
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 15 September 2022
Sec. Cancer Epidemiology and Prevention
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.991843
This article is part of the Research TopicEarly Palliative Care for Cancer PatientsView all 11 articles
 Anna Collins1*
Anna Collins1* Vijaya Sundararajan1Brian Le2
Vijaya Sundararajan1Brian Le2 Linda Mileshkin3Susan Hanson4
Linda Mileshkin3Susan Hanson4 Jon Emery5Jennifer Philip1,2,6
Jon Emery5Jennifer Philip1,2,6Background: While multiple clinical trials have demonstrated benefits of early palliative care for people with cancer, access to these services is frequently very late if at all. Establishing evidence-based, disease-specific ‘triggers’ or times for the routine integration of early palliative care may address this evidence-practice gap.
Aim: To test the feasibility of using defined triggers for the integration of standardised, early palliative (STEP) care across three advanced cancers.
Method: Phase II, multi-site, open-label, parallel-arm, randomised trial of usual best practice cancer care +/- STEP Care conducted in four metropolitan tertiary cancer services in Melbourne, Australia in patients with advanced breast, prostate and brain cancer. The primary outcome was the feasibility of using triggers for times of integration of STEP Care, defined as enrolment of at least 30 patients per cancer in 24 months. Triggers were based on hospital admission with metastatic disease (for breast and prostate cancer), or development of disease recurrence (for brain tumour cohort). A mixed method study design was employed to understand issues of feasibility and acceptability underpinning trigger points.
Results: The triggers underpinning times for the integration of STEP care were shown to be feasible for brain but not breast or prostate cancers, with enrolment of 49, 6 and 10 patients across the three disease groups respectively. The varied feasibility across these cancer groups suggested some important characteristics of triggers which may aid their utility in future work.
Conclusions: Achieving the implementation of early palliative care as a standardized component of quality care for all oncology patients will require further attention to defining triggers. Triggers which are 1) linked to objective points within the illness course (not dependent on recognition by individual clinicians), 2) Identifiable and visible (heralded through established service-level activities) and 3) Not reliant upon additional screening measures may enhance their feasibility.
Patients with advanced cancer suffer numerous distressing physical symptoms, psychological morbidity and unmet information and psychosocial needs (1–4). Despite assigning high priority to symptom relief, open communication and collaborative decision making (5), such needs are frequently not recognised nor managed in routine oncology care (6, 7).. Addressing these needs are core tasks of palliative care, and increasingly meta-analyses demonstrate the benefits of early palliative care for patients, including improved symptom management, quality-of-life and care satisfaction; reduced rates of hospitalization and emergency department presentations, and for family carers, improved quality-of-life and care satisfaction (8–13).
Despite benefits and recommendations from peak professional bodies (ASCO, ESMO) (14–16), in practice ‘early’ palliative care referrals are not routine and access to palliative care frequently occurs very late in the illness course (17). Our earlier work demonstrated only 59% of decedents with metastatic non-small cell lung, small cell lung, prostate and breast cancers in Victoria, Australia received a palliative approach to care, a median of 27 days prior to death (17). A repeat of these analyses (almost 10 years on) for decedents from cancer in 2018 revealed 67% had a palliative care referral, but at a later time, median 20 days before death (18). Equivalent data on cancer decedents from the United Kingdom (19) and other international jurisdictions demonstrated palliative care referral 53 days and 18.9 days prior to death respectively (20). As such, there remains a significant evidence-practice gap associated with the implementation of early palliative care in routine cancer care.
Barriers to palliative care referral have been identified, including: concerns about difficulty of referral, fear of destroying patient hope associated with perceptions of palliative care (21) and uncertainty over the ‘best time’ to refer (22). The literature has variably defined ‘early’, including to mean at least 3-4 months prior to death to confer benefits (8), within 3 months of advanced cancer diagnosis for patients with a life expectancy of 1 year or less (23), and ideally engagement with palliative care spanning 6-18 months before death (24).
An approach which seeks to standardise the timing of ‘early’ palliative care referral would do much to overcome such barriers, including through increasing patient acceptance of referrals, as it represents a ‘routine’ care pathway (25). Similarly, standardisation would reduce variations and inequities in access to care. Such a standardised time of introduction should be based on evidence and be tailored to the disease characteristics and likely history, allowing for consideration of balancing the potential for maximal outcome benefit versus managing the volume of early consultations and resourcing implications (23, 24). Yet to date, few studies have explored the role of systematic triggers for timely palliative care referral (26–29).
We previously examined population level hospital admission datasets to map health care use by patients with high grade glioma (HGG) and metastatic breast, prostate as well as lung cancers (17, 30–32). This work demonstrated potential disease-specific transition points in the illness course which heralded subsequent poor prognosis (defined as less than 6 months) and subsequent increased health service utilisation (17). These ‘transition points’ or ‘triggers’ represented times for the integration of early palliative care as part routine clinical practice when we recommended that palliative care should be routinely introduced, if not already in place, to maximise patient and carer benefit (33). These triggers for palliative care are linked with electronic health records or usual systems of clinical care, may prompt clinicians and in this way, serve to augment clinician-based decision making (24). However, there is a clear need for the testing of such cancer specific time points as triggers for referral to palliative care occurring as ‘standard quality care’ (17).
Responding to this gap, we undertook a randomised, phase 2 feasibility trial of a standardised outpatient model of ‘early’ palliative care [Standardised Early Palliative Care: STEP Care] for advanced cancer patients and their family carers, with referrals occurring at the defined disease-specific, evidence-based trigger points. The trial sought to test the feasibility and preliminary efficacy of using defined triggers for the the integration of standardised, early palliative (STEP) care across three advanced cancers. This paper reports on the feasibility of triggers.
The trial was undertaken at four metropolitan tertiary cancer services in Melbourne, Victoria, each with active inpatient and outpatient palliative care consultation services. Central multi-site ethical approval was provided by the Human Research Ethics Committee at St Vincent’s Hospital Melbourne [HREC 179/16], and the trial registered with the Australian and New Zealand Clinical Trial Registry [ACTRN12617000534381]. Funding was provided by the Victorian Cancer Agency [Grant number: HSR15022] and the St Vincent’s Hospital Foundation (private philanthropic donation).
