 Diocésio Alves Pinto de Andrade1,2*
Diocésio Alves Pinto de Andrade1,2* Andréa Paiva Gadelha Guimarães1,3
Andréa Paiva Gadelha Guimarães1,3 Andréia Cristina de Melo1,4
Andréia Cristina de Melo1,4 Angélica Nogueira-Rodrigues1,5Larissa Müller Gomes1,6
Angélica Nogueira-Rodrigues1,5Larissa Müller Gomes1,6 Mariana Scaranti1,7Joyce Maria Lisboa Maia1,8Alessandra Menezes Morelle1,9Candice Amorim de Araújo Lima Santos1,10
Mariana Scaranti1,7Joyce Maria Lisboa Maia1,8Alessandra Menezes Morelle1,9Candice Amorim de Araújo Lima Santos1,10 Cristiano de Pádua Souza1,11Daniela de Freitas1,12Donato Callegaro Filho1,13Eduardo Paulino1,4Elge Werneck Araújo Júnior1,14Juliana Martins Pimenta1,15Marcela Bonalumi dos Santos1,6Michelle Samora de Almeida1,16Ronaldo Pereira Souza1,3Samantha Cabral1,17
Cristiano de Pádua Souza1,11Daniela de Freitas1,12Donato Callegaro Filho1,13Eduardo Paulino1,4Elge Werneck Araújo Júnior1,14Juliana Martins Pimenta1,15Marcela Bonalumi dos Santos1,6Michelle Samora de Almeida1,16Ronaldo Pereira Souza1,3Samantha Cabral1,17 Fernando Cotait Maluf1,15
Fernando Cotait Maluf1,15- 1Brazilian Gynecologic Oncology Group, EVA, São Paulo, Brazil
- 2InORP Oncoclínicas Group, Ribeirão Preto, Brazil
- 3AC Camargo Cancer Center, São Paulo, Brazil
- 4Brazilian Nacional Cancer Institute – INCA, Rio de Janeiro, Brazil
- 5Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 6CPO Oncoclínicas Group, São Paulo, Brazil
- 7DASA – Hospital 9 de Julho, São Paulo, Brazil
- 8Cancer Treatment Center, MedRadius –, Maceió, Brazil
- 9Hospital Moinhos de Vento, Porto Alegre, Brazil
- 10Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Recife, Brazil
- 11Barretos Cancer Hospital, Barretos, Brazil
- 12Hospital Sírio-Libanês, São Paulo, Brazil
- 13Hospital Israelita Albert Einstein, São Paulo, Brazil
- 14IHOC Oncoclínicas Group, Curitiba, Brazil
- 15Hospital Beneficiência Portuguesa de São Paulo, São Paulo, Brazil
- 16Hospital do Coração HCOR Oncologia, São Paulo, Brazil
- 17Universidade de São Paulo, São Paulo, Brazil
Background: Endometrial cancer is of increasing concern in several countries, including Brazil, in part because of an ageing population, declines in fertility, and the increasing prevalence of obesity. Although endometrial tumors had lagged behind other cancer types in terms of treatment improvements, molecular characterization of these tumors is paving the way for novel therapies and an expansion of the therapeutic arsenal. We aimed to help medical oncologists who manage patients with recurrent or metastatic endometrial cancer in the Brazilian healthcare setting.
Methods: The panel, composed of 20 medical oncologists, convened in November 2021 to address 50 multiple-choice questions on molecular testing and treatment choices. We classified the level of agreement among panelists as (1) consensus (≥75% choosing the same answer), (2) majority vote (50% to <75%), or (3) less than majority vote (<50%).
Results: Consensus was present for 25 of the 50 questions, whereas majority vote was present for an additional 23 questions. Key recommendations include molecular testing for every patient with recurrent/metastatic endometrial cancer; choice of first-line treatment according to microsatellite instability and HER2, with the addition of programmed death ligand 1 (PD-L1) and hormone receptors (HRs) for second-line therapy; carboplatin and paclitaxel as the preferred option in first-line treatment of HER2-negative disease, with the addition of trastuzumab in HER2-positive disease; pembrolizumab plus lenvatinib as a key option in second line, regardless of HER2, PD-L1 or HRs; and various recommendations regarding treatment choice for patients with distinct comorbidities.
Conclusion: Despite the existing gaps in the current literature, the vast majority of issues addressed by the panel provided a level of agreement sufficient to inform clinical practice in Brazil and in other countries with similar healthcare environments.
Introduction
Cancer of the uterine corpus is currently the most frequent gynecological malignancy in the US and the sixth most commonly diagnosed neoplasm in women worldwide, with 417,000 new cases estimated for 2020 (1, 2). Even though incidence rates for uterine cancer vary up to 10-fold across countries, and the highest rates are found in North America and Eastern and Northern Europe, incidence rates have been rising worldwide, and countries with historically lower rates have had the largest proportional increase in incidence (3). Although only 7,840 new cases of tumors of the uterine corpus have been estimated for Brazil in 2023 (4), this country had the third largest average annual percent increase (nearly 5%) in incidence in a recent worldwide survey (3, 5, 6). Reasons for the rising incidence of uterine tumors remain incompletely understood, but an ageing population, declines in the fertility rate and the increasing prevalence of obesity are likely to play a major role (1, 7, 8). Endometrial cancer, which accounts for most neoplasms of the uterine corpus – since uterine sarcomas account for only approximately 3-7% of cases (9) – has a median age at diagnosis of 63 years and a strong association with obesity (10, 11). In fact, the association between obesity and endometrial cancer is stronger than for any other common cancer type, and between 36.5% to 54.9% of all uterine corpus tumors in the US are attributable to obesity across different States in that country (7, 10, 12, 13). The use of unopposed estrogen and tamoxifen are also recognized risk factors for endometrial cancer, and changes in the prevalence of these factors likely play a role in current trends for this disease (8, 10, 11, 14).
