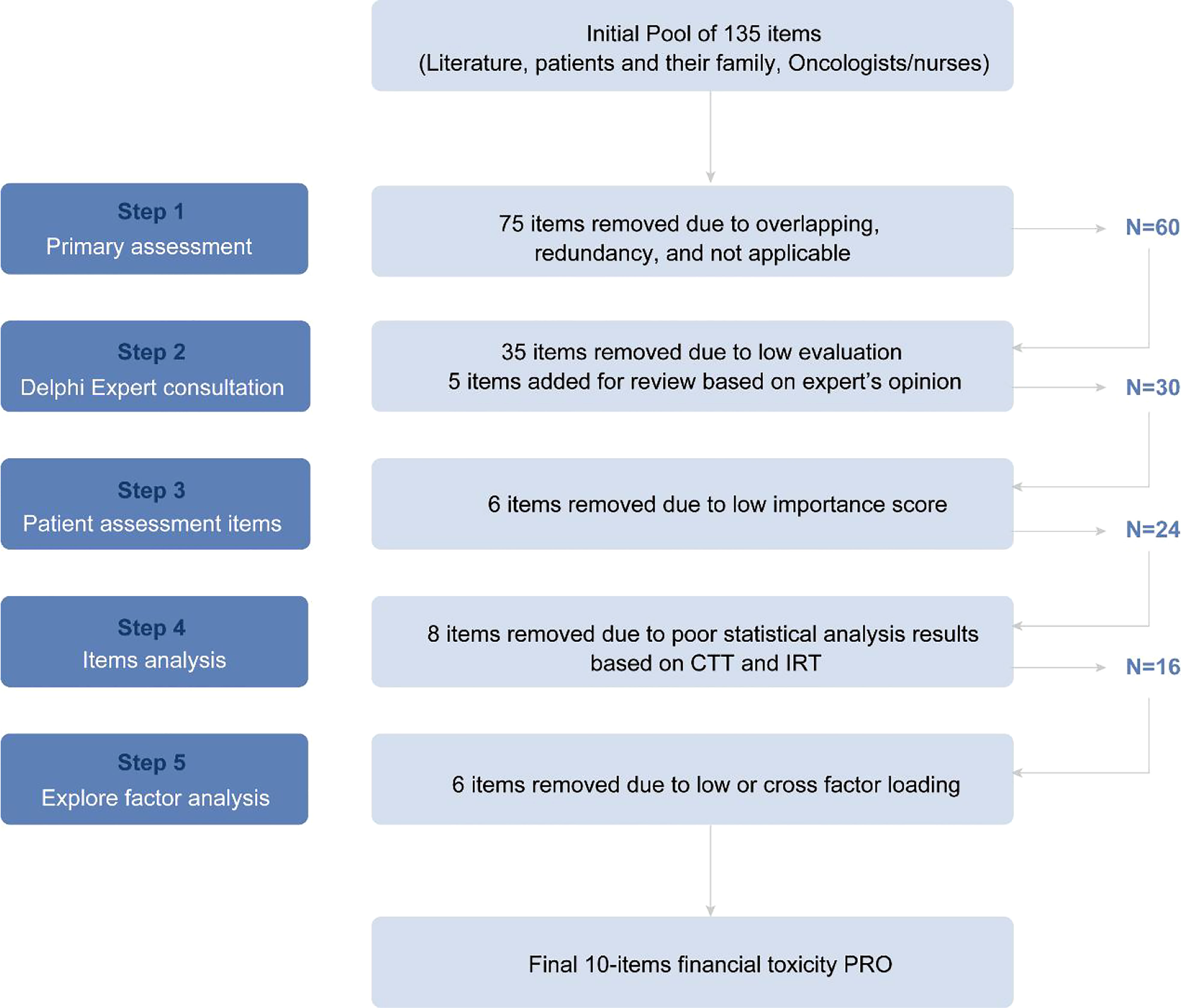
Figure 2 Flow chart of items inclusion and deletion.
The Cronbach’s α for the 10-item instrument was 0.838. The Cronbach’s α for factor 1 and factor 2 were comparable at 0.856 and 0.865, respectively. The test-retest reliability of the measure was 0.909 from a sample size of 23 patients who were assessed twice within 14 days. The result of CITC and CAID were shown Table 3.
