 Cinara Sacomori
Cinara Sacomori Mónica Belén Martinez-Mardones2,3
Mónica Belén Martinez-Mardones2,3
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
GENERAL COMMENTARY article
Front. Oncol. , 25 April 2023
Sec. Surgical Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1150181
A Commentary on
Functional bowel complaints and the impact on quality of life after colorectal cancer surgery in the elderly
by Ketelaers SHJ, van Heinsbergen M, Orsini RG, Vogelaar FJ, Konsten JLM, Nieuwenhuijzen GAP, Rutten HJT, Burger JWA and Bloemen JG (2022) Front. Oncol.12:832377. doi: 10.3389/fonc.2022.832377
We would like to congratulate Ketelaers et al. (2022) (1) on their article regarding prevalence of low anterior resection syndrome (LARS) complaints and the impact on quality of life in the elderly after colorectal cancer surgery. Their article concerns a population-based study of 1623 older adults who underwent colorectal cancer surgery with primary anastomosis. The study showed that, for rectal cancer patients, younger patients (<70 years) had a high probability to develop major LARS compared to older patients (≥70 years), with a prevalence of 57.3% and 40.6%, respectively, OR= 0.63 (p=0.04). For colon cancer patients, the study showed the prevalence of major LARS symptoms as similar between younger and older patients: 20.4% and 22.2%, respectively. In addition, patients with major LARS presented significantly impaired quality of life (1). This study used the LARS score questionnaire, which is a very popular tool among clinicians and researchers.
LARS is usually defined as a bowel function disorder after rectal resection impairing quality of life. A recently published consensus of experts and patients concluded that, to meet the definition of LARS, a patient must have had a sphincter-preserving rectal anterior resection and experience at least one of the following symptoms with one consequence. Symptoms included: variable/unpredictable bowel function, altered stool consistency, increased stool frequency, repeated painful stools, emptying difficulties, urgency, incontinence, and soiling. Possible consequences include: toilet dependence, preoccupation with bowel function, dissatisfaction with bowels, strategies and compromises, and impact on mental and emotional wellbeing, social and daily activities, relationships and intimacy, roles, commitments and responsibilities (2).
Recently, the term “LARS” has become more widely used, and studies have reported LARS-like symptoms not only among rectal cancer patients who underwent low anterior resection (LAR) (3, 4), but also among patients with sigmoid (5, 6), colon (7), and ovarian (8) cancers, as well as in non-cancer non-operative (5) patients. The Ketelaers et al. (2022) (1) study included patients with and without LAR. The previously mentioned studies have in common the use of the LARS score questionnaire and the detection of some degree of LARS among participants. The fact that the LARS score identifies people who have not undergone a LAR as presenting LARS suggests the questionnaire may lack specificity.
We do not agree with the use of the term “LARS” in reference to patients that have not been submitted to the specific surgical procedure, the LAR. We believe that doing so will create confusion among clinicians and researchers about what is being assessed or reported. Is it possible to refer to “LARS” (major, minor) when patients have not undergone a LAR? Thus, the aim of this commentary is to discuss the most appropriate terminology when reporting bowel/anorectal symptoms, when using the LARS score, among people who did not experience a LAR.
The LARS score was proposed by Emmertsen and Laurberg (2012) (9), and submitted for international validation (10), with proposed normative data (11). A classification has been recommended for the total score: no LARS (0–20 points), minor LARS (21–29 points), and “major LARS” (30–42 points) (11). LARS score is a short and easy to apply/understand questionnaire. However, there is some discussion on its accuracy. Some studies showed a high prevalence of LARS among the general population, i.e., with preserved rectum, indicating low specificity but high sensitivity of the instrument (2).
It is worth noting that the items in the LARS score assess some aspects of bowel function that can feasibly be applied to many other health conditions, not only after a patient has undergone a LAR. Thus, there is a need for more studies on the validity of the LARS score in people with other health conditions. We agree with the use of the LARS score with other populations to assess bowel symptoms, but we do not agree with indicating that those people who have not undergone a LAR as presenting LARS (major, minor); because the latter is the diagnosis of a condition that is traditionally only associated with the LAR procedure.
There are other short questionnaires on the topic, such as the Wexner and Vaisey scales (Table 1). But these scales do not assess urgency, changes in the frequency of defecation, or the amount of accidental bowel leakage (soiling, moderate, or great amount of leakage), which are very common symptoms among colorectal cancer patients. The International Consultation on Incontinence Questionnaire Bowel Module (ICIQ-B) is a more complete questionnaire for the assessment of bowel function (12), including all the relevant aspects, but it is much longer than the previously mentioned scales.
