 Jiayuan Zhao
Jiayuan Zhao Yujia Kong
Yujia Kong Yang Xiang
Yang Xiang Junjun Yang
Junjun Yang- National Clinical Research Center for Obstetric & Gynecologic Diseases/Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China
Background: Gynecological cancer is one of the most common cancers in women. The quality of life (QoL) or psychological impact has emerged as an outcome indicator in many clinical trials of gynecological cancer and gained much concern in the clinical setting at the start of the 21st century. Our paper conducted a bibliometric analysis of QoL or psychological impact on gynecological cancer patients to show the status and hotspots.
Methods: Related publications from 2000 to 2022 were included by screening from the Web of Science Core Collection (WOSCC) on 26 June 2022. The bibliometrics was analyzed and visualized by bibliometrix R-package, VOSviewer, and CiteSpace V.
Results: A total of 6,479 publications were included in our study. The publications in this field were increased annually. The United States (n = 2,075) was the country with the most published papers. Sydney University (n = 167) was the most productive affiliation. Gynecologic Oncology and Journal of Clinical Oncology were the most relevant and most cited sources, respectively. The article written by Bray F et al. has the highest citation. Kim J and Aaronson NK ranked first in most productive author and most co-cited author, respectively. The keywords “mortality”, “fertility preservation”, and “palliative care” have bursts till 2022, which represented the frontiers of this field.
Conclusion: Our study provides an overall analysis of QoL or psychological impact on gynecological cancer patients, which can serve as a reference in future research.
1 Introduction
Gynecological cancer mainly consists of cervical cancer, endometrial cancer, ovarian cancer, and gestational trophoblastic neoplasia. In 2020, gynecological cancer accounted for 14.4% of new cancer cases of women among 9.2 million new cases (source: GLOBOCAN 2020). Cervical cancer is the fourth most common cancer in women, followed by endometrial cancer ranking sixth, and ovarian cancer ranking eighth (1). During treatment, gynecological cancer patients often need to undergo surgery, chemotherapy, radiotherapy, targeted immunotherapy, etc. They have to cope with the side effects of these treatments, which undoubtedly cause physical and psychological impacts on them. The postoperative complications include infections such as febrile morbidity, pneumonia, and urinary tract infection and non-infection symptoms such as lymphocyst, ureteral fistula, and premature ovarian failure (2). The chemotherapy and radiotherapy complications can affect the hematological system (i.e., leukopenia, anemia, and thrombocytopenia), digestive system (i.e., indigestion, nausea, vomiting, and diarrhea), genitourinary system (sexual dysfunction, urinary frequency, and incontinence), respiratory system (dyspnea), and skin (i.e., hair loss and skin rash) and cause sleep disorders and so on. The psychological impact includes anxiety and depression or even post-traumatic stress disorder (3–5). In addition to the side effects of the treatment, with the progression of gynecological cancer, patients may suffer from cancer cachexia syndrome, which is characterized by specific energy metabolism alterations and symptoms such as fatigue, anorexia, nausea, anemia, and immunodepression (6). These complications cause heavy burdens on gynecological cancer patients, reduce their quality of life (QoL), or cause psychological problems without remedy (7). With the variety of treatment options and drug combinations available, many clinical trials evaluate QoL and psychological impact as outcome indicators, which help clinical decision making (6, 8–11). As researchers point out, after treatment for locally advanced cervical cancer, worsening of QoL was observed in sexual enjoyment, peripheral neuropathy, and menopausal symptoms. Moreover, the neoadjuvant chemotherapy group experienced a lower burden of menopausal symptoms and higher scores in sexual/vaginal functioning than the chemoradiation group (11).
Many instruments and scales are applied to help gynecologists assess their patients’ QoL or mental health, such as the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 30 Version 3 (EORTC QLQ-C30), Hospital Anxiety and Depression Scale (HADS), Female Sexual Function Index (FSFI), and Functional Assessment of Cancer Therapy-General Version 4 (FACT-G). These questionnaires are usually used in combination to score patients (12–14).
Bibliometrics analyzes publication records and presents them visually through the application of mathematical and statistical methods (15, 16). Bibliometric analysis relies on science mapping tools, such as CiteSpace (17–19), VOSviewer (20), and HistCite (21).
Since the start of the 21st century, more and more articles and reviews have emerged on QoL or psychological impact on gynecologic oncology patients. In this paper, we did a bibliometric analysis to identify the global trends, the network of collaboration, research directions, etc., of this field from 2000 to 2022. As we know, this is the first bibliometric analysis targeted at QoL or the psychologic impact of gynecologic oncology patients.
2 Methods
2.1 Data collection
On 26 June 2022, an advanced document retrieval was performed on the Web of Science Core Collection (WOSCC database). The publication date was limited from 1 January 2000 to 1 June 2022. The search formula was listed as follows:
#1 ((((((((TS=(Quality of Life)) OR TS=(Life Quality)) OR TS=(Health-Related Quality Of Life)) OR TS=(Health Related Quality Of Life)) OR TS=(HRQOL)) OR TS=(psychological impact)) OR TS=(emotional impact)) OR TS=(Psychological Wellbeing)) OR TS=(mental health)
#2((((((TS=(gynecology oncology)) OR TS=(gynecologic cancer)) OR TS=(gynecologic neoplasm)) OR TS=(cervical cancer)) OR TS=(ovarian cancer)) OR TS=(endometrial cancer)) OR TS=(gestational trophoblastic neoplasia)
Publication date 2000-01-01 – 2022-06-01
#1 AND #2
The detailed search process is outlined in Figure 1. Articles and reviews were included in this bibliography analysis, and the language was restricted to English. Eventually, a total of 6,479 publications were selected and exported in plain text file format for full record and cited reference.
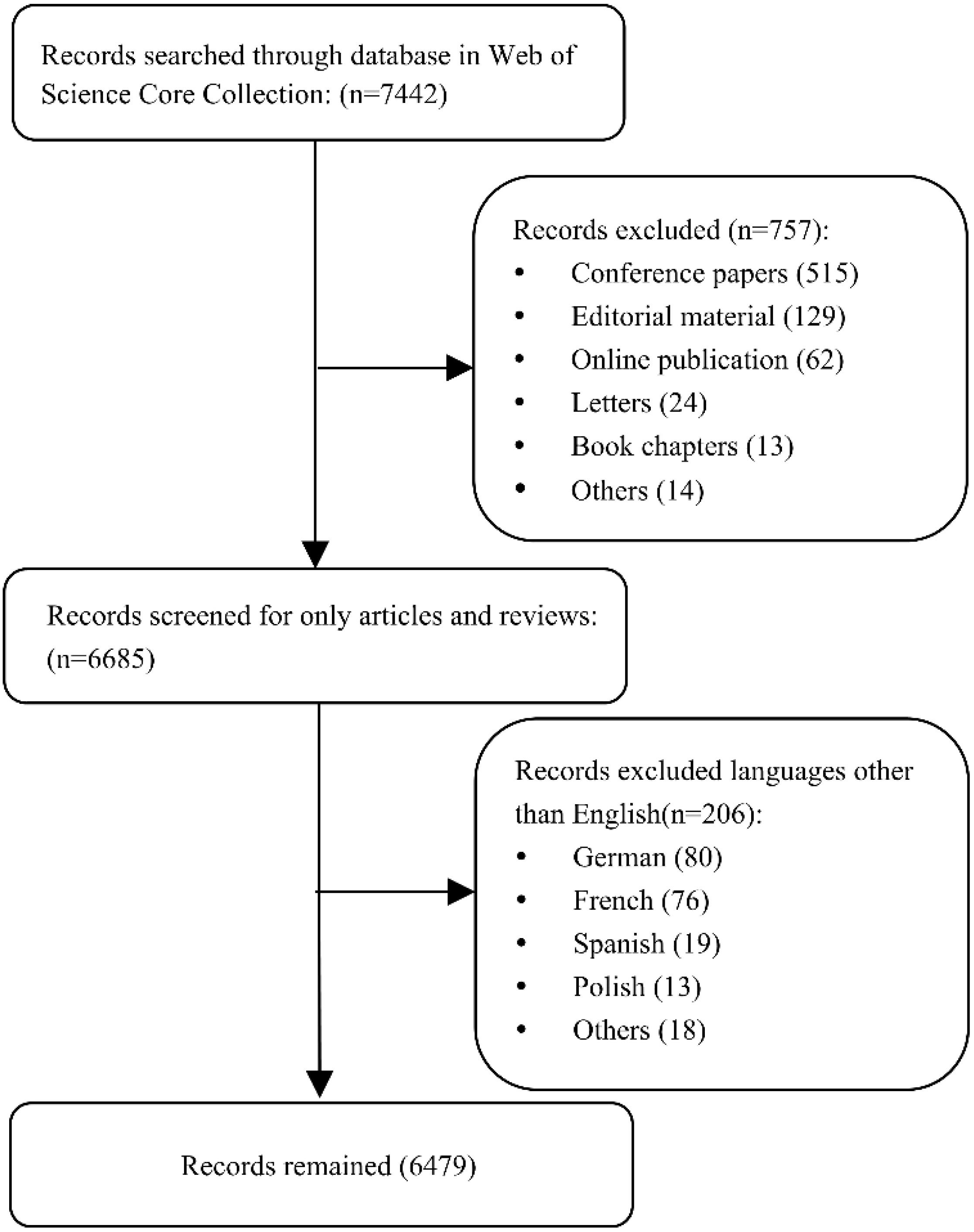
Figure 1 The process of record selection.
