
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 19 May 2023
Sec. Skin Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1142170
 Veronika Tóth1*
Veronika Tóth1* Stefani Christina Diakoumakou2
Stefani Christina Diakoumakou2 Enikő Kuroli1Béla Tóth1Daniella Kuzmanovszki1József Szakonyi1Kende Kálmán Lőrincz1Beáta Somlai1
Enikő Kuroli1Béla Tóth1Daniella Kuzmanovszki1József Szakonyi1Kende Kálmán Lőrincz1Beáta Somlai1 Sarolta Kárpáti1
Sarolta Kárpáti1 Péter Holló1
Péter Holló1Background: The possible correlation between melanoma and Parkinson’s disease (PD) has been intensively studied. In this work, we aimed to assess the coincidence of skin malignancies and PD at a dermato-oncological university centre in Central-Eastern Europe, Hungary.
Methods: From 2004 to 2017, a retrospective analysis of the centre’s database was performed based on International Statistical Classification of Diseases-10 codes.
Results: Out of the patients who visited the clinic during the study period, 20,658 were treated for malignant skin tumours. Over the 14 years, 205 dermatological patients had PD simultaneously, 111 (54%) of whom had at least one type of skin malignancy: melanoma (n=22), basal cell carcinoma (BCC) (n=82), or squamous cell carcinoma (SCC) (n=36) (in some patients, multiple skin tumours were identified). Compared to the age- and sex-matched control group, patients with PD had a significantly lower risk for basal cell carcinoma (OR, 0.65; 95% CI, 0.47–0.89, p=0.0076) and for all skin tumours (OR, 0.74; 95% CI, 0.56–0.98, p=0.0392) but not for melanoma.
Conclusions: We found a decreased risk of all skin tumours and basal cell carcinoma and an unchanged risk of melanoma among patients with PD. However, it should be kept in mind that some large-scale meta-analyses suggest a higher incidence of melanoma after a diagnosis of PD, indicating the importance of skin examination in this vulnerable population.
The connection between Parkinson’s disease (PD) and melanoma was first described by Skibba in 1972, presenting a case of multiple primary melanomas in a patient with PD treated with levodopa (1). Afterwards, although levodopa remained a “gold standard” in the treatment of PD, several reports presented melanoma cases among patients treated with levodopa (2–7). These observations resulted in concern with levodopa treatment, and in some countries, the warning of the possible risk was included in the drug leaflet. A case of melanocytic hyperactivation simulating acral lentiginous melanoma in a patient with PD treated with levodopa was published recently (8). The theory suggests that the association between levodopa therapy and melanoma development is based on the shared biochemical pathway of dopamine and melanin synthesis, yet currently, most reports deny this supposed connection (9–15).
The mechanism by which melanoma develops more frequently in PD patients and why patients with melanoma more frequently have PD than the general population have not yet been clarified. Although several mechanisms have been proposed, the data are contradictory. The background of both diseases seems to be multifactorial, and both genetic and environmental factors may play a role in their pathomechanisms (8, 9, 16–24).
Mutations in shared genetic factors such as Parkin, DJ-1, LRRK2, α-synuclein, PLA2G6, EIF4G1, and SYNJ1 gene/protein can contribute to the association between the two diseases. Parkin is a tumour suppressor gene that encodes a ubiquitin ligase found in several cancers and up to half of patients with early-onset familial PD. Loss or mutation of the gene interferes with the degradation of cyclin E; consequently, its level increases and forces the cell to divide faster (25, 26). The role of the mutant DJ-1 oncogene, a sensor of oxidative stress, was found in different tumour types and proven to cause early-onset hereditary PD. Mutant LRRK2 causes both familial and sporadic PD and is responsible for 30%–40% of late-onset PD cases in the Ashkenazi Jewish population and North African Arab Berbers population. A multinational study from five centres demonstrated that LRRK2 G2019S mutation carriers have an overall increased risk, especially for breast and hormone-related cancers, compared to non-carriers (27). Further theory has been based on alpha-synuclein, a small soluble protein expressed primarily in presynaptic terminals of neural tissue and in both benign and malignant melanocytic lesions and certain other tumours. Alpha-synuclein production is equally increased in dopaminergic neuronal cells in patients with PD and in melanoma cells (28–30). Pigmentation can be another potential common pathway; according to a meta-analysis, red hair and certain MC1R gene variants, which are both risk factors for melanoma, can increase the occurrence of PD as well (31). In addition, changes in low-penetrance genes (e.g., glutathione S-transferase M1 gene, cytochrome p450 debrisoquine hydroxylase, and vitamin D receptor gene) together with environmental factors (e.g., socioeconomic status, smoking, and sun-bathing habits) can equally contribute to the association between the two diseases (32, 33). However, certain authors deny any association or the role of common genetic background (34, 35).
