
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol., 07 March 2023
Sec. Cancer Epidemiology and Prevention
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1091329
This article is part of the Research TopicUniversal Health Coverage and Global Health in OncologyView all 13 articles
 Nam Phong Nguyen1*
Nam Phong Nguyen1* Ulf Lennart Karlsson2
Ulf Lennart Karlsson2 David Lehrman1
David Lehrman1 Thandeka Mazibuko1Tatul Saghatelyan3
Thandeka Mazibuko1Tatul Saghatelyan3 Juliette Thariat4Brigitta G. Baumert5
Juliette Thariat4Brigitta G. Baumert5 Vincent Vinh-Hung6Olena Gorobets7
Vincent Vinh-Hung6Olena Gorobets7 Huan Giap8Sankalp Singh9
Huan Giap8Sankalp Singh9 Alexander Chi10Graciana Alessandrini11Abhinav Ahluwalia12Francis Durosinmi-Etti13
Alexander Chi10Graciana Alessandrini11Abhinav Ahluwalia12Francis Durosinmi-Etti13 Jorge Zegarra Cárdenas14Koniba Diabate15Joan Oboite1Eromosele Oboite1Tahir Mehmood16Te Vuong17
Jorge Zegarra Cárdenas14Koniba Diabate15Joan Oboite1Eromosele Oboite1Tahir Mehmood16Te Vuong17 Lyndon Kim18Brandi R. Page19
Lyndon Kim18Brandi R. Page19Older cancer patients are disproportionally affected by the Coronavirus 19 (COVID-19) pandemic. A higher rate of death among the elderly and the potential for long-term disability have led to fear of contracting the virus in these patients. This fear can, paradoxically, cause delay in diagnosis and treatment that may lead to a poor outcome that could have been prevented. Thus, physicians should devise a policy that both supports the needs of older patients during cancer treatment, and serves to help them overcome their fear so they seek out to cancer diagnosis and treatment early. A combination of telemedicine and a holistic approach, involving prayers for older cancer patients with a high level of spirituality, may improve vaccination rates as well as quality of life during treatment. Collaboration between health care workers, social workers, faith-based leaders, and cancer survivors may be crucial to achieve this goal. Social media may be an important component, providing a means of sending the positive message to older cancer patients that chronological age is not an impediment to treatment.
Coronavirus Disease 19 (COVID 19) is a pandemic of unprecedented and epic proportion which affects older patients disproportionally. A high rate of hospitalization and death has been reported among adults over 65 years of age (1). Among older patients who survived the infection, long-term complications such as dementia has been reported (2). Delirium during the viral infection may lead to later brain damage in this vulnerable population (3). Other studies also corroborated a higher rate of respiratory failure, fatigue, and dementia in older patients due likely to pre-existing comorbidities (4). Older cancer patients in particular, face compounded risk. They are likely to suffer a higher risk of severe illness, intensive care unit admission, mechanical ventilation, and death compared to non-cancer patients (5). Up to 28% of cancer patients admitted for COVID-19 infection died during hospital stay due to advanced age and multiple comorbidities such as high blood pressure and cardiovascular disease (6). Patients with hematologic malignancies are at a higher risk of death compared with patients with other solid tumors (7, 8). Other studies have corroborated the high mortality rate associated with old age, cancer, and COVID-19 infection (9). Thus, it is not surprising that patient fear of exposure to the virus has led to delayed diagnosis of cancer due to cancellation of diagnostic imaging procedures such as mammography or colonoscopy (10). Even though fear of virus infection was felt across the general population during the pandemic, its impact was greatest among older patients leading to anxiety and depression (11–13). Cancer patients undergoing active treatment also experienced a high level of emotional distress about the risk of infection (14). As a result, delay or avoidance of medical care increases significantly during the pandemic in the US and across the world (15). This behavior may have led to increased mortality among older cancer patients and minorities who already experience significant challenges in obtaining quality care in a reasonable time frame (16). As an international organization devoted to the care of older cancer patients, women, and minorities, the International Geriatric Radiotherapy Group (http://www.igrg.org) would like to propose a practical health care policy to support these vulnerable patients during the pandemic.
Older patients, who at higher risk for death if infected with SARS-CoV-2, expressed fear during the COVID-19 pandemic across the globe. Using different testing scales such as the five-point fear of COVID-19 scale (FCV-19S), 44% of adults age 65 or older (n=500) admitted to fear of being exposed to the virus (12). This group of patients had preexisting comorbidities and were taking one to three medications at the survey time. Even though 98% of participants were fit, 35% suffered from loneliness, and depression. Those with a history of coronary artery disease, congestive heart failure, and chronic obstructive pulmonary disease expressed the worst fear of the virus which was compounded by social media news. In another study of 843 adults of at least 60 years of age, 28% expressed the fear of losing their lives to the virus. Their anxiety level was proportional to their age. Those who were 80 years-old or older expressed the worst fear (13). Fear of the virus is universal among older adults across the world, affecting all ethnicities (12, 17–21). The media plays a significant role in exacerbating older adults’ fear (20). There was a significant correlation between fear, insomnia, and depression likely due to catastrophizing, a negative thinking style characterized by the expectation of the worst possible outcome within a situation (20–22). As a result, in one study, 81% of the participants expressed moderate to severe depression leading to a high rate of insomnia (19). Among different ethnic groups in the United States, older African Americans developed the highest fear level likely related to the odds of death if infected (23–25). Concerns about contracting the disease and fear of racial bias in testing and treatment likely compound the anxiety (26). Thus, any public policy should take into consideration the ethnic diversity and the role of socio-economic inequalities in coping with the pandemic, and provide measures that address their concerns.
Older cancer patients in particular, face dual risk. Decreased immunity, advanced age, and comorbidities significantly increase the risks of death after contracting the virus (7, 27–29). Patients with hematologic malignancies are at higher risk of death compared with those with other types of cancer (7, 29). Thus, specific recommendations are needed for this type of malignancy. Regardless of the type of cancer, patients are concerned that coronavirus infection is a more life-threatening condition than cancer. As a result, cancer patients express fear and anxiety about the risk of virus exposure and the consequences of systemic treatment on their already altered immune system (30–33). In a survey, 66% of cancer patients were alarmed by the wide community spread of COVID-19, and this was the top cause of their anxiety (30). The fear of death is compounded by the anxiety of dying alone if infected for both patients and their loved ones (31–33). In light of these fears, it is understandable that older cancer patients expressed the highest level of anxiety and depression among those surveyed (34).
The fear of coronavirus infection has led to a significant decrease in cancer diagnosis. In a study of 82 patients with suspected breast cancer diagnosed on mammography, the rates of patients declining biopsy was 9.3% and 35.9% before and after the pandemic, respectively (35). The reason offered for refusal of the procedure was the fear of getting infected during the pandemic. In another study, the number of radiographic exams was significantly reduced during the pandemic compared with previous years, in an area affected by the pandemic. The number of radiographic exams performed was 211 in 2020 and ranged from 360 to 390 in the previous years (36). The combination of delayed biopsy procedures and radiographic exams has led to a precipitous decline in cancer diagnosis. For example, pathological diagnosis during the first six months of 2020 was reduced by 22.7% compared with the same time frame during the previous three years (37). Decreases were seen in the absolute number of pathologic specimen from all cancer sites but the lung, prostate, and gynecologic malignancies showed the steepest decline. Those three types of cancer are diagnosed with clinical exams, blood tests like PSA level, PAP smears, and radiographic exams which suggests a decline in outpatient clinic visits and/or hospital visits. Indeed, there was a significant reduction in the number of hospital visits and diagnostic procedures performed, including biopsy, colonoscopy, and mammography (38). The cancer-related hospitalization rate was reduced by 21%, and admissions were significantly reduced for all age groups. The reduction of procedures performed was 29%, 57%, and 55% for biopsies, colonoscopies, and mammograms, respectively. Other studies also corroborated a significant delay or decline in cancer diagnosis during the pandemic that was linked to a reduction in outpatient dental visits for oral cancer, and outpatient medical visits, for breast, prostate, and non-metastatic cancers, as well as various other types of cancer (39–45). Even though the decrease in cancer diagnosis was observed across all ages, individuals aged 64 or above were the most affected (42). Comparing the age groups 64 and older and younger than 64, reduction in cancer diagnosis was 35.2% and 25.2%, respectively. Another study also corroborated the significant decline in cancer diagnosis in older persons. In a multi-center cohort of 30 hospitals with specialization in the treatment of gastrointestinal cancers, the rate of cancer diagnosis in patients aged 65 or older was reduced to 42.4% and 17% during the lockdown and post lockdown period, respectively (43). This reduction in diagnosis of non-metastatic cancer in older patients is particularly worrisome because the prevalence of cancer increases with age. Early cancer diagnosis is critical to improving the survival of those vulnerable individuals with multiple comorbidities.
