 Binwei Lin1,2†
Binwei Lin1,2† Feng Gao
Feng Gao Dai Wu
Dai Wu Xiaobo Du
Xiaobo Du
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 23 September 2022
Sec. Radiation Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.995612
This article is part of the Research Topic365 Days of Progress In Radiation OncologyView all 7 articles
FLASH radiotherapy (FLASH-RT) is a novel radiotherapy technology defined as ultra-high dose rate (≥ 40 Gy/s) radiotherapy. The biological effects of FLASH-RT include two aspects: first, compared with conventional dose rate radiotherapy, FLASH-RT can reduce radiation-induced damage in healthy tissue, and second, FLASH-RT can retain antitumor effectiveness. Current research shows that mechanisms of the biological effects of FLASH-RT are related to oxygen. However, due to the short time of FLASH-RT, evidences related to the mechanisms are indirect, and the exact mechanisms of the biological effects of FLASH-RT are not completely clear and some are even contradictory. This review focuses on the mechanisms of the biological effects of FLASH-RT and proposes future research directions.
Cancer is one of the leading causes of human death (1). Radiotherapy, as one of the main treatments for cancer, can improve the overall survival time (2) and quality of life (3) and can achieve a radical cure (4) in patients with malignancy. However, the overall anti-tumor effect of radiotherapy is still limited (5). The dose limitation of organs at risk surrounding the cancer leads to the relatively insufficient target dose, and this may be the key factor affecting the anti-tumor effect. Modern radiotherapy technologies, such as volumetric modulated arc therapy, tomotherapy, and proton radiotherapy, can optimize the dose distribution (6, 7) and reduce the toxicity in normal tissues; however, the enhancement of anti-tumor effect is limited (8).
FLASH radiotherapy (FLASH-RT) is a novel radiotherapy technology defined as ultra-high dose rate (≥ 40 Gy/s) radiotherapy. Compared with conventional radiotherapy (COVN-RT), FLASH-RT can effectively reduce the toxicity in normal tissues and provide similar anti-tumor effects, which is defined as the FLASH effect (9). Preclinical studies have confirmed that FLASH-RT can effectively reduce the toxicities in lung (10, 11), intestine (12), brain (13), and skin (14), and retain the anti-tumor effect on cancer (11, 15, 16). Due to these encouraging results, FLASH-RT is considered as a revolutionary technology in the field of radiotherapy (17). However, due to the short time of FLASH-RT, evidences regarding the mechanism of FLASH effect are indirect. Therefore, the exact mechanisms of the biological effects of FLASH-RT are not completely clear and some are even contradictory.
The purpose of this review is to provide a relatively brief literature review and discuss the mechanism of the FLASH effect and mainly review the research progress in two aspects: physical-chemical mechanism and biological mechanism.
The mechanism of FLASH effect included the physical-chemical mechanism and biological mechanism, the organs involved include lung, brain, intestine, skin etc (Figure 1 and Table 1).
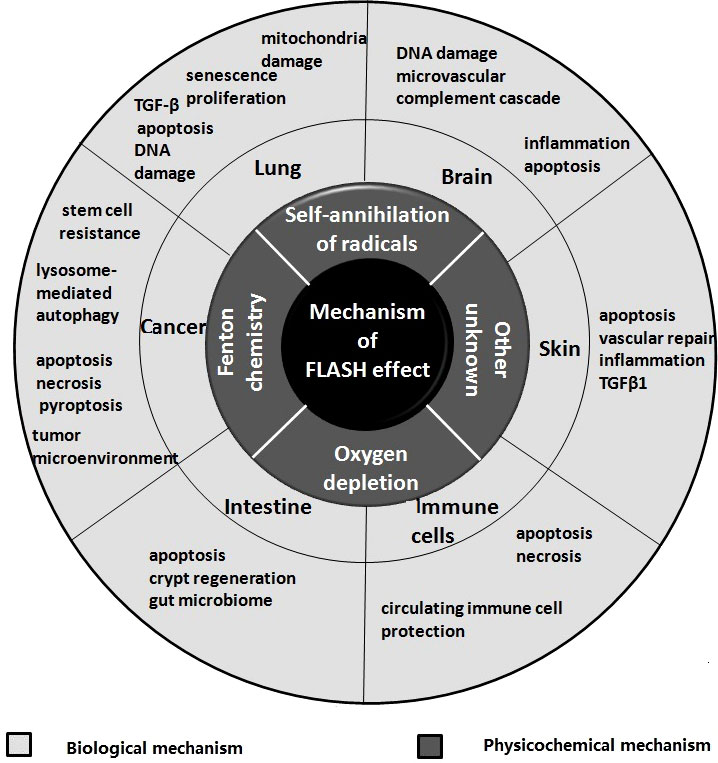
Figure 1 Themechanisms of FLASH effect.
