 Rahel Kasteler
Rahel Kasteler
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 02 May 2023
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1150166
This article is part of the Research Topic Late Effects of Pediatric, Adolescent, and Young Adult Brain Tumor Survivors View all 5 articles
Introduction: Survival of children and adolescents diagnosed with central nervous system (CNS) tumors massively improved over the last decades due to better diagnostics, treatment, and supportive care. However, morbidity is still the highest of all cancer entities in this age group with neurocognitive late-effects being one of the most severe.
Aim: With this systematic review, we aim to summarize interventions designed to prevent or improve neurocognitive late-effects in CNS tumor patients.
Method: We searched PubMed on August 16th 2022 and included publications studying interventions for neurocognitive late-effects in pediatric and adolescent patients and survivors diagnosed with a CNS tumor. We included any form of neurocognitive intervention during treatment or following treatment completion. We considered all types of studies except for expert opinions and case reports.
Results: The literature search resulted in 735 publications. We included 43 publications in the full text screening and 14 met our inclusion criteria. Of those, two assessed the impact of pharmacological interventions, three of exercise interventions, five of online cognitive training, and four assessed behavioral interventions. Different neuropsychological test batteries and imaging were used to measure the impact of the respective interventions. Most studies showed a positive impact of the interventions in single to several of the subtests used.
Conclusion: We found several intervention studies indicating improvement of neurocognitive problems in children and adolescent CNS tumor survivors. In this population exercise interventions or online cognitive training might mitigate or improve neurocognitive late-effects.
Improvement in diagnostics, treatment, and supportive care of pediatric and adolescent central nervous system (CNS) tumor patients led to an increase in survival over the last decades (1, 2). Morbidity in pediatric, adolescent and adult CNS tumor survivors is still very high compared to other cancer entities (3–5). This is owed to the location of the cancer itself and to the severity of the treatment modalities, including a combination of chemotherapy, neurosurgery and radiotherapy to the brain (6). Neurocognitive late-effects are commonly reported to be of the most severe ones and can impact long-term development and impair life goals such as education, employment or independence (3, 7). Thus, interventions to mitigate neurocognitive late-effects in CNS tumor survivors are urgently needed. With this systematic review, we aim to summarize interventions designed to improve neurocognitive late-effects in pediatric or adolescent CNS tumor patients or survivors.
We performed this review according to the PRISMA guidelines for reporting systematic reviews and meta-analyses (8).
We conducted a systematic literature search in PubMed on August 16th 2022. We did not restrict the search for date of publication or language. We built the search strategy around six concepts according to the PICO framework (Supplementary Table 1) (9). We identified MeSH terms and free text words for each concept, which we finally combined. For the population of interest, we included the concepts of “central nervous system tumors” (including specific types of CNS tumors but also broad terms), “children and adolescents”, “survivors” and “patients”. For the outcome, we chose terms related to “neurocognition” and “interventions”. For each review article identified with our search, we screened the reference list for relevant original articles.
To be included in this review, the studies had to report on cancer patients or survivors who were diagnosed with a CNS tumor during childhood or adolescence, and who received any form of neurocognitive intervention during treatment or following treatment completion. For a study cohort to be considered “children or adolescents”, at least 75% of participants had to be aged less than 18 years at the time of the cancer diagnosis. We excluded studies that did not fulfil the inclusion criteria, case reports, case series (n ≤ 14), commentaries, editorial letters, poster abstracts and review articles.
The primary outcome of this review was to describe neurocognitive interventions applied in children and adolescents diagnosed with CNS tumors. The impact of the neurocognitive interventions on neurocognition was the secondary outcome.
Two reviewers (MO and KS) screened all titles and abstracts separately and excluded those not fulfilling the inclusion criteria. Any disagreements were discussed and resolved by a third reviewer (RK). Two other reviewers (RK and PF) independently checked all retrieved full texts for adherence. Disagreement was resolved by a third reviewer (MO). Data from the eligible studies were extracted to a standard sheet including the first author, year of publication, patients’ age at diagnosis, sample size, study design, type of neurocognitive intervention, and the impact of the intervention on neurocognition, if reported. We summarized the neurocognitive interventions thematically. We assessed the quality, relevance and reliability of each included study by using the appropriate critical appraisal tool from the Joanna Briggs Institute (10), including the checklists for randomized controlled trials and quasi-experimental studies (Supplementary Table 2). Since these tools do not use any categorization, we made a classification with three categories. If all criteria of the respective checklist were fulfilled, we assigned the study to “Quality 1”. If a controlled trial was not truly randomized or did not use a crossover design to overcome differences in study group characteristics, we assigned the study to “Quality 2”. If a quasi-experimental study had no control group, the study was assigned to “Quality 2”. If an additional point from the checklist for both types of studies was insufficiently covered, we assigned the study to “Quality 3”.
