
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 11 August 2022
Sec. Gastrointestinal Cancers: Hepato Pancreatic Biliary Cancers
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.963753
 Matthew Ledenko1
Matthew Ledenko1 Samuel O. Antwi2
Samuel O. Antwi2 Shiho Arima3
Shiho Arima3 Julia Driscoll1
Julia Driscoll1 Junji Furuse4Heinz-Josef Klümpen5Finn Ole Larsen6
Junji Furuse4Heinz-Josef Klümpen5Finn Ole Larsen6 David K. Lau7,8
David K. Lau7,8 Annett Maderer9,10
Annett Maderer9,10 Alice Markussen6
Alice Markussen6 Markus Moehler9,10Lynn E. Nooijen11Walid L. Shaib12Niall C. Tebbutt13Thierry André14Makoto Ueno15Rachel Woodford16
Markus Moehler9,10Lynn E. Nooijen11Walid L. Shaib12Niall C. Tebbutt13Thierry André14Makoto Ueno15Rachel Woodford16 Changhoon Yoo17Mark M. Zalupski18
Changhoon Yoo17Mark M. Zalupski18 Tushar Patel1*
Tushar Patel1*Cholangiocarcinoma (CCA) is a heterogeneous group of malignancies arising from the biliary tract. Three main types of CCA are recognized: intrahepatic, distal CCA, and perihilar CCA. These cancers have poor prognosis because they often progress without symptoms and are typically diagnosed at advanced stage. Surgical interventions with microscopically negative resection margins (R0) can be curative but are not an option for nearly two-thirds of patients who present with unresectable disease (1). Moreover, the intrinsic and acquired chemoresistance of these tumors limits responses to therapy (2–4).
Understanding the determinants of chemoresistance in these cancers can improve our knowledge of disease pathogenesis, progression, and help improve therapeutic response. In general, mortality associated with primary liver cancers is higher in males than females, which could be due to sex-dependent biological effects, intrinsic differences in the natural history of tumor progression, or sex-related alterations in therapeutic responses (5). Further, males and females could respond differently to treatment due to sex-dependent variation in metabolism, drug pharmacokinetic or pharmacodynamic activities (6), but the impact of sex on therapeutic response in CCA is not known. In most reports of treatment trials, outcome data from study participants are combined for males and females, which may mask sex-based variation in treatment responses. A glaring gap in treatment trials data is that most trials do not perform randomization by sex. To evaluate the possibility that therapeutic responses in CCA differ by biological sex, we conducted a systematic review of the effect of sex on the outcomes of treatments in reported therapeutic trials.
A systematic search strategy for identifying studies was developed in accordance with the PRISMA guidelines. The approach was prospectively registered on PROSPERO on 19/09/2021 (Registration number CRD42021273679). The strategy was applied to the following databases/registers: PubMed.gov, Clinicaltrials.gov, Cochrane Central Register of Controlled Trials, EMBASE via Ovid, the World Health Organization’s International Clinical Trial Registry Platform, and Google Scholar. Search inputs used combinations of medical subject headings (MeSH) and Boolean operator searching to find both non-randomized and randomized trials. Combinations of the search terms were used, such as: “cholangiocarcinoma” [MeSH], “biliary tract neoplasms” [MeSH], “cholangiocarcinoma” [Tiab], OR “biliary cancer”, AND “Overall survival”. The searches performed, terms used and results for each database and registry are described in Supplementary Tables S1, S2.
Inclusion criteria were defined a priori as any study that had enrolled a minimum of four patients with CCA, with all patients aged 18 years or more and which involved a therapeutic treatment arm. Exclusion criteria included adjuvant therapeutic trials that involved the concomitant use of surgery, radiation, immunotherapy, or other treatments besides drug therapy, trials that involved direct tumoral infusion (e.g., intrahepatic administration) or trials that explicitly focused on palliative care.
Data from all database or registry searches were extracted into excel spreadsheets and included the following information: first author, year, identification number (e.g., PubMed ID, NCT-ID), title, and a link to the full text. Duplicates within datasets were identified and removed through manual and automated cross comparing. Two independent reviewers subsequently reviewed each record for retrieval. Discrepancies in agreement were very few and each of them was discussed together to arrive at consensus. Studies that were accepted by both reviewers were reviewed for specific sex-related outcomes for data extraction. The corresponding author for each study was contacted by email, with a follow-up request for those who did not respond after two weeks. The email included a standardized data request form to the listed corresponding author for each eligible study.
For each study, data for mean age, number of patients, body mass index (BMI), socioeconomic status (SES), history of prior resections and the median and range of overall survival (OS) and progression-free survival (PFS) were requested for males and females separately. All data were subsequently logged and used in the analysis. None of the studies were able to provide SES data. Although not specifically requested, data from studies that provided 95% confidence interval (CI) data was accepted. Sex-specific survival data visualization was performed using bar graphs, scatter plots, and bubble plots. Risk of bias was not assessed due to the lack of sex-based randomization. Each of the studies included had verified in their published reports that written informed consent was obtained from study participants, and that the study protocols conformed to the ethical guidelines of the 1975 Helsinki Declaration as reflected in a priori approvals by their respective institutional human subjects research committees.
The results of the screening and literature searches are outlined in the flow chart (Figure 1). A total of 2,621 records were obtained from all searches, of which 564 records were removed for being duplicates. The remaining 2,057 records were screened for eligibility by two independent reviewers. Of these, 201 were identified as being appropriate for this review by consensus of both reviewers and were selected. Contact information was identified for 184 studies, and the corresponding or senior authors were contacted by e-mail. Of these, 104 did not respond to two separate requests, and 40 had non-functional emails. Amongst those who responded,12 indicated that the requested data was not collected or was missing, 10 responded that they were unable to provide the data or that it was not readily available, 4 met the criteria but provided data for participants that did not meet criteria and 15 provided CCA-specific data for inclusion in this analysis. Each of the 15 studies was further reviewed for appropriateness. Each met the inclusion criteria and the datasets provided were deemed to be suitable for analysis and inclusion in this review.
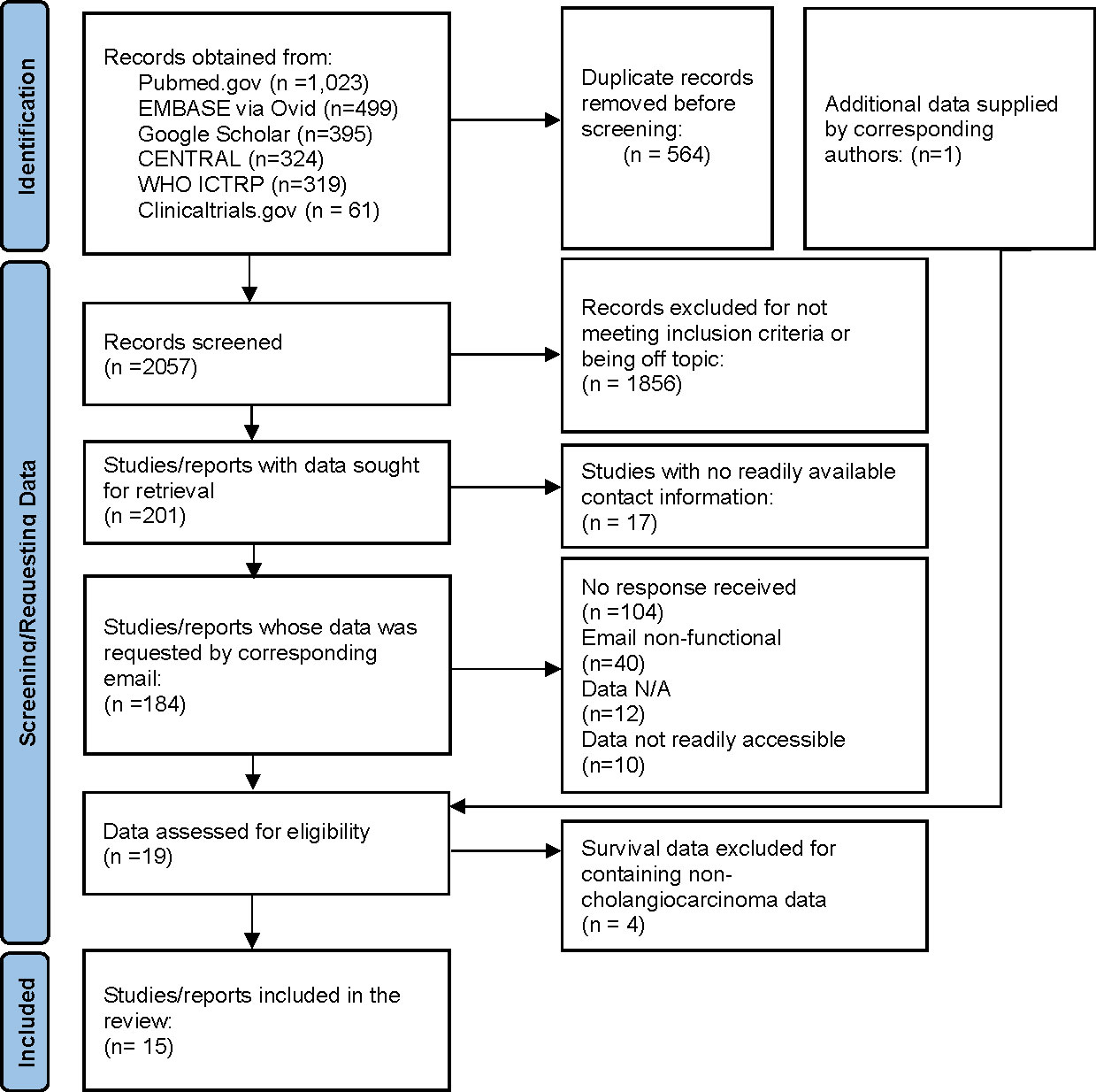
Figure 1 Identification of studies. Flowchart of the systematic search to identify studies and selection of studies included in the analysis.
The fifteen studies reported data from 587 patients with CCA of which 309 were males and 278 were females. Characteristics of these studies are listed in Table 1 (7–21). The trials were performed between 2008 and 2021, and the recruitment sites spanned multiple global locations including North America, Europe, Asia, South America, and Australia. Treatment allocation was randomized in 4 trials and was non-randomized in 11 trials. However, randomization was not performed by sex in any of the studies.
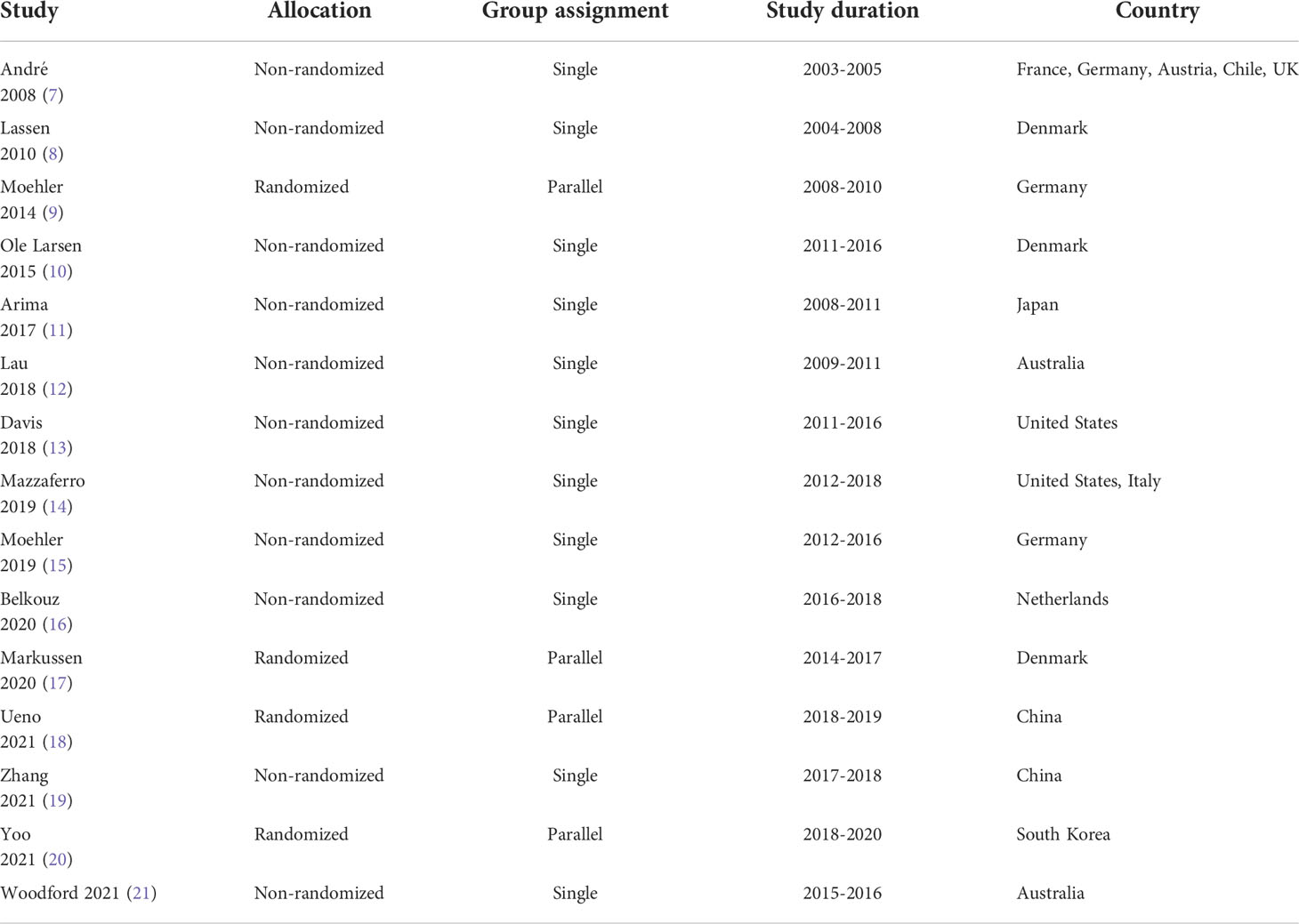
Table 1 Characteristics of studies included in the review.
Of the fifteen studies, four had parallel assignments (i.e., eight treatment groups) whereas 11 had a single group assessment. Therefore, there were 19 separate treatment groups for analysis. Sixteen of the 19 patient groups had a female-to-male mean age ratio between 0.9 and 1.1, indicating similar spread of age across groups. The survival data for males and females in each of these 19 groups is presented in Table 2. All except one of the treatment groups (8) included patients with unresectable or metastatic disease. Sixteen of the 19 treatment groups included patients with either intrahepatic or extrahepatic CCA, while one group included only intrahepatic CCA. Tumor location was not specified in two of the groups (Supplementary Table S3).

Table 2 Survival data of included studies.
The analysis indicated that females have a tendency towards a higher overall survival than males enrolled in treatment trials of CCA (Figure 2). There were several treatment groups that had higher total female overall survival rates, such as derazantinib, capecitabine + nab-paclitaxel, and gemcitabine + cisplatin (GemCis) + afatinib. The differences were most noticeable for FOLFIRINOX treatment in which the female-to-male ratio of median OS was 2.83. The median OS was higher in females in most of the other treatment regimens, with a female-to-male ratio in overall survival above 1.1 in 14 treatment groups. In the rest of the treatment groups, three had ratios ranging from 1.1 to 0.9, and only two had a ratio below 0.9.
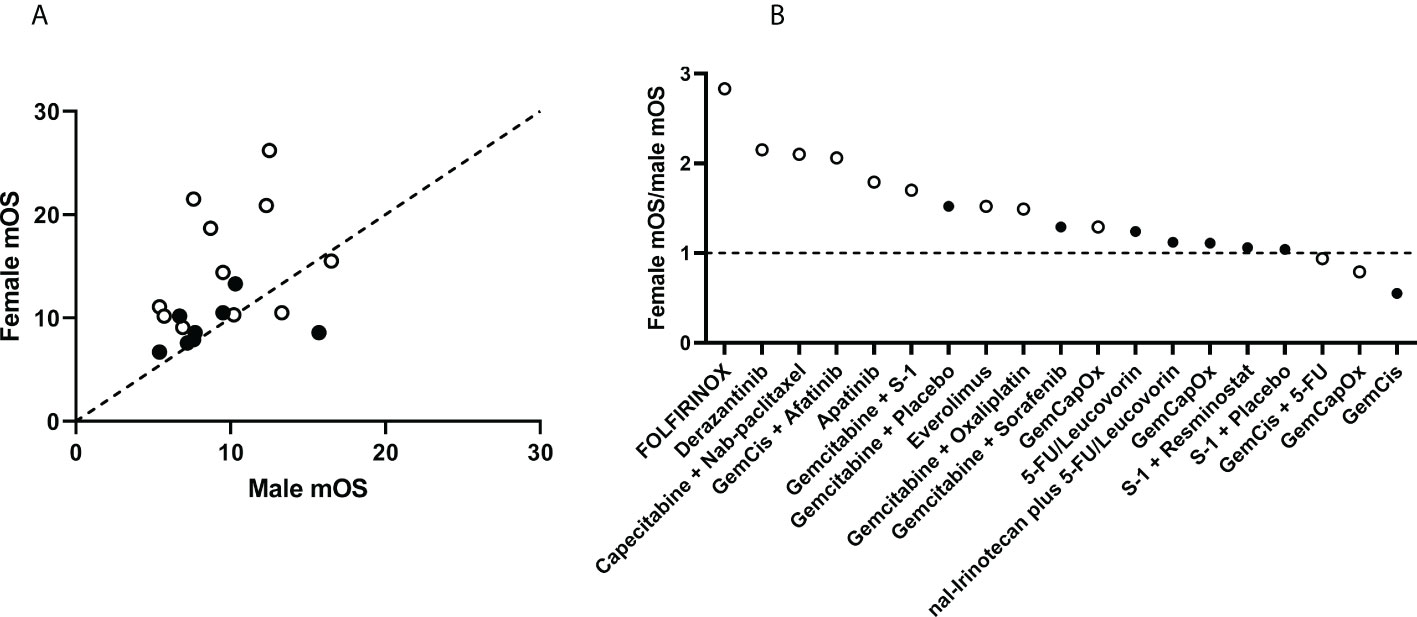
Figure 2 Comparison of median overall survival (OS) in female and male participants in treatment trials of cholangiocarcinoma. (A) Data were obtained from participants in 19 treatment groups from 15 studies. Treatment groups above the dotted line of equivalence have a higher overall survival in females compared with males. (B) The ratio of median OS in females to median OS in males is plotted for each treatment group. Treatments with higher median OS in females are plotted above the dotted line, with ratio >1. Randomized of treatment was performed in studies represented by solid dots, non-randomized studies as open dots.
The data on median PFS in these studies differed from those for overall survival. While differences in median PFS data were observed, these had an equal distribution above and below the equivalence line indicative of varying effects between the sexes (Figure 3). Seven treatment groups had median PFS ratios above 1.1, five had ratios from 1.1-0.9, and seven had ratios below 0.9. Notably, more extreme differences were observed in studies with a smaller sample size, whereas larger studies showed more moderate differences (Figure 4). Of note, higher survival rates were noted in males in only one treatment regimen with GemCis, with a female-to-male ratio < 1.0 for both median OS and median PFS.
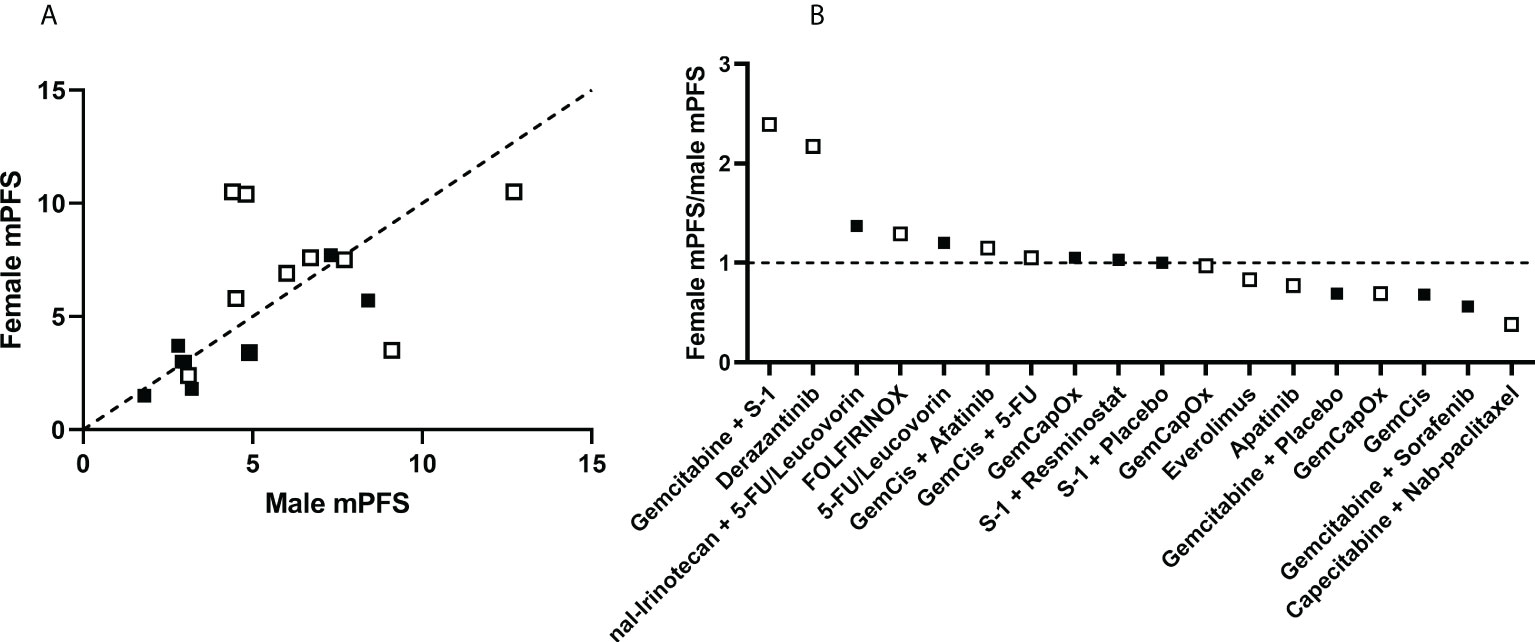
Figure 3 Comparison of disease progression in female and male participants in treatment trials of cholangiocarcinoma. (A) Data were obtained from participants in 19 treatment groups from 15 studies. Treatment groups above the dotted line of equivalence have a higher median progression free survival (mPFS) in females compared with males. (B) The ratio of mPFS in females to mPFS in male is plotted for each treatment group. Treatments with higher mPFS in females are plotted above the dotted line, with ratio >1. Randomized of treatment was performed in studies represented by solid dots, non-randomized studies as open dots.
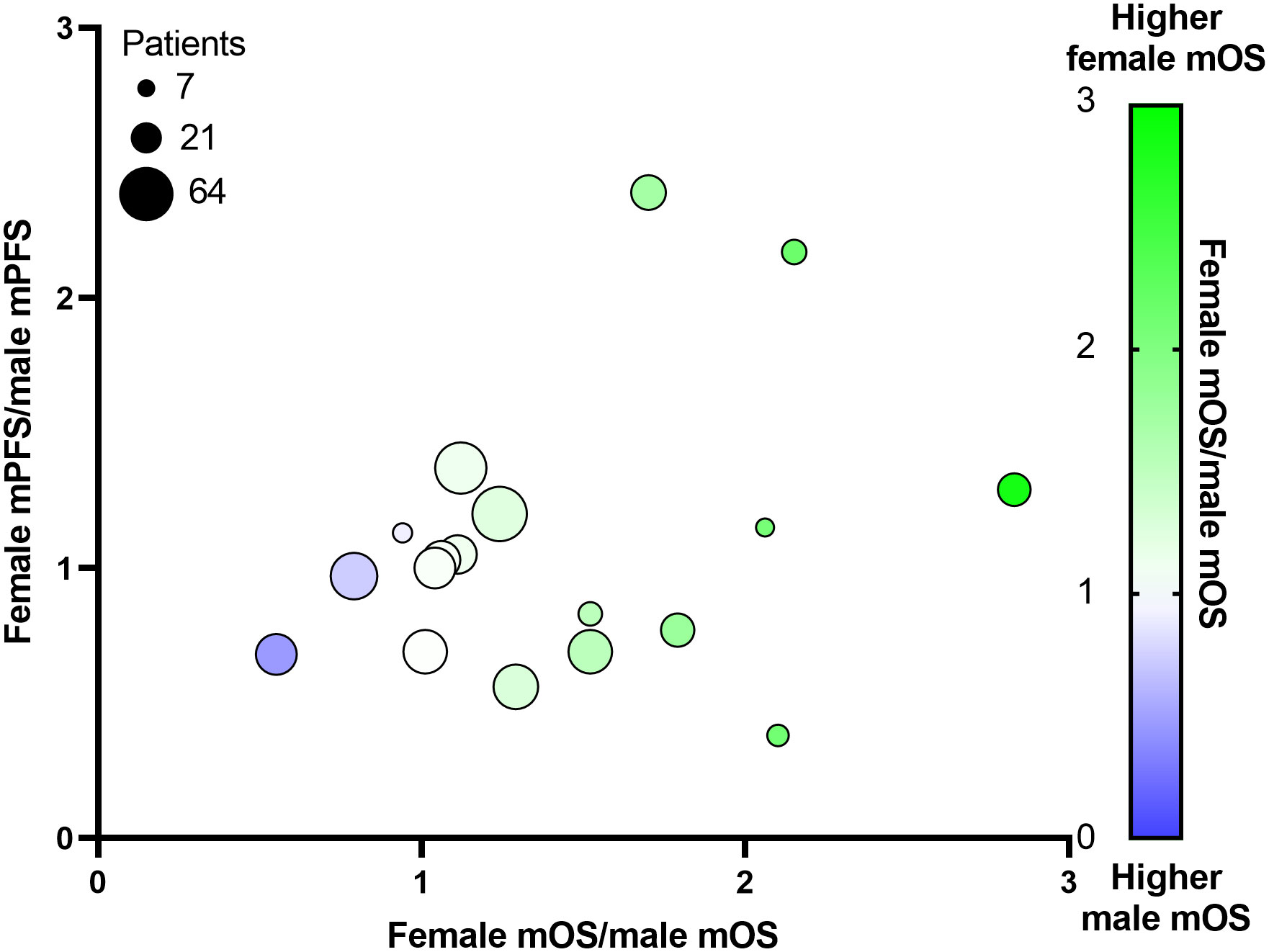
Figure 4 Relationship between study size, median overall survival (mOS) and median progression-free survival (mPFS) in males and female participants of treatment trials in cholangiocarcinoma. The female-to-male ratio of mOS is plotted against the female-to-male ratio of mPFS. The size of the plot is proportional to the number of participants in the treatment group.
Understanding the effects of biological sex on responses to gemcitabine-based regimens is clinically relevant but also of high importance. Both before and more so after the landmark ABC-02 study established GemCis as the standard of care, gemcitabine has been widely used for the treatment of CCA. To evaluate this further, we examined the potential sex-related differences in survival outcomes across treatment regimens containing gemcitabine. Survival data was compiled from 10 treatment groups which included gemcitabine (Table 2, Supplementary Figure S1). Outcomes across treatment groups were heterogeneous, with exception to the gemcitabine, capecitabine, and oxaliplatin (GemCapOx) treatment groups, which had a median OS within 0.2 months of each other. Out of the ten treatment groups, median OS was higher in females in six groups, with the greatest effect noted for treatment with gemcitabine + S-1. For the other four groups, median OS was equivalent (e.g., for GemCapOx) or better in males (e.g. GemCis or gemcitabine + oxaliplatin). While dosage schedules and the number of study participants were comparable across all three GemCapOx treatment groups, an improved OS in males was observed in only one of the three studies (Supplementary Table 3).
As noted above, the biological sex-associated impact on disease-free progression was also notably distinct from those for overall survival. Similar sex-based effects in progression-free and overall survival data were noted for a few treatments (Table 2, Supplementary Figure S1B). For others, sex-based effects varied between disease progression and overall survival. For instance, while median OS was higher in females treated with gemcitabine + sorafenib or gemcitabine + placebo, these were different for median PFS in the same studies. Of note the median PFS was lower in both sexes with sorafenib treatment compared to placebo and suggesting sorafenib might be similarly intolerable for both sexes.
We next analyzed outcomes in treatments which did not contain gemcitabine (Table 2, Supplementary Figure S2). Out of nine treatment groups, median OS was higher in females than in males in seven studies but similar in only two studies. In a randomized trial of 5-FU/leucovorin or 5-FU/leucovorin with nal-irinotecan, overall survival in females exceeded that of males by 0.9 and 1.3 months respectively. However, the same was not true for a randomized study of S-1 + placebo and S-1 + resminostat in which female median OS was only slightly higher (0.3 months) in males indicating then absence of a significant relationship between sex and outcomes. In this trial, male-to-female ratios for median PFS were like those for OS.
While a higher median PFS was observed in females treated with 5-FU/nal-irinotecan (Table 2, Supplementary Figure S2B), the data was more varied in studies with other treatments, with four having higher median PFS in males, and two being similar between sexes. Discordant effects in median PFS and median OS between males and females were noted for other treatment groups, such as with everolimus and capecitabine + nab-paclitaxel.
While gemcitabine has remained a critical part of CCA treatment regimens, there are many novel therapies that have demonstrated verifiable and significant promise. Pemigatinib and ivosidenib, both of which were approved by the Food and Drug Administration in 2020-2021 for selective use in a subgroup of CCA with FGFR2 alterations are evolving options for the treatment of CCA in certain settings. As newer therapeutic regimens undergo testing, it will be pertinent to understand any sex-related effects on survival outcomes.
A major gap in evolving treatments for CCA is an understanding of the effect of biological sex on outcomes of treatment. As treatment options for CCA evolve, this knowledge will be essential not only for the design and conduct of the most appropriate clinical trial designs, but also guide towards appropriate selection of treatment options for patients with CCA. In this analysis, a distinctive sex-related difference in overall survival was observed in an analysis of responses to treatment from participants in completed trials of CCA. The data herein was comprised from 587 patients of which 47% were females. Females enrolled in treatment trials of CCA had a higher OS than males in two-thirds of all treatment groups. In contrast, disease progression, as determined by the median PFS across all treatment groups had similar outcomes between the sexes.
The mortality from CCA is lower among females compared with males in recent data from the United States, with a risk ratio of 0.78 (95% CI 0.77–0.79) (22). Thus, the impact of sex on treatment outcomes is important, and especially so given the increasing CCA incidence and mortality from CCA observed in the United States and many other countries (23). There are several factors that can contribute to sex-dependent differences, such as sex-dependent effects on the underlying liver disease, pathobiological processes or concomitant comorbidities. For example fibrogenesis can occur in a sex-dependent manner in non-alcoholic fatty liver disease. Etiological factors, such as cirrhosis, viral hepatitis, presence and extent of sarcopenia and smoking can also contribute (24). In particular, smoking can impact both first line and neoadjuvant chemotherapy responses in some cancers (25, 26). Variable responses in different types of tumors to therapeutic interventions such as surgical resection and chemotherapy could also contribute to disparities in survival. Most of the studies reported herein aggregated intrahepatic and extrahepatic CCA data precluding tumor type-specific analyses. Complete data on tumor type, underlying liver disease or etiology, or smoking history were not available for the studies reported but warrant specific assessment in future clinical trials. While sex can affect drug metabolism, responses, and resistance, the effect of biological sex on treatment responses has not previously been widely recognized as a potential contributor to these differences. Differences in epigenetic changes between cis and trans participants raises the complexities involved and need for consideration for trans gender identities as well (27).
This study has several limitations. None of the studies involved randomization by sex. Moreover, patient-based characteristics that could potentially confound the observations, such as BMI or SES could not be accounted for. Thus, sex-dependent differences in recruitment, disease severity, BMI, SES may all have contributed. While this may be less likely given the effects were observed across multiple diverse trials, future trials with sex-based randomization and comparability across groups would be necessary to completely evaluate these possibilities. Many of the studies had small sample sizes. While low numbers of patient enrollments are characteristic of many studies of CCA, which is a rare disease, a smaller sample size can skew results of treatment effects. The absence of sex-specific reporting of survival outcomes in reported trials was particularly noteworthy and highlights a major limitation. Of the 184 publications initially identified, few if any reported non-aggregated data on survival in females and males. A further challenge with retrospective systematic reviews is the susceptibility to selection bias introduced due to inaccessible or lost data. In this context, sequestration and non-sharing of trial data by individuals or organizations hampers progress and erodes the trust placed by participants who enroll in trials to advance medical knowledge.
Some drugs such as 5-FU, cisplatin, and nab-paclitaxel have sex-dependent effects in different tissues (28). Sex-dependent expression of phase I and phase II drug metabolizing enzymes can result in differential metabolism and clearance, and thereby impact therapeutic efficacy of many drugs (29, 30). Amongst these, the regulation and expression of cytochrome P450 (CYP) gene and enzyme families are of particular importance as these genes are sex-based, and dependent on enhancer of zest homolog 1 and 2 (31). For example, CYP3A4 has higher expression levels in female livers and has been implicated in the biotransformation of more than 50% of all clinically used drugs (32). Differential regulation of CYP gene and enzyme families could thereby contribute to sex differences in outcomes.
Intrinsic or acquired resistance to drugs contributes to the difficulty in treating CCA. Variable effects on gene expression, and regulation of metabolic pathways can all contribute to sex differences in drug resistance. P-glycoprotein serves as an important ATPase transporter protein that can operate as a drug efflux pump for a variety of drugs. Commonly found in hepatocytes and intestinal enterocytes, overexpression of P-gp is linked to multidrug resistance and worse clinical outcomes in cancer (33). A higher hepatic expression of P-gp in men could thus account for the higher overall mortality rates observed in men with CCA compared with women (34). Hormonal differences can further impact on sex-dependent differences. In addition to direct endocrinological effects, the activity of certain P-gp and CYP isoforms can be regulated by progesterone and estrogen levels, respectively (35, 36). However, the relationships in the liver-related CYP and P-gp isoforms are poorly understood.
The results of this analysis raise awareness and a call for action to consider sex-based differences in outcomes while designing future treatment trials for CCA or in the management of CCA. Randomization based on biological sex, and consideration of gender-based dosing may need to be considered where data on sex differences in drug efficacy and metabolism is available.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
TP and ML contributed equally to the writing of the manuscript; TP oversaw the design and execution of the review; ML performed the systematic searches, data acquisition, and data processing; rest of authors contributed data and/or performed a critical review of the manuscript. All authors contributed to the article and approved the submitted version.
Support for this study was provided by the James C and Sarah K Kennedy Deanship and Alfred D. and Audrey M. Petersen Professorship at Mayo Clinic to TP.
We are grateful for the contributions of all participants in the treatment trials, the investigators who provided data including Wei He and Ulrik Lassen, and for members of the Patel Lab for their insights.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.963753/full#supplementary-material
5-FU, 5-fluorouracil; BMI, body mass index; CI, confidence interval; CYP, cytochrome P450; GemCapOx, gemcitabine, capecitabine, oxaliplatin; GemCis, gemcitabine and cisplatin; FOLFIRINOX, 5-flourouracil, leucovorin, irinotecan, oxaliplatin; iCCA, intrahepatic cholangiocarcinoma; mOS, median overall survival; mPFS, median progression-free survival; Nal-Irinotecan, nanoliposomal irinotecan; P-gp, p-glycoprotein; SES, socioeconomic status.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Huang YK, Wang M, Sun YDi, Costanzo N, Mitchell C, Achuthan A, et al. Macrophage spatial heterogeneity in gastric cancer defined by multiplex immunohistochemistry. Nat Commun (2019) 10(1):3928. doi: 10.1038/s41467-019-11788-4
3. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet (2016) 388(10060):2654–64. doi: 10.1016/S0140-6736(16)30354-3
4. Zhang M, Hu S, Min M, Ni Y, Lu Z, Sun X, et al. Dissecting transcriptional heterogeneity in primary gastric adenocarcinoma by single cell RNA sequencing. Gut (2020). doi: 10.1136/gutjnl-2019-320368
5. Seiwert TY, Burtness B, Mehra R, Weiss J, Berger R, Eder JP, et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): an open-label, multicentre, phase 1b trial. Lancet Oncol (2016) 17(7):956–65. doi: 10.1016/S1470-2045(16)30066-3
6. Desbois M, Udyavar AR, Ryner L, Kozlowski C, Guan Y, Dürrbaum M, et al. Integrated digital pathology and transcriptome analysis identifies molecular mediators of T-cell exclusion in ovarian cancer. Nat Commun (2020) 11(1):5583. doi: 10.1038/s41467-020-19408-2
7. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med (2013) 369(2):134–44. doi: 10.1056/NEJMoa1305133
8. Zhang X, Shi M, Chen T, Zhang B. Characterization of the immune cell infiltration landscape in head and neck squamous cell carcinoma to aid immunotherapy. Mol Ther Nucleic Acids (2020) 22:298–309. doi: 10.1016/j.omtn.2020.08.030
9. Zeng D, Zhou R, Yu Y, Luo Y, Zhang J, Sun H, et al. Gene expression profiles for a prognostic immunoscore in gastric cancer. Br J Surg (2018) 105(10):1338–48. doi: 10.1002/bjs.10871
10. Jiang Y, Zhang Q, Hu Y, Li T, Yu J, Zhao L, et al. ImmunoScore signature: A prognostic and predictive tool in gastric cancer. Ann Surg (2018) 267(3):504–13. doi: 10.1097/SLA.0000000000002116
11. Wang S, Xiong Y, Zhang Q, Su D, Yu C, Cao Y, et al. Clinical significance and immunogenomic landscape analyses of the immune cell signature based prognostic model for patients with breast cancer. Brief Bioinform (2021) 22(4):bbaa311. doi: 10.1093/bib/bbaa311
12. Shen S, Wang G, Zhang R, Zhao Y, Yu H, Wei Y, et al. Development and validation of an immune gene-set based prognostic signature in ovarian cancer. EBioMedicine (2019) 40:318–26. doi: 10.1016/j.ebiom.2018.12.054
13. Yu G, Wang LG, Han Y, He QY. clusterProfiler: an r package for comparing biological themes among gene clusters. Omics (2012) 16(5):284–7. doi: 10.1089/omi.2011.0118
14. Jiang S, Zhang Y, Zhang X, Lu B, Sun P, Wu Q, et al. GARP correlates with tumor-infiltrating T-cells and predicts the outcome of gastric cancer. Front Immunol (2021) 12:660397. doi: 10.3389/fimmu.2021.660397
15. Zhang X, Xiao R, Lu B, Wu H, Jiang C, Li P, et al. Kinase DYRK2 acts as a regulator of autophagy and an indicator of favorable prognosis in gastric carcinoma. Colloids Surf B Biointerfaces (2022) 209(Pt 1):112182. doi: 10.1016/j.colsurfb.2021.112182
16. Camp RL, Dolled-Filhart M, Rimm DL. X-Tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res (2004) 10(21):7252–9. doi: 10.1158/1078-0432.CCR-04-0713
17. Wang J, Xu P, Hao Y, Yu T, Liu L, Song Y, et al. Interaction between DNMT3B and MYH11 via hypermethylation regulates gastric cancer progression. BMC Cancer (2021) 21(1):914. doi: 10.1186/s12885-021-08653-3
18. Huang X, Zhang G, Tang T, Liang T. Identification of tumor antigens and immune subtypes of pancreatic adenocarcinoma for mRNA vaccine development. Mol Cancer (2021) 20(1):44. doi: 10.1186/s12943-021-01310-0
19. Fakih M, Ouyang C, Wang C, Tu TY, Gozo MC, Cho M, et al. Immune overdrive signature in colorectal tumor subset predicts poor clinical outcome. J Clin Invest (2019) 129(10):4464–76. doi: 10.1172/JCI127046
20. Kulkarni HS, Elvington ML, Perng YC, Liszewski MK, Byers DE, Farkouh C, et al. Intracellular C3 protects human airway epithelial cells from stress-associated cell death. Am J Respir Cell Mol Biol (2019) 60(2):144–57. doi: 10.1165/rcmb.2017-0405OC
21. Nagarsheth N, Wicha MS, Zou W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat Rev Immunol (2017) 17(9):559–72. doi: 10.1038/nri.2017.49
22. Hu J, Yu A, Othmane B, Qiu D, Li H, Li C, et al. Siglec15 shapes a non-inflamed tumor microenvironment and predicts the molecular subtype in bladder cancer. Theranostics (2021) 11(7):3089–108. doi: 10.7150/thno.53649
23. Comprehensive molecular characterization of gastric adenocarcinoma. Nature (2014) 513(7517):202–9. doi: 10.1038/nature13480
24. Cristescu R, Lee J, Nebozhyn M, Kim KM, Ting JC, Wong SS, et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat Med (2015) 21(5):449–56. doi: 10.1038/nm.3850
25. Pernot S, Terme M, Radosevic-Robin N, Castan F, Badoual C, Marcheteau E, et al. Infiltrating and peripheral immune cell analysis in advanced gastric cancer according to the Lauren classification and its prognostic significance. Gastric Cancer (2020) 23(1):73–81. doi: 10.1007/s10120-019-00983-3
26. Mendiola M, Pellinen T, Ramon-Patino JL, Berjon A, Bruck O, Heredia-Soto V, et al. Prognostic implications of tumor-infiltrating T cells in early-stage endometrial cancer. Mod Pathol (2022) 35(2):256–65. doi: 10.1038/s41379-021-00930-7
27. Pare L, Pascual T, Segui E, Teixido C, Gonzalez-Cao M, Galvan P, et al. Association between PD1 mRNA and response to anti-PD1 monotherapy across multiple cancer types. Ann Oncol (2018) 29(10):2121–8. doi: 10.1093/annonc/mdy335
28. Tosi A, Cappellesso R, Dei Tos AP, Rossi V, Aliberti C, Pigozzo J, et al. The immune cell landscape of metastatic uveal melanoma correlates with overall survival. J Exp Clin Cancer Res (2021) 40(1):154. doi: 10.1186/s13046-021-01947-1
29. Wang P, Chen Y, Long Q, Li Q, Tian J, Liu T, et al. Increased coexpression of PD-L1 and TIM3/TIGIT is associated with poor overall survival of patients with esophageal squamous cell carcinoma. J Immunother Cancer (2021) 9(10):e002836. doi: 10.1136/jitc-2021-002836
30. Mezheyeuski A, Bergsland CH, Backman M, Djureinovic D, Sjöblom T, Bruun J, et al. Multispectral imaging for quantitative and compartment-specific immune infiltrates reveals distinct immune profiles that classify lung cancer patients. J Pathol (2018) 244(4):421–31. doi: 10.1002/path.5026
31. Lee KH, Kim EY, Yun JS, Park YL, Do SI, Chae SW, et al. The prognostic and predictive value of tumor-infiltrating lymphocytes and hematologic parameters in patients with breast cancer. BMC Cancer (2018) 18(1):938. doi: 10.1186/s12885-018-4832-5
32. Su S, Liao J, Liu J, Huang D, He C, Chen F, et al. Blocking the recruitment of naive CD4+ T cells reverses immunosuppression in breast cancer. Cell Res (2017) 27(4):461–82. doi: 10.1038/cr.2017.34
33. Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol (2002) 3(11):991–8. doi: 10.1038/ni1102-991
34. Adams S, Gray RJ, Demaria S, Goldstein L, Perez EA, Shulman LN, et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol (2014) 32(27):2959–66. doi: 10.1200/JCO.2013.55.0491
35. Yoshihara K, Shahmoradgoli M, Martínez E, Vegesna R, Kim H, Torres-Garcia W, et al. Inferring tumour purity and stromal and immune cell admixture from expression data. Nat Commun (2013) 4:2612. doi: 10.1038/ncomms3612
36. Şenbabaoğlu Y, Gejman RS, Winer AG, Liu M, Van Allen EM, de Velasco G, et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol (2016) 17(1):231. doi: 10.1186/s13059-016-1092-z
37. Hornburg M, Desbois M, Lu S, Guan Y, Lo AA, Kaufman S, et al. Single-cell dissection of cellular components and interactions shaping the tumor immune phenotypes in ovarian cancer. Cancer Cell (2021) 39(7):928–944.e6. doi: 10.1016/j.ccell.2021.04.004
38. Zhang D, He W, Wu C, Tan Y, He Y, Xu B, et al. Scoring system for tumor-infiltrating lymphocytes and its prognostic value for gastric cancer. Front Immunol (2019) 10:71. doi: 10.3389/fimmu.2019.00071
Keywords: Biliary cancers, chemotherapy, gemcitabine, therapeutic response, survival
Citation: Ledenko M, Antwi SO, Arima S, Driscoll J, Furuse J, Klümpen H-J, Larsen FO, Lau DK, Maderer A, Markussen A, Moehler M, Nooijen LE, Shaib WL, Tebbutt NC, André T, Ueno M, Woodford R, Yoo C, Zalupski MM and Patel T (2022) Sex-related disparities in outcomes of cholangiocarcinoma patients in treatment trials. Front. Oncol. 12:963753. doi: 10.3389/fonc.2022.963753
Received: 07 June 2022; Accepted: 25 July 2022;
Published: 11 August 2022.
Edited by:
Sergio A. Gradilone, University of Minnesota Twin Cities, United StatesReviewed by:
Luca Fabris, University of Padua, ItalyCopyright © 2022 Ledenko, Antwi, Arima, Driscoll, Furuse, Klümpen, Larsen, Lau, Maderer, Markussen, Moehler, Nooijen, Shaib, Tebbutt, André, Ueno, Woodford, Yoo, Zalupski and Patel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tushar Patel, UGF0ZWwudHVzaGFyQG1heW8uZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.