Even though survival has improved since the mid-1970s for most common cancer types, neoplasms of the uterine corpus represent an exception, largely because of the lack of major treatment advances over the last few decades (2). In recent years, however, molecular characterization of endometrial tumors has become a key component in treatment decisions for patients with recurrent and metastatic disease, and an increased understanding of the molecular basis for different uterine cancers has paved the way for novel therapies for these patients (8, 10, 15–17). As a result, the practicing oncologist has witnessed the recent expansion of the knowledge base and the therapeutic arsenal against recurrent and metastatic endometrial cancer (15, 18). This is particularly evident in second- and subsequent-line treatment, given recent clinical trials of agents with activity against specific molecular subgroups. To informe decisions in the Brazilian healthcare setting, a panel of experts convened in an attempt to establish consensus recommendations in this country for the management of patients with endometrial cancer that is metastatic at diagnosis or presenting as recurrent disease not amenable to local control. The current article presents the results of that panel.
Panel composition and methodology
The panel was composed by 20 medical oncologists from Brazil, with expertise in gynecological oncology, and working in institutions representing diverse geographic and socioeconomic settings in this country. The panel was coordinated by a committee composed of three of the current authors (DAPA, APGG and FCM), who prepared the 50 multiple-choice questions addressed by the panel and coordinated its conduct by teleconference in November 2021. To provide their recommendations, panel members were expected to take into account the published scientific literature and their own clinical experience. Recommendations were provided in an anonymous manner using an online system that also allowed tabulation of results after the end of the voting period for each question. The questions aimed to elicit recommendations regarding molecular testing and the choice of treatment for patients with recurrent or metastatic endometrial cancer, with particular emphasis on treatment past the first line.
The results for each of the 50 questions addressed by the panel were analyzed descriptively. The level of agreement among voters was ascertained by classifying responses to each question as (1) consensus, (2) majority vote, or (3) less than majority vote. If at least 75% of the voting panel members provided a particular recommendation, consensus was present. If between 50% and 74.9% of the voting members provided a particular recommendation, this was considered as majority vote. For each question, voters had the option to abstain when they felt impeded to provide a qualified response for any reason; of note, recommendation percentages included the option “abstain” in their denominator. The panel was made possible by an educational grant from Merck, Sharp & Dohme, who had no influence on the creation of the questions, the panel conduct, or the writing of the article, all of which rest under the entire responsibility of the authors. Approval by an ethics committee was not required, given the nature of this specific manuscript that only involved expert contributors (the authors). No human subjects were involved.