Of 735 potentially relevant publications resulting from our literature search, we excluded 692 publications after title and abstract screening and included 43 for full text screening. Fourteen publications met our inclusion criteria (Figure 1 and Table 1), 12 did not report on pediatric brain tumors, two were on adult patients or mixed populations only, four reported on other outcomes, and 11 were the wrong study designs (e.g. reviews). Regarding the patient population, most studies did not reflect the typical distribution of pediatric and adolescent CNS tumors but described selected groups of patients or survivors. Astrocytoma, the most frequent cancer type often accounted for a small proportion only. Medulloblastoma was the most frequent diagnosis reported followed by ependymoma. Among the 14 included studies, only two were double-blind, placebo controlled randomized controlled trials (RCTs) (11, 12), one of them with crossover design (11). Three studies were not blinded RCTs (13–15), one of them had a crossover design (14). Four studies had a quasi-randomized controlled crossover design (16–19), and two studies were controlled intervention trials (20, 21). Three studies were single-arm intervention trials without a control-group (22–24). In the quality assessment only one study met all quality criteria and was thus graded Quality 1 (12). Three studies were categorized as quasi-experimental studies due to lack of control groups (22–24) and were rated Quality 2 as they met most quality criteria. The remaining studies were rated Quality 3 because additional quality criteria were not met or not reported (Table 1). Even though in most included studies neuropsychological tests were performed to assess the outcomes, the test batteries and subtests used were different. Memory was assessed by Automated Working Memory Assessment (AWMA) (22), Cambridge Neuropsychological Test Automated Battery (CANTAB) (17–19), Children’s Auditory Verbal Learning Test-2 (CAVLT-2) (11), List Sorting Working Memory (LSWM) (11, 15), Picture Sequence Memory Test (PSM) from the NIH toolbox (11, 15), Rey Auditory Verbal Learning Test (RAVLT) (11, 14), Wechsler Intelligence Scale for Children (WISC-III/IV) (12, 14, 20), or Wide Range Assessment of Memory and Learning (WRAML-2) (20, 23). Processing speed and attention was assessed mainly by the CANTAB test battery (11, 18, 19). Other tests used to assess processing speed were WISC IV (14, 23), mean reaction time on correct answers on Attention Network Tasks (ANT) (12), or Pattern Comparison Processing