2.2 Visualization and statistical tools
Bibliometrix R-package (http://www.bibliometrix.org) provides tools for quantitative bibliometrics and scientometrics research. It runs on RStudio v.4.1.2 software (RStudio, PBC, Boston, MA, USA). It can produce a descriptive analysis of a bibliographic data frame, as well as build a network for analyzing bibliographic coupling, co-citation, collaboration, and co-occurrence (22). We used it to extract the most relevant countries, journals, and locally cited publications as tables. RStudio was also used to conduct the geographic visualization analysis of country collaboration.
VOSviewer (version 1.6.18, the Centre for Science and Technology Studies at Leiden University (Netherlands)) is a software tool for the creation of maps based on network data and for visualizing and exploring these maps. VOSviewer can be used to construct networks of publications, journals, authors, research institutions, countries, keywords, or terms. With VOSviewer, bibliographic database files (such as Web of Science files) can be used to build a network. This software can be freely downloaded from www.vosviewer.com (20). In this analysis, we constructed a geographic map of countries and institutional networks based on the co-authorship links, and a publications network based on the citation links. The world borders of the geographic map were downloaded from https://www.tudelft.nl/en/librarv/research-analvtics/case-21-tu-delft-top-collaborators-2. Based on Clement Lev’s “Map of Countries” plugin for Gephi software, graph nodes are used to represent the country borders and their coordinates (23).
CiteSpace V6.1.R2 (Drexel University, Philadelphia, PA, United States) is a Java application for analyzing and visualizing co-citation networks (24). It can be freely downloaded from http://cluster.cis.drexel.edu/~cchen/citespace/download/. The new version 6.1.R2 was built on 20 June 2022. It can be used to build a cooperative network of authors, institutions, or countries; co-occurrence analysis of terms, keywords, or categories; co-citation analysis of references, authors, or journals; and coupling analysis of the paper (17). In this analysis, we use CiteSpace software to draw the dual-map overlay of journals, citation bursts of the top 20 reference and top 20 keywords, a network of authors, and the timeline view of the keywords. The parameter settings were set in the following: the timespan: 2000–2022 (Slice Length = 2), selection criteria: top 50 per slice, link retaining factor (LRF) = 3.0, look back years (LBY) = 5, e for top N (e) = 1.0.
GraphPad Prism 9.0 was used to draw the line graph of annual production and perform a linear regression based on this line graph. The coefficient of determination (R2) represents the proportion of variance in the dependent variable that can be predicted. The closer the R2 value is to 1, the better the fitting; and the closer it is to 0, the worse the fitting.
3 Results
3.1 Distribution of included publications
In total, 6,479 publications were included in our study with the timespan from 2000 to 2022. There were 5,092 articles and 1,387 reviews, which account for 78.59% and 21.41%, respectively.
The number of published papers on the research of life quality or psychological impact of gynecology oncology patients is shown in Figure 2. For the purpose of linear regression analysis, only publications from 2000 to 2021 are shown. In general, it has increased year by year. It can be seen that the rise slowed down in 2000–2003, while in recent years (2019–2021), the rise has been rapid, with an increase of about 50 papers per year.
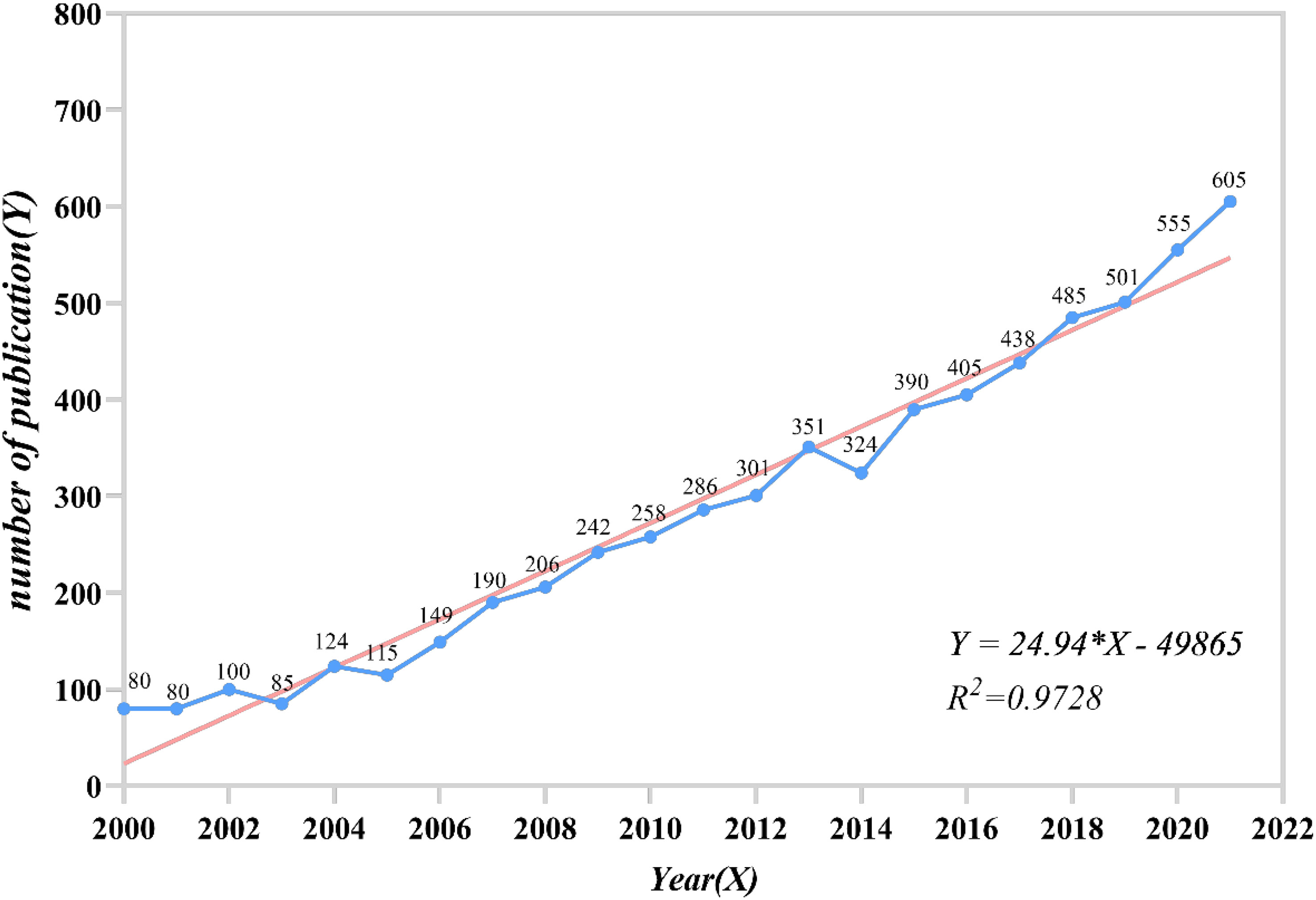
Figure 2 The number of published papers from 2000 to 2021.
3.2 Geographical distribution of the publications
The geographic visualization analysis of country collaboration based on the co-authorship analysis of VOSviewer and RStudio is shown in Figure 3. To visualize clearly, only a minimum number of documents, not more than 20, were included in this map, which contained 38 countries. The top 10 most relevant countries according to the corresponding author’s country are listed in Table 1. The listed countries published a total of 5,031 articles, accounting for 77.5% of the total. The United States ranked first (n = 2,075, 32.0%), followed by China (n = 572, 8.8%), the United Kingdom (n = 509, 7.9%), Australia (n = 342, 5.3%), Italy (n = 340, 5.2%), and so on. Table 1 also shows single-country publications (SCPs), multiple-country publications (MCPs), and MCP ratio (MCP/articles). France is the country with the highest MCP ratio (0.344), and Japan is the country with the lowest (0.052) in the top 10 list.