Although the epidemiological data are occasionally controversial, large-scale meta-analyses mostly confirmed the positive association between PD and melanoma. The authors of a large meta-analysis involving 40 studies (2,317,408 PD patients) found that PD patients had decreased risks for urogenital, gastrointestinal, lung, and haematological malignancies but increased risks for melanoma and brain cancer compared to controls (36). Similarly, in another meta-analysis of 14 studies, PD patients had decreased risks for general, colon, rectal, and lung cancer but increased risks for brain cancer and melanoma. In contrast, when the LRRK2 G2019S mutation was present in PD patients, increased risks for general, colon, haematological, and brain cancer were observed (37). A meta-analysis of the cancer incidence of 577,013 patients suffering from eight different central nervous system disorders showed that the co-occurrence of PD and melanoma was higher, while general, lung, prostate, and colorectal cancer co-occurrence was lower in cases of PD than in control patients (38). The results of a recent systematic review and meta-analysis of 292,275 PD patients in 24 studies showed that the risk of melanoma after, but not before, the diagnosis of PD was significantly higher (39). Another meta-analysis also confirmed the importance of the time of melanoma diagnosis; the authors found that the occurrence of melanoma was significantly higher only after the diagnosis of PD (40).
The connection between PD and non-melanoma skin cancer (NMSC) is contradictory. Some authors have reported that patients suffering from PD have a higher risk for NMSCs (16, 18, 41), especially for basal (42, 43) and squamous cell carcinoma of the head and neck region (44, 45). Others described a significantly lower frequency of any skin cancer and non-melanoma skin cancers (37, 46). Lerman et al. found weak or no association between PD and squamous cell carcinoma (47). PD can be associated not only with skin malignancies but also with a wide spectrum of skin disorders, such as seborrheic dermatitis, sweating disorders, bullous pemphigoid, rosacea, and perioral dermatitis (48, 49).
Various studies have investigated the connection between PD and extracutaneous malignancies. Many authors found a significantly lower risk for all malignancies among patients with PD, including colorectal, lung, and larynx cancer, while breast, prostate, renal, and thyroid cancer risk was reported to be higher than expected (16, 18, 38, 50, 51). In contrast, Lin et al. found that, in Taiwan, PD was not associated with breast, ovarian, or thyroid cancers, but increased hazard ratios were found in cases of 16 cancers, including gastrointestinal tract cancers and lung and brain tumours (52). Bajaj et al. conducted a large review of the literature involving more than 100,000 patients. They found significantly reduced overall cancer risk ratios among patients with PD (53).
Since studies focusing on the association of PD and skin tumours were mainly carried out in the USA (15, 19, 20, 54–58) and in Western European populations, such as the United Kingdom (50, 59), Germany (38), Sweden (60), Denmark (13, 38, 61, 62), Portugal (49), Israel (10, 63), and Taiwan (50, 52), we aimed to assess the co-occurrence of skin malignancies and PD among patients from an academic dermato-oncology centre in Hungary, a Central-Eastern European country.
A retrospective analysis of the database of the Department of Dermatology, Venereology, and Dermatooncology at Semmelweis University was performed between 1 January 2004 and 31 December 2017. The total number of patients who visited the department during the 14-year examination because of any skin malignancy was 20,658. To identify patients with melanoma, NMSC, and PD, we used International Statistical Classification of Diseases-10 (ICD-10) codes; patients with melanoma were selected by the c4300–c4390 codes, squamous cell carcinoma by the c4401–c4491 codes, and basal cell carcinoma by the c4402–c4492 codes. The patients with PD were collected based on the ICD-10 code G20. Combining the patient populations of the four different diagnoses, we selected those patients who had melanoma or NMSC associated with PD. Data on skin tumours and PD were obtained by reviewing the patient’s medical history.
Control group. Because the mean age of the patients diagnosed with PD and skin tumours was different, in addition to these diseases affecting the two sexes differently, for each patient with PD, five age- and sex-matched controls without PD were selected randomly from the patients of the department from 2004 to 2017. These five control patients had the same sex and were born in the same year as the studied patient. Consequently, 205 patients with PD associated with skin disease were matched with 1,025 age- and sex-matched control patients with skin disease but no PD.
First, descriptive statistics were performed. The association between PD and melanoma and basal and squamous cell carcinoma was assessed separately. To examine the odds of having skin malignancy in PD patients, we used GraphPad Prism 9.3.1 (147) software. Odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated for each group from contingency tables. An OR >1 indicated a positive association, and an OR <1 indicated a negative association between a given skin tumour and PD. Comparing the ORs of different tumour types, we used the case numbers (number of skin tumours) instead of the number of patients because, contrary to most other malignant disorders, tumours of the skin are often multiple. Consequently, in the case of calculation with the number of patients instead of the number of skin neoplasms, cases were lost. Since we had a small sample size, to calculate the correlation between our categorical variables, we used Fisher’s exact tests to determine whether the difference was statistically significant. A probability value of <0.05 was considered statistically significant.
From 2004 to 2017 at the Department of Dermatology, Venereology, and Dermatooncology at Semmelweis University, 20,658 patients were treated for skin malignancy. A total of 6,300 patients had melanoma, 11,983 had basal cell carcinoma, and 2,375 had squamous cell carcinoma.