Speed Test from the NIH toolbox (15). Other tests used to assess attention were Conners Continuous Performance Test (CPT II) (14, 23), Map Mission (14), visual scanning from Dellis-Kaplan Executive Function Test (D-KEFS) (14), or ANT (12). Executive functioning was assessed by Behavior Rating Inventory of Executive Function (BRIEF) (24), D-KEFS (14), or Flanker Inhibitory Control and Attention Test from the NIH toolbox (15). Two studies used imaging findings to assess the impact of the intervention (18, 19).
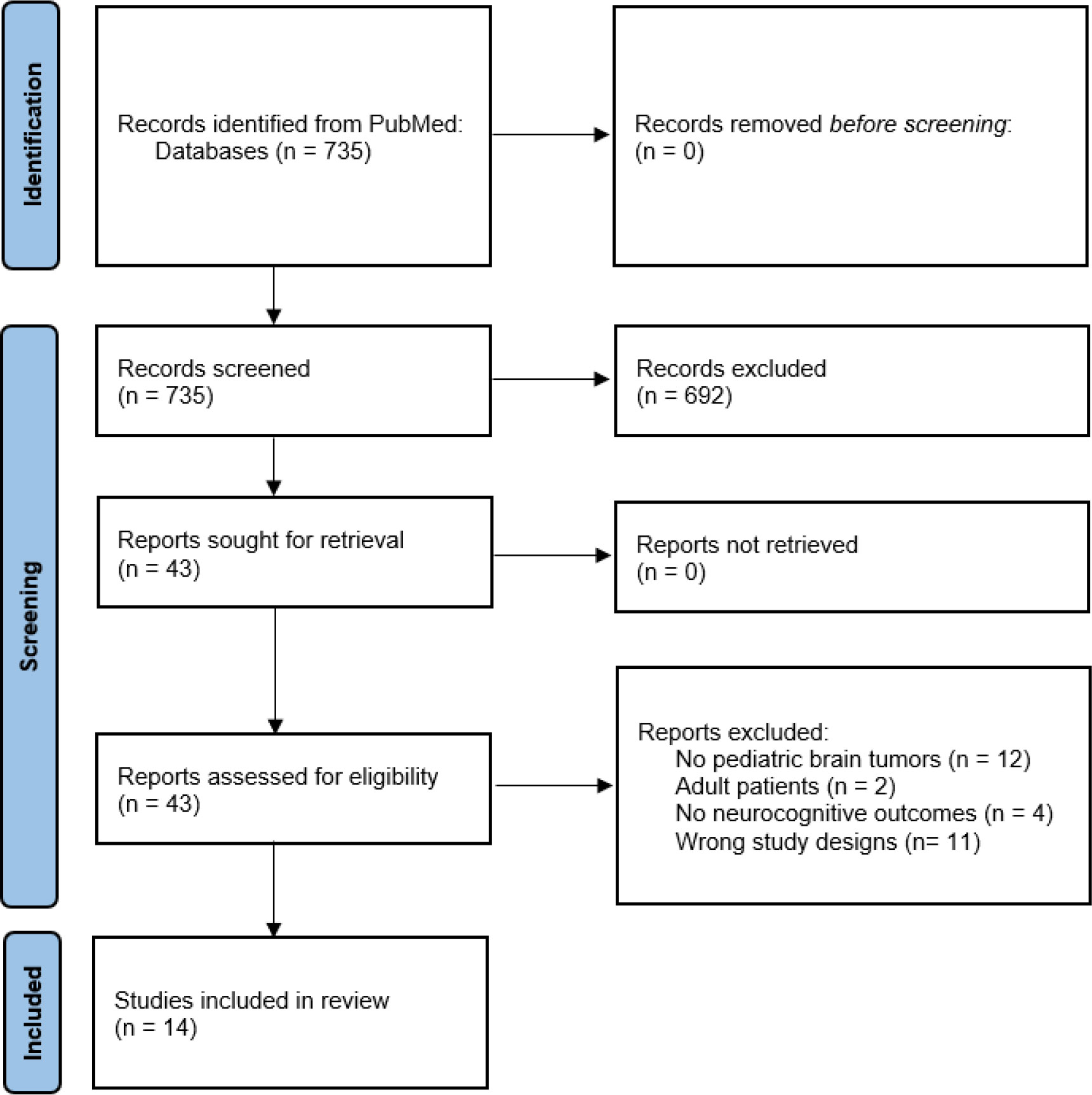
Figure 1 PRISMA 2020 flow diagram for systematic review.
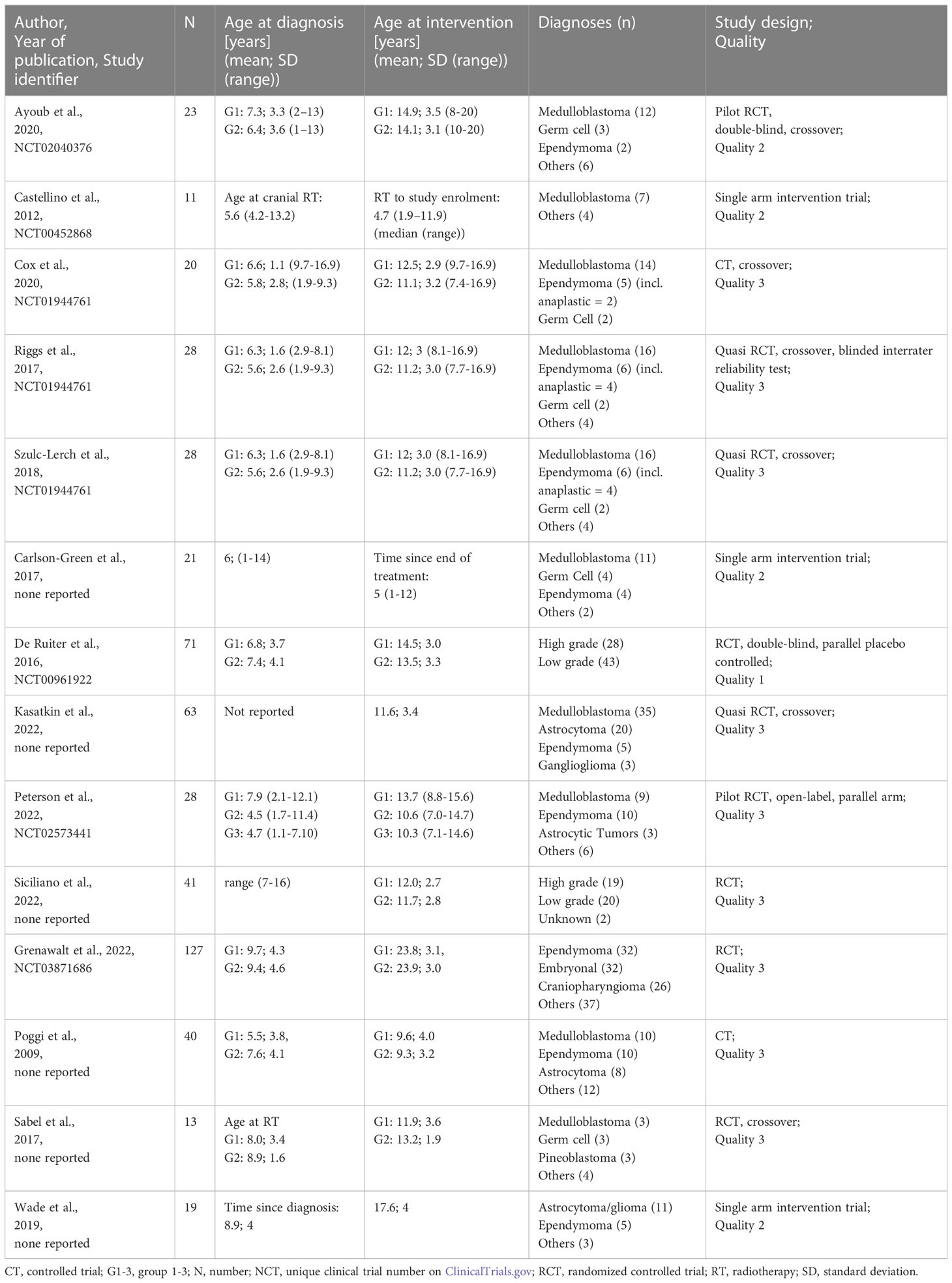
Table 1 Study characteristics of included publications.
The 14 included publications studied different types of interventions to prevent or improve neurocognitive late-effects in children or adolescents diagnosed with CNS tumors. The reported interventions can be divided into pharmacological interventions (11, 23), exercise interventions (16, 18, 19), online cognitive training (12, 15, 17, 20, 22), and behavioral interventions (13, 14, 21, 24). The intervention and outcomes are summarized in Table 2.
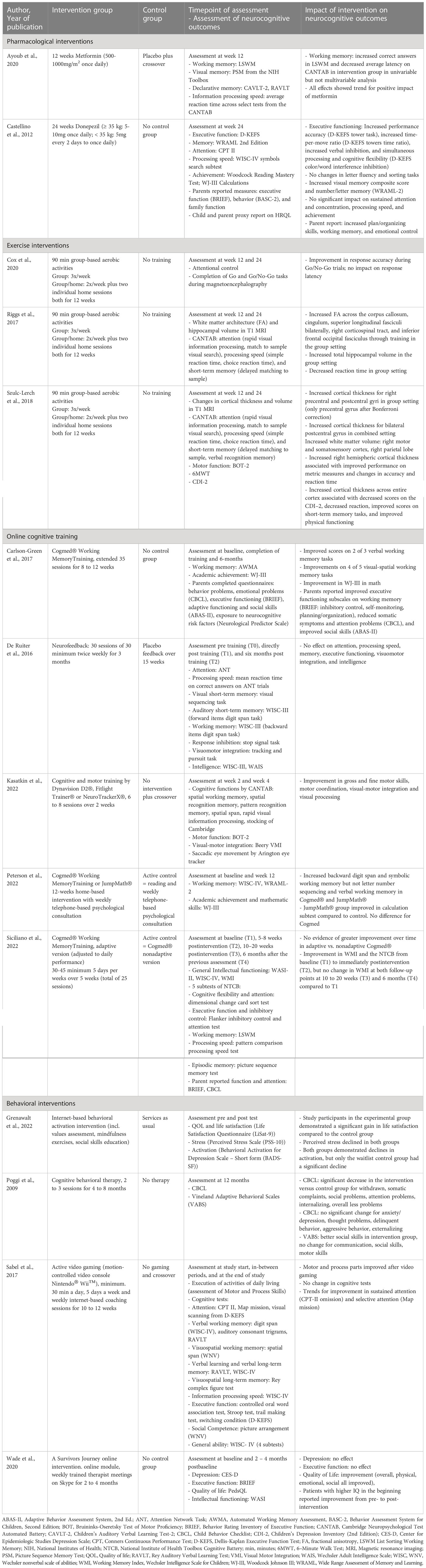
Table 2 Interventions to improve neurocognitive outcomes and impact of intervention.