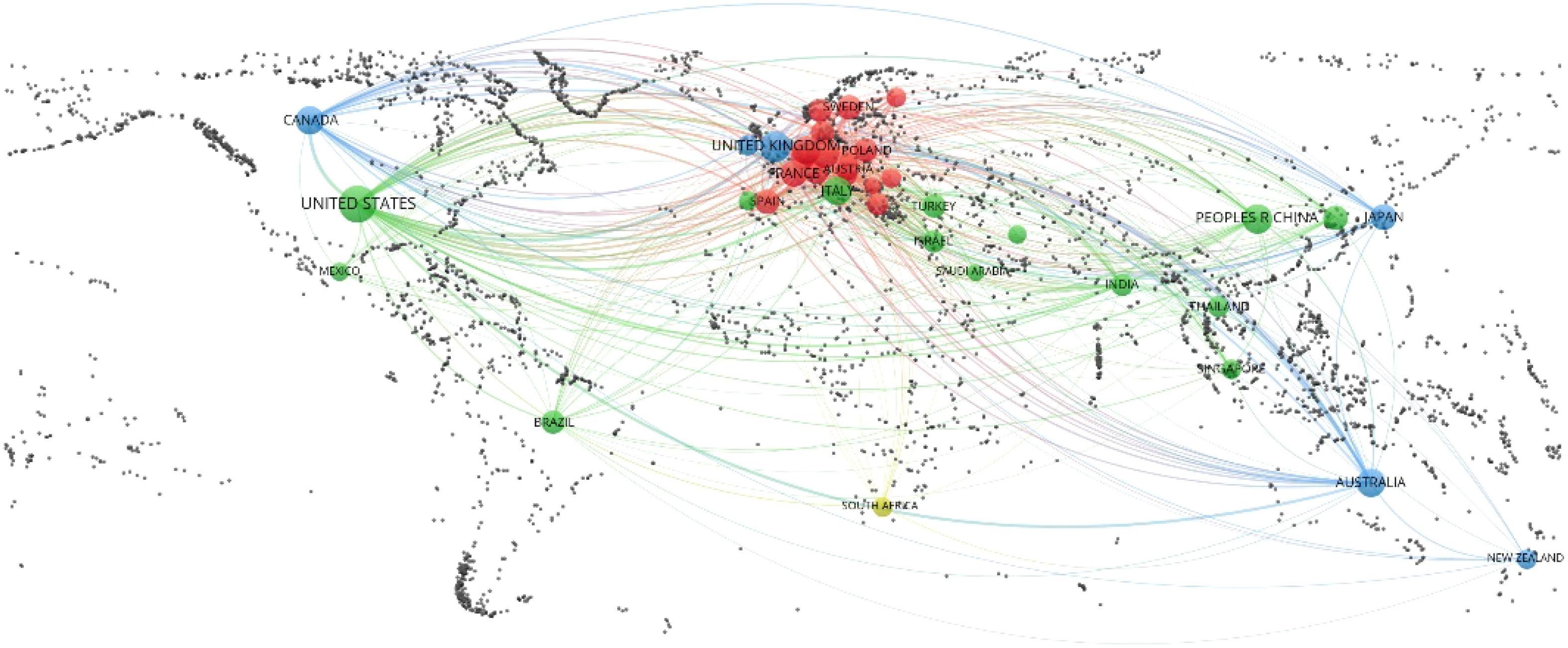
Figure 3 The geographic visualization analysis of country collaboration based on the co-authorship analysis of VOSviewer (Taiwan is annexed to the People’s Republic of China; England, Scotland, Northern Ireland, and Wales were incorporated into the United Kingdom).
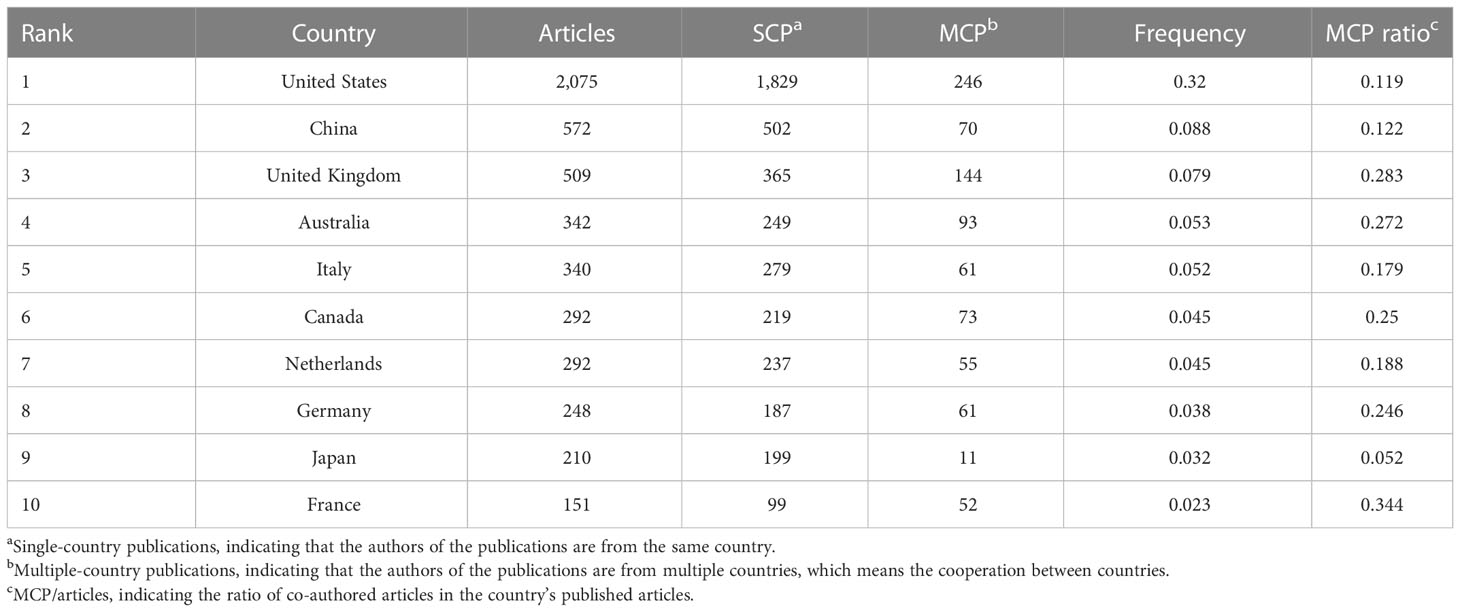
Table 1 Top 10 most relevant countries by corresponding authors.
3.3 The distribution of institutions
The institution network based on the co-authorship analysis is listed in Figure 4.
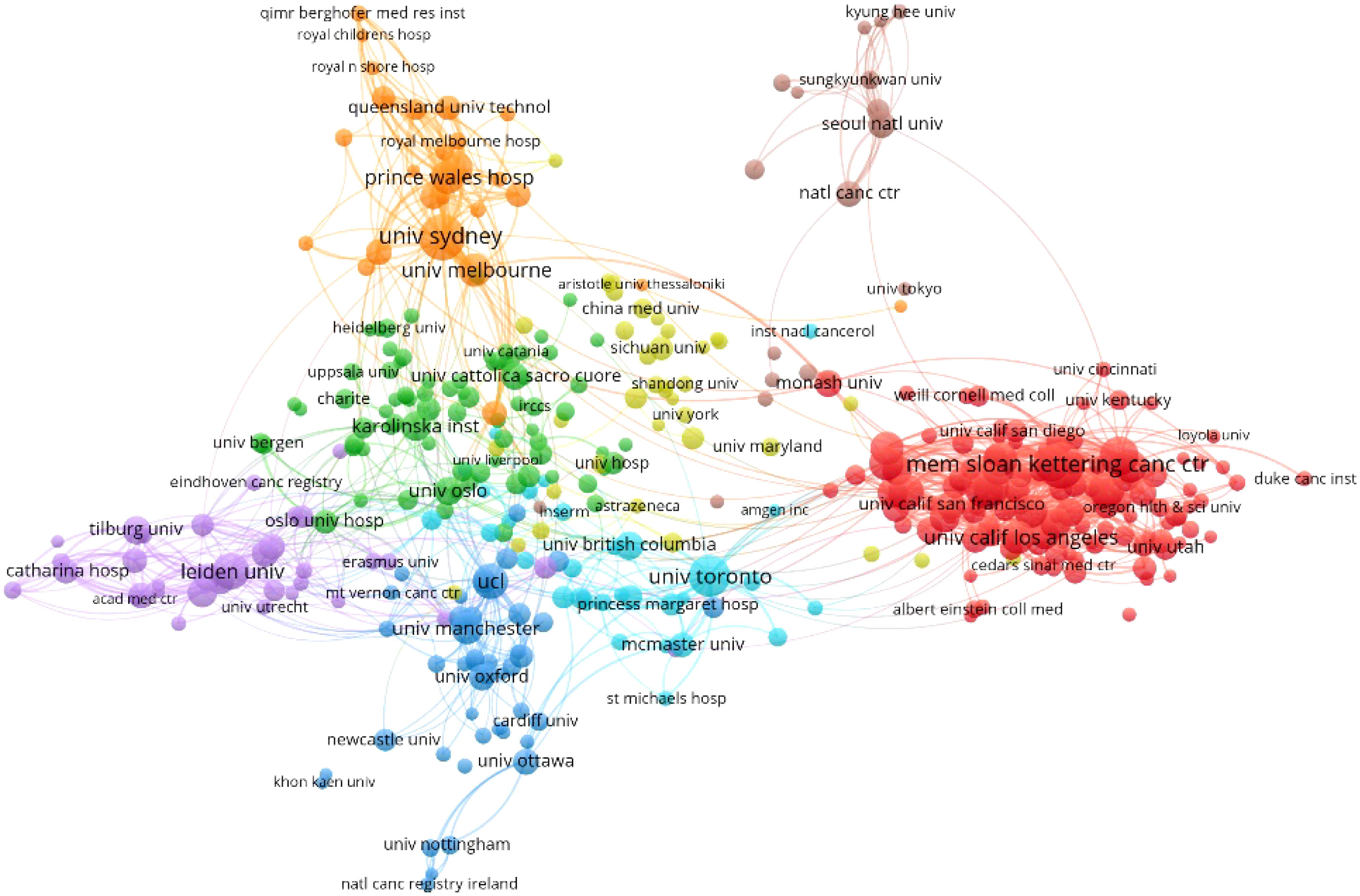
Figure 4 The co-authorship of the institution network.