Over the 14 years, 205 patients visited the department due to a skin disease and PD simultaneously. The ratio of male to female patients was 61.5% to 38.5%. Of the 205 patients, 94 had no skin malignancy, while 111 (54%) patients had malignant skin tumours. The mean age of the studied patients was 78 ± 8.4 years, with a median age of 79 years. The youngest patient was 47 years old, and the oldest patient was 96 years old. The mean age at PD onset was 72.2 ± 9.5 years, while the mean age at the diagnosis of the first skin malignancy at the department was 77.9 ± 8 years (Table 1).
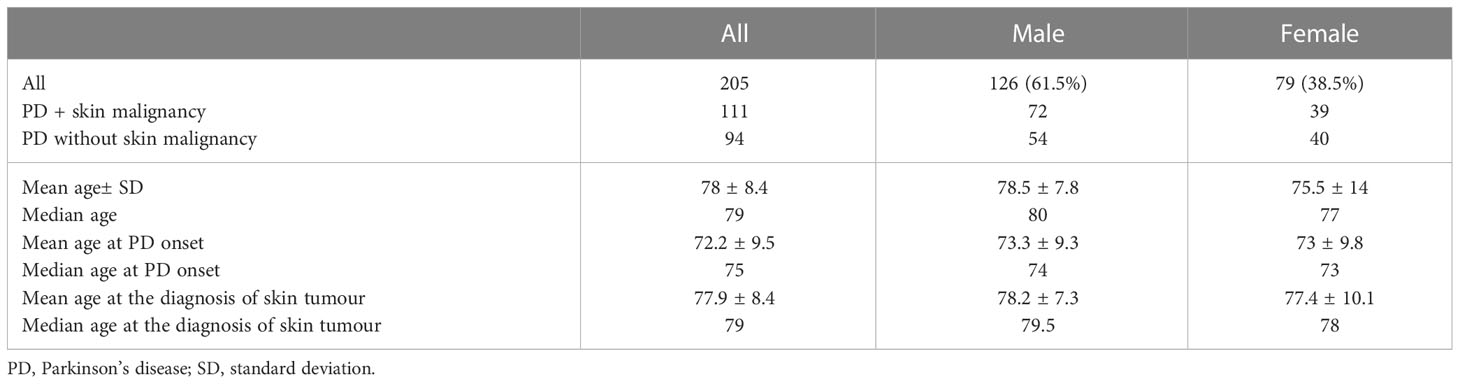
Table 1 Demographic data of patients with simultaneous malignant or non-malignant skin disease and PD.
Multiple skin tumours were frequent among these 111 patients; 65 of them had only one skin malignancy, and in the remaining 46 patients, multiple tumours occurred. Altogether, 140 skin malignancies (positive events), 22 melanomas, 82 basal cell carcinomas, and 36 squamous cell carcinomas were diagnosed in the 111 patients. In addition, we found some rare skin tumours simultaneously with PD: two trichilemmal carcinomas, a malignant fibrous histiocytoma, an atypical fibroxanthoma, and a Merkel cell carcinoma. There were 27 patients who had different types of skin malignancies simultaneously, and one patient had 35 malignant skin tumours, including melanomas, trichilemmal carcinomas, and basal and squamous cell carcinomas.
We randomly coupled each of the 205 patients with PD with five age- and sex-matched patients who did not have PD from the department from 2004 to 2017. Consequently, 205 patients with PD and 1,025 control patients were matched. A total of 560 patients were negative for skin tumours, while 465 patients had a total of 1,127 skin malignancies (total events): 132 melanomas, 752 basal cell carcinomas, and 243 squamous cell carcinomas (on some patients, multiple skin tumours occurred).
Assessing the odds of all skin malignancies, it proved to be significantly decreased among the patients with PD (OR, 0.74; 95% CI, 0.56–0.98; p=0.0392). The odds proved to be significantly decreased as well in cases of basal cell carcinoma and PD (OR, 0.65; 95% CI, 0.47–0.89; p=0.0076). On the other hand, the results did not show a significant correlation between PD and melanoma or PD and squamous cell carcinoma (Table 2).

Table 2 Comparison of skin malignancies in patients with or without PD; odds ratios of skin malignancies among patients with PD.
Single and multiple skin malignancies equally developed more frequently in men than in women, which was noticeable for every type of skin tumour. Seven of 19 patients suffering from melanoma had additional basal cell carcinomas, and two had additional squamous cell carcinomas as well (Table 3).

Table 3 Sex distribution of skin malignancies in patients with Parkinson’s disease.
The average age at melanoma diagnosis was 73±11.5 years (men, 75.5±6.8 years; women, 69±16 years). The most frequent localisation was the head–neck area (41% of the melanomas). All of these patients were treated orally with anti-Parkinson’s agents. A total of 10 patients received levodopa/benserazide, six received amantadine, five received ropinirole, five received selegiline, three received rasagiline, two received levadopa/carbidopa/entacapone, and two received pramipexole. One patient was treated with rotigotine, biperiden hydrochloride, procyclidine, and carbidopa/levodopa.