The trial had patient and public involvement embedded within the research team (SH), and additionally through the guidance of an advisory group comprising community contributors who met regularly with the research team (quarterly meetings) across the life of the trial. This group had a significant role in shaping the following areas: grant application, review of patient consent forms and plain language summary, review of language to introduce the study, input into selection of research outcomes and qualitative question guides, trouble-shooting recruitment, and grounding interpretation of study results.
The primary outcome was the feasibility of using triggers for times of integration of STEP Care, with a view to proceeding to a definitive Phase 3 randomised trial, which would evaluate effectiveness of STEP Care (compared to usual best practice cancer care) for patients with advanced breast or prostate cancer or high grade glioma (HGG). The specific feasibility endpoint was defined as enrolment of at least 30 patients in each disease cohort (total n=90) in 24 months, at which time those cancers not meeting feasibility cut off were ceased. Secondary aims to examine the preliminary efficacy of STEP Care on patient- and carer- reported outcomes, including quality of life, mood, symptoms, illness understanding, and overall survival will be reported elsewhere. Consistent with the exploratory study aims, the feasibility endpoint was determined by the authors primarily balancing pragmatic considerations around the available study timeframe. It was consistent with other phase II studies of this nature (34) and also considered the minimum sample required to determine a preliminary estimate of effect size for secondary patient-reported outcomes which would be the subject of a future phase III definitive trial.
We conducted a phase 2, multi-site, open-label, parallel-arm, Randomized Controlled Trial (RCT) of usual Best Practice Cancer Care +/- STEP Care according. This RCT development aligned with the Medical Research Council (MRC) Framework for the development and testing of Complex Interventions (35, 36) which prioritises phased, sequential, intervention development leading towards implementation (35, 36). The nature and timing of the triggered early palliative care was thus underpinned by our exploratory data resulting from Phase 1 qualitative (22, 37–39) and health service use studies (17, 30, 31, 40) which defined transition points or triggers for the integration of early palliative care.
The triggers for STEP Care as defined for this feasibility trial included (Table 1): for prostate- first multiday admission where patient had any metastatic disease; for breast- first multiday admission where patient had metastatic disease including at least one visceral site; for brain- any hospital presentation with first recurrence of HGG (determined by radiological or surgical evidence). Given our earlier state-wide population cohort studies of cancer decedents found first palliative care occurred a median of <30 days prior to death (17, 18), these triggers were selected to offer an objective time for systematic identification of a cohort likely to benefit from palliative care earlier in the disease trajectory.
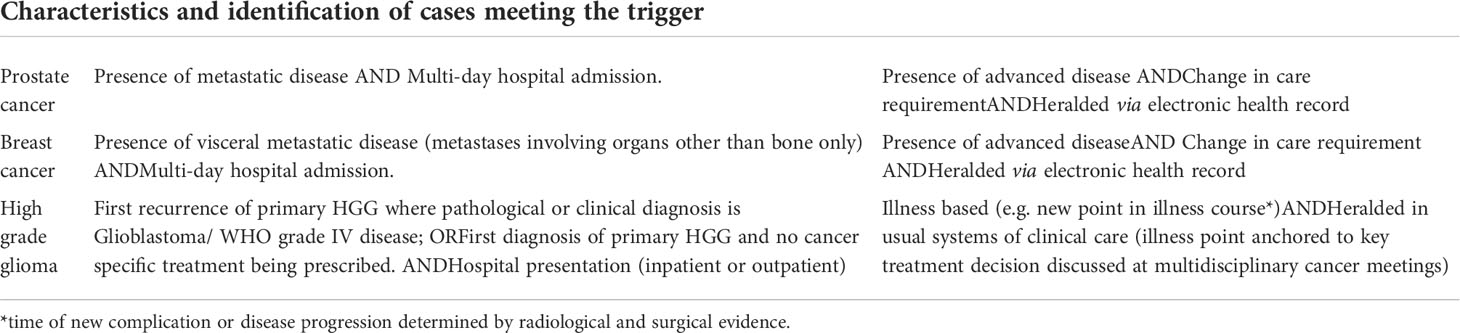
Table 1 Trigger definitions.
The point of hospitalisation with the disease characteristics outlined was selected because it was: not reliant upon individual clinician judgement of prognosis or of the person’s needs; common to most patients with these cancer illnesses; and could be identified within the electronic health record. An anticipated life expectancy of between 6 and 24 months has been advocated as appropriate for patient inclusion in early palliative care (24, 41). These points of hospitalization were previously found in our population studies to have a median survival of approximately 6 months (42), thus balancing the imperatives for early palliative care input against common service concerns about capacity to respond (41) and relevant to the variable and not infrequently long metastatic illness course experienced particularly by the breast and prostate cohorts.
Participants included adult patients with advanced breast, prostate and brain cancers as identified by the defined triggers (Table 1), and in attendance at the included hospital sites at this time. Further eligibility requirements included the ability to provide informed consent, to comply with study procedures, and an ability to understand written and spoken English. Exclusion criteria for patients included those less than 18 years, those previously seen by hospital consultancy palliative care services within the previous 12 months or presenting with needs required urgent palliative care review, or those who were more than 30 days following the identified cancer-specific trigger. Patients meeting the eligibility criteria who were identified by a mechanism other than the route specified (Table 1) could be included in the study, however none were referred in this way.
Consecutive eligible inpatients and outpatients from participating cancer treatment centres were approached for potential study inclusion by research staff. At patient identification, clinical teams were asked to confirm eligibility, permission was sought from the patient to provide information about the study, with those willing to proceed completing a study consent form. Information on eligibility along with reasons for refusal to participate were recorded.
Patient-level randomisation was centralised and coordinated by an independent Trial Coordinator. The randomisation schedule involved 1:1 allocation and used the minimisation method to ensure a balanced distribution between groups with respect to the patient’s tumour type and hospital site.
All patients received usual oncological care through their health care providers, including systemic therapy, radiotherapy, surgery or other treatments deemed appropriate. In addition, those patients randomised to usual care were able to be referred to palliative care services at any time at the treating clinician’s discretion.
Those patients randomised to the intervention arm received STEP Care in addition to Standard Best Practice Cancer Care. STEP Care consisted of, at minimum, monthly Palliative Care consultations for at least 3 months. These consultations were primarily delivered in the outpatient setting. All STEP Care consultations were conducted by a Palliative Care Physician or Specialist Nurse and involved a series of activities (Table 2) which were documented according to a framework adapted from the PC-NAT-PD (43).