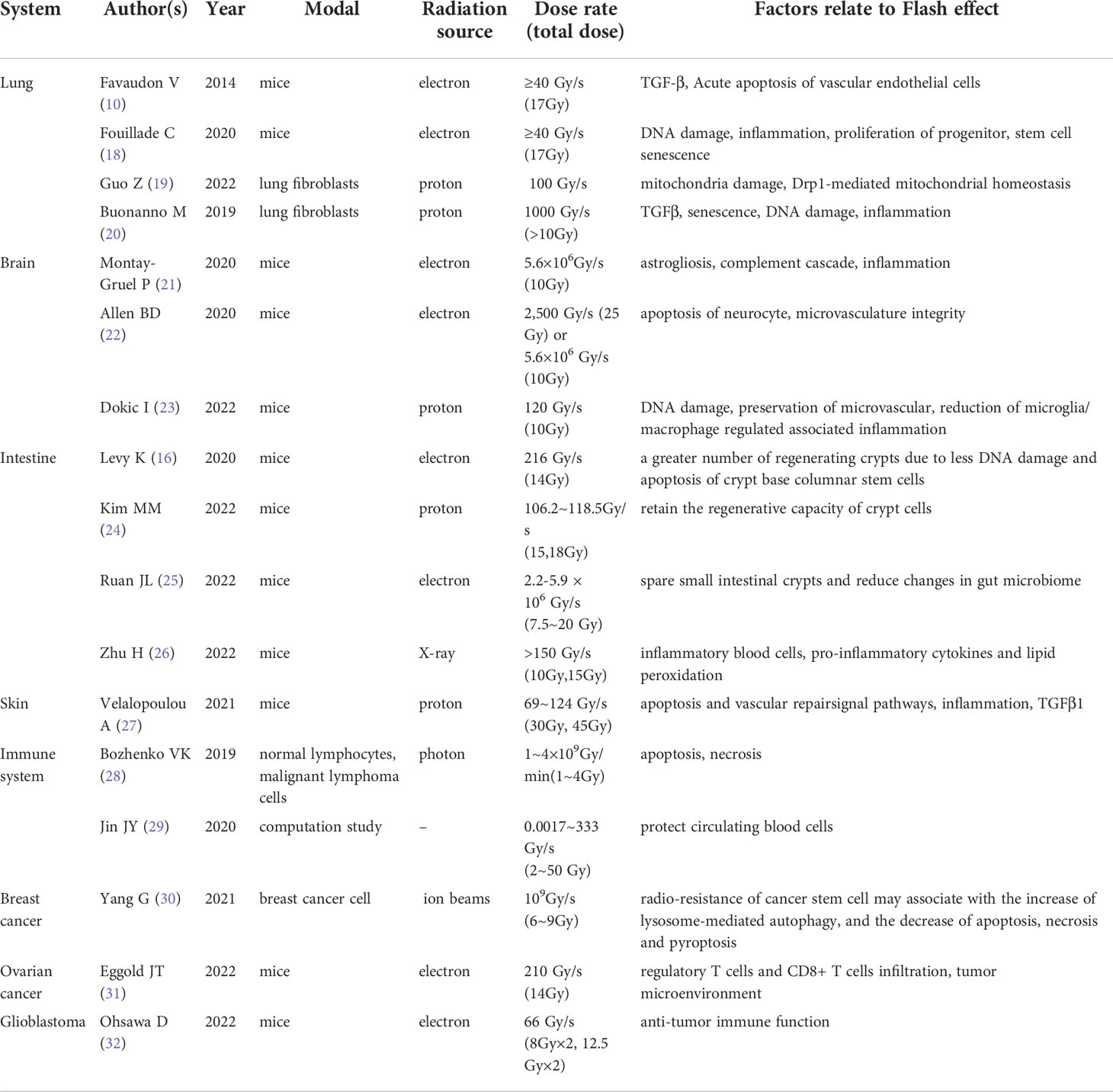
Table 1 Summary of published studies on FLASH effect mechanism.
Free radicals produced by radiation are the root cause of radiation damage. Some studies try to explain the effects of FLASH-RT and COVN-RT by the differences of physical-chemical reaction after radiation.
Oxygen is considered as an important radiation sensitizer (33). Compared with hypoxic tissue, oxygen rich tissue has stronger radiosensitivity under the same radiation conditions (34). As FLASH-RT can complete the irradiation in a very short time (microseconds), the oxygen in the tissue is rapidly exhausted, and it is too fast to be supplemented by the circulating blood. This results in the relative lack of oxygen in the tissue compared with COVN-RT (irradiation completed in a few minutes), which may be one of the reasons why FLASH-RT can protect the normal tissue (35).The basis for the formation of this hypothesis comes from the early in vitro studies on bacteria (36) and mammalian cells (37). It is believed that hypoxia can lead to radiation resistance under ultra-high dose rate irradiation, and this resistance effect reached the maximum under nitrogen condition (oxygen concentration: 0%) (37). Hornsey et al. further supported this hypothesis through in vivo experiments. When the dose rate was >6 krad/min, the mortality after whole-body irradiation (in the oxygen inhalation state during irradiation) decreased; however, when the mice were in the nitrogen breathing state during irradiation, the protective effect of ultra-high dose rate radiotherapy was lost (38).