Two studies investigated pharmacological interventions. Ayoub et al. studied metformin and found a trend for increased working memory and information processing speed if administered over 12 weeks (11). According to Castellino et al, donepezil increased executive functioning and visual memory as well as number/letter memory in a single-arm intervention trial (23).
Three publications reported different outcomes of the same quasi-randomized controlled trial with crossover design on aerobic exercise training (study identifier: NCT01944761) (16, 18, 19). The group studied the impact of repeated group-based or mixed group- and home-based aerobic activities three times a week for 12 weeks. One publication showed improved response accuracy in those with training compared to those without (16). The second publication reported increased white matter architecture and hippocampal volume in those with training (18). When comparing the group-based and the mixed group- and home-based setting, the group-based setting decreased reaction time as an indicator for improved processing speed. The third publication found increased cortical thickness across the entire cortex on imaging (19). This was associated with improved scores on short-term memory tasks and improved physical functioning as well as a decrease in depression and reaction time. The increase in right hemispheric cortical thickness on the other hand was associated with an improvement of metric measures and accuracy in reaction time (19).
Five publications reported on online cognitive training (12, 15, 17, 20, 22). Most of them reported on commercially available online programs. Carlson-Green et al. found some improvement in verbal and visual working memory tasks as well as improvement in academic achievement after 35 sessions of Cogmed® Working Memory Training over 8-12 weeks (22). In the study by Siciliano et al., Cogmed® improved working memory right after the end of the intervention but not in the longer term. It made no difference whether the adaptive or non-adaptive version of the program was used (15). Cogmed® performed similarly to JumpMath® with an increase of working memory in the study by Peterson et al. (20). Additionally, calculation subtests improved in persons using JumpMath® compared to those working with Cogmed® (20). De Ruiter et al. compared online neurofeedback to placebo feedback in 30 sessions over three months and found no effect on attention, processing speed, memory, executive functioning, visuomotor integration, and intelligence (12). Kasatkin et al. showed in a crossover trial that cognitive and motor training with Dynavision D2®, Fitlight Trainer® and NeuroTrackerX® in 6 to 8 sessions over 2 weeks improved gross and fine motor skills, motor coordination, visual-motor integration, and visual processing in the intervention group.
Four publications reported on behavioral interventions, three were internet-based programs (13, 14, 24) and one was a person-to-person cognitive behavioral therapy program (21). According to Grenawalt et al. the behavioral activation intervention increased life satisfaction and slowed down activation in the intervention group (13). When combining active gaming and internet-based coaching sessions, Sabel et al. could show improvement in motor and processing skills but not in cognitive tests (14). Wade et al. used “A Survivors Journey” online modules and could show improved quality of life in participants but no improvement in executive or intellectual functioning (24). The more traditional cognitive behavioral therapy sessions studied by Poggi et al. reduced attention problems in the intervention group (21).
We found 14 publications reporting on interventions to mitigate or improve neurocognitive late-effects in pediatric or adolescent CNS tumor patients and survivors and could identify four different types of interventions: pharmacological interventions, exercise interventions, online cognitive training, and behavioral interventions. The effects of most interventions were rather small and inconsistent in comparison. In addition, the approaches used to measure the outcomes differed and direct comparison of different interventions was not possible.
The studies on pharmacological interventions examined well known drugs with good safety profiles. However, both studies were small with less than 25 participants each, and not optimally designed. Ayoub et al. studied metformin, a drug known as first-line treatment in diabetes mellitus type 2 (25) and experimentally used in the treatment of Alzheimer’s disease associated with diabetes mellitus type 2 (26). The randomized-controlled pilot-feasibility study of Ayoub tried to overcome the small participant number by setting up a crossover design. Nevertheless, no robust effects of metformin on neurocognitive late-effects in pediatric CNS tumor survivors could be observed in the multivariable analysis, only a trend (11). An explanation for the lack of a clear effect of metformin in CNS tumor survivors could be that these patients do not suffer from diabetes mellitus type 2 and that the improvement in patients with Alzheimer’s disease is a secondary effect of controlled metabolism and not due to the direct effects of metformin on the brain itself. Castellino et al. studied donepezil, a cholinesterase inhibitor used in the treatment of dementia where it showed some improvement in executive functioning, cognitive abilities, and behavioral symptoms (27). Even though the investigators found an increase in executive functioning and memory in CNS tumor survivors, the single-arm intervention trial cannot distinguish the drug effects on neurocognitive problems from improvement through other parallel supports that have not been studied (e.g., support at school, rehabilitation programs) (23). Both interventions need to be reevaluated in larger populations with comparison groups.