Panel recommendations
Patient assessment before treatment
Table 1 displays results pertaining to the nine questions related to patient assessment. Consensus was reached for two of those questions: (1) every patient with recurrent/metastatic endometrial cancer should undergo molecular testing before treatment initiation; and (2) computed tomography scan of the chest and abdomen are recommended for baseline assessment before treatment. Moreover, majority vote was present for five of the remaining seven questions: (1) 50% of panelists recommended a more complete histopathological and molecular assessment that includes tumor grade, histological subtype, and the status of microsatellite instability (MSI), HER2, p53, programmed death ligand 1 (PD-L1), polymerase epsilon (POLE), and hormone receptors; (2) 64.7% of panelists recommended that HER2 assessment is necessary in specific cases (and an additional 29.4% recommend it for all cases); (3) 52.9% of panelists recommended against testing for PD-L1; (4) 58.8% did not recommend the assessment of tumor mutational burden (although 41.2% of voters recommended it in specific circumstances); and (5) 52.9% of panelists recommended CA125 assessment. Finally, there was more heterogeneity for the two remaining questions. However, if response options are pooled, 73.4% of voters recommended the assessment of MSI “always”, “mostly” or “in some specific cases”. Likewise, a total of 83.4% of voters recommended the assessment of hormone receptors “always”, “mostly” or “in some specific cases”. Of note, there were no abstentions for questions related to patient assessment.
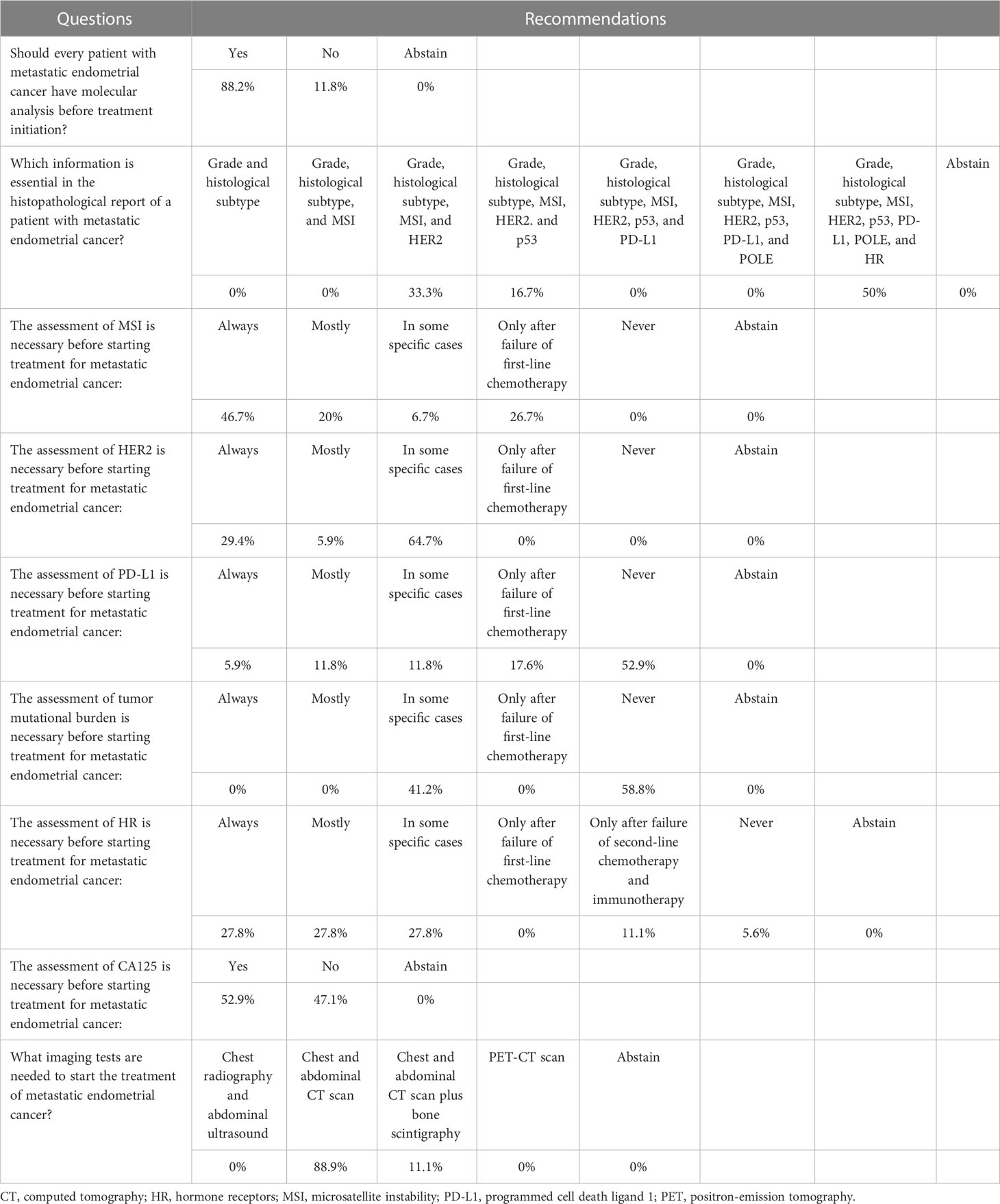
Table 1 Questions related to patient assessment before treatment initiation.
First-line treatment
As shown in Table 2, consensus was reached for four of six questions pertaining to first-line treatment: (1) first-line treatment should differ according to MSI and HER2 statuses; (2) chemotherapy should be used in first-line treatment of HER2-negative disease; (3) chemotherapy plus trastuzumab should be used in first-line treatment of HER2-positive disease; and (4) the conventional regimen of carboplatin (area under the curve 5-6) and paclitaxel (175 mg/m2 every 3 weeks) should be used in the first-line treatment of HER2-negative disease. Majority vote was reached for the remaining two questions: (1) 56.3% of panelists recommended that chemotherapy should not be used alone in first-line treatment of HER2-positive disease; and (2) 66.6% of voters recommended six as the standard number of cycles for first-line treatment.
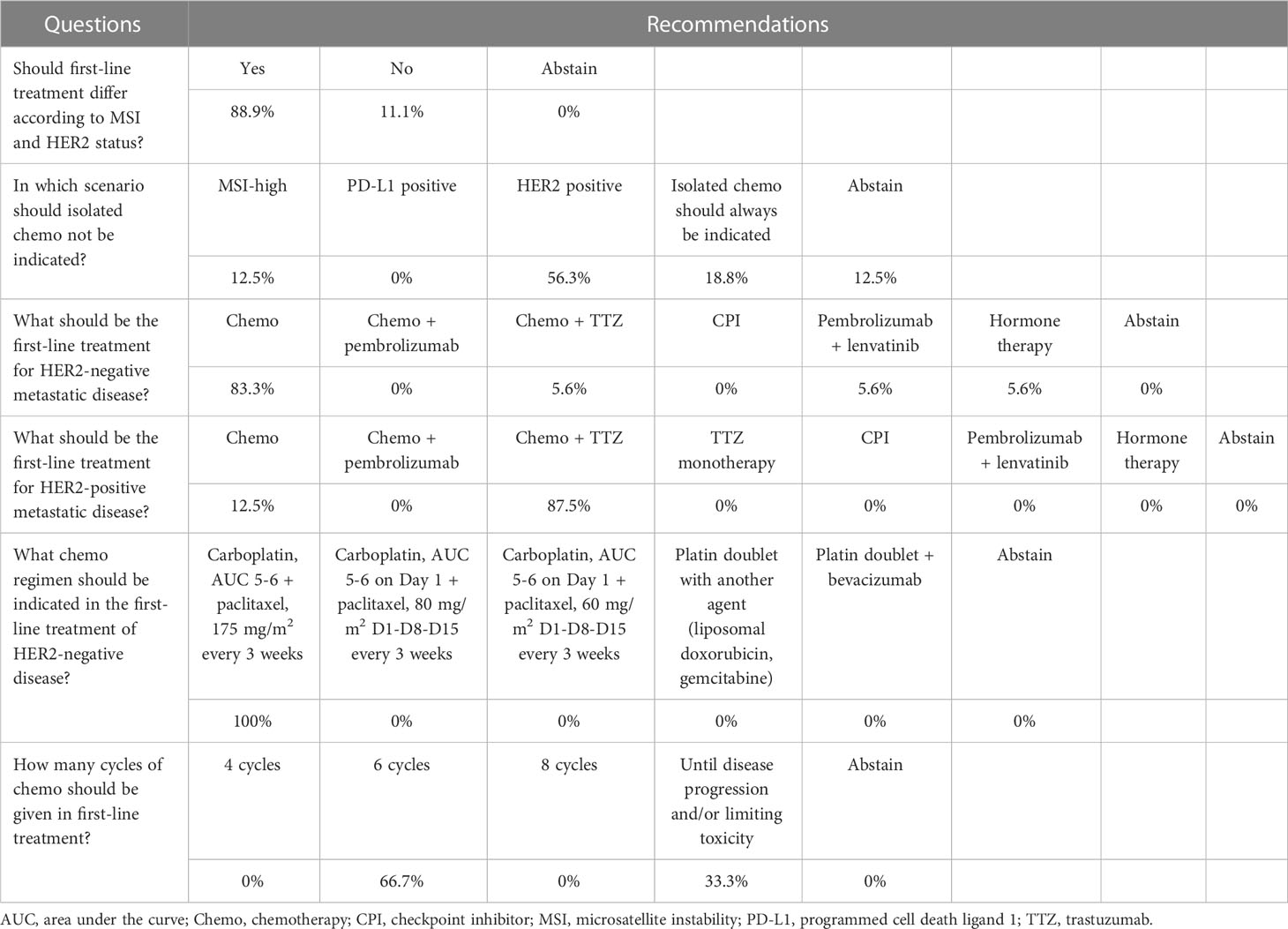
Table 2 Questions related to first-line treatment.
