
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 09 January 2023
Sec. Cancer Epidemiology and Prevention
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.957325
This article is part of the Research Topic Clinical Cancer Research in Vulnerable Populations View all 7 articles
 Dorah Mrema1,2*
Dorah Mrema1,2* James Samwel Ngocho1,3
James Samwel Ngocho1,3 Alex Mremi1
Alex Mremi1 Maryam Amour4Rogathe Machange1,3Benjamin C. Shayo2,5
Maryam Amour4Rogathe Machange1,3Benjamin C. Shayo2,5 Julius P. Alloyce6
Julius P. Alloyce6 Evaline Ndosi6Beatus T. Shirima1Device Fande1Rahma Shehoza1
Evaline Ndosi6Beatus T. Shirima1Device Fande1Rahma Shehoza1 Emmanuel Balandya4
Emmanuel Balandya4 Bruno Sunguya4
Bruno Sunguya4 Stephen E. Mshana7Alfred K. Mteta1Eligius Lyamuya4John Bartlett8
Stephen E. Mshana7Alfred K. Mteta1Eligius Lyamuya4John Bartlett8 Blandina T. Mmbaga1,3
Blandina T. Mmbaga1,3Background: Cervical cancer (CC) is more prevalent in women living with human immunodeficiency virus (HIV) infection compared to the general population. The magnitude is high among all countries burdened with HIV—Tanzania is no exception. Despite the unprecedented risk, women living with HIV (WLHIV) may not be aware of the risk and might have unfounded beliefs thereof. This study aimed to determine the knowledge, awareness, and beliefs on CC screening among WLHIV attending a clinic at the Kilimanjaro Christian Medical Centre (KCMC) in Northern Tanzania.
Methods: This hospital-based cross-sectional study was conducted among 327 WLHIV attending care and treatment clinic (CTC) at KCMC. A pre-tested questionnaire was used to collect quantitative data. Both descriptive and regression methods were used to determine CC knowledge, awareness, and beliefs as well as factors associated with knowledge of CC among WLHIV using SPSS version 23.
Results: Participants’ mean age was 46 ± 10.4 years. Although just half (54.7%) of WLHIV had insufficient knowledge of CC, the majority of the participants (83.5%) were able to recognize at least three risk factors, but with limited understanding of symptoms and prevention. The majority held positive beliefs on CC and screening practices. Factors associated with good knowledge of CC included being married (AOR: 3.66, 95% CI: 1.84–7.28), having used ART for at least 2 years (AOR: 4.08, 95% CI: 1.36–12.21), and having previously screened for CC (AOR: 1.62, 95% CI: 1.01–2.59).
Conclusion: WLHIV attending care and treatment center had insufficient knowledge about CC screening. To further improve screening and treatment for CC, at both facility and community levels, targeted awareness and education campaigns are warranted.
Cervical cancer (CC) is the fourth most common cause of cancer-related deaths with over 300,000 deaths per year worldwide (1, 2). Approximately 85% of CC deaths occur in low- and middle-income countries (LMICs). It is the most diagnosed cancer among Tanzanian women, and the leading cause of cancer-related morbidity and mortality among women in sub-Saharan Africa (SSA) and in Tanzania (3) (4). The annual incidence of CC is 9,770 cases per 100,000 women with a mortality rate of 6,695 (5). Early treatment of precancerous lesions may reduce the incidence by an estimated 80% (2). Limited access to prevention and treatment programs increases the prevalence of advanced disease compared to high-income countries where primary and secondary prevention programs aid early detection and increase survival rates (2). Increasing CC screening coverage has been reported to reduce the CC incidence.
Women and girls contribute to 53% of 38 million people living with human immunodeficiency virus globally (6). The burden varies from one region and country to another, with more than two-thirds of the global burden of new HIV infections in SSA (7). Women living with HIV (WLHIV) are four to five times more likely to develop invasive CC compared to their counterparts in the general population. Routine screening for pre-invasive lesions remains one of the most important public health interventions that can halt the growing burden of CC (4, 8).
Addressing the burden of CC through prevention requires a knowledgeable and well-informed population, especially those at risk. The challenges of low public awareness and overall low healthcare-seeking behavior among WLHIV need to be addressed in promoting CC prevention (9–11). In 2014 in Tanzania, the Ministry of Health (MoH) introduced an integrated screening of CC within Care and Treatment Clinics (CTC) for HIV. Under this approach, women testing positive for HIV are required to start CC screening during the initiation of antiretroviral therapy (ART) and are followed up annually.
However, hindrances towards early detection include poor knowledge, limited awareness, and wrong beliefs associated with CC screening among women (12). Beliefs that cancer is untreatable have been reported to negatively affect implementation of early detection of CC among women. The belief that pap smear is painful further contributes to poor participation in CC screening (13). Lack of knowledge among WLHIV hinders CC prevention and treatment (14, 15). The knowledge gap in late-stage presentation is among the factors behind the high mortality rate in low- and middle-income countries (LMICs) (16). The challenge is more apparent in rural than in urban areas (17, 18). Evidence is scarce regarding CC knowledge, awareness, and beliefs among WLHIV in this setting. Therefore, this study was designed to assess the level of knowledge, awareness, and beliefs of CC among HIV-infected women in Tanzania who visited the CTC at Kilimanjaro Christian Medical Centre (KCMC).
This hospital-based cross-sectional study was conducted at the CTC in KCMC, a zonal referral hospital in Northern Tanzania located in Moshi urban district. KCMC hospital is among the four zonal referral hospitals in Tanzania and receives patients from five different regions of Northern Zone, including self-referrals. The CTC provides follow-up, enrollment of HIV patients including CD4 cell count, HIV viral load testing, education, and counseling in addition to other services.
The study population included WLHIV attending the KCMC-CTC during the study period, June to September 2020. It included WLHIV aged 18–70 years who were followed for at least 1 year from the date of their HIV diagnosis. Approximately 800 WLHIV attended CTC at KCMC during that time.
The sample size was obtained using the precision approach with a single proportion (19). Through this approach, of the 800 WLHIV who attended CTC during the study period, a total of 327 women consented to participate and met the inclusion criteria and thus were recruited into this study. A systematic sampling method was employed to obtain the study sample. Since not all participants attended in the specific clinic day, we started with the first client of the day and used the sampling interval of two to select the subsequent participants until the end of that clinic day. All potential participants who came to CTC for follow-up visit in every clinic day were checked for eligibility criteria at the entrance desk of which the sequential numbers were given according to the arrival order. Also, to avoid multiple enrollments of the same participants, we used stickers on participant case record.
The dependent variables of this study were knowledge, awareness, and beliefs on CC. Knowledge about CC was measured by asking participants if they had ever heard of CC, and knowledge of its symptoms and signs, risk factors, and prevention. Knowledge of the signs and symptoms was measured using 7 items; risk factors, 10 items; and prevention, 6 items. Our pre-tested questionnaire was developed with questions adapted from a tool that was used and validated in Ethiopia (20). Each correct response was given a score of 1; otherwise, a score of 0 was given when the respondent gives a wrong response or does not know the correct response. The computation of the score was made; if the participants identified at least three risk factors, they were regarded to have good knowledge, and if they identified at least three signs or symptoms of CC, they were also deemed to have good knowledge; this was the same for prevention methods: if participants identified at least three methods for prevention of CC, they were regarded to have good knowledge. Scores below these thresholds were considered poor. The conclusive definition of this categorization was from our tool and according to other studies (20).
Participants were considered “aware” if they mentioned at least one of the known methods for CC screening. These are visual inspection with acetic acid (VIA) and pap smear; otherwise, they were considered not aware about CC. Participants unable to mention at least one of these methods was regarded as “not aware”. Beliefs on CC screening were measured by using Likert scale questions. This tool is validated and has been used in educational studies in Tanzania (21). Additionally, we assessed the participants’ source of information concerning CC by using multiple response questions.
Independent variables included social characteristics and information on HIV status and CC, such as age in years, marital status, education level, occupation, number of children, ethnicity, duration living with HIV in years, duration on ART in years, and current treatment. Age was categorized as ≤45 years and ≥45 years. Marital status was characterized as single/never married, married, and divorced/widow. The level of education was categorized into three groups: primary or no formal education for those women with no formal or primary education, secondary level for women who attend at least one class in secondary school, and university/college level for those with university education level. Participant’s occupation was categorized into two: employed and unemployed. Number of children was dichotomized as having ≤2 and having ≥3.
A pre-tested questionnaire was used to gather data on baseline characteristics (age, level of education, marital status, occupation, and clinical characteristics), awareness, knowledge, attitude, and beliefs of CC and CC screening. This questionnaire was prepared in English and translated to Swahili; the local language used by almost everyone in Tanzania. Prior to data collection, the research team conducted a 2-day training for data collectors to familiarize them with the data collection tools, ethics, and data collection techniques. Fourth year medical students, two diploma nurses, and one master’s degree graduate nurse participated in data collection. The tool was pre-tested among 15 women with the aim of correcting inappropriate responses. We did not have changes on the developed tool. HIV data were collected from participants’ clinic records known as CTC card no 2 (CTC2). The filled questionnaires were reviewed and cross-checked before entry into SPSS 23.0 for statistical analysis.
The cleaned dataset was analyzed using descriptive and regression techniques to address the specific objectives. The descriptive analyses were carried out to describe participants. To assess the factors associated with CC knowledge among WLHIV, regression analyses using binary and multivariable logistic regression analysis were performed. The univariate analyses were used to determine the factors associated with the knowledge of CC. Variables that showed associations with the knowledge and those at p < 0.2 were entered into the multivariate analysis model. Age was also added into the multivariate model despite the assumption of the level of association above. A 95% confidence interval with a p-value of less than 0.05 was regarded as statistically significant.
A total of 327 WLHIV with a mean age (SD) of 46 ± 10.4 years were enrolled in this study. The majority [212 (64.8%)] had primary or non-formal education; 140 (44.6%) were divorced/widowed. More than half were unemployed [280 (85.6%)], with 47 (14.4) employed. The median number of children was 2 with an interquartile range of 2–3 children. The participants had a median duration of 12 (7–14, 22) years since being confirmed HIV positive with the majority [200 (61.2%)] having had at least 10 years since being confirmed HIV positive. The median duration on ART use was 9 (5–12, 22) years, with most of them [286 (87.5%)] being women still on first-line treatment (Table 1).
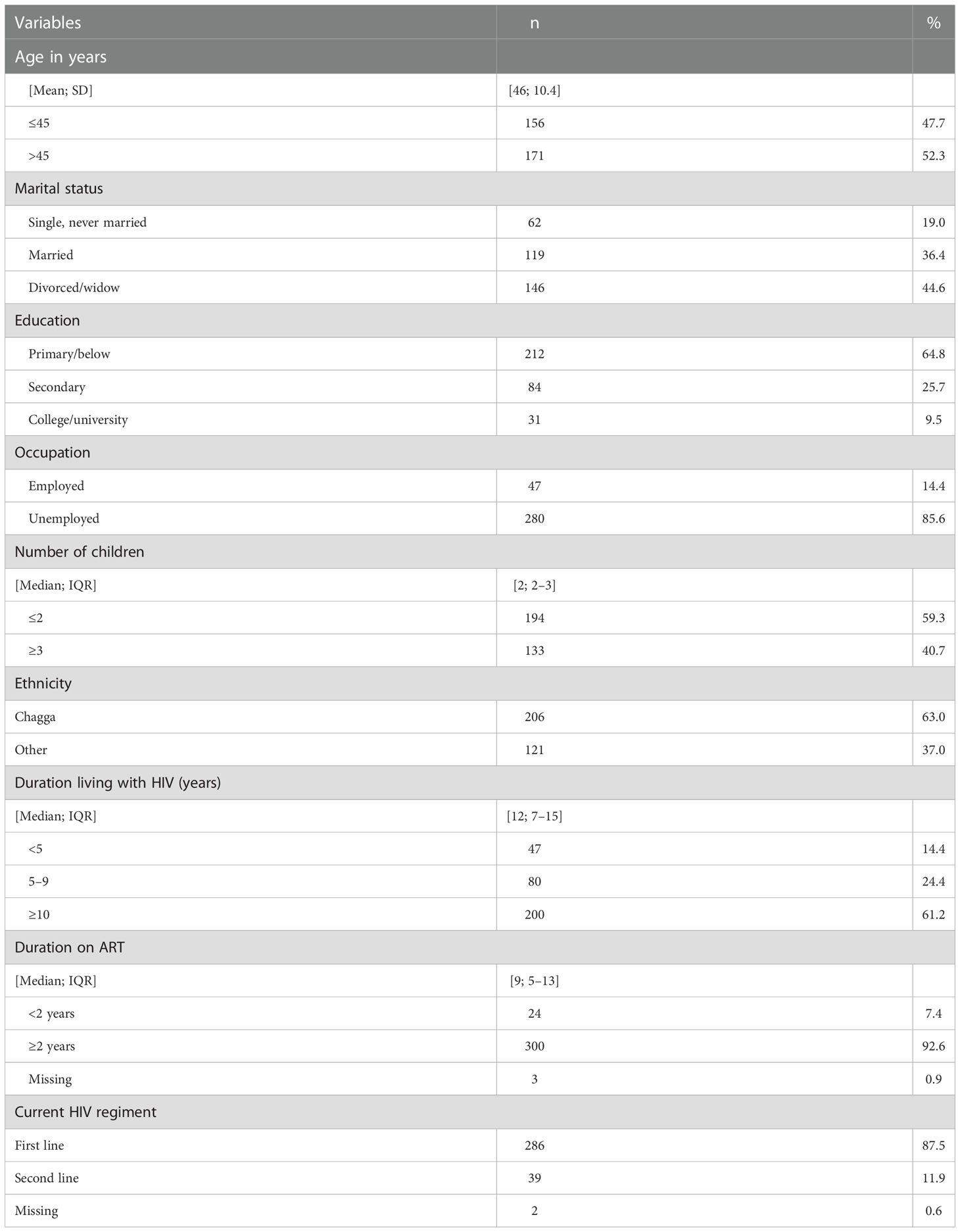
Table 1 Characteristics of the participants (N = 327).
Regarding specific knowledge of CC, the majority of women (273; 83.5%) recognized at least three risk factors for CC. The major risk factors of CC reported by the participants included being HIV infected, low body immunity, early sexual practices, and multiple sexual partners. However, 75 (22.9%) women did not recognize that HIV-infected women are at risk of having CC, whereas many of them [182 (55.7%)] reported the use of oral contraceptives as increasing the risk of CC (Table 2). With regard to knowledge of symptoms and signs of CC, 191 (58.4%) women were able to mention some clinical symptoms of CC. These included unusual bleeding and pain after sexual intercourse, postmenopausal excessive vaginal bleeding, abnormal bleeding between periods, and other signs like swelling of the vagina and severe abdominal pain (Table 2).

Table 2 Knowledge and awareness of CC among WLHIV.
A majority of WLHIV [288 (88.1%)] agreed that CC is preventable; regular medical checkup/screening, vaccines, and delaying first sexual intercourse were the most identified preventive measures. Ninety-six percent of the participants reported previously hearing about CC screening; however, their knowledge of CC screening methods was poor. About 51.1% were able to mention the VIA method and only 15.3% mentioned the pap smear method (Table 2).
In addition, most (90.8%) of the participants reported having heard information about CC from healthcare providers (doctor or nurses), followed by information from radio/television (72.7%) and relatives/friends (54.3%). Other sources of information on CC were flyers, magazines/newspaper, at work, church, and social media (such as WhatsApp, Twitter, and Instagram).
Regarding the cause of CC, 40 (12.2%) indicated that they agreed CC is caused by the HIV virus. When it came to screening for CC, using Likert scale mean scores, 195 (59.6%) (score of 4.5) WLHIV strongly agreed that CC screening generally gives a sense of control over the course of the disease whereas 163 (49.8%) (score 4.2) reported that it is worth doing CC screening. Furthermore, 158 (48.3%) and 97 (29.7%) agreed and strongly agreed that CC screening detects pre-cancerous cells before symptoms, respectively. In addition, 207 (63.3%) strongly agreed that CC screening helps in prevention of carcinoma of the cervix. Low scores were observed on the perception that CC screening is embarrassing, very painful, and not necessary if there are no signs and symptoms, and that they were afraid to take the cancer screening test and/or worried about being diagnosed with CC (Table 3).