In this network, only a minimum number of documents of not more than 10 were included, containing 390 organizations. The map shows the largest set of connected items consisting of 389 notes. It contains eight clusters.
The top 10 institutions that contributed to the publications are listed in Table 2. As we can see, most top 10 affiliations came from the United States (n = 6) and one each from Australia, the United Kingdom, Canada, and the Netherlands. The University of Sydney contributes the most (n = 167) in this field, followed by Memorial Sloan Kettering Cancer Center (n = 166) and The University of Texas MD Anderson Cancer Center (n = 164). Memorial Sloan Kettering Cancer Center contributed the most citations (n = 8,399).

Table 2 The top 10 institutions that contributed to the publications.
3.4 Journals
Figure 5 shows the dual-map overlay of journals, with the citing journal in which source articles were published on the left and the cited journal in which references were published on the right. Each spline curve started from a citing journal and pointed to a cited journal. Citing and cited journals are marked with ovals (25). Two green paths and one orange path are demonstrated as main citation paths through z-score analysis. The green paths present that the publications from the medicine/medical/clinical fields were most citing the health/nursing/medicine fields of journals (z = 9.13, f = 24,980) and the molecular/biology/genetics fields of journals (z = 4.98, f = 13,896). The orange path presents that the publications from the molecular/biology/genetics fields were most cited by the molecular/biology/immunology fields of journals (z = 1.67, f = 5042).

Figure 5 The dual-map overlay of journals that contributed to publications.
Table 3 lists the top 10 most relevant journals and most cited journals. Gynecologic Oncology contributed the highest publication numbers (n = 469). Among the top 10 relevant lists, the Journal of Clinical Oncology has the highest impact factor (IF = 50.769), and it also ranked first in the top 10 most cited journals (n = 18,100). The journal with the highest IF in the cited source list was the Lancet (IF = 202.731), followed by the New England Journal of Medicine (IF = 176.079) and JAMA-Journal of the American Medical Association (IF = 157.335). Moreover, it could be seen that four journals are in both the most relevant list and most cited list, namely, Gynecologic Oncology, Cancer, International Journal of Gynecological Cancer, and Journal of Clinical Oncology.
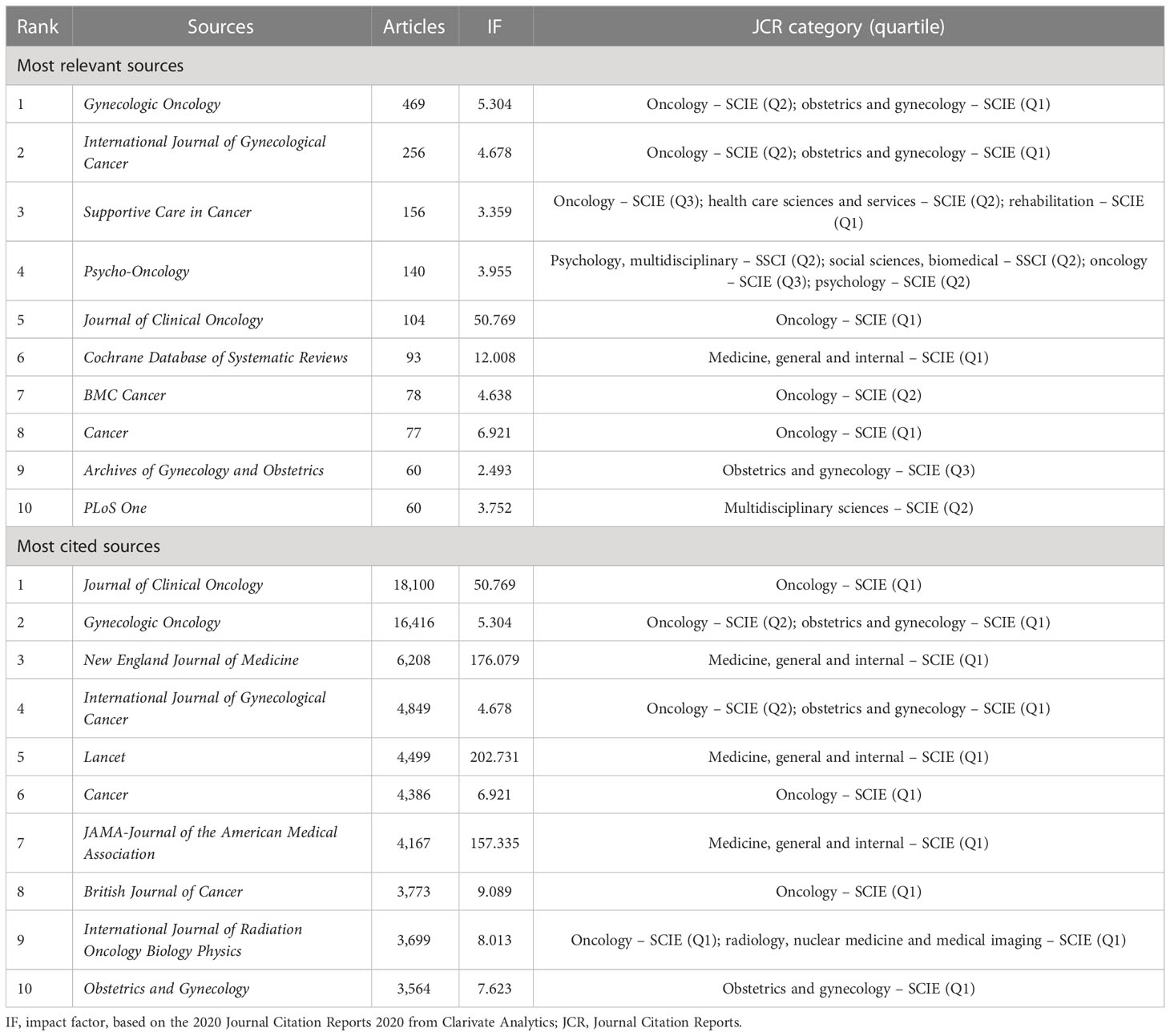
Table 3 Most relevant journals and most cited journals.
3.5 Top cited publications and reference burst
The citation of the document network is shown in Figure 6. The network was based on the number of times they cited each other. There are 748 citations in this document, which meets our minimum requirement of 60. Finally, the largest set of connected items consisted of 496 items and 22 clusters. Table 4 lists the top 20 cited papers according to local citations. The global citation, which means the citation based on the Web of Science database, was also listed in Table 4. The article (Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries) written by Bray F et al. (26) in 2018 had the highest citation both locally (n = 149) and globally (n = 42,425). The top 12 had a local citation of more than 100 times.
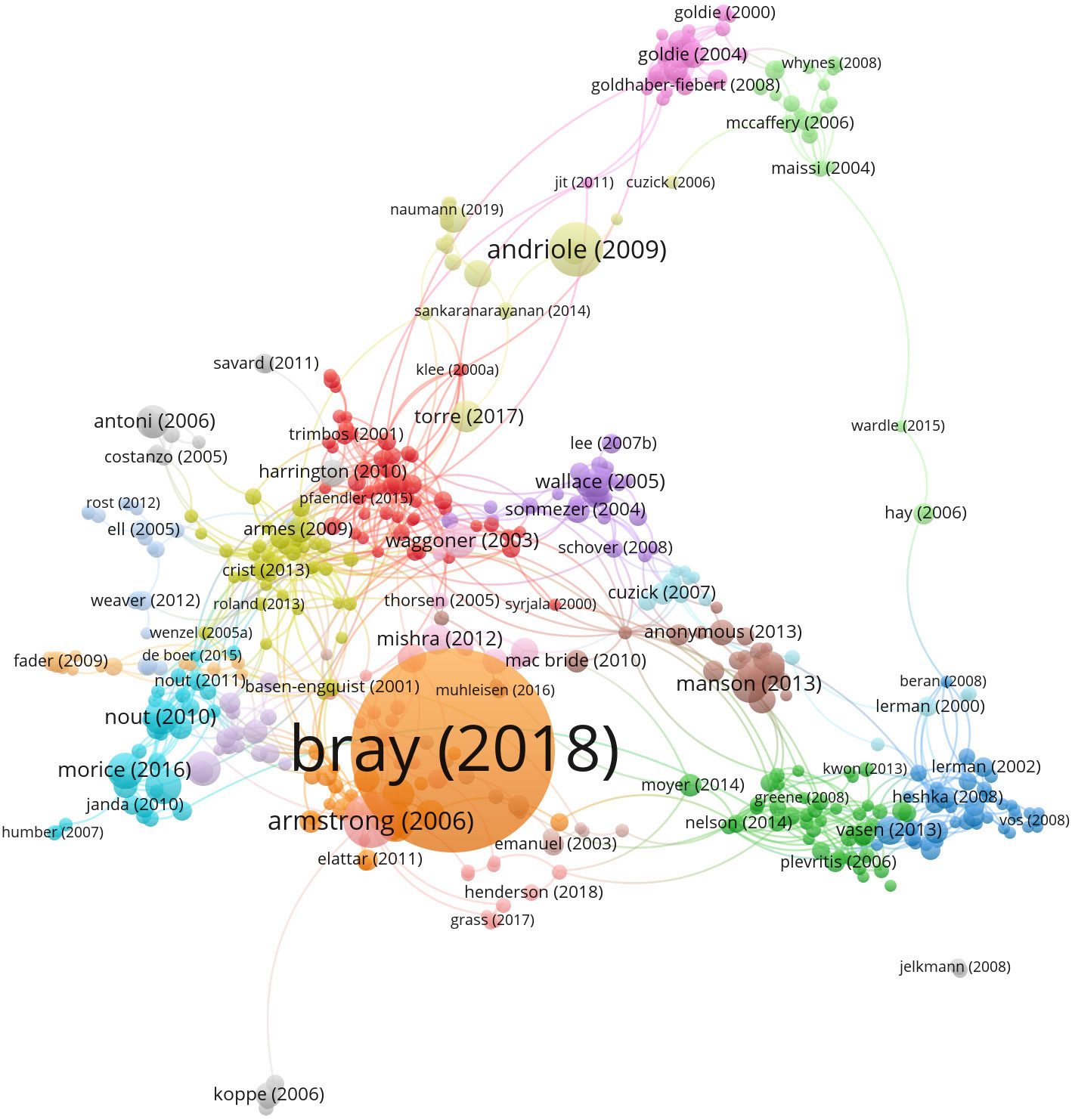
Figure 6 The citation of document network.