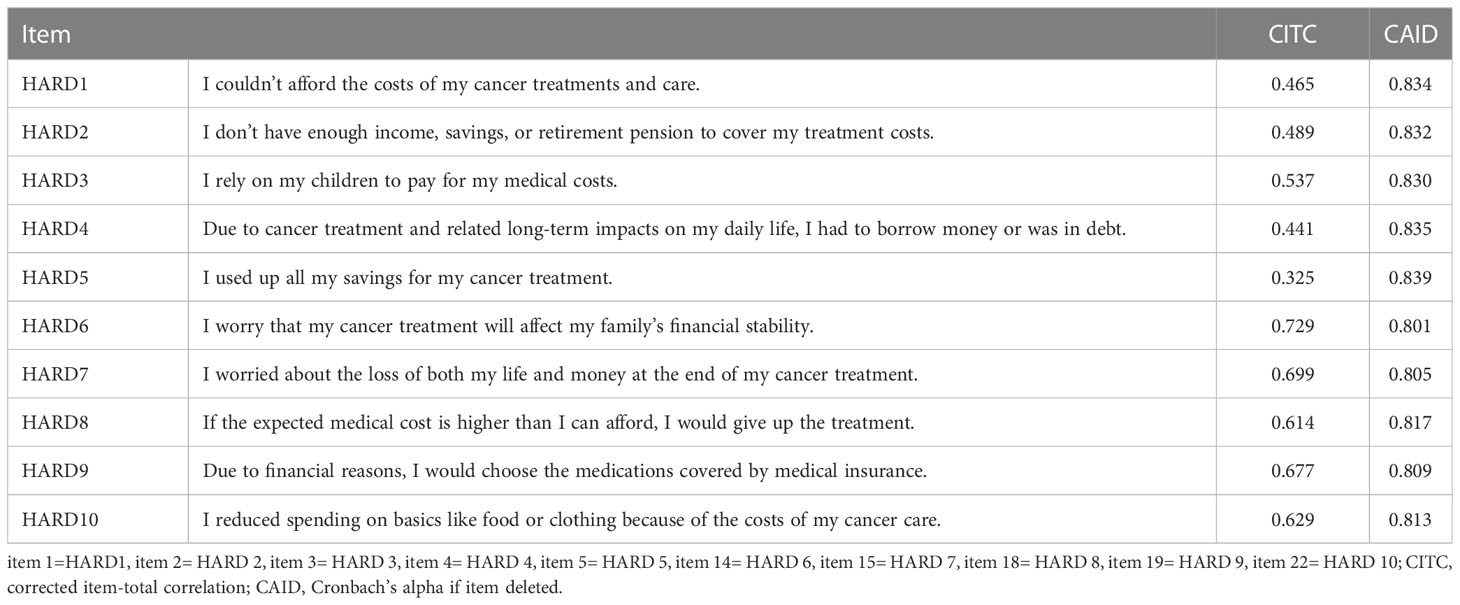
Table 3 Results of the reliability analysis.
The results of CFA showed that the tool had good structural validity; the loading of each factor ranged from 0.548 to 0.884. The corrected model fit indices were ideal (RMSEA=0.075, SRMR=0.041, GFI=0.956, CFI=0.964, TLI=0.949) (see Figure 3). The correlation coefficient between the total score of the COST scale and the HARDS total score of this measuring tool was 0.523 (P<0.01), which indicated that the criterion validity of the HARDS was satisfactory. The AVE of the two factors were 0.555 and 0.558, respectively. The CR value of the two factors were 0.859 and 0.860, respectively.