Increasing evidences show that the hypothesis of oxygen depletion cannot fully explain the protective effect of FLASH-RT on normal tissues. Firstly, Jansen et al. measured the change of oxygen content in pure water after FLASH-RT, and found that although FLASH-RT could indeed consume more oxygen than COVN-RT, it could not deplete all oxygen (39). Moreover, when the total dose of FLASH-RT was 10 Gy, oxygen consumption was not detected in vitro (39).This contradicted the result that 10 Gy FLASH-RT can better preserve the neural function of mice than COVN-RT in animal experiments (40, 41). Secondly, Epp et al. found that the protective effect of FLASH-RT on mammalian cells occurred when the oxygen concentration is very low (less than 0.5%) (37). Adrian et al. (42) found that FLASH-RT showed a higher cell survival rate than COVN-RT only under hypoxic conditions (oxygen concentration less than 4.4%) and when the total dose exceeded 5-10Gy. One possible explanation is that only when the oxygen concentration is low, FLASH-RT can completely consume the oxygen. However, Gabriel et al. (43) found that the protective effect of FLASH-RT was observed in MDA-MB-231, MCF7 and HeLa cell lines under normoxic conditions (air oxygen concentration). Moreover, the protective effect of FLASH-RT was also observed in oxygen rich tissues such as lung (10). In addition the oxygen depletion hypothesis cannot explain that FLASH-RT and COVN-RT have similar antitumor effects. Because the tumor tissue is relatively hypoxic, FLASH-RT will lead to tumor cell resistance rather than retain the anti-tumor effect.
Since the oxygen depletion hypothesis cannot fully explain the FLASH effect, Spitz et al. (44) believed that the difference in metabolism of peroxidized compounds and labile iron content between the tumor and normal tissue may be the mechanism of FLASH-RT in reducing normal tissue damage and retaining anti-tumor effect. Compared with tumor tissues, normal tissues retain the metabolic process of peroxidized compounds, therefore, normal tissues have lower peroxidized compounds than tumor tissues, and the labile iron content in normal tissues is lower, which is not conducive to the damage of Fenton chemistry to normal tissues (44). However, Spitz et al. only reasoned from the theoretical model, and subsequent experimental verification, especially the use of animal model of gene knockout of key metabolic enzymes, is very important to verify the Spitz ‘s theory.
Abolfath et al. (45) found that FLASH effect was related to O2 concentration by simulating DNA damage models under different conditions. In normal tissues (oxygen concentration 4%-5%), oxygen and DNA molecules form reactive oxygen species (ROS) after radiation. Compared with COVN-RT, the concentration of ROS under FLASH-RT was higher, which lead to the reorganization of ROS free radicals. Subsequently, as the ROS load was reduced, the damage of FLASH-RT to normal tissues was lowered. However, in tumor tissues, the presence of hypoxia (oxygen concentration <0.4%), the production of ROS decreased, resulting in the loss of tissue protection. Labarbe et al. (46) further proposed a theoretical model based on the formation and decay dynamics of ROS. It was found that peroxyl radicals (ROO) was the key component leading to radiation damage, and there was a correlation between the area under the ROO. curve and the probability of normal tissue complications. Compared with COVN-RT, the production rate of ROO. under FLASH-RT was significantly higher. The reduction of ROO. caused by free radical recombination may play a major role in the tissue protection of FLASH-RT. Lai et al. (47) also concluded by using micro-Monte Carlo simulation method that when the dose rate is 107Gy/s and the dose reached 30Gy, it was difficult to exhaust the tissue oxygen with an initial concentration of 0.01%-21%. Compared with COVN-RT, FLASH-RT has higher instantaneous ROO. concentration, and the decrease of ROO. content caused by self-recombination may be the reason of FLASH effect. However, the theory of free radical recombination only comes from model inference. Because the time of free radical recombination is very short, it is difficult to verify it under experimental conditions. Interestingly, Blain et al. (48) found that the production of H2O2 (one kind of ROS) was significantly reduced in FLASH-RT group when compared with that in COVN-RT group though in vitro study. Moreover, the decrease degree of H2O2 is negatively correlated with the dose rate. When the FLASH dose rate is lower than 100Gy/s, the decrease of H2O2 is more dramatic. When the FLASH dose rate exceeded 60000Gy/s, the decrease degree of H2O2 reaches a platform (38% ± 4%). However, H2O2 cannot represent ROS, future studies are needed to compare the differences of other ROS between FLASH-RT and COVN-RT.
The reduction of stem cell senescence may play an important role in FLASH-RT protection effect. Unlike apoptosis, senescent cells could secrete prion flammatory cytokines, such as IL-6, TGF-β and IL-1α, and lead to subsequent pulmonary fibrosis (18). Moreover, the stem cell senescence hinders the process of cell regeneration after radiation injury (18, 49). Fouillade et al. (49) conducted a preclinical study to evaluate the role of stem cell senescence in the protection of normal tissues by FLASH-RT. C57BL/6J mice were irradiated under FLASH-RT (>40Gy/s, 17Gy) and COVN-RT (<0.003Gy/s, 17 Gy) conditions using electron. They found that compared with COVN-RT group, FLASH-RT had less lung injury and similar anti-tumor effect. Further studies showed that the lung protective effect of FLASH-RT may be related to the retention of stem cell replication ability, because they found that the number of senescence stem cells (reduced or disappeared replication ability) in the FLASH-RT group decreased by 50% compared with the COVN-RT group. More importantly, Fouillade et al. compared the lung injury between TERC-/- mice (mice with extremely short telomeres, simulating the state of stem cells senescence) and wild mice, the phenomenon of FLASH-RT on lung protection disappeared in TERC-/- mice. Yang et al. (30) compared the damage ability of FLASH-RT to tumor stem cells and normal tumor cells in vitro. They concluded that under the condition of FLASH-RT (109Gy/s, 6~9Gy), tumor stem cells and normal tumor cells both will undergo apoptosis, scorch, and necrosis after irradiation. However, tumor stem cells have stronger radiation resistance than normal tumor cells. The radiation resistance of cancer stem cells may be related to the increase of lysosome mediated autophagy. Due to Yang et al. (30) did not compare the damage of FLASH-RT and COVN-RT on tumor stem cells, whether tumor stem cells affect the retention anti-tumor effect of FLASH-RT needs further study.