Table 4 Top 20 locally cited publications in QoL or mental health of gynecologic oncology patients.
The top 20 references with the strongest citation bursts are shown in Figure 7. The basic meaning of burst detection is that the value of variable changes significantly in a short period of time. The reference with the strongest bursts was published by Bray F et al. in 2018 (strength = 71.11) followed by Siegel RL et al. in 2015 (strength = 35.84) and Ferlay J et al. in 2015 (strength = 30.69). Notably, the article written by Bray F et al. was also with the highest local and global citation numbers listed before. The citation bursts began in 2003 with Rebbeck TR et al. (from 2003 to 2007), Kauff ND et al. (from 2003 to 2007), and Rossouw JE et al. (from 2003 to 2007). The latest citation burst was detected in 2019 due to the article published by Bray F et al. (from 2019 to 2022).
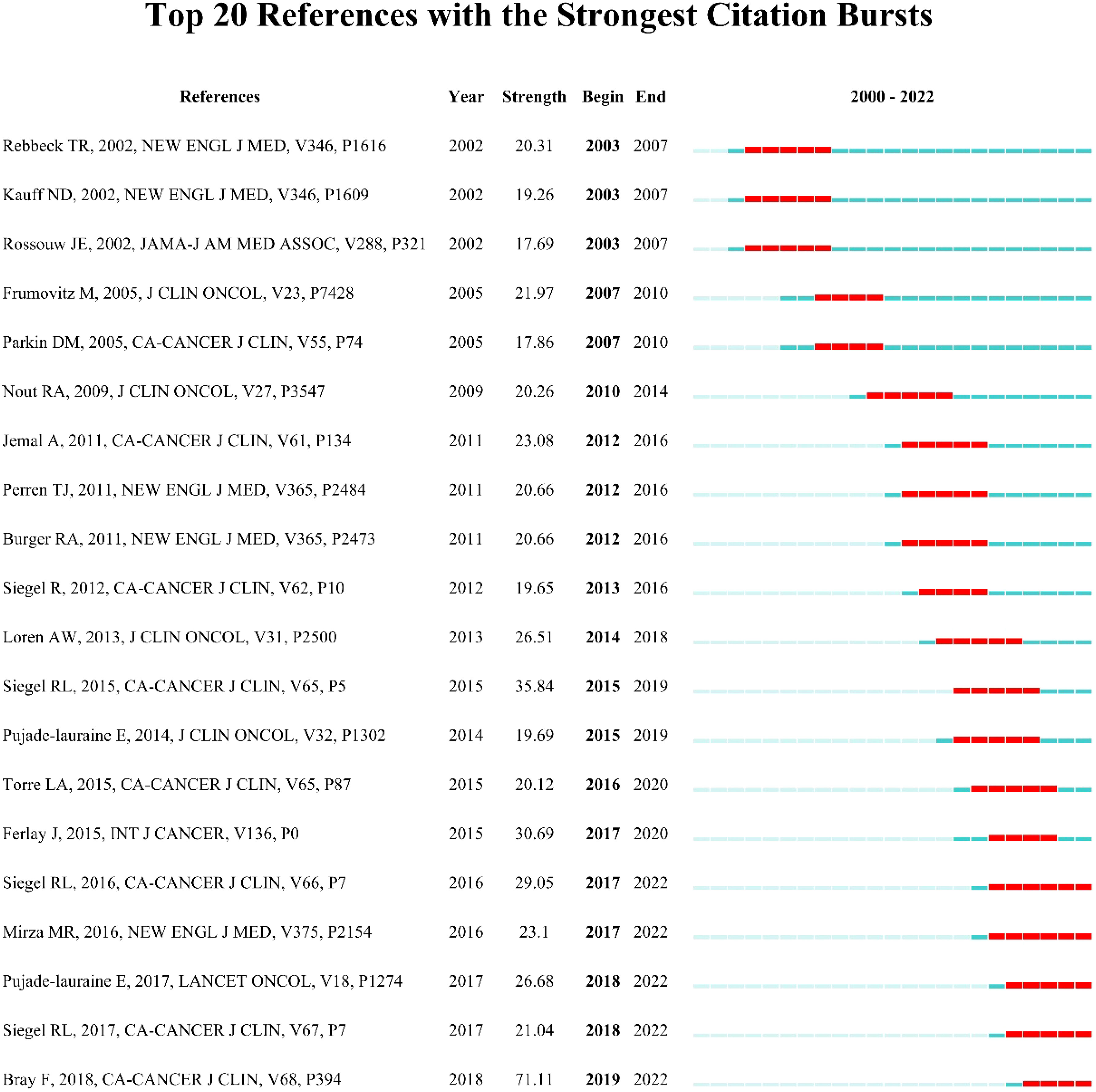
Figure 7 Top 20 references with the strongest citation bursts.
3.6 Contributions of authors
The network of authors and the cluster by keywords are presented in Figure 8. The modularity Q = 0.8285 (Q > 0.3 implies a reasonable clustering structure), and the weighted mean silhouette S = 0.9413 (S > 0.5 means reasonable clustering, and S > 0.7 implies convincing clustering). The largest cluster, #0, was tagged as uterine cervical neoplasms. It could be seen that authors Kim J and Lee J were in this cluster. Table 5 lists the top 10 relevant and most co-cited authors. Kim J was the most productive author with 63 publications, followed by Friedlander M (61 publications) and Lee J (55 publications). The author co-citation analysis of cited paper showed that Aaronson NK ranks first with a count of 426, followed by Siegel RL (356) and Jemal A (334).
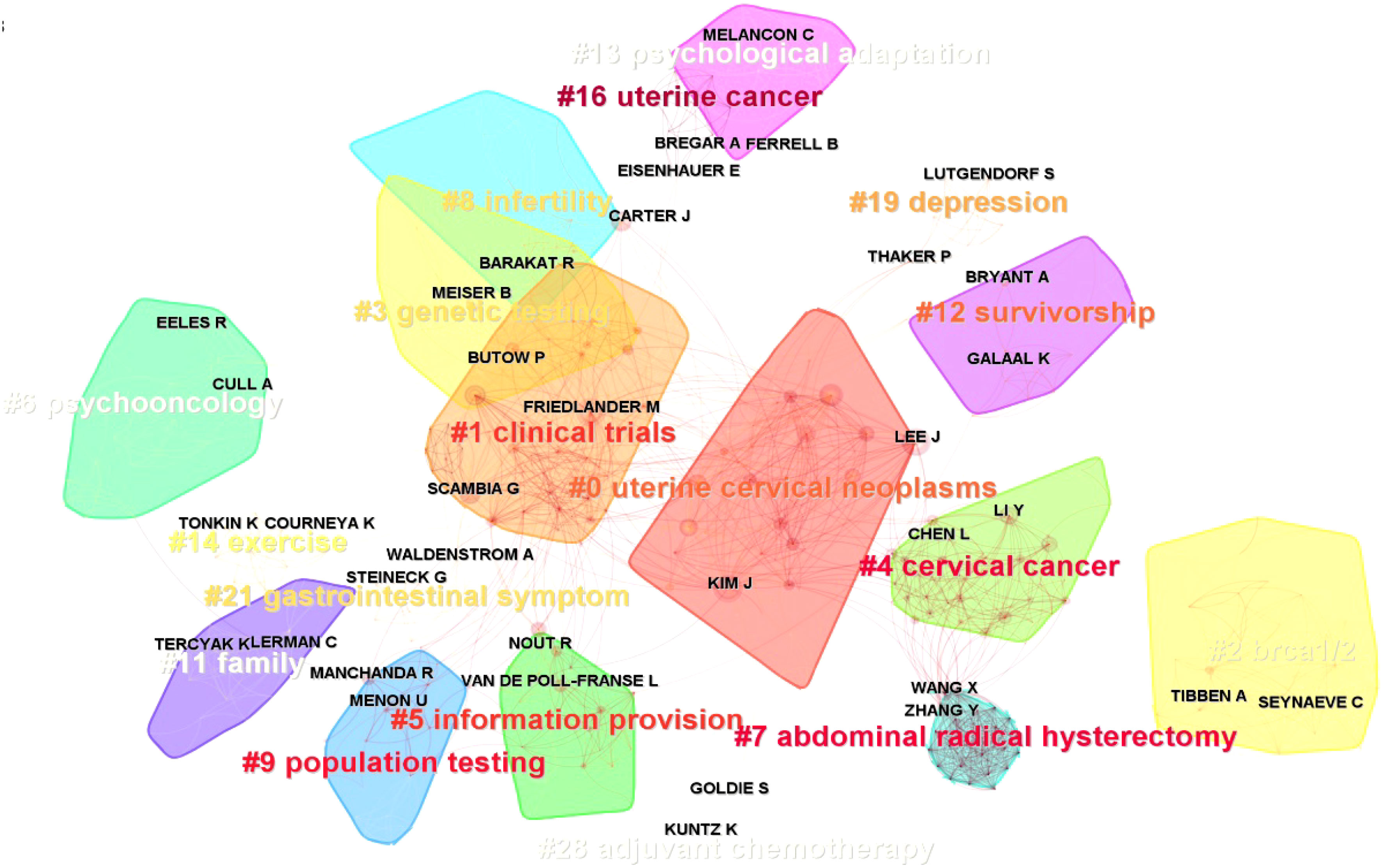
Figure 8 The network of authors involved in quality of life (QoL) or mental health of gynecologic oncology patients.

