
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 09 February 2023
Sec. Thoracic Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1115156
This article is part of the Research TopicPrimary and Acquired Resistance in Lung CancerView all 10 articles
 Greta Alì1
Greta Alì1 Anello Marcello Poma2
Anello Marcello Poma2 Iosè Di Stefano2Carmelina Cristina Zirafa3Alessandra Lenzini3
Iosè Di Stefano2Carmelina Cristina Zirafa3Alessandra Lenzini3 Giulia Martinelli2
Giulia Martinelli2 Gaetano Romano3Antonio Chella4
Gaetano Romano3Antonio Chella4 Editta Baldini5
Editta Baldini5 Franca Melfi3
Franca Melfi3 Gabriella Fontanini2*
Gabriella Fontanini2*Introduction: Non-small cell lung cancer (NSCLC) is the leading cause of cancer incidence and mortality worldwide. Neoadjuvant chemo-immunotherapy has led to clinical benefits in resectable NSCLC in comparison to chemo-therapy alone. Major pathological response (MPR) and pathological complete response (pCR) have been used as surrogates of neoadjuvant therapy response and clinical outcomes. However, the factors affecting the pathological response are still controversial. Therefore, in this study we retrospectively examined MPR and pCR in two different cohorts of NSCLC patients, 14 treated by chemotherapy and 12 by chemo-immunotherapy in the neoadjuvant setting.
Methods: In resected tumor specimens, different histological characteristics were evaluated: necrosis, fibrosis, inflammation, presence of organizing pneumonia, granuloma, cholesterol cleft, and reactive epithelial alterations. In addition, we evaluated how MPR impacts on event-free survival (EFS) and overall survival (OS). In a small group of patients treated by chemo-immunotherapy, a gene expression analysis of the Hippo pathway was performed both in preoperative biopsies and matched post-surgical specimens.
Results: We observed a better pathological response in the chemo-immunotherapy treated cohort: 6/12 patients (50.0%) achieved a MPR ≤10% and 1/12 (8.3%) achieved pCR both on primary tumor and on lymph nodes. On the contrary, no patient treated with chemotherapy alone achieved pCR or MPR ≤10%. A higher amount of stroma in the neoplastic bed was observed in patients treated with immuno-chemotherapy. Moreover, patients achieving better MPR (including pCR) had significantly improved overall survival (OS) and event-free survival (EFS). After neoadjuvant chemo-immunotherapy, residual tumors showed a remarkable upregulation of genes consistent with the activation of YAP/TAZ. Also, alternative checkpoint, such as CTLA-4, were enhanced.
Discussion: Our findings showed that neoadjuvant chemo-immunotherapy treatment improves MPR and pCR thus resulting in better EFS and OS. Moreover, a combined treatment could induce different morphological and molecular changes in comparison to chemotherapy alone, thus giving new insights in the assessment of pathological response.
Non-small cell lung cancer (NSCLC) is the greatest cause of cancer death. Despite recent improvements in the treatment of advanced NSCLC, little is known about therapy efficacy in resectable tumors (1, 2). Although the advances in staging, surgical techniques, and the introduction of adjuvant chemotherapy for stage II and III NSCLC, a large number of operated patients experience disease recurrence (3). In particular, patients with resectable NSCLC at high risk of recurrence may benefit from neoadjuvant or adjuvant chemotherapy, but the 5-year overall survival is reached only in 5% of cases (4). In recent years, immunotherapy emerged as a therapeutic option for lung cancer, and neoadjuvant immunotherapy can be a good alternative for patients with resectable NSCLC. In the neoadjuvant setting immunotherapy, a combination of chemotherapy and immunotherapy, and targeted therapies are currently under investigation (5–7).
However, there are no established guidelines about the assessment of response to neoadjuvant therapy on resected lung cancer specimens. Over the years, different approaches have been used to assess pathological response, including pathological complete response (pCR) and major pathological response (MPR) (8, 9). Previous studies have suggested a positive association between pathological response, mainly pCR, and clinical outcome of patients. It has been demonstrated that patients with NSCLC showing a MPR of 10% or less have a significantly better outcome after neoadjuvant chemotherapy (10–12). As regards immunotherapy alone data are still limited.,. However, a neoadjuvant chemo-immunotherapy may increase the proportion of patients achieving a major pathological response (MPR) (13, 14). Indeed, available studies (15) showed that neoadjuvant chemo-immunotherapy can be more effective than chemotherapy alone in patients with resectable NSCLC. However, a considerable percentage of tumors do not completely respond to neoadjuvant chemo-immunotherapy, and patients may develop early disease progression (16). Thus, the identification of patients without a substantial pathological response is crucial to adjust treatment. To date, no studies have compared the pathological response to chemotherapy and to chemo-immunotherapy in NSCLC. In this study we retrospectively examined the efficacy of neoadjuvant chemotherapy and chemo-immunotherapy in patients with NSCLC comparing the MPR and several histological characteristics such as necrosis, fibrosis, and inflammation both in the tumor and in the collateral lung parenchyma. In addition, we evaluated how MPR impacts on event-free survival (EFS) and overall survival (OS). Moreover, in a small group of patients treated with chemo-immunotherapy, we performed a gene expression analysis of the Hippo pathway, crucial for tissue repair and associated with treatment resistance, both in preoperative biopsies and matched post-surgical specimens.
We retrospectively enrolled 26 NSCLC patients, including 14 who had received chemotherapy and 12 who had received chemo-immunotherapy in the neoadjuvant setting, from April 2017 to January 2021 and from December 2018 to October 2021, respectively. In detail, Surgical specimens of patients were collected from the archives of the Operative Unit of Pathological Anatomy III of the University Hospital of Pisa. In detail, tumors included 14 adenocarcinoma (ADC), 8 squamous cell carcinoma (SCC), 1 adenosquamous carcinoma, 1 pleomorphic carcinoma, and 2 large cell neuroendocrine carcinoma obtained from patients who underwent surgical resection at the Department of Cardiothoracic Surgery of the University Hospital of Pisa. For 5 patients treated with combined chemo-immunotherapy, we also collected pre-surgical biopsies. Participation in this study required informed consent. Treatment regimens and indications for surgery were determined by a multidisciplinary team. All patients received surgery within 4-6 weeks after neoadjuvant chemo-immunotherapy or chemotherapy. In detail, 14 patients received 2-4 cycles of a conventional platinum-based doublet chemotherapy regimen, whereas 12 patients received 2-6 cycles of a conventional platinum-based doublet chemotherapy regimen combined with PD-1 (pembrolizumab, n=4) or PD-L1 inhibitors, (atezolizumab in 6 cases and durvalumab in 2 cases). As per standard institutional procedures, all surgical resections were performed with thoracotomy, video-assisted thoracoscopic surgery, or robotic-assisted pulmonary resection.
Clinical information including patient sex, age, molecular status, PD-L1 immunohistochemical expression, EFS, and OS, were reviewed for each patient. EFS was considered as the time from the start of neoadjuvant treatment until disease progression. OS was considered from the start of therapy to the date of death or censored at the last follow-up. This study was approved by the ethics committee “Comitato Etico di Area Vasta Nord Ovest” (CEAVNO) for Clinical Experimentation (Protocol Number: ID19211).
Information on neoadjuvant therapy, such as medication and course of treatment, was documented. Tumors were staged according to the American Joint Committee on Cancer Lung Cancer Staging, 8th edition (17). The pathological response was assessed independently by two pathologists (GA and IDS) that evaluated both pCR and MPR. MPR was defined as residual viable tumor cells in the primary tumor bed and sampled lymph nodes. MPR was reported both as a continuous variable and using the 10% cut-off, whereas pCR was defined as the complete absence of residual viable tumor cells in the primary tumor (8, 9).
In detail, according to the recommendations of The International Association for the Study of Lung Cancer (IASLC) (9), if the tumor bed was small (≤ 3 cm) the tumor was entirely sampled. If the tumor bed was larger than 3 cm, the tumor was cut in serial sections approximately 0.5 cm thick and after gross inspection the most representative cross section showing viable tumor was sampled (at least one cross section of the entire tumor). If no viable tumor was identified in the cross sections, the remaining tumor tissue was examined histologically to see if any viable tumor was present. Besides tumor cells, the percentages of major components of the tumor bed such as necrosis and stroma (which includes inflammatory cells and fibrosis) were calculated with the total adding up to 100%, as previously described (9). The percentage of residual viable tumor was estimated by comparing the estimated cross-sectional area of the viable tumor foci with estimated cross-sectional areas of necrosis, fibrosis, and inflammation on each hematoxylin and eosin slide. The results for all slides were averaged together to determine the mean values for each patient (10). For lymph node pathological response, the same approach was used for histological evaluation that was used for the resected lung cancer.
Moreover, we calculated the pathological regression (PR) evaluated as 100 - the percentage of residual viable tumor cells. Finally, we evaluated other histological features in the tumor microenvironment such as inflammation, fibrosis, presence of organizing pneumonia, granuloma, cholesterol cleft, and reactive epithelial alterations.
PD-L1 expression before treatment was detected by using the rabbit monoclonal primary antibody SP263 and the expression was evaluated by tumor proportion score (TPS).