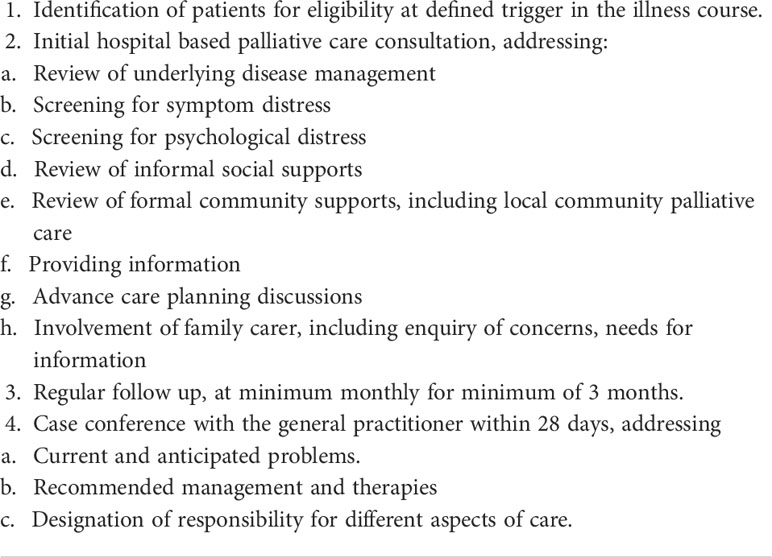
Table 2 Key components of STEP Care intervention.
Demographic, clinical, and treatment data were collected from patient medical records. Mixed method study data were collected to assess the feasibility and acceptability of the triggers as prompting referral to the standardized early palliative care intervention. Measures of feasibility were assessed according to the number of eligible participants identified, consented and completing the study. Acceptability of the STEP Care intervention was assessed according to the number of withdrawals from the study, the completeness of delivery and timing of STEP care consultations for those assigned to the intervention arm, and the development of any adverse events. In addition, semi structured qualitative data with providing perspectives of purposively sampled participating oncology and palliative care clinicians, was supplemented to explore issues of feasibility and acceptability associated with using triggers for the integration of early palliative care.
Feasibility outcomes were summarised using descriptive statistics, including frequency counts and percentages (categorical variables), and mean/standard deviation or median/interquartile range (continuous variables) as appropriate. Qualitative data aligned to the primary outcome of feasibility and acceptability was subjected to a thematic analysis (44) to supplement the basic descriptive analyses consistent with the study aims.
Of 513 patients identified as meeting the cancer-specific trigger point (141 brain, 118 prostate, 254 breast), 406 were not eligible to approach for study participation (58 brain, 106 prostate, 242 breast), most commonly owing to already being linked into palliative care (n=183, 45%), or presenting with needs requiring immediate referral to palliative care (n=71, 18%), or cognitive impairment (n=42, 10%) (Table 3). Of the 107 patients identified as eligible, 42 (39%) declined study participation, mostly citing they were not interested at this time (23, 55%) as opposed to high levels of distress (n=3, 7%), or the time commitment involved (n=2, 5%). The remaining 65 (61%) participants were consented for study participation and underwent random assignment.
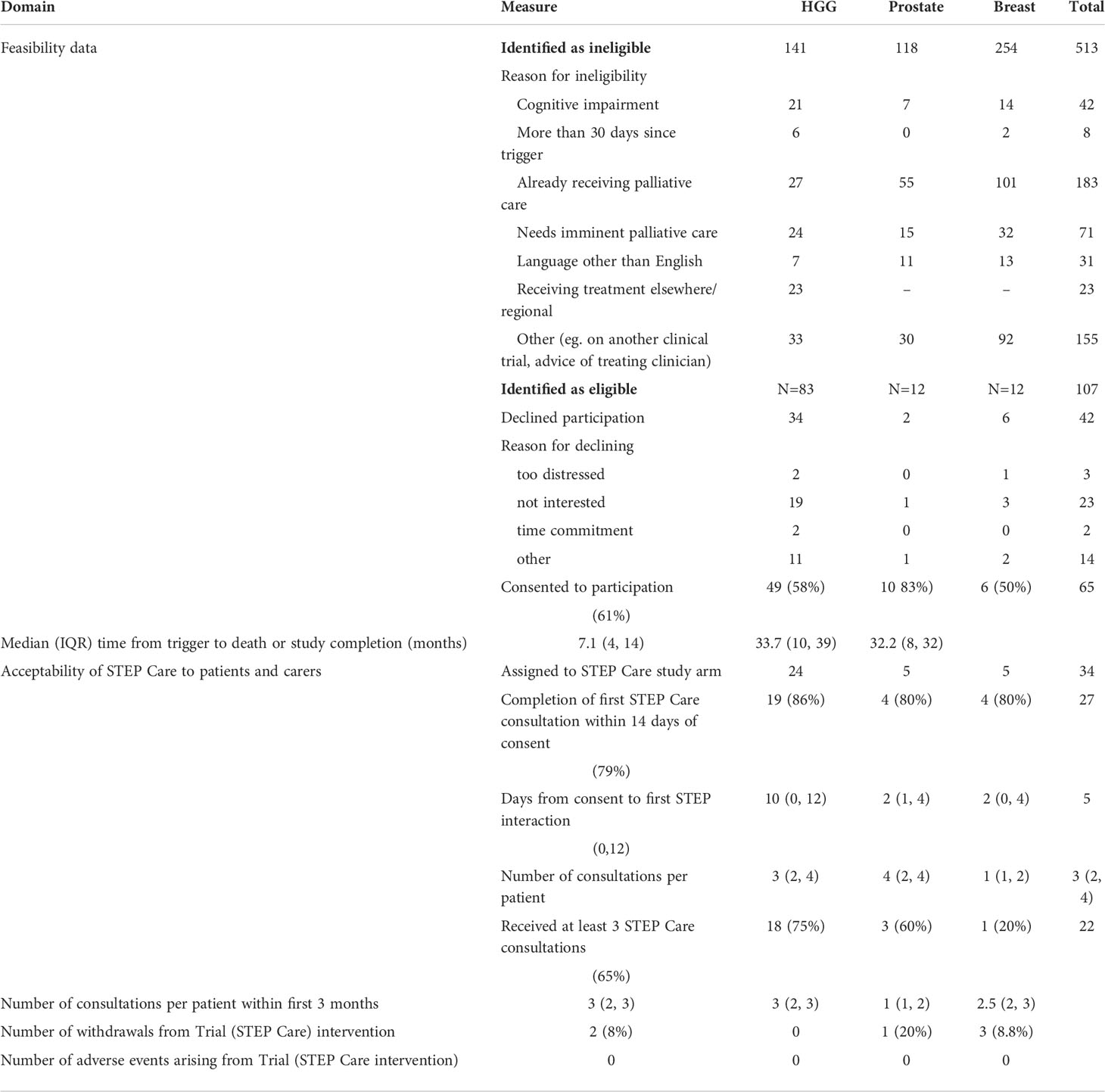
Table 3 Feasibility and acceptability data.