Table 5 Top 10 most productive authors and most co-cited authors.
3.7 Keywords
A cluster of keywords was made by CiteSpace V software and presented as a timeline view of keywords (Figure 9A). The timeline view could make the newly emerged keywords be recognized easily. The red circle in this figure shows the citation bursts. The clusters were labeled by #0 genetic testing, #1 paclitaxel, #2 quality of life, #3 cervical cancer, and so on. Figure 9B shows the top 20 keywords with the strongest citation bursts. The “psychological impact” had the strongest bursts (strength = 37.03, 2002–2012), followed by “palliative care” (strength = 25.73, 2018–2022). The keywords “mortality” (2016–2022), “fertility preservation” (2016–2022), and “palliative care” (2018–2022) have bursts till 2022.
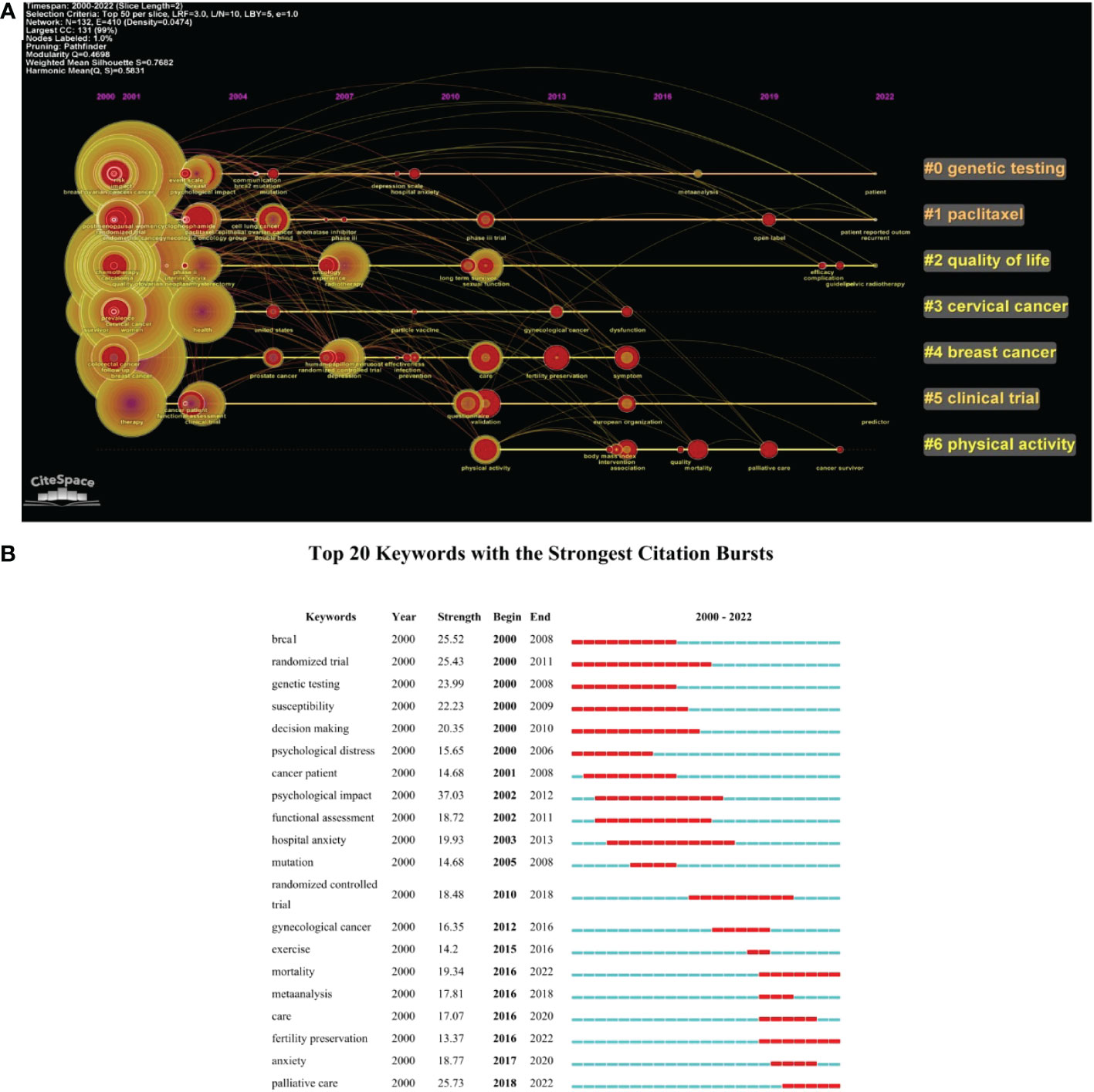
Figure 9 (A) The timeline view of the keywords (with citation bursts in red rings). (B) Top 20 keywords with the strongest citation bursts.
4 Discussion
Our paper conducted a bibliometric analysis of QoL or psychological impact on gynecological cancer patients to show the status and hotspots in this field. The full record and cited references of 6,479 articles and reviews were included in our study from the WOSCC database. Bibliometrix R-package, VOSviewer, and CiteSpace V were applied to extract the items such as countries, institutions, journals, authors, references, and keywords; drew the collaboration network of these items; and pointed the citation bursts.
The United States was the most published country (n = 2,075), with about four times as many publications as China (n = 572, the second) and the United Kingdom (n = 509, the third). Among the top 10 countries, only China is a developing country. As for institutions, although the University of Sydney (Australia) ranked first with 167 papers, the following two institutions were from the United States with a similar number of publications as the top 1, Memorial Sloan Kettering Cancer Center—the world’s largest private cancer research center (n = 166)—and the University of Texas MD Anderson Cancer Center (n = 164). Moreover, six of the top 10 active institutions were from the United States. The other three institutions also came from developed countries, i.e., Canada, the Netherlands, and the United Kingdom. As we can observe, the distribution of countries and institutions was extremely unbalanced, and the United States dominated in this field. Institutions in those developed countries usually have sufficient funding and sound management. They can organize large clinical trial projects, and their patients may have high follow-up rates due to advanced online communication. In addition, most of the standardized scales for QoL or mental health were developed in western contexts (12), so it may be more difficult for developing countries to collect the exact perceptions of their patients.
The most cited publications listed in Table 4 are basically all from 2000 to 2010, except for the first one (26), which was published in 2018. Articles published after 2011 may not have sufficient citations due to the short period of time rather than being less important. Citation bursts of reference could remedy this deficiency to some extent, as the bursts of references can show the active research topics with the time (46). The bursts of keywords can also reflect the trend in this field. The “randomized trial” had the widest year range of bursts (from 2000 to 2011). Then, it was gradually replaced by the related keyword “randomized controlled trial” (from 2010 to 2018). “Meta-analysis” had a burst from 2016 to 2018. The changes in these three keywords can be summarized as an evolution of the active article type in this field. The keywords “mortality”, “fertility preservation”, and “palliative care” are hotspot keywords will a duration until 2022. Mortality is mostly one of the most important endpoints in clinical trials, which deserves attention. The mortality rate of gynecological cancer patients is decreasing year by year substantially (1) (26). Several factors contribute to this, including primary prevention, widespread screening, increased accuracy of diagnosis, treatment efficacy, surgery, radiation and chemotherapy progress, and multidisciplinary treatment of patients (47).