For all samples, tumor cell percentage was estimated independently by two expert pathologists and tumor component was enriched by manual macrodissection before nucleic acid extraction. In detail, total RNA was purified from three-to-four unstained formalin-fixed paraffin embedded (FFPE) sections (10 µm-thick) using the Qiagen RNeasy FFPE kit (Qiagen, Hilden, Germany), and according to the manufacturer’s suggestions. RNA quality and concentration were assessed using an Xpose spectrophotometer (Trinean, Gentbrugge, Belgium). About 150 ng of total RNA were used for gene expression analysis using the nCounter system (nanoString Technologies, Seattle, WA, USA). A custom panel of 88 genes was designed including 10 housekeeping genes (i.e., CLTC, EDC3, GAPDH, GUSB, HPRT1, MRPS5, NUBP1, PGK1, PRPF38A, SF3A3), 4 genes encoding for immune checkpoint proteins (i.e., CD274, CTLA4, PDCD1, VSIR) and 74 genes belonging to the Hippo pathway. The complete list of genes is reported in Supplementary Table S1. Total RNA was hybridized with capture and reporter probes at 60°C for 20 hours; cleanup of samples and counts of digital reports were performed as described by the manufacturer (nanoString Technologies).
Continuous variables are presented as median and interquartile range (IQR) and were tested by the Mann-Whitney test or by the Kruskal-Wallis test followed by the Dunn test. Categorical variables were tested by the Fisher exact test. Correlations between continuous variables were evaluated by Pearson correlation.
For gene expression analysis, raw counts were normalized using the nCounter Advanced Analysis (nanoString Technologies). Differentially expressed genes were computed following the procedures of the nCounter Advanced Analysis. P-values were adjusted by the Benjamini-Hochberg method, and a false discovery rate (FDR) of 0.05 was considered significant. Principal component analysis (PCA) was performed using PCAtools v.2.10.0 package, while hierarchical clustering was carried out using heatmap3 v. 1.1.9 package. Optimal cut-off for MPR was assessed by the Contal and O’Quigley’s method and using the survMisc v.0.5.6 package. Survival curves were estimated by the Kaplan-Meier method following the procedures of survival v.3.4-0 package and plotted using survminer v.0.4.9 package. Hazard ratio (HR) was estimated using the Cox regression method.
All analysis and plots were generated in R environment v.4.1.2 (https://www.r-project.org/, last accessed November 14, 2022) unless otherwise specified.
Clinico-pathological characteristics of patients are summarized in Table 1. Twenty-three patients with resectable NSCLC were included: 8 were females and 18 males aged from 41 to 78 years old (median age of 66 years). Twelve patients were treated with combined chemo-immunotherapy and 14 with chemotherapy. Most patients (50.8%) had stage IA to IB disease, 5 (19.2%) had stage IIB, 7 (26.2%) had stage IIIA and IIIB, and one (3.8%) patient had stage IVA. For the combined immuno-chemotherapy treated patients, 10 (83.3%) had a PD-L1 TPS of 1% or higher and 2 (16.7%) had TPS of 50% or higher. For chemotherapy treated patients, 3 (21.4%) had PD-L1 negative, 9 (64.2%) had tumor with low PD-L1 expression (TPS 1-49%), and 2 (14.4%) had tumor with high PD-L1 (TPS ≥ 50%).
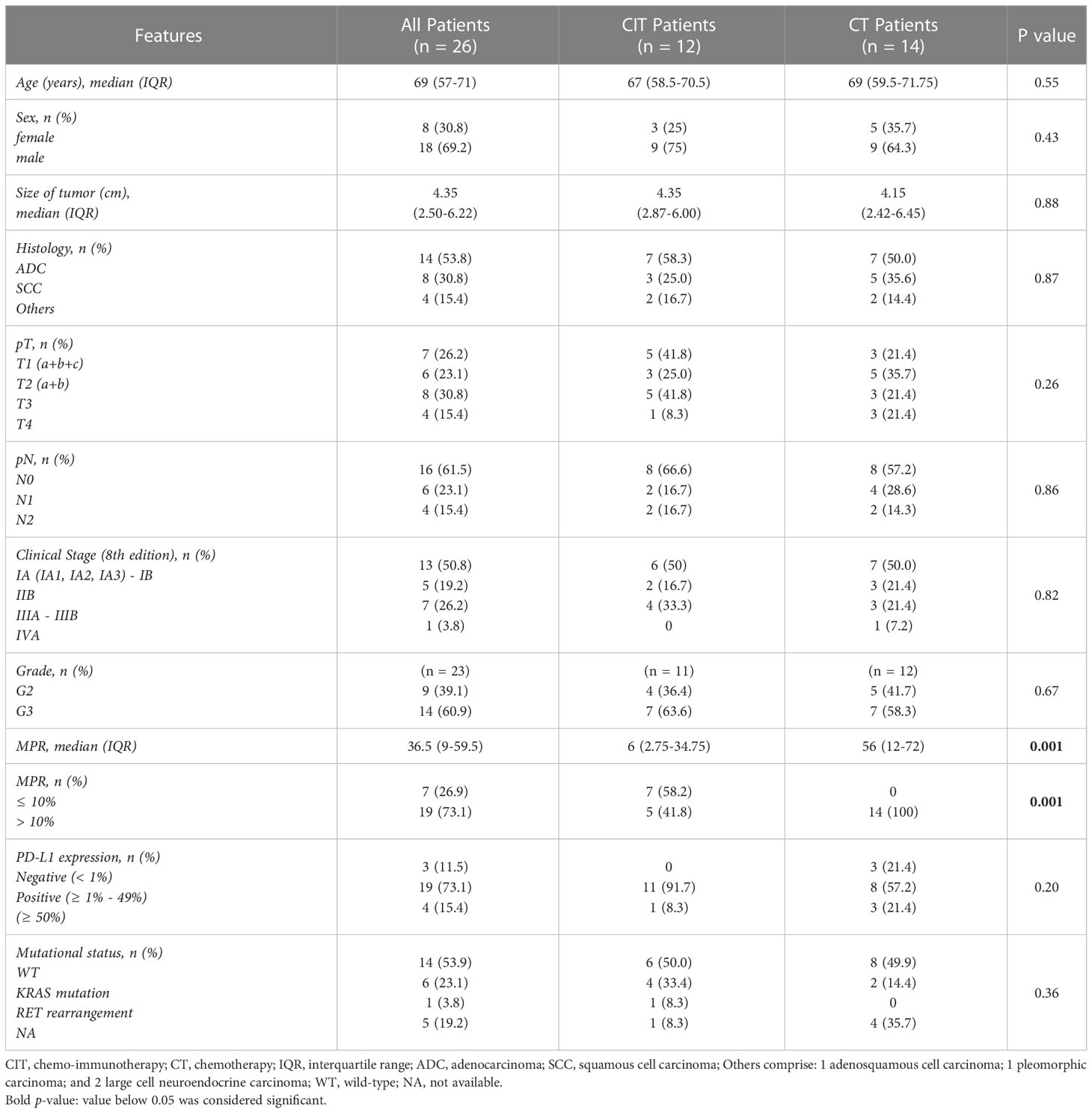
Table 1 Clinicopathological characteristics and pathological response of NSCLC patients according to treatment regimens.
No significant differences between the two neoadjuvant therapy groups were observed in terms of age, sex, histological tumor type, size of tumors, TNM stage, grade, PD-L1 expression, and mutational status (Table 1).
Major pathological response was different between the two cohorts of patients both as continuous variable (p < 0.0001) and considering the 10% cut-off (p < 0.0001) (Table 1). In detail, 7 patients treated with combined immuno-chemotherapy (58.3%) achieved a MPR ≤10% and one patient (3.8%) pCR in the primary tumor and sampled lymph nodes. On the other hand, no chemotherapy treated patients achieved MPR ≤10% or pCR (Figure 1). The waterfall plot shows pathological regression in the resected primary lung tumor after neoadjuvant treatment (Figure 2).
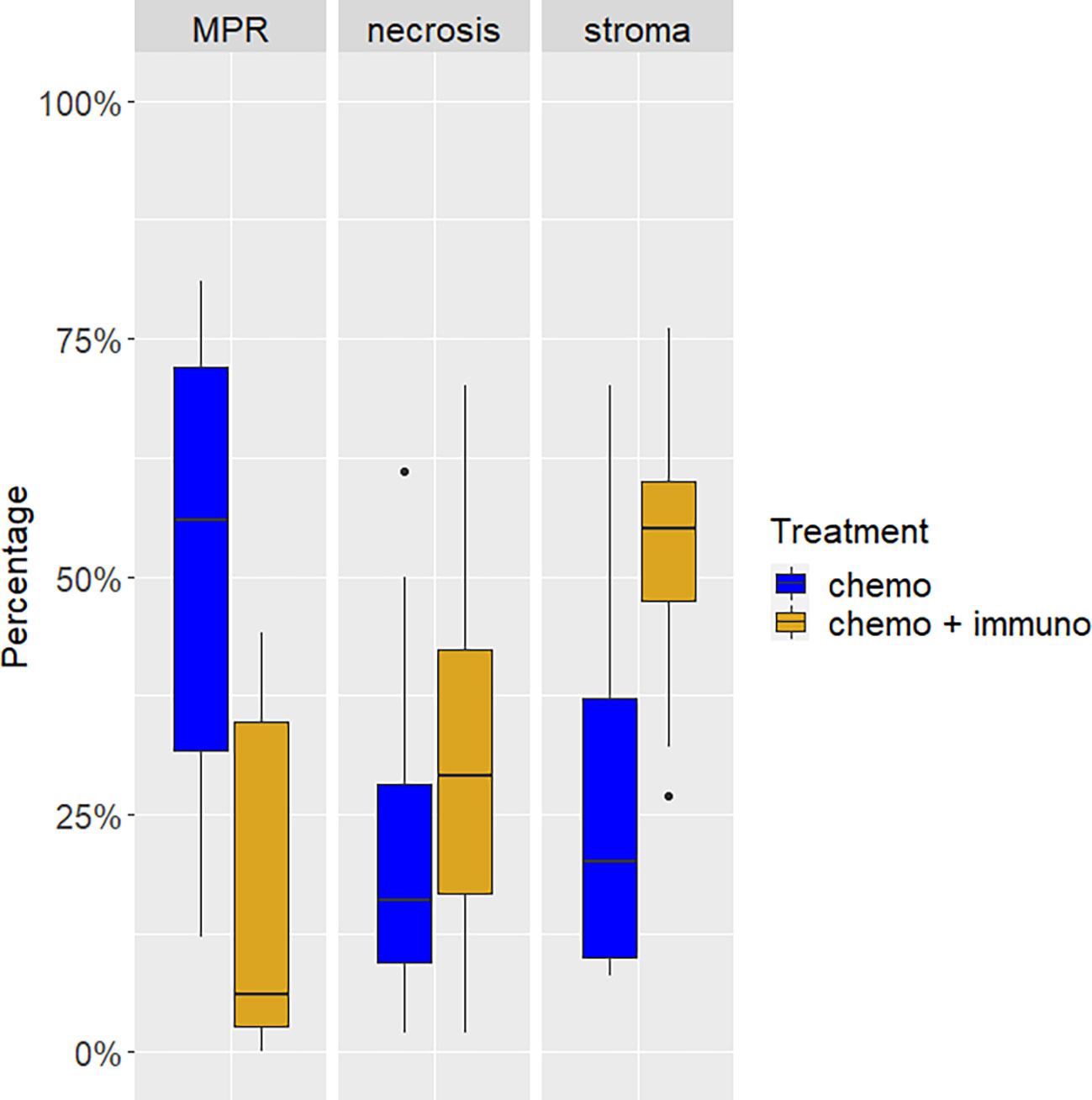
Figure 1 Tumor composition after neoadjuvant treatment with chemo- or chemo-immunotherapy. The proportion of viable tumor cells (major pathological response, MPR) was lower in tumors from patients of the chemo-immunotherapy cohort. These cases showed also a higher proportion of necrosis and stroma.