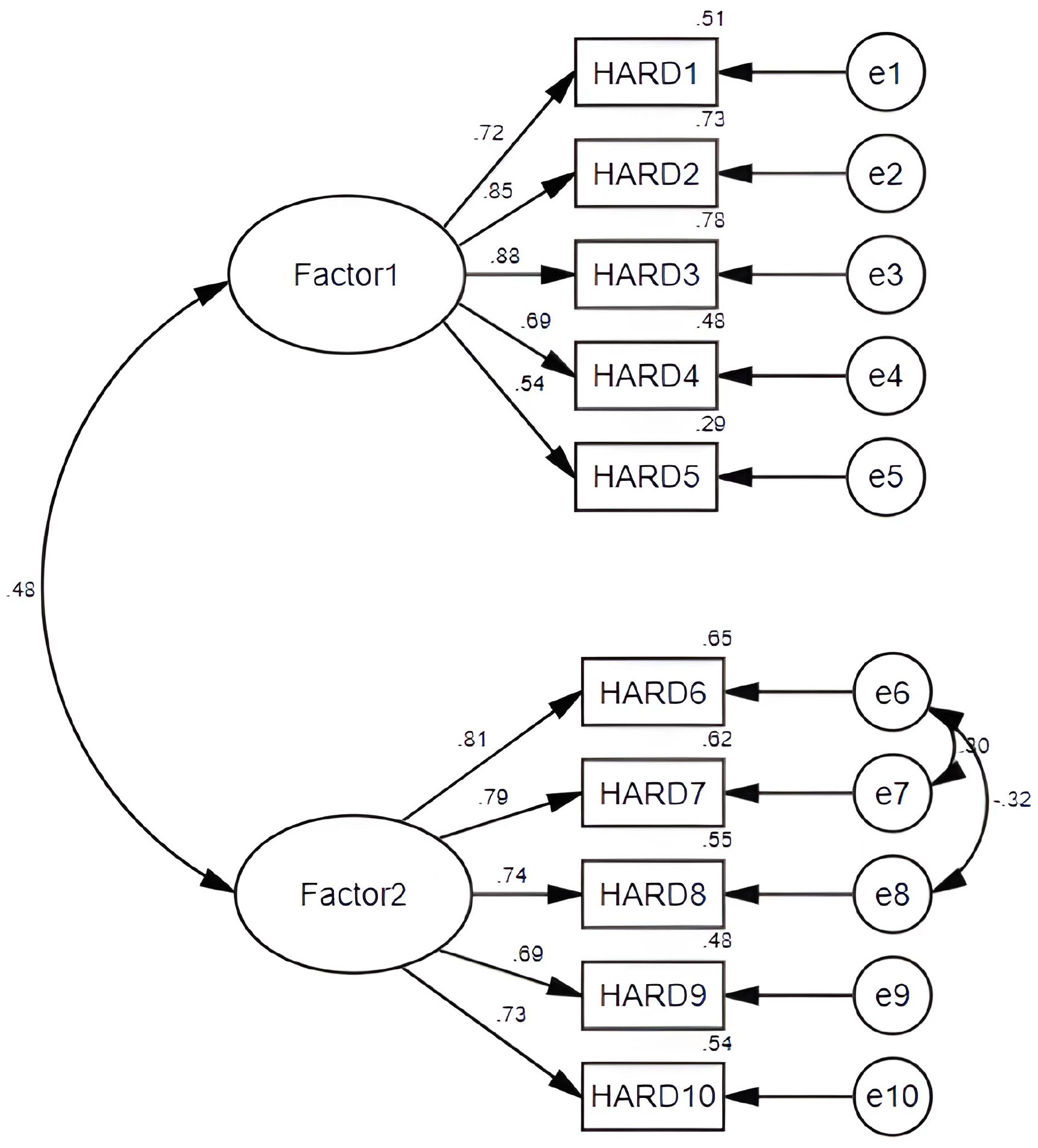
Figure 3 A two-factor model for the HARD from confirmatory factor analysis.
The mean score of the HARDS for financial hardship was 20.4 (standard deviation = 6.4). The ROC analysis results suggested this cut-off score of 18.5 could provide a balance between acceptable levels of sensitivity (0.64) and specificity (0.59). When the sample was stratified based on this cut-off score, 42% of samples were defined as having higher financial hardship.
The influencing factors of high financial hardship included socioeconomic status (i.e., employment, household income, education, and medical insurance type), social support, loneliness, frailty status, cancer site, out-of-pocket costs, and medical decision-making patterns. Higher socioeconomic status of patients was associated with lower financial hardship (OR=0.427, 95%CI:0.326~0.560). Samples with frailty had a higher probability (OR=1.817) of financial hardship than those who were non-frail (see Table 4).