The average Breslow thickness of all melanomas among male patients was 8.27±10.9 mm. Out of the 13 male patients with melanoma, six had advanced, thick tumours with a high average thickness of 12.6±12.5 mm. Two of these six patients also developed second primary in situ melanoma (n=3). We had a male patient who had 35 different malignant skin tumours (one melanoma, nine basal cell carcinomas, 24 squamous cell carcinomas, and one trichilemmal carcinoma), most of which developed in sun-exposed areas. The patient’s PD was diagnosed 8 years earlier than the melanoma, and he was treated with amantadine and levodopa/carbidopa/entacapone followed by levodopa/benserazide.
In two of the six female patients, the histological data of the primary melanoma remained unknown. The other four melanomas were thin and belonged to the IA or IB tumour stage.
During the 14 years examined, we found a significant association between PD and skin malignancies, with lower odds of having all skin malignancies or basal cell carcinoma among the PD patients of our department.
Some data suggest that the total cancer risk is reduced in patients with PD (51, 62, 64). In the largest recent meta-analysis according to data from more than 17,000,000 patients in 63 studies, PD was inversely associated with total cancer risk, while there was no significant association between NMSC and PD (65). Reviewing the literature, Bajaj et al. established a decreased risk of non-melanoma skin cancer in cases of PD (OR, 0.79) (52). As in the case of extracutaneous tumours, many authors found a decreased risk of basal cell carcinoma, while others established a positive connection (40, 48, 49, 66). These data are partially in accordance with our results showing decreased odds for all skin cancers and basal cell carcinoma. Since BCC is the most frequent human malignancy, its lower risk can be in the background of the decreased total skin tumour risk in cases of PD.
Among the patients with PD, the number of basal cell carcinomas was less than half (25 vs. 57), and the number of squamous cell carcinomas was approximately one-third (10 vs. 26) in women than in men. A higher number of basal and squamous cell carcinomas was also reported in men in the general population, where the risk factors for multiple NMSCs are age, history of ≥10 sunburns, male sex, and family history of melanoma (67–69). Among our patients, multiple NMSCs were four times more common in men than in women. Moreover, we had a male patient who had 35 primary skin malignancies. This number of NMSCs associated with PD is unique in the literature (44, 45). Salemi et al. reported a 79-year-old male and a 98-year-old female patient who had PD and multiple squamous cell carcinomas in the head–neck region. They supposed that a proapoptotic gene (LDOC1L, leucine zipper, downregulated in cancer 1-like gene) may have played a pathogenetic role in the development of these malignancies (46). Our patient worked as a physical education teacher, which suggests periodic outdoor activities. He took amantadine, a light-sensitising drug against PD. While most of his malignancies developed in sun-affected areas, UV radiation and drug-induced photosensitivity may have played a role in tumour formation.
Our data showed no association between PD and squamous cell carcinoma or melanoma, which contradicts the results of some large-scale meta-analyses (36–38).
Some explanations for this contradiction may be raised. For example, Lee et al. did not find increased melanoma risk in their meta-analysis among LRRK2 G2019S gene mutation carrier PD patients (37). Genetic analysis was not part of the study, and the authors could not determine whether it affected the results. Another reason for this contradiction might be technical: our study was performed at a dermato-oncological university centre in Central-Eastern Europe. The medical history of each patient treated for skin cancer was documented thoroughly. To identify the PD patients, we used the ICD-10 codes. However, if the neurodegenerative disease was mentioned in the medical history but not represented with an ICD-10 code, we failed to find the patient, who consequently dropped out of the study. Furthermore, most of the large reviews were conducted in Western Europe and the USA (37, 39, 40). It may also be hypothesised that in these countries, the healthcare system pays more attention to and cares for elderly and lonely PD patients, while in Central-Eastern Europe, these patients do not reach dermato-oncological centres in time with a skin tumour, which may result in a lower number of patients in these centres suffering from both melanoma and PD.
The sex distribution of our patients was in accordance with the literature that reports a higher incidence rate of PD among men than women (70). In the group of male patients treated for PD and melanoma, the average Breslow thickness was high (8.27±10.9 mm). All four female patients with known primary tumours had early-stage melanomas, with an average Breslow thickness of 0.5±0.5 mm. The thicker tumours of our male patients treated with PD are in accordance with the reported thicker melanomas among men in the general population (71, 72). The most frequent localisations of melanomas were the sun-exposed skin surfaces, particularly the head–neck area and the arms (68.5%), which emphasises the role of UV radiation and anti-Parkinson’s drug-induced photosensitivity as two potential environmental factors (30, 44–47). Levodopa was the most often administered anti-Parkinson’s agent in our patients with concomitant melanoma (13/19). This drug is the gold standard in the treatment of PD, although it was previously considered a predisposing factor for melanoma; currently, most authors deny the connection (9–15). Since Breslow thickness is one of the most important independent prognostic factors for melanoma (73), the high rate of thick tumours mostly developed on sun-exposed skin surfaces and the non-decreased risk of melanoma emphasise the importance of UV protection and regular oncodermatological screening among men living with PD.