The retention of the stem cell division ability by FLASH-RT may only partially explain the protective effect of FLASH-RT on normal tissues, and there may be other relevant mechanisms for the retention of the anti-tumor effect (27). Simultaneously, more studies are needed to verify the experimental results of Fouillade et al.
Radiation damage has been shown to be a sterile inflammatory process (50), and immune function plays an important role in radiation injury (51). TGF-β has been proved to be an inflammatory factor that participates in the process of DNA damage, repair and cellular inflammatory response and promotes the formation of radiation-induced pulmonary fibrosis (52). Several studies show that the expression of TGF-β in FLASH-RT group was significantly decreased when compared with COVN-RT group (10, 20, 27). Fouillade et al (49) studied the role of immune inflammatory change in lung injury after FLASH-RT. The animal model and radiotherapy parameters used in the study were consistent as previously described. The results showed that FLASH-RT had less expression of pro-inflammatory factor gene (EGR1) and lower up-regulation of inflammatory factor (TGF-β1, NF-KB) than COVN-RT. Zhu et al. (26) reported the changes of immune and inflammatory responses after FLASH-RT(>150Gy/s, 10Gy and 15Gy) irradiation on the intestine of mice(BALB/c). X-ray was used in Zhu’s study. They found that compared with COVN-RT, the mice in FLASH-RT group had lower intestinal toxicity, inflammatory blood cells (leukocytes, lymphomas, neutrophils), pro-inflammatory cytokines (TNF- α, IL-6, IL-10) and lipid peroxidation were significantly reduced. Preclinical studies suggest that the increase of chronic neuritis associated with microglia activation may be related to radiation-induced brain injury (53, 54). Montay-Gruel et al. (21) studied the brain damage of mice (C57BL/6J) caused by FLASH-RT(5.6 × 106Gy/s, 10Gy) and COVN-RT(0.1Gy/s, 10Gy) using electron beam. They found that the expression level of the markers (GFAP, TLR4) that activate astrocyte proliferation in the brain of FLASH-RT group were significantly lower than that in COVN-RT group. Recently, the experimental results of Dokic et al. (23) also supported that FLASH-RT reduced microglia/macrophage regulated inflammation compared with COVN-RT.
Circulating immune cells may have an important impact on the repair of normal tissues after radiotherapy (55) and the anti-tumor effect (56, 57). Therefore, the protection of circulating immune cells by FLASH-RT may be part of the mechanism of FLASH effect. Jin et al. (29) used computer simulation to evaluate the effects of FLASH-RT and COVN-RT on circulating immune cells. They found that the killing rate of FLASH-RT on circulating immune cells was significantly lower than that of COVN-RT (5%-10% vs 90%-100%). However, it should be noted that this research was only computer simulation, and the research results needed to be verified by experiments. Moreover, only the circulating immune cells were considered in this study, rather than the evaluation of immune cells in immune organs and tumor tissues. Whether FLASH-RT can protect the whole immune function needs to be studied in the future. Eggold et al. (31) evaluated the effect of FLASH-RT on immune cells in tumor by establishing an animal model of peritoneal ovarian cancer. It was found that regulatory T cells decreased and CD8+ T cells increased in tumors treated with FLASH-RT(210 Gy/s,14Gy) and COVN-RT(0.126 Gy/s,14Gy). When compared with COVN-RT, FLASH-RT group had significantly more T cell infiltration, especially CD8+ T. When radiotherapy was combined with PD-1 inhibitor, the anti-tumor effect of FLASH-RT group was better than that of COVN-RT group. The reliability of the results of Eggold’s study needs to be confirmed by more preclinical studies, however, this study suggested that FLASH-RT combined with immunotherapy may have bright prospects.
Immune function may also play an important role in preserving the antitumor effect of FLASH-RT. Recently, Liljedahl et al. (32) used tumor bearing mice to compare the anti-tumor effect of FLASH-RT(66 Gy/s, 8Gy×2 fractions and 12.5 Gy×2 fractions) and COVN-RT(0.133Gy/s, 8Gy×2 fractions and 12.5 Gy×2 fractions), and re-challenged the cured mice after radiotherapy to evaluate the long-term anti-tumor effect. They found that FLASH-RT and COVN-RT had similar anti-tumor effect (median survival time: 100 days vs 100 days, p>0.05). Cured mice (FLASH-RT: 8 mice; COVN-RT: 6 mice) were then rechallenged with tumor. The results showed that tumor re-growth was not detected in the additional 100 days.