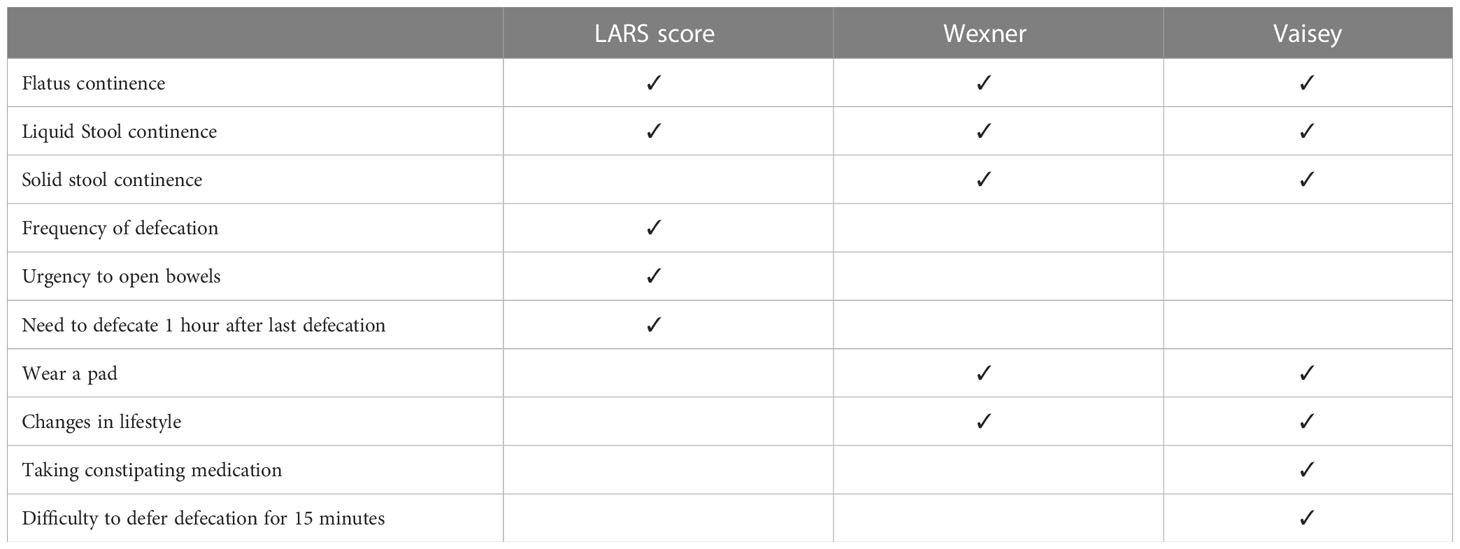
Table 1 Comparison of items of LARS score, Wexner and Vaisey.
For research purposes, we recommend the more comprehensive questionnaires (ICIQ-B, the Bowel Function Instrument of the Memorial Sloan Kettering Cancer Centre) that will assess more dimensions of the construct. For clinical purposes, the LARS score combined with other fecal incontinence scales (e.g., Wexner, Vaisey) and clinical assessment might be more feasible. However, we recommend interpreting only individual and general scores of the LARS score questionnaire to determine bowel/anorectal symptoms. The use of the classification of LARS (minor, major) should be restricted to patients who have undergone a LAR.
In addition, there is a need to standardize terminology to systematically assess and report symptoms, signs, and dysfunctions related to anorectal/bowel dysfunctions. In this effort, the International Continence Society (2019) proposed a classification of anorectal dysfunctions for males (13) and females (14) considering symptoms, signs, examination, and any relevant diagnostic investigations. In general, symptoms are classified as: anorectal incontinence (gas and fecal, liquid or solid), anorectal sensory symptoms (rectal hyposensitivity, rectal hypersensitivity), anorectal storage symptoms (increased frequency, urgency), defecatory or post-defecatory symptoms (constipation, feeling of incomplete evacuation, straining, manual defecatory assistance), anorectal pain, anorectal sexual dysfunction, miscellaneous, and anorectal prolapse (13, 14).
Meanwhile, the International Classification of Functioning, Disability and Health (ICF) terminology classifies these functions at category b5 (functions of the digestive, metabolic, and endocrine systems), subcategory b525 which is identified as defecation functions (functions of elimination, fecal consistency, frequency of defecation; fecal continence, flatulence; impairments such as constipation, diarrhea, watery stool and anal sphincter incompetence or incontinence).
In conclusion, a better definition or use of standardized terminology to describe anorectal/bowel function is imperative, mainly in topics that require interdisciplinary approaches (gastroenterologists, coloproctologists, surgeons, oncologists, nurses, and pelvic floor physiotherapists, among others). Interdisciplinary and patient-centered approaches as the consensus on the LARS definition, by Keane et al. (2020) (2), greatly contribute to the development of better care practices and comprehension of the LARS and other anorectal/bowel symptoms and dysfunctions.
CS proposed the idea and wrote the manuscript. MM-M, LL and LS revised and contributed to the manuscript. All authors contributed to the article and approved the submitted version.