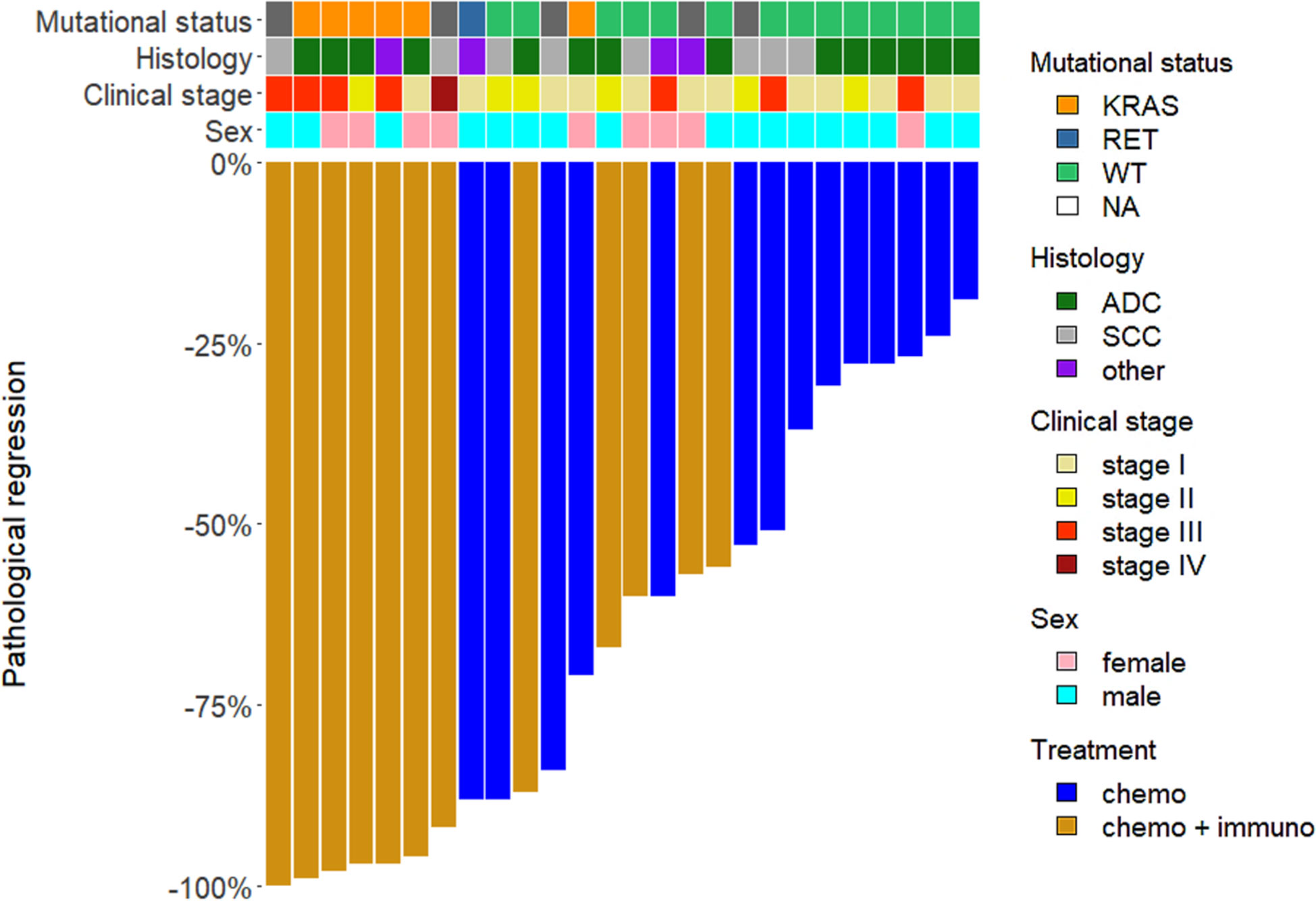
Figure 2 Waterfall plot of pathological response. The bars represent patients according to the different neoadjuvant treatments, chemotherapy alone (chemo) and chemo-immunotherapy (chemo-immuno). The upper rows show clinic-pathological characteristics of patients (mutational status, histology, clinical stage, sex). WT, wild-type; NA, not available; ADC, adenocarcinoma; SCC, squamous cell carcinoma.
To further explore the pathological response after treatment, we evaluated also several histological features on tumor specimens and in the surrounding lung parenchyma (Figures 3A–F). We observed a significantly higher amount of stroma in the neoplastic bed in the cohort of patients treated with immuno-chemotherapy (p = 0.004) (Figure 1). The evaluation of stroma included fibrosis and inflammation in the tumor bed. However, we did not observe statistically significant differences in terms of fibrosis and inflammation as well as the presence of organizing pneumonia, granuloma, cholesterol cleft, and reactive epithelial alterations. Although these morphological characteristics did not reach statistical significance in the two different treatment cohorts, they were less prominent or absent in patients treated with chemotherapy alone. The complete list of histological features is summarized in Table 2.
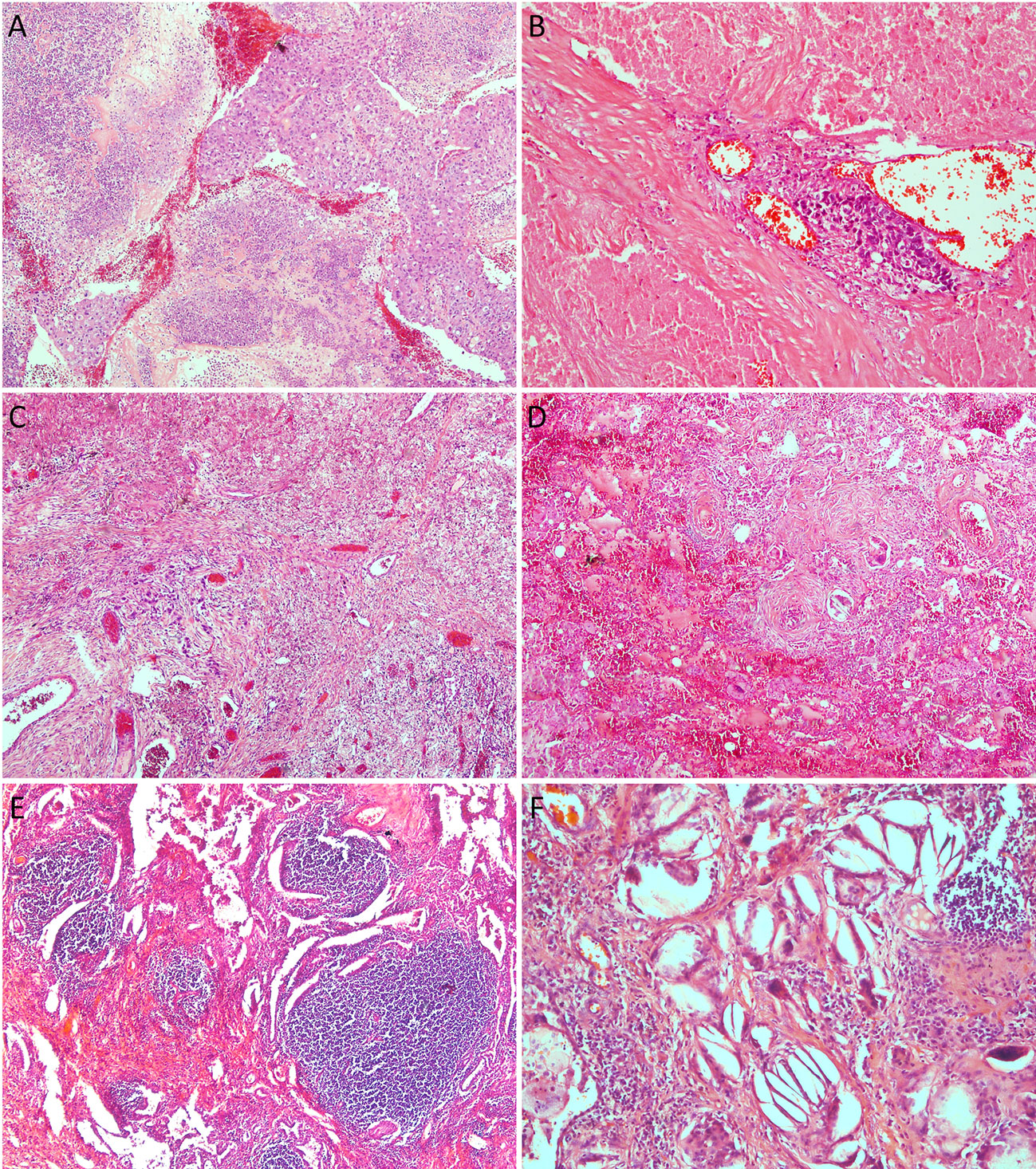
Figure 3 Histologic features after neoadjuvant therapy: (A), area of solid nests of chemotherapy treated squamous cell carcinoma surrounded by necrotic areas (magnification x 10); (B), chemo-immunotherapy treated tumor with a large area of necrosis showing a single focus of viable adenocarcinoma (magnification x 20); (C), focus of atypical cells of chemo-immunotherapy treated tumor with adenocarcinoma histology surrounded by dense fibrosis (magnification x 4); (D), chemotherapy treated tumor with larger area of dense fibrosis with abundant foamy histiocytes (magnification x 4); (E), this area of chemo-immunotherapy treated tumor shows fibrosis with extensive inflammatory infiltrate of lymphocytes and plasma cells (magnification x 4); (F), high power of the same tumor showing chronic inflammation, cholesterol clefts, foamy histiocytes, and fibrosis.