Second-line treatment
A total of 33 questions addressed issues related to second-line treatment. The first three of these questions have their corresponding recommendations shown pictorially in Figure 1, whereas the remaining 30 questions are shown in Table 3. Although the three questions depicted in Figure 1 had only majority vote for one single answer, in all three cases two answers can be pooled to establish a consensus minimum duration of progression-free interval of 6 months before patients are re-exposed to carboplatin and paclitaxel after having stable disease or partial response to first-line treatment, and of 3 months after complete response.
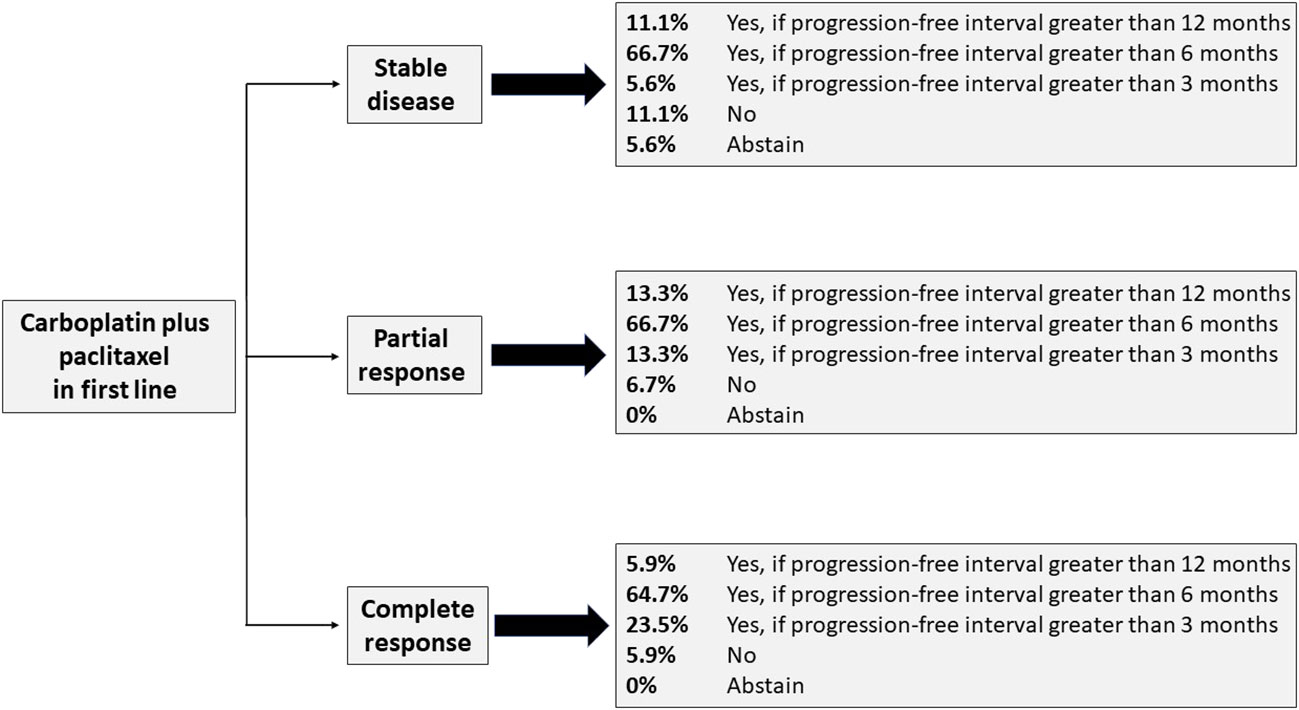
Figure 1 Recommendations for re-exposure to carboplatin and paclitaxel according to response to first-line therapy.