Zooming out to a global perspective, in Asia, delayed cancer diagnosis is often compounded by health inequalities between different socio-economic strata. In lower socio-economic strata, families are often overcrowded, with many generations living together. Older patients are at high risk of viral infection as younger family members are exposed to the virus while working full time during the pandemic (a necessity when under economic pressure). In addition, reallocation of health care workers and resources toward COVID-19 duties has further overwhelmed the already fragile health system (46). Thus, with the onset of the pandemic, cancer screening procedures were either completely stopped or reduced to less than 25%. The number of cancer diagnosis was reduced to 54% (47). Table 1 summarizes cancer diagnosis delay during the pandemic.
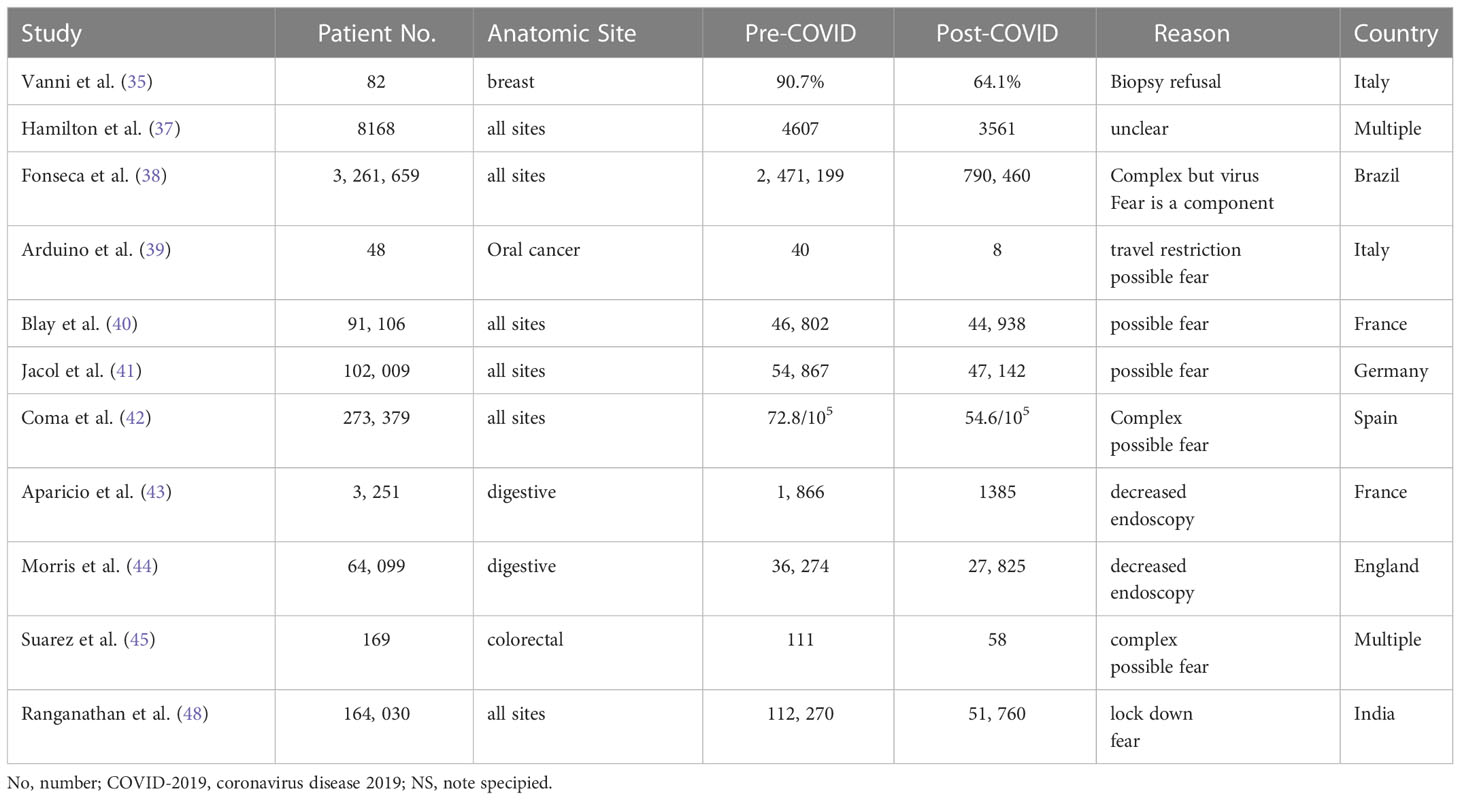
Table 1 Decrease in cancer diagnosis during COVID-19 pandemic.
In a root cause analysis of the decreased emergency room visits during the pandemic, fear of the virus was the principal cause of the patients not going to the hospital even though they had life threatening medical conditions such as myocardial infarction or stroke. The hospital was seen as a reservoir for the virus with infection spreading through coughing and aerosol-generating procedures (49). In addition, there were concerns that the hospital did not take adequate measures to protect the patients from infection. Thus, it is reasonable to postulate that older patients who may have cancer would not seek medical attention due to the fear of death from SARS-CoV-2 infection. Therefore, any proposed solution to support older cancer patients should include measures to allay their fear.
As a result of COVID-19 fear and/or decreased hospital admissions, the number of surgical procedures for cancer was decreased during the pandemic (38, 44). A survey of surgical oncologists across 69 European institutions revealed an average reduction of 29.3% for all types of oncologic surgery due to a reduction of outpatient clinic visits and a reduction of hospital beds or operating room availability (47). Of the physicians surveyed, 89.9% reported that fear of COVID-19 was the reason for the patients’ clinic appointment cancellations. Another study (50) reported that one of the main reasons for the reduced oncologic surgical procedures was the decrease on the number of endoscopic procedures performed in older cancer patients. Compared with the previous year, only 51% of older patients underwent diagnostic endoscopies. In addition, most of older individuals underwent palliative surgery rather than curative resection which may reflect their frailty status and/or it could reflect prioritizing younger patients for treatment (50). Other studies also corroborate the reduction in cancer surgery during the COVID-19 pandemic, and the pandemic was also associated with a significant delay in surgical treatment leading to a more advanced stage at diagnosis compared with pre-pandemic years (51–53). As a result, emergency surgery and non-curative resection were performed more frequently during the pandemic (54). For various reasons ranging from COVID-19 fear to delayed elective surgery, cancer surgery for all anatomic sites was significantly reduced (47, 50–56). It is postulated that the reduction in cancer surgery was related to decreased emergency room visits due to the widespread fear of the virus. However, the issue is more complex as patients may delay treatment, and this can lead to more severe symptoms and prolonged hospitalizations due to the severity of the disease (57, 58). As an ominous sign, the decrease and/or delay of surgery for cancer patients was also associated with a delay to adjuvant treatment such as chemotherapy which may further increase mortality rate (51).
The efficacy of systemic chemotherapy depends on adherence to the treatment. Any chemotherapy postponement may lead to disease recurrence. In a study of 3661 patients who received chemotherapy on an outpatient basis, the rates of chemotherapy postponement were 11.2% and 14.2% before and after the pandemic, respectively. In patients who had chemotherapy postponement, 17.4% stated that the reason was fear of COVID-19’s in light of their depressed immune system. Advanced age was the most common predictor of chemotherapy postponement (59). Importantly, among those who expressed fear and anxiety due to the virus, the introduction of telemedicine with patient education decreased the postponement rate to 4.6%, suggesting that this modality could be key to alleviating patients’ anxiety and improving treatment compliance. Other studies also reported a delay or modification of chemotherapy schedule, of up to 43.6% during the pandemic (60–66). In a study of 1472 cancer patients who received treatment at a tertiary cancer center, chemotherapy was delayed or discontinued in 51.6% and 12.6% of the patients, respectively (62). Of the patients who were showing a response to therapy before the pandemic, 10.3% had disease progression, and 73% of these patients died. Older age (60+), and disease progression were risk factors for death. More patients died from cancer progression than from COVID-19 infection. Another study also highlights the impact of oncology treatment interruption on survival. Among 112 head and neck cancer patients undergoing chemotherapy either alone or combined with radiotherapy, 71 discontinued treatment during the pandemic, and 31% of these showed disease progression or death (63). Even though many factors may have influenced treatment discontinuation, in one study of patients receiving adjuvant chemotherapy for early breast cancer, old age was a significant factor influencing the decision to discontinue treatment due to the fear of getting infected with SARS-CoV-2 while undergoing chemotherapy (66). Thus, all future policy should focus on avoiding treatment interruption, while also protecting patients from COVID-19 during treatment.
Radiotherapy treatment traditionally requires a course of five to seven weeks daily treatment to be curative depending on the cancer anatomic sites and histology. Delay or discontinuation of treatment may lead to a high risk of recurrence. Because of the necessity for long treatment time, it is inevitable that due to the prolonged lock down period, cancer patients may experience delayed and/or discontinued treatment. For example, in one study of 209 cancer patients, only 46.4% completed their radiotherapy course (67). In other studies, screening of patients for viral infection during treatment may also have led to unnecessary treatment interruption as patients with low grade fever are required to stay home as a safety measure (68). Up to 88.3% of the patients experienced radiotherapy delay or interruption due to various reasons (69). Many patients experienced a treatment break of at least 45 days (70). Coronavirus infection and fear of coronavirus infection also played a part in radiotherapy disruption (71, 72). Table 2 summarizes cancer treatment delay or discontinuation during the pandemic.