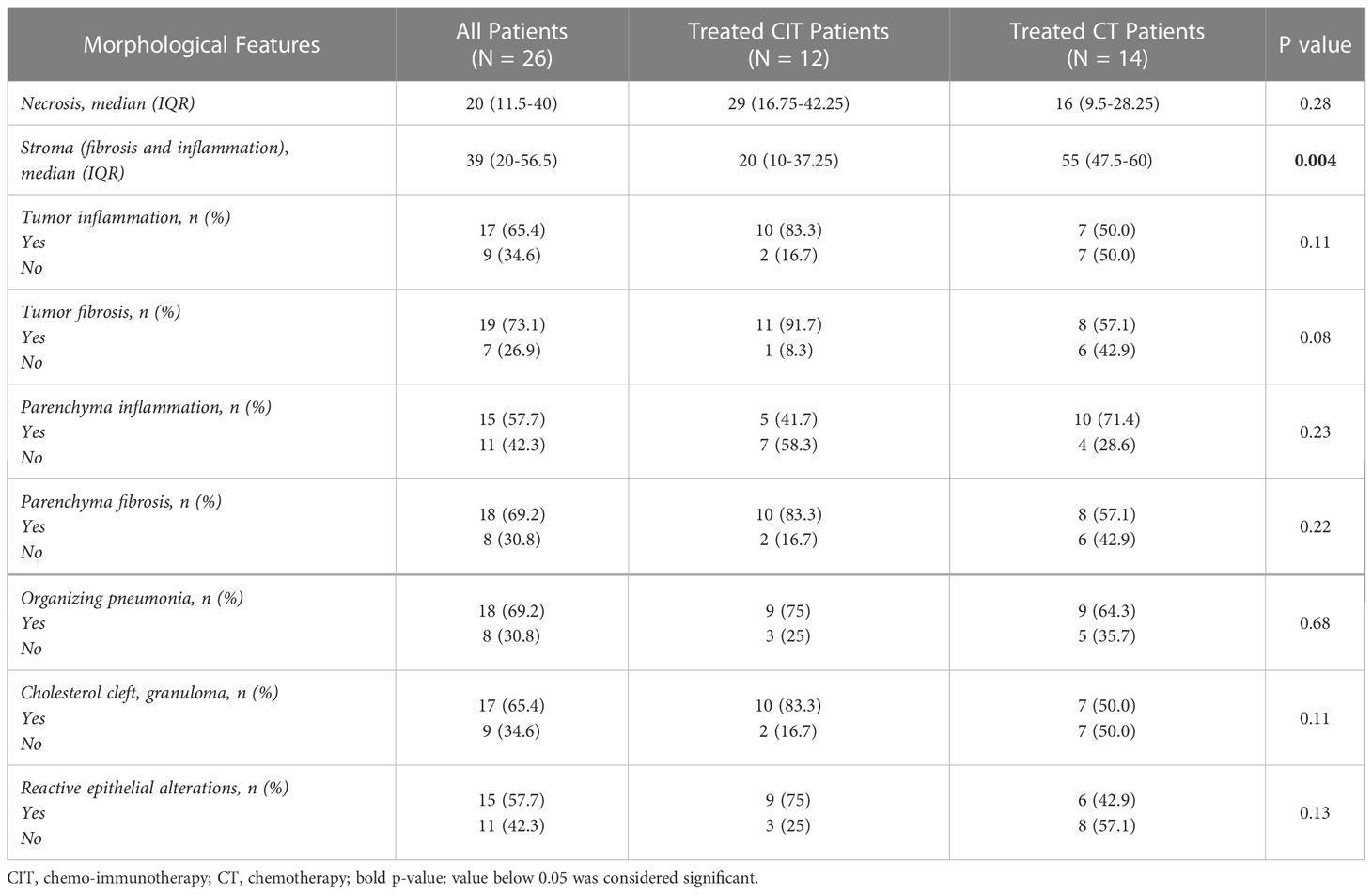
Table 2 Morphological characteristics of tumors after neoadjvant treatment.
Although no significant correlations were found between PD-L1 immunohistochemical expression and MPR, necrosis, and stroma, we observed a trend showing that PD-L1 levels positively correlated with MPR both in the general cohort and in patients treated with combination therapy. On the contrary, the amount of stroma positively correlated with PD-L1 expression levels only in the combined treated patients (Figures 4A–F).
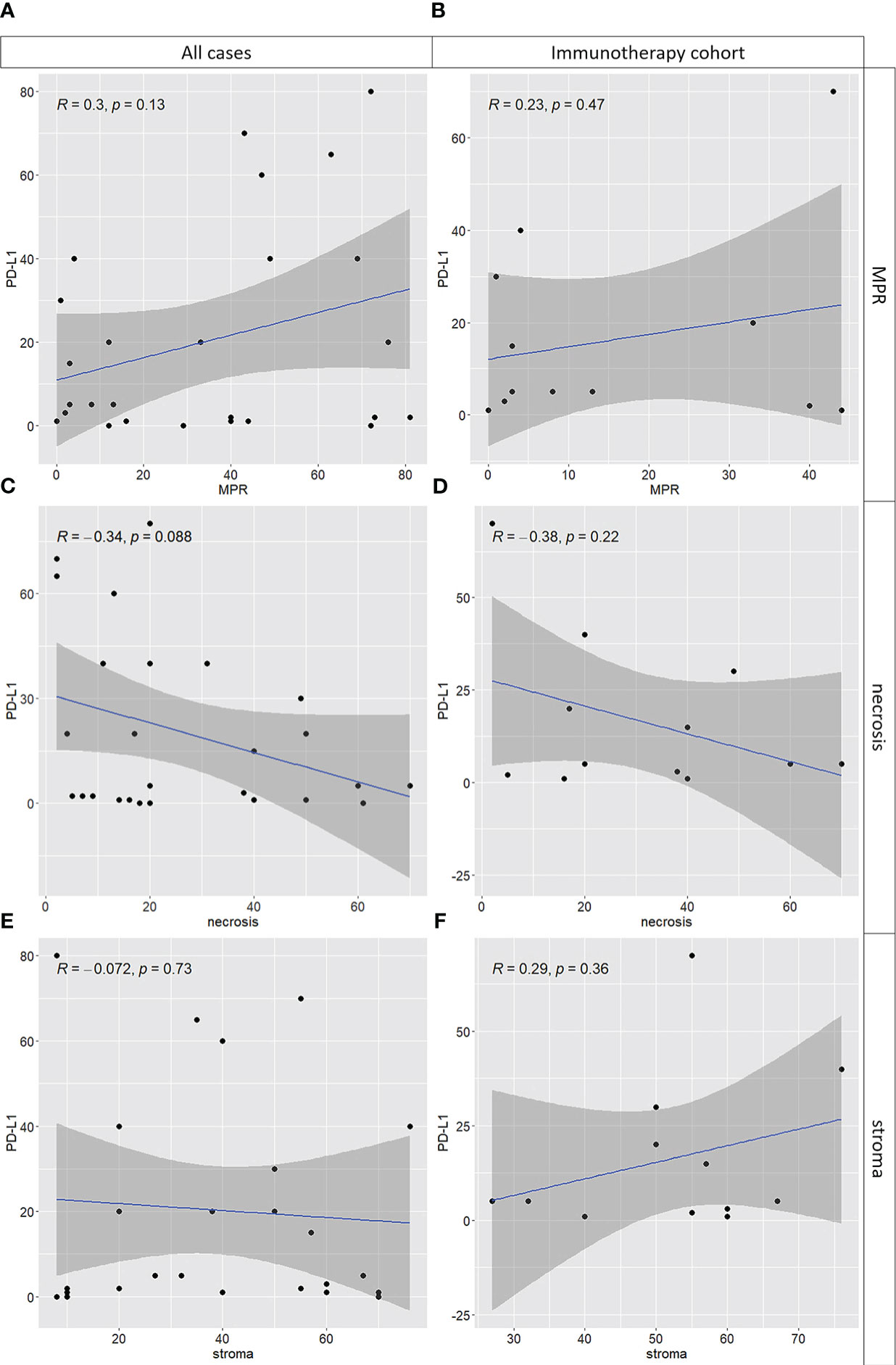
Figure 4 Correlations between PD-L1 tumor proportion score in naïve tumor and tumor components after neoadjuvant treatment including major pathological response (MPR), necrosis and stroma (i.e, inflammatory cells and fibrosis). On the left (i.e., panels A, C, E) the entire cohort of cases was used; on the right (i.e., panels B, D, F) only cases treated with chemo-immunotherapy were used. While for MPR (A, B) and necrosis (C, D) the results are consistent, a mild positive correlation between PD-L1 levels and stroma is observed in the chemo-immunotherapy cohort only (F), not in the entire cohort (E).