Vascular injury caused by radiotherapy is considered to be an important part of radiation injury (58, 59). Favaudon et al. (10) found that FLASH-RT can reduce the acute apoptosis of bronchial vessels compared with COVN-RT. Two studies focus on brain injury showed that FLASH-RT was superior to COVN-RT in protecting the integrity of microvessels in the brain, which may be conducive to the preservation of cognitive function by FLASH-RT (22, 23). However, the current research evidence only supports that FLASH-RT has less vascular damage than COVN-RT, and the impact of FLASH-RT on the upstream gene regulatory pathway is not clear.
Three preclinical studies show that the protective effect of FLASH-RT on intestinal tract may be related to the protection of intestinal crypt cells by FLASH-RT (16, 24, 25). Ruan et al. (25) also found that FLASH-RT has less impact on intestinal flora than COVN-RT, which may be more conducive to the protection of intestinal function. Guo et al. (19) found that FLASH-RT can reduce mitochondrial damage mediated by Dynamin-1-like protein. Jay et al. (60) believed that FLASH-RT may produce an early transient strong acidic environment, which may be one of the mechanisms of FLASH-RT to protect normal tissues. Ohsawa et al. (61) studied the effect of proton FLASH-RT (40 Gy/s) and COVN-RT (0.05 Gy/s) on DNA damage. They found that compared with COVN-RT, the single strand DNA breakage in FLASH-RT group was significantly reduced, but the double strand DNA breakage was similar. Ohsawa et al. (61) speculated that the FLASH-RT might effectively reduce non lethal damage, such as cell senescence, genomic instability and cell transformation.
The mechanism of FLASH effect include physical-chemical mechanism, biological mechanism and others, which involved oxygen depletion, Fenton effect, free radical recombination, stem cells, immune function, blood vessels, etc. But the published results on the mechanism of FLASH effect can not fully explain the FLASH effect. More studies are needed to clarify the real mechanisms of FLASH-RT and the weight values of different mechanisms.
BL and DH draft the manuscript, FG, YY, DW, YZ, GF, and TD participated in the data review and collection for the study. XD conceived of the study, and participated in its design and coordination. All authors contributed to the article and approved the submitted version.
This work was financially supported by the NHC Key Laboratory of Nuclear Technology Medical Transformation (Mianyang Central Hospital) (grantnos. 2022HYX008) and Natural Science Foundation of Sichuan Province (grant no.2022NSFSC0849).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Pineros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer (2021) 149:778–89. doi: 10.1002/ijc.33588
2. Cozzi S, Alì E, Bardoscia L, et al. Stereotactic body radiation therapy (SBRT) for Oligorecurrent/OligoprogressiveMediastinal and hilar lymph node metastasis: A systematic review. Cancers (Basel) (2022) 14(11):2680. doi: 10.3390/cancers14112680
3. Rim CH, Park S, Yoon WS, Shin IS, Park HC. Radiotherapy for bone metastases of hepatocellular carcinoma: a hybrid systematic review with meta-analyses. Int J Radiat Biol (2022):1–12. doi: 10.1080/09553002.2022.2094020
4. Jicman Stan D, Niculet E, Lungu M, Onisor C, Rebegea L, Vesa D, et al. Nasopharyngeal carcinoma: A new synthesis of literature data (Review). ExpTher Med (2022) 23(2):136. doi: 10.3892/etm.2021.11059
5. Delaney G, Jacob S, Featherstone C, Barton M. The role of radiotherapy in cancer treatment: estimating optimal utilization from a review of evidence-based clinical guidelines. Cancer (2005) 104(6):1129–37. doi: 10.1002/cncr.21324
6. Cheng YK, Kuo SH, Yen HH, Wu JH, Chen YC, Huang MY. The prognostic significance of pretreatment squamous cell carcinoma antigen levels in cervical cancer patients treated by concurrent chemoradiation therapy and a comparison of dosimetric outcomes and clinical toxicities between tomotherapy and volumetric modulated arc therapy. Radiat Oncol (2022) 17(1):91. doi: 10.1186/s13014-022-02063-w
7. Paganetti H, Botas P, Sharp GC, Winey B. Adaptive proton therapy. Phys Med Biol (2021) 66(22):TR01. doi: 10.1088/1361-6560/ac344f