We could identify one trial reporting different aspects of neurocognition including anatomical changes in the brain after exercise intervention in three separate publications (16, 18, 19). The trial was relatively small with only 28 participants. The hypothesis of the trial was that higher fitness levels might improve cognitive function in pediatric CNS tumor survivors due to improved organization of white matter and increased cortical volumes. This effect was shown in healthy children before (28). Similar effects could also be shown in the three publications indicating that physical exercise should be promoted in survivors of pediatric and adolescent CNS tumors. This trial only examined aerobic exercise activities, but non-aerobic either high-intensity or low-intensity exercise were not studied. It might be helpful to evaluate these modalities in the future because not all pediatric CNS tumor survivors will be able to participate in aerobic exercise training.
Cogmed® Working MemoryTraining was the most frequently studied application for online cognitive training (29). Cogmed® is a computer game-like training program claiming to improve working memory and attention with a non-adaptive and an adaptive version available. The adaptive version adjusts the tasks to the participants daily performance. The included studies showed that working memory improved but improvements did not differ much when compared to other home-based online cognitive trainings such as JumpMath® (20, 30). Additionally, the adaptive version of Cogmed® did not influence the improvement compared to the non-adaptive version (15). Other cognitive training such as the combination of Dynavision D2® (31), Fitlight Trainer® (32), and NeuroTrackerX® (33) also showed cognitive improvement. These results suggest that online cognitive programs improve the working memory, but that the program itself does not matter, as long as there is some online cognitive training done. If online cognitive training is used, we suggest keeping to local practices and availabilities.
Few to no effects on neurocognitive problems in pediatric CNS tumor survivors could be observed in all three internet-based behavioral interventions (13, 14, 24). On the other hand, Poggi et al. could show that traditional person-to-person cognitive behavioral therapy decreased attention problems. These findings differ from the general population where person-to-person and internet-based behavioral interventions were similarly effective (34). One possible explanation being that children and adolescents might already have had contact with psychological liaison service during diagnosis and treatment and are already used to person-to-person contact. Additionally, fatigue is a common late-effect after treatment of CNS tumors and might influence concentration and perseverance in internet-based interventions (35).
In this review we focused on interventions aiming to improve neurocognitive problems in pediatric and adolescent CNS tumor patients or survivors. The 14 included studies used many different neurocognitive assessment tools leading to a variability in the assessment of success of the studied interventions. The variety in interventions and outcome measures made direct comparison difficult and prohibits an estimate of superiority or inferiority of the investigated interventions. A further limitation of the included publications were the small sample sizes. Consequently, the findings often resulted only in the reporting of trends or small effects of the studied interventions. For future research we recommend studying larger patient numbers and to perform preferably international and harmonized collaborations to assess efficacy of interventions to mitigate neurocognitive problems in pediatric and adolescent CNS tumor patients or survivors.
We found several publications indicating improvement of neurocognitive problems in pediatric and adolescent CNS tumor survivors like exercise interventions or online cognitive training. Both intervention types can be implemented relatively easily in daily practice if respective resources are available or via remote access from home. Aerobic exercise training can be instructed by local physiotherapists in group or personalized settings. For online cognitive training interventions we suggest keeping to local practices and availabilities as there seems to be no big difference in the outcomes between the different programs examined.
RK: acquisition, analysis, interpretation of data, writing manuscript and final approval of manuscript. PF: acquisition, analysis, interpretation of data, writing manuscript and final approval of manuscript. MO: acquisition, analysis, interpretation of data, review of manuscript and final approval of manuscript. KS: conception of work, acquisition, analysis, interpretation of data, review of manuscript and final approval of manuscript. All authors contributed to the article and approved the submitted version.