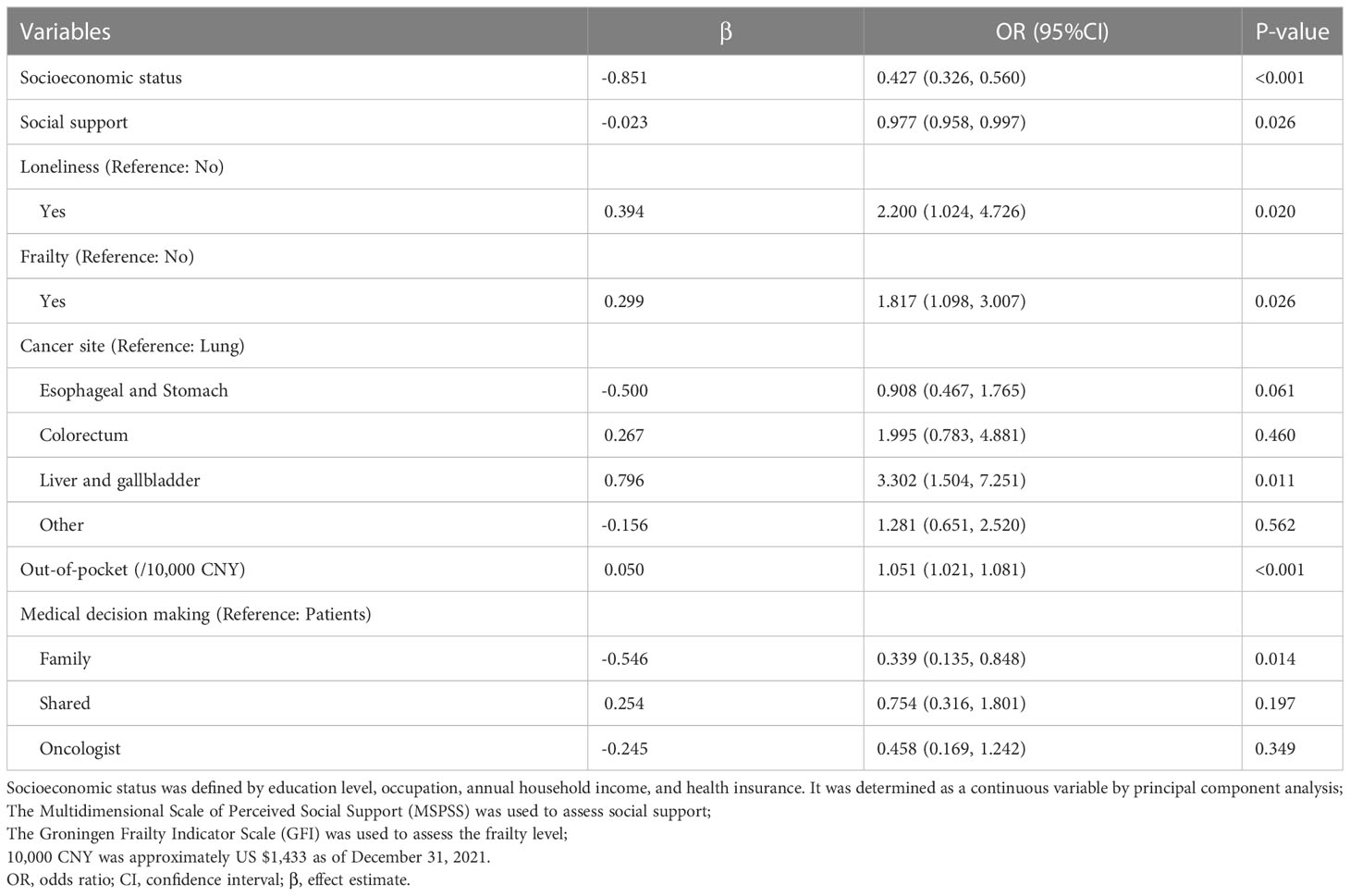
Table 4 Results of Logistic regression analysis (Reference: Lower financial hardship).
The HARDS, containing 10 items, is a new tool for measuring cancer related financial hardship for older patients in China, that takes about 5 minutes per patient to measure. The HARDS captures the subjective financial distress and objective medical burden. The HARDS based on PROM can reflect the specificity of older cancer survivors’ experiences. The collection and use of PROM such as the HARDS can help with medical decision-making, early identification of financial hardships, and improvements to HRQoL and prognosis. In this study, we used the COSMIN checklist to evaluate the methodological quality of studies on the measurement properties of PROM measuring financial hardship for older cancer survivors (29). And the validity and reliability of the HARDS as a screening tool for financial hardship have been tested. We also determined the cut-off score that predicted a poor outcome for HRQoL, as well as features that characterize older survivors with a high level of financial hardship.