8. Lin SH, Hobbs BP, Verma V, Tidwell RS, Smith GL, Lei X, et al. Randomized phase IIB trial of proton beam therapy versus intensity-modulated radiation therapy for locally advanced esophageal cancer. J Clin Oncol (2020) 38(14):1569–79. doi: 10.1200/JCO.19.02503
9. Favaudon V, Labarbe R, Limoli CL. Model studies of the role of oxygen in the FLASH effect. Med Phys (2022) 49(3):2068–81. doi: 10.1002/mp.15129
10. Favaudon V, Caplier L, Monceau V, Pouzoulet F, Sayarath M, Fouillade C, et al. Ultrahigh dose-rate flash irradiation increases the DifferentialResponse between normal and tumor tissue in mice. Sci Trans Med (2014) 6(245):245ra93–245ra93. doi: 10.1126/scitranslmed.3008973
11. Gao F, Yang Y, Zhu H, Wang J, Xiao D, Zhou Z, et al. First demonstration of the FLASH effect with ultrahigh dose rate high-energy X-rays. Radiother Oncol (2022) 166:44–50. doi: 10.1016/j.radonc.2021.11.004
12. Loo BW, Schuler E, Lartey FM, Rafat M, King GJ, Trovati S, et al. (P003)Delivery of ultra-rapid flash radiation therapy and demonstration ofNormal tissue sparing after abdominal irradiation of mice. Int J Radiat Oncol (2017) 98:E16. doi: 10.1016/j.ijrobp.2017.02.101
13. Simmons DA, Lartey FM, Schüler E, Rafat M, King G, Kim A, et al. Reduced cognitive deficits after FLASH irradiation ofWholeMouse brain are AssociatedWith less hippocampal dendritic spine loss and neuroinflammation. Radiother Oncol (2019) 139:4–10. doi: 10.1016/j.radonc.2019.06.006
14. Singers Sørensen B, Krzysztof Sitarz M, Ankjærgaard C, Johansen J, Andersen CE, Kanouta E, et al. In vivo validation and tissue sparing factor for acute damage of pencil beam scanning proton FLASH. Radiother Oncol (2022) 167:109–15. doi: 10.1016/j.radonc.2021.12.022
15. Montay-Gruel P, Acharya MM, Gonçalves Jorge P, Petit B, Petridis IG, Fuchs P, et al. Hypo-fractionated FLASH-RT as an effective treatment against glioblastoma that reduces neurocognitive side effects in mice. Clin Cancer Res (2020) 27(3):775–84. doi: 10.1158/1078-0432.CCR-20-0894
16. Levy K, Natarajan S, Wang J, Chow S, Eggold JT, Loo PE, et al. Abdominal FLASH irradiation reduces radiation-induced gastrointestinal toxicity for the treatment of ovarian cancer in mice. Sci Rep (2020) 10(1):21600. doi: 10.1038/s41598-020-78017-7
17. Maxim PG, Keall P, Cai J. FLASH radiotherapy: Newsflash or flash in the pan? Med Phys (2019) 46(10):4287–90. doi: 10.1002/mp.13685
18. Citrin DE, Shankavaram U, Horton JA, Shield W 3rd, Zhao S, Asano H, et al. Roleof type II pneumocyte senescence in radiation-induced lung fibrosis. J Natl Cancer Inst (2013) 105:1474–84. doi: 10.1093/jnci/djt212
19. Guo Z, Buonanno M, Harken A, Zhou G, Hei TK. Mitochondrial damage response and fate of normal cells exposed to FLASH irradiation with protons. Radiat Res (2022) 197(6):569–82. doi: 10.1667/RADE-21-00181.1
20. Buonanno M, Grilj V, Brenner DJ. Biological effects in normal cells exposed to FLASH dose rate protons. Radiother Oncol (2019) 139:51–5. doi: 10.1016/j.radonc.2019.02.009
21. Montay-Gruel P, Markarian M, Allen BD, Baddour JD, Giedzinski E, Jorge PG, et al. Ultra-High-Dose-Rate FLASH irradiation limits reactive gliosis in the brain. Radiat Res (2020) 194(6):636–45. doi: 10.1667/RADE-20-00067.1
22. Allen BD, Acharya MM, Montay-Gruel P, Jorge PG, Bailat C, Petit B, et al. Maintenance of tight junction integrity in the absence of vascular dilation in the brain of mice exposed to ultra-High-Dose-Rate FLASH irradiation. Radiat Res (2020) 194(6):625–35. doi: 10.1667/RADE-20-00060.1
23. Dokic I, Meister S, Bojcevski J, Tessonnier T, Walsh D, Knoll M, et al. Neuroprotective effects of ultra-high dose rate FLASH Bragg peak proton irradiation. Int J Radiat Oncol Biol Phys (2022) 113(3):614–23. doi: 10.1016/j.ijrobp.2022.02.020
24. Kim MM, Verginadis II, Goia D, Haertter A, Shoniyozov K, Zou W, et al. Comparison of FLASH proton entrance and the spread-out Bragg peak dose regions in the sparing of mouse intestinal crypts and in a pancreatic tumor model. Cancers (Basel) (2021) 13(16):4244. doi: 10.3390/cancers13164244
25. Ruan JL, Lee C, Wouters S, Tullis IDC, Verslegers M, Mysara M, et al. Irradiation at ultra-high (FLASH) dose rates reduces acute normal tissue toxicity in the mouse gastrointestinal system. Int J Radiat Oncol Biol Phys (2021) 111(5):1250–61. doi: 10.1016/j.ijrobp.2021.08.004