MO was supported by a grant from Swiss Cancer Research (HSR-5219-11-2020).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1150166/full#supplementary-material
1. Schindler M, Belle FN, Grotzer MA, von der Weid NX, Kuehni CE. (SPOG) SPOG. Childhood cancer survival in Switzerland (1976-2013): time-trends and predictors. Int J Cancer (2017) 140(1):62–74. doi: 10.1002/ijc.30434
2. Girardi F, Allemani C, Coleman MP. Worldwide trends in survival from common childhood brain tumors: a systematic review. J Glob Oncol (2019) 5:1–25. doi: 10.1200/JGO.19.00140
3. Krull KR, Hardy KK, Kahalley LS, Schuitema I, Kesler SR. Neurocognitive outcomes and interventions in long-term survivors of childhood cancer. J Clin Oncol (2018) 36(21):2181–9. doi: 10.1200/JCO.2017.76.4696
4. Robison LL, Green DM, Hudson M, Meadows AT, Mertens AC, Packer RJ, et al. Long-term outcomes of adult survivors of childhood cancer. Cancer (2005) 104(11 Suppl):2557–64. doi: 10.1002/cncr.21249
5. Gunn ME, Lähdesmäki T, Malila N, Arola M, Grönroos M, Matomäki J, et al. Late morbidity in long-term survivors of childhood brain tumors: a nationwide registry-based study in Finland. Neuro Oncol (2015) 17(5):747–56. doi: 10.1093/neuonc/nou321
6. Duffner PK. Risk factors for cognitive decline in children treated for brain tumors. Eur J Paediatr Neurol (2010) 14(2):106–15. doi: 10.1016/j.ejpn.2009.10.005
7. Mulhern RK, Merchant TE, Gajjar A, Reddick WE, Kun LE. Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol (2004) 5(7):399–408. doi: 10.1016/S1470-2045(04)01507-4
8. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PloS Med (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
9. Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak (2007) 7:16. doi: 10.1186/1472-6947-7-16
10. J B. critical appraisal tools. Joanna Briggs Institute. Available at: https://jbi.global/critical-appraisal-tools.
11. Ayoub R, Ruddy RM, Cox E, Oyefiade A, Derkach D, Laughlin S, et al. Assessment of cognitive and neural recovery in survivors of pediatric brain tumors in a pilot clinical trial using metformin. Nat Med (2020) 26(8):1285–94. doi: 10.1038/s41591-020-0985-2
12. de Ruiter MA, Oosterlaan J, Schouten-van Meeteren AY, Maurice-Stam H, van Vuurden DG, Gidding C, et al. Neurofeedback ineffective in paediatric brain tumour survivors: results of a double-blind randomised placebo-controlled trial. Eur J Cancer (2016) 64:62–73. doi: 10.1016/j.ejca.2016.04.020
13. Grenawalt TA, Tansey TN, Phillips BN, Strauser DR, Rosenthal DA, Wagner S. Effectiveness of internet-based behavioral activation on quality of life among young adult survivors of childhood brain tumor: a randomized controlled trial. Disabil Rehabil (2022), 1–8. doi: 10.1080/09638288.2022.2094478
14. Sabel M, Sjölund A, Broeren J, Arvidsson D, Saury JM, Gillenstrand J, et al. Effects of physically active video gaming on cognition and activities of daily living in childhood brain tumor survivors: a randomized pilot study. Neurooncol Pract (2017) 4(2):98–110. doi: 10.1093/nop/npw020
15. Siciliano RE, Thigpen JC, Desjardins L, Cook JL, Steele EH, Gruhn MA, et al. Working memory training in pediatric brain tumor survivors after recent diagnosis: challenges and initial effects. Appl Neuropsychol Child (2022) 11(3):412–21. doi: 10.1080/21622965.2021.1875226
16. Cox E, Bells S, Timmons BW, Laughlin S, Bouffet E, de Medeiros C, et al. A controlled clinical crossover trial of exercise training to improve cognition and neural communication in pediatric brain tumor survivors. Clin Neurophysiol (2020) 131(7):1533–47. doi: 10.1016/j.clinph.2020.03.027
17. Kasatkin V, Deviaterikova A, Shurupova M, Karelin A. The feasibility and efficacy of short-term visual-motor training in pediatric posterior fossa tumor survivors. Eur J Phys Rehabil Med (2022) 58(1):51–9. doi: 10.23736/S1973-9087.21.06854-4
18. Riggs L, Piscione J, Laughlin S, Cunningham T, Timmons BW, Courneya KS, et al. Exercise training for neural recovery in a restricted sample of pediatric brain tumor survivors: a controlled clinical trial with crossover of training versus no training. Neuro Oncol (2017) 19(3):440–50. doi: 10.1093/neuonc/now177