The last follow-up was in June 2022. For all patients, the overall median follow-up was 23 months (interquartile range, IQR, 16 – 32 months). In the chemotherapy treated patient cohort, the median follow-up was 16 months (IQR, 16 – 26). In the combined immuno-chemotherapy cohort, the median follow-up was 29 months (IQR, 22 – 35 months).
In univariate analysis and considering the entire cohort of patients, MPR was predictive of long-term OS (p = 0.04) and EFS (p = 0.04) after neoadjuvant therapy. In particular the best cut-off was 33% of viable tumor cells, which significantly stratified patients according to EFS (p = 0.02), and OS (p = 0.01) (Figures 5A–D).
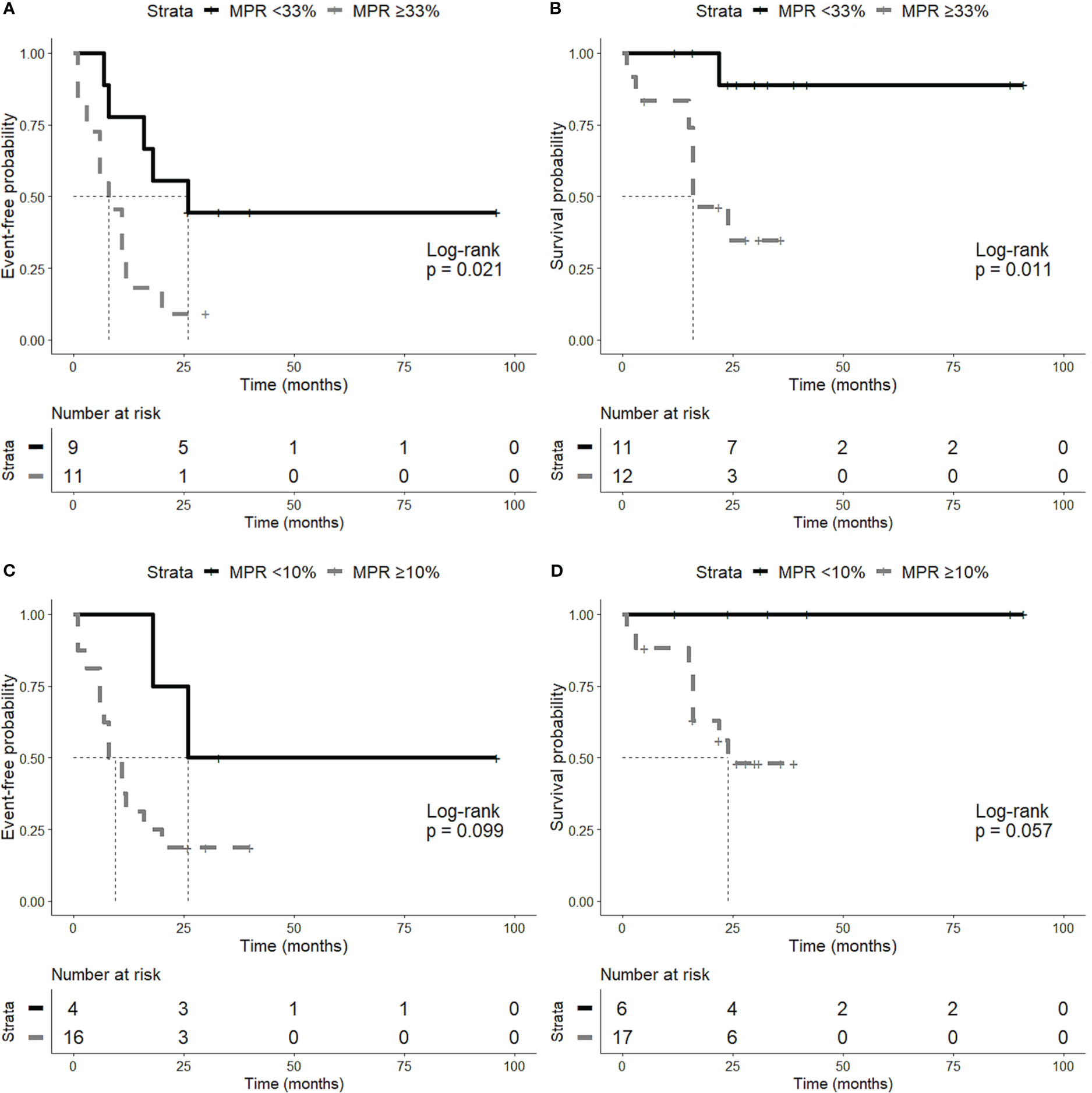
Figure 5 Time-to-event analyses. Patients were stratified according to the best cut-off of major pathological response (MPR) (i.e., 33% of viable tumor cells). Patients with less than 33% of viable tumor cells showed a better event-free survival (EFS) (A) and overall survival (OS) (B). The classic 10% MPR cut-off was also tested and showed the same trend both on EFS (C) and OS (D).
Regarding histopathological features of tumors, the amount of necrosis was associated with a longer EFS (p = 0,02), whereas no association was observed between necrosis and OS.
We observed also a trend for a better overall survival of patients treated with chemo-immunotherapy (p = 0.07) and, as expected, a trend for a better outcome of patients with stage I or II disease both in EFS (p = 0.12) and OS (p = 0.12).
Finally, we performed a multivariate analysis including MPR, stage and treatment. While higher disease stage was predictive of poor EFS (p = 0.02) and OS (p = 0.05), MPR was associated with EFS independently of stage and treatment regimen (p = 0.02) (Table 3).
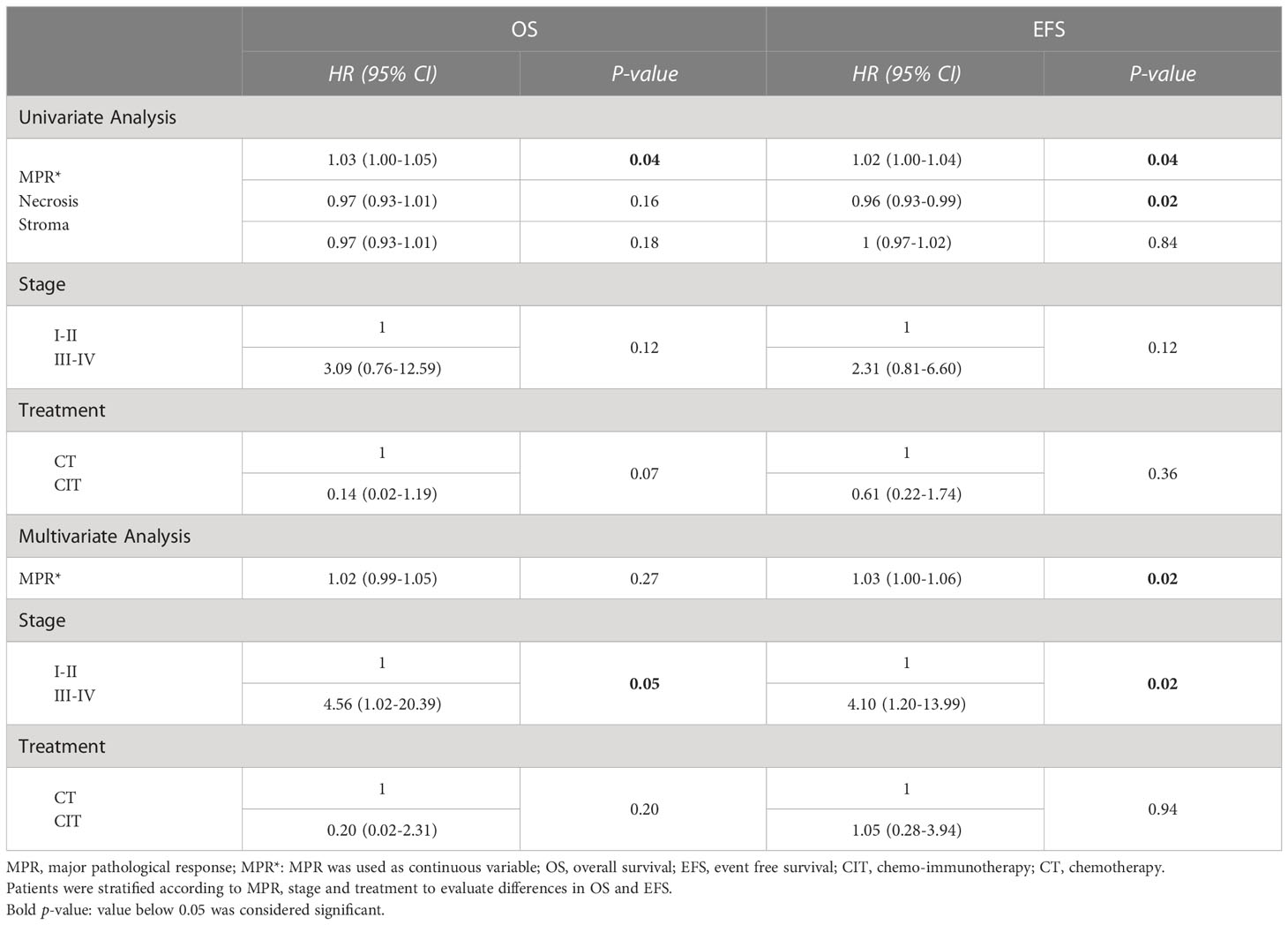
Table 3 Univariate and multivariate time-to-event analyses.