Current instruments measuring cancer related financial hardship include the FIT (17), the COST (30), and the Breast Cancer Finances Survey (BCFS) (30, 31). The FIT was designed specifically for head and neck cancer, the COST was designed for patients with advanced cancer, and the BCFS was designed exclusively for breast cancer patients. Applicability of these instruments to other cancer stages and sites may be limited. To our knowledge, the COST is currently the most commonly used validated instrument to measure financial hardship in cancer survivors (31, 32). However, the COST measure has only one family item which is a summary statement (27); thus, the financial hardship on families has not been fully taken into consideration. In this study, cancer-related financial worries and stress among older adults extended into their families, especially those of their adult children. Our instrument assessed financial hardships from the perspectives of both an individual and their family. Therefore, the HARDS captures the family’s financial situation and covers material factors, psychological measures, and coping strategies to comprehensively measure financial hardship.
Like other studies that have developed and validated measures of financial toxicity, our study also uses the COST as the gold standard for criterion validity (17, 18, 33). For example, factor analysis and item reduction were performed on the patients as validity testing. The instrument demonstrated reasonably good psychometric properties, which provide useful information for practical applications. Thus, HARDS is a valid, reliable tool. But one of the job-related items of COST “I am concerned about keeping my job and my income” might be less sensitive to older survivors. In China, the older population in rural and urban areas aged 60 were 175 million and 75 million, respectively, and nearly 70% of older people lived in rural areas (34). Rural residents lack pension support and expect to work in agriculture-related activities until relatively late in their lives. Furthermore, older adults in urban areas usually have retired, so their job and salary were rarely affected due to cancer treatment. Despite deleting this job-related item, the rest of 10 items retained were representative of the COST with a score ranging from 0 to 40. The results still indicated that the newly developed HARDS correlated well with the modified COST.
This study also determined a proposed cut-off score for the HARDS measure. The cut-off score predicted an adverse outcome for HRQoL and categorized the level of high or low financial hardship. Forty-two percent of the patients had a high level of financial hardship in our study. A prior study indicated close to 20% of older adults with advanced cancer experience financial hardship in USA (35). In the USA, most respondents were aged 65, and older adults often had Medicare, while lower-income people were enrolled in Medicaid (36). These insurance programs help them pay for medical services, including hospitalization, prescription drugs, home health care, and hospice care. However, China has implemented a basic medical insurance system, in which UEBMI is mandatory for employees in urban areas, while unemployed residents in urban areas and rural residents are covered by the URRBMI (37). In China, most of the older patients are farmers, and they are a relatively disadvantaged population with low incomes. A previous study indicated that older cancer survivors from rural areas have to bear higher hidden costs of transportation and rent for their homes (27). Moreover, rural residents are covered by URRBMI, which has a lower reimbursement ratio than UEBMI. Thus, the cancer-related financial hardship prevalence in rural patients is higher than in those with pension support and prior non-agricultural employment (38). A considerable proportion of older patients still struggle against financial hardship despite the availability of basic health insurance. There is a gap that needs to be addressed between financial hardship and government assistance (39, 40). Therefore, these medical insurance policies need to be constantly improved to alleviate the burden of cancer-related costs.
The strengths of our study included the integration of qualitative interviews with quantitative findings, and the inclusion of a broad stakeholder group with experts from a diverse, yet significant group of oncology-related fields, patients, and their families. This study shows a comprehensive understanding of older cancer survivors and their family members’ financial hardship.
This study is an original study in the field of cancer survivorship in China that provides evidence for improving the quality of cancer care. The incorporation of financial toxicity assessments into observational research will ensure a patient centered foundation in the evaluation of financial distress, as HARDS is a quick and reproducible measurement that could be used in clinical practice to identify patients early who may be at risk of financial hardship and may benefit most from intervention. Oncology providers (oncologists and nurses) are important agents in patient cancer care experiences, discussions about financial toxicity of cancer care should be initiated by an informed oncologist and managed by the entire healthcare team. The collection and use of the HARDS can help with enhancing shared decision-making between oncologists and patients to reduce costs. Long-term solutions must include policy shifts involving how we set and negotiate anti-cancer prices and insure patients. The HARDS may help increase awareness of patient financial distress and cancer treatment cost sparking discussions among health policy makers and other stakeholders to develop multidisciplinary strategies for mitigating financial toxicity.