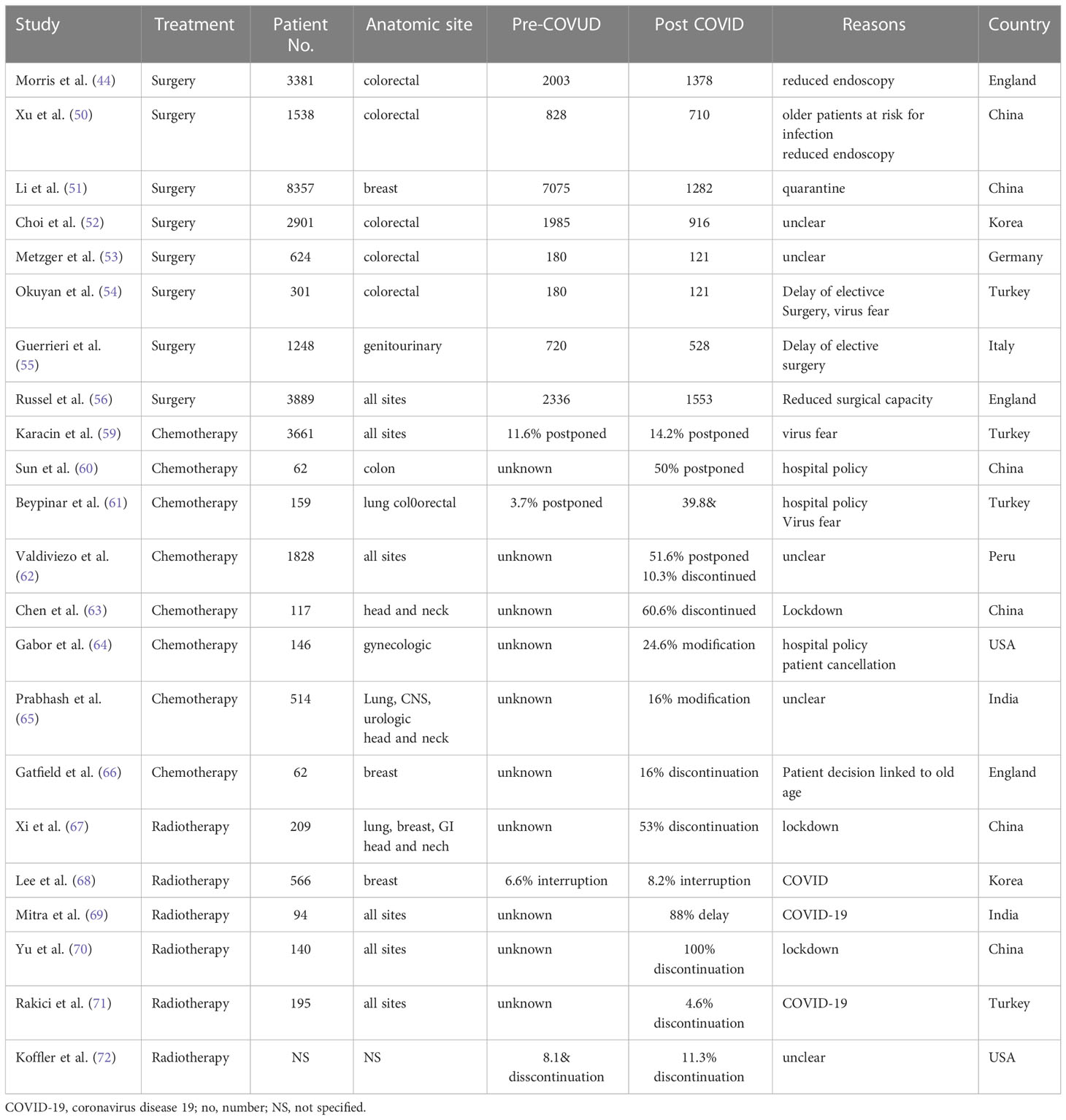
Table 2 Decrease or delay in cancer treatment during COVID-19 pandemic.
It is clear that COVID-19 has affected early cancer diagnosis and has disrupted cancer treatment during the pandemic regardless of age, sex, or socio-economic status. However, the most affected were older cancer patients who, besides their fear of getting infected, also face other challenges in obtaining quality care such as social isolation, transportation difficulties, and age discrimination. While most cancer patients who contracted viral infection during the early phase of the pandemic only experienced a temporary interruption of their treatment, greater delays and modifications of treatment plans may have been considered necessary for older cancer patients (73). Thus, we propose a strategy combining modern technology such as telemedicine and spiritual support such as prayer, to improve the care of older patients during the COVID-19 pandemic, as it is very likely that the virus will remain with us in the foreseeable future.
To be effective, any measure that aims to improve older cancer patients’ quality of care should include their caregivers: spouses, children, grandchildren, or friends if the patient is single. Cancer patient caregivers have to coordinate all the physicians’ appointments into their work schedule, become patient advocates, provide emotional support to the patient, and manage the side effects of the treatment such as nausea and vomiting from chemotherapy. As a result, cancer caregivers develop a high level of anxiety and depression facing a task that they are unprepared for (74). In addition, minority patients often have a higher rate of depression than Caucasians, which is likely related to a lower socio-economic status (75). They also face transportation and communication barriers with health care professionals (76). Minority patients tend to instead rely on spirituality to overcome fears and find hope, to a greater extend than other ethnic groups (77, 78). Across the world, lower socio-economic status is also associated with a higher level of mental distress and depression similar to levels in minority patients. In the time of COVID-19, prayer and faith are the coping mechanisms for those patients. It seems logical to group them as economically disadvantaged (ED) patients to reflect the challenges that they face into obtaining quality of care.
The immediate impact of telemedicine is a reduced risk of SARS-CoV-2 infection while providing care to older cancer patients and their caregivers in the comfort of their home environment. Its real-time approach allows the patients and their caregivers active participation with the medical team which results in a high level of satisfaction (79). The Veterans Health Administration system, among the nation’s largest health care system, has successfully implemented telemedicine for cancer patients (80). Both medical oncologists and radiation oncologists can conduct preliminary telehealth visit with the patients and the caregivers. Surgical oncology consultation can also be conducted virtually for low-risk procedures or in cases that require only imaging for surgical planning. If the patient is suspected to have cancer, an electronic consultation is requested by the primary care physician. The case is then reviewed by an expert or discussed through a virtual tumor board. Biopsy and further work-up can be arranged afterward. This approach is innovative because it reduces the need for transportation for patients who live in rural areas far away from medical centers. The state of Alaska also delivers a telehealth network to provide education to Native and Alaskans cancer survivors that is tailored to their culture (81). Thus, telemedicine may improve the quality of life (QOL) of minority older cancer patients and their caregivers by focusing on special aspect of their culture such as spirituality as a support mechanism.
The first message by the medical team through virtual meeting should highlight the clinic or hospital safety measures to prevent coronavirus infection such as temperature check, screening for COVID-19 exposure, personal protection equipment (PPE), full vaccination of the medical staff, a COVID-19 testing policy, and strict adherence to a clean environment. If a patient tests positive for the virus, what are the measures taken to keep the other patients safe? Those are the two main concerns expressed during a survey by patients who were afraid to seek emergency care due to the fear of the virus (49).
Once the patient and the caregiver are reassured, the medical team should introduce themselves. Ideally, the medical team should include oncologists (medical, surgical, and radiation oncologist), a geriatrician, a patient navigator, a social worker, a home health nurse, a faith-based leader, and if needed a translator for non-English speaking patients. Many telemedicine platforms are now available to provide virtual consultation with multiple health care providers at the same time for patients and their family members who may live in different states. This will give the patients and their caregivers the confidence that they will be in charge with a professional team to assess all their needs from daily transportation to spirituality. This is particularly important for ED cancer patients who often feel that their spiritual needs are not supported by their health care providers (82).
The medical team should also emphasize that the side effects that the patient may experience during treatment such as nausea, vomiting, or pain can be managed through telemedicine to avoid unnecessary visits to the emergency room which would further expose them to the virus. Caregivers’ education is particularly important for older cancer patients due to their frailty and possible mental issues. Stress and anxiety should be assessed through questionnaires, and mental health referral should be initiated if needed. Patient spiritual needs can also be assessed through questionnaires. Once the patients and their caregivers are satisfied with the initial consultation, further in-person or virtual follow-up visits can be scheduled. If a high level of religiosity is expressed by the patients and/or their caregivers, further follow-up visits can also be arranged to take place virtually with the religious representative.