Gene expression analysis was performed in a small set of samples, namely 5 tumors from patients treated with neoadjuvant chemo-immunotherapy. For each case, both pre- and post-surgical tissue samples were analyzed to observe changes of Hippo gene expression. Differences between pre- and post-surgical samples were remarkable at unsupervised analyses. In fact, pre- and post-surgical samples were clearly separated at PCA (Figure 6A) and heatmap (Figure 6B), with only one exception in the latter. Six genes were significantly upregulated in post-surgical samples (Figure 6C), namely ETS1, FAT4, STAT5A, ETS2, CTLA4 and LATS2. In Table 4 are reported genes with an FDR below 0.15.
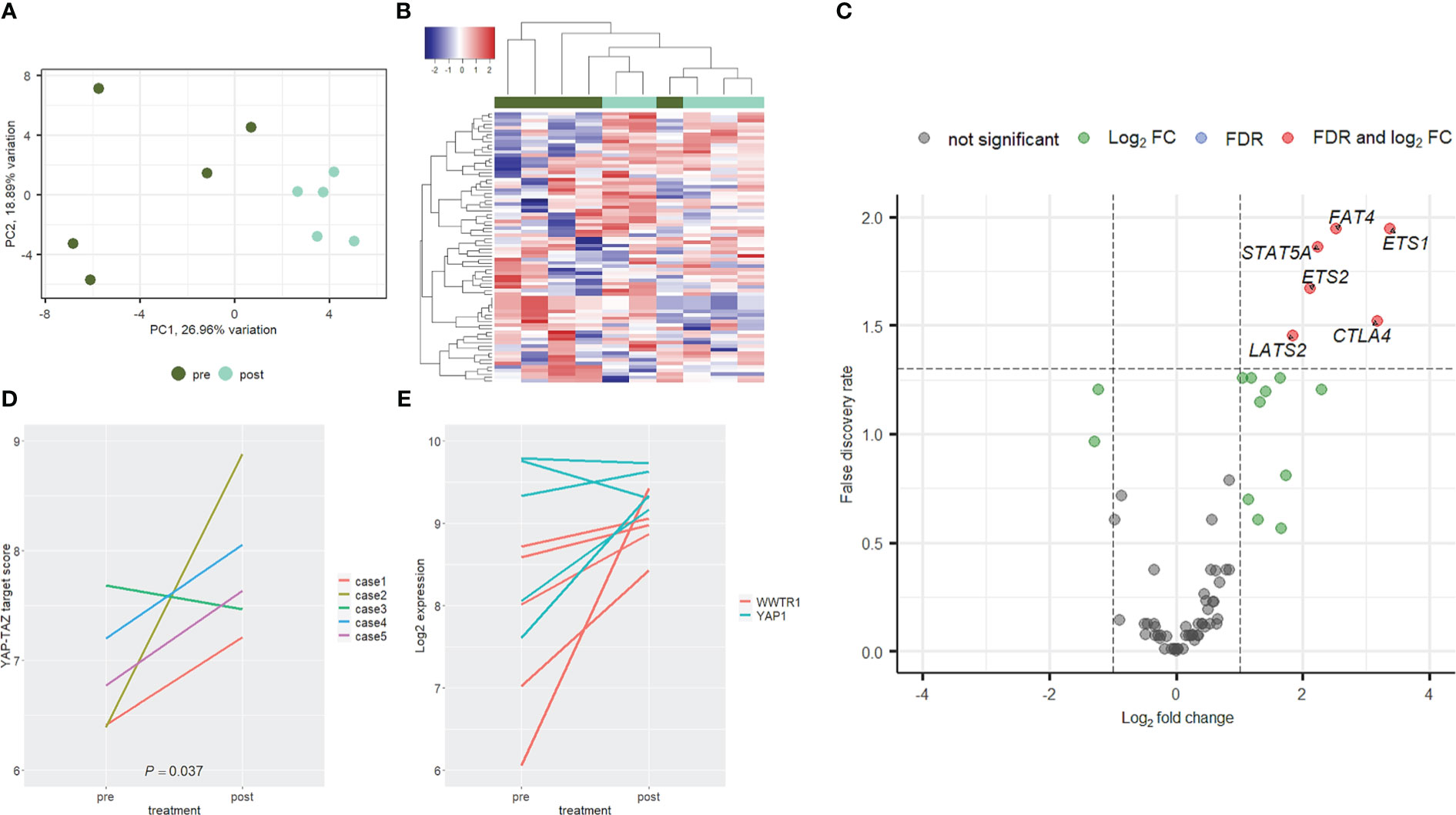
Figure 6 Expression profile of Hippo genes. Paired naïve (green) and post-surgical (cyan) tumors from the chemo-immunotherapy cohort clearly separated at PCA (A) and hierarchical clustering (B) analyses. In post-surgical specimens a trend towards gene upregulation was observed (C), with six genes significantly deregulated (red dots). YAP-TAZ target score was significantly upregulated in post-surgical samples (D). This was consistent with a trend towards upregulation of genes encoding for YAP and TAZ (i.e., YAP1 and WWTR1 respectively, especially the latter) (E).
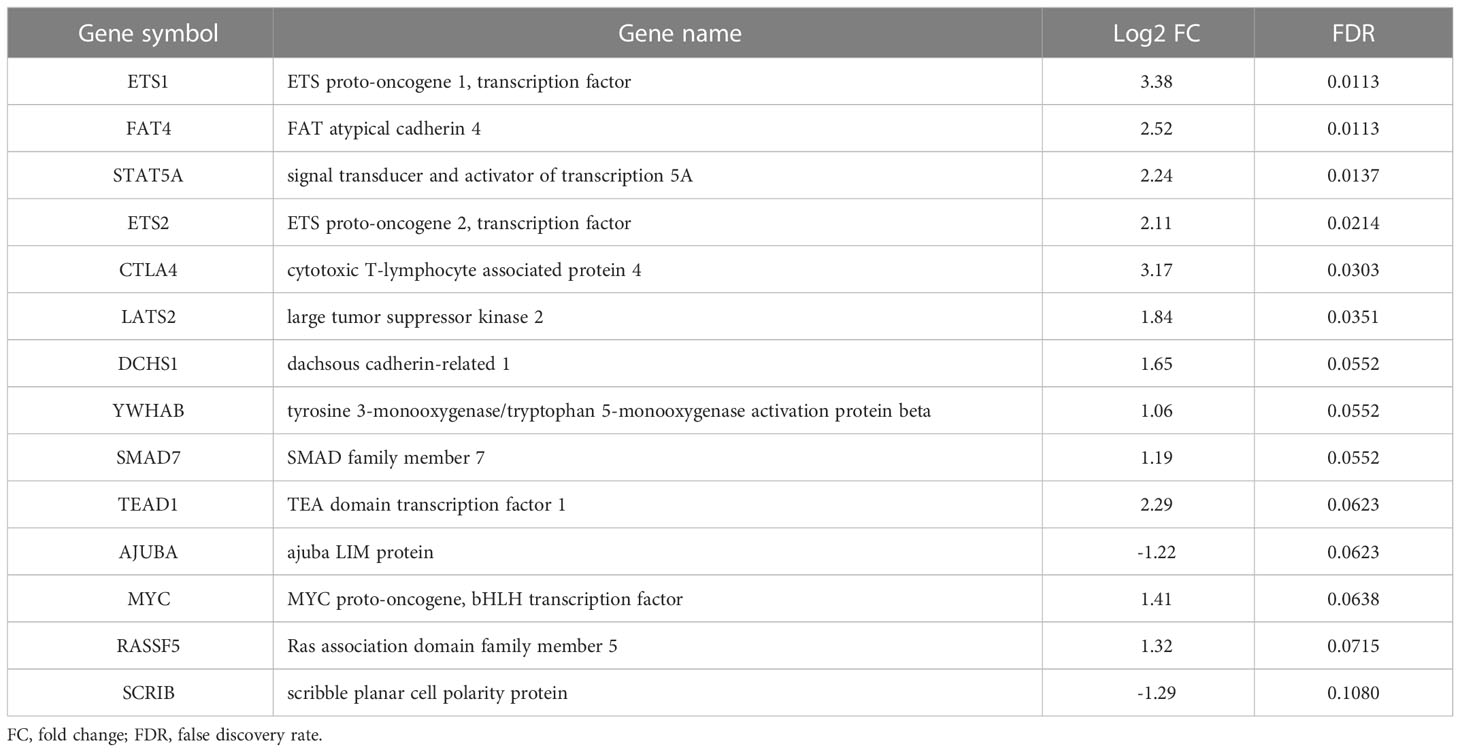
Table 4 Genes deregulated after adjuvant chemo-immunotherapy.