In conclusion, this is the first study that analysed the association between skin tumours and PD in Central-Eastern Europe. While the majority of the studies focused on the risk of melanoma in PD patients, our examination was extended to other skin malignancies, such as basal and squamous cell carcinoma. The risk of all skin malignancies was significantly lower, which may be related to the similarly decreased risk of basal cell carcinoma in patients with PD. Despite this encouraging result, the OR of melanoma was not influenced. Moreover, we noticed a large proportion of high-risk melanomas among men, mostly in sun-exposed areas, while women had incipient melanomas. In conclusion, UV protection and regular oncodermatological screening remain highly important, especially for male patients treated for PD, to prevent or to notice potentially lethal melanoma tumours earlier.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The study plan was reviewed and approved by Semmelweis University Regional and Institutional Committee of Science and Research Ethics. Approval number: 209/2021.
Conceptualization: BS and VT; methodology: BT; investigation: DK; software: KL and JS; original draft preparation: SD; review and editing: EK; supervision: SK and PH. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BCC, basal cell carcinoma; CI, confidence interval; ICD-10, International Statistical Classification of Diseases-10; LRRK2, leucine-rich repeat kinase 2; MC1R, melanocortin-1 receptor; NMSC, non-melanoma skin cancer; OR, odds ratio; PD, Parkinson’s disease; SCC, squamous cell carcinoma.
1. Skibba JL, Pinckley J, Gilbert EF, Johnson RO. Multiple primary melanoma following administration of levodopa. Arch Pathol (1972) 93:556–61.
2. Robinson E, Wajsbort J, Hirschowitz B. Levodopa and malignant melanoma. Arch Pathol (1973) 95:213.
3. Lieberman AN, Shupack JL. Levodopa and melanoma. Neurology (1978) 24:340–3. doi: 10.1212/WNL.24.4.340
4. Sober AJ, Wick MM. Levodopa therapy and malignant melanoma. JAMA (1978) 240:554–5. doi: 10.1001/jama.1978.03290060056015
5. Bernstein JE, Medenica M, Soltani K, Solomon A, Lorincz AL. Levodopa administration and multiple primary cutaneous melanomas. Arch Dermatol (1980) 116:1041–4. doi: 10.1001/archderm.1980.01640330079019
6. Paisán-Ruiz C, Houlden H. Common pathogenic pathways in melanoma and Parkinson disease. Neurology (2021) 75:1653–5. doi: 10.1212/WNL.0b013e3181fb4466
7. Charles J, Templier I, Leroux D, Salameire D, Robert C, Lantuejoul S, et al. Twenty-two cutaneous primary melanomas in a patient with high genetic predisposition to melanoma receiving levodopa therapy for parkinson's disease. Pigment Cell Melanoma Res (2009) 22:851–3. doi: 10.1111/j.1755-148X.2009.00624.x
8. Porcar Saura S, Guillén Climent S, Pinazo Canales MI, Monteagudo C. Melanocytic hyperactivation simulating an acral lentiginous melanoma in a patient with Parkinson disease treated by levodopa. Am J Dermatopathol (2021) 43(3):238–41. doi: 10.1097/DAD.0000000000001807
9. Inzelberg R, Israeli-Korn SD. The particular relationship between parkinson’s disease and malignancy: a focus on skin cancers. J Neural Transm (2009) 116:1503–7. doi: 10.1007/s00702-009-0322-x
10. Inzelberg R, Rabey JM, Melamed E, Djaldetti R, Reches A, Badarny S, et al. High prevalence of malignant melanoma in Israeli patients with parkinson's disease. J Neural Transm (Vienna) (2011) 118:1199–207. doi: 10.1007/s00702-011-0580-2
11. Fiala K, Whetteckey J, Manyam B. Malignant melanoma and levodopa in parkinson's disease: causality or coincidence? Parkinsonism Relat Disord (2003) 9:321–7. doi: 10.1016/s1353-8020(03)00040-3
12. Siple J, Schneider D, Wanlass W, Rosenblatt B. Levodopa therapy and the risk of malignant melanoma. Ann Pharmacother (2000) 34:382–5. doi: 10.1345/aph.19150
13. Olsen J, Friis S, Frederiksen K. Malignant melanoma and other types of cancer preceding Parkinson disease. Epidemiology (2006) 17:582–7. doi: 10.1097/01.ede.0000229445.90471.5e
14. Vermeij JD, Winogrodzka A, Trip J, Weber WE. Parkinson’s disease, levodopa-use and the risk of melanoma. Parkinsonism Relat Disord (2009) 15:551–3. doi: 10.1016/j.parkreldis.2009.05.002