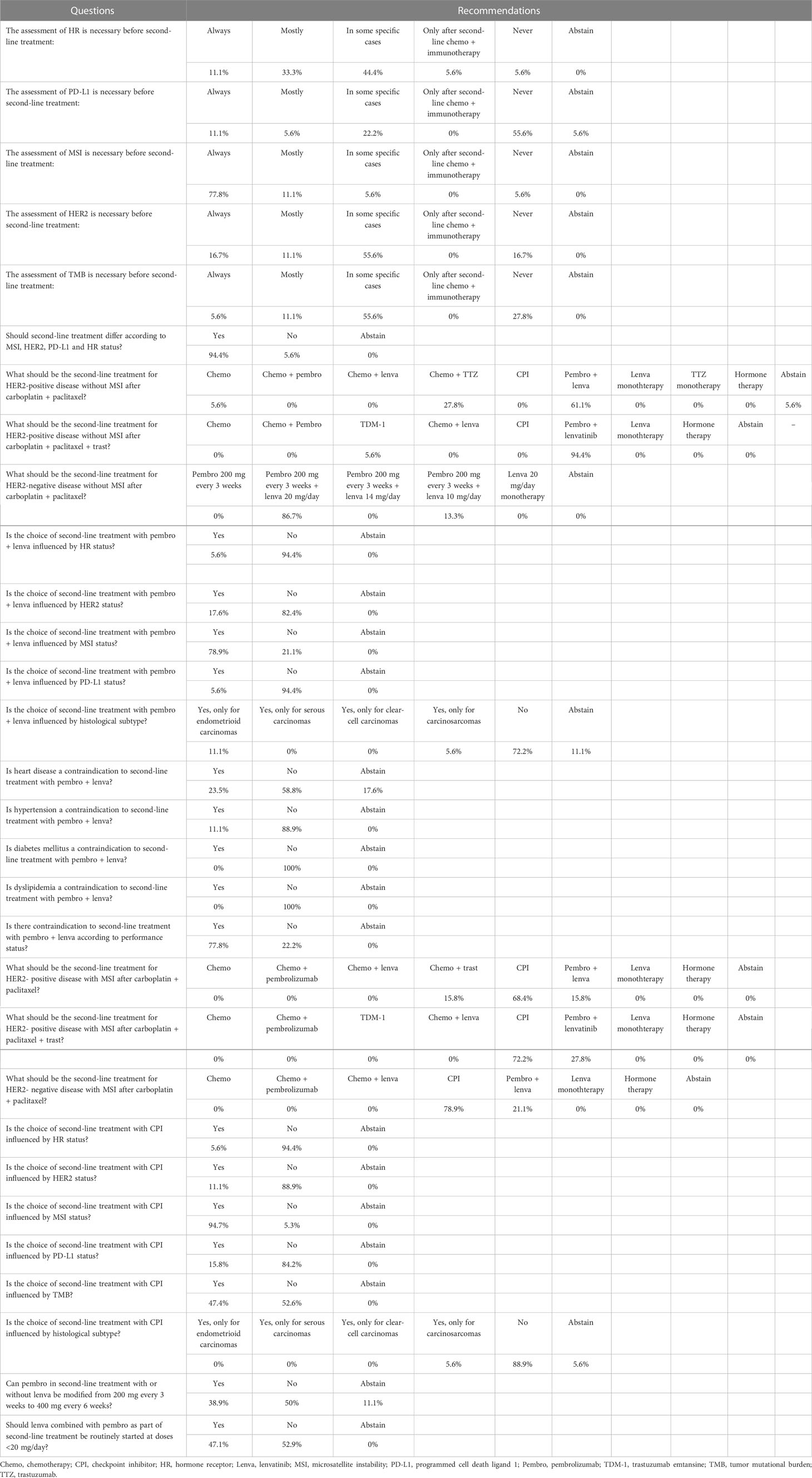
Table 3 Questions related to second-line treatment.
As shown in Table 3, consensus was reached for 18 of the remaining 30 questions pertaining to second-line treatment: (1) the assessment of MSI is necessary before second-line treatment; (2) the choice of second-line treatment should be guided by MSI, HER2, PD-L1 and hormone receptor status; (3) pembrolizumab plus lenvatinib should be the treatment of choice for HER2-positive disease without MSI after the regimen of carboplatin, paclitaxel and trastuzumab; (4) pembrolizumab, 200 mg every 3 weeks, plus lenvatinib, 20 mg/day, should be the second-line treatment for HER2-negative disease without MSI after carboplatin plus paclitaxel; the choice of second-line treatment with pembrolizumab plus lenvatinib should not be influenced by (5) hormone receptor status, (6) HER2 status or (7) PD-L1 status, but (8) should be influenced by MSI status; neither (9) hypertension nor (10) diabetes mellitus or (11) dyslipidemia are contraindications for second-line treatment with pembrolizumab plus lenvatinib, but (12) poor performance status is; (13) second-line treatment for HER2-negative disease with MSI after carboplatin plus paclitaxel should be an immune checkpoint inhibitor; the choice of second-line treatment with a checkpoint inhibitor should not be influenced by (14) hormone receptor status, (15) HER2 status, (16) PD-L1 status or (17) histological subtype, but (18) should be guided by MSI status.
Majority vote was present for 11 of 30 questions related to second-line treatment, whereas for one question there was less than majority vote (see Table 3). It should be noted, however, that for some of these questions the response options can be pooled in a manner that indicates a clear preference for somewhat similar interventions. This is the case, for example, of the need to assess hormone receptors before second-line treatment: 11.1% of panelists indicated that this should always be done, 33.3% that this should be done in most cases, and 44.4% that this should be done in specific cases. On the other hand, some questions with a majority vote indicated a clear dichotomy of opinions, such as whether the choice of second-line treatment with an immune checkpoint inhibitor should be influenced by tumor mutational burden; in this case, 47.4% of voters believe the choice would depend on that assessment, whereas 52.6% believe that it would not.
Treatment past two lines
Two questions addressed treatment beyond two lines. For the first, about what should be the choice after first-line treatment with carboplatin plus paclitaxel and second-line treatment with pembrolizumab plus lenvatinib, 82.4% of panelists recommended chemotherapy regimens other than carboplatin plus paclitaxel. For the question of how many lines of chemotherapy should a patient receive, regardless of histological subtype or biomarkers, 73.7% of voters indicated that the number of lines should not be fixed but rather guided by the continued presence of adequate performance status.
Discussion
To our knowledge, this is the first consensus meeting conducted in Brazil to address the management of advanced endometrial cancer. Previous work from our country has successfully addressed the surgical management of this disease, which is of increasing concern in many countries (3, 19). As many other middle-income countries, the healthcare system in Brazil is subject to accessibility constraints, and local practice guidelines are relatively scarce. We believe the current work can help medical oncologists to make decisions and base their practice on consensus recommendations. Nevertheless, consensus was present for only 25 of the 50 questions, in many cases as a reflection of current doubts in the literature. On the other hand, majority vote was present for an additional 23 questions, and less than majority vote was present for only three questions. Therefore, for the vast majority of issues addressed by the panel, there seems to be a sufficient level of agreement among members to guide clinical practice.