Compared with other socio-economic groups, ED cancer caregivers carry a higher burden in taking care of loved ones while facing many challenges such as transportation issues in getting to physician appointment or treatment sessions, lack of access to computers for disease information and education, and in the case of Latinos or other immigrant cancer patients, a language barrier (76, 83, 84). However, it has been reported that ED patients cope well with adversity through spirituality as they are traditionally very religious (77, 78, 82, 85, 86). Spirituality is defined as an individual’s sense of peace, purpose, and connection to others, and beliefs about the meaning of life. In simple terms, it is a holistic belief that there is more in life than what is perceived on a sensory and physical level that connects people and the universe together. Common spiritual themes include life after death, seeking non-material happiness, and compassion for others. This aspect of their care is often overlooked by health care providers who may not be aware of cultural diversity. Thus, involvement of faith-based leaders and bilingual patient navigators in addition to health care workers, may help older ED cancer patients and their caregivers navigate through the treatment journey and improve their QOL. In contrast to the healthcare setting prevalent in the United States, in the Eastern world, spirituality, prayer, and meditation are more widely acceptable practices amongst all strata of society. The practice of prayer, meditation, and yoga, as well as other forms of spirituality have shown a definite role in reducing anxiety and improving QOL in cancer patients (87, 88). We therefore believe that inclusion of faith-based leaders in patient care is likely to be welcomed.
There is a good chance that telehealth may become widely adopted by ED older cancer patients, their caregivers, and globally. Surveys among Latinos and Africans Americans in inner cities or rural areas reveal a high level of enthusiasm for participation in telemedicine. Immediate feedback, reduced waiting time, increased access to specialists and access to multiple medical opinions are among the advantages that have been reported (89, 90). As an illustration of the popularity of telemedicine, among 10,657 adults of multiple ethnicities, Latinos and Africans Americans had a significantly higher rate of telemedicine participation than Caucasian Americans (91). Fear of COVID-19 may have accounted for the highest rate of telemedicine use among African Americans (92). A virtual environment may also be more conductive to overcoming mistrust among ED patients about discrimination by the healthcare system (92). A positive message is particularly important to encourage the COVID vaccination rate among ED cancer patients (93).
Preliminary data supports the efficacy of spiritual therapy in improving QOL in cancer patients and their caregivers, across the world (94–98). As an illustration, a randomized study of 65 breast cancer patients who underwent radiotherapy reported that those who received spiritual therapy had significantly increased well-being as assessed by the cancer QOL C-30 and breast cancer specific questionnaire BR-23 compared with the control group (96). Even though the study was small, it highlights the impact of psychotherapy utilizing religious technique to empower the patient to attain a non-material understanding of self, universe, incidences and phenomena. Prayer reduces anxiety and help patients cope with their disease. Other studies also corroborate the importance of spiritual therapy to improve cancer patient QOL across different cultures (94, 96–98). Both cancer patients and caregivers benefit from spiritual therapy. In previous studies, cancer patients or caregivers who possess high spirituality level also enjoy better QOL, compared with those who do not, due to enhanced ability to cope with the severe distress induced by their disease (99–101). In these studies, those with a high level of spirituality are defined as those who feel the presence of God in their life and believe that God may protect and heal their suffering. This feeling was reinforced by reading of the scripture which included stories of miraculous survival in impossible circumstances (100). Thus, as ED cancer patients and their caregivers have a generally high level of spirituality, prayers conducted virtually by a faith-based leader should improve their QOL before, during, and after cancer treatment.
The feasibility of virtual based chaplaincy has been investigated in one study. In a survey of 711 cancer patients who were screened for distress level, 212 expressed a high level of spirituality. Out of those, 124 spoke on the phone with the chaplain. An in-depth survey about spirituality and chaplain intervention was conducted, and on this basis 41 patients were scheduled for further intervention either by phone (n=30), or in person (n=11) (102). Even though this study was small, it highlights efficacy of conducting spiritual therapy in a virtual mode. During the pandemic, virtual prayers were conducted successfully as a group through a Zoom or Telegram platform. Participants who experienced loneliness due to isolation and social distancing, expressed a sense of harmony and connection to others and God which helped them to cope with the pandemic stress (103). By incorporating a faith-based leader in the telemedicine team, it is feasible that cancer patients and their caregivers who express a high spiritual level may benefit from virtual spiritual therapy.
COVID-19 vaccination should be recommended for older cancer patients, and in particular minorities, due to their high risk of death if infected. However, vaccine hesitancy is highest among African Americans and Hispanics. Vaccination hesitancy was 41.6% and 30.2% for African Americans and Hispanics, respectively compared with 26.3% for adult Caucasians Americans (104). The reason for vaccination hesitancy is complex but includes mistrust of the US government among other reasons (93). Thus, it is critical to promote a public health campaign about the safety and efficacy of COVID-19 vaccine to increase vaccination rate in minority cancer patients. Among those who receive vaccination, the protection rate conferred by the vaccine is not known with certainty. Even when fully vaccinated with a second boost dose, seroconversion rate in cancer patients was 88% and 70% for patients with solid tumors and hematologic malignancies, respectively (105). However, other studies have reported a lower seroconversion rate for patients with hematologic malignancies following vaccination which may improve with a third or a fourth vaccine dose (106, 107). As those patients are at high risk of death if infected, they should avoid public exposure. The role of telemedicine is particularly important to monitor older patients with hematologic malignancies.They should take proper COVID-19 protection measures, such as social distancing and wearing an N-95 respiratory mask during clinic visits. They should also be reassured that many measures have been in place to protect them from virus exposure during their time in the clinic. Trust of the medical system is fundamental to patient adherence to treatment.
In 1999, Ambassador Reverend Andrew Young declared in public his diagnosis of early prostate cancer to encourage young African Americans to get regular prostate cancer screening. He was treated with surgery and remains cancer-free to this day. This same time of action is needed during the COVID-19 pandemic. Public figures should follow Ambassador Reverend Young’s example and promote the need for early cancer diagnosis, as cancer when caught early is curable due to advance in treatment technology. As an illustration, early stage non-small cell lung cancer has an excellent rate of local control and minimal complications among older and frail patients with stereotactic body radiotherapy who are not candidates for surgery (108). The public message should continue to allay the fear of COVID-19, be positive about the effectiveness of the vaccine, and target ED patients and older people to seek early diagnosis and cancer treatment. Most ED patients have poor knowledge of cancer symptoms and/or face barriers to access cancer screening (109, 110). Lack of education about precision medicine, unmet psychosocial needs, and financial burdens are frequently cited by ED cancer patients as barriers to accessing quality treatment (110). Thus, social media interventions if conducted properly, may be effective in reaching that specific demographic for education and reassurance that chronological age is not an impediment for cancer treatment. A meta-analysis of social media intervention reported that use of a social media platform may be an effective way to improve basic cancer knowledge, increase cancer screening rates, and alleviate psychological distress through social support (111). As an illustration, pictures of sun-damaged skin and testimony from cancer survivors are powerful ways to educate a large public audience about the risk of skin cancer and the benefit of sunscreen (112). However, it is important to have a social influencer from the same ethnic, cultural, and age group who speaks out in simple terms in order to modify the behavior of those targeted (113). Participation of individuals from diverse ethnic groups and cultures in social media such as YouTube or Facebook may be more effective because of the sense of connection between the social influencer and their followers. There are many social media sites available, but according to the Pew Institute survey, YouTube and Facebook are the ones most predominantly used by individuals aged 65 or older (https://www.pewresearch.org). The current trend is very encouraging: many celebrities have opened up about their cancer diagnosis on World Cancer Day 2022, such as Karim Abdul Jabar who had chronic leukemia in 2008 and recently at the age of 73 was diagnosed with prostate cancer. Actress Jane Fonda also communicated her diagnosis of non-Hodgkin’s lymphoma through Instagram at the age of 84 and has begun her chemotherapy. Her message was very positive and reflected confidence about a good outcome. We hope that more older women will be encouraged by her example to seek medical care early if cancer is suspected. The role of faith-based social influencers was illustrated in a study which encouraged ED patients to seek cancer screening. Out of 778 ED patients who were not aware of cancer risks and the needs for early cancer screening, over a third had discussed cancer screening with their primary care providers following enrollment (114). Collaboration between health communication professionals and faith-based leaders was critical in educating those patients to seek cancer screening, with potentially life-saving consequences. As an international research network dedicated to older cancer patients, minorities, and women who are frequently excluded from clinical trials, we also hope that social media will be used in the future to attract older cancer patients to participate in clinical trials. Their enrollment in prospective studies will be crucial to develop guidelines to manage this vulnerable population.
During the pandemic, many professional groups have advocated the use of hypofractionated radiotherapy to shorten the treatment course of cancer patients and to reduce the risk of exposure to the SARS-CoV-2 virus (115, 116). Given the reduced mobility of older cancer patients, preexisting comorbidities, and/or frailty, this delivery of higher biological doses of radiation within a shorter treatment time may be particularly advantageous. The reduced need for daily transportation without sacrificing treatment effectiveness is an extra incentive for ED patients. As an illustration, a once a week treatment for six weeks has been reported to be well tolerated among 486 older breast cancer patients following surgery with excellent local control and survival (117). Thus, hypofractionated radiotherapy alone or associated with systemic therapy should be investigated in future prospective studies for older cancer patients (118).