Several potential limitations should be considered in interpreting the results of the study. First, the study findings might not be representative of all older cancer patients, as this study did not include individuals who were not admitted to the hospital and did not receive treatment due to severe financial difficulties. Therefore, the level of financial hardship in older populations may be underestimated. Second, the financial toxicity of PROM in China may differ from older cancer survivors in other countries due to social and cultural differences, so the extrapolation of the instrument may be limited. It needs cross-cultural validation and adaption in other eastern countries. Third, this study used a cross-sectional survey in the instrument validation stage, but the trajectory of cancer and medical treatment for survivors is complicated and long-term; thus, a prospective study is needed to determine how financial toxicity changes over time.
In this study, we report the development and validation of the HARDS to measure financial hardship among older cancer survivors in China. This study found that poor quality of life was associated with a higher level of financial hardship, and the severity cut-off score of the new instrument was obtained. Finally, we also identified several influencing factors on higher financial hardship, such as low socioeconomic status, poor social support, loneliness, frailty, high out-of-pocket costs, and more.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
LL: Conceptualization, data curation, software, writing-original draft, and writing–review, and editing. AZ: Writing, data curation, review, software, and editing. MS: Conceptualization, methodology, formal analysis, and writing–review, and editing. XS: Writing–review, and editing. DS: Writing–review, and editing. JC: Writing–review, and editing. NY: Supervision, and writing–review, and editing. All authors contributed to the article and approved the submitted version.
The paper is supported by National Natural Science Foundation of China (Grant No.31900785).
We are grateful to Dr. David T. Eton from Mayo Clinic, Rochester, MN, United States for his kind help in writing–review and editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1151465/full#supplementary-material
1. Zafar SY, Abernethy AP. Financial toxicity, part I: a new name for a growing problem. Oncology (2013) 27(2):80–1:149.
2. Corrigan KL, Fu S, Chen YS, Kaiser K, Roth M, Peterson SK, et al. Financial toxicity impact on younger versus older adults with cancer in the setting of care delivery. Cancer (2022) 128(13):2455–62. doi: 10.1002/cncr.34220
3. Smith GL, Lopez-Olivo MA, Advani PG, Ning MS, Geng Y, Giordano SH, et al. Financial burdens of cancer treatment: A systematic review of risk factors and outcomes. J Natl Compr Canc Netw (2019) 17(10):1184–92. doi: 10.6004/jnccn.2019.7305
4. Chan RJ, Gordon LG, Tan CJ, Chan A, Bradford NK, Yates PA, et al. Relationships between financial toxicity and symptom burden in cancer survivors: A systematic review. J Pain Symptom Manage (2019) 57(3):646–60. doi: 10.1016/j.jpainsymman.2018.12.003
5. Pannier ST, Warner EL, Fowler B, Fair D, Salmon SK, Kirchhoff AC. Age-specific patient navigation preferences among adolescents and young adults with cancer. J Cancer Educ (2019) 34(2):242–51. doi: 10.1007/s13187-017-1294-4
6. Meng Q, Mills A, Wang L, Han Q. What can we learn from china’s health system reform? BMJ (2019) 365:l2349. doi: 10.1136/bmj.l2349
7. Li Y, Zhao Y, Yi D, Wang X, Jiang Y, Wang Y, et al. Differences exist across insurance schemes in China post-consolidation. PloS One (2017) 12(11):e0187100. doi: 10.1371/journal.pone.0187100
8. Xiong X, Zhang Z, Ren J, Zhang J, Pan X, Zhang L, et al. Impact of universal medical insurance system on the accessibility of medical service supply and affordability of patients in China. PloS One (2018) 13(3):e0193273. doi: 10.1371/journal.pone.0187100
9. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
10. Maomao C, He L, Dianqin S, Siyi H, Xinxin Y, Fan Y, et al. Current cancer burden in China: epidemiology, etiology, and prevention. Cancer Biol Med (2022) 19(8):2095–3941. doi: 10.20892/j.issn.2022.0231
11. Jiang H, Zhao M, Tian G, Zhao Z, Ding D, Yin M. Perceived effect of financial risk protection by the urban-rural resident basic medical insurance scheme: a mixed-methods study of rural residents in China. BMJ Open (2021) 11(10):e047699. doi: 10.1136/bmjopen-2020-047699
12. Su M, Lao J, Zhang N, Wang J, Anderson RT, Sun X, et al. Financial hardship in Chinese cancer survivors. Cancer (2020) 126(14):3312–21. doi: 10.1002/cncr.32943
13. Cao M, Li H, Sun D, Chen W. Cancer burden of major cancers in China: A need for sustainable actions. Cancer Commun (2020) 40(5):205–10. doi: 10.1002/cac2.12025
14. He L, Wu H, Li M, Deng X. A qualitative meta-synthesis of the caregiving experiences of adult children providing care for cancer patients in China: implications for multidisciplinary healthcare teams. Health Soc Care Community (2022) 30(6):e3829–42. doi: 10.1111/hsc.14073
15. He L, van Heugten K. Chinese Migrant workers’ care experiences: A model of the mediating roles of filial piety. Qual Health Res (2020) 30(11):1749–61. doi: 10.1177/1049732320925420
16. de Souza JA, Yap BJ, Hlubocky FJ, Wroblewski K, Ratain MJ, Cella D, et al. The development of a financial toxicity patient-reported outcome in cancer: The COST measure: Financial PRO measure in cancer. Cancer (2014) 120(20):3245–53. doi: 10.1002/cncr.28814
17. Hueniken K, Douglas CM, Jethwa AR, Mirshams M, Eng L, Hope A, et al. Measuring financial toxicity incurred after treatment of head and neck cancer: Development and validation of the financial index of toxicity questionnaire. Cancer (2020) 126(17):4042–50. doi: 10.1002/cncr.33032
18. Riva S, Bryce J, De Lorenzo F, Del Campo L, Di Maio M, Efficace F, et al. Development and validation of a patient-reported outcome tool to assess cancer-related financial toxicity in Italy: a protocol. BMJ Open (2019) 9(9):e031485. doi: 10.1002/cncr.33032
19. Riva S, Efficace F, Di Maio M, Bryce J, Del Campo L, De Lorenzo F, et al. A qualitative analysis and development of a conceptual model assessing financial toxicity in cancer patients accessing the universal healthcare system. Support Care Cancer (2021) 29(6):3219–33. doi: 10.1007/s00520-020-05840-z
20. Xu B, Hu L, Cheng Q. A systematic review of financial toxicity among cancer patients in China. Asia Pac J Oncol Nurs (2022) 9(8):100071. doi: 10.1016/j.apjon.2022.04.010
21. Jeon M, Youn N, Kim S. What are the late effects of older gastric cancer survivors? a scoping review. Asia Pac J Oncol Nurs (2022) 9(11):100113. doi: 10.1016/j.apjon.2022.100113
22. Altice CK, Banegas MP, Tucker-Seeley RD, Yabroff KR. Financial hardships experienced by cancer survivors: a systematic review. J Natl Cancer Institute (2017) 109(2):djw205. doi: 10.1093/jnci/djw205
23. Gagnier JJ, Lai J, Mokkink LB, Terwee CB. COSMIN reporting guideline for studies on measurement properties of patient-reported outcome measures. Qual Life Res (2021) 30(8):2197–218. doi: 10.1007/s11136-021-02822-4
24. Liu L, Cao Y, Su M, Zhang J, Miao Y, Yao N. Financial toxicity among older cancer survivors in China: a qualitative study of oncology providers’ perceptions and practices. Support Care Cancer (2022) 30(11):9433–40. doi: 10.1007/s00520-022-07303-z
25. Su M, Yao N, Liu L, Cheng J, Sun X, Yue H, et al. Older cancer survivors living with financial hardship in China: a qualitative study of family perspectives. Psycho-Oncology (2022) 31(4):661–70. doi: 10.1002/pon.5854
26. Hu Q, Qin Z, Zhan M, Wu B, Chen Z, Xu T. Development of a trigger tool for the detection of adverse drug events in Chinese geriatric inpatients using the Delphi method. Int J Clin Pharm (2019) 41(5):1174–83. doi: 10.1007/s11096-019-00871-x