Interview and focus group data was obtained from oncology and palliative care clinicians (n=19) who were directly or peripherally involved in the STEP care trial as a member of the treating teams involved in the care of included breast, prostate or brain cancer patients. This included perspectives from palliative care nurses (n=3) and consultants (n=6), and oncology nurses (n=3) and consultants (n=7).
The triggers underpinning times for the integration of standardised, early palliative care (STEP care) were shown to be feasible for brain, but not breast or prostate cancers, with total enrolment of 49, 6 and 10 patients across the three disease groups respectively. The breast and prostate groups were determined not feasible and ceased at the pre-specified 24 month timeframe, with recruitment for the brain cohort (then n=38) continuing through to 36 months.
The cancer specific triggers used in this trial appeared to be ‘too late’ for the breast and prostate groups, with high rates of these participants identified already having a previous palliative care referral (breast: 101/254, 40%; prostate: 55/118, 47%) as compared to the brain group (27/141, 20%), and additional breast (32/254, 13%) and prostate (15/118, 13%) cancer patients identified as having urgent palliative care needs. These data suggest earlier involvement may have been helpful.
“If there’s been an admission in the setting of metastatic disease that can often mean that there are symptoms and they’re not doing so well at home and (we) get the palliative care team involved” (Oncology consultant)
“Many of the patients (breast, prostate) have been seen by palliative care already” (Palliative care nurse)
On the other hand, the median overall survival of the cohort from the identified trigger until death or censored at study completion was 9 months (Figure 1). The median follow-up time from the trigger was: for brain 7.1 (4.1, 14.1) months, for breast 32.15 (8.4, 32.4) months, and for prostate 33.65 (10.3, 39.4) months. This suggests the triggers were aligned with a period where a person is likely to benefit from palliative care, and highlights the resourcing challenge in groups such as breast and prostate where a person may experience palliative care needs over a long metastatic illness course.
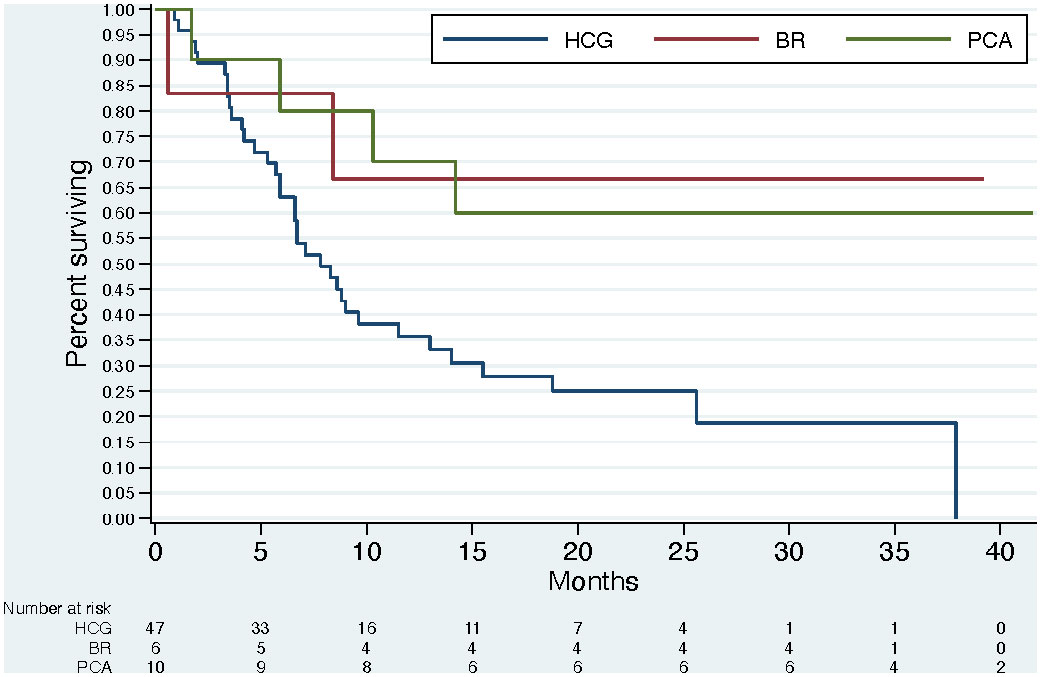
Figure 1 Overall Survival by Cancer Type.
The feasible trigger associated with care of the brain cancer cohort was illness based (e.g. at time of new progressive disease or a new complication of the illness) and heralded in usual clinical systems of care (anchored to key treatment decision discussed at multidisciplinary cancer meetings). The ‘not feasible’ triggers of breast and prostate cancer care were at a time of advanced illness (though not necessarily a new development of progressive disease or complication), when care requirements changed and required screening of the electronic health medical records to identify patients.
Qualitative data from clinicians revealed that electronic medical records within the included hospital settings were not yet established for real time prompting of eligible patients. This was largely because relevant data such as the cancer diagnosis that may be uncovered within the admission and recorded in the patient’s electronic health record was only ‘coded’ by hospital administrative teams following the patient discharge. This meant that administrative teams could not generate an automatic list of ‘eligible’ patients meeting the identified trigger in real time, which reduced the feasibility for breast and prostate triggers since it therefore required usual care teams to additionally screen inpatients for eligibility. This was compared to the brain patient cohort, where the trigger was anchored to a new illness development which prompted discussion in usual clinical care systems – specifically the multidisciplinary cancer team meeting. For brain patients, no additional surveillance over and above usual care processes was required to identify people meeting eligibility.
