
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 23 March 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1130595
This article is part of the Research TopicNovel Targeted Drugs for Indolent Lymphoid MalignanciesView all 6 articles
 Anna Wolska-Washer1,2†
Anna Wolska-Washer1,2† Tadeusz Robak3,4*†
Tadeusz Robak3,4*†Zanubrutinib (BGB-3111, Brukinsa®, BeiGene) is a next-generation irreversible inhibitor of Bruton’s tyrosine kinase (BTK), developed by BeiGene in 2012 for the treatment of B-cell malignancies. It was designed to minimize off-target inhibition of TEC- and EGFR-family kinases. Zanubrutinib is more selective than ibrutinib for BTK versus EGFR, FGR, FRK, HER2, HER4, ITK, JAK3, LCK, BLK and TEC. In addition, compared to ibrutinib, zanubrutinib has improved oral absorption and better target occupancy. Zanubrutinib demonstrated a lower incidence of off-target toxicities and reduced severity than ibrutinib. Moreover, zanubrutinib is similar to acalabrutinib, with less activity against TEC and ITK. The preliminary phase 1 results suggest that zanubrutinib has clinical activity and the drug is well tolerated in patients with B-cell lymphoid malignancies. Recent clinical trials have found it to demonstrate excellent efficacy and good tolerability in patients with chronic lymphocytic leukemia (CLL), Waldenstrom macroglobulinemia (WM) and mantle cell lymphoma (MCL). In recent phase 3 studies, zanubrutinib was compared with ibrutinib in patients with relapsed/refractory (R/R) MW and RR CLL. In both trials, zanubrutinib was found to demonstrate clinically meaningful advantages in safety and tolerability over ibrutinib; in particular, it was associated with a lower risk of atrial fibrillation/flutter and major bleeding events. In the recent SEQUOIA study, comparing zanubrutinib with bendamustine and rituximab (BR) in patients with previously untreated CLL, zanubrutinib significantly improved progression-free survival versus BR, with an acceptable safety profile consistent with previous studies. Zanubrutinib also demonstrated good activity and tolerability in patients with R/R MCL, marginal zone lymphoma and follicular lymphoma. Trials examining the efficacy and safety of the combination of zanubrutinib with obinutuzumab venetoclax and other drugs are ongoing. This review summarizes the clinical efficacy and safety of zanubrutinib in lymphoid malignancies.
Bruton’s tyrosine kinase (BTK) is a major source of pathogenic signaling in numerous lymphoproliferative malignancies (1–12) (Table 1). The BTK gene encodes a 659-amino acid, protein-tyrosine kinase with several domains (Pleckstrin homology, Tec homology, SRC homology, catalytic domain) (13). The name is attributed to Ogden C Bruton, who first reported that mutations of BTK and the resulting lack of appropriate signaling resulted in X-linked agammaglobulinemia with impaired B lymphocyte development and function (14). The activity of BTK has been found to be implicated in the development and propagation of various B-cell lymphoid malignancies (15, 16). Therefore, BTK function blockage has become an attractive therapeutic option in B-cell malignancies, as well as autoimmune diseases (14).
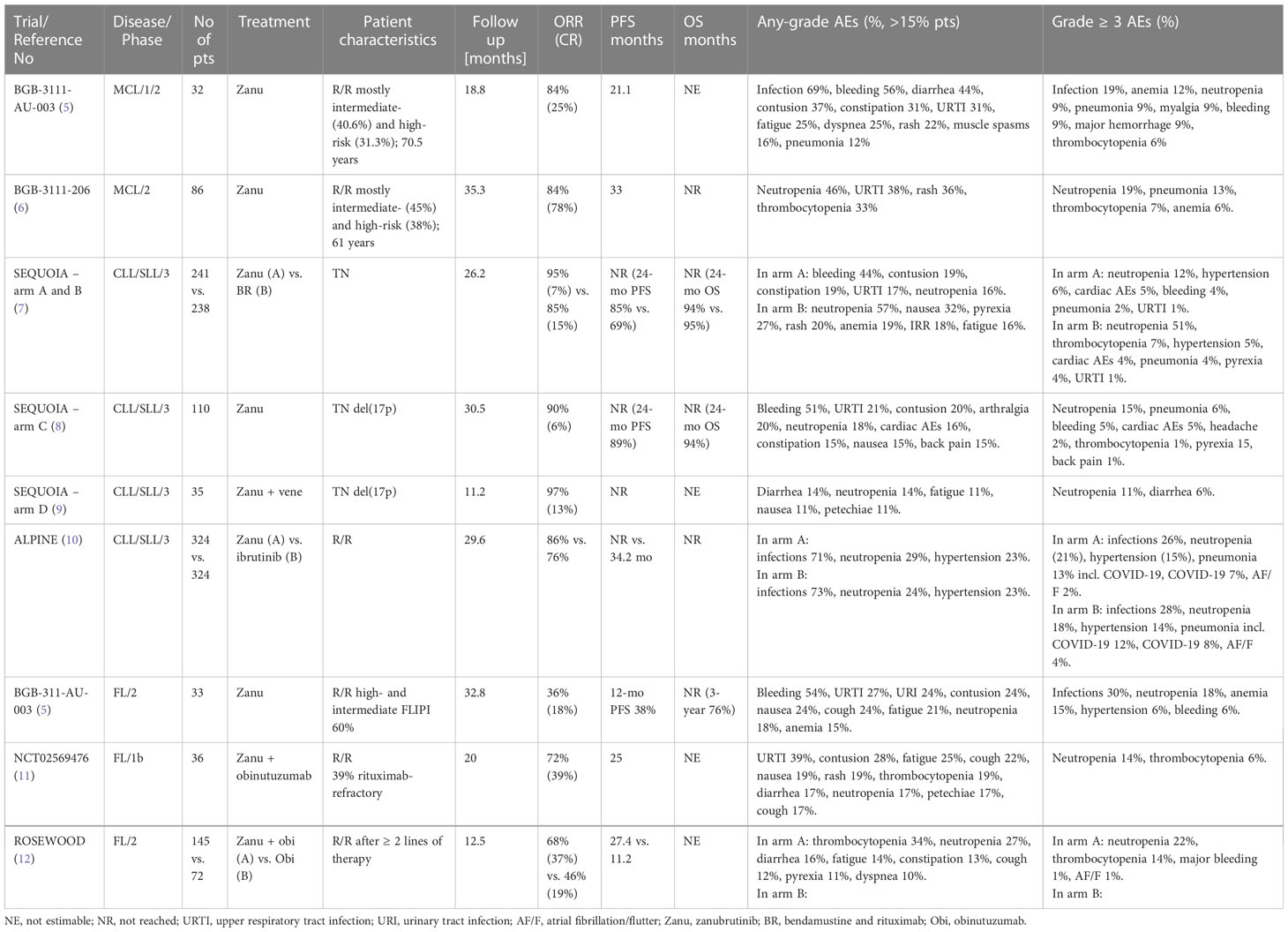
Table 1 Clinical trials of zanubrutinib in B-cell lymphoid malignancies.
The first-in-class BTK inhibitor approved for use by the US Food and Drug Administration (FDA) was ibrutinib (PCI-32765, Imbruvica, Janssen), which was initially registered in November 2013 for relapsed/refractory (R/R) mantle cell lymphoma (MCL) and in February 2014 for R/R chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) (17). Soon the indications also included Waldestrom macroglobulinemia (WM), marginal zone lymphoma (MZL) and recently chronic graft-versus-host disease (GVHD). Ibrutinib binds covalently to a cysteine residue at the 481 amino acid position on BTK and blocks the subsequent downstream signal transduction (18). However, ibrutinib is not a selective BTK inhibitor, and its off-target action results in a number of side effects (19). Its capacity to bind kinases with Cys481 residues and other without such domains leads to several specific side effects, i.e. skin rash (EGFR, SRC kinases), bleeding (BTK/Tec kinases), infectious complications (ITK kinases), headache and atrial fibrillation (SRC kinases) (20–23). The second generation of BTK inhibitors, acalabrutinib and zanubrutinib, have been designed to reduce the off-target activity of ibrutinib and yet enhance efficacy (24).
Zanubrutinib (BGB-3111, Brukinsa®, BeiGene USA, Inc., San Mateo, CA, USA) is an orally-available, second-generation BTK inhibitor (25, 26). It binds covalently to the same Cys481 residue of BTK as ibrutinib, but shows increased specificity with decreased inhibition of other kinases i.e. EGFR, HER2, ITK, JAK3, TEC, BMX and BLK (27). The maximum serum concentration is achieved two hours after a single oral administration, with the area under the curve (AUC) depending on the dose (28). The half maximal inhibitory concentration (IC50) was only 0.3 nM and the median BTK occupancy in the nodal samples was 95% with 320mg QD and 100% with 160mg BID. The latter dose was chosen for further investigation. This review presents the current state of knowledge regarding the use of zanubrutinib in lymphoid malignancies including MCL, WM, CLL/SLL and other diseases.