The classification of endometrial tumors has been predominantly based on morphology, with increasing use of ancillary testing, such as immunohistochemistry. Moreover, molecular subtyping increasingly provides prognostic insight and helps the practicing clinician in making treatment decisions (8, 10, 17, 20). Importantly, randomized trials – such as Postoperative Radiation Therapy in Endometrial Cancer (PORTEC) 4a and the RAINBO trials program – are ongoing to assess the validity of making adjuvant treatment decisions for early-stage disease based on molecular classification (21, 22). In the advanced-disease setting, molecular tumor features can already be used to guide therapy, particularly in uterine serous cancers and MSI tumors (10, 23–26). The vast majority of panel members consider the assessment of MSI and HER2 as essential for all patients before treatment initiation, with division of opinions about other markers, such as tumor mutational burden, p53, PD-L1, POLE, and hormone receptors (Table 1). Likewise, there is a predominant view that molecular markers, particularly MSI and HER2, should guide second-line therapy (Table 2). It should be noted that POLE mutations are identified with the use of sequencing, which may not be widely available. POLE and p53 are important to define molecular classification, but they do not yet influence the choice of treatment (27). PD-L1 proved to be a predictor of response in other tumors, such as lung cancer (28), but it did not influence therapeutic responses with immunotherapy in the treatment of endometrial cancer (29). Furthermore, the assessment of tumor mutational burden may be restricted to large referral centers, and up to now it has not been shown to influence treatment choices or prognostic assessment among patients with endometrial cancer (30).
The current results indicate consensus among panel members that patients with HER2-positive tumors benefit from the addition of trastuzumab to first-line therapy with carboplatin and paclitaxel. Even though the evidence in the literature is restricted to uterine serous tumors (15, 23), and based on a phase 2 trial with 61 patients, the current panel indicates HER2 testing as an essential step in patients who are candidates to first-line therapy and a preference for adding trastuzumab to such treatment, thus increasing progression-free survival (Table 2) (23). For all other endometrial tumors, the literature suggests, and the panel indicates by consensus, that carboplatin plus paclitaxel remains the standard of care in the first line, with a median progression-free survival of 13 months and overall survival of 37 months (31). Of note, recent results indicate that the regimen of carboplatin plus paclitaxel is also the standard of care for uterine carcinosarcoma (32).
Re-exposure to carboplatin plus paclitaxel is indicated by the panel – and corroborated by a retrospective study (33) – when the progression-free interval is at least 6 months, but a shorter interval is considered appropriate for patients with a complete response to first-line therapy (Figure 1). Indeed, the panel recommends by consensus that chemotherapy regimens other than carboplatin plus paclitaxel be used after failure of first-line treatment with this regimen and failure of second-line treatment with pembrolizumab plus lenvatinib. As suggested by several of the panel recommendations for second-line therapy, the latter regimen seems to be the currently preferred option in second line for patients without MSI, even for those with HER2-positive disease, regardless of previous treatment with trastuzumab (Table 2). In KEYNOTE-775, a phase 3 trial, the combination of pembrolizumab plus lenvatinib improved the objective response rate, progression-free survival, and overall survival, regardless of MSI status, when compared with chemotherapy of physician’s choice in patients with one or two prior lines of therapy (34), thus confirming results from a previous single-arm trial (KEYNOTE-146) (29, 35). The latter results led to the approval of this combination in several countries, including Brazil, and to the design of an ongoing phase 3 trial in the first line, in comparison with carboplatin plus paclitaxel (36).
The panel addressed issues related to the toxicity of the combination of pembrolizumab plus lenvatinib and expressed greater concern with its use in patients with poor performance status or with heart disease; on the other hand, there is little concern for patients with hypertension, dyslipidemia, or diabetes mellitus (Table 3). The toxicity associated with this combination includes hypertension, fatigue, nausea/vomiting, diarrhea, decreased appetite, weight loss, hypothyroidism, hand-foot syndrome, musculoskeletal pain, stomatitis, and proteinuria (34, 35, 37). These adverse reactions may usually be managed with supportive care medications and judicious lenvatinib dose modifications (37).
As in other tumor types, the role of immunotherapy is expanding in endometrial cancer. Single-agent checkpoint inhibitors are also an option among patients with disease progression after the first line. Pembrolizumab was approved in 2017 for patients with mismatch repair deficiency or MSI-high tumors (including endometrial cancer), based on aggregate results from five single-arm trials (38). Subsequent results from the single-arm trial, KEYNOTE-158, among patients with previously treated, advanced endometrial cancer with mismatch repair deficiency or MSI-high, have shown an objective response rate of 48%, median progression-free survival of 13.1 months, and median overall survival that was not reached at the time of reporting (24). Other checkpoint inhibitors are under investigation for advanced endometrial cancer, and these include dostarlimab, recently approved in the US for recurrent, mismatch repair deficiency tumors based on results from the ongoing GARNET trial (26). Of note, the panel indicated a preference, at least by majority vote, for the use of a checkpoint inhibitor as the preferred option for second-line treatment of HER2-negative or HER2-positive disease with MSI, whether or not trastuzumab has been used in the first line (Table 3).
There seems to be no strong preference for the use of hormone therapy by the current panel, considering the settings investigated and the questions posed to members. Nevertheless, it should be noted that patients with advanced or recurrent endometrioid endometrial tumors with low-volume disease and a long disease-free interval, especially if they have insufficient conditions for chemotherapy, can be treated with progesterone; this is even more important for tumors that are positive for hormone receptors, particularly if they are grade 1 or 2, even though no randomized trials have compared this approach versus chemotherapy in the first line (10, 15). Likewise, hormone therapy can be an option for patients with more limited performance status or for treatment past the first line in selected cases.
Despite its findings and potential relevance for practicing clinicians, our consensus has some limitations, including (1) the fact that not all 20 physicians answered the 50 questions asked, (2) the need to rely on scientific literature with lower level of evidence and/or grades of recommendation (e.g., phase 2 trials) to define consensus regarding some of the settings for which no higher level exists, and (3) the amalgamation of recommendations without a distinction between public and private healthcare settings in our country.