19. Szulc-Lerch KU, Timmons BW, Bouffet E, Laughlin S, de Medeiros CB, Skocic J, et al. Repairing the brain with physical exercise: cortical thickness and brain volume increases in long-term pediatric brain tumor survivors in response to a structured exercise intervention. NeuroImage Clin (2018) 18:972–85. doi: 10.1016/j.nicl.2018.02.021
20. Peterson RK, Longo C, Cunningham T, Janzen L, Guger S, Monteiro L, et al. Impact of home-based cognitive or academic intervention on working memory and mathematics outcomes in pediatric brain tumor survivors: the keys to succeed pilot randomized controlled clinical trial. Child Neuropsychol (2022) 28(8):1116–40. doi: 10.1080/09297049.2022.2061933
21. Poggi G, Liscio M, Pastore V, Adduci A, Galbiati S, Spreafico F, et al. Psychological intervention in young brain tumor survivors: the efficacy of the cognitive behavioural approach. Disabil Rehabil (2009) 31(13):1066–73. doi: 10.1080/09638280802509546
22. Carlson-Green B, Puig J, Bendel A. Feasibility and efficacy of an extended trial of home-based working memory training for pediatric brain tumor survivors: a pilot study. Neurooncol Pract (2017) 4(2):111–20. doi: 10.1093/nop/npw015
23. Castellino SM, Tooze JA, Flowers L, Hill DF, McMullen KP, Shaw EG, et al. Toxicity and efficacy of the acetylcholinesterase (AChe) inhibitor donepezil in childhood brain tumor survivors: a pilot study. Pediatr Blood Cancer (2012) 59(3):540–7. doi: 10.1002/pbc.24078
24. Wade SL, Narad ME, Moscato EL, LeBlond EI, King JA, Raj SP, et al. A survivor's journey: preliminary efficacy of an online problem-solving therapy for survivors of pediatric brain tumor. Pediatr Blood Cancer (2020) 67(2):e28043. doi: 10.1002/pbc.28043
25. Benavides S, Striet J, Germak J, Nahata MC. Efficacy and safety of hypoglycemic drugs in children with type 2 diabetes mellitus. Pharmacotherapy (2005) 25(6):803–9. doi: 10.1592/phco.2005.25.6.803
26. Koenig AM, Mechanic-Hamilton D, Xie SX, Combs MF, Cappola AR, Xie L, et al. Effects of the insulin sensitizer metformin in Alzheimer disease: pilot data from a randomized placebo-controlled crossover study. Alzheimer Dis Assoc Disord (2017) 31(2):107–13. doi: 10.1097/WAD.0000000000000202
27. Bowen DM, Francis PT, Pangalos MN, Stephens PH, Procter AW. Treatment strategies for alzheimer's disease. Lancet (1992) 339(8785):132–3. doi: 10.1016/0140-6736(92)91050-I
28. Chaddock L, Pontifex MB, Hillman CH, Kramer AF. A review of the relation of aerobic fitness and physical activity to brain structure and function in children. J Int Neuropsychol Soc (2011) 17(6):975–85. doi: 10.1017/S1355617711000567
29. Cogmed® working MemoryTraining: neural assembly int AB. Available at: https://www.cogmed.com/.
30. JUMP math. Available at: https://jumpmath.org/.
31. Dynavision D2®: dynavision global holdings LLC. Available at: https://www.dynavisioninternational.com/.
32. Fitlight trainer®: FITLIGHT® corp. Available at: https://www.fitlighttraining.com/.
33. NeuroTrackerX®. Available at: https://www.neurotrackerx.com/.
34. Esfandiari N, Mazaheri MA, Akbari-Zardkhaneh S, Sadeghi-Firoozabadi V, Cheraghi M. Internet-Delivered versus face-to-Face cognitive behavior therapy for anxiety disorders: systematic review and meta-analysis. Int J Prev Med (2021) 12:153. doi: 10.4103/ijpvm.ijpvm_208_21
Keywords: late-effects, pediatric brain tumors, intervention, neurocognition, children, adolescent and young adult
Citation: Kasteler R, Fuchs P, Otth M and Scheinemann K (2023) Interventions to improve neurocognitive late-effects in pediatric and adolescent CNS tumor patients and survivors - a systematic review. Front. Oncol. 13:1150166. doi: 10.3389/fonc.2023.1150166
Received: 23 January 2023; Accepted: 12 April 2023;
Published: 02 May 2023.
Edited by:
Sabine Mueller, University of California, San Francisco, United StatesReviewed by:
Yasmin Lassen, Aarhus University Hospital, DenmarkCopyright © 2023 Kasteler, Fuchs, Otth and Scheinemann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rahel Kasteler, rahel.kasteler@ksa.ch
†These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.