Zanubrutinib was first granted approval in November 2019 by the FDA for the treatment of patients with R/R MCL. The decision was based on the results of a phase 1/2 trial BGB-3111-AU-003 (NCT02343120) and a phase 2 clinical trial BGB-3111-206 (NCT03206970) (Table 1) (5, 6). The phase 1/2 trial enrolled 32 patients with mostly intermediate- and high-risk MCL, who received a total daily dose of 320mg of zanubrutinib (6). Median follow-up was 18.8 months and the median time on treatment was 15.4 months. The primary reason for treatment discontinuation was disease progression (31.3%) and adverse events (AEs; 25%). The overall response rate (ORR) was 84%, with complete remission (CR) achieved in 25% of patients, and a median time to response (CR and partial response (PR) of 2.8 months. It was found that 160mg twice-daily administration was slightly more effective than 320mg once-daily dosing. The median progression-free survival (PFS) was 21.1 months and overall survival (OS) was 83% and 64.4% at 12 and 24 months, respectively. The phase 2 clinical trial included 86 patients who had received a median of two prior lines of treatment and were mostly high- and intermediate-risk (5). At a median follow-up of 18.4 months, the median number of 28-day cycles of treatment was 19.3 and nearly 40% of patients had discontinued therapy. The main reasons were progressive disease (46%) and AEs (15.4%). The ORR was 84% with 68.6% of subjects achieving CR, and the median time to response was 2.7 months. Overall, the treatment proved safe and well tolerated in both the abovementioned trials. The most common AEs of any grade were diarrhea (15.1 – 48.8%), upper respiratory tract infections (31.3 – 34.9%), contusion (4.7 – 37.5%) and constipation (31.3%). The grade ≥3 AEs of special interest included anemia (5.8 – 12.5%), neutropenia (9.4 – 19.8%), infections (18.8%), pneumonia (9.4 – 10.5%), myalgia (9.4%), thrombocytopenia (4.7 – 6.3%), bleeding (1.2 – 9.4%), major hemorrhage (1.2 – 9.4%), hypertension (3.1 – 3.5%), atrial fibrillation/flutter (AF/F; 3.1%), and tumor lysis syndrome (TLS; 6.3%). A longer follow-up (median 35.3 months) did not reveal an increase of the incidence of AEs, with 45.3% of patients continuing the treatment (29). The ORR was 83.7% and CR of 77.9%. Subgroup analysis identified better outcomes in patients < 65 years old, classic histology vs. blastoid histology, TP53 wild type, and Ki67 ≤ 30%. Median duration of response (DOR) was not reached. Median progression free survival (PFS) was 33 months and median OS was not reached. During the extended follow-up, no cases of AF/F, grade ≥3 cardiac AEs, second primary malignancies or tumor lysis syndrome (TLS) were reported. A pooled analysis of long-term outcomes showed that second-line treatment yielded greater benefits in terms of OS in R/R MCL compared to later-line zanubrutinib treatment (30). Given the data, zanubrutinib shows remarkable activity in a heavily-pretreated or elderly population. Standard first-line treatment regimens (R-CHOP, BR) for elderly patients ineligible for autoSCT give median PFS from 13 to 35 months. The outcomes in the ≥ 2-line setting are worse. Targeted agents i.e. BTKis combined with bcl-2 inhibitor and monoclonal antibodies might lead to favorable outcome, but still around 2 years of PFS (31).
Zanubrutinib is currently being evaluated in clinical trials in treatment-naïve (TN) MCL. A phase 3 study comparing zanubrutinib and rituximab treatment followed by zanubrutinib monotherapy to rituximab and bendamustine in transplant-ineligible patients started in 2019 and is planned to enroll 500 participants randomized 1:1 to two treatment arms (NCT04002297) (32). The rationale behind that combination was based on the outcome of patients with R/R MCL who received rituximab with ibrutinib (33). At a median follow-up of 16.5 months, the ORR was 88% with 44% CRs and 44% PRs. Zanubrutinib with its better specificity towards BTK does not hamper the rituximab-induced antibody-dependent cell-mediated cytotoxicity as much as ibrutinib, so such combination might be even more effective (34). Perhaps the addition of zanubrutinib to the standard of care R-CHOP/R-DHAP in younger newly-diagnosed patients could spare the necessity to consolidate the treatment with autologous stem cell transplantation (ASCT). The assumption is based on a randomized Triangle trial presented at ASH Annual Meeting in 2022 in 870 patients treated with ibrutinib as the addition to standard chemotherapy with or without ASCT, and followed by ibrutinib maintenance (35). The results demonstrated high efficacy with good tolerability of ibrutinib during the induction phase and maintenance without the ASCT with a 3-year failure-free survival (FFS) of 86% vs. 72% after the standard treatment followed by the ASCT. The analysis whether ASCT can be safely omitted in patients receiving BTKi is still ongoing.
Patients with MCL and TP53 mutations fare worse with standard chemoimmunotherapy with a median OS of 1.8 years (36). In a multicenter, investigator-initiated phase 2 BOVen trial zanubrutinib was evaluated in combination with obinutuzumab and venetoclax in previously untreated TP53 mutant MCL (36). At the time of presentation, 12 patients have been analyzed of the 25 total planned accrual. The grade 3 treatment-related AEs included infusion-related reaction (17%), neutropenia (8%) and elevation of transaminases (8%). Tumor lysis syndrome (TLS) was not observed. At a median follow up of 4 months (range 0 - 11 months), one patient has progressed and eleven patients remained on study in continued response. The preliminary results were promising, and eight out of ten evaluable patients achieved PET CR at cycle 3. Longer follow-up data are pending.
A phase 2 trial of treatment-naïve (TN) MCL young and fit patients (BRIDGE; NCT04736914), which started in China in 2021 examined the addition of zanubrutinib to three cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) alternating with three cycles of R-DHAOx (rituximab, cisplatin, cytarabine, and dexamethasone) followed by autologous stem cell transplantation (ASCT) and zanubrutinib maintenance for two years; it is planned to enroll 47 patients in the study.
Another approach involved the use of zanubrutinib plus rituximab (ZR) induction therapy until achieving CR or up to 12 cycles, followed by 4 cycles of R-DHAOx chemoimmunotherapy and zanubrutinib maintenance for one year in 17 TN MCL patients (37). Preliminary results indicate a CR rate of 88% after four cycles of ZR, with all patients having negative MRD in the bone marrow. The most common AEs were thrombocytopenia, rash, neutropenia, subcutaneous hemorrhage, and fatigue. The MRD status was found to be consistent with the imaging findings and might become a predictor of response in future trials. However, the data needs further analysis. The improved safety profile of zanubrutinib monotherapy is currently being tested in a phase 2 trial in patients with B-cell lymphoid malignancies previously treated and intolerant to ibrutinib or acalabrutinib (NCT04116437) (Table 2). The inability to use anticoagulants or gastric acid-reducing medication concurrently with acalabrutinib is one of the inclusion criteria.
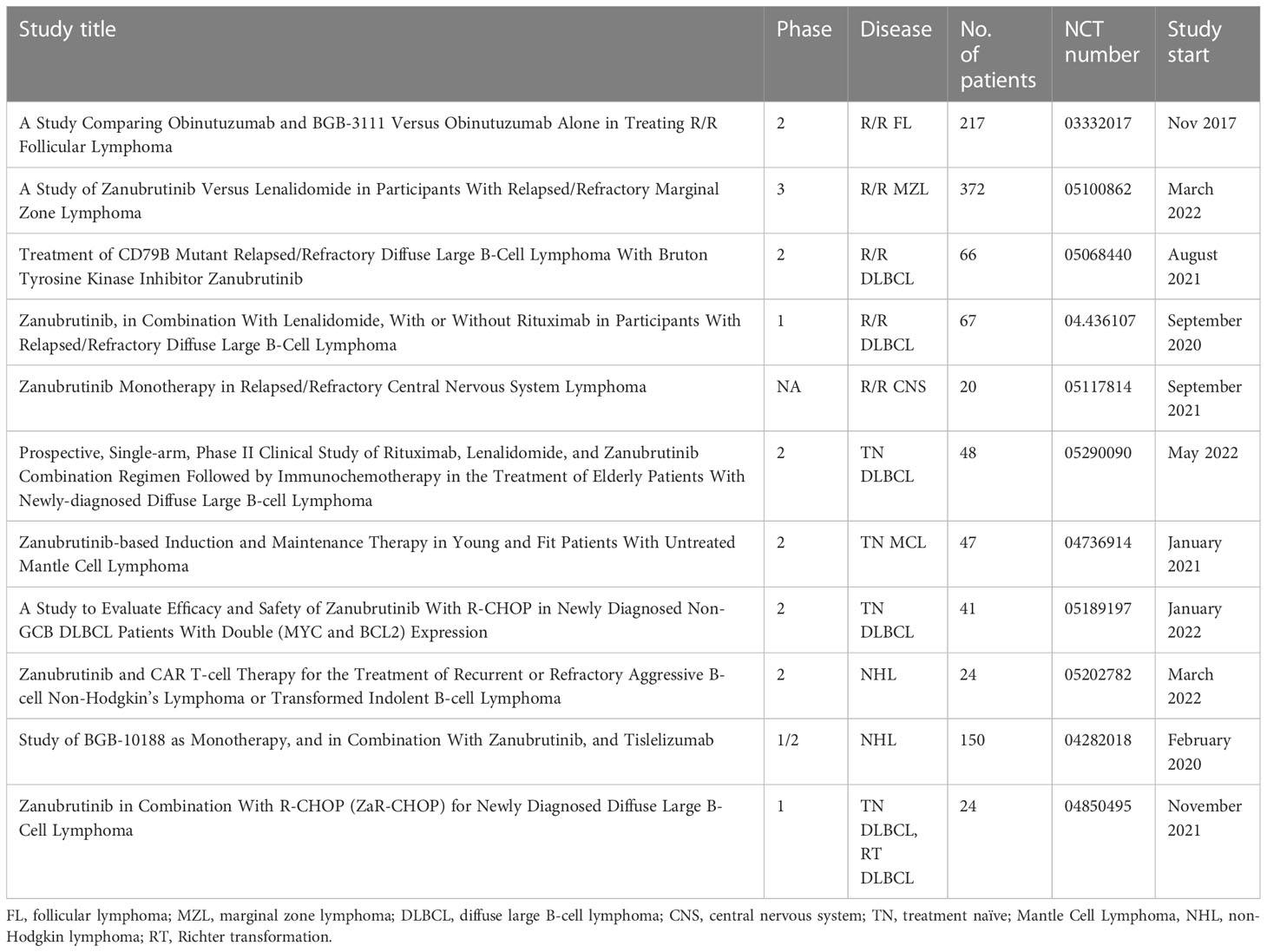
Table 2 Ongoing clinical studies with zanubrutinib in lymphoid malignancies.
Waldeström’s macroglobulinemia is a rare type of non-Hodgkin lymphoma (NHL) with a median age of 70 years at diagnosis (38). The majority of cases will present with the bone marrow as the primary site of involvement (62%). The treatment is administered in patients with active disease defined as i.e. worsening of cytopenias, spleno- or hepatomegaly, lymphadenopathy and general symptoms, as WM is a type of indolent lymphoma (39). The cells of WM present a constitutive activation of the B-cell receptor (BCR) signaling with over 90% of patients harboring the activating mutations in the adaptor protein MYD88 (MYD88L265P), and another 30% to 40% of patients having an additional mutation in the chemokine receptor CXCR4 (CXCR4WHIM) (40). Patients with wild-type MYD88 and/or mutated CXCR4 have poorer outcomes. Other mutations downstream of BTK and interleukin-1 receptor-associated kinase (IRAK) induce nuclear factor kB (NF-kB) activation and resemble those found in diffuse large B-cell lymphoma (41).