“Having an easy mechanism of referral is really important … I think there’s particular patients when we’ve got some big life decisions to discuss at our M.D.M, that would be a good time to bring in palliative care” (Surgical Oncology – Urology)
“I think it provides a standardised pathway that you can offer to patients, and an easy access pathway … and it keeps it at the front of your mind.” (Oncology nurse)
Of the 65 participants, 34 were assigned to receive the STEP Care Intervention (24 brain, 5 breast, 5 prostate). Of these, 27 (79%) completed the first consultation within 14 days as per protocol, a median (IQR) of 5 days (0, 12) following identification and consent (Table 3), suggesting the responsiveness of the palliative care teams who were able to facilitate an initial review within the planned timeframe. Most patients (22, 65%) received a ‘minimum dose’ of 3 (monthly) consultations as prescribed, with a median (IQR) of 3 (2, 4) consultations per patient across the study period. These data suggest that the timing of the trigger was broadly acceptable to patients who continued to attend appointments. Of note, there were 3 patients (9%) who withdrew from the STEP Care intervention due to increasing illness burden, and no adverse events recorded.
The triggers also appeared to be acceptable to clinicians who described standardization of practices around referral to palliative care referral as reassuring to both themselves and the patients.
“It (the trigger) gives permission to refer people and it is normalised under the medical pathway … I think. the formality … gives it a much more medical procedural thing rather than an esoteric, nebulous sort of thing … by having the defined (trigger) points” (Oncology consultant)
“Before. it was difficult because … I felt I needed … some problem to be able to put in that referral. Whereas having a trigger allows us to be able to much more fluidly, you know, send through that referral.” (Oncology nurse)
“The key you know, (having) flags that teams can recognise as a point for a referral as opposed to … where it could be a bit more subjective. These clear kind of delineated flags for a referral … certainly gets our foot in the door with a lot of patients earlier” (Palliative care consultant)
Having a trigger also meant that conversations around referral to palliative care were easier.
“I think something like this for a junior clinician nurse, it gives them something tangible that they can open the discussion with” (Oncology consultant)
“There’s none of that having to break through the barrier of, you know, referring to pall care. It’s just an automatic thing so there’s no barrier to break because it happens all the time anyway.” (Oncology nurse)
For most patients, clinicians perceived the 3 consultations delivered at time of the trigger was adequate to introduce the role of early pc, put some key plans in place, help with family discussions, and facilitate relationships so that subsequent contact could be initiated by the patient or their carer if and when the need arises.
“…It’s really good to have that concurrent pathway where we can link patients in from an early point,…As things progress it makes things much easier when you get further down the line as well, in terms of having them already linked in, knowing what services are available and making that transition.” (Oncology Consultant)
“some (patients) at those earlier stages … may have a significant survival trajectory still but have other potential symptoms or things that could be managed in the interim period of time … so they’re not getting to the end stage before being referred” (Palliative Care Consultant)
Similarly for palliative care clinicians, having triggers was perceived as a means to build relationships between palliative care and referring teams that enabled the longer term care of patients to be met. In this way, the triggers were seen as providing patients with a universal opportunity to be linked with palliative care.
“Although there’s lots of rhetoric about taking a population-based approach to palliative care, when you are constrained by resources, you retreat and do what you just have to do to manage, don’t you. So, I think this has been really positive in helping us look at these specific groups, and it’s increased out dialogue with our referrers.”(Palliative Care Consultant)
As noted, the defined triggers for prostate or breast cancer patients were not useful since many patients were already linked to palliative care services, or already had high supportive care needs identified which had prompted earlier referral.
“I think just maybe having a look at the (trigger) points and just seeing umm how, if there’s certain groups that are coming in … too late. And then just revising those.” (Palliative Care Consultant)
Other staff highlighted that while having a trigger was useful for some patients, the circumstances of other patients necessitated the need for flexibility around timing of palliative care referral.
“I tend to tailor it per patient rather than having an automatic criteria for which I would refer someone because I just think everyone’s very individual.” (Surgical oncology)
Similarly, triggers were sometimes seen as interfering with practices of a staged approach to the introduction of palliative care or the providers ‘clinical intuition’ regarding the right time.
“I don’t think right now is the best time for me to … refer to palliative care. But, you know, as weeks go on and they settle in, you develop—we develop, as nurses and clinicians there, the best way of knowing what is the right time to introduce it.” (Cancer nurse)
Identifying the cohort of people who will benefit from palliative care and enacting this access in a timely manner requires new approaches in service delivery. This trial tested the feasibility of novel, evidence-based, cancer-specific, illness-based triggers for the integration of standardized early palliative care across three advanced cancer groups. The triggers as defined were shown feasible by our endpoint for the brain but not prostate or breast cancer groups. Achieving the implementation of early palliative care as a standardized component of quality care for all oncology patients will require attention to further defining triggers which can help reduce variation and enhance the equity of care. In this trial the successful trigger was characterized by being 1) linked to objective points within the illness course at a new development in the illness (thus, not dependent on recognition by individual clinicians), 2) Identifiable and visible (heralded through established systems of clinical care or service-level activities) and 3) Not reliant upon additional screening measures. While these are early data in the field, these characteristics are likely to be important to inform the development of feasible triggers going forward.
In this study, and others (45) we have sought through exploring triggers to test a universal approach to identifying the group of people who may benefit from palliative care. A handful of other single-centre studies have similarly examined models of ‘triggered palliative care consultation’, often also initiated on criteria involving hospitalisation, and these have reported variable outcomes (26, 27, 29). Adelson and colleagues used a hybrid of automatic criteria relating to health service use (prior hospital within 30 days; or > 7 bed days) and active symptoms for prompting palliative care referral, resulting in a two-fold increase in rates of consultation and a significant reduction of hospital re-admission (26). Rocque and colleagues demonstrated improved illness understanding following implementation of triggered palliative care for all hospitalised cancer patients with metastases, but this resulted in a minimal impact upon patient-reported symptoms, hospice utilisation, and cost of care (29). DiMartino and colleagues reported triggered palliative care for hospitalized solid tumour and gynecologic patients increased uptake, but this did not result in earlier timing of consultations (27).
Our approach to standardizing early palliative care differed in that it sought to test the feasibility of cancer specific triggers to initiate a prescribed palliative care intervention, which was then delivered in outpatient settings. The triggers, defined upon pre-identified health service parameters, differed for different cancers, and thus meant our results also reflected some nuance in the understanding of different cancer types and the feasibility of the respective triggers. In this way we have begun to define those characteristics of a successful trigger and also of those not likely to be successful. In this trial, a successful trigger was linked to a clear, new development in the illness, was identifiable and heralded in usual service systems, and did not rely on additional screening. Since the characteristics of services differ, local factors will necessarily inform the implementation of such a trigger into routine practice. The views of the referrers as to the acceptability of the trigger as point of referral to palliative care will be essential, with a successful trigger one that reflects and is adapted to local service conditions and agreed upon by referrers.