To evaluate the activation of YAP and TAZ (encoded by YAP1 and WWTR1 genes respectively) two approaches were used. First, a YAP-TAZ target score was built by averaging the expression level of 3 validated targets (i.e., AMOTL2, LATS2 and PTPN14, DOI: 10.1016/j.celrep.2018.10.001). Second, the mRNA expression of YAP1 and WWTR1 were evaluated. As presented in Figure 6D, YAP-TAZ target score was always higher in post-surgical samples with one exception. These results were confirmed by the pre- and post-surgical levels of YAP1 and WWTR1. In fact, after neoadjuvant immunotherapy, both genes were upregulated, especially WWTR1 (Figure 6E).
In resectable NSCLC preoperative treatments, including immunotherapy, can improve clinical outcomes and patients survival (6).
To date, there are limited data establishing the prognostic relationship between pathological response after neoadjuvant therapy in resectable NSCLC and clinical outcome, making it an interesting research area. Pathological response has been proposed as a surrogate indicator of benefit to neoadjuvant therapy in order to evaluate the effectiveness of agents tested in clinical trial (18). Numerous studies showed that neoadjuvant chemotherapy treated patients with lung cancer that achieve a MPR ≤10% have a significantly improved survival (10, 12, 19). Therefore, pathological response, including pCR and MPR, can be relevant to assess the impact of neoadjuvant chemo-immunotherapy (10).
Studies evaluating the effect of neoadjuvant immunotherapy in resectable NSCLC have shown a median pathological response of 50-92.5%. In particular, a MPR defined as 10% or less of residual viable tumor cells in the resected primary tumor was reported in 40.5-56.7% of cases, while cPR, defined as no viable tumor within the resected specimen, was reported in 15-33% and 8.1-10% for primary lesions and lymph nodes respectively. These responses are better than those reported for patients treated with neoadjuvant chemotherapy (5, 13, 20–23).
In the present study, we retrospectively analyzed 26 NSCLC patients treated with neoadjuvant therapy of which 14 with chemotherapy alone and 12 with chemo-immunotherapy. In agreement with literature data (5, 13, 20–23), we observed a better pathological response in the chemo-immunotherapy cohort: six patients (50.0%) achieved a MPR and one patient a pCR both on primary tumor and on lymph nodes (8.3%). On the contrary, no patient treated with chemotherapy alone achieved pCR or MPR.
In comparison to our results, Shi L and collaborators reported a higher pathological response in squamous cell lung carcinoma treated with neoadjuvant chemo-immunotherapy (24), with 66.7% of patients achieving MPR and 39.7% cases achieving a pCR. This discrepancy could be due to the different type of specimens included in the study. In fact, they analyzed only squamous histology, whereas we analyzed also adenocarcinoma, large cell neuroendocrine carcinoma, and adenosquamous carcinoma. Previous data showed that squamous cell carcinoma demonstrates a different response to immunotherapy in comparison to non-squamous cell carcinoma, with much more infiltration of immune cells and higher expression of PD-L1 (25–27). Even after neoadjuvant chemotherapy, squamous cell carcinoma shows a greater MPR than adenocarcinoma (28).
Recently, new clinical trials showed an improved EFS in patients treated with neoadjuvant chemo-immunotherapy or immunotherapy alone, as compared to chemotherapy treated patients (5, 6, 29). CheckMate-816 clinical trial compared neoadjuvant nivolumab plus chemotherapy versus neoadjuvant chemotherapy showing longer EFS in patients who achieved pathological response (5). In the present study, we observed a significant association between MPR after neoadjuvant treatment and prognosis. In particular, we observed an association between MPR and both EFS (p = 0.04) and OS (p = 0.04). These findings were also confirmed by multivariate analysis showing that MPR was associated with EFS independently of stage and treatment regimen (p = 0.02). We observed also a trend for a better overall survival of patients treated with chemo-immunotherapy (p = 0.07) and, as expected, a trend for a better outcome of patients with stage I and II disease both in EFS (p = 0.12) and OS (p = 0.12). However, these results did not reach statistical significance probably due to the small number of cases.
Although promising, our results show that a considerable percentage of neoadjuvant chemo-immunotherapy treated patients (40%–75%) still do not achieve MPR or pCR, presenting a higher risk of relapse (5, 23, 30). Thus, the identification of predictive biomarkers of pathological response in resectable NSCLC is needed.
Cottrell and collaborators suggested that immunotherapy responsive tumors showed specific histological changes reflecting a state of immune activation (31). This finding could explain lack of correlation between pathological and radiological responses reported after neoadjuvant immunotherapy, related to the increased size of tumor on imaging caused by the infiltration of T-cells and macrophages, neovascularization and fibrosis (32).
In our study, we evaluated other histological features of tumor bed including necrosis and stroma. Regarding the amount of necrosis, we didn’t observe any significant difference between the two treatment cohorts, whereas we observed a significantly higher amount of stroma in the neoplastic bed in the immuno-chemotherapy treated patients. This observation agrees with previous studies showing a greater amount of fibrosis in patients treated with chemo plus immunotherapy compared to patients treated with chemotherapy alone (18).
Regarding the identification of predictive factors for neoadjuvant treatments, we evaluated immunohistochemical PD-L1 expression since it is a critical marker to guide patient selection for immunotherapy in advanced NSCLC. However, we did not find associations between PD-L1 expression and pathological response or other histological features. We observed only a trend showing that PD-L1 levels positively correlated with MPR both in the general cohort and with MPR and stroma in patients treated with combination therapy. Although some studies reported a greater benefit from the combined chemo-immunotherapy in patients with a high PD-L1 immunohistochemical expression (33, 34), others suggested a lack of correlation between PD-L1 expression of pre-treatment specimens and patients’ response (24, 30). Therefore, PD-L1 expression should not be considered a good predictive marker for neoadjuvant chemo-immunotherapy. Probably an optimal approach should not be based on the analysis of a single marker, but it should be more comprehensive evaluating not only the tumor but also its microenvironment.
In this study, after neoadjuvant chemo-immunotherapy, residuals tumors showed the upregulation of YAP1 and WWTR1, which encode for YAP and TAZ respectively. Consistently, YAP/TAZ target expression was enhanced. These findings are consistent with high levels of fibrosis in these tumors since the activation of YAP/TAZ is crucial in regulating tissue repair (doi: 10.1038/s41573-020-0070-z). However, this activation could suggest also the selection of cells resistant to treatment (doi: 10.1016/j.cell.2014.06.004), and could open new perspectives in further lines of treatment. Similarly, the enhanced expression of CTLA4 after treatment with PD-1 or PD-L1 agonists, could be a resistance mechanism that should be considered after progression to PD-1/PD-L1 blockade.
Several limitations associated with the present study should be mentioned. First, the small sample size made it difficult to obtain robust statistical results and a further validation is warranted. Second, this was a retrospective, non-randomized single-center study needing to be confirmed in prospective cohorts. Moreover, our study lacks long-term follow up that will be necessary to evaluate the efficacy of neoadjuvant chemo-immunotherapy on recurrence and survival in resectable NSCLC.
In conclusion, despite these limitations, our study demonstrated that the combination of immunotherapy and chemotherapy in neoadjuvant setting significantly improves pathological response in comparison to chemotherapy alone. At the same time, we suggested that chemo-immunotherapy could induce different morphological and molecular changes of treated specimens, both of the tumor and of the collateral lung parenchyma, in comparison to chemotherapy alone. These differences can impact on specimens processing and scoring in the evaluation of pathological response, and can increase our knowledge of biological and histological features of responders and non-responders to different neoadjuvant therapies.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by “Comitato Etico di Area Vasta Nord Ovest” (CEAVNO) for Clinical Experimentation (Protocol Number: ID19211). The patients/participants provided their written informed consent to participate in this study.