Women of childbearing age who are diagnosed with gynecological cancer represent approximately 21% of those diagnosed (48). As survival rates of gynecologic cancer are increasing, the fertility preservation of reproductive-age women becomes an important part of improving QoL. Fertility-sparing surgical approaches and assisted reproductive technologies (ARTs) can be used as fertility preservation strategies (49). For patients who undergo radiation therapy as adjuvant therapy for fertility without having surgery, ovarian transposition and cryopreservation of oocytes or embryos are the preferred treatments (50). Many new techniques such as antiapoptotic/cell-preserving agents (51), and stem cell technologies (52) are being developed in fertility preservation. Palliative care focuses on providing specialized medical care to alleviate the symptoms and stress of patients suffering from serious illnesses (53). The palliative care team can work with the oncologists to provide support, manage symptoms, and plan advanced care. According to a comparative study, patients who died while in hospice care had an improved QoL when compared to those who were not in hospice care (54). Patients with gynecological cancer, symptom distress, and sexual functional status can also benefit from palliative care (55).
Nowadays, multiple effective treatments for gynecologic cancer have increased the survival rate of patients and improved their QoL. However, this cannot change the fact of incomplete reproductive organs, sexual dysfunction, the side effects of treatments, or the variable recurrence rate, which each patient of gynecological cancer has to face. The psychological impact caused by these facts can be heavy. Patients may suffer from stress, anxiety, depression, sexual dysfunction, and sleep deprivation (56). Many clinical trials have made efforts to improve the QoL and psychological health of their gynecologic cancer patients after treatment. However, two meta-analyses showed that psychosocial interventions (57) and exercise interventions (58) did not demonstrate improvements in QoL. Future studies are needed to explore possible strategies to improve QoL and psychological health after gynecologic cancer treatment.
Our study has some strengths: first of all, it is the first to perform a bibliometric analysis of QoL or psychological impacts of gynecologic cancer patients, and it provides a general view of this field and shows the hotspots and trends. In addition, this study used various bibliometric tools such as bibliometrix R-package, VOSviewer, and CiteSpace V, which enabled better visual analysis. However, there are also some limitations:
1. We only retrieved publications from the WOSCC database, and publications from other databases such as Scopus and PubMed were not included in our local dataset.
2. Only one author screened the publications and extracted information from the database, which may cause bias. However, these works were automatically generated through the website or map tools, which were not manually processed, so there was less chance of error.
3. Using the most cited publications to judge papers may have limits. The highest cited publication is Global Cancer Statistics (Bray F, 2018), which is less relevant to our topics, while some other valuable papers published recently may not be on our list due to the low citations.
5 Conclusion
Overall, our study provides a bibliometric analysis of QoL or psychological impact on gynecological cancer patients. For survivors of gynecologic cancer, attention should be focused on the recovery of their sexual function, the preservation of their fertility, and the maintenance of their feminine image as an important part of improving their QoL and promoting their psychological health. Our study can provide an overview and research hotspots in this field for future studies. It is hoped that further research will provide strategies for improving the QoL and psychological health of women with gynecologic cancer.
Author contributions
JZ participated in data collection, data analysis, and drafting of the paper. YK participated in putting forward the idea, and the drafting and editing of the paper. YX and JY participated in the editing of the paper. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
QoL, quality of life; WOSCC, Web of Science Core Collection; SCP, single-country publication; MCP, multiple-country publication; IF, impact factor; JCR, Journal Citation Reports.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Fleming ND, Ramirez PT, Soliman PT, Schmeler KM, Chisholm GB, Nick AM, et al. Quality of life after radical trachelectomy for early-stage cervical cancer: A 5-year prospective evaluation. Gynecol Oncol (2016) 143(3):596–603. doi: 10.1016/j.ygyno.2016.10.012
3. King MT, Stockler MR, O'Connell RL, Buizen L, Joly F, Lanceley A, et al. Measuring what matters MOST: validation of the measure of ovarian symptoms and treatment, a patient-reported outcome measure of symptom burden and impact of chemotherapy in recurrent ovarian cancer. Qual Life Res (2018) 27(1):59–74. doi: 10.1007/s11136-017-1729-8
4. Rogers L, Siu SS, Luesley D, Bryant A, Dickinson HO. Radiotherapy and chemoradiation after surgery for early cervical cancer. Cochrane Database Syst Rev (2012) 5(5):CD007583. doi: 10.1002/14651858.CD007583.pub3
5. Ye S, Yang J, Cao D, Lang J, Shen K. A systematic review of quality of life and sexual function of patients with cervical cancer after treatment. Int J Gynecol Cancer (2014) 24(7):1146–57. doi: 10.1097/IGC.0000000000000207
6. Macciò A, Madeddu C, Gramignano G, Mulas C, Floris C, Sanna E, et al. A randomized phase III clinical trial of a combined treatment for cachexia in patients with gynecological cancers: evaluating the impact on metabolic and inflammatory profiles and quality of life. Gynecol Oncol (2012) 124(3):417–25. doi: 10.1016/j.ygyno.2011.12.435
7. Sekse RJT, Dunberger G, Olesen ML, Østerbye M, Seibaek L. Lived experiences and quality of life after gynaecological cancer-an integrative review. J Clin Nurs (2019) 28(9-10):1393–421. doi: 10.1111/jocn.14721
8. Manchanda R, Burnell M, Gaba F, Desai R, Wardle J, Gessler S, et al. Randomised trial of population-based BRCA testing in ashkenazi jews: long-term outcomes. BJOG (2020) 127(3):364–75. doi: 10.1111/1471-0528.15905
9. Maughan K, Clarke C. The effect of a clinical nurse specialist in gynaecological oncology on quality of life and sexuality. J Clin Nurs (2001) 10(2):221–9. doi: 10.1046/j.1365-2702.2001.00465.x
10. Suvaal I, Hummel SB, Mens JM, van Doorn HC, van den Hout WB, Creutzberg CL, et al. A sexual rehabilitation intervention for women with gynaecological cancer receiving radiotherapy (SPARC study): design of a multicentre randomized controlled trial. BMC Cancer (2021) 21(1):1295. doi: 10.1186/s12885-021-08991-2
11. Nunes de Arruda F, da Costa S, Bonadio R, Dornellas A, Pereira D, de Bock GH, et al. Quality of life of locally advanced cervical cancer patients after neoadjuvant chemotherapy followed by chemoradiation versus chemoradiation alone (CIRCE trial): a randomized phase II trial. Int J Gynecol Cancer (2020) 30(6):749–56. doi: 10.1136/ijgc-2019-001134
12. Spagnoletti BRM, Bennett LR, Keenan C, Shetty SS, Manderson L, McPake B, et al. What factors shape quality of life for women affected by gynaecological cancer in south, south East and East Asian countries? a critical review. Reprod Health (2022) 19(1):70. doi: 10.1186/s12978-022-01369-y
13. Agarwal S, Bodurka DC. Symptom research in gynecologic oncology: a review of available measurement tools. Gynecol Oncol (2010) 119(2):384–9. doi: 10.1016/j.ygyno.2010.07.009
14. White ID, Sangha A, Lucas G, Wiseman T. Assessment of sexual difficulties associated with multi-modal treatment for cervical or endometrial cancer: A systematic review of measurement instruments. Gynecol Oncol (2016) 143(3):664–73. doi: 10.1016/j.ygyno.2016.08.332
15. Youn BY, Lee SY, Cho W, Bae KR, Ko SG, Cheon C. Global trends of nutrition in cancer research: A bibliometric and visualized analysis study over the past 10 years. Int J Environ Res Public Health (2022) 19(7):4165. doi: 10.3390/ijerph19074165
16. Zyoud SH, Al-Jabi SW, Amer R, Shakhshir M, Shahwan M, Jairoun AA, et al. Global research trends on the links between the gut microbiome and cancer: a visualization analysis. J Transl Med (2022) 20(1):83. doi: 10.1186/s12967-022-03293-y
17. Chen C, Song M. Visualizing a field of research: A methodology of systematic scientometric reviews. PloS One (2019) 14(10):e0223994. doi: 10.1371/journal.pone.0223994
18. Chen C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol (2006) 57(3):359–77. doi: 10.1002/asi.20317
19. Chen C. Science mapping: A systematic review of the literature. J Data Inf Sci (2017) 2(2):1–40. doi: 10.1515/jdis-2017-0006
20. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
21. Garfield E. From the science of science to scientometrics visualizing the history of science with HistCite software. J Informetrics (2009) 3(3):173–9. doi: 10.1016/j.joi.2009.03.009
22. Aria M, Cuccurullo C. Bibliometrix: An r-tool for comprehensive science mapping analysis. J Informetrics (2017) 11(4):959–75. doi: 10.1016/j.joi.2017.08.007
