
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 14 October 2022
Sec. Cancer Epidemiology and Prevention
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.989713
This article is part of the Research TopicEarly Palliative Care for Cancer PatientsView all 11 articles
 Antonella Galiano1†
Antonella Galiano1† Stefania Schiavon2†Mariateresa Nardi3Irene Guglieri4Ardi Pambuku2
Stefania Schiavon2†Mariateresa Nardi3Irene Guglieri4Ardi Pambuku2 Rosalba Martino5Maital Bolshinsky1Sabina Murgioni1Rossana Intini1Caterina Soldà1Dario Marino1Francesca Daniel1
Rosalba Martino5Maital Bolshinsky1Sabina Murgioni1Rossana Intini1Caterina Soldà1Dario Marino1Francesca Daniel1 Chiara De Toni1Chiara Pittarello1
Chiara De Toni1Chiara Pittarello1 Benedetta Chiusole1
Benedetta Chiusole1 Alessandra Anna Prete1Davide Bimbatti1Floriana Nappo1
Alessandra Anna Prete1Davide Bimbatti1Floriana Nappo1 Mario Caccese1
Mario Caccese1 Francesca Bergamo1
Francesca Bergamo1 Antonella Brunello1*
Antonella Brunello1* Sara Lonardi6‡Vittorina Zagonel1‡
Sara Lonardi6‡Vittorina Zagonel1‡Background: Early activation of palliative care for patients with advanced cancer is central in the treatment trajectory. At the Veneto Institute of Oncology, a simultaneous-care outpatient clinic (SCOC) has been active since 2014, where patients are evaluated by an oncologist together with a palliative care team. Recently, we reported on consecutive patients admitted at SCOC from 2018 to 2021 in terms of appropriateness, process, and outcome indicators. Here, we report further analysis in the same group of 753 patients, evaluating other parameters and the correlation between symptom intensity, gender, age, and survival.
Methods: SCOC data were retrieved from a prospectively maintained database.
Results: Among the patients, 42.2% were women, and the median age was 68 years, with 46.7% of patients aged ≥70 years. The most prevalent disease type was gastrointestinal cancer (75.2%), and 90.9% of the patients had metastatic disease. The median score for the distress thermometer was 4; the vast majority of the patients (98.6%) reported physical problems, and 69.4% presented emotional issues. Younger women demonstrated a significantly greater median distress than other patients (p=0.0018). Almost all symptoms had a higher prevalence on the 0–3 Edmonton Symptom Assessment Scale (ESAS) score, except for fatigue. About 43.8% of the patients received systemic anticancer treatment (SAT) in the last 60 days of life, 15.0% of whom received SAT in the last month and 3.1% in the last 2 weeks. For some symptoms, women frequently had more ESAS >3. Pain and nausea were significantly less reported by older patients compared with younger adults. Men had a lower risk of having MUST score ≥ 2 (p=0.0311). Men and older patients showed a lower prognosis awareness (p=0.0011 and p=0.0049, respectively). Older patients received less SAT within the last 30 days of life (p=0.0006) and had death risk decreased by 20.0%.
Conclusion: Our study identified two subgroups of patients with advanced cancer who require special attention and support due to important symptoms’ burden detected by Patient Reported Outcome Measures tests: women and younger adults. These categories of patients require special attention and should be provided early access at SCOC. The role of an oncologist remains crucial to intercept all patients in need of early palliative care and balancing trade-offs of anticancer treatment in advanced metastatic disease.
There is mounting evidence on the crucial role of early activation of palliative care in patients’ cancer journey, especially in the advanced stage of the disease (1). Indeed, numerous studies have shown that this approach improves the quality of life and, in some cases, even patients’ survival (2–6). As a result, early palliative care is now recommended by most prominent international oncology scientific societies and is included in their guidelines (7–10).
Despite such evidence, outcomes obtained with this approach are not consistently reported and appear to be related to several key elements through which early palliative care benefits patients and caregivers (11). In addition, the heterogeneity related to different organizational models, the availability of palliative care teams, as well as the cultural and social-health aspects across different countries, to date, do not allow suggesting a unique model for early palliative care delivery (11, 12).
The Veneto Institute of Oncology (IOV) takes charge of more than 5,000 new cancer patients in need of systemic treatment per year. IOV is an Organization of European Cancer Institutes (OECI) certified Comprehensive Cancer Center, and since 2012, the Oncology Department has obtained the European Society of Medical Oncology (ESMO) certification as a Designated Center of integration of oncology and palliative care (ESMO-DC). Since 2017, the Institute has adopted a procedure with standardized referral criteria through (1) routine screening of supportive care needs at oncology visits; (2) filling in a referral form by oncologists at the time of the visit; the form was defined by oncology and palliative care teams for identifying patients with palliative care needs; (3) a system in place to trigger referral when patients meet the criteria; and (4) activation of simultaneous care outpatients clinic (SCOC), in which the oncologist and the palliative care team (a palliative care physician, a physician specialized in clinical nutrition, a psycho-oncologist, and a nurse navigator) assess together, through validated tools, the needs of patients with the aim to deliver personalized, timely patient-centered care and improve patient and caregiver outcomes (13). This embedded model meets internationally agreed criteria for optimizing the early inclusion of palliative care in the care pathway (14, 15). In order to ensure an early referral of patients with metastatic disease, patients’ assessment is based on symptom’s burden and life expectancy, and through the activation of a simultaneous care clinic, the oncologist and the palliative care team share the patient’s journey (13). Recently, we reported the data on our series of 753 patients evaluated at SCOC from January 2018 to December 2021 in terms of indicators of appropriateness, process, and outcome provided by the Institute's procedure (13). In this work, we report the data from further analyses performed in the same group of 753 patients, evaluating a number of other parameters and the correlation between symptom intensity, gender, age, and survival.
This study was conducted at the Veneto Institute Oncology (IOV), Padua, Italy. The study population was composed of patients referred to SCOC between January 2018 and December 2021. Selection criteria were the availability of the referral form filled in by the oncologist and cancer-directed treatment planned. SCOC data were retrieved from a prospectively maintained database: demographic and clinic information, distress thermometer (DT), Edmonton Symptom Assessment Scale (ESAS), and Malnutrition Universal Screening Tool (MUST). These three scales (DT, ESAS, and MUST) are used because of the following characteristics:
● The DT is a simple tool developed by the National Comprehensive Cancer Network (NCCN), which provides effective screening for symptoms of distress. The instrument is a self-reported tool using a Likert rating scale (0 to 10) and additionally identifies sources of distress using a Problem List (PL) (16).
● The ESAS is a measure of symptom burden that includes a Likert rating of nine symptoms, on a scale from 0 (best) to 10 (worst), which has been adopted for routine needs screening during the SCOC visit (17).
● The MUST identifies patients who are malnourished or are at risk of malnutrition; a score of 0 indicates a low risk of malnutrition, a score of 1 indicates medium risk, and a score ≥ 2 indicates a high risk (18, 19).
We also analyzed whether there were significant differences by gender, age (age less than, or equal to, and over 70 years), and type of cancer, with regard to a series of variables:
1. DT
2. ESAS: type of symptoms and intensity
3. MUST
4. Awareness of the cancer prognosis (total, partial, absent)
5. Systemic anticancer treatment (SAT) at the end of life (last 60, 30, and 14 days)
6. Unplanned visits to the emergency room (ER)
7. Place of death (hospital vs. hospice or home)
8. Actual survival at the time of SCOC referral
The patients’ characteristics were described by descriptive analysis. The comparisons were tested using chi-square tests, Fisher’ exact tests, and log-rank tests, as appropriate. For the survival analysis, all patients entered into the study at the date of SCOC were followed up until 31 January 2022 or the date of death, whichever came first. Median survival was calculated with the Kaplan–Meier method. The following variables were analyzed: ESAS, MUST, territorial services activation, prognosis awareness, chemotherapy within the last 30 days of life, unplanned access in the ER, place of death, actual and estimated survival; figures were drawn for gender and age comparisons including only the significant results. The place of death and the end-of-life chemotherapy were assessed for deceased patients. Cox’s proportional hazards model was fitted to the data to evaluate the association between the actual survival and the variables of interest (gender, age class, and tumor site). Logistic, multinomial, and cumulative logit models were used to test the association between the category variables, previously considered in the bivariate analysis, and the variables of interest. R Version 4.2.0 was used to perform all statistical analyses. The level of significance was set at 5%.
Demographic and patients’ clinical characteristics are shown in Table 1. Among the patients, 318 were women (42.2%), and the median age was 68 years (range: 60–76 years), with 352 patients (46.7%) aged 70 years and older. The most prevalent disease type was gastrointestinal cancer (566 patients, 75.2%). A total of 661 (87.8%) patients had a Karnofsky performance status (KPS) ≥70, 684 (90.9%) patients had metastatic disease, and 223 (29.6%) patients received more than two lines of therapy. The time from cancer diagnosis to the first SCOC visit was less than 1 year for 351 patients (51.8%). The median survival of the overall population from SCOC visit was 7.3 months (95% CI: 6.5–8.0).
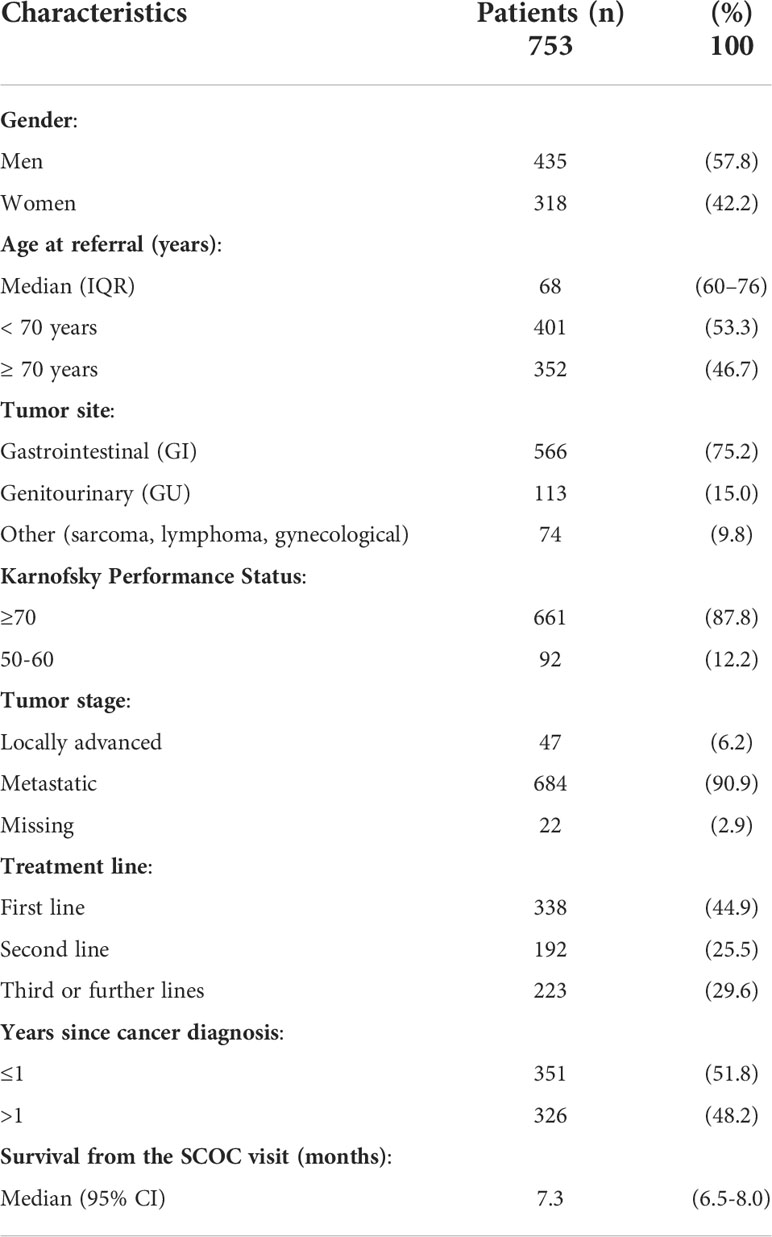
Table 1 Patients’ characteristics.
The median score for DT was 4 (range: 0–9), with the vast majority of patients (98.6%) reporting physical problems and more than half (69.4%) presenting emotional issues, as shown in Figure 1. Family and practical problems and spiritual concerns were present in a small percentage of patients (1.0%, 0.7%, and 0.0%, respectively). Younger women reported a significantly greater median distress compared with other patients (5 vs. 4, p=0.0018, Figure 2).
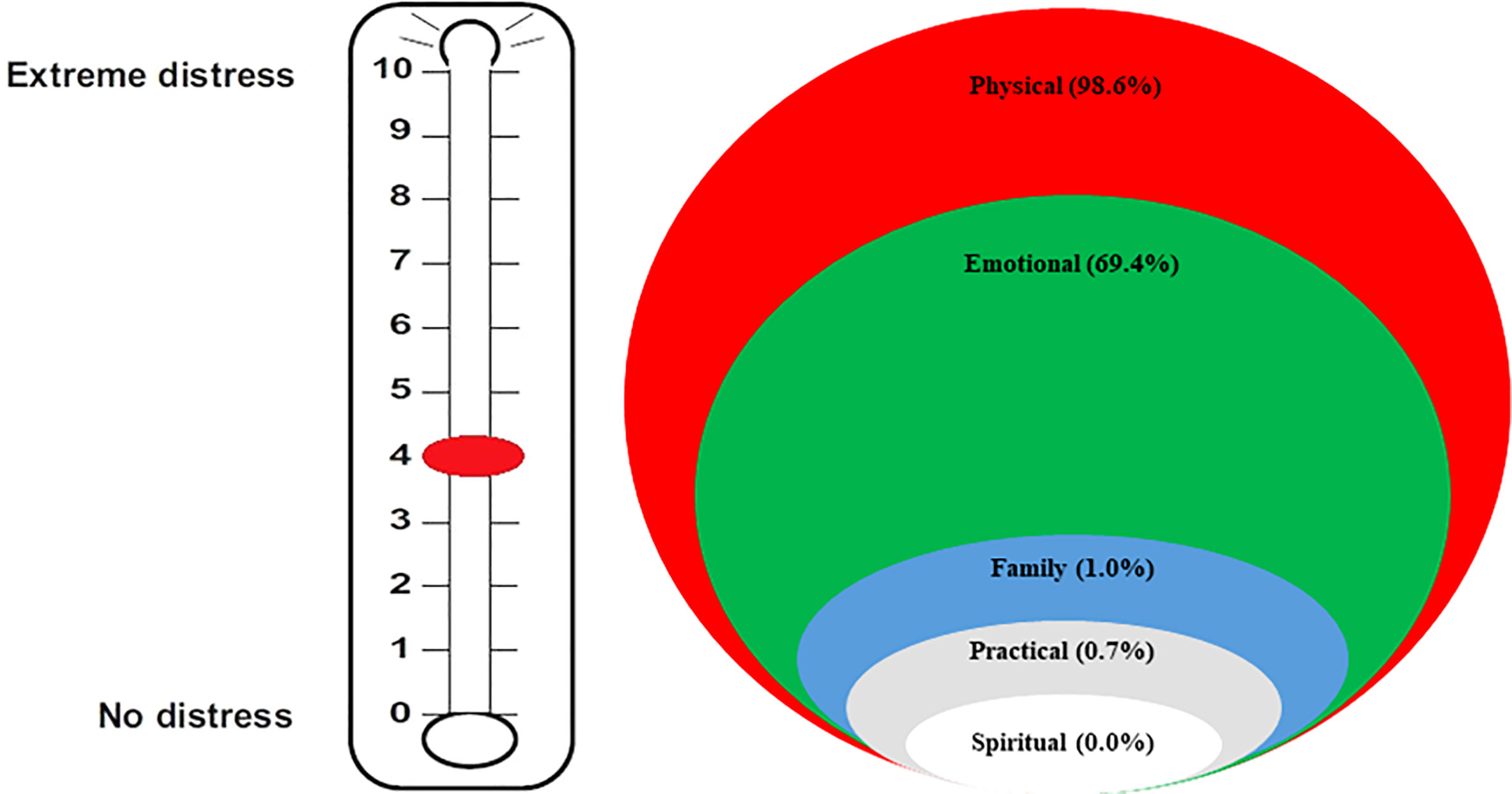
Figure 1 Results according to distress thermometers: median score and burden of distress in the different areas.
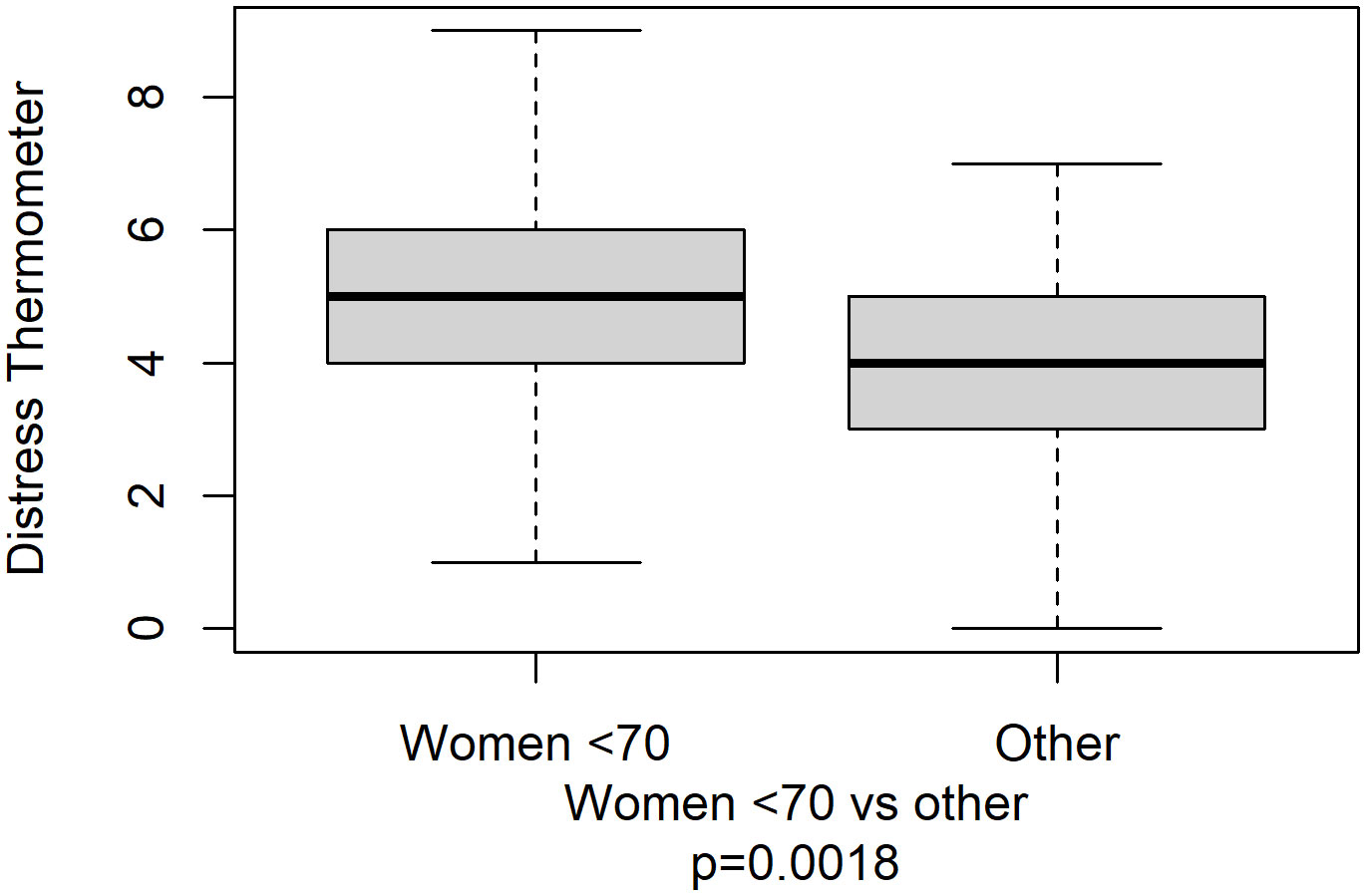
Figure 2 Distress thermometer’s boxplot by women under 70 years versus others.
ESAS symptoms by three levels of severity are shown in Figure 3. Almost all symptoms had a higher prevalence in the 0–3 score range, except for fatigue, which was experienced with an intensity of 7–10 in 281 patients (41.7%). A total of 175 patients had three or more symptoms with an intensity of 7–10. The median survival for these patients was 5.6 months (95% CI: 4.7–7.4), whereas the median survival for the other patients was 7.7 months (95% CI: 6.8–8.6; log-rank test’s p-value=0.0232) (Table 2).
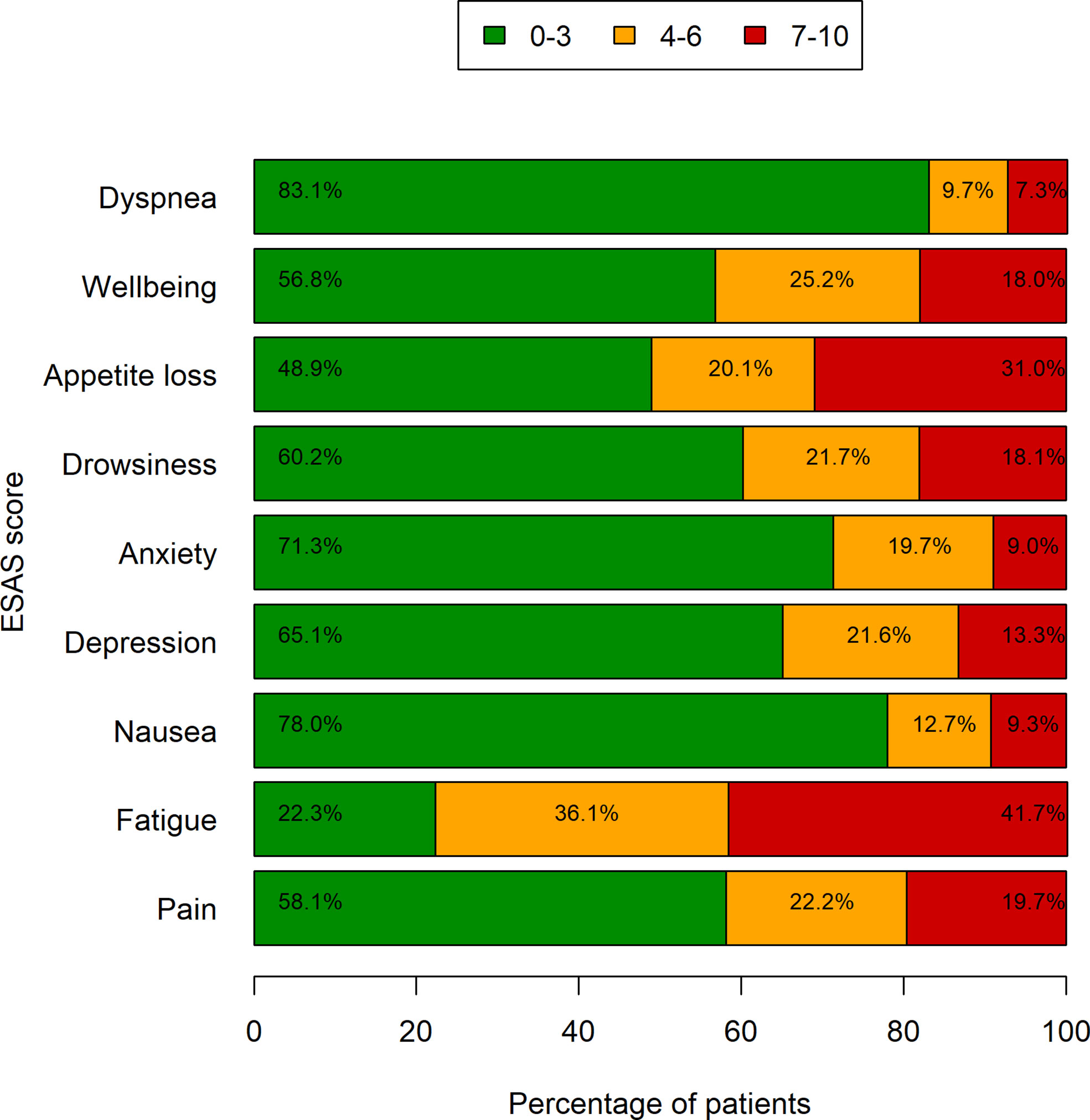
Figure 3 Symptom severity by ESAS. Bars represent the frequencies of symptoms grouped by three levels of severity (data missing in up to 92 patients).

Table 2 Survival according to worse symptom’s burden by ESAS.
As of 31 January 2022, 552 (73.3%) patients were deceased. The median number of days between the last administration of SAT and patient death was 66 (range: 1–1193 days). A total of 242 patients (43.8%) received SAT in the last 60 days of life, among which 83 (15.0%) received SAT during the last month and 17 (3.1%) in the last 2 weeks of life (Table 3). The median age of patients who received SAT in the last 30 days was 63 years (IQR: 57–69), which is lower than the rest of the group (68 years, IQR: 60–76, p=0.0005). Nearly half (47.0%) of the patients who received SAT in the last 30 days of life were being treated in the first line. The median survival from the SCOC visit for these patients was 3.4 months (95% CI: 1.8–4.5) compared with 5.9 months (95% CI: 5.5–6.4) for the other patients (p <0.0001). For this group of patients, the hospital was the more frequent place of death (60.0% vs. 25.5% in other patients, p<0.0001). There were no differences with regard to unplanned access to the ER, hospital admission, number of lines of treatment, and years for patients treated or not treated with SAT in the last month of life.

Table 3 Systemic anticancer treatment (SAT) at the end of life.
ESAS symptoms with intensity greater than 3 were differently distributed according to gender, with women reporting higher prevalence of appetite loss, pain, wellbeing, depression, and anxiety compared with men (see Figure 4). No difference was observed for dyspnea, which was the only symptom more frequent in men (women: 14.8% vs. men: 18.6%, p=0.2388, data not shown).
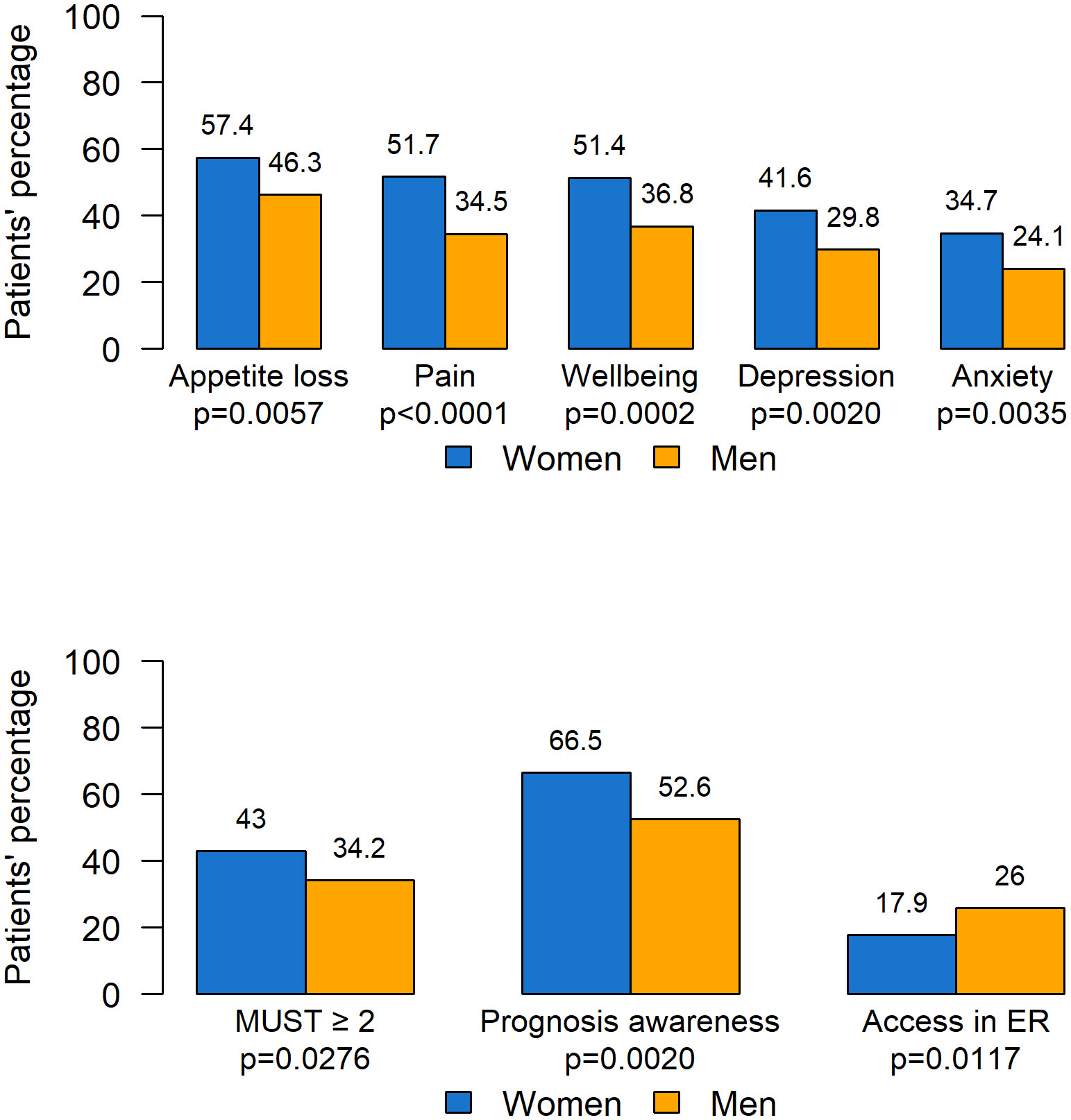
Figure 4 Statistically significant difference according to gender. ER, Emergency room.
MUST scores were worse for women, with 117 (43.0%) having a score ≥ 2 (patients at higher risk of malnutrition), compared with men (130, 34.2%, p=0.0276).
More women were found to have complete awareness of the disease prognosis compared to men (66.5% vs. 52.6%). Moreover, men presented more unplanned access to the ER (26.0% vs. 17.9% for women, p=0.0117). No significant differences according to gender were found in territorial services activation, the number of patients undergoing SAT in the last 30 days of life, the place of death, and survival.
Figure 5 summarizes significant differences according to the age of patients. With regard to ESAS, pain (p=0.0373) and nausea (p=0.0296) had a higher prevalence in younger compared to older patients. As for prognosis awareness, 209 patients (64.3%) aged <70 years reported total prognosis awareness compared with 148 (51.9%) patients aged ≥ 70 years. SAT in the last 30 days of life was administered to 63 (20.0%) adults aged <70 years and to 20 (8.4%) older patients (p=0.0003). Also, a significant difference was observed with regard to the place of death, occurring in hospital for 38.4% younger subjects compared with 22.7% for older patients. Moreover, older patients had better survival, with median survival for adults aged <70 years being 6.3 months (95% CI: 5.7–7.2) compared with 8.8 months (95% CI: 7.5–10.1) for patients aged ≥ 70 years (p=0.0006). No other significant differences were found.
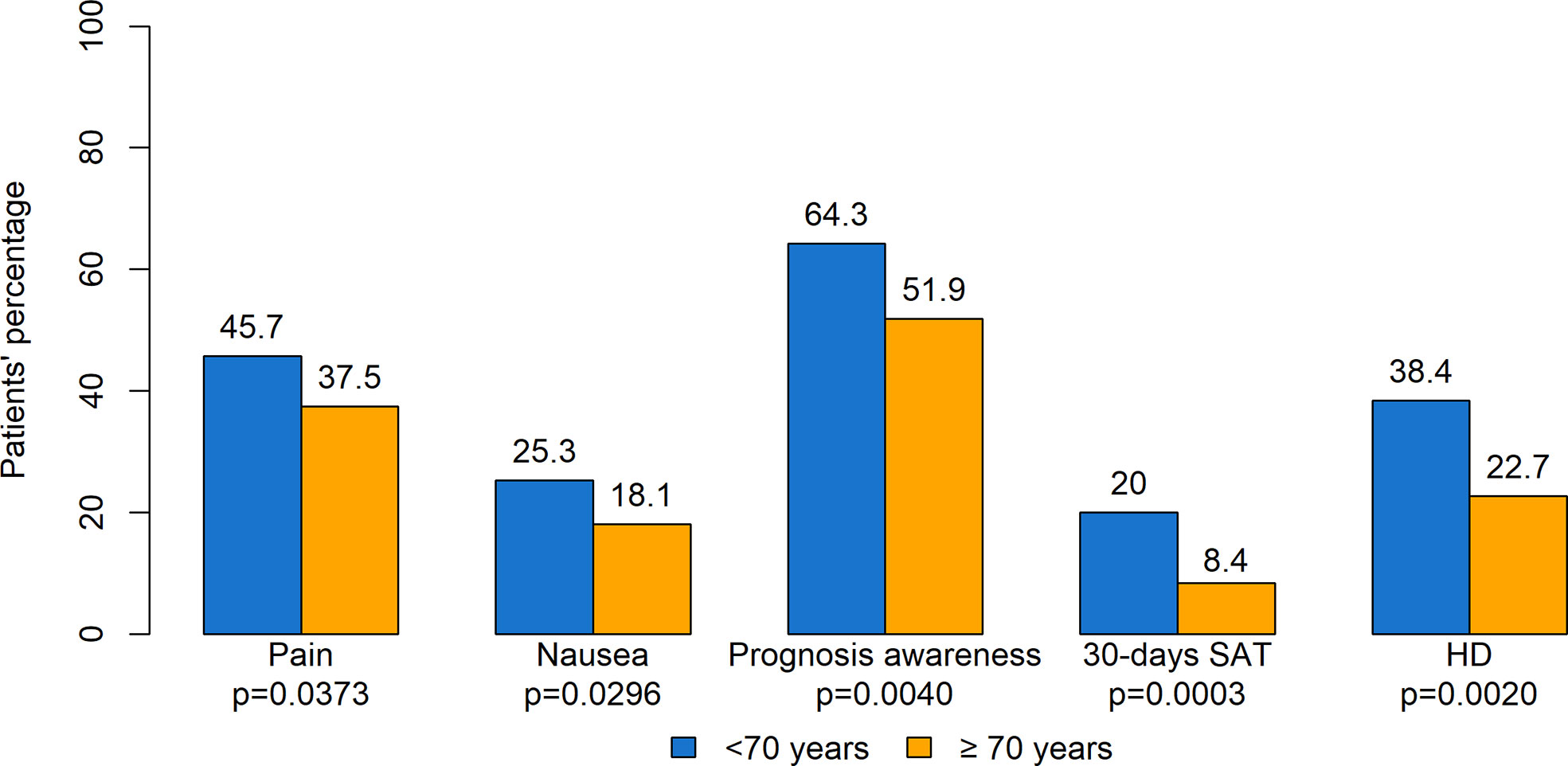
Figure 5 Statistically significant difference according to age. SAT, systemic anticancer therapy; HD, hospital death.
Regression models were developed taking into account the variables of interest. As reported in Table 4, multivariate analysis confirmed the statistically significant difference in the ESAS score by gender (women’s ESAS score >3 for the symptoms pain, nausea, depression, anxiety, appetite loss, and wellbeing), MUST (lower risk of having a score ≥ 2 in men), and a higher awareness of cancer prognosis in women. Patients aged 70 years and older also had 20% lower risk of death (p=0.0072). Elderly patients received less SAT within the last 30 days of life as well as in the last 2 months (OR=0.6, p=0.0058, data not shown). With regard to the tumor site, only mortality risk resulted significant in multivariate analysis, being 1.5 times higher for GI cancers compared with other cancer types (p=0.0099).
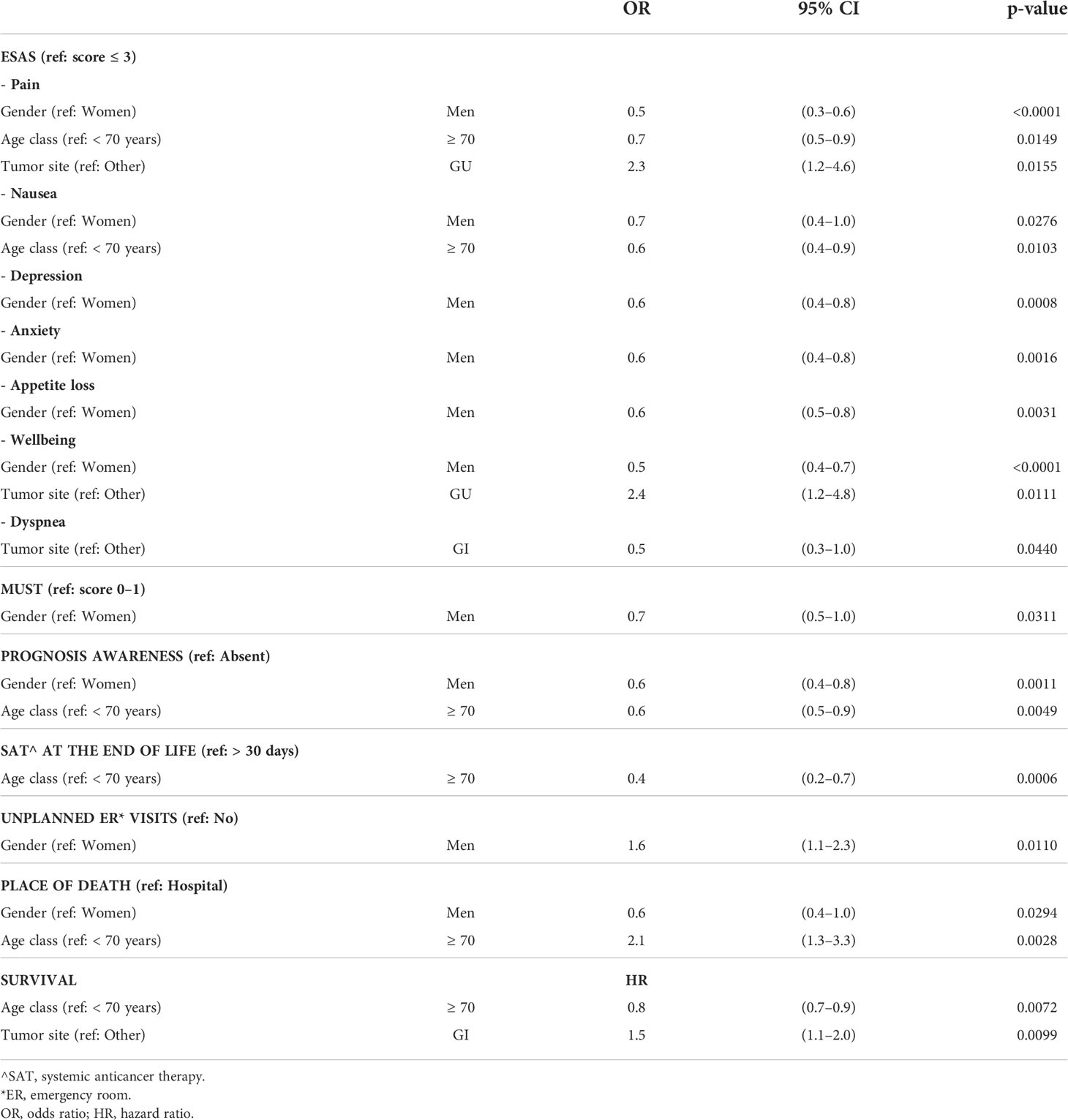
Table 4 Results by multivariate analysis.
Early integration of palliative care in the cancer patient’s care path is today regarded as an essential goal to optimize the quality of life in the advanced stage of the disease and is best delivered in outpatient clinics (1). There is no single model of palliative care that is appropriate for all settings (11). The embedded model put in place in our Department, in which the palliative care team shares the SCOC with the oncologist, meets all the criteria proposed by international consensus to ensure timely activation of palliative care (20). This innovative organizational model allows intercepting cancer patients in an advanced stage of disease who need global care. The needs of each patient are addressed through the systematic use of validated Patient Reported Outcome Measures (PROMs), and this allows the customization of the patient’s journey and future end-of-life care decisions. In particular, the joint presence of an oncologist together with the palliative care team facilitates dialogue with patients and caregivers on advance care planning, end-of-life provisions, and preferential death location (21). Sharing resources between oncology and palliative care services is also cost-effective and may encourage collaborative education and research (11, 15). New organizational models are a challenge and an important resource to guarantee assistance to cancer patients also in the COVID era and in every phase of the illness trajectory (Andrè Ilbawi, WHO Cancer Control Officer, Opening Session at ASCO 2022 congress, the 4th June 2022).
A previous paper by our group described the organizational model of embedded systemic early palliative care for patients with advanced cancer and the results of the last 4 years of activity as assessed through indicators of outcome, process, and appropriateness (13). The present work reports the results concerning symptoms burden, SAT at the end of life, difference by age, gender, and survival in the same group of 753 patients referred to SCOC in the period 2018–2021.
The DT, first described by Roth et al. in 1998, was developed for assessing distress in cancer patients (16). Since then, several experiences have been published regarding this easy-to-use tool with the ability to intercept at a glance the main problems of the patient (22, 23). A wide proportion of cancer patients, ranging between 25% and 60%, report distress when they are assessed (24). The median DT score in our patients was 4 (range: 0–9), with 98.6% of the patients experiencing physical problems, 69.4% emotional problems, and only 1.0%, 0.7%, and 0.0% reporting familiar, practical, and spiritual problems, respectively. This very low frequency of practical, family, and spiritual problems might look surprising, taking into account other studies, particularly American experiences, in which up to 80% of the patients with cancer attribute their distress to financial stressors (25, 26). This may be due to several reasons, including the different Italian healthcare system (which guarantees the coverage of most of cancer therapies compared with the American insurance system), the different social aspects of family relationships, and more widespread religious beliefs, as well as the patients’ reluctance to involve the doctor on problems other than oncological disease.
Fatigue was highly relevant in our patients’ population, reported by 92.7% with the DT and confirmed by the ESAS assessment. Notably, for ESAS > 3, fatigue was detected in 77.8% of the patients. Indeed, fatigue constitutes the most distressing patient-related symptom in terms of intensity and frequency that negatively affects their quality of life (27–29), although, unfortunately, nothing at this time has been shown to effectively relieve this symptom (30). Fatigue is multifactorial, related both to the treatment (surgery, chemotherapy, and radiation therapy) and to the tumor itself. It is usually underestimated by physicians, and its management remains one of the greatest unmet needs for patients with advanced cancer. Fatigue has been inadequately discussed and undertreated (31) due to lack of agreement on its measurement, inadequate understanding of the biology, and difficulty in conducting clinical trials of fatigue interventions (32). According to systematic meta-analyses and recently published studies, evidence-based management of cancer-related fatigue should be focused on behavioral and psychological interventions (33, 34), since pharmacological intervention has shown limited effect. Also, literature report on cancer-related fatigue seems to be more pronounced in women than in men, especially at the end of life (35).
ESAS was confirmed in our experience as one of the most valuable tools for detecting type and intensity of symptoms in metastatic cancer patients. In line with literature data (36), nearly one-fourth of the patients with advanced cancer in our cohort experienced three or more symptoms with an intensity of 7/10 or greater, exhibiting a strong correlation with survival. ESAS is confirmed as an important tool for identifying a group of patients with high symptom burden who require immediate support and assistance by the palliative care team (36, 37). Assessment of patient’s needs allows providing more effective support, relevant to every person’s individual experience, and it is necessary for setting priorities for resource allocation (31).
With regard to SAT at the end of life, our study showed that 43.8% of the patients received anticancer therapy during the last 60 days of life, of which 15% was within the last 30 days and 3.1% within the last 2 weeks of life. These figures can be partially justified by the good KPS that, on average, patients presented at the time of their first SCOC visit and that guides oncologists in their decision-making. In fact, almost half of the patients who received SAT in the last 30 days of life are therapy naïve. Furthermore, younger patients were more often treated with SAT at the end of life likely due to oncologists’ attitude of offering at least one opportunity for treatment even though cancer was in the advanced stage at diagnosis. SAT use in the last 14 days in our series compares favorably with the rate of 7% reported by Bakitas (4), 9.3% of an Italian study (38), as well as the rate of 13.6% observed by Greer et al. (39). Based on the analysis of SEER-Medicare, an overly aggressive care is associated with more than 10% of patients receiving SAT in the last 14 days (40). As for the patients who received SAT within 30 or 60 days, our results are in line with those reported in the literature in Italy (41, 42) and in other countries (43–45). Although the use of SAT in patients who are close to death has been increasing over time (46), little information is available about the clinical effect of such treatment (47). The extent of the contribution of SAT at the end of life and the role of advanced state of disease per se in hastening patients’ death cannot be further assessed in our experience, just like other reports in the literature, i.e., Zhu et al. (44). Indeed, our data confirm those by an American report in which SAT in the last 30 days of life was associated with an increased rate of death in the hospital (48, 49). Interestingly, older patients were found to receive less SAT during the last 60 days of life, in line with literature data (44, 48); they lived longer and died more frequently in hospice or at home. Indeed, as reported by Wright et al., perceptions of better end-of-life care are associated with earlier hospice enrolment, avoidance of ICU admission in the last 30 days of life, and deaths outside the hospital, among family members of elderly patients who died with lung or colorectal cancer (50). These findings are supportive of advance care planning consistent with patients’ preferences (50, 51) and may help both granting patients’ wishes regarding the place of death (52) as well as reducing caregivers’ distress (53).
The role of oncologists is strategic not only for the proper management of SCOC patients but also for an accurate estimation of prognosis in order to avoid therapeutic aggressiveness at the end of life when not justified. Continuing education of medical oncologists in palliative care remains critical for both providing the first level of palliative care, with systematic use of PROMs in clinical practice, and facilitating early access to an integrated SCOC (13). Prognosis, indeed, needs to be taken into account in the decision-making process, and several tools may help in the prognosis assessment, such as the Pap score (54). A systematic review of mortality predictors in patients with advanced cancer has been recently published (55). The “surprise question” and general clinical and laboratory variables are non-tumor-specific predictors of mortality within 3–24 months in patients with advanced cancer. This translates in the recommendation to pay more attention in the advanced stage of disease to clinical and laboratory parameters, which are not cancer-related, rather than to the type of tumor. In fact, a new validated machine-learning model to predict 6-month prognosis in patients with advanced solid tumors has been proposed (56), which can be useful and may support shared decision-making discussions between oncologists and patients with regard to considering a further line of SAT.
In addition, our data prove that there are significant differences with regard to gender and age. Women experienced a higher frequency of pain, anxiety, depression requiring psychological support in 22% of the subjects, loss of appetite, and higher MUST score values (100% requiring nutritional support), together with a higher frequency of total awareness of cancer prognosis compared with men. In particular, subgroup analysis by DT results showed that adult women had a significantly higher median distress compared with the rest of the cancer patient population.
Evaluation by age revealed a significantly lower median survival in younger subjects; in the same group, prevalence of pain was higher, along with awareness of prognosis. Such differences were confirmed in multivariate analysis. Indeed, age and gender might be differently impacted by early palliative care interventions, as reported in the study by Nipp et al. (57). No significant differences were found in our cohort by disease subgroups, except for lower dyspnea and lower survival in patients with GI cancer, as well higher pain and lower wellbeing in patients with GU cancer. This suggests, as reported by Chalkidis et al. and confirmed by a systematic review of mortality predictors in patients with advanced cancer, that patients with advanced solid tumors may converge to a common pathway at end of life, regardless of the cancer type, at which point patient-specific factors unrelated to cancer are the most important (55, 56).
In conclusion, to summarize it with the metaphor that Zimmermann has recently proposed, our study confirms the importance of introducing early palliative care as an umbrella for cancer patients and caregivers that must be opened before it starts to rain (58).
This study has some limitations. Although the results are in line with other similar reports in the literature, data collection was limited to one single center, which restricts the extrapolation of the results to the general population. Given the observational nature of this study, it was not possible to evaluate the effectiveness of this approach in comparison with a control group. The oncologist’s reasons for referring patients to SCOC and anticancer treatment decision-making were not factored in, although they would provide additional information.
Our data confirm the importance of assessing PROMs by oncologists in clinical practice for a thorough evaluation of type and extent of needs of advanced cancer patients undergoing systemic cancer treatment. Oncologists must also be trained in the use of validated prognostic tools in order to refrain from proposing anticancer therapy at the end of life when not indicated. A fully embedded model in which the oncologist evaluates patients with advanced stage disease together with a palliative care team can facilitate the patients’ approach to palliative care and allows for direct sharing among the palliative care team regarding treatment options, life expectancy, and patient awareness of prognosis. Proper resources should be allocated in order to fulfill model requirements (59).
Our data confirm the importance of assessing PROMs in order to acknowledge the type and extent of needs of advanced cancer patients. Italian cultural, social, and healthcare background may partly justify the low prevalence of social and spiritual issues detected in a relevant group of cancer patients with advanced stage of disease, and confirm the general presence of good family support, which is also assessed by the high percentage of patients who died at home (37.8%). Our study identified two subgroups of patients who require special attention and support due to the important symptom’s burden detected by PROMs: women who experienced higher frequency of pain, anxiety, depression, loss of appetite, and higher MUST scores, together with a higher frequency of total awareness of the prognosis; and younger adult subjects who have a shorter life expectancy, experience more intense pain and nausea, are more aware of the prognosis, and die more often in a hospital. These categories of patients with advanced stage of disease, regardless of the tumor type, require special attention to provide early referral to SCOC for adequate symptoms’ relief and proper care planning.
The overall SCOC performance was good as evaluated by some parameters such as the low percentage of patients receiving SAT at the end of life, the place of death, and the number of unplanned visits at the ER.
The role of the oncologist remains crucial to identify all patients in need of early palliative care through the systematic use of PROMs, which are now part of clinical practice (60). Assessment of patients’ needs should be done across the board on all patients with metastatic cancer, and then, through joint evaluation at SCOC, the categories of patients in greatest need can be identified. Changing perspective in the evaluation of patients is mandatory for oncologists in order to intercept the true needs of patients with cancer in advanced disease. Defining an accurate estimate of prognosis remains strategic in order to avoid SAT at the end of life, especially as second or further treatment line, which can contribute to being detrimental for patients’ survival and/or the quality of life for patients and caregivers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was reviewed and approved by Veneto Institute of Oncology Ethics Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization, VZ, AG, SS, AB, and SL. Data collection, VZ, AG, SS, MN, IG, AP, RM, MB, SM, CS, DM, FD, CDT, CP, BC, AAP, DB, FN, MC, FB, RI, AB and SL. Statistical analysis: CDT; original draft preparation, VZ, AG, AB, CDT, SS, and SL. Review and editing, all authors. All authors contributed to the article and approved the submitted version.
This study was supported by Ricerca Corrente 2022, Italian Ministry of Health and by a charitable donation by Maria Sanvido.
We thank Dr. Leonardo Trentin for essential contribution in setting up the Simultaneous Care Outpatient Clinic.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hui D, Bruera E. Integrating palliative care into the trajectory of cancer care. Nat Rev Clin Oncol (2016) 13:159–71. doi: 10.1038/nrclinonc.2015.201
2. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med (2010) 363:733–42. doi: 10.1056/NEJMoa1000678
3. Haun MW, Estel S, Rücker G, Friederich HC, Villalobos M, Thomas M, et al. Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev (2017) 6:1–94. doi: 10.1002/14651858.CD011129.pub2
4. Bakitas MA, Tosteson TD, Li Z, Lyons KD, Hull JG, Li Z, et al. Early versus delayed initiation of concurrent palliative oncology care: Patient outcomes in the ENABLE III randomized controlled trial. J Clin Oncol (2015) 33:1438–45. doi: 10.1200/JCO.2014.58.6362
5. Zimmermann C, Swami N, Krzyzanowska M, Hannon B, Leighl N, Oza A, et al. Early palliative care for patients with advanced cancer: A cluster-randomised controlled trial. Lancet (2014) 383:1721–30. doi: 10.1016/S0140-6736(13)62416-2
6. Maltoni M, Scarpi E, Dall’Agata M, Zagonel V, Bertè R, Ferrari D, et al. Systematic versus on-demand early palliative care: Results from a multicentre, randomised clinical trial. Eur J Cancer (2016) 65:61–8. doi: 10.1016/j.ejca.2016.06.007
7. Cherny NI, Catane R, Kosmidis P, ESMO Taskforce on Supportive and Palliative Care. ESMO takes a stand on supportive and palliative care. Ann Oncol (2003) 14:1335–7. doi: 10.1093/annonc/mdg379
8. Ferrell BR, Temel JS, Temin S, Alesi ER, Balboni TA, Basch EM, et al. Integration of palliative care into standard oncology care: American society of clinical oncology clinical practice guideline update. J Clin Oncol (2017) 35:96–112. doi: 10.1200/JCO.2016.70.1474
9. Levy MH, Adolph MD, Back A, Block S, Codada SN, Dalal S, et al. Palliative care. J Natl Compr Canc Netw (2012) 10:1284–309. doi: 10.6004/jnccn.2012.0132
10. Zagonel V, Franciosi V, Brunello A, Biasco G, Broglia C, Cattaneo D, et al. Position paper of the Italian association of medical oncology on early palliative care in oncology practice (Simultaneous care). Tumori (2017) 103:9–14. doi: 10.5301/tj.5000593
11. Mathews J, Hannon B, Zimmermann C. Models of integration of specialized palliative care with oncology. Curr Treat Options Oncol (2021) 22:44. doi: 10.1007/s11864-021-00836-1
12. Hui D, Bansal S, Strasser F, Morita T, Caraceni A, Davis M, et al. Indicators of integration of oncology and palliative care programs: An international consensus. Ann Oncol (2015) 26:1953–9. doi: 10.1093/annonc/mdv269
13. Brunello A, Galiano A, Schiavon S, Nardi M, Feltrin A, Pambuku A, et al. Simultaneous care in oncology: A 7-year experience at ESMO designated centre at veneto institute of oncology, Italy. Cancers (Basel) (2022) 14:2568. doi: 10.3390/cancers14102568
14. Kaasa S, Loge JH, Aapro M, Albreht T, Anderson R, Bruera E, et al. Integration of oncology and palliative care: a lancet oncology commission. Lancet Oncol (2018) 19:e588–653. doi: 10.1016/S1470-2045(18)30415-7
15. Hui D, Cherny NI, Wu J, Liu D, Latino NJ, Strasser F. Indicators of integration at ESMO designated centres of integrated oncology and palliative care. ESMO Open (2018) 3:e000372. doi: 10.1136/esmoopen-2018-000372
16. Roth AJ, Kornblith AB, Batel-Copel L, Peabody E, Scher HI, Holland JC. Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer (1998) 82:1904–8. doi: 10.1002/(sici)1097-0142(19980515)82
17. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton symptom assessment system (ESAS): A simple method for the assessment of palliative care patients. J Palliat Care (1991) 7:6–9. doi: 10.1177/082585979100700202
18. Weekes CE, Elia M, Emery PW. The development, validation and reliability of a nutrition screening tool based on the recommendations of the British association for parenteral and enteral nutrition (BAPEN). Clin Nutr (2004) 23:1104–12. doi: 10.1016/j.clnu.2004.02.003
19. Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical nutrition in cancer. Clin Nutr (2021) 40:2898–913. doi: 10.1016/j.clnu.2021.02.005
20. Hui D, Heung Y, Bruera E. Timely palliative care: Personalizing the process of referral. Cancers (Basel) (2022) 14:1047. doi: 10.3390/cancers14041047
21. Miccinesi G, Caraceni A, Garetto F, Zaninetta G, Bertè R, Broglia CM, et al. The path of Cicely Saunders: The “Peculiar beauty” of palliative care. J Palliat Care (2020) 35:3–7. doi: 10.1177/0825859719833659
22. Donovan KA, Handzo G, Corbett C, Vanderlan J, Brewer BW, Ahmed K. NCCN distress thermometer problem list update. J Natl Compr Canc Netw (2022) 20:96–8. doi: 10.6004/jnccn.2022.0004
23. Ownby KK. Use of the distress thermometer in clinical practice. J Adv Pract Oncol (2019) 10:175–9.
24. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology (2001) 10:19–28. doi: 10.1002/1099-1611(200101/02)10
25. Yabroff KR, Dowling EC, Guy GP Jr, Banegas MP, Davidoff A, Han X, et al. Financial hardship associated with cancer in the United States: Findings from a population-based sample of adult cancer survivors. J Clin Oncol (2016) 34:259–67. doi: 10.1200/JCO.2015.62.0468
26. Kera T, Kawai H, Yoshida H, Hirano H, Kojima M, Fujiwara Y, et al. Physical and psychological characteristics of the community-dwelling elderly with heart disease. Nihon Koshu Eisei Zasshi (2017) 64:3–13. doi: 10.11236/jph.64.1_3
27. Rau KM, Shun SC, Chiou TJ, Lu CH, Ko WH, Lee MY, et al. A nationwide survey of fatigue in cancer patients in Taiwan: An unmet need. Jpn J Clin Oncol (2020) 50:693–700. doi: 10.1093/jjco/hyaa038
28. Rodin R, Swami N, Pope A, Hui D, Hannon B, Le LW, et al. Impact of early palliative care according to baseline symptom severity: Secondary analysis of a cluster-randomized controlled trial in patients with advanced cancer. Cancer Med (2022) 11:1869–78. doi: 10.1002/cam4.4565
29. Klasson C, Helde Frankling M, Warnqvist A, Sandberg C, Nordström M, Lundh-Hagelin C, et al. Sex differences in the effect of vitamin d on fatigue in palliative cancer care-a Post hoc analysis of the randomized, controlled trial ‘Palliative-d’. Cancers (Basel) (2022) 14:746. doi: 10.3390/cancers14030746
30. Wang T, Molassiotis A, Chung BPM, Tan JY. Unmet care needs of advanced cancer patients and their informal caregivers: A systematic review. BMC Palliat Care (2018) 17:96. doi: 10.1186/s12904-018-0346-9
31. Lewandowska A, Rudzki G, Lewandowski T, Rudzki S. The problems and needs of patients diagnosed with cancer and their caregivers. Int J Environ Res Public Health (2020) 18:87. doi: 10.3390/ijerph18010087
32. Barsevick AM, Irwin MR, Hinds P, Miller A, Berger A, Jacobsen P, et al. Recommendations for high-priority research on cancer-related fatigue in children and adults. J Natl Cancer Inst (2013) 105:1432–40. doi: 10.1093/jnci/djt242
33. Mustian KM, Alfano CM, Heckler C, Kleckner AS, Kleckner IR, Leach CR, et al. Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: A meta-analysis. JAMA Oncol (2017) 3:961–8. doi: 10.1001/jamaoncol.2016.6914
34. Lobefaro R, Rota S, Porcu L, Brunelli C, Alfieri S, Zito E, et al. Cancer-related fatigue and depression: A monocentric, prospective, cross-sectional study in advanced solid tumors. ESMO Open (2022) 7:100457. doi: 10.1016/j.esmoop.2022.100457
35. Husain AF, Stewart K, Arseneault R, Moineddin R, Cellarius V, Librach SL, et al. Women experience higher levels of fatigue than men at the end of life: A longitudinal home palliative care study. J Pain Symptom Manage (2007) 33:389–97. doi: 10.1016/j.jpainsymman.2006.09.019
36. Hui D, Bruera E. The Edmonton symptom assessment system 25 years later: Past, present, and future developments. J Pain Symptom Manage (2017) 53:630–43. doi: 10.1016/j.jpainsymman.2016.10.370
37. Hui D, Mori M, Watanabe SM, Caraceni A, Strasser F, Saarto T, et al. Referral criteria for outpatient specialty palliative cancer care: An international consensus. Lancet Oncol (2016) 17:e552–9. doi: 10.1016/S1470-2045(16)30577-0
38. L’assistenza nel fine vita in oncologia. Valutazioni da dati amministrativi in Emilia-romagna. Dossier, (2016) 259–2016. ISSN 1591-223x.
39. Greer JA, Pirl WF, Jackson VA, Muzikansky A, Lennes IT, Heist RS, et al. Effect of early palliative care on chemotherapy use and end-of-life care in patients with metastatic non-small-cell lung cancer. J Clin Oncol (2012) 30:394–400. doi: 10.1200/JCO.2011.35.7996
40. Earle CC, Neville BA, Landrum MB, Souza JM, Weeks JC, Block SD, et al. Evaluating claims-based indicators of the intensity of end-of-life cancer care. Int J Qual Health Care (2005) 17:505–9. doi: 10.1093/intqhc/mzi061
41. Maltoni M, Scarpi E, Dall’Agata M, Schiavon S, Biasini C, Codecà C, et al. Systematic versus on-demand early palliative care: A randomised clinical trial assessing quality of care and treatment aggressiveness near the end of life. Eur J Cancer (2016) 69:110–8. doi: 10.1016/j.ejca.2016.10.004
42. Formoso G, Marino M, Guberti M, Grilli RG. End-of-life care in cancer patients: how much drug therapy and how much palliative care? Record linkage study in northern Italy. BMJ Open (2022) 12:e057437. doi: 10.1136/bmjopen-2021-057437
43. Woldie I, Elfiki T, Kulkarni S, Springer C, McArthur E, Freeman N. Chemotherapy during the last 30 days of life and the role of palliative care referral, a single center experience. BMC Palliat Care (2022) 21:20. doi: 10.1186/s12904-022-00910-x
44. Zhu Y, Tang K, Zhao F, Zang Y, Wang X, Li Z, et al. End-of-life chemotherapy is associated with poor survival and aggressive care in patients with small cell lung cancer. J Cancer Res Clin Oncol (2018) 144:1591–9. doi: 10.1007/s00432-018-2673-x
45. Saito AM, Landrum MB, Neville BA, Ayanian JZ, Earle CC. The effect on survival of continuing chemotherapy to near death. BMC Palliat Care (2011) 10:14. doi: 10.1186/1472-684X-10-14
46. Earle CC, Neville BA, Landrum MB, Ayanian JZ, Block SD, Weeks JC. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol (2004) 22:315–21. doi: 10.1200/JCO.2004.08.136
47. Murillo JR Jr, Koeller J. Chemotherapy given near the end of life by community oncologists for advanced non-small cell lung cancer. Oncologist (2006) 11:1095–9. doi: 10.1634/theoncologist.11-10-1095
48. Näppä U, Lindqvist O, Rasmussen BH, Axelsson B. Palliative chemotherapy during the last month of life. Ann Oncol (2011) 22:2375–80. doi: 10.1093/annonc/mdq778
49. Prigerson HG, Bao Y, Shah MA, Paulk ME, LeBlanc TW, Schneider BJ, et al. Chemotherapy use, performance status, and quality of life at the end of life. JAMA Oncol (2015) 1:778–84. doi: 10.1001/jamaoncol.2015.2378
50. Wright AA, Keating NL, Ayanian JZ, Chrischilles EA, Kahn KL, Ritchie CS, et al. Family perspectives on aggressive cancer care near the end of life. JAMA (2016) 315:284–92. doi: 10.1001/jama.2015.18604
51. Hoerger M, Greer JA, Jackson VA, Park ER, Pirl WF, El-Jawahri A, et al. Defining the elements of early palliative care that are associated with patient-reported outcomes and the delivery of end-of-Life care. J Clin Oncol (2018) 36(11):1096–102. doi: 10.1200/Jco.2017.75.6676
52. Fereidouni A, Rassouli M, Salesi M, Ashrafizadeh H, Vahedian-Azimi A, Barasteh S. Preferred place of death in adult cancer patients: A systematic review and meta-analysis. Front Psychol (2021) 12:704590. doi: 10.3389/fpsyg.2021.704590
53. Mercadante S, Piccione T, Spinnato F, Scordi MC, Perricone C, Pumilia U, et al. Caregiver distress in home palliative care. Am J Hosp Palliat Care (2022) 23:10499091221080450. doi: 10.1177/10499091221080450
54. Scarpi E, Nanni O, Maltoni M. Development and validation of the PaP score nomogram for terminally ill cancer patients. Cancers (Basel) (2022) 14:2510. doi: 10.3390/cancers14102510
55. Owusuaa C, Dijkland SA, Nieboer D, van der Heide A, van der Rijt CCD. Predictors of mortality in patients with advanced cancer-a systematic review and meta-analysis. Cancers (Basel) (2022) 14:328. doi: 10.3390/cancers14020328
56. Chalkidis G, McPherson J, Beck A, Newman M, Yui S, Staes C. Development of a machine learning model using limited features to predict 6-month mortality at treatment decision points for patients with advanced solid tumors. JCO Clin Cancer Inform (2022) 6:e2100163. doi: 10.1200/CCI.21.00163
57. Nipp RD, Greer JA, El-Jawahri A, Traeger L, Gallagher ER, Park ER, et al. Age and gender moderate the impact of early palliative care in metastatic non-small cell lung cancer. Oncologist (2016) 21:119–26. doi: 10.1634/theoncologist.2015-0232
58. Zimmermann C, Mathews J. Palliative care is the umbrella, not the rain–a metaphor to guide conversations in advanced cancer. JAMA Oncol (2022) 8:681–2. doi: 10.1001/jamaoncol.2021.8210
59. Gaertner J, Maier BO, Radbruch L. Resource allocation issues concerning early palliative care. Ann Palliat Med (2015) 4:156–61. doi: 10.3978/j.issn.2224-5820.2015.07.02
Keywords: simultaneous care, early palliative care (EPC), symptom assessment, advanced cancer, end of life chemotherapy, patient-centered care
Citation: Galiano A, Schiavon S, Nardi M, Guglieri I, Pambuku A, Martino R, Bolshinsky M, Murgioni S, Intini R, Soldà C, Marino D, Daniel F, De Toni C, Pittarello C, Chiusole B, Prete AA, Bimbatti D, Nappo F, Caccese M, Bergamo F, Brunello A, Lonardi S and Zagonel V (2022) Simultaneous care in oncology: Assessment of benefit in relation to symptoms, sex, and age in 753 patients. Front. Oncol. 12:989713. doi: 10.3389/fonc.2022.989713
Received: 08 July 2022; Accepted: 05 September 2022;
Published: 14 October 2022.
Edited by:
Pål Klepstad, Norwegian University of Science and Technology, NorwayReviewed by:
Eleonora Anna Mess, Wroclaw Medical University, PolandCopyright © 2022 Galiano, Schiavon, Nardi, Guglieri, Pambuku, Martino, Bolshinsky, Murgioni, Intini, Soldà, Marino, Daniel, De Toni, Pittarello, Chiusole, Prete, Bimbatti, Nappo, Caccese, Bergamo, Brunello, Lonardi and Zagonel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonella Brunello, YW50b25lbGxhLmJydW5lbGxvQGlvdi52ZW5ldG8uaXQ=
†These authors share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.