GA, EB, FM, and GF contributed to conception and design of the study. AL, AC, and GM organized the database. AP performed the statistical analysis. GA and IS wrote the first draft of the manuscript. GA, GR, and CZ wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1115156/full#supplementary-material
1. Arriagada R, Bergman B, Dunant A, Le Chevalier T, Pignon JP, Vansteenkiste J. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med (2004) 350:351–60. doi: 10.1056/NEJMoa031644
2. Burdett S, Pignon JP, Tierney J, Tribodet H, Stewart L, Le Pechoux C, et al. Adjuvant chemotherapy for resected early-stage non-small cell lung cancer. Cochrane Database Syst Rev (2015) 3:CD011430. doi: 10.1002/14651858.CD011430
3. Martin J, Ginsberg RJ, Venkatraman ES, Bains MS, Downey RJ, Korst RJ, et al. Long-term results of combined-modality therapy in resectable non– small-cell lung cancer. J Clin Oncol (2002) 20:1989–95. doi: 10.1200/JCO.2002.08.092
4. Arriagada R, Dunant A, Pignon JP, Bergman B, Chabowski M, Grunenwald D, et al. Long-term results of the international adjuvant lung cancer trial evaluating adjuvant cisplatin-based chemotherapy in resected lung cancer. J Clin Oncol (2010) 28:35–42. doi: 10.1200/JCO.2009.23.2272
5. Forde PM, Spicer J, Lu S, Provencio M, Mitsudomi T, Awad MM, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med (2022) 386:1973–85. doi: 10.1056/NEJMoa2202170
6. Cascone T, William WN, Weissferdt A, Leung CH, Lin HY, Pataer A, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: the phase 2 randomized NEOSTAR trial. Nat Med (2021) 27:504–14. doi: 10.1038/s41591-020-01224-28
7. Bott MJ, Yang SC, Park BJ, Adusumilli PS, Rusch VW, Isbell JM, et al. Initial results of pulmonary resection after neoadjuvant nivolumab in patients with resectable non-small cell lung cancer. J Thorac Cardiovasc Surg (2019) 158:269–76. doi: 10.1016/j.jtcvs.2018.11.124
8. Rojas F, Parra ER, Wistuba II, Haymaker C, Solis Soto LM. Pathological response and immune biomarker assessment in non-Small-Cell lung carcinoma receiving neoadjuvant immune checkpoint inhibitors. Cancers (Basel) (2022) 14:2775. doi: 10.3390/cancers14112775
9. Travis WD, Dacic S, Wistuba I, Sholl L, Adusumilli P, Bubendorf L, et al. IASLC multidisciplinary recommendations for pathologic assessment of lung cancer resection specimens after neoadjuvant therapy. J Thorac Oncol (2020) 15:709–40. doi: 10.1016/j.jtho.2020.01.005
10. Pataer A, Kalhor N, Correa AM, Raso MG, Erasmus JJ, Kim ES, et al. Histopathologic response criteria predict survival of patients with resected lung cancer after neoadjuvant chemotherapy. J Thorac Oncol (2012) 7:825–32. doi: 10.1097/JTO.0b013e318247504a
11. Chaft JE, Rusch V, Ginsberg MS, Paik PK, Finley DJ, Kris MG, et al. Phase II trial of neoadjuvant bevacizumab plus chemotherapy and adjuvant bevacizumab in patients with resectable nonsquamous non-small-cell lung cancers. J Thorac Oncol (2013) 8:1084–90. doi: 10.1097/JTO.0b013e31829923ec
12. Junker K, Thomas M, Schulmann K, Klinke F, Bosse U, Müller KM. Tumour regression in non-small-cell lung cancer following neoadjuvant therapy. histological assessment. J Cancer Res Clin Oncol (1997) 123:469–477. doi: 10.1007/BF01192200
13. Shu CA, Gainor JF, Awad MM, Chiuzan C, Grigg CM, Pabani A, et al. Neoadjuvant atezolizumab and chemotherapy in patients with resectable non-small-cell lung cancer: An openlabel, multicentre, single-arm, phase 2 trial. Lancet Oncol (2020) 21:786–95. doi: 10.1016/S1470-2045(20)30140-6
14. Rothschild SI, Zippelius A, Eboulet EI, Savic Prince S, Betticher D, Bettini A, et al. Durvalumab in addition to neoadjuvant chemotherapy in patients with stage IIIA(N2) non-small-cell lung cancer-a multicenter single-arm phase II trial. J Clin Oncol (2021) 39:2872–80. doi: 10.1200/JCO.21.00276
15. Chen X, MA K. Neoadjuvant therapy in lung cancer: What is most important: Objective response rate or major pathological response? Curr Oncol (2021) 28:4129–38. doi: 10.3390/curroncol28050350
16. Mouillet G, Monnet E, Milleron B, Puyraveau M, Quoix E, David P, et al. Pathologic complete response to preoperative chemotherapy predicts cure in early-stage non-small-cell lung cancer: combined analysis of two IFCT randomized trials. J Thorac Oncol (2012) 7:841–9. doi: 10.1097/JTO.0b013e31824c7d92
17. Rusch VW, Chansky K, Kindler HL, Nowak AK, Pass HI, Rice DC, et al. Staging and prognostic factors committee, advisory boards, and participating institutions. prognostic factors committee, the IASLC mesothelioma staging project: Proposals for the m descriptors and for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for mesothelioma. J Thorac Oncol (2016) 11:2112–9. doi: 10.1016/j.jtho.2016.09.124
18. Weissferdt A, Pataer A, Vaporciyan AA, Correa AM, Sepesi B, Moran CA, et al. Agreement on major pathological response in NSCLC patients receiving neoadjuvant chemotherapy. Clin Lung Cancer (2020) 21:341–8. doi: 10.1016/j.cllc.2019.11.003
19. Hellmann MD, Chaft JE, William WN Jr., Rusch V, Pisters KM, Kalhor N, et al. Pathological response after neoadjuvant chemotherapy in resectable non-small-cell lung cancers: Proposal for the use of major pathological response as a surrogate endpoint. Lancet Oncol (2014) 15:e42–50. doi: 10.1016/S1470-2045(13)70334-6
20. Cao C, Guo A, Chen C, Chakos A, Bott M, Yang CJ, et al. Systematic review of neoadjuvant immunotherapy for patients with non-small cell lung cancer. Semin Thorac Cardiovasc Surg (2021) 33:850–7. doi: 10.1053/j.semtcvs.2020.12.012
21. Gao S, Li N, Gao S, Xue Q, Ying J, Wang S, et al. Neoadjuvant PD-1 inhibitor (Sintilimab) in NSCLC. J Thorac Oncol (2020) 15:816–26. doi: 10.1016/j.jtho.2020.01.017
22. Pignon JP, Tribodet H, Scagliotti GV, Douillard JY, Shepherd FA, Stephens RJ, et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE collaborative group. J Clin Oncol (2008) 26:3552–9. doi: 10.1200/JCO.2007.13.9030
23. Provencio M, Nadal E, Insa A, García-Campelo MR, Casal-Rubio J, Dómine M, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol (2020) 21:1413–22. doi: 10.1016/S1470-2045(20)30453-8
24. Shi L, Meng Q, Tong L, Li H, Dong Y, Su C, et al. Pathologic response and safety to neoadjuvant PD-1 inhibitors and chemotherapy in resectable squamous non-small-cell lung cancer. Front Oncol (2022) 12:956755. doi: 10.3389/fonc.2022.956755
25. Chen Q, Fu YY, Yue QN, Wu Q, Tang Y, Wang WY, et al. Distribution of PD-L1 expression and its relationship with clinicopathological variables: An audit from 1071 cases of surgically resected non-small cell lung cancer. Int J Clin Exp Pathol (2019) 12:774–86.
26. Shen D, Wang J, Wu J, Chen S, Li J, Liu J, et al. Neoadjuvant pembrolizumab with chemotherapy for the treatment of stage IIB-IIIB resectable lung squamous cell carcinoma. J Thorac Dis (2021) 13:1760–8. doi: 10.21037/jtd-21-103
27. Ling Y, Li N, Li L, Guo C, Wei J, Yuan P, et al. Different pathologic responses to neoadjuvant anti-PD-1 in primary squamous lung cancer and regional lymph nodes. NPJ Precis Oncol (2020) 4:32. doi: 10.1038/s41698-020-00135-2
28. Qu Y, Emoto K, Eguchi T, Aly RG, Zheng H, Chaft JE, et al. Pathologic assessment after neoadjuvant chemotherapy for NSCLC: Importance and implications of distinguishing adenocarcinoma from squamous cell carcinoma. J Thorac Oncol (2019) 14:482–93. doi: 10.1016/j.jtho.2018.11.017
29. Lee JM, Kim AW, Marjanski T, Falcoz PE, Tsuboi M, Wu YL, et al. Important surgical and clinical end points in neoadjuvant immunotherapy trials in resectable NSCLC. JTO Clin Res Rep (2021) 2:100221. doi: 10.1016/j.jtocrr.2021.100221
30. Provencio M, Serna-Blasco R, Nadal E, Insa A, García-Campelo MR, Casal Rubio J, et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non-Small-Cell lung cancer (NADIM phase II trial). J Clin Oncol (2022) 40:2924–33. doi: 10.1200/JCO.21.02660
31. Cottrell TR, Thompson ED, Forde PM, Stein JE, Duffield AS, Anagnostou V, et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for quantitative immune-related pathologic response criteria (irPRC). Ann Oncol (2018) 29:1853–60. doi: 10.1093/annonc/mdy218
32. Nishino M, Hatabu H, Hodi FS. Imaging of cancer immunotherapy: Current approaches and future directions. Radiology (2019) 290:9–22. doi: 10.1148/radiol.2018181349
33. Wang J, Yu X, Barnes G, Leaw S, Bao Y, Tang B. The effects of tislelizumab plus chemotherapy as first-line treatment on health-related quality of life of patients with advanced squamous non-small cell lung cancer: Results from a phase 3 randomized clinical trial. Cancer Treat Res Commun (2021) 30:100501. doi: 10.1016/j.ctarc.2021.100501
34. Zhou C, Wang Z, Sun Y, Cao L, Ma Z, Wu R, et al. Sugemalimab versus placebo, in combination with platinum-based chemotherapy, as first-line treatment of metastatic non-small-cell lung cancer (GEMSTONE-302): Interim and final analyses of a double-blind, randomised, phase 3 clinical trial. Lancet Oncol (2022) 23:220–33. doi: 10.1016/S1470-2045(21)00650-1
Keywords: non-small cell lung cancer, neoadjuvant therapy, chemo-immunotherapy, pathological response, prognosis, biomarkers
Citation: Alì G, Poma AM, Di Stefano I, Zirafa CC, Lenzini A, Martinelli G, Romano G, Chella A, Baldini E, Melfi F and Fontanini G (2023) Different pathological response and histological features following neoadjuvant chemotherapy or chemo-immunotherapy in resected non-small cell lung cancer. Front. Oncol. 13:1115156. doi: 10.3389/fonc.2023.1115156
Received: 03 December 2022; Accepted: 31 January 2023;
Published: 09 February 2023.
Edited by:
Mohamed Rahouma, NewYork-Presbyterian, United StatesReviewed by:
Lorenzo Belluomini, University of Verona, ItalyCopyright © 2023 Alì, Poma, Di Stefano, Zirafa, Lenzini, Martinelli, Romano, Chella, Baldini, Melfi and Fontanini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriella Fontanini, Z2FicmllbGxhLmZvbnRhbmluaUB1bmlwaS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.