15. Lo RY, Tanner CM, Van Den Eeden SK, Albers KB, Leimpeter AD, Nelson LM. Comorbid cancer in parkinson's disease. Mov Disord (2010) 25:1809–17. doi: 10.1002/mds.23246
16. Ferreira J, Neutel D, Mestre T, Coehlo M, Rosa M, Rascol O, et al. Skin cancer and parkinson’s disease. Mov Disord (2010) 25:139–48. doi: 10.1002/mds.22855
17. Pan T, Li X, Jankovic J. The association between parkinson’s disease and melanoma. Int J Cancer (2011) 128:2251–60. doi: 10.1002/ijc.25912
18. Disse M, Reich H, Lee PK, Schram SS. A review of the association between Parkinson disease and malignant melanoma. Dermatol Surg (2011) 42:141–6. doi: 10.1097/DSS.0000000000000591
19. Bertoni JM, Arlette JP, Fernandez HH, Fitzer-Attas C, Frei K, Hassan MN, et al. Increased melanoma risk in Parkinson disease: a prospective clinicopathological study. Arch Neurol (2010) 67:347–52. doi: 10.1001/archneurol.2010.1
20. Constantinescu R, Elm J, Auinger P, Sharma S, Augustine EF, Khadim L, et al. Malignant melanoma in early-treated parkinson's disease: the NET-PD trial. Mov Disord (2014) 29:263–5. doi: 10.1002/mds.25734
21. Nikolaou V, Stratigos AJ. Emerging trends in the epidemiology of melanoma. Br J Dermatol (2014) 170:11–9. doi: 10.1111/bjd.12492
22. Lubbe SJ, Escott-Price V, Brice A, Gasser T, Pittman AM, Bras J, et al. Rare variants analysis of cutaneous malignant melanoma genes in parkinson's disease. Neurobiol Aging (2016) 48:222.e1–e7. doi: 10.1016/j.neurobiolaging.2016.07.013
23. Ye Q, Wen Y, Al-Kuwari N, Chen X. Association between parkinson’s disease and melanoma: putting the pieces together. Front Aging Neurosci (2020) 12:60. doi: 10.3389/fnagi.2020.00060
24. Bose A, Petsko GA, Eliezer D. Parkinson’s disease and melanoma: co-occurrence and mechanisms. J Parkinsons Dis (2018) 8(3):385–98. doi: 10.3233/JPD-171263
25. Hu HH, Kannengiesser C, Lesage S, André J, Mourah S, Michel L, et al. PARKIN inactivation links parkinson's disease to melanoma. J Natl Cancer Inst (2015) 108:1–8. doi: 10.1093/jnci/djv340
26. Levin L, Srour S, Gartner J, Kapitansky O, Qutob N, Dror S, et al. Parkin somatic mutations link melanoma and parkinson's disease. J Genet Genomics (2016) 43:369–79. doi: 10.1016/j.jgg.2016.05.005
27. Agalliu I, San Luciano M, Mirelman A, Giladi N, Waro B, Aasly J, et al. Higher frequency of certain cancers in LRRK2 G2019S mutation carriers with Parkinson disease: a pooled analysis. JAMA Neuro (2015) 72:58–65. doi: 10.1001/jamaneurol.2014.1973
28. George JM. The synucleins. Genome Biol (2002) 3:reviews3002. doi: 10.1186/gb-2001-3-1-reviews3002
29. Pan T, Zhu J, Hwu WJ, Jankovic J. The role of alpha-synuclein in melanin synthesis in melanoma and dopaminergic neuronal cells. PloS One (2012) 7:e45183. doi: 10.1371/journal.pone.0045183
30. Matsuo Y, Kamitani T. Parkinson’s disease-related protein, α-synuclein, in malignant melanoma. PloS One (2010) 5:e10481. doi: 10.1371/journal.pone.0010481
31. Chen X, Feng D, Schwarzschild MA, Gao X. Red hair, MC1R variants, and risk for parkinson's disease - a meta-analysis. Ann Clin Transl Neurol (2017) 4(3):212–6. doi: 10.1002/acn3.381
32. Tacik P, Curry S, Fujioka S, Strongosky A, Uitti RJ, van Gerpen JA, et al. Cancer in parkinson’s disease. Parkinsonism Relat Disord (2016) 31:28–33. doi: 10.1016/j.parkreldis.2016.06.014
33. Rugbjerg K, Friis S, Lassen CF, Ritz B, Olsen JH. Malignant melanoma, breast cancer and other cancers in patients with parkinson's disease. Int J Cancer (2012) 131:1904–11. doi: 10.1002/ijc.27443
34. Senkevich K, Bandres-Ciga S, Yu E, Liyanage UE, International Parkinson Disease Genomics Consortium (IPDGC), Noyce AJ, et al. No evidence for a causal relationship between cancers and parkinson's disease. J Parkinsons Dis (2021) 11(2):801–9. doi: 10.3233/JPD-202474
35. Dong J, Gao J, Nalls M, Gao X, Huang X, Han J, et al. Susceptibility loci for pigmentation and melanoma in relation to parkinson's disease. Neurobiol Aging (2014) 35:1512.e5–10. doi: 10.1016/j.neurobiolaging.2013.12.020
36. Leong YQ, Lee SWH, Ng YK. Cancer risk in Parkinson disease: an updated systematic review and meta-analysis. Eur J Neurol (2021) 28(12):4219–37. doi: 10.1111/ene.15069