It is clear that COVID-19 may increase the mortality rate of cancer patients regardless of age, due to delayed diagnosis and/or treatment. Many algorithms have been proposed to estimate the mortality risk following the pandemic which is currently far from over (119, 120). On the other hand, the pandemic also highlights the plight of older cancer patients who are frequently excluded from clinical trials (121). It is a paradox that although cancer prevalence increases with age, the number of older patients recruited in cancer clinical trials is low. As an illustration, in a review of 356 cancer trials, 67.7% either impose a strict upper age limit or a criterion on performance status which would reliably exclude older adults (122). Thus, public awareness and social media exposure may have a positive impact on clinical investigators, influencing them to review and reconsider those strict criteria for older cancer patients recruitment into clinical trials. Support and education through social media about the challenges facing older cancer patients may lead to innovative solutions to help them enroll in clinical trials, as older cancer patients may be socially isolated and less computer savvy than the younger generations (123, 124). In addition thanks in large part to the pandemic, the use of telemedicine has been accepted by the public, government, and the physician community as a convenient and potentially cost-saving measure to deliver quality care at a distance (125). Thus, on the positive side, COVID-19 has provided lessons on how to prepare and protect the most vulnerable segment of our society, older cancer patients, from future pandemics.
Older cancer patients have suffered disproportionally during the pandemic. Their fear of death due to viral infection has led to a delay in early cancer diagnosis and treatment. We propose telemedicine combined with spiritual therapy and a strong message through social media, as a way to allay the fear of these patients. In addition, we propose the development of treatment strategies that take into consideration ethnicity and culture for personalized treatment.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
All authors collected the data, discuss the data analysis, and review the final draft. All authors contributed to the article and approved the submitted version.
The authors would like to thank Dayleen DeRiggs and Carpe Diem Biomedical Writing and Editing for the help in editing this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Mueller AL, McNamara MS, Sinclair DA. Why does COVID-19 disproportionately affect older people. Aging (2020) 12:9959–81. doi: 10.18632/aging.103344
2. Freudenburg-Hua Y, Makhnevich A, Li W, Liu Y, Qiu M, Marziliano A, et al. Psychotropic medication use is associated with greater 1-year incidence of dementia after COVID-19 hospitalization. Front Med (2022) 9:841326. doi: 10.3389/fmed.2022.841326
3. Inouye SK. The importance of delirium and delirium prevention in older adults during lockdowns. JAMA Insights (2021) 325:1779–80. doi: 10.1001/jama.2021.2211
4. Cohen K, Ren S, Heath K, Dasmarinas MC, Jubilo KG, Guo Y, et al. Risk of persistent and new clinical sequelae among adults aged 65 years old and older during the post-acute phase of SARS-Cov-2 infection: Retrospective cohort study. BMJ (2022) 376:e068414. doi: 10.1136/bmj-2021-068414
5. El-Gohary GM, Hashmi S, Styczynski J, Kharfan-Dabaja MA, Alblooshi RM, de la Camara R, et al. The risk and prognosis of COVID-19 infection in cancer patients. Hematol Oncol Stem Cell Ther (2022) 15:45–53. doi: 10.1016/j.hemonc.2020.07.005
6. Lee LYU, Cazier J, Angelis V, Arnold R, Bisht V, Campton NA, et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatment. Lancet (2020) 395:1919–26. doi: 10.1016/S0140-6736(20)31173-9
7. Fillmoore NR, La J, Szalat RE, Tuck DP, Nguyen V, Yildirim C, et al. Prevalence and outcome of COVID-19 infection in cancer patients: A national veterans affair study. J Nat Cancer Inst (2021) 113:691–8. doi: 10.1093/jnci/djaa159
8. Li H, Baldwin E, Zhang X, Kenost C, Luo W, Calhoun EA, et al. Comparison and impact of COVID-19 for patients with cancer: a survival analysis of fatality rate controlling for age, sex, and cancer type. BMJ Health Care Inform (2021) 28:e100341. doi: 10.1136/bmjhci-2021-100341
9. Desai A, Gupta R, Advani S, Ouellette L, Kuderer NM, Lyman GH, et al. Mortality in hospitalized patients with cancer and coronavirus disease 2019: A systemic review and meta-analysis of cohort studies. Cancer (2021) 127:1459–68. doi: 10.1002/cncr.33386
10. Tsang S, Avery AR, Duncan GE. Fear and depression linked to COVID-19 exposure. a study of adult twins during the pandemic. Psychiatry Res (2021) 296:113699. doi: 10.1016/j.psychres.2020.113699
11. Budak EA, Karahan M, Han CC. Evaluation of anxiety and fear of COVID-19 in patients admitted to an ophthalmology outpatient clinic. Int J Clin Pract (2021) 75:e14519. doi: 10.1111/jcp.14519
12. Agrawal S, Drozdz M, Makuch S, Pietraszek A, Sobienszczanska M, Mazur Z. The assessment of fear of COVID-19 among the elderly population: a cross-sectional study. J Clin Med (2021) 10:5537. doi: 10.3390/jcm10235537
13. Yadav UN, Yadav OP, Singh DR, Ghimire S, Rayamajhee B, Mistry SK, et al. Perceived fear of COVID-19 and its associated factors among Nepalese older adults in eastern Nepal: a cross-sectional study. PloS One (2021) 16:e0244825. doi: 10.1371/journal.pone.0254825
14. Sigorski D, Sobczuk P, Osmola M, Kuc K, Walerzak A, Wilk M, et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open (2020) 5:e000970. doi: 10.1136/esmoopen-2020-000970
15. Czeisler ME, Marynak K, Clarke KEN, Salah Z, Shakya I, Thierry JM, et al. Delay or avoidance of medical care because of COVID-19-related concerns-united states, June 2020. MMWR Morb Mort Wkly Rep (2020) 69:1250–7. doi: 10.15585/mmwr.mm6936a4
16. Popescu T, Karlsson U, Vinh-Hung V, Trigo L, Thariat J, Te V, et al. Challenges facing radiation oncologists in the management of older cancer patients: Consensus of the international geriatric radiotherapy group. Cancers (2019) 11:1030371. doi: 10.3390/cancers11030371
17. Gyasi AM. Fighting COVID-19: Fear and internal conflict among older adults in Ghana. J Gerontolol Soc Work (2020) 63:688–90. doi: 10.1080/01634372.2020.1766630
18. Caycho-Rodriguez T, Tomas JM, Barboza-Palomino M, Ventura-Leon A, Gallegos M, Reyes-Bossio M, et al. Assessment of fear of COVID-19 in older adults: Validation of the fear of COVID-19 scale. Int J Ment Health Addict (2022) 20:1231–45. doi: 10.1007/s11469-020-00438-2
19. Parlapani A, Holeva V, Vasiliki A, Sereslis K, Athanasiodou M, Godosidis A, et al. Intolerance of uncertainty and loneliness in older adults during the pandemic. Front Psychiatry (2020) 11:842. doi: 10.3389/fpsyt.2020.00842
20. Ahorsu DK, Lin C, Pakpour AH. The association between health status and insomnia, mental health, and preventive behaviors: The mediating role of fear of COVID-19. Gerontol&Geriatr Med (2021) 7:1–9. doi: 10.1177/2333721420966081
21. Han MFY, Mahendran R, Yu J. Association between fear of COVID-19, affective symptoms and risk perception among community dwelling older adults during a COVID-19 lockdown. Front Psychol (2021) 12:638831. doi: 10.3389/fpsyg.2021.638831
23. Nino M, Harris C, Drawve G, Kirkpatrick KM. Race and ethnicity, gender, and age on perceived threats and fear of COVID-19: Evidence from two national data sources. SSM Popul Health (2021) 13:100717. doi: 10.1016/j.ssmph.2020.100717
24. Jacobs M, Burch AE. Anxiety during the pandemic: Racial and ethnic differences in the trajectory of fear. J Affect Disord (2021) 292:58–66. doi: 10.1016/j.jad.2021.05.027
25. Chatters LM, Taylor HO, Taylor RJ. Older black americans during COVID-19: Race and age double jeopardy. Health Educ Behav (2020) 47:855–60. doi: 10.1177/1090198120965513
26. Sneed RS, Key K, Bailey S, Johnson-Lawrence V. Social and psychological consequences of the COVID-19 pandemic in africans americans communities. Trauma Psych (2020) 12:446–8. doi: 10.1037/tra0000881