Fondo Nacional de Desarrollo Científico y Tecnológico FONDECYT INICIACIÓN PROJECT number 11191016, CONICYT, Government of Chile, Santiago de Chile.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ketelaers SHJ, van Heinsbergen M, Orsini RG, Vogelaar FJ, Konsten JLM, Nieuwenhuijzen GAP, et al. Functional bowel complaints and the impact on quality of life after colorectal cancer surgery in the elderly. Front Oncol (2022) 12:832377. doi: 10.3389/fonc.2022.832377
2. Keane C, Fearnhead NS, Bordeianou LG, Christensen P, Basany EE, Laurberg S, et al. International consensus definition of low anterior resection syndrome. Dis Colon Rectum (2020) 3:274–84. doi: 10.1097/DCR.0000000000001583
3. Christensen P, Baeten C IM, Espín-Basany E, Martellucci J, Nugent KP, Zerbib F, et al. Management guidelines for low anterior resection syndrome – the MANUEL project. Color Dis (2021) 23(2):461–75. doi: 10.1111/codi.15517
4. Trenti L, Galvez A, Biondo S, Solis A, Vallribea-Valls F, Espin-Basany E, et al. Quality of life and anterior resection syndrome after surgery for mid to low rectal cancer: A cross-sectional study. Eur J Surg Oncol (2018) 44(7):1031–9. doi: 10.1016/j.ejso.2018.03.025
5. Keane C, O’Grady G, Bissett I, Woodfield J. Comparison of bowel dysfunction between colorectal cancer survivors and a non-operative non-cancer control group. Color Dis (2020) 22(7):806–13. doi: 10.1111/codi.14966
6. van Heinsbergen M, Janssen-Heijnen ML, Leijtens JW, Slooter GD, Konsten JL. Bowel dysfunction after sigmoid resection underestimated: Multicentre study on quality of life after surgery for carcinoma of the rectum and sigmoid. Eur J Surg Oncol (2018) 44(8):1261–7. doi: 10.1016/j.ejso.2018.05.003
7. van Heinsbergen M, den Haan N, Maaskant-Braat AJ, Melenhorst J, Belgers EH, Leijtens JW, et al. Functional bowel complaints and quality of life after surgery for colon cancer: Prevalence and predictive factors. Color Dis (2020) 22(2):136–45. doi: 10.1111/codi.14818
8. Yasin I, Saeed Usmani A, Mohsin J, Bin AR, Kahlid N, Syed AA. Prevalence and risk factors of low anterior resection syndrome in epithelial ovarian cancer surgery. Cureus (2022) 14(3):e23180. doi: 10.7759/cureus.23180
9. Emmertsen J, Laurberg K. Low anterior resection syndrome score: Development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg (2012) 255(5):922–8. doi: 10.1097/SLA.0b013e31824f1c21
10. Juul T, Ahlberg M, Biondo S, Emmertsen KJ, Espin E, Jimenez LM, et al. International validation of the low anterior resection syndrome score. Ann Surg (2014) 259(4):728–34. doi: 10.1097/SLA.0b013e31828fac0b
11. Juul T, Elfeki H, Christensen P, Laurberg S, Emmertsen KJ, Bager P. Normative data for the low anterior resection syndrome score (LARS score). Ann Surg (2019) 269(6):1124–8. doi: 10.1097/SLA.0000000000002750
12. Cotterill N, Norton C, Avery KNL, Abrams P, Donovan JL. Psychometric evaluation of a new patient-completed questionnaire for evaluating anal incontinence symptoms and impact on quality of life: the ICIQ-b. Dis Colon Rectum (2011) 54(10):1235–50. doi: 10.1097/DCR.0b013e3182272128
13. D’Ancona C, Haylen B, Oelke M, Abranches-Monteiro L, Arnold E, Goldman H, et al. The international continence society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol Urodyn (2019) 38(2):433–77. doi: 10.1002/nau.23897
Keywords: low anterior resection syndrome (LARS), colorectal cancer, questionnaire, anorectal dysfunction, bowel symptoms
Citation: Sacomori C, Martinez-Mardones MB, Lorca LA and Solé LI (2023) Commentary: Functional bowel complaints and the impact on quality of life after colorectal cancer surgery in the elderly. Front. Oncol. 13:1150181. doi: 10.3389/fonc.2023.1150181
Received: 09 March 2023; Accepted: 13 April 2023;
Published: 25 April 2023.
Edited by:
Panagiotis Lainas, Hôpital Antoine-Béclère, FranceReviewed by:
Michael Lim, York and Scarborough Teaching Hospitals, United KingdomCopyright © 2023 Sacomori, Martinez-Mardones, Lorca and Solé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cinara Sacomori, Y3NhY29tb3JpQHVkZC5jbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.