Probably the greatest single-agent activity in WM is demonstrated by the Bruton’s tyrosine kinase inhibitor ibrutinib (42, 43). The final results of the iNNOVATE phase 3 clinical trial in rituximab-sensitive patients with TN WM or R/R WM showed that median PFS was not reached in the ibrutinib plus rituximab group, compared to 20.3 months for those on rituximab only (44). The results were independent of prior treatment status, MYD88 and CXCR4 mutation status, or key patient characteristics. A substudy analysis found that single agent ibrutinib administered to patients who failed to achieve any response or relapsing < 12 months after their last rituximab-based treatment demonstrated an overall median PFS of 39 months (45). Patients with MYD88L265P/CXCR4WHIM and MYD88L265P/CXCR4WT subtypes achieved median PFS of 18 months and not reached, respectively. Therefore, BTK inhibition is an interesting option in WM. The first-in-human phase 1/2 study of zanubrutinib was BGB-3111 AU-003 in patients with TN or R/R WM (46). The dose chosen was 160mg twice daily, based on the almost complete BTK occupancy. The study included 24 TN and 53 R/R BTKi-naïve WM patients. With respective median follow-ups of 23.5 and 36 months, the ORR was 100% in TN WM and 93.9% in R/R WM, and the major response rate (MRR; PR or better) was 87.5% and 79.6%, respectively. Median time to response was 2.8 months in both groups and median PFS was not reached in either group. However, there was no correlation between the depth of response with PFS. The treatment was well tolerated, and AEs included grade 1 contusion (32.5%), grade ≥3 neutropenia (15.6%), grade 3 anemia (9.1%), major hemorrhage (3.9%), AF/F (5.2%), grade 3 hypertension (3.9%), any-grade headache (18.2%), and grade 3 diarrhea (2.6%).
A direct comparison between ibrutinib and zanubrutinib was made in a phase 3 ASPEN trial in patients with R/R MYD88L265P WM or TN WM ineligible for standard immunochemotherapy (47). The primary end point was CR and a very good partial response (VGPR). A total of 201 patients were randomized. At a median follow-up of 19.4 months, a higher, but not statistically significant, rate of VGPR was observed for zanubrutinib vs ibrutinib (28% vs 19%, respectively), although no CRs were reported. Median time to achieve VGPR was 5.6 months for zanubrutinib vs 22.1 months for ibrutinib in TN WM, and 4.7 (zanubrutinib) vs 5.1 months (ibrutinib) for R/R MW. Median duration of response (DOR) and PFS were not reached, and approximately 85% of patients were progression free at 18 months. Zanubrutinib induced major responses in patients with CXCR4WHIM in 3.1 months vs 6.6 months for ibrutinib. Perhaps the most important result was the sustained reduction of the IgM concentration in favor of zanubrutinib which may lead to lower WM-related morbidity (48). A substudy analysis of the ASPEN trial was performed in a group of patients with wild-type MYD88 (MYD88WT) or inconclusive MYD88 (49). The study included 28 subjects in total: five TN and 23 R/R. At a median follow-up of 17.9 months, PFS and OS have not been reached. The ORR among the confirmed MYD88WT cases was 81%, with 27% desmonstrating VGPR and 50% of major responses. The most common any-grade AEs reported in the zanubrutinib arm were neutropenia in 29%, upper respiratory tract infection in 24%, and diarrhea in 21% of patients. The most common any-grade AEs in the ibrutinib arm were diarrhea (32%), upper respiratory tract infections (29%), contusion (24%), and muscle spasms (24%). Grade ≥3 hypertension and pneumonia were seen more often for ibrutinib vs. zanubrutinib. Grade ≥3 neutropenia was observed more often for zanubrutinib. Any grade and grade ≥3 AF/F was reported in 15% and 4% for ibrutinib compared to 2% and 0% for zanubrutinib. Zanubrutinib showed superiority in MYD88WTCXCR4WHIM cases over ibrutinib. Neither of the studied BTKis achieved CR which reflects the difficulty in eradicating WM even with targeted treatment. Perhaps combination therapies will help to obtain deeper responses. Venetoclax has been found to sensitize WM cells in vitro to BTKi by lowering the bcl-2-mediated signaling (50).
Zanubutinib was investigated in a combination with ixazomib and dexamethasone in a phase 2 clinical trial in twenty newly-diagnosed symptomatic patients with WM (NCT04463953) (51). The majority (70%) of patients were less than 65 years old, and had intermediate- (60%) and high-risk (20%) disease. The ORR was 100% and the median time to response was 3.7 months. All patients recovered their normal hemoglobin concentration, and measurable residual disease (MRD) was undetectable in two patients. The median follow-up was 12.3 months (range 5.4 – 23.4) and all subjects were alive at study data analysis. The treatment was well tolerated with few grade ≥ 3 AEs (rash and neutropenia). The study will publish updated results.
Given the rarity of WM and its indolent nature, it is difficult to demonstrate meaningful results as they are usually based on PFS. Standard therapies (BR, BDR, CDR) give PFS of about 6 years (52). Targeted therapies may offer MRD negativity so probably combination treatment options are the key to reach for long PFS. Other measurements such as the MRD status are therefore needed to predict the long term outcome.
Marginal zone lymphoma (MZL) represents about 5% to 15% of all non-Hodgkin lymphomas in the Western world (53). The survival of MZL cells depends on constitutive BCR signaling, and is mediated through a net of multiple kinases, including BTK (54). Ibrutinib proved its efficacy in MZL and has become a drug of choice in R/R MZL (55). In September 2021, zanubrutinib received accelerated approval for R/R MZL for patients who have received at least one anti-CD20-based treatment (56). The approval was based on two clinical trials. A phase 1/2 multicenter study BGB-3111-AU-003 (NCT02343120) included 20 patients with R/R MZL, with nine extranodal MZL, five nodal MZL, and six splenic MZL subtypes (57). The majority of patients had received rituximab-based monotherapy and the median number of lines of therapy was two. The most commonly reported AEs were diarrhea, contusion and rash (in 35%), upper respiratory tract infection and neutropenia (in 30%), nasopharyngitis and pyrexia (in 25.0%), and sinusitis, nausea, fatigue, and musculoskeletal pain (in 20%). The most common grade ≥ 3 AEs were neutropenia (20%), anemia (15%), thrombocytopenia (10%), and pyrexia (10%). Bleeding events of any grade were reported in 12 patients (60%). Grade ≥3 bleeding or CNS bleeding of any grade were reported in 2 patients. Grade 3 hypertension was reported in one patient, and atrial fibrillation/flutter was not observed. The ORR was 80% with CR 20%. The best ORR was achieved in nodal MZL (100%), compared to extranodal MZL (88.9%) and splenic MZL (50%). Median time to response was 2.8 months. At a median follow-up of 33.8 months, the estimated PFS and OS rates at 24 months were 72% and 83.9%, respectively. In a phase 2 MAGNOLIA trial (BGB-3111-214), a total of sixty-eight patients with R/R MZL were enrolled (58). With a median follow-up of 15.7 months, the ORR was 68.2% with CR 25.8%, and the ORR was similar among all MZL subtypes. The ORR in a group of elderly patients (≥75 years) was 94.4%. The median DOR and PFS were not reached, except in patients with increased LDH whose PFS was 15.5 months. Overall survival at 12 months was 95.3%. The most common AEs were diarrhea (22.1%), contusion (20.6%), constipation (14.7%). Any-grade neutropenia was reported in 13.2% of patients and grade ≥ 3 neutropenia was found in 10.3% of subjects. No patients experienced any major bleeding, and grade 3 atrial fibrillation and grade 2 atrial flutter were reported in two patients. In the final analysis of the trial, with a median follow-up of 28 months and a median duration of 24 months, 66 patients were evaluable for efficacy (59). The ORR was 64%, 76%, 66.7% and 50% in extranodal, nodal, splenic, and unknown subtypes, respectively. The CR rate ranged from 8.3% for splenic to 40% for extranodal MZL. The most common AEs were bruising (23.5%), diarrhea (22.1%), constipation (17.6%), arthralgia (14.7%), pyrexia (14.7%), upper respiratory tract infection (13.2%), abdominal pain and back pain (each 11.8%). The most common grade ≥3 AEs were neutropenia (8.8%) and COVID-19 pneumonia (5.9%). Patients who achieved good responses continue in a long-term extension study (NCT04170283). Despite the low rate of complete remissions in patients with MZL, zanubrutinib achieves high PFS and is a valuable option especially in this usually older population of patients. One must bear in mind possible side effects with long-term duration treatment and potential drug interactions.
Zanubrutinib proved successful as monotherapy in a series of phase 1/2 studies (BGB-3111-1002, BGB-3111-AU-003, BGB-3111-205) in TN and R/R CLL/SLL patients (28, 60, 61). A pooled analysis of the data of 211 patients (19 TN, and 192 R/R) identified an ORR of 95.4% (100% vs. 91% in the TN compared to the R/R group) (62). With a median follow-up of 12.9 months to 30.5 months, patients with one prior line of treatment achieved a 98.9% ORR, compared to 90.7% ORR for those with >1 prior therapies. Comparable efficacy was observed, irrespective of high-risk genomic aberrations, with a response being achieved by 86% to 100% of patients with del17p/TP53mut and 82% with unmutated IGHV. The median time to response was 2.8 months. The majority of responses were PRs (from 66.7% to over 80% of responses). The treatment was well tolerated and the most common all-grade AEs included neutropenia (up to 69.2%), thrombocytopenia (up to 42%), anemia (up to 30%), petechiae, purpura, or contusion (up to 35% in total), hematuria (up to 40%), and upper respiratory tract infection (up to 45%). The most common treatment-emergent grade ≥ 3 AEs were neutropenia (up to 44%), thrombocytopenia (up to 15.4%), and upper respiratory tract infection (up to 9.9%). Atrial fibrillation/flutter was reported in four patients overall in the three analyzed trials (62).