27. Meng Y, Lu W, Guo E, Liu J, Yang B, Wu P, et al. Cancer history is an independent risk factor for mortality in hospitalized COVID patients. J Hematol Oncol (2020) 13:75. doi: 10.1186/s13045-020-00907-0
28. Ferrari BL, Ferreira CJ, Menezes M, De Marchi P, Canedo J, De Melo AC, et al. Determinants of COVID-19 mortality in patients with cancer in a community hospital. J Glob Oncol (2021) 7:46–55. doi: 10.1200/GO.20.00444
29. Lee LYW, Caziez J, Starkey T, Brigg SE, Arnold R, Bisht V, et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumor subtype and patient demographics: A prospective cohort study. Lancet Oncol (2020) 21:1309–16. doi: 10.1016/S1470-2045(20)30442-3
30. Ng KYY, Zhou S, Tan SH, Ishak NDB, Ghoh ZZS, Chua JY, et al. Understanding the psychologic impact of COVID-19 pandemic on patients with cancer, their caregivers, and healthcare workers in Singapore. JCO Glob Oncol (2020) 6:1494–509. doi: 10.1200/GO.20.00374
31. Feder S, Smith D, Griffin H, Shreve ST, Kinder D, Kutney-Lee A, et al. Why couldn’t I go in to see him. bereaved families’ perception of end of life communication during COVID-19. JAGS (2021) 69:587–92. doi: 10.1111/jgs.16993
32. Olufadewa II, Adesina MA, Oladokun B, Baru A, Oladele RI, Iyanda TO, et al. I Was scare I might die alone: a qualitative study on the physical and psychological experience of COVID-19 survivors and the quality of care received at health facilities. Int J Travel Med Glob Health (2020) 8:51–7. doi: 10.34172/ijtmgh.2020.09
33. Selman LE, Chamberlain C, Sowden R, Chao D, Selman D, Taubert M, et al. Sadness, despair, and anger when a patient dies alone from COVID-19. a thematic content analysis of twitter data from bereaved family members and friends. Palliative Med (2021) 35:1267–76. doi: 10.1177/02692163211017026
34. Gultekin M, Ak S, Ayhan A, Strojna A, Pletnev A, Fagotti A, et al. Perspective, fears, and expectation of patients with gynaecological cancers during the COVID-19 pandemic: A pan-European study of the European network of gynaecological cancer advocacy group (ENGAGe). Cancer Med (2020) 10:208–19. doi: 10.1002/cam4.3605
35. Vanni G, Materrazzo M, Pellicciaro M, Ingallinella S, Rho M, Santori F, et al. Breast cancer and COVID-19: The effect of fear on patient decision-making process. In Vivo (2020) 34:1651–9. doi: 10.21873/invivo.11957
36. Quaquarini E, Saltalamachia G, Presti D, Caldana G, Tibollo V, Malovini A, et al. Impact of COVID-19 break on cancer patient care and treatment: Data from an outpatient oncology clinic in lombardi (Italy). Cancers (2020) 12:2941. doi: 10.3390/cancers12102941
37. Hamilton AC, Donnelly DW, Loughrey MB, Turkington RC, Fox C, Fitzpatrick D, et al. Inequalities in the decline and recovery of pathological cancer diagnosis during the first six months of the COVID-19 pandemic: a population-based survey. Br J Cancer (2021) 125:798–805. doi: 10.1038/s41416-021-01472-0
38. Fonseca GA, Normando PG, Loureiro LVM, Rodrigues REF, Oliveira VA, Melo MDT, et al. Reduction in the number of procedures and hospitalizations and increase in cancer mortality during the COVID-19 pandemic in Brazil. JCO Global Oncol (2021) 7:4–9. doi: 10.1200/GO.20.00471
39. Arduino PG, Conrotto D, Broccoletti R. The outbreak of novel coronarovirus disease (COVID-19) caused a worrying delay in the diagnosis of oral cancer in north-west Italy: The Turin metropolitan area experience. Oral Dis (2021) 27(Suppl 3):742–3. doi: 10.1111/odi.13362
40. Blay JY, Boucher S, Le Vu B, Cropet C, Chabaud S, Perol D, et al. Delayed care for patients with newly diagnosed cancer during COVID-19 and estimated impact on cancer mortality in France. ESMO Open (2021) 6:1–11. doi: 10.1016/j.esmoop.2021.100134
41. Jacob L, Loosen SH, Kalder M, Luedde T, Roderburg C, Kostev K. Impact of the COVID-19 pandemic on cancer diagnoses in general and specialized practices in Germany. Cancers (2021) 13:408. doi: 10.3390/cancers13030408
42. Coma E, Guiriguet C, Mora N, Marzo-Castillejo M, Benitez M, Mendez-Boo L, et al. Impact of the COVID-19 pandemic and related control measures on cancer diagnosis in Catalonia: a time-series analysis of primary care electronic health records covering about 5 million people. BMJ Open (2021) 11:e047567. doi: 10.1136/bmjopen-2020-047567
43. Aparicio T, Layese R, Hemery F, Tournigand C, Paillaud E, De Angelis N, et al. Effect of lockdown on digestive cancer care among older patients during the first wave of COVID-19: The CADIGCOVAGE multicentre cohort study. Digestive Liver Dis (2022) 54:10–8. doi: 10.1016/j.dld.2021.09.017
44. Morris EJA, Godacre R, Spata E, Mafham M, Finan PJ, Shelton J, et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: a population-based study. Lancet Gastroenterol Hepatol (2021) 6:199–208. doi: 10.1016/S2468-1253(21)00005-4
45. Suarez J, Mata E, Guerra A, Jimenez G, Montes M, Arias F, et al. Impact of the COVID-19 pandemic during spain’s state of emergency on the diagnosis of colorectal cancer. J Surg Oncol (2021) 123:32–6. doi: 10.1002/jso.26263
46. De Guzman R, Malik M. Dual challenge of cancer and COVID-19: Impact on health care and socioeconomic systems in Asia pacific. JCO Global Oncol (2020) 6:906–12. doi: 10.1200/GO.20.00227
47. Stoss C, Steffani M, Pergolini I, Hartmann D, Radenkovic D, Novotny A, et al. Impact of the COVID-19 pandemic on surgical oncology in Europe. Dig Surg (2021) 38:259–165. doi: 10.1159/000515186
48. Ranganathan P, Sengar M, Chinnaswamy G, Agrawal G, Arumugham R, Bhatt R, et al. Impact of COVID-19 in cancer care in India: A cohort study. Lancet Oncol (2021) 22:970–6. doi: 10.1016/S1470-2045(21)00240-0
49. Wong LE, Hawkins JE, Langness S, Murrell KL, Iris P, Samman A. Where are all the patients? addressing COVID-19 fear to encourage sick patients to seek emergency care. NEJM Catalyst (2020) 3:1–12. doi: 10.1056/CAT.20.0193
50. Xu Y, Huang Z, Zheng CZ, Li C, Zhang Y, Guo T, et al. The impact of COVID-19 pandemic on colorectal cancer patients: a single center retrospective study. BMC Gastroenterol (2021) 21:185. doi: 10.1186/s12876-021-01768-8
51. Li J, Wang H, Geng C, Liu Z, Lin Y, Nie J, et al. Suboptimal declines and delays in early breast cancer treatment after COVID-19 restrictions in china: a national survey of 8397 patients in the first quarter of 2020. EClin Med (2020) 26:100503. doi: 10.1016/j.eclinm.2020.100503
52. Choi JY, Park IJ, Lee HG, Cho E, Kim YL, Kim CW, et al. Impact of COVID-19 pandemic on surgical treatment patterns for colorectal cancer in a tertiary medical facility in Korea. Cancers (2021) 13:1221. doi: 10.3390/cancers13092221
53. Metzer K, Mrosek J, Zittel S, Pilz M, Held T, Adeberg S, et al. Treatment delay and tumor size in patients with oral cancer during the pandemic. Head Neck (2021) 43:3493–7. doi: 10.1002/hed.26858
54. Okuyan GC, Yildirim M. The effect of COVID-19 pandemic on the outcomes of surgically treated colorectal diseases. Ann Surg Treat Res (2022) 103:104–11. doi: 10.4174/astr.2022.103.2.104
55. Guerrieri R, Rovati L, Dell’Oglio P, Galfano A, Raggazoni L. Impact of the COVID-19 pandemic on urologic oncology. surgery: Implications for moving forward. J Clin Med (2022) 11:171. doi: 10.3390/jcm11010171
56. Russell B, Moss C, Monroy-Iglesias M, Roberts G, Dickinson H, Haire K, et al. Radical cancer treatment is safe during COVID-19: The real world experience of a large London-based comprehensive cancer centre during the first wave. Br J Cancer (2022) 127:1289–95. doi: 10.1038/s41416-022-01909-0
57. Mulita F, Vallas M, Tchabashvili L, Liolis E, Iliopoulos F, Drakos N. The impact of the COVID-19 outbreak on emergency surgery: a Greek emergency experience. Gastroenterol Rev (2021) 16:95. doi: 10.5114/pg.2021.104739
58. Mulita F, Sotiropoulou M, Vailas M. A multifaceted virus. non reducible and strangulated effect of COVID-19. J Trauma Acute Care Surg (2021) 91:e34. doi: 10.1097/TA.0000000000003219
59. Karacin C, Bilgetekin I, Basai FB, Oksuzoglu O. How does COVID-19 fear and anxiety affect chemotherapy adherence in patients with cancer. Future Oncol (2020) 16:2283–93. doi: 10.2217/fon-2020-0592
60. Sun L, Xu Y, Zhang T, Yang Y. Impact of the COVID-19 outbreak on adjuvant chemotherapy for patients with stage II or III colon cancer: Experiences from a muliticentre clinical trial in China. Curr Oncol (2020) 27:159–62. doi: 10.3747/co.27.6529