26. Zhu H, Xie D, Yang Y, Huang S, Gao X, Peng Y, et al. Radioprotective effect of X-ray abdominal FLASH irradiation: Adaptation to oxidative damage and inflammatory response may be benefiting factors. Med Phys (2022) 49(7):4812–22. doi: 10.1002/mp.15680
27. Velalopoulou A, Karagounis IV, Cramer GM, Kim MM, Skoufos G, Goia D, et al. FLASH proton radiotherapy spares normal epithelial and mesenchymal tissues while preserving sarcoma response. Cancer Res (2021) 81(18):4808–21. doi: 10.1158/0008-5472.CAN-21-1500
28. Bozhenko VK, Ivanov AV, Kulinich TM, Smirnov VP, Shishkin AM, Solodky VA. Comparison of biological effects of ?-radiation of low and ultra-high dose rate on lymphocytes and cultured human malignant lymphoma cells. Bull Exp Biol Med (2019) 166(6):785–7. doi: 10.1007/s10517-019-04440-0
29. Jin JY, Gu A, Wang W, Oleinick NL, Machtay M, Spring Kong FM. Ultra-high dose rate effect on circulating immune cells: A potential mechanism for FLASH effect? Radiother Oncol (2020) 149:55–62. doi: 10.1016/j.radonc.2020.04.054
30. Yang G, Lu C, Mei Z, Sun X, Han J, Qian J, et al. Association of cancer stem cell radio-resistance under ultra-high dose rate FLASH irradiation with lysosome-mediated autophagy. Front Cell Dev Biol (2021) 9:672693. doi: 10.3389/fcell.2021.672693
31. Eggold JT, Chow S, Melemenidis S, Wang J, Natarajan S, Loo PE, et al. Abdominopelvic FLASH irradiation improves PD-1 immune checkpoint inhibition in preclinical models of ovarian cancer. Mol Cancer Ther (2022) 21(2):371–81. doi: 10.1158/1535-7163.MCT-21-0358
32. Liljedahl E, Konradsson E, Gustafsson E, Jonsson KF, Olofsson JK, Ceberg C, et al. Long-term anti-tumor effects following both conventional radiotherapy and FLASH in fully immunocompetent animals with glioblastoma. Sci Rep (2022) 12(1):12285. doi: 10.1038/s41598-022-16612-6
33. Read J. Mode of action of X-raydoses given with different oxygenconcentrations. Br J Radiol (1952) 25:336–8. doi: 10.1259/0007-1285-25-294-336
34. Spiro IJ, Ling CC, Stickler R, Gaskill J. Oxygen radiosensitisation at low dose rate. Br J Radiol. (1985) 58(688):357–63. doi: 10.1259/0007-1285-58-688-357
35. Weiss H, Epp ER, Heslin JM, Ling CC, Santomasso A. Oxygen depletion in cells irradiated at ultra-high dose-rates and at conventional dose-rates. Int J Radiat Biol Relat Stud Phys Chem Med (1974) 26(1):17–29. doi: 10.1080/09553007414550901
36. Dewey DL, Boag JW. Modification of the oxygen EffectWhen bacteria are GivenLarge pulses of radiation. Nature (1959) 183(4673):1450. doi: 10.1038/1831450a0
37. Epp ER, Weiss H, Djordjevic B, Santomasso A. The radiosensitivity of cultured mammalian cells exposed to single high intensity pulses of electrons in various concentrations of oxygen. Radiat Res (1972) 52(2):324–32. doi: 10.2307/3573572
38. Hornsey S, Bewley DK. Hypoxia in mouse intestine induced by electron irradiation at high dose-rates. Int J Radiat Biol Relat Stud Phys Chem Med (1971) 19(5):479–83. doi: 10.1080/09553007114550611
39. Jansen J, Knoll J, Beyreuther E, Pawelke J, Skuza R, Hanley R, et al. Does FLASH deplete oxygen? experimental evaluation for photons, protons, and carbon ions. Med Phys (2021) 48(7):3982–90. doi: 10.1002/mp.14917
40. Montay-Gruel P, Acharya MM, Petersson K, Alikhani L, Yakkala C, Allen BD, et al. Long-term neurocognitive benefits of FLASH radiotherapy driven by reduced reactive oxygen species. Proc Natl Acad Sci USA (2020) 117(41):25946–7. doi: 10.1073/pnas.1901777116
41. Montay-Gruel P, Bouchet A, Jaccard M, Patin D, Serduc R, Aim W, et al. X-Rays can trigger the FLASH effect: Ultra-high dose-rate synchrotron light source prevents normal brain injury after whole brain irradiation in mice. Radiother Oncol (2018) 129(3):582–8. doi: 10.1016/j.radonc.2018.08.016
42. Adrian G, Konradsson E, Lempart M, Bäck S, Ceberg C, Petersson K. The FLASH effect depends on oxygen concentration. Br J Radiol (2020) 93(1106):20190702. doi: 10.1259/bjr.20190702
43. Adrian G, Konradsson E, Beyer S, Wittrup A, Butterworth KT, McMahon SJ, et al. Cancer cells can exhibit a sparing FLASH effect at low doses under normoxic In vitro-conditions. Front Oncol (2021) 11:686142. doi: 10.3389/fonc.2021.686142
44. Spitz DR, Buettner GR, Petronek MS, St-Aubin JJ, Flynn RT, Waldron TJ, et al. An integrated physico-chemical approach for explaining the differential impact of FLASH versus conventional dose rate irradiation on cancer and normal tissue responses. Radiother Oncol (2019) 139:23–7. doi: 10.1016/j.radonc.2019.03.028