In the context of this clinical trial, with necessarily tight eligibility parameters, the triggers enacted for prostate and breast cancer were shown to be not feasible, or ‘too late’. This was largely reflecting the high number of people already receiving, or needing imminent palliative care at the identified trigger, thus rendering them ineligible in the clinical trial context. Despite this, it was interesting that our survival data on the participants in these cohorts, albeit small numbers, was broadly consistent with the literature recommending palliative care input for those with a life expectancy of 6-24 months (24, 41). Going forward in clinical practice and outside of a trial setting, this may suggest that these trigger points as outlined are not unreasonable as a ‘minimum standard’ to prompt the initiation of palliative care if not already in place. Alternatively, these triggers could be adapted to earlier in the disease course, such as at the time of second line treatment. In this case, these triggers could be linked to identification via the systems whereby care is reviewed such as in the multi-disciplinary cancer meeting. Preliminary pilot testing, as undertaken here, would first be required to establish feasibility.
An alternative approach to using triggers, is to instead focus palliative care referral prompted by needs, with those identified as having greater or complex needs receiving specialist palliative care (46, 47). Such an approach seeks to target the limited resources of palliative care upon those who may benefit most, and is based in a population-centred model. The concept of ‘complexity’ at the centre of this approach however is not well defined (48). Furthermore, in order for referral of those with complex needs to occur, an assessment of needs by referring clinicians must take place. Such an assessment is frequently not part of their usual consultation, is not built into usual workflows and would constitute an additional task in an already busy consultation. As such it may be overlooked. Even when such needs are assessed, acting upon these does not occur routinely for many patients (7, 49).
Hui et al. (24) have attempted to bring this discussion of triggers and needs together in a service innovation which seeks to apply routine systematic screening, an established defined set of referral criteria which, if reached, triggers a referral to palliative care for appropriate patients. In addition an adequately staffed outpatient specialist palliative care service is available to respond to these referrals (24). In this way standardisation of practice is achieved with attendant equity of access for patients, but focused on those with greatest needs who may most benefit. The resources required for the systematic screening and implementation in this model will not however, be available in a number of centres.
Our focus on using triggers which may be built into usual care systems offers an approach which also will standardise the time of referral and address issues of equity of access. The opportunity to automate these triggers based in electronic systems associated with electronic medical records means fewer resources are required to standardise identification of the patient cohort. An electronic prompt to clinicians could serve as a reminder, reducing clinical uncertainty and reinforcing the service expectations (24). Clinicians, so prompted, could consider their response which may include consideration of activities of palliative care such as review of symptom burden, or discussion of goals and preferences, or it may include a referral to specialist palliative care. A system using electronic prompts needs to be as accompanied by clearly communicated but not overly prescriptive guidance, thus reducing uncertainty whilst not reducing physician agency (50). An effective trigger-prompt system would be one where clinicians are reminded of palliative care benefits and retain the decision making about how and when those are best enacted.
There are limitations to this trial that require mention, including a focus on those patients who were cared for in large cancer centres (where neuro-oncology units exist) and who may not be representative of all cancer patients. Similarly those people who did not speak English were excluded - a group which constitutes up to 21% of the Australian population (51). Furthermore our study was around the feasibility of using triggers for a trial of early palliative care, not simply referral to palliative care for all comers. As such, the eligibility criteria to enter the trial were likely to rule out some patients that may otherwise have welcomed (or benefited from) palliative care referral. This includes some participants excluded based on other clinical trial participation. Given the increasing potential for many patients to be accessing clinical trials of novel systemic therapies moving forward, future early palliative care trials may need to carefully consider this parameter, which will likely substantially reduce the available sample who may otherwise benefit from early palliative care. Nonetheless, by structuring the feasibility of triggers as time for referral within a trial, we were able to measure outcomes in a standardized formal manner including delivery and acceptability. We recognise that there are many parameters which impact upon feasibility and acceptability outcomes and our trial necessarily chooses selected measures likely not capturing all of these attendant influences.
We contend that key to the implementation of early, timely palliative care into clinical care is the development of novel ways of identifying the cohort of people who will benefit. The use of triggers offers an approach which provides standardization of the cohort identification and therefore will reduce variation and enhance equity of access to early palliative care. Characteristics of a successful trigger are that it is linked to a clear, new development in the illness, is identifiable and heralded in usual service systems and does not rely on additional screening. Future research focused upon linking these triggers to electronic clinical prompt systems offers interesting ways forward. The need to tailor the triggers and attendant responses to local conditions will be core to successful implementation endeavours.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The trial involving human participants was reviewed and approved by St. Vincent’s Hospital Melbourne HREC. All participants provided their written informed consent to participate in this study.
JP was the lead investigator and obtained the study funding. JP & AC were responsible for the study conduct, had access to the data, and co-authored the first draft. All authors contributed to the study protocol, interpretation and, contributed to the manuscript.