Conclusion
Given that at least majority vote was present for 47 of the 50 questions addressed by the panel, we believe that the current work can help medical oncologists treating patients with endometrial cancer in Brazil and in other countries with similar healthcare environments to make decisions informed by the current recommendations, which are based on the scientific literature and expert opinion. Nevertheless, several questions regarding the management of these patients remain, either because of knowledge gaps in the literature or because some topics have not been addressed by the current panel. Therefore, continued effort is needed to ensure adequate dissemination and implementation of current best practices in this and other fields in oncology.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
All authors contributed equally to the development of the project and the writing of the paper. The panel was coordinated by a committee composed of three of the current authors (DA, AG and FM). All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors thank Dendrix Research Ltd, for medical writing support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1133277/full#supplementary-material
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA: Cancer J Clin (2023) 73(1):17–48. doi: 10.3322/caac.21763
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
3. Lortet-Tieulent J, Ferlay J, Bray F, Jemal A. International patterns and trends in endometrial cancer incidence, 1978-2013. J Natl Cancer Inst (2018) 110(4):354–61. doi: 10.1093/jnci/djx214
4. Santos MO, Lima FCS, Martins LFL, Oliveira JFP, Almeida LM, Cancela MC. Estimativa de incidência de câncer no brasil, 2023-2025. Rev Bras Cancerol (2023) 69(1). doi: 10.32635/2176-9745.RBC.2023v69n1.3700
5. Paulino E, de Melo AC, Silva-Filho AL, Maciel LF, Thuler LCS, Goss P, et al. Panorama of gynecologic cancer in Brazil. JCO Glob Oncol (2020) 6:1617–30. doi: 10.1200/GO.20.00099
6. Paulino E, Nogueira-Rodrigues A, Goss PE, Faroni L, Guitmann G, Strasser-Weippl K, et al. Endometrial cancer in Brazil: Preparing for the rising incidence. Rev Bras Ginecol Obstet. (2018) 40(10):577–9. doi: 10.1055/s-0038-1673644
7. Onstad MA, Schmandt RE, Lu KH. Addressing the role of obesity in endometrial cancer risk, prevention, and treatment. J Clin Oncol (2016) 34(35):4225–30. doi: 10.1200/JCO.2016.69.4638
8. Baiden-Amissah REM, Annibali D, Tuyaerts S, Amant F. Endometrial cancer molecular characterization: The key to identifying high-risk patients and defining guidelines for clinical decision-making? Cancers (Basel). (2021) 13(16):3988. doi: 10.3390/cancers13163988
9. Roberts ME, Aynardi JT, Chu CS. Uterine leiomyosarcoma: A review of the literature and update on management options. Gynecol Oncol (2018) 151(3):562–72. doi: 10.1016/j.ygyno.2018.09.010
10. Lu KH, Broaddus RR. Endometrial cancer. N Engl J Med (2020) 383(21):2053–64. doi: 10.1056/NEJMra1514010
11. Bray F, Dos Santos Silva I, Moller H, Weiderpass E. Endometrial cancer incidence trends in Europe: Underlying determinants and prospects for prevention. Cancer Epidemiol Biomarkers Prev (2005) 14(5):1132–42. doi: 10.1158/1055-9965.EPI-04-0871
12. Reeves GK, Pirie K, Beral V, Green J, Spencer E, Bull D, et al. Cancer incidence and mortality in relation to body mass index in the million women study: cohort study. BMJ (2007) 335(7630):1134. doi: 10.1136/bmj.39367.495995.AE
13. Islami F, Goding Sauer A, Gapstur SM, Jemal A. Proportion of cancer cases attributable to excess body weight by US state, 2011-2015. JAMA Oncol (2019) 5(3):384–92. doi: 10.1001/jamaoncol.2018.5639
14. Constantine GD, Kessler G, Graham S, Goldstein SR. Increased incidence of endometrial cancer following the women’s health initiative: An assessment of risk factors. J Womens Health (Larchmt). (2019) 28(2):237–43. doi: 10.1089/jwh.2018.6956
15. Crosbie EJ, Kitson SJ, McAlpine JN, Mukhopadhyay A, Powell ME, Singh N. Endometrial cancer. Lancet (London England). (2022) 399(10333):1412–28. doi: 10.1016/S0140-6736(22)00323-3
16. Cancer Genome Atlas Research N, Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, et al. Integrated genomic characterization of endometrial carcinoma. Nature (2013) 497(7447):67–73. doi: 10.1038/nature12325
17. Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. (2021) 31(1):12–39. doi: 10.1136/ijgc-2020-002230
18. Rutten H, Verhoef C, van Weelden WJ, Smits A, Dhanis J, Ottevanger N, et al. Recurrent endometrial cancer: Local and systemic treatment options. Cancers (Basel) (2021) 13(24):6275. doi: 10.3390/cancers13246275
19. Ribeiro R, Fontes Cintra G, Barrozo A, Tieko Tsunoda A, Pupo Nogueira A, Andreazza Laporte G, et al. Brazilian Society of surgical oncology guidelines for surgical treatment of endometrial cancer in regions with limited resources. J Surg Oncol (2020) 121(5):730–42. doi: 10.1002/jso.25797
20. Wang M, Hui P. A timely update of immunohistochemistry and molecular classification in the diagnosis and risk assessment of endometrial carcinomas. Arch Pathol Lab Med (2021) 145(11):1367–78. doi: 10.5858/arpa.2021-0098-RA
21. van den Heerik A, Horeweg N, Nout RA, Lutgens L, van der Steen-Banasik EM, Westerveld GH, et al. PORTEC-4a: international randomized trial of molecular profile-based adjuvant treatment for women with high-intermediate risk endometrial cancer. Int J Gynecol Cancer. (2020) 30(12):2002–7. doi: 10.1136/ijgc-2020-001929