Given the promising results of the initial early phase trials, zanubrutinib was further studied in two phase 3 clinical trials in TN (SEQUOIA) and R/R (ALPINE) CLL patients (Table 1) (7, 8). The outcomes of these trials led to the approval of zanubrutinib by the FDA in January 2023 for the treatment of adult TN and R/R CLL/SLL patients. However, neither of them studied zanubrutinib in younger, fitter patients. Zanubrutinib is already present among the recommended therapeutic options regardless of the risk factors by the German Society for Hematology and Medical Oncology (DGHO; https://www.dgho.de/). The SEQUOIA study included 590 patients unsuitable for fludarabine-cyclophosphamide-rituximab treatment because of age ≥ 65 years, comorbidities assessed as more than six points on the Cumulative Illness Rating Scale (CIRS), creatinine clearance less than 70mL/min, or medical history of frequent infections (7). Between October 2017 and July 2019, patients without del(17p) were randomized to receive either zanubrutinib monotherapy or rituximab with bendamustine (BR), and subjects with del(17p) were assigned to a third arm with zanubrutinib monotherapy. The estimated 24-month PFS was 85.5% with zanubrutinib and 69.5% with BR, and no difference in OS between the two groups. No significant difference in PFS was observed in patients with mutated IGHV, and zanubrutinib was as effective as BR among patients with SLL or mutated TP53. The ORR was 94.6% with zanubrutinib, and 85.3% with BR, and most responses were PRs. Richter transformation occurred in 2% and less than 1% of patients in the zanubrutinib and the BR group. Seven and six percent of patients had died at data cutoff. In patients with del(17p), 14% had progressed or died at the median follow-up of 30.5 months, but the median PFS was not reached. The estimated 24-month PFS was 88.9%, and the estimated 24-month OS was 93.6%. The most common grade ≥ 3 AEs in both groups were neutropenia (11% to 15% with zanubrutinib and 58% with BR) and infections (16% with zanubrutinib and 19% with BR). Adverse events of special interest with zanubrutinib were also reported: AF/F in 3%, major bleeding events 5% to 7% (compared to 2% with BR) and second primary malignancies of any grade in approximately 13% to 22% (compared to 9% with BR). The concomitant use of anticoagulants was not prohibited. The zanubrutinib group, excluding patients with del(17p), experienced 16 deaths during the study, compared to 14 with the BR group. No sudden deaths were reported. An analysis of patient-reported outcomes at weeks 12 and 24 of therapy found that zanubrutinib treatment significantly improved general health score, physical and role functioning, and reduced diarrhea, fatigue and nausea/vomiting, compared to BR (63). However, one has to bear in mind that the patients randomized to zanubrutinib continued the treatment while BR patients would have completed the therapy at week 24.
Treatment with BTK inhibitors in continuous monotherapy may not be optimal, as most responses are PRs and only the minority of patients achieve CR (64). There are long-term safety concerns including cardiac events and the risk of rapid progression following BTKi cessation (65, 66). Some patients might find the ongoing need for therapy unacceptable and difficult to comply in real-life scenarios. One possible solution is to combine BTKis with other targeted therapeutic options to induce deeper responses that will allow for treatment discontinuation once appropriate level of disease control has been achieved, currently indicated by minimal residual disease (MRD). Given the excellent outcome of patients with del(17p) on zanubrutinib monotherapy, a non-randomized arm D of the SEQUOIA study was added for TN CLL patients and del(17p) (9). The treatment involved an initial three months of zanubrutinib followed by combination treatment with venetoclax up to 12-24 months, depending on the outcome including MRD status. At the first data cutoff in June 2021, 35 patients were enrolled and 31 reached the initial efficacy assessment. The ORR was 96.8%, with one patient having PD on combination therapy. The regimen was well tolerated with mostly neutropenia and diarrhea, and one worsening of preexisting AF. The trial was yet too immature to give data on the MRD.
In the second phase 3 ALPINE non-inferiority trial comparing zanubrutinib to ibrutinib in patients with R/R CLL/SLL, 652 patients were enrolled between November 2018 and December 2020 (10). The published interim analysis included 415 patients randomized to receive zanubrutinib (n=207) or ibrutinib (n=208). At a median follow-up of 15 months, a significantly higher ORR was observed with zanubrutinib compared to ibrutinib (78.3% vs. 62.5%, respectively). In patients with unfavorable risk factors: the ORR was 80.5% for zanubrutinib vs. 50% in del(17p)/TP53mut, 83.6% vs. 69.1% in del(11q). The PFS at 12 months was 94.9% with zanubrutinib and 84% with ibrutinib, also favorable for zanubrutinib in a subgroup with del(17p)/TP53mut (91.5% vs. 74.4%). Treatment discontinuation due to AEs was observed in 7.8% of patients on zanubrutinib compared to 13% on ibrutinib, and infections were the most common reason (2.9% in each arm). Adverse events of special interest reported in zanubrutinib and ibrutinib groups were: AF/F (2.5% vs. 10.1%), anemia (13.2% vs. 15.5%), major hemorrhage (2.9% vs. 3.9%), hypertension (16.7% vs. 16.4%), secondary primary malignancies (8.3% vs. 6.3%). With a median follow-up of 29.6 months at the final analysis per protocol, the PFS rate at 24 months was 78.4% for zanubrutinib and 65.9% for ibrutinib (10). Median PFS with zanubrutinib was not reached, and median PFS with ibrutinib was 34.2 months. Zanubrutinib also showed benefit in high-risk patients with longer PFS (HR: 0.52 [95% CI:0.30-0.88]). Moreover, patients who received zanubrutinib monotherapy reported improved key health-related quality of life endpoints including general health, physical functioning, fatigue, and diarrhea (67).
A phase 1 trial with zanubrutinib combined with obinutuzumab, administered until unacceptable toxicity or disease progression, was conducted in a cohort of 45 TN or R/R CLL/SLL patients (11). Among patients with CLL/SLL there were 49% with unmutated IGHV, 41% with del17p)/TP53mut, 26% with del(11q) and 23% with a complex karyotype. With a median follow-up of 29 months, the ORR was 100% for TN CLL/SLL, and 92% for R/R CLL/SLL patients, including 30% and 28% of CRs, respectively. In high-risk patients the ORR was 100% (TN) and 80% (R/R), with 50% (TN) and 20% (R/R)reaching CR. The median PFS was not reached, and the estimated event-free rate at 24 months was 90.4%. Three out of six TN patients who achieved CR were also MRD negative at the 10-4 detection limit. The most common grade ≥ 3 AEs were neutropenia (31.1%), pneumonia (8.9%), thrombocytopenia (6.7%). There were no cases of AF/F or major hemorrhage. Neutropenia occurred more often during the combination of ibrutinib and obinutuzumab in the iLLUMINATE study (36% of grade ≥ 3) (68). The question remains whether the combination of zanubrutinib and obinutuzumab will improve PFS, as no such advantage has been found for combined ibrutinib and rituximab therapy over ibrutinib monotherapy (69). Zanubrutinib is not yet approved for the treatment of CLL/SLL. However, due to its potency and selectivity it has already become one of the recommended options by the NCCN Guidelines Version 1.2023. Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma.
A different approach is currently being studied in a phase 2 clinical trial of the combination treatment with zanubrutinib, obinutuzumab and venetoclax, administered according to the MRD status in TN CLL/SLL patients (70). Thirty-nine patients were enrolled in this study. After a median follow-up of 25.8 months, 33 of 37 (89%) evaluable patients had undetectable MRD in the peripheral blood and bone marrow below the 10-4 limit, meaning that therapy could be stopped, after a median of ten cycles. After a median 15.8 months of observation after stopping treatment, 31 out of those 33 patients were still MRD-negative. With a median duration of treatment of 10 months, this combination was well tolerated with the most common all-grade AEs: thrombocytopenia (59%), fatigue (54%), neutropenia (51%; grade ≥ 3 18%), bruising (51%). The trial is currently recruiting patients with TP53-mutated MCL (NCT03824483) (Table 2).
The MRD assessment and/or the idea of guiding the therapy duration according to the MRD status in CLL is currently being studied in multiple trials. Resistance to targeted drugs may become an issue with subsequent relapses. Intermittent administration of therapy when treatment is stopped once the response has been achieved might prevent the otherwise inevitable emergence of drug resistance (see https://www.isrctn.com/ISRCTN51675454).
In addition to MCL, VM and CLL/SLL zanubrutinib has a potential in the treatment of other lymphoid malignancies including diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL).
Diffuse large B-cell lymphoma is one of the most common lymphoma subtypes in the adult population and its incidence increases with age (71). In addition, increasing age is associated with a higher incidence of comorbidities and inability to treat patients with sufficient intensity i.e. R-miniCHOP (72, 73). Bruton’s tyrosine kinase was found to be expressed in a substantial number of cases, especially in the non-germinal center B-cell-like (GCB) subtype (74). Moreover, BTK expression correlated positively with higher international prognostic index (IPI), and worse outcome after treatment with rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP). A chemotherapy-free regimen was studied in a phase 2 trial with the BTKi ibrutinib, combined with lenalidomide and rituximab (iR2) (75). In a group of 30 treatment-naïve unfit or frail patients over 75 years of age, the ORR was 66.7% with 56.7% of CRs. However, there was a 10% incidence of atrial fibrillation with the majority of cases being grade 3. Zanubrutinib was studied as monotherapy in a phase 2 study in 41 patients with R/R non-GCB DLBCL after a median of two prior treatment lines (76). At a median follow-up of 6.8 months, the ORR was 29.3% with 17.1% CR. Median PFS and OS were 2.8 and 8.4 months, respectively. The most common treatment emergent grade ≥ 3 AEs were neutropenia (n=3), pneumonia (n=2), abdominal (n=2), and death of unknown cause (n=2). There were no cases of AF/F, major hemorrhage or tumor lysis syndrome. A SMART study examined the effect of zanubrutinib combined with lenalidomide and rituximab as the sole 21-day regimen for newly-diagnosed elderly patients (6 – 8 cycles), or as the initial 2 - 3 cycles followed by chemotherapy, if the patient was unable to tolerate chemotherapy at the beginning, as the so called SMART-START approach (77). Median age in the SMART arm was 82, compared with 67 in the SMART-START arm. Eleven out of 31 patients were on zanubrutinib, 16 used ibrutinib, and four were on olerabrutinib. Chemotherapy regimens included: R-CHOP, R-DAEPOCH, R-Gmox/RminiCHOP. In the whole study group, the SMART and the SMART-START groups demonstrated respective ORR values of 87.5% and 92.3%, and respective OS of 89% and 91% at a median follow-up of 15.4 months. The median number of SMART cycles was 5 with a median time to response of 1.2 months. In the SMART-START arm, 23% of patients achieved CR before chemotherapy. The study was retrospective and therefore might not provide objective data. A prospective trial with a ‘gentle initiation’ phase was studied in a group of 26 treatment-naïve elderly patients with DLBCL and a median age of 76 years (78). Patients received two cycles of zanubrutinib, lenalidomide and rituximab (ZR2), followed by four cycles of RCHOP. The outcome of the initial phase was 100% ORR (35% CR and 65% PR) regardless of the lymphoma subtype (non-GCB vs. GCB DLBCL). The treatment was well tolerated and proved remarkably successful in an elderly population with DLBCL. The most common all-grade AEs were neutropenia and anemia (both 38.5%), and thrombocytopenia (nearly 35%). At a median follow-up of 9.8 months, the median PFS and OS were not reached. A few patients continued ZR2 without the additional immunochemotherapy and achieved remissions at the end of the planned treatment schedule. The latter finding opens a new era for unfit patients ineligible for intensive chemotherapy who have limited options of therapy. Further studies are warranted, given the promising results of zanubrutinib in this patient population.