Funding was provided by the Victorian Cancer Agency [Grant number: HSR15022] and the St. Vincent’s Hospital Foundation (private philanthropic donation).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chang VT, Hwang SS, Feuerman M, Kasimis BS, Thaler HT. The memorial symptom assessment scale short form (MSAS-SF). Cancer (2000) 89(5):1162–71. doi: 10.1002/1097-0142(20000901)89:5<1162::AID-CNCR26>3.0.CO;2-Y
2. Hwang SS, Chang VT, Cogswell J, Alejandro Y, Osenenko P, Morales E, et al. Study of unmet needs in symptomatic veterans with advanced cancer: incidence, independent predictors and unmet needs outcome model. J Pain Symptom Manage (2004) 28(5):421–32. doi: 10.1016/j.jpainsymman.2004.02.023
3. Gattellari M, Voigt KJ, Butow PN, Tattersall MHN. When the treatment goal is not cure: are cancer patients equipped to make informed decisions? J Clin Oncol (2002) 20(2):503–13. doi: 10.1200/JCO.2002.20.2.503
4. Girgis A, Breen S, Stacey F, Lecathelinais C. Impact of two supportive care interventions on anxiety, depression, quality of life and unmet needs in patients with nonlocalized breast and colorectal cancers. . J Clin Oncol (2009) 27(36):6180–90. doi: 10.1200/JCO.2009.22.8718
5. Steinhauser KE, Christakis NA, Clipp EC, Mcneilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians and other care providers. JAMA (2000) 284(19):2476–82. doi: 10.1001/jama.284.19.2476
6. Seow H, Sussman J, Martelli-Reid L, Pond G, Bainbridge D. Do high symptom scores trigger clinical actions? an audit after implementing electronic symptom screening. J Oncol Pract (2012) 8(6):e142–e48. doi: 10.1200/JOP.2011.000525
7. Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom monitoring with apteint-reported outcomes during routine cancer treatment: A randomized controlled trial. J Clin Oncol (2015); 34(6):557–65. doi: 10.1200/JCO.2015.63.0830
8. Davis MP, Temel JS, Balboni T, Glare P. A review of the trials which examine early integration of outpatient and home palliative care for patients with serious illnesses. Ann palliative Med (2015) 4(3):99–121. doi: 10.3978/j.issn.2224-5820.2015.04.04
9. Fulton JJ, LeBlanc TW, Cutson TM, Porter Starr KN, Kamal A, Ramos K, et al. Integrated outpatient palliative care for patients with advanced cancer: a systematic review and meta-analysis. Palliative Med (2019) 33(2):123–34. doi: 10.1177/0269216318812633
10. Gaertner J, Siemens W, Meerpohl JJ, Antes G, Meffert C, Xander C, et al. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: systematic review and meta-analysis. bmj (2017) 357:j2925. doi: 10.1136/bmj.j2925
11. Haun MW, Estel S, Rücker G, Friederich HC, Villalobos M, Thomas M, et al. Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev (2017) 6:CD011129. doi: 10.1002/14651858.CD011129.pub2
12. Hoerger M, Wayser GR, Schwing G, Suzuki A, Perry LM. Impact of interdisciplinary outpatient specialty palliative care on survival and quality of life in adults with advanced cancer: a meta-analysis of randomized controlled trials. Ann Behav Med (2019) 53(7):674–85. doi: 10.1093/abm/kay077
13. Kavalieratos D, Corbelli J, Zhang D, Dionne-Odom JN, Ernecoff NC, Hanmer J, et al. Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA (2016) 316(20):2104–14. doi: 10.1001/jama.2016.16840
14. Davis MP, Temel JS, Balboni T, Glare P. A review of the trials with examine early integration of outpatient and home palliative care for patients with serious illnesses. Ann Palliative Med (2015) 4(3):99–121. doi: 10.3978/j.issn.2224-5820.2015.04.04
15. Smith TJ, Temin S, Alesi ER, Abernathy AP, Balboni T, Basch E, et al. American Society of clinical oncology provisional clinical opinion: the integration of palliative care into standard oncology care. J Clin Oncol (2012) 30(8):880–87. doi: 10.1200/JCO.2011.38.5161
16. (ANZSPM) TANZSoPM. Timely referral to specialist palliative care services for patients with progressive solid tumours. Australia: Australian and New Zealand Society for Palliative Medicine (2014).
17. Collins A, Sundararajan V, Burchell J, Millar J, McLachlan S-A, Krishnasamy M, et al Transition points for the routine integration of palliative care in patients with advanced cancer. J Pain symptom Manage (2018) 56(2):185–94. doi: 10.1016/j.jpainsymman.2018.03.022
18. Philip J, Collins A, Warwyk O, Sundararajan V, Le B. Is the use of palliative care services increasing? a comparison of current versus historical palliative care access using health service datasets for patients with cancer. Palliat Med (2022) 24:2692163221118205. doi: 10.1177/02692163221118205
19. Allsop MJ, Ziegler LE, Mulvey MR, Russell S, Taylor R, Bennett MI. Duration and determinants of hospice-based specialist palliative care: A national retrospective cohort study. Palliative Med (2018) 32(8):1322–33. doi: 10.1177/0269216318781417
20. Jordan RI, Allsop MJ, ElMokhallalati Y, Jackson CE, Edwards HL, Chapman EJ, et al. Duration of palliative care before death in international routine practice: a systematic review and meta-analysis. BMC Med (2020) 18(1):1–25. doi: 10.1186/s12916-020-01829-x
21. Collins A, McLachlan S-A, Philip J. Initial perceptions of palliative care: An exploratory qualitative study of patients with advanced cancer and their family caregivers. Palliative Med (2017) 31(9):825–32. doi: 10.1177/0269216317696420
22. Le B, Mileshkin L, Doan K, Saward D, Spruyt O, Yoong J, et al. Acceptability of early integration of palliative care in patients with incurable lung cancer. J Palliative Med (2014) 17(5):553–58. doi: 10.1089/jpm.2013.0473
23. Hui D, Mori M, Watanabe SM, Caraceni A, Strasser F, Saarto T, et al. Referral criteria for outpatient specialty palliative cancer care: an international consensus. Lancet Oncol (2016) 17(12):e552–e9. doi: 10.1016/S1470-2045(16)30577-0
24. Hui D, Heung Y, Bruera E. Timely palliative care: Personalizing the process of referral. Cancers (Basel) (2022) 14(4):1047. doi: 10.3390/cancers14041047
25. Philip J, Collins A. Routine integration of palliative care: what will it take? Med J Aust (2015) 203(10):385. doi: 10.5694/mja15.00994
26. Adelson K, Paris J, Horton JR, Hernandez-Tellez L, Ricks D, Morrison RS, et al. Standardized criteria for palliative care consultation on a solid tumor oncology service reduces downstream health care use. J Oncol Pract (2017) 13(5):e431–e40. doi: 10.1200/JOP.2016.016808
27. DiMartino LD, Weiner BJ, Hanson LC, Weinberger M, Birken SA, Reeder-Hayes K, et al. The impact of two triggered palliative care consultation approaches on consult implementation in oncology. Healthcare (Amst). (2019) 7(1):38–43. doi: 10.1016/j.hjdsi.2017.12.001
28. Gemmell R, Yousaf N, Droney J. "Triggers" for early palliative care referral in patients with cancer: a review of urgent unplanned admissions and outcomes. Support Care Cancer (2020) 28(7):3441–9. doi: 10.1007/s00520-019-05179-0
29. Rocque GB, Campbell TC, Johnson SK, King J, Zander MR, Quale RM, et al. A quantitative study of triggered palliative care consultation for hospitalized patients with advanced cancer. J Pain symptom Manage (2015) 50(4):462–9. doi: 10.1016/j.jpainsymman.2015.04.022
30. Sundararajan V, Bohensky MA, Moore G, Brand CA, Lethborg C, Gold M, et al. Mapping the patterns of care, the receipt of palliative care and the site of death for patients with malignant glioma. J Neurooncology (2014) 116(1):119–26. doi: 10.1007/s11060-013-1263-7
31. Philip J, Hudson P, Bostanci A, Street A, Horey DE, Aranda S, et al. Metastatic non-small cell lung cancer: a benchmark for quality end-of-life cancer care? Med J Aust (2015) 202(3):139–43. doi: 10.5694/mja14.00579
32. Hudson P, Trauer T, Kelly B, O'Connor M, Thomas K, Summers M, et al. Reducing the psychological distress of family caregivers of home-based palliative care patients: long-term effects from a randomised controlled trial. Psycho-Oncology (2014); 24(1):19–24. doi: 10.1002/pon.3610
33. Collins A, Sundararajan V, Philip J. Transition points for the routine integration of palliative care in patients with advanced cancer. J Pain Symptom Manage (2018) 56(2):185–94. doi: 10.1016/j.jpainsymman.2018.03.022
34. Dhollander N, Smets T, De Vleminck A, Lapeire L, Pardon K, Deliens L. Is early integration of palliative home care in oncology treatment feasible and acceptable for advanced cancer patients and their health care providers? a phase 2 mixed-methods study. BMC Palliat Care (2020) 19(1):174. doi: 10.1186/s12904-020-00673-3
35. Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. Br Med J (2000) 321(7262):694. doi: 10.1136/bmj.321.7262.694
36. Moore GF, Audrey S, Barker S, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions. medical research council. Br Med J (2015) 350:h1258. doi: 10.1136/bmj.h1258
37. Collins A, Lethborg C, Brand C, Gold M, Moore G, Sundararajan V, et al. The challenges and suffering of caring for people with primary malignant glioma: qualitative perspetives on improving current supportive and palliative care practices. BMJ Supportive Palliative Care (2014) 4(1):68–76. doi: 10.1136/bmjspcare-2012-000419
38. Philip J, Collins A, Brand C, Gold M, Moore G, Sundararajan V. Health care professionals' perspectives of living and dying with primary malignant glioma: Qualitative implications for a unique cancer trajectory. Palliative Supportive Care (2013) 13(6):1519–27. doi: 10.1017/S1478951513000576
39. Philip J, Collins A, Brand CA, Moore G, Lethborg C, Sundararajan V, et al. "I'm just waiting.": An exploration of the experience of living and dying with primary malignant glioma. Supportive Care Cancer (2014) 22(2):389–97. doi: 10.1007/s00520-013-1986-1
40. Collins A, Sundararajan V, Brand C, Moore G, Lethborg C, Gold M, et al. Clinical presentation and patterns of care for short-term survivors of malignant glioma. J Neurooncology (2014) 119(2):333–41. doi: 10.1007/s11060-014-1483-5
41. Davis MP, Strasser F, Cherny N. How well is palliative care integrated into cancer care? a MASCC, ESMO, and EAPC project. Support Care Cancer (2015) 23(9):2677–85. doi: 10.1007/s00520-015-2630-z
42. Collins A, Sundararajan V, Burchell J, Millar J, McLachlan S-A, Krishnasamy M, et al. Transition points for the routine integration of palliative care in patients with advanced cancer. J Pain symptom Manage (2018) 56(2):185–94. doi: 10.1016/j.jpainsymman.2018.03.022
43. Waller A, Girgis A, Currow DC, Lecathelinais S. Development of the palliative care needs assessment tool (PC-NAT) for use by multi-disciplinary health professionals. Palliative Med (2008) 22(8):956–64. doi: 10.1177/0269216308098797
44. Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol (2022) 9(1):3. doi: 10.1037/qup0000196
45. Philip J, Le Gautier R, Collins A, Nowak AK, Le B, Crawford GB, et al. Care plus study: a multi-site implementation of early palliative care in routine practice to improve health outcomes and reduce hospital admissions for people with advanced cancer: a study protocol. BMC Health Serv Res (2021) 21(1):1–10. doi: 10.1186/s12913-021-06476-3
46. Waller A, Girgis A, Lecathelinais C, Scott W, Foot L, Sibbritt D, et al. Validity, reliability and clinical feasibility of a needs assessment tool for people with progressive cancer. Psycho-Oncology (2010) 19(7):726–33. doi: 10.1002/pon.1624
47. Hui D, Titus A, Curtis T, Ho-Nguyen VT, Frederickson D, Wray C, et al. Implementation of the Edmonton symptom assessment system for symptom distress screening at a community cancer center: a pilot program. oncologist (2017) 22(8):995–1001. doi: 10.1634/theoncologist.2016-0500
48. Finucane AM, Swenson C, MacArtney JI, Perry R, Lamberton H, Hetherington L, et al. What makes palliative care needs “complex”? a multisite sequential explanatory mixed methods study of patients referred for specialist palliative care. BMC palliative Care (2021) 20(1):1–11. doi: 10.1186/s12904-020-00700-3
49. Seow H, Sussman J, Martelli-Reid L, Pond G, Bainbridge D Do high symptom scores trigger clinical actions? an audit after implementing electronic symptom screening. J Oncol Pract (2012) 8(6):e142–e8. doi: 10.1200/JOP.2011.000525
50. Bange EM, Courtright KR, Parikh RB. Implementing automated prognostic models to inform palliative care: more than just the algorithm. BMJ Qual Saf (2021) 30(10):775–8. doi: 10.1136/bmjqs-2021-013510
Keywords: early palliative care, outpatient palliative care, cancer, personalized palliative care, clinical trial, phase II
Citation: Collins A, Sundararajan V, Le B, Mileshkin L, Hanson S, Emery J and Philip J (2022) The feasibility of triggers for the integration of Standardised, Early Palliative (STEP) Care in advanced cancer: A phase II trial. Front. Oncol. 12:991843. doi: 10.3389/fonc.2022.991843
Received: 12 July 2022; Accepted: 26 August 2022;
Published: 15 September 2022.
Edited by:
Marco Maltoni, University of Bologna, ItalyCopyright © 2022 Collins, Sundararajan, Le, Mileshkin, Hanson, Emery and Philip. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Collins, YW5uYS5jb2xsaW5zQHN2aGEub3JnLmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.