45. Abolfath R, Grosshans D, Mohan R. Oxygen depletion in FLASH ultra-high-dose-rate radiotherapy: A molecular dynamics simulation. Med Phys (2020) 47(12):6551–61. doi: 10.1002/mp.14548
46. Labarbe R, Hotoiu L, Barbier J, Favaudon V. A physicochemical model of reaction kinetics supports peroxyl radical recombination as the main determinant of the FLASH effect. Radiother Oncol (2020) 153:303–10. doi: 10.1016/j.radonc.2020.06.001
47. Lai Y, Jia X, Chi Y. Modeling the effect of oxygen on the chemical stage of water radiolysis using GPU-based microscopic Monte Carlo simulations, with an application in FLASH radiotherapy. Phys Med Biol (2021) 66(2):025004. doi: 10.1088/1361-6560/abc93b
48. Blain G, Vandenborre J, Villoing D, Fiegel V, Fois GR, Haddad F, et al. Proton irradiations at ultra-high dose rate vs. conventional dose rate: Strong impact on hydrogen peroxide yield. Radiat Res (2022). doi: 10.1667/RADE-22-00021.1
49. Fouillade C, Curras-Alonso S, Giuranno L, Quelennec E, Heinrich S, Bonnet-Boissinot S, et al. FLASH irradiation spares lung progenitor cells and limits the incidence of radio-induced senescence. Clin Cancer Res (2020) 26(6):1497–506. doi: 10.1158/1078-0432.CCR-19-1440
50. Yahyapour R, Amini P, Rezapour S, Cheki M, Rezaeyan A, Farhood B, et al. Radiation-induced inflammation and autoimmune diseases. Mil Med Res (2018) 5(1):9. doi: 10.1186/s40779-018-0156-7
51. Najafi M, Motevaseli E, Shirazi A, Geraily G, Rezaeyan A, Norouzi F, et al. Mechanisms of inflammatory responses to radiation and normal tissues toxicity: clinical implications. Int J Radiat Biol (2018) 94(4):335–56. doi: 10.1080/09553002.2018.1440092
52. Wang J, Xu Z, Wang Z, Du G, Lun L. TGF-beta signaling in cancer radiotherapy. Cytokine (2021) 148:155709. doi: 10.1016/j.cyto.2021.155709
53. Acharya MM, Baulch JE, Lusardi TA, Allen BD, Chmielewski NN, Baddour AA, et al. Adenosine kinase inhibition protects against cranial radiation-induced cognitive dysfunction. Front Mol Neurosci (2016) 9:42. doi: 10.3389/fnmol.2016.00042
54. Zhou H, Liu Z, Liu J, Wang J, Zhou D, Zhao Z, et al. Fractionated radiation-induced acute encephalopathy in a young rat model: cognitive dysfunction and histologic findings. AJNR Am J Neuroradiol (2011) 32:1795–800. doi: 10.3174/ajnr.A2643
55. Wirsdörfer F, Jendrossek V. The role of lymphocytes in radiotherapy-induced adverse late effects in the lung. Front Immunol (2016) 1214:7:591. doi: 10.3389/fimmu.2016.00591
56. Campian JL, Ye X, Brock M, Grossman SA. Treatment-related lymphopenia in patients with stage III non-small-cell lung cancer. Cancer Invest (2013) 31:183–8. doi: 10.3109/07357907.2013.767342
57. Davuluri R, Jiang W, Fang P, Xu C, Komaki R, Gomez DR, et al. Lymphocyte nadir and esophageal cancer survival outcomes after chemoradiation therapy. Int J Radiat Oncol Biol Phys (2017) 99(1):128–35. doi: 10.1016/j.ijrobp.2017.05.037
58. Fauquette W, Amourette C, Dehouck MP, Diserbo M. Radiation-induced blood-brain barrier damages: An in vitro study. Brain Res (2012) 1433:114–26. doi: 10.1016/j.brainres.2011.11.022
59. Yuan H, Gaber MW, McColgan T, Naimark MD, Kiani MF, Merchant TE. Radiation-induced permeability and leukocyte adhesion in the rat blood-brain barrier: modulation with anti-ICAM-1 antibodies. Brain Res (2003) 969:59–69. doi: 10.1016/S0006-8993(03)02278-9
60. Jay-Gerin JP. Ultra-high dose-rate (FLASH) radiotherapy: Generation of early, transient, strongly acidic spikes in the irradiated tumor environment. Cancer Radiother (2020) 24(4):332–4. doi: 10.1016/j.canrad.2019.11.004
Keywords: FLASH radiotherapy, conventional dose-rate radiotherapy, mechanism, oxygen, radiobiology
Citation: Lin B, Huang D, Gao F, Yang Y, Wu D, Zhang Y, Feng G, Dai T and Du X (2022) Mechanisms of FLASH effect. Front. Oncol. 12:995612. doi: 10.3389/fonc.2022.995612
Received: 16 July 2022; Accepted: 22 August 2022;
Published: 23 September 2022.
Edited by:
Timothy James Kinsella, Warren Alpert Medical School, Brown University, United StatesReviewed by:
P. Jack Hoopes, Dartmouth College, United StatesCopyright © 2022 Lin, Huang, Gao, Yang, Wu, Zhang, Feng, Dai and Du. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaobo Du, ZHV4aWFvYm8yMDA1QCAxMjYuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.