22. Kasius JC, Pijnenborg JMA, Lindemann K, Forsse D, van Zwol J, Kristensen GB, et al. Risk stratification of endometrial cancer patients: FIGO stage, biomarkers and molecular classification. Cancers (Basel) (2021) 13(22): 5848. doi: 10.3390/cancers13225848
23. Fader AN, Roque DM, Siegel E, Buza N, Hui P, Abdelghany O, et al. Randomized phase II trial of carboplatin-paclitaxel versus carboplatin-Paclitaxel-Trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/neu. J Clin Oncol (2018) 36(20):2044–51. doi: 10.1200/JCO.2017.76.5966
24. O’Malley DM, Bariani GM, Cassier PA, Marabelle A, Hansen AR, De Jesus Acosta A, et al. Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: Results from the KEYNOTE-158 study. J Clin Oncol (2022) 40(7):752–61. doi: 10.1200/JCO.21.01874
25. Oaknin A, Gilbert L, Tinker AV, Brown J, Mathews C, Press J, et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-h) or proficient/stable (MMRp/MSS) endometrial cancer: Interim results from GARNET-a phase I, single-arm study. J Immunother Cancer (2022) 10(1):e003777. doi: 10.1136/jitc-2021-003777
26. Oaknin A, Tinker AV, Gilbert L, Samouelian V, Mathews C, Brown J, et al. Clinical activity and safety of the anti-programmed death 1 monoclonal antibody dostarlimab for patients with recurrent or advanced mismatch repair-deficient endometrial cancer: A nonrandomized phase 1 clinical trial. JAMA Oncol (2020) 6(11):1766–72. doi: 10.1001/jamaoncol.2020.4515
27. León-Castillo A, de Boer SM, Powell ME, Mileshkin LR, Mackay HJ, Leary A, et al. Molecular classification of the PORTEC-3 trial for high-risk endometrial cancer: Impact on prognosis and benefit from adjuvant therapy. J Clin Oncol (2020) 38(29):3388–97. doi: 10.1200/JCO.20.00549
28. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-Positive non-Small-Cell lung cancer. N Engl J Med (2016) 375(19):1823–33. doi: 10.1056/NEJMoa1606774
29. Makker V, Taylor MH, Aghajanian C, Oaknin A, Mier J, Cohn AL, et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer. J Clin Oncol (2020) 38(26):2981–92. doi: 10.1200/JCO.19.02627
30. Vanderwalde A, Spetzler D, Xiao N, Gatalica Z, Marshall J. Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients. Cancer Med (2018) 7(3):746–56. doi: 10.1002/cam4.1372
31. Miller DS, Filiaci VL, Mannel RS, Cohn DE, Matsumoto T, Tewari KS, et al. Carboplatin and paclitaxel for advanced endometrial cancer: Final overall survival and adverse event analysis of a phase III trial (NRG Oncology/GOG0209). J Clin Oncol (2020) 38(33):3841–50. doi: 10.1200/JCO.20.01076
32. Powell MA, Filiaci VL, Hensley ML, Huang HQ, Moore KN, Tewari KS, et al. Randomized phase III trial of paclitaxel and carboplatin versus paclitaxel and ifosfamide in patients with carcinosarcoma of the uterus or ovary: An NRG oncology trial. J Clin Oncol (2022) 40(9):968–77. doi: 10.1200/JCO.21.02050
33. Rubinstein M, Halpenny D, Makker V, Grisham RN, Aghajanian C, Cadoo K. Retreatment with carboplatin and paclitaxel for recurrent endometrial cancer: A retrospective study of the memorial Sloan Kettering cancer center experience. Gynecol Oncol Rep (2019) 28:120–3. doi: 10.1016/j.gore.2019.04.002
34. Makker V, Colombo N, Herráez AC, Santin AD, Colomba E, Miller DS, et al. Lenvatinib plus Pembrolizumab for Advanced Endometrial Cancer. N Engl J Med (2022) 386(5):437–48. doi: 10.1056/NEJMoa2108330
35. Makker V, Rasco D, Vogelzang NJ, Brose MS, Cohn AL, Mier J, et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer: an interim analysis of a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol (2019) 20(5):711–8. doi: 10.1016/S1470-2045(19)30020-8
36. Marth C, Tarnawski R, Tyulyandina A, Pignata S, Gilbert L, Kaen D, et al. Phase 3, randomized, open-label study of pembrolizumab plus lenvatinib versus chemotherapy for first-line treatment of advanced or recurrent endometrial cancer: ENGOT-en9/LEAP-001. Int J Gynecol Cancer. (2022) 32(1):93–100. doi: 10.1136/ijgc-2021-003017
37. Makker V, Taylor MH, Oaknin A, Casado Herraez A, Orlowski R, Dutta L, et al. Characterization and management of adverse reactions in patients with advanced endometrial carcinoma treated with lenvatinib plus pembrolizumab. Oncologist (2021) 26(9):e1599–e608. doi: 10.1002/onco.13883
Keywords: endometrial cancer, consensus, Brazil, metastatic, recurrence
Citation: de Andrade DAP, Guimarães APG, de Melo AC, Nogueira-Rodrigues A, Gomes LM, Scaranti M, Maia JML, Morelle AM, Santos CAdAL, Souza CdP, de Freitas D, Callegaro Filho D, Paulino E, Júnior EWA, Pimenta JM, Santos MBd, de Almeida MS, Souza RP, Cabral S and Maluf FC (2023) Management of patients with recurrent/metastatic endometrial cancer: Consensus recommendations from an expert panel from Brazil. Front. Oncol. 13:1133277. doi: 10.3389/fonc.2023.1133277
Received: 28 December 2022; Accepted: 23 February 2023;
Published: 09 March 2023.
Edited by:
Sarah M. Temkin, National Institutes of Health (NIH), United StatesReviewed by:
Elina Urpilainen, Oulu University Hospital, FinlandCasey Cosgrove, The Ohio State University, United States
Copyright © 2023 de Andrade, Guimarães, de Melo, Nogueira-Rodrigues, Gomes, Scaranti, Maia, Morelle, Santos, Souza, de Freitas, Callegaro Filho, Paulino, Júnior, Pimenta, Santos, de Almeida, Souza, Cabral and Maluf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diocésio Alves Pinto de Andrade, ZGlvY2VzaW9AeWFob28uY29t