37. Lee JYS, Ng JH, Saffari SE, Tan EK. Parkinson's disease and cancer: a systematic review and meta-analysis on the influence of lifestyle habits, genetic variants, and gender. Aging (Albany NY) (2022) 14(5):2148–73. doi: 10.18632/aging.203932
38. Catalá-López F, Suárez-Pinilla M, Suárez-Pinilla P, Valderas JM, Gómez-Beneyto M, Martinez S, et al. Inverse and direct cancer comorbidity in people with central nervous system disorders: a meta-analysis of cancer incidence in 577,013 participants of 50 observational studies. Psychother Psychosom (2014) 83(2):89–105. doi: 10.1159/000356498
39. Huang P, Yang XD, Chen SD, Xiao Q. The association between parkinson’s disease and melanoma: a systematic review and meta-analysis. Trans Neurodegeneration (2015) 4:21. doi: 10.1186/s40035-015-0044-y
40. Liu R, Gao X, Lu Y, Chen H. Meta-analysis of the relationship between Parkinson disease and melanoma. Neurology (2011) 76:2002–9. doi: 10.1212/WNL.0b013e31821e554e
41. Krasowska D, Gerkowicz A, Mlak R, Leziak M, Małecka-Massalska T, Krasowska D. Risk of nonmelanoma skin cancers and parkinson's disease - meta-analysis and systematic review. Cancers (Basel) (2021) 13(4):587. doi: 10.3390/cancers13040587
42. Dobrev H, Nocheva D, Vutova N, Hristova R. Basal cell carcinoma and squamous cell carcinoma in a patient with Parkinson disease. Research (2014) 1:800. doi: 10.13070/rs.en.1.800
43. Hiraldo A, Gómez-Moyano E, Martínez S, Sanz A. Melanomas and basal cell carcinomas in a patient with Parkinson disease. Actas Dermosifiliogr (2010) 101:95–6. doi: 10.1016/j.ad.2009.05.002
44. Salemi M, Giuffrida D, Giuffrida MC, Soma PF, Rolfo A, Cimino L, et al. LDOC1 gene expression in two patients with head and neck squamous cell carcinomas and parkinson's disease. Tumori (2012) 98:86e–8e. doi: 10.1700/1125.12418
45. Calogero A, Soma P, Giuffrida M, Giuffrida D, La Vignera S, Romano C, et al. PARP1 and CASP3 gene expression in a patient with multiple head and neck squamous cell carcinoma and Parkinson disease. Hum Cell (2011) 26:44–6. doi: 10.1007/s13577-011-0021-4
46. Gao X, Ning Y. Cancer and parkinson's disease: the odd couple. Drugs Today (Barc) (2011) 47(3):215–22. doi: 10.1358/dot.2011.47.3.1519657
47. Lerman S, Amichai B, Weinstein G, Shalev V, Chodick G. Parkinson's disease, melanoma, and keratinocyte carcinoma: a population-based study. Neuroepidemiology (2018) 50(3-4):168–73. doi: 10.1159/000487855
48. Niemann N, Billnitzer A, Jankovic J. Parkinson's disease and skin. Parkinsonism Relat Disord (2021) 82:61–76. doi: 10.1016/j.parkreldis.2020.11.017
49. Shahid W, Satyjeet F, Kumari R, Raj K, Kumar V, Afroz MN, et al. Dermatological manifestations of parkinson's disease: clues for diagnosis. Cureus (2020) 12(10):e10836. doi: 10.7759/cureus.10836
50. Sun LM, Liang JA, Chang SN, Sung FC, Muo CH, Kao CH. Analysis of parkinson's disease and subsequent cancer risk in Taiwan: a nationwide population-based cohort study. Neuroepidemiology (2011) 37:114–9. doi: 10.1159/000331489
51. Ong EL, Goldacre R, Goldacre M. Differential risks of cancer types in people with parkinson's disease: a national record-linkage study. Eur J Cancer (2014) 50:2456–62. doi: 10.1016/j.ejca.2014.06.018
52. Lin PY, Chang SN, Hsiao TH, Huang BT, Lin CH, Yang PC. Association between Parkinson disease and risk of cancer in Taiwan. JAMA Oncol (2015) 1:633–40. doi: 10.1001/jamaoncol.2015.1752
53. Bajaj A, Driver JA, Schernhammer ES. Parkinson's disease and cancer risk: a systematic review and meta-analysis. Cancer Causes Control (2010) 21:697–707. doi: 10.1007/s10552-009-9497-6
54. Shalaby SY, Louis ED. Increased odds of melanoma: parkinson's disease, essential tremor, dystonia versus controls. Neuroepidemiology (2016) 46:128–36. doi: 10.1159/000443794
55. Kareus SA, Figueroa KP, Cannon-Albright LA, Pulst SM. Shared predispositions of parkinsonism and cancer: a population-based pedigree-linked study. Arch Neurol (2012) 69:1572–7. doi: 10.1001/archneurol.2012.2261
56. Gao X, Simon KC, Han J, Schwarzschild MA, Ascherio A. Family history of melanoma and Parkinson disease risk. Neurology (2009) 73:1286–91. doi: 10.1212/WNL.0b013e3181bd13a1