23. Levallois C. Excel/csv converter to network, plugins-For-Gephi. (2013). doi: 10.5281/zenodo.17717.
24. Chen C. Searching for intellectual turning points: Progressive knowledge domain visualization. Proc Natl Acad Sci USA (2004) 101(Suppl.):5303–10. doi: 10.1073/pnas.0307513100
25. Chen C, Leydesdorff L. Patterns of connections and movements in dual-map overlays: A new method of publication portfolio analysis. J Assoc Inf Sci Technol (2014) 65(2):334–51. doi: 10.1002/asi.22968
26. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries [published correction appears in CA cancer J clin. 2020 Jul;70(4):313]. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
27. Greimel ER, Kuljanic Vlasic K, Waldenstrom AC, Waldenstrom AC, Duric VM, Jensen PT, Singer S, et al. The European organization for research and treatment of cancer (EORTC) quality-of-Life questionnaire cervical cancer module: EORTC QLQ-CX24. Cancer (2006) 107(8):1812–22. doi: 10.1002/cncr.22217
28. Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med (2006) 354(1):34–43. doi: 10.1056/NEJMoa052985
29. Basen-Engquist K, Bodurka-Bevers D, Fitzgerald MA, Webster K, Cella D, Hu S, et al. Reliability and validity of the functional assessment of cancer therapy-ovarian. J Clin Oncol (2001) 19(6):1809–17. doi: 10.1200/JCO.2001.19.6.1809
30. Jensen PT, Groenvold M, Klee M, Thranov I, Petersen MA, Machin D. Longitudinal study of sexual function and vaginal changes after radiotherapy for cervical cancer. Int J Radiat Oncol Biol Phys (2003) 56(4):937–49. doi: 10.1016/S0360-3016(03)00362-6
31. Greimel E, Bottomley A, Cull A, Waldenstrom AC, Arraras J, Chauvenet L, et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-OV28) in assessing the quality of life of patients with ovarian cancer. Eur J Cancer (2003) 39:1402–8. doi: 10.1016/S0959-8049(03)00307-1
32. Wenzel L, DeAlba I, Habbal R, Kluhsman BC, Fairclough D, Krebs LU, et al. Quality of life in long-term cervical cancer survivors. Gynecol Oncol (2005) 97(2):310–7. doi: 10.1016/j.ygyno.2005.01.010
33. Vistad I, Fosså SD, Dahl AA. A critical review of patient-rated quality of life studies of long-term survivors of cervical cancer. Gynecol Oncol (2006) 102(3):563–72. doi: 10.1016/j.ygyno.2006.03.050
34. Park SY, Bae DS, Nam JH, Park CT, Cho CH, Lee JM, et al. Quality of life and sexual problems in disease-free survivors of cervical cancer compared with the general population. Cancer (2007) 110(12):2716–25. doi: 10.1002/cncr.23094
35. van Oostrom I, Meijers-Heijboer H, Lodder LN, Duivenvoorden HJ, van Gool AR, Seynaeve C, et al. Long-term psychological impact of carrying a BRCA1/2 mutation and prophylactic surgery: a 5-year follow-up study. J Clin Oncol (2003) 21(20):3867–74. doi: 10.1200/JCO.2003.10.100
36. Nout RA, Smit VT, Putter H, Jürgenliemk-Schulz IM, Jobsen JJ, Lutgens LC, et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): An open-label, non-inferiority, randomised trial. Lancet (2010) 375:816–23. doi: 10.1016/S0140-6736(09)62163-2
37. Jensen PT, Groenvold M, Klee MC, Thranov I, Petersen MA, Machin D. Early-stage cervical carcinoma, radical hysterectomy, and sexual function. A Longitudinal Study Cancer (2004) 100(1):97–106. doi: 10.1002/cncr.11877
38. Madalinska JB, Hollenstein J, Bleiker E, van Beurden M, Valdimarsdottir HB, Massuger LF, et al. Quality-of-life effects of prophylactic salpingo-oophorectomy versus gynecologic screening among women at increased risk of hereditary ovarian cancer. J Clin Oncol (2005) 23(28):6890–8. doi: 10.1200/JCO.2005.02.626
39. Juraskova I, Butow P, Robertson R, Sharpe L, McLeod C, Hacker N. Post-treatment sexual adjustment following cervical and endometrial cancer: a qualitative insight. Psychooncology (2003) 12(3):267–79. doi: 10.1002/pon.639
40. Wenzel LB, Donnelly JP, Fowler JM, Habbal R, Taylor TH, Aziz N, et al. Resilience, reflection, and residual stress in ovarian cancer survivorship: a gynecologic oncology group study. Psychooncology (2002) 11(2):142–53. doi: 10.1002/pon.567
41. Greimel ER, Winter R, Kapp KS, Haas J. Quality of life and sexual functioning after cervical cancer treatment: a long-term follow-up study. Psychooncology (2009) 18(5):476–82. doi: 10.1002/pon.1426
42. Korfage IJ, Essink-Bot ML, Mols F, van de Poll-Franse L, Kruitwagen R, van Ballegooijen M. Health-related quality of life in cervical cancer survivors: a population-based survey. Int J Radiat Oncol Biol Phys (2009) 73(5):1501–9. doi: 10.1016/j.ijrobp.2008.06.1905
43. Maissi E, Marteau TM, Hankins M, Moss S, Legood R, Gray A. Psychological impact of human papillomavirus testing in women with borderline or mildly dyskaryotic cervical smear test results: cross sectional questionnaire study. BMJ (2004) 328(7451):1293. doi: 10.1136/bmj.328.7451.1293
44. Meiser B. Psychological impact of genetic testing for cancer susceptibility: an update of the literature. Psychooncology (2005) 14(12):1060–74. doi: 10.1002/pon.933
45. Bradley S, Rose S, Lutgendorf S, Costanzo E, Anderson B. Quality of life and mental health in cervical and endometrial cancer survivors. Gynecol Oncol (2006) 100(3):479–86. doi: 10.1016/j.ygyno.2005.08.023
46. Chen C, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: a scientometric update (2000 - 2014). Expert Opin Biol Ther (2014) 14(9):1295–317. doi: 10.1517/14712598.2014.920813
47. La Rosa VL, Shah M, Kahramanoglu I, Cerentini TM, Ciebiera M, Lin LT, et al. Quality of life and fertility preservation counseling for women with gynecological cancer: an integrated psychological and clinical perspective. J Psychosom Obstet Gynaecol (2020) 41(2):86–92. doi: 10.1080/0167482X.2019.1648424
48. McKenzie ND, Kennard JA, Ahmad S. Fertility preserving options for gynecologic malignancies: A review of current understanding and future directions. Crit Rev Oncol Hematol (2018) 132:116–24. doi: 10.1016/j.critrevonc.2018.09.020
49. Taylan E, Oktay K. Fertility preservation in gynecologic cancers. Gynecol Oncol (2019) 155(3):522–9. doi: 10.1016/j.ygyno.2019.09.012
50. Willows K, Lennox G, Covens A. Fertility-sparing management in cervical cancer: balancing oncologic outcomes with reproductive success. Gynecol Oncol Res Pract (2016) 3:9. doi: 10.1186/s40661-016-0030-9
51. Li F, Turan V, Lierman S, Cuvelier C, De Sutter P, Oktay K. Sphingosine-1-phosphate prevents chemotherapy-induced human primordial follicle death. Hum Reprod (2014) 29(1):107–13. doi: 10.1093/humrep/det391
52. White YA, Woods DC, Takai Y, Ishihara O, Seki H, Tilly JL. Oocyte formation by mitotically active germ cells purified from ovaries of reproductive-age women. Nat Med (2012) 18(3):413–21. doi: 10.1038/nm.2669
53. Lefkowits C, Solomon C. Palliative care in obstetrics and gynecology. Obstet Gynecol (2016) 128(6):1403–20. doi: 10.1097/AOG.0000000000001739
54. Wallston KA, Burger C, Smith RA, Baugher RJ. Comparing the quality of death for hospice and non-hospice cancer patients. Med Care (1988) 26(2):177–82. doi: 10.1097/00005650-198802000-00008
55. Mullen MM, Cripe JC, Thaker PH. Palliative care in gynecologic oncology. Obstet Gynecol Clin North Am (2019) 46(1):179–97. doi: 10.1016/j.ogc.2018.10.001
56. Alanazi MT, Alanazi NT, Alfadeel MA, Bugis BA. Sleep deprivation and quality of life among uterine cancer survivors: systematic review. Support Care Cancer (2022) 30(3):2891–900. doi: 10.1007/s00520-021-06589-9
57. Kalter J, Verdonck-de Leeuw IM, Sweegers MG, Aaronson NK, Jacobsen PB, Newton RU, et al. Effects and moderators of psychosocial interventions on quality of life, and emotional and social function in patients with cancer: An individual patient data meta-analysis of 22 RCTs. Psychooncology (2018) 27(4):1150–61. doi: 10.1002/pon.4648
Keywords: quality of life, psychologic, genital neoplasms, female, bibliometrics, VOSviewer, CiteSpace
Citation: Zhao J, Kong Y, Xiang Y and Yang J (2023) The research landscape of the quality of life or psychological impact on gynecological cancer patients: A bibliometric analysis. Front. Oncol. 13:1115852. doi: 10.3389/fonc.2023.1115852
Received: 04 December 2022; Accepted: 10 January 2023;
Published: 07 February 2023.
Edited by:
Paolo Scollo, Kore University of Enna, ItalyReviewed by:
Alessia Passanisi, Kore University of Enna, ItalySonia La Spina, Cannizzaro Hospital, Italy
Copyright © 2023 Zhao, Kong, Xiang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junjun Yang, eWFuZ2p1bmp1bkBwdW1jaC5jbg==