61. Beypinar I, Urun M. Intravenous chemotherapy adherence of cancer patients in time of COVID-19 crisis. Int J Hematol Oncol (2020) 30:133–8. doi: 10.4999/uhod.204528
62. Valdiviezo N, Alcarraz C, Castro D, Salas R, Begazo-Mollo V, Galvez-Villanueva M, et al. Oncological care during first Peruvian national emergency COVID-19 pandemic. Cancer Mang Res (2022) 14:1075–85. doi: 10.2147/CMAR.S350038
63. Chen G, Wu Q, Jiang H, Zhong Y. The impact of COVID-19 pandemic on head and neck cancer patients. Oral Oncol (2020) 110:104881. doi: 10.1016/j.oraloncology.2020.104881
64. Gabor L, Gowthaman D, Gressel G, Kuo DY, Nevadunsky N, Bansal N. The impact of SARS-COV2 pandemic on the delivery of chemotherapy for gynenologic cancer at a tertiary care institution in the united states epicenter. Gynecol Oncol (2021) 162:S298. doi: 10.1016/j.ygyno.2021.12.004
65. Prabhash K, Noronha V, Shah D, Mokal S, Kapoor A, Patil VM, et al. Deviation from cancer treatment during the first wave of COVID-19 pandemic in India: A cross-sectional study. Cancer Res Stat Treat (2022) 5:212–9. doi: 10.4103/crst.crst_115_22
66. Gatfield E, Bataineh A, El Kurdi B, Mukesh MB, Loo SW. Factors associated with systemic anti-cancer treatment discontinuation for early breast cancer during the COVID-19 pandemic. Eur J Cancer Care (2022) 31(6):e13668. doi: 10.1111/ecc.13668
67. Xie C, Wang X, Liu H, Bao Z, Yu J, Zhong Y, et al. Outcomes in radiotherapy-treated patients with cancer during the COVID-19 outbreak. JAMA Oncol (2020) 6:1457–8. doi: 10.1001/jamaoncol.2020.2783
68. Lee S, Heo J. COVID-19 pandemic: a new cause for unplanned treatment interruption. Med Oncol (2022) 39:5. doi: 10.1007/s12032-021-01604-9
69. Mitra S, Simson DK, Khurana H, Tandon S, Ahlawat P, Bansal N, et al. Treatment delay during radiotherapy of cancer patients due to COVID-19 pandemic. Asian Pac J Cancer Prev (2020) 23:2415–20. doi: 10.31557/APJCP.2022.23.7.2415
70. Yu D, Hu W, Chen L, Fu Z, Song Q, Li X. Effect of radiotherapy interruption due to COVID-19 outbreak. Radiother Oncol (2021) 155:1–2. doi: 10.1016/j.radonc.2020.09.055
71. Uslu GH, Kucuktutu E, Rakici SY. COVID-19 and radiotherapy: the ordeal faced by the patients and the staff during the pandemic in the first year. J Radiat Cancer Res (2022) 155:1–2. doi: 10.4103/jrcr.jrcr_14_22
72. Koffler D, Ma DC, Eckstein J, Sidiqi A, Adair N, Joseph S, et al. Impact of the COVID-19 pandemic on radiation treatment termination patterns at a large multi-center institution. Int J Radiat Oncol Biol Phys (2021) 111:3056. doi: 10.1016/j.ijrobp.2021.07.1394
73. Pramesh CS, Chinnaswamy G, Sengar M, Ranganathan P, Badwe R. COVID-19 and cancer care in India. Nat Cancer (2021) 21:1257–9. doi: 10.1038/s43018-021-00290-w
74. Grunfeld E, Coyle D, Whelan T, Clinch J, Reyno L, Earle CC, et al. Family caregiver burden: Results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ (2004) 150:1795–801. doi: 10.1503/cmaj.1031205
75. Ettman CK, Cohen GH, Abdallah SM, Galea S. Do assets explain the relation between race/ethnicity and probable depression in US adults. PloS One (2020) 15:e0239618. doi: 10.1371/journal.pone.0239618
76. Schwartz A, Jenkins CL. Barriers and facilitator to cancer treatment adherence for older rural africans americans: Understanding the experience from the view of patients and their caregivers. J Famil Soc Work (2020) 20:20–34. doi: 10.1080/10522158.2019.1658250
77. Sterba KR, Burris JL, Heiney SP, Ruppel MB, Ford ME, Japka J. We both trusted and leaned on the lord: a qualitative study on religiousness and spirituality among africans americans cancer survivors and their caregivers. Qual Life Res (2014) 23:1909–20. doi: 10.1007/s11136-014-0654-3
78. Juarez G, Branin JJ, Rosales M. Perception of QOL among caregivers of Mexican ancestry of adults with advanced cancer. Qual Life Res (2014) 24:1729–40. doi: 10.1007/s11136-014-0911-5
79. Lopez AM, Avery D, Krupinski E, Lazarus S, Weinstein R. Increasing access to care via telehealth: The Arizona experience. J Amb Care Manag (2005) 28:16–23. doi: 10.1097/00004479-200501000-00003
80. Jiang CY, El-Kpuri NT, Elliot D, Shields J, Caram MEV, Frankel TL, et al. Telehealth for cancer care in veterans: Opportunities and challenges revealed by COVID. JCO Oncol Pract (2020) 17:22–9. doi: 10.1200/OP.20.00520
81. Doorenbos AZ, Demiris G, Towle C, Kundu A, Revels L, Colven R, et al. Developing the native people for cancer control. Telemed eHealth (2011) 17:30–4. doi: 10.1089/tmj.2010.0101
82. Delgado-Guay MO, Palma A, Duarte E, Grez M, Tupper L, Liu DD, et al. Association between spirituality, religiosity, spiritual pain, symptom distress, and quality of life among Latin American patients with advanced cancer. J Palliat Med (2021) 24:1606–15. doi: 10.1089/jpm.2020.0776
83. Martin MY, Sanders S, Griffin JM, Oster RA, Ritchie C, Phelan S, et al. Racial variation in the cancer caregiving experience: A multi-site study of colorectal and lung cancer caregivers. Cancer Nurs (2012) 35:249–56. doi: 10.1097/NCC.0b013e3182330850
84. Kayser K, DeMarco RF, Stokes C, DeSanto-Madeya S, Higgins PC. Delivery palliative care to patients and caregivers in inner-cities communities: Challenges and opportunities. Palliat Support Care (2014) 12:369–78. doi: 10.1017/S1478951513000230
85. Hastings JF, Nugraheni SE, Neighbors HW. Africans americans, caregiving, and physical health ratings: Does culture, religion and spirituality provide support? Race Soc Prol (2020). doi: 10.1007/s12552-020-09302-3
86. Juarez G, Branin JJ, Rosales M. The cancer caregiving experience of caregivers of Mexican ancestry. Hisp Care Int Health (2014) 12:120–6. doi: 10.1891/1540-4153.12.3.120
87. George SM, Hamilton A, Baker RS. How do low-income urban African americans and latinos feel about telemedicine? a diffusion of innovation analysis. Int J Telemed Appl (2012) 715194:1–9. doi: 10.1155/2012/715194
88. Joshi AM, Mehta SA, Mehta AO, Ughade SN, Randhe KS. Effect of yoga therapy on psychological distress and quality of life in head and neck cancer patients undergoing radiotherapy. Yoga Mimamsa (2021) 53:82–90. doi: 10.4103/ym.ym_97_21
89. Aggawal S, Sharma R, Aggarwal A, Shrma R. Voice of cancer patients. analysis of use and efficacy of yoga and medication in cancer patients. J Clin Oncol (2018) 15(suppl):e18801–e8801. doi: 10.1200/jco2018.36.15_SUPPL.E18801
90. Ghaddar S, Vatcheva RP, Alvarado SG, Mykita L. Understanding the intention to use telehealth services in underserved Hispanic border communities. J Med Internet Res (2020) 22:e212012. doi: 10.2196/21012
91. Campos-Castillos C, Anthony D. Racial and ethnic differences in self-reported telehealth use during the COVID-19 pandemic: A secondary analysis of a US survey of internet users from late march. J Am Med Inform Assoc (2021) 28:119–25. doi: 10.1093/jamia/ocaa221
92. Ramos SQ, Warren R, Shedlin M, Melkus G, Kershaw T, Vorderstrasse A. A framework for using eHealth intervention to overcome medical distrust among sexual minority men of color living with chronic conditions. Behav Med (2019) 45:166–76. doi: 10.1080/08964289.2019.1570074
93. Nguyen NP, Oboite E, Oboite J, Thandeka M, Vuong T, Baumert BG, et al. COVID-19 vaccination among minority cancer patients: Recommendation of the international geriatric radiotherapy group. Arch Clin BioMed Res (2021) 5:415–8. doi: 10.26502/acbr.50170174
94. Sankhe A, Dalal K, Agarwal V, Sarve P. Spiritual care therapy on quality of life in cancer patients and their caregivers: A prospective non-randomized single-cohort study. J Relig Health (2017) 56:725–31. doi: 10.1007/s10943-016-0324-6
95. Jafari N, Zamani A, Farajzadegan Z, Bahrami F, Emami H, Loghmani A. The effect of spiritual therapy for improving the quality of life of women with breast cancer: a randomized controlled trial. Psychol Health Med (2013) 18:56–69. doi: 10.1080/13548506.2012.679738
96. Zamaniyan S, Bolhari J, Naziri Z, Akrami M, Hosseini S. Effectiveness of spiritual group therapy on quality of life and spiritual well-being among breast cancers. Iran J Med Sci (2016) 41:140–4.