57. Driver JA, Logroscino G, Buring JE, Gaziano JM, Kurth T. A prospective cohort study of cancer incidence following the diagnosis of parkinson's disease. Cancer Epidemiol Biomarkers Prev (2007) 16:1260–5. doi: 10.1158/1055-9965.EPI-07-0038
58. Constantinescu R, Romer M, Kieburtz K, DATATOP Investigators of the Parkinson Study Group. Malignant melanoma in early parkinson's disease: the DATATOP trial. Mov Disord (2007) 22:720–2. doi: 10.1002/mds.21273
59. Becker C, Brobert GP, Johansson S, Jick SS, Meier CR. Cancer risk in association with Parkinson disease: a population-based study. Parkinsonism Relat Disord (2010) 16:186–90. doi: 10.1016/j.parkreldis.2009.11.005
60. Wirdefeldt K, Weibull CE, Chen H, Kamel F, Lundholm C, Fang F, et al. Parkinson's disease and cancer: a register-based family study. Am J Epidemiol (2014) 179:85–94. doi: 10.1093/aje/kwt232
61. Olsen JH, Jørgensen TL, Rugbjerg K, Friis S. Parkinson Disease and malignant melanoma in first-degree relatives of patients with early-onset melanoma. Epidemiology (2011) 22:109–12. doi: 10.1097/EDE.0b013e3181fe21a8
62. Olsen JH, Friis S, Frederiksen K, McLaughlin JK, Mellemkjaer L, Møller H. Atypical cancer pattern in patients with parkinson's disease. Br J Cancer (2005) 92:201–5. doi: 10.1038/sj.bjc.6602279
63. Peretz C, Gurel R, Rozani V, Gurevich T, El-Ad B, Tsamir J, et al. Cancer incidence among parkinson's disease patients in a 10-yrs time-window around disease onset: a large-scale cohort study. Parkinsonism Relat Disord (2016) 28:68–72. doi: 10.1016/j.parkreldis.2016.04.028
64. Jansson B, Jankovic J. Low cancer rates among patients with parkinson's disease. Ann Neurol (1985) 17:505–9. doi: 10.1002/ana.410170514
65. Zhang X, Guarin D, Mohammadzadehhonarvar N, Chen X, Gao X. Parkinson's disease and cancer: a systematic review and meta-analysis of over 17 million participants. BMJ Open (2021) 11(7):e046329. doi: 10.1136/bmjopen-2020-046329
66. Ferreira J, Silva JM, Freire R, Pignatelli J, Guedes LC, Feijó A, et al. Skin cancers and precancerous lesions in parkinson's disease patients. Mov Disord (2007) 22(10):1471–5. doi: 10.1002/mds.21575
67. Asgari MM, Moffet HH, Ray GT, Quesenberry CP. Trends in basal cell carcinoma incidence and identification of high-risk subgroups, 1998-2012. JAMA Dermatol (2015) 151:976–81. doi: 10.1001/jamadermatol.2015.1188
68. Nasser N, Filho N, Lehmkuhl RL. Squamous cell cancer–31-year epidemiological study in a city of south Brazil. Bras Dermatol (2015) 90:21–6. doi: 10.1590/abd1806-4841.20153465
69. Qureshi AA, Wei-Passanese EX, Li T, Han J. Host risk factors for the development of multiple non-melanoma skin cancers. J Eur Acad Dermatol Venereol (2013) 27:565–70. doi: 10.1111/j.1468-3083.2012.04483.x
70. Wooten GF, Currie LJ, Bovbjerg VE, Lee JK, Patrie J. Are men at greater risk for parkinson’s disease than women? J Neurol Neurosurg Psychiatry (2004) 75:637–9. doi: 10.1136/jnnp.2003.020982
71. Tóth V, Hatvani Z, Somlai B, Hársing J, László JF, Kárpáti S. Risk of subsequent primary tumor development in melanoma patients. Pathol Oncol Res (2013) 19:805–10. doi: 10.1007/s12253-013-9647-8
72. Moreno-Ramírez D, Ojeda-Vila T, Ríos-Martín JJ, Nieto-García A, Ferrándiz L. Role of age and sex in the diagnosis of early-stage malignant melanoma: a cross-sectional study. Acta Derm Venereol (2015) 95:940–2. doi: 10.2340/00015555-2115
Keywords: Parkinson’s disease, risk, skin malignancy, melanoma, nonmelanoma skin cancer
Citation: Tóth V, Diakoumakou SC, Kuroli E, Tóth B, Kuzmanovszki D, Szakonyi J, Lőrincz KK, Somlai B, Kárpáti S and Holló P (2023) Cutaneous malignancies in patients with Parkinson’s disease at a dermato-oncological university centre in Hungary. Front. Oncol. 13:1142170. doi: 10.3389/fonc.2023.1142170
Received: 11 January 2023; Accepted: 03 May 2023;
Published: 19 May 2023.
Edited by:
Sapna Patel, University of Texas MD Anderson Cancer Center, United StatesReviewed by:
Martin Emiliano Cesarini, INEBA Institute of Neurosciences Buenos Aires, ArgentinaCopyright © 2023 Tóth, Diakoumakou, Kuroli, Tóth, Kuzmanovszki, Szakonyi, Lőrincz, Somlai, Kárpáti and Holló. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Veronika Tóth, dG90aC52ZXJvbmlrYUBtZWQuc2VtbWVsd2Vpcy11bml2Lmh1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.