27. Dar MA, Chauhan R, Murti K, Trivedi V, Dhingra S. Development and validation of subjective financial distress questionnaire (SFDQ): a patient reported outcome measure for assessment of financial toxicity among radiation oncology patients. Front Oncol (2021) 11:819313. doi: 10.3389/fonc.2021.819313
28. Lam KH, Kwa VIH. Validity of the PROMIS-10 global health assessed by telephone and on paper in minor stroke and transient ischaemic attack in the Netherlands. BMJ Open (2018) 8(7):e019919. doi: 10.1136/bmjopen-2017-019919
29. Prinsen CAC, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet HCW, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res (2018) 27(5):1147–57. doi: 10.1007/s11136-018-1798-3
30. de Souza JA, Yap BJ, Wroblewski K, Blinder V, Araújo FS, Hlubocky FJ, et al. Measuring financial toxicity as a clinically relevant patient-reported outcome: The validation of the COmprehensive score for financial toxicity (COST). Cancer (2017) 123(3):476–84. doi: 10.1002/cncr.30369
31. Desai A, Gyawali B. Financial toxicity of cancer treatment: Moving the discussion from acknowledgement of the problem to identifying solutions. EClinicalMedicine (2020) 20:100269. doi: 10.1016/j.eclinm.2020.100269
32. Witte J, Mehlis K, Surmann B, Lingnau R, Damm O, Greiner W, et al. Methods for measuring financial toxicity after cancer diagnosis and treatment: a systematic review and its implications. Ann Oncol (2019) 30(7):1061–70. doi: 10.1093/annonc/mdz140
33. Ripamonti CI, Chiesi F, Di Pede P, Guglielmo M, Toffolatti L, Gangeri L, et al. The validation of the Italian version of the COmprehensive score for financial toxicity (COST). Support Care Cancer (2020) 28(9):4477–85. doi: 10.1007/s00520-019-05286-y
34. Chen X, Chen J, Gong J, Jia Y, Meng Q, Wang G, et al. Challenges faced by elderly care and outstanding problems in elderly care services in rural China. J China Agric Univ (Soc Sci Ed) (2021) 38(04):64–77. doi: 10.13240/j.cnki.caujsse.2021.04.005
35. Arastu A, Patel A, Mohile SG, Ciminelli J, Kaushik R, Wells M, et al. Assessment of financial toxicity among older adults with advanced cancer. JAMA Netw Open (2020) 3(12):e2025810. doi: 10.1001/jamanetworkopen.2020.25810
36. Cochran AL, McDonald NC, Prunkl L, Vinella-Brusher E, Wang J, Oluyede L, et al. Transportation barriers to care among frequent health care users during the COVID pandemic. BMC Public Health (2022) 22:1783. doi: 10.1186/s12889-022-14149-x
37. Weng L, Hu Y, Sun Z, Yu C, Guo Y, Pei P, et al. Place of death and phenomenon of going home to die in Chinese adults: A prospective cohort study. Lancet Reg Health West Pac (2022) 18:100301. doi: 10.1016/j.lanwpc.2021.100301
38. Su M, Zhang N, Cai Y, Wang J, Anderson R, Yao N, et al. Work and income changes after cancer in rural China: a cross-sectional survey. Cancer Med (2019) 8(18):7859–68. doi: 10.1016/j.lanwpc.2021.100301
39. Smith SK, Nicolla J, Zafar SY. Bridging the gap between financial distress and available resources for patients with cancer: a qualitative study. J Oncol Pract (2014) 10(5):e368–372. doi: 10.1200/JOP.2013.001342
Keywords: older cancer survivors, health outcome, patient-reported outcome measure, financial hardship, financial toxicity
Citation: Liu L, Zhang A, Su M, Sun X, Shao D, Cheng J and Yao NA (2023) The development and validation of a patient-reported outcome measure to assess financial hardship among older cancer survivors in China: hardship and recovery with distress survey. Front. Oncol. 13:1151465. doi: 10.3389/fonc.2023.1151465
Received: 26 January 2023; Accepted: 28 March 2023;
Published: 21 April 2023.
Edited by:
Helen Parsons, University of Minnesota Twin Cities, United StatesReviewed by:
Anao Zhang, University of Michigan, United StatesCopyright © 2023 Liu, Zhang, Su, Sun, Shao, Cheng and Yao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mingzhu Su, c3VtaW5nemh1QG1haWwuc2R1LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.