97. Vallurupalli M, Lauderdale K, Balboni MJ, Phelps AC, Block SD, Ng AK, et al. The role of spirituality and religious coping in the quality of life of patients with advanced cancer receiving palliative radiation therapy. J Support Oncol (2012) 10:81–7. doi: 10.1016/j.suponc.2011.09.003
98. Ichihara K, Ouchi S, Okayama S, Kinoshita F, Miyashita M, Morita T, et al. Effectiveness of spiritual care using spiritual assessment sheet for advanced cancer patients: a pilot randomized trial. Palliat Support Care (2019) 17:46–53. doi: 10.1017/S1478951518000901
99. Garduno-Ortega O, Morales-Cruz J, Hunter-Hernandez M, Gany F, Costas-Muniz R. Spiritual well-being, depression, and quality of life among latina breast cancer survivors. J Relig Health (2021) 60:1895–907. doi: 10.1007/s10943-020-01147-9
100. Hamilton JB. Emotional suffering and the use of spirituality as a resource among African American cancer survivors. J Cancer Educ (2021) 34:409–11. doi: 10.1007/s13187-019-01558-7
101. Leow LQH, Chan M, Chan SWC. Predictors of change in quality of life of family caregivers of patients near the end of life with advanced cancer. Cancer Nurs (2014) 37:391–400. doi: 10.1097/NCC.0000000000000101
102. Sprik P, Keenan AJ, Boselli D, Cheeseboro S, Meadors P, Grossoehme D. Feasibility and acceptability of a telephone-based chaplaincy intervention in a large, outpatient oncology center. Support Care Cancer (2021) 29:1275–85. doi: 10.1007/s00520-020-05598-4
103. Keisari S, Biancalani G, Tavelli E, Fassina S, Testoni I. Spirituality during COVID-19 in northern Italy: The experience in participating an online prayer group. Pastoral Psychol (2022) 71:201–15. doi: 10.1007/s11089-022-00998-1
104. Khubchandani J, Macias Y. COVID-19 vaccine hesitancy in hispanics and African americans: A review and recommendations for practice. Brain Behav Immun Health (2021) 15:100207. doi: 10.1016/j.bbih.2021.100277
105. Javadina SA, Alizadeh K, Mojadadi M, Nikbakht F, Dashti F, Joudi M, et al. COVID-19 vaccination in patients with malignancy. a systemic review and meta-analysis of the efficacy and safety. Front Endocrinolol (2022) 13:860238. doi: 10.3389/fendo.2022.860238
106. Thakkar A, Pradhan K, Duva B, Carreno JM, Sahu S, Thiruthuvanathan V, et al. Efficacy and longevity of immune response to 3rd COVID-19 vaccine and effectiveness of a 4th dose in severely immunocomprommised patients with cancer. medRxiv (2022). doi: 10.1101/2022.07.05.22277281
107. Tzarfati KH, Gutwein O, Apel A, Rahimi-Levene N, Sadovnik M, Harel L, et al. BNT162b2 COVID-19 vaccine is significantly less effective in patients with hematologic malignancies. Am J Hematol (2021) 96:1195–203. doi: 10.1002/ajh.26284
108. Nguyen NP, Godinez J, Shen W, Vinh-Hung V, Gorobets H, Thariat J, et al. Is surgery indicated for elderly patients with early stage nonsmall cell cancer in the era of stereotactic body radiotherapy? Medicine (2016) 96:e5212. doi: 10.1097/MD.0000000000005212
109. Niksic M, Rachet B, Warburton FG, Forbes LJL. Ethnic differences in cancer symptom awareness and barriers to seeking medical help in England. Br J Cancer (2016) 115:146–4. doi: 10.1038/bjc.2016.158
110. Patel MI, Agrawal M, Duron Y, O’Brien D, Koontz Z. Perspective of low income and minority populations with lung cancer. JCO Oncol Pract (2022) 18:e1374–1382. doi: 10.1200/OP.22.00052
111. Han CJ, Lee YJ, Demiris G. Interventions using social media for cancer prevention and management. a systematic review. Cancer Nurs (2018) 41:e19–31. doi: 10.1097/NCC.0000000000000534
112. Dela Garza H, Maymone MBC, Vashi NA. Impact of social media on skin cancer prevention. Int J Environ Res Pub Health (2021) 18:5002. doi: 10.3390/ijerph18095002
113. Bandura A. Social cognitive theory of mass communication. Media Psychol (2001) 3:265–99. doi: 10.1207/S1532785XMEP0303_03
114. Maxwell AE, Lucas-Wright A, Santifer RE, Vargas C, Gatson J, Chang LC. Promoting cancer screening in partnership with health ministries in 9 American churches in south Los Angeles: an implementation pilot study. Prev Chronic Dis (2019) 16:190135. doi: 10.5888/pcd16.190135
115. Parashar B, Chen WC, Herman JM, Potters L. Disease site-specific guidelines for curative radiation treatment during limited surgery and hospital avoidance: A radiation oncology perspective from the epicenter of COVID-19 pandemic. Cureus (2020) 12:e8190. doi: 10.7759/cureus.8190
116. Thompson DJ, Yom SS, Saeed H, El Naqa I, Ballas L, Bentzen SM, et al. Radiation fractionation schedules published during the COVID-19 pandemic: a systemic review of the quality of evidence and recommendations for future development. Int J Radiat Oncol Biol Phys (2020) 108:379–89. doi: 10.1016/j.ijrobp.2020.06.054
117. Sanz J, Zhao M, Rodriguez N, Granado R, Foro P, Reig A, et al. Once-weekly hypofractionated radiotherapy for breast cancer in elderly patients: Efficacy and tolerance in 486 patients. BioMed Res Int (2018) 8321871:1–9. doi: 10.1155/2018/8321871
118. Vinh-Hung V, Gorobets O, Duerinckx A, Dutta S, Oboite E, Oboite J, et al. Is immunotherapy at reduced dose and radiotherapy for older patients with locally advanced non-small cell lung cancer feasible? a narrative review by the international geriatric radiotherapy group. Transl Cancer Res (2022) 11:3298–308. doi: 10.21037/tcr-22-821
119. Lai AG, Pasea L, Banerjee A, Hall G, Denaxas S, Chang WH, et al. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and mortality: Near real-time data on cancer care, cancer deaths and a population-based cohort study. BMJ Open (2020) 10:e043828. doi: 10.1136/bmjopen-2020-043828
120. Sud A, Jones ME, Broggio J, Loveday C, Torr B, Garrett A, et al. Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann Oncol (2020) 31:1065–74. doi: 10.1016/j.annonc.2020.05.009
121. Lewis JH, Kilgore ML, Goldman DP, Trimble EL, Kaplan R, Montello MJ, et al. Participation of patients 65 years of age or older in cancer clinical trials. J Clin Oncol (2016) 21:1383–9. doi: 10.1200/JCO.2003.08.010
122. Krysa K, Kowalczyk E, Borysowski J, Lachota M, Pasierski T. Exclusion of older adults from clinical trials in cancer related pain. Front Med (2022) 9:945481. doi: 10.3389/fmed.2022.945481
123. Han CJ, Lee YJ, Demiris G. Interventions using social media for cancer prevention and management. Cancer Nurs (2018) 31:e19–31. doi: 10.1097/NCC.0000000000000534
124. Criado JI, Sandoval-Almazan R, Gil Garcia JR. Government innovation through social media. Gov Inf Quaterly (2013) 30:319–26. doi: 10.1016/j.giq.2013.10.003
Keywords: older, cancer patients, pandemic, fear, telemedicine, spiritual treatment
Citation: Nguyen NP, Karlsson UL, Lehrman D, Mazibuko T, Saghatelyan T, Thariat J, Baumert BG, Vinh-Hung V, Gorobets O, Giap H, Singh S, Chi A, Alessandrini G, Ahluwalia A, Durosinmi-Etti F, Zegarra Cárdenas J, Diabate K, Oboite J, Oboite E, Mehmood T, Vuong T, Kim L and Page BR (2023) Impact of COVID-19 pandemic on older cancer patients: Proposed solution by the International Geriatric Radiotherapy Group. Front. Oncol. 13:1091329. doi: 10.3389/fonc.2023.1091329
Received: 06 November 2022; Accepted: 18 January 2023;
Published: 07 March 2023.
Edited by:
Marine Hovhannisyan, Yerevan State Medical University, ArmeniaReviewed by:
Prabakaran D.S., Chungbuk National University, Republic of KoreaCopyright © 2023 Nguyen, Karlsson, Lehrman, Mazibuko, Saghatelyan, Thariat, Baumert, Vinh-Hung, Gorobets, Giap, Singh, Chi, Alessandrini, Ahluwalia, Durosinmi-Etti, Zegarra Cárdenas, Diabate, Oboite, Oboite, Mehmood, Vuong, Kim and Page. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nam Phong Nguyen, TmFtUGhvbmcuTmd1eWVuQHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.