A phase 3 PHOENIX study evaluated the efficacy of ibrutinib combined with R-CHOP in the TN non-germinal center DLBCL (79). In a subpopulation of patients < 60 years of age, ibrutinib plus R-CHOP improved PFS and OS (HR 0.56 and 0.33, respectively); however, no such effect was demonstrated in older patients, with the combination treatment leading to higher toxicity. The ORR was similar in both treatment arms, with a slightly higher CR rate with ibrutinib (71.2% vs. 69.9%). It is necessary to mention that the analysis in the younger subpopulation was performed post hoc. Zanubrutinib plus R-CHOP showed improved outcomes in forty-four patients with DE DLBCL in a single-arm phase 2 study (80). The response rate after six cycles of ZR-CHOP was 68% CRs, 2.3% PRs and 6.8% progressive disease (PD). Ten patients died during the study and five patients progressed during or soon after the completion of the treatment. The toxicities were manageable, and grade ≥ 3 AEs were similar or less frequent than in the PHOENIX study. Promising results were also demonstrated in a cohort of R/R DLBCL patients with zanubrutinib in combination with lenalidomide in a phase 1 study (81). Another approach was studied in a multicenter phase 2 trial of zanubrutinib and lenalidomide added to R-miniCHOP in a population of elderly patients with non-GCB DLBCL (82). Sixteen patients were eligible for evaluation. The ORR was nearly 94% with 62.5% CRs. The most common AEs were neutropenia and thrombocytopenia. Zanubrutinib might become a potent addition to either reduced-intensity chemotherapy as in mini-CHOP in TN DLBCL or R/R DLBCL with otherwise dismal prognosis.
Three formulations of the chimeric antigen receptor T cell (CAR-T) therapy, axicabtagene ciloleucel, tisagenlecleucel, and lisocabtagene maraleucel, have been approved by the FDA for the treatment of relapsed/refractory DLBCL patients (83). The ZUMA-7, BELINDA, and TRANSFORM phase 3 clinical trials showed significant efficacy of CAR-Ts in the second line of treatment, and challenged the second line standard of care (SOC) with autologous stem cell transplantation. Median PFS significantly improved after CAR-Ts in ZUMA-7 and TANSFORM trials compared to SOC (14.7 and 14.8 months vs. 3.7 and 5.7 months, respectively). BELINDA trial failed to demonstrate superiority of CAR-Ts over SOC, which has been explained by a longer waiting period before the actual CAR-T infusion etc. There is still place for SOC with autoSCT procedure, however it might not be plausible for unfit or frail patients. Moreover, CAR-T therapy carries risk of complications such as prolonged cytopenia, cytokine release syndrome, relapse, and the timely availability or the quality of patient’s lymphocytes might become a hurdle (84). The place of BTK inhibitors in this setting is yet to be determined, and the question whether they should come before or after CAR-Ts is open. Perhaps these agents, including zanubrutinib, could be administered concurrently as immune modifiers after CAR-T infusion, as well as synergizing with the anti-lymphoma effect. There is a single case report on zanubrutinib combined with an oral histone deacetylase inhibitor (HDACi), chidamide, in a 70-year old patient with DLBCL who relapsed 12 months after CAR-T therapy (85). He failed salvage chemotherapy with gemcitabine, dexamethasone and cisplatin, and suffered from progressive and symptomatic lung infiltration. The treatment with zanubrutinib and chidamide brought immense relief within two weeks and a CT scan confirmed CR two months into the treatment which was sustained at a 10-month follow-up. The CAR-T clone was not detected at the time of relapse and CD19 was still present on tumor cells; therefore, it was proposed that the effect was achieved due to the synergistic effect of zanubrutinib and chidamide, rather than augmentation of CAR-Ts. The exact mechanisms are yet to be determined. The tumor DNA analysis in the studied case detected the mutations in TP53 (47.6%) and NOTCH1 (35%), without mutations in MYD88, CD79b, EP300 or CREBBP. Chidamide was chosen based on its inhibitory effect on the BTK pathway signaling, decreasing mutant TP53 expression, and ease of administration (oral). This study showed potential in the tailoring of the combined targeted treatment based on the results of the mutational status in the signaling pathways in the tumor cells. Previous studies showed that CD79B mutation carries a higher risk for unfavorable outcome in patients with DLBCL (86). The preliminary results of a phase 2 study in 137 patients with CD79A/CD79B-mutant TN and R/R DLBCL found the addition of zanubrutinib to augment R-CHOP or salvage therapy (87). With a median follow-up of 6.4 months (range 2.6 – 24.5 months), 12 TN and 9 R/R patients were evaluable for response. There were 10 CRs and 2 PRs in TN DLBCL, and 5 CRs and 2 PRs in R/R DLBCL. The most common grade ≥3 AEs in TN and R/R cohort were: neutropenia (26.7% and 60%, respectively), anemia (26.7% and 60%, respectively), thrombocytopenia (26.7% and 50%, respectively) and infection (20% in both). This study is still ongoing and awaiting survival data in the future.
Follicular lymphoma is one of the most common non-Hodgkin lymphoma subtypes in the Western world (88). It affects mainly elderly patients and presents an indolent course with remissions and subsequent relapses (71). The current approach depends on the stage of the disease, but is based on anti-CD20 antibodies and classical chemotherapy like CHOP or bendamustine. Newer agents include targeting molecules such as BTK inhibitors, phosphatidylinositol-3-kinase (PI3K) inhibitors or lenalidomide (an immunomodulatory agent) (89). However, due to the indolent course of the disease and long follow-up, it is difficult to demonstrate an absolute benefit in terms of OS or even PFS. Therefore, a good approach might be either to maximally reduce the disease burden at the expense of the likelihood of AEs, or keep the disease under control with fewer side effects. Chemotherapy-free regimens might meet both the criteria when given in combination or monotherapy.
Zanubrutinib was administered as monotherapy in 33 patients with R/R FL in the BGB-311-AU-003 phase 2 trial (57). A median age was 63 years and most patients presented with intermediate/high FLIPI score (60.6%) and extranodal disease (54.5%). The median number of prior therapies was three. At a median follow-up of 33.9 months, median PFS was 10.4 months and median OS was not reached. The ORR was 36.4%, with 18.2% CRs and 18.2% PRs. Progressive disease was reported in 15.2% of patients. The median time to response was 2.7 months. Grade ≥ 3 AEs included neutropenia (18.2%), urinary tract infection (18.1%), anemia (15.2%), pneumonia (9.1%), hypertension (6.1%), abdominal pain (6.1%). No incidents of AF/F were observed. One patient experienced serious hematuria. Twelve patients (36.4%) had dose interruptions due to AE, and three patients (9.1%) discontinued zanubrutinib because of AE, with a median relative dose intensity of 97.9%. Better results were observed with a combination of zanubrutinib and obinutuzumab in a phase 1b trial in a total of 36 patients with R/R FL (11). A median age was 59 years of age and a median number of prior lines of therapy was 2. Thirty-nine percent of patients were refractory to rituximab. The median duration of zanubrutinib treatment was 20 months. The most common AEs were upper respiratory tract infection (39%), contusion (28%), fatigue (25%), cough (22%), diarrhea (17%), hypertension (8%), and major hemorrhage (3%). No AF/F was observed. The most common grade ≥ 3 AEs were neutropenia (14%) and thrombocytopenia (5.6%). The ORR at a median follow-up of 20 months was 72% with 39% CRs. Median PFS was 25 months. Half of patients discontinued the study because of progression, patient’s or investigator’s decision, and AE. The results of this study were favorable given the heavily-pretreated population.
The ROSEWOOD phase 2 randomized trial compared the efficacy and safety of zanubrutinib plus obinutuzumab (ZO) vs. obinutuzumab (O) alone in R/R FL patients (12). Two hundred and seventeen patients after ≥ two lines of therapy (including an anti-CD20 antibody and an alkylating agent) were randomized 2:1 to receive either ZO (n=145) or O (n=72). At a median follow-up of 12.5 months, the ORR was 68.3% with ZO and 45.8% with O, and the CR rate was 37.2% (ZO) vs. 19.4% (O). Median PFS was 27.4 months with ZO compared to 11.2 months with O. The ORR for 29 patients who crossed over to the ZO arm was 24.1%. The most common AEs in the ZO arm were thrombocytopenia (34.3%), neutropenia (27.3%), diarrhea (16.1%), fatigue (14.0%), constipation (13.3%), cough (11.9%), pyrexia (11.2%), and dyspnea (10.5%). Grade ≥3 AEs with incidence > 5% with ZO were neutropenia (22.4%) and thrombocytopenia (14.0%); incidence of atrial fibrillation was 0.7% and major bleeding was 1.4%. Zanubrutinib with obinutuzumab demonstrated superior efficacy to obinutuzumab alone in this heavily-pretreated population. Idelalisib proved its efficacy in a population of R/R FL patients who failed on their previous chemoimmunotherapy or relapsed within six months (90). Moreover, dual inhibition of PI3K and BTK signaling might overcome emerging resistant to these single agents. In a phase 2 study, a PI3K inhibitor, zandelisib, was administered with zanubrutinib in a group of 31 patients after a median of two previous lines of therapy (91). The ORR was 80% with 20% CRs, and the preliminary median PFS was 22.4 months with a median follow-up of 11.1 months. The depth of response was observed to increase over time. The spectrum of AEs was not different from those observed for single agents and did not lead to increased treatment discontinuation. However, idelalisib and other PI3K inhibitors might lead to serious complications including diarrhea due to colitis, liver enzyme elevation, pneumonitis, infections, and intestinal perforation in a significant number of patients (92). Idelalisib is no longer indicated for FL or SLL by the FDA (92). The international development of zandelisib has also been terminated and will only continue in Japan (93). The only PI3K inhibitor approved for FL by the FDA is copanlisib, but there are currently no ongoing trials of copanlisib in combination with zanubrutinib.
Zanubrutinib is a next-generation irreversible inhibitor of BTK developed by BeiGene in 2012 for the treatment of B-cell malignancies with a great activity and a higher specificity towards BTK. It has proved its efficacy in several non-Hodgkin lymphomas in monotherapy, as well as in combination with other targeted, chemotherapy-free agents. In our opinion, the future of zanubrutinib lies among combination therapies, either as a lead-in before the classical cytotoxic agents, or as an added modality with bcl-2 inhibitor, monoclonal antibodies, bi-clonal antibodies, or immunotoxins. Moreover, zanubrutinib might enhance the efficacy of CAR-T cell therapy in lymphoma. Aiming at deepening the response in indolent lymphomas with multi-agent regimens is currently being evaluated. Such approach enables MRD-guided limited duration of treatment and presumably prevents the development of resistance. On the other hand, such efficacious regimens carry the risk of adverse events that might only be tolerated and managed in fitter patients; even so, in such cases, the anticipated benefit would outweigh the inevitable risks.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This work was supported by the grants from the Medical University of Lodz, Poland (No. 503/1-093-01/503-11-004 and 503/1093-1/503-11- 003).
We thank Edward Lowczowski from the Medical University of Lodz for editorial assistance.
TR has received honoraria and research funding from Acerta, AstraZeneca, Beigene, AbbVie and Janssen. AW-W has received honoraria and research funding from BeiGene and AstraZeneca. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Saba NS, Liu D, Herman SEM, Underbayev C, Tian X, Behrend D, et al. Pathogenic role of b-cell receptor signaling and canonical NF-κB activation in mantle cell lymphoma. Blood (2016) 128:82–92. doi: 10.1182/blood-2015-11-681460
2. Davis RE, Ngo VN, Lenz G, Tolar P, Young RM, Romesser PB, et al. Chronic active b-cell-receptor signalling in diffuse large b-cell lymphoma. Nature (2010) 463:88–92. doi: 10.1038/nature08638
3. Cinar M, Hamedani FS, Mo Z, Cinar B, Amin HM, Alkan S. Bruton tyrosine kinase is commonly overexpressed in mantle cell lymphoma and its attenuation by ibrutinib induces apoptosis. Leuk Res (2013) 37:1271–7. doi: 10.1016/j.leukres.2013.07.028
4. Burger JA, Chiorazzi N. B cell receptor signaling in chronic lymphocytic leukemia. Trends Immunol (2013) 34:592. doi: 10.1016/J.IT.2013.07.002
5. Song Y, Zhou K, Zou D, Zhou J, Hu J, Yang H, et al. Treatment of patients with relapsed or refractory mantle–cell lymphoma with zanubrutinib, a selective inhibitor of bruton’s tyrosine kinase. Clin Cancer Res (2020) 26:4216–24. doi: 10.1158/1078-0432.CCR-19-3703/75971/AM/TREATMENT-OF-PATIENTS-WITH-RELAPSED-OR-REFRACTORY
6. Tam CS, Opat S, Simpson D, Cull G, Munoz J, Phillips TJ, et al. Zanubrutinib for the treatment of relapsed or refractory mantle cell lymphoma. Blood Adv (2021) 5:2577–85. doi: 10.1182/BLOODADVANCES.2020004074
7. Tam CS, Brown JR, Kahl BS, Ghia P, Giannopoulos K, Jurczak W, et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Lancet Oncol (2022) 23:1031–43. doi: 10.1016/S1470-2045(22)00293-5
8. Tam CS, Robak T, Ghia P, Kahl BS, Walker P, Janowski W, et al. Zanubrutinib monotherapy for patients with treatment naïve chronic lymphocytic leukemia and 17p deletion. Haematologica (2020) 106(9):2354–63. doi: 10.3324/haematol.2020.259432
9. Tedeschi A, Ferrant E, Flinn IW, Tam CS, Ghia P, Robak T, et al. Zanubrutinib in combination with venetoclax for patients with treatment-naïve (TN) chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL) with del(17p): Early results from arm d of the SEQUOIA (BGB-3111-304) trial. Blood (2021) 138:67–7. doi: 10.1182/BLOOD-2021-144336
10. Brown JR, Eichhorst B, Hillmen P, Jurczak W, Kaźmierczak M, Lamanna N, et al. Zanubrutinib or ibrutinib in relapsed or refractory chronic lymphocytic leukemia. N Engl J Med (2023) 388:319–32. doi: 10.1056/NEJMOA2211582
11. Tam CS, Quach H, Nicol A, Badoux X, Rose H, Miles Prince H, et al. Zanubrutinib (BGB-3111) plus obinutuzumab in patients with chronic lymphocytic leukemia and follicular lymphoma. Blood Adv (2020) 4:4802–11. doi: 10.1182/BLOODADVANCES.2020002183
12. Zinzani PL, Mayer J, Auer R, Bijou F, de Oliveira AC, Flowers C, et al. Zanubrutinib plus obinutuzumab (ZO) versus obinutuzumab (O) monotherapy in patients (pts) with relapsed or refractory (R/R) follicular lymphoma (FL): Primary analysis of the phase 2 randomized ROSEWOOD trial. J Clin Oncol (2022) 40(16_suppl):7510–0. doi: 10.1200/JCO.2022.40.16_suppl.7510
13. Efremov DG, Turkalj S, Laurenti L. Mechanisms of b cell receptor activation and responses to b cell receptor inhibitors in b cell malignancies. Cancers (Basel). (2020) 12:1396. doi: 10.3390/CANCERS12061396
14. Ponader S, Burger JA. Bruton’s tyrosine kinase: from X-linked agammaglobulinemia toward targeted therapy for b-cell malignancies. J Clin Oncol (2014) 32:1830–9. doi: 10.1200/JCO.2013.53.1046
15. de Weers M, Verschuren MCM, Kraakman MEM, Mensink RGJ, Schuurman RKB, van Dongen JJM, et al. The bruton’s tyrosine kinase gene is expressed throughout b cell differentiation, from early precursor b cell stages preceding immunoglobulin gene rearrangement up to mature b cell stages. Eur J Immunol (1993) 23:3109–14. doi: 10.1002/eji.1830231210
16. Robak T, Witkowska M, Smolewski P. The role of bruton’s kinase inhibitors in chronic lymphocytic leukemia: current status and future directions. Cancers (Basel). (2022) 14:771. doi: 10.3390/cancers14030771
17. Robak P, Robak T. Novel synthetic drugs currently in clinical development for chronic lymphocytic leukemia. Expert Opin Investig Drugs (2017) 26:1249–65. doi: 10.1080/13543784.2017.1384814
18. Woyach JA, Bojnik E, Ruppert AS, Stefanovski MR, Goettl VM, Smucker KA, et al. Bruton’s tyrosine kinase (BTK) function is important to the development and expansion of chronic lymphocytic leukemia (CLL). Blood (2014) 123:1207–13. doi: 10.1182/BLOOD-2013-07-515361
19. Palma M, Mulder TA, Österborg A. BTK inhibitors in chronic lymphocytic leukemia: biological activity and immune effects. Front Immunol (2021) 12:686768. doi: 10.3389/FIMMU.2021.686768
20. Tuomi JM, Bohne LJ, Dorey TW, Jansen HJ, Liu Y, Jones DL, et al. Distinct effects of ibrutinib and acalabrutinib on mouse atrial and sinoatrial node electrophysiology and arrhythmogenesis. J Am Heart Assoc (2021) 10:e022369. doi: 10.1161/JAHA.121.022369
21. Tillman BF, Pauff JM, Satyanarayana G, Talbott M, Warner JL. Systematic review of infectious events with the bruton tyrosine kinase inhibitor ibrutinib in the treatment of hematologic malignancies. Eur J Hematol (2018) 100:325–34. doi: 10.1111/EJH.13020
22. Shatzel JJ, Olson SR, Tao DL, McCarty OJT, Danilov AV, DeLoughery TG. Ibrutinib-associated bleeding; pathogenesis, management, and risk reduction strategies. J Thromb Hemost. (2017) 15:847. doi: 10.1111/JTH.13651
23. Sibaud V, Beylot-Barry M, Protin C, Vigarios E, Recher C, Ysebaert L. Dermatological toxicities of bruton’s tyrosine kinase inhibitors. Am J Clin Dermatol (2020) 21:799–812. doi: 10.1007/S40257-020-00535-X
24. Tullemans BME, Karel MFA, Léopold V, ten Brink MS, Baaten CCFMJ, Maas SL, et al. Comparison of inhibitory effects of irreversible and reversible btk inhibitors on platelet function. Eur J Hematol (2021) 2:685–99. doi: 10.1002/JHA2.269
25. BRUKINSA® (zanubrutinib) BTK inhibitor official BeiGene website. Available at: https://www.brukinsa.com/.
27. Guo Y, Liu Y, Hu N, Yu D, Zhou C, Shi G, et al. Discovery of zanubrutinib (BGB-3111), a novel, potent, and selective covalent inhibitor of bruton’s tyrosine kinase. J Med Chem (2019) 62:7923–40. doi: 10.1021/ACS.JMEDCHEM.9B00687
28. Tam CS, Trotman J, Opat S, Burger JA, Cull G, Gottlieb D, et al. Phase 1 study of the selective BTK inhibitor zanubrutinib in b-cell malignancies and safety and efficacy evaluation in CLL. Blood (2019) 134:851–9. doi: 10.1182/BLOOD.2019001160
29. Song Y, Zhou K, Zou D, Zhou J, Hu J, Yang H, et al. Zanubrutinib in relapsed/refractory mantle cell lymphoma: long-term efficacy and safety results from a phase 2 study. Blood (2022) 139:3148–58. doi: 10.1182/BLOOD.2021014162
30. Song Y, Zhou K, Zou D, Li D, Hu J, Yang H, et al. Long-term outcomes of second-line vs later-line zanubrutinib treatment in patients with relapsed/refractory MCL: an updated pooled analysis. Blood (2022) 140:6501–3. doi: 10.1182/BLOOD-2022-162135
31. Martin P, Cohen JB, Wang M, Kumar A, Hill B, Villa D, et al. Treatment outcomes and roles of transplantation and maintenance rituximab in patients with previously untreated mantle cell lymphoma: results from large real-world cohorts. J Clin Oncol (2023) 41:554. doi: 10.1200/JCO.21.02698
32. Dreyling M, Tam CS, Wang M, Smith SD, Ladetto M, Huang H, et al. A phase III study of zanubrutinib plus rituximab versus bendamustine plus rituximab in transplant-ineligible, untreated mantle cell lymphoma. Future Oncol (2021) 17:255–62. doi: 10.2217/FON-2020-0794
33. Wang ML, Lee H, Chuang H, Wagner-Bartak N, Hagemeister F, Westin J, et al. Ibrutinib in combination with rituximab in relapsed or refractory mantle cell lymphoma: a single-centre, open-label, phase 2 trial. Lancet Oncol (2016) 17:48–56. doi: 10.1016/S1470-2045(15)00438-6
34. Flinsenberg TWH, Tromedjo CC, Hu N, Liu Y, Guo Y, Thia KYT, et al. Differential effects of BTK inhibitors ibrutinib and zanubrutinib on NK-cell effector function in patients with mantle cell lymphoma. Haematologica (2020) 105:e76. doi: 10.3324/HAEMATOL.2019.220590
35. Dreyling M, Doorduijn JK, Gine E, Jerkeman M, Walewski J, Hutchings M, et al. Efficacy and safety of ibrutinib combined with standard first-line treatment or as substitute for autologous stem cell transplantation in younger patients with mantle cell lymphoma: Results from the randomized triangle trial by the European MCL network. Blood (2022) 140(Supplement 1):1–3. doi: 10.1182/BLOOD-2022-163018
36. Kumar A, Soumerai JD, Abramson JS, Batlevi CL, Chadha P, Dogan A, et al. Preliminary safety and efficacy from a multicenter, investigator-initiated phase ii study in untreated TP53 mutant mantle cell lymphoma with zanubrutinib, obinutuzumab, and venetoclax (BOVen). Blood (2021) 138(Supplement 1):3540. doi: 10.1182/blood-2021-151831
37. Cai Q, Xia Y, Liu P, Zhang Y, Huang H, Gao Y, et al. Frontline treatment with zanubrutinib plus rituximab (ZR) followed by short course r-dhaox shows potent efficacy in patients with mantle cell lymphoma (MCL) - preliminary results of phase II CHESS clinical trial. Blood (2022) 140:9356–7. doi: 10.1182/BLOOD-2022-166237
38. Castillo JJ, Olszewski AJ, Kanan S, Meid K, Hunter ZR, Treon SP. Overall survival and competing risks of death in patients with Waldenstrom macroglobulinaemia: an analysis of the surveillance, epidemiology and end results database. Br J Haematol (2015) 169:81–9. doi: 10.1111/BJH.13264
39. Staber PB, Kersten MJ. EHA endorsement of ESMO clinical practice guidelines for diagnosis, treatment, and follow-up for Waldenstrom's macroglobulinemia. Hemasphere (2021) 5:e634. doi: 10.1097/HS9.0000000000000634
40. Burnworth B, Wang Z, Singleton TP, Bennington A, Fritschle W, Bennington R, et al. Clone-specific MYD88 L265P and CXCR4 mutation status can provide clinical utility in suspected waldenström macroglobulinemia/lymphoplasmacytic lymphoma. Leuk Res (2016) 51:41–8. doi: 10.1016/J.LEUKRES.2016.10.008
41. Hunter ZR, Xu L, Tsakmaklis N, Demos MG, Kofides A, Jimenez C, et al. Insights into the genomic landscape of MYD88 wild-type Waldenstrom's macroglobulinemia. Blood Adv (2018) 2:2937–46. doi: 10.1182/BLOODADVANCES.2018022962
42. Treon SP, Tripsas CK, Meid K, Warren D, Varma G, Green R, et al. Ibrutinib in previously treated Waldenstrom's macroglobulinemia. N Engl J Med (2015) 372:1430–40. doi: 10.1056/NEJMOA1501548
43. Dimopoulos MA, Trotman J, Tedeschi A, Matous JV, Macdonald D, Tam C, et al. Ibrutinib for patients with rituximab-refractory Waldenstrom's macroglobulinaemia (iNNOVATE): an open-label substudy of an international, multicentre, phase 3 trial. Lancet Oncol (2017) 18:241–50. doi: 10.1016/S1470-2045(16)30632-5
44. Buske C, Tedeschi A, Trotman J, García-Sanz R, MacDonald D, Leblond V, et al. Ibrutinib plus rituximab versus placebo plus rituximab for Waldenstrom's macroglobulinemia: final analysis from the randomized phase III iNNOVATE study. J Clin Oncol (2022) 40:52–62. doi: 10.1200/JCO.21.00838
45. Trotman J, Buske C, Tedeschi A, Matous JV, MacDonald D, Tam CS, et al. Single-agent ibrutinib for rituximab-refractory waldenström macroglobulinemia: Final analysis of the substudy of the phase III innovateTM trial. Clin Cancer Res (2021) 27:5793–800. doi: 10.1158/1078-0432.CCR-21-1497
46. Trotman J, Opat S, Gottlieb D, Simpson D, Marlton P, Cull G, et al. Zanubrutinib for the treatment of patients with waldenström macroglobulinemia: 3 years of follow-up. Blood (2020) 136:2027–37. doi: 10.1182/BLOOD.2020006449
47. Tam CS, Opat S, D’Sa S, Jurczak W, Lee HP, Cull G, et al. A randomized phase 3 trial of zanubrutinib vs ibrutinib in symptomatic waldenström macroglobulinemia: the ASPEN study. Blood (2020) 136:2038–50. doi: 10.1182/BLOOD.2020006844
48. Kapoor P, Treon SP. The race to stymie BTK: zanu zings. Blood (2020) 136:1997–9. doi: 10.1182/BLOOD.2020008197
49. Dimopoulos M, Sanz RG, Lee H-P, Trneny M, Varettoni M, Opat S, et al. Zanubrutinib for the treatment of MYD88 wild-type waldenström macroglobulinemia: a substudy of the phase 3 ASPEN trial. Blood Adv (2020) 4:6009–18. doi: 10.1182/BLOODADVANCES.2020003010
50. Cao Y, Yang G, Hunter ZR, Liu X, Xu L, Chen J, et al. The BCL2 antagonist ABT-199 triggers apoptosis, and augments ibrutinib and idelalisib mediated cytotoxicity in CXCR4 wild-type and CXCR4 WHIM mutated waldenstrom macroglobulinaemia cells. Br J Haematol (2015) 170:134–8. doi: 10.1111/BJH.13278
51. Yu Y, Yi S, Wenjie X, Wang T, Yan Y, Liu W, et al. Zanubrutinib plus ixazomib and dexamethasone for newly diagnosed symptomatic waldenström macroglobulinemia: A prospective, phase II study. Blood (2022) 140:3587–8. doi: 10.1182/BLOOD-2022-162338
52. Castillo JJ, Gustine JN, Meid K, Dubeau TE, Severns P, Xu L, et al. Response and survival for primary therapy combination regimens and maintenance rituximab in waldenström macroglobulinaemia. Br J Haematol (2018) 181:77–85. doi: 10.1111/BJH.15148
53. Zucca E, Arcaini L, Buske C, Johnson PW, Ponzoni M, Raderer M, et al. Marginal zone lymphomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2020) 31:17–29. doi: 10.1016/j.annonc.2019.10.010
54. Lue JK, O’Connor OA, Bertoni F. Targeting pathogenic mechanisms in marginal zone lymphoma: from concepts and beyond. Ann Lymphoma. (2020) 4:7–7. doi: 10.21037/AOL-20-20
55. Cavalloni C, Varettoni M, Rattotti S, Arcaini L. Evaluating ibrutinib for the treatment of relapsed/refractory marginal zone lymphoma. Expert Opin Pharmacother. (2021) 22:1643–9. doi: 10.1080/14656566.2021.1941864
56. Steward J. Brukinsa (zanubrutinib) FDA approval history - drugs.com. Available at: https://www.drugs.com/history/brukinsa.html.
57. Phillips T, Chan H, Tam CS, Tedeschi A, Johnston P, Oh SY, et al. Zanubrutinib monotherapy in relapsed/refractory indolent non-Hodgkin lymphoma. Blood Adv (2022) 6:3472–9. doi: 10.1182/BLOODADVANCES.2021006083
58. Opat S, Tedeschi A, Linton K, McKay P, Hu B, Chan H, et al. The MAGNOLIA trial: Zanubrutinib, a next-generation bruton tyrosine kinase inhibitor, demonstrates safety and efficacy in relapsed/refractory marginal zone lymphoma. Clin Cancer Res (2021) 27:6323–32. doi: 10.1158/1078-0432.CCR-21-1704/673971/AM/THE-MAGNOLIA-TRIAL-ZANUBRUTINIB-A-NEXT-GENERATION
59. Opat S, Tedeschi A, Hu B, Linton KM, McKay P, Chan H, et al. Long-term efficacy and safety of zanubrutinib in patients with relapsed/refractory (R/R) marginal zone lymphoma (MZL): Final analysis of the magnolia (BGB-3111-214) trial. Blood (2022) 140:573–6. doi: 10.1182/BLOOD-2022-163371
60. Xu W, Yang S, Zhou K, Pan L, Li Z, Zhou J, et al. Treatment of relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma with the BTK inhibitor zanubrutinib: phase 2, single-arm, multicenter study. J Hematol Oncol (2020) 13:48. doi: 10.1186/S13045-020-00884-4
61. Song Y, Sun M, Qi J, Xu W, Zhou J, Li D, et al. A two-part, single-arm, multicentre, phase I study of zanubrutinib, a selective bruton tyrosine kinase inhibitor, in Chinese patients with relapsed/refractory b-cell malignancies. Br J Haematol (2022) 198:62–72. doi: 10.1111/BJH.18162
62. Xu W, Yang S, Tam CS, Seymour JF, Zhou K, Opat S, et al. Zanubrutinib monotherapy for naïve and relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma: a pooled analysis of three studies. Adv Ther (2022) 39:4250–65. doi: 10.1007/S12325-022-02238-7
63. Ghia P, Barnes G, Yang K, Tam C, Hillmen P, Robak T, et al. Patient-reported outcomes from a phase 3 randomized study of zanubrutinib versus bendamustine plus rituximab (BR) in patients with treatment-naïve (TN) CLL/SLL. HemaSphere (2022) 6:560–1. doi: 10.1097/01.HS9.0000845532.14560.fe
64. Burger JA, Barr PM, Robak T, Owen C, Ghia P, Tedeschi A, et al. Long-term efficacy and safety of first-line ibrutinib treatment for patients with CLL/SLL: 5 years of follow-up from the phase 3 RESONATE-2 study. Leukemia (2020) 34:787–98. doi: 10.1038/S41375-019-0602-X
65. Boriani G, Menna P, Morgagni R, Minotti G, Vitolo M. Ibrutinib and Bruton’s tyrosine kinase inhibitors in chronic lymphocytic leukemia: focus on atrial fibrillation and ventricular tachyarrhythmias/sudden cardiac death. Chemotherapy (2022). doi: 10.1159/000528019
66. Hampel PJ, Ding W, Call TG, Rabe KG, Kenderian SS, Witzig TE, et al. Rapid disease progression following discontinuation of ibrutinib in patients with chronic lymphocytic leukemia treated in routine clinical practice. Leuk Lymphoma. (2019) 60:2712–9. doi: 10.1080/10428194.2019.1602268
67. Hillmen P, Brown J, Lamanna N, O’Brien S, Tam C, Qiu L, et al. Health-related quality of life outcomes associated with zanubrutinib vs ibrutinib monotherapy in patients with relapsed/refractory (RR) CLL/SLL: results from the randomized phase 3 ALPINE trial. (The 27th Congress of the European Hematology Association (EHA):EHA Library Vienna, Austria) (2022). Available at: https://library.ehaweb.org/eha/2022/eha2022-congress/357523/peter.hillmen.health-related.quality.of.life.outcomes.associated.with.html?f=listing%3D3%2Abrowseby%3D8%2Asortby%3D1%2Amedia%3D1.
68. Moreno C, Greil R, Demirkan F, Tedeschi A, Anz B, Larratt L, et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol (2019) 20:43–56. doi: 10.1016/S1470-2045(18)30788-5
69. Burger JA, Sivina M, Jain N, Kim E, Kadia T, Estrov Z, et al. Randomized trial of ibrutinib vs ibrutinib plus rituximab in patients with chronic lymphocytic leukemia. Blood (2019) 133:1011–9. doi: 10.1182/BLOOD-2018-10-879429
70. Soumerai JD, Mato AR, Dogan A, Seshan VE, Joffe E, Flaherty K, et al. Zanubrutinib, obinutuzumab, and venetoclax with minimal residual disease-driven discontinuation in previously untreated patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: a multicentre, single-arm, phase 2 trial. Lancet Haematol (2021) 8:e879–90. doi: 10.1016/S2352-3026(21)00307-0
71. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the united states, 1992-2001. Blood (2006) 107:265–76. doi: 10.1182/BLOOD-2005-06-2508
72. Janssen-Heijnen MLG, van Spronsen DJ, Lemmens VEPP, Houterman S, Verheij KDGW, Coebergh JWW. A population-based study of severity of comorbidity among patients with non-hodgkin’s lymphoma: prognostic impact independent of international prognostic index. Br J Haematol (2005) 129:597–606. doi: 10.1111/J.1365-2141.2005.05508.X
73. Peyrade F, Jardin F, Thieblemont C, Thyss A, Emile JF, Castaigne S, et al. Attenuated immunochemotherapy regimen (R-miniCHOP) in elderly patients older than 80 years with diffuse large b-cell lymphoma: a multicentre, single-arm, phase 2 trial. Lancet Oncol (2011) 12:460–8. doi: 10.1016/S1470-2045(11)70069-9
74. Han YB, Yang JM, Kwon HJ, Lee JO, Lee JS, Paik JH. Clinicopathologic and prognostic significance of bruton’s tyrosine kinase expression in diffuse large b-cell lymphoma. Anticancer Res (2021) 41:5677–92. doi: 10.21873/ANTICANRES.15384
75. Xu PP, Shi ZY, Qian Y, Cheng S, Zhu Y, Jiang L, et al. Ibrutinib, rituximab, and lenalidomide in unfit or frail patients aged 75 years or older with de novo diffuse large b-cell lymphoma: a phase 2, single-arm study. Lancet Healthy Longev (2022) 3:e481–90. doi: 10.1016/S2666-7568(22)00123-4
76. Yang H, Xiang B, Song Y, Zhang H, Zhao W, Zou D, et al. Zanubrutinib monotherapy for relapsed or refractory non-germinal center diffuse large b-cell lymphoma. Blood Adv (2022) 6:1629–36. doi: 10.1182/BLOODADVANCES.2020003698
77. Zhu Y, Zhang X, Wei J, Yang C, Tong H, Mai W, et al. Rituximab, lenalidomide and BTK inhibitor as frontline treatment for elderly or unfit patients with diffuse large b-cell lymphoma: a real-world analysis of single center. Exp Hematol Oncol (2022) 11:57. doi: 10.1186/S40164-022-00314-W
78. Chen X, Lei T, Yu H, Li C, Han S, Peng S, et al. Gentle initiation” rituximab, lenalidomide and zanubrutinib chemo-free regimen followed by immunochemotherapy for elderly/frail patients with newly diagnosed diffuse large b-cell lymphoma: an investigator initiated, single arm, phase 2 trial. Blood (2022) 140(Supplement 1):9452–3. doi: 10.1182/BLOOD-2022-164486
79. Younes A, Sehn LH, Johnson P, Zinzani PL, Hong X, Zhu J, et al. Randomized phase III trial of ibrutinib and rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone in non-germinal center b-cell diffuse large b-cell lymphoma. J Clin Oncol (2019) 37:1285–95. doi: 10.1200/JCO.18.02403
80. He Q, Xie L, Zhao R, Ma J, Wang H, Li J, et al. Zanubrutinib plus RCHOP(ZR-CHOP) regimen achieves high complete response rate in the treatment of newly-diagnosed double-expression diffuse large b cell lymphoma. Blood (2022) 140(Supplement 1):6614–5. doi: 10.1182/BLOOD-2022-168859
81. Zhang H, Zhou K, Cheng Y, Zhang L, Yang H, Zou L, et al. Preliminary safety and efficacy of zanubrutinib in combination with lenalidomide in patients with relapsed/refractory diffuse large b-cell lymphoma. Blood (2022) 140(Supplement 1):3750–2. doi: 10.1182/blood-2022-155979
82. Sun J, Xu Y, Yang M, Wang H, Yu W, You L, et al. The ZR2-MiniCHOP Study:zanubrutinib, lenalidomide, rituximab, cyclophosphamide, vincristine, epirubicin and prednisone in elderly patients with previously untreated diffuse large b-cell lymphoma. Blood (2022) 140(Supplement 1):3756. doi: 10.1182/blood-2022-158723
83. Albanyan O, Chavez J, Munoz J. The role of CAR-T cell therapy as second line in diffuse large b-cell lymphoma. Ther Adv Hematol (2022) 13:20406207221141510. doi: 10.1177/20406207221141511
84. Dahi PB, Moskowitz CH, Giralt SA, Lazarus HM. Novel agents may positively impact chemotherapy and transplantation in subsets of diffuse large b-cell lymphoma. Expert Rev Hematol (2019) 12:407–18. doi: 10.1080/17474086.2019.1596793
85. Zhu W, Tao S, Miao W, Liu H, Yuan X. Case report: dual inhibition of HDAC and BTK for diffuse large b-cell lymphoma after failure to CD19-targeted CAR-T therapy. Front Immunol (2022) 13:894787. doi: 10.3389/FIMMU.2022.894787
86. Xu PP, Shen R, Shi ZY, Cheng S, Wang L, Liu Y, et al. The prognostic significance of CD79B mutation in diffuse large b-cell lymphoma: a meta-analysis and systematic literature review. Clin Lymphoma Myeloma Leuk. (2022) 22:e1058. doi: 10.1016/J.CLML.2022.08.006
87. Yao Z, Yan Z, Yao S, Wang H, Chu J, Zhao S, et al. Preliminary results of a phase ii study of zanubrutinib combined with immunochemotherapy in patients with CD79A/CD79B-mutant diffuse large b-cell lymphoma. Blood (2022) 140:3767–8. doi: 10.1182/BLOOD-2022-165944
88. Dreyling M, Ghielmini M, Rule S, Salles G, Ladetto M, Tonino SH, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2021) 32:298–308. doi: 10.1016/j.annonc.2020.11.008
89. Ollila TA, Olszewski AJ. Chemotherapy-free management of follicular and marginal zone lymphoma. Cancer Manag Res (2021) 13:3935–52. doi: 10.2147/CMAR.S267258
90. Gopal AK, Kahl BS, de Vos S, Wagner-Johnston ND, Schuster SJ, Jurczak WJ, et al. PI3Kδ inhibition by idelalisib in patients with relapsed indolent lymphoma. N Engl J Med (2014) 370:1008–18. doi: 10.1056/NEJMOA1314583
91. Soumerai JD, Diefenbach CS, Samaniego F, Kumar A, Tsai ML, Asch AS, et al. Safety and efficacy of the PI3Kδ inhibitor zandelisib in combination with the BTK inhibitor zanubrutinib in patients with Relapsed/Refractory (R/R) follicular lymphoma (FL) or mantle cell lymphoma (MCL). Blood (2022) 140:189–91. doi: 10.1182/BLOOD-2022-157563
92. Company statements. Gilead statement on zydelig® U.S. indication for follicular lymphoma and small lymphocytic leukemia. Available at: https://www.gilead.com/news-and-press/company-statements/gilead-statement-on-zydelig-us-indication-for-follicular-lymphoma-and-small-lymphocytic-leukemia.
93. MEI and kyowa kirin to discontinue developing zandelisib outside Japan. Available at: https://www.pharmaceutical-technology.com/news/mei-kyowa-kirin-zandelisib/.
Keywords: zanubrutinib, chronic lymphocytic leukemia, DLBCL, mantle cell lymphoma, marginal zone lymphoma, Waldenstrom macroglobulinaemia
Citation: Wolska-Washer A and Robak T (2023) Zanubrutinib for the treatment of lymphoid malignancies: Current status and future directions. Front. Oncol. 13:1130595. doi: 10.3389/fonc.2023.1130595
Received: 23 December 2022; Accepted: 06 March 2023;
Published: 23 March 2023.
Edited by:
Narendranath Epperla, The Ohio State University, United StatesReviewed by:
Sabarish Ayyappan, The University of Iowa, United StatesCopyright © 2023 Wolska-Washer and Robak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tadeusz Robak, cm9iYWt0YWRAY3NrLnVtZWQubG9kei5wbA==
†ORCID: Anna Wolska-Washer, orcid.org/0000-0001-8838-2098
Tadeusz Robak, orcid.org/0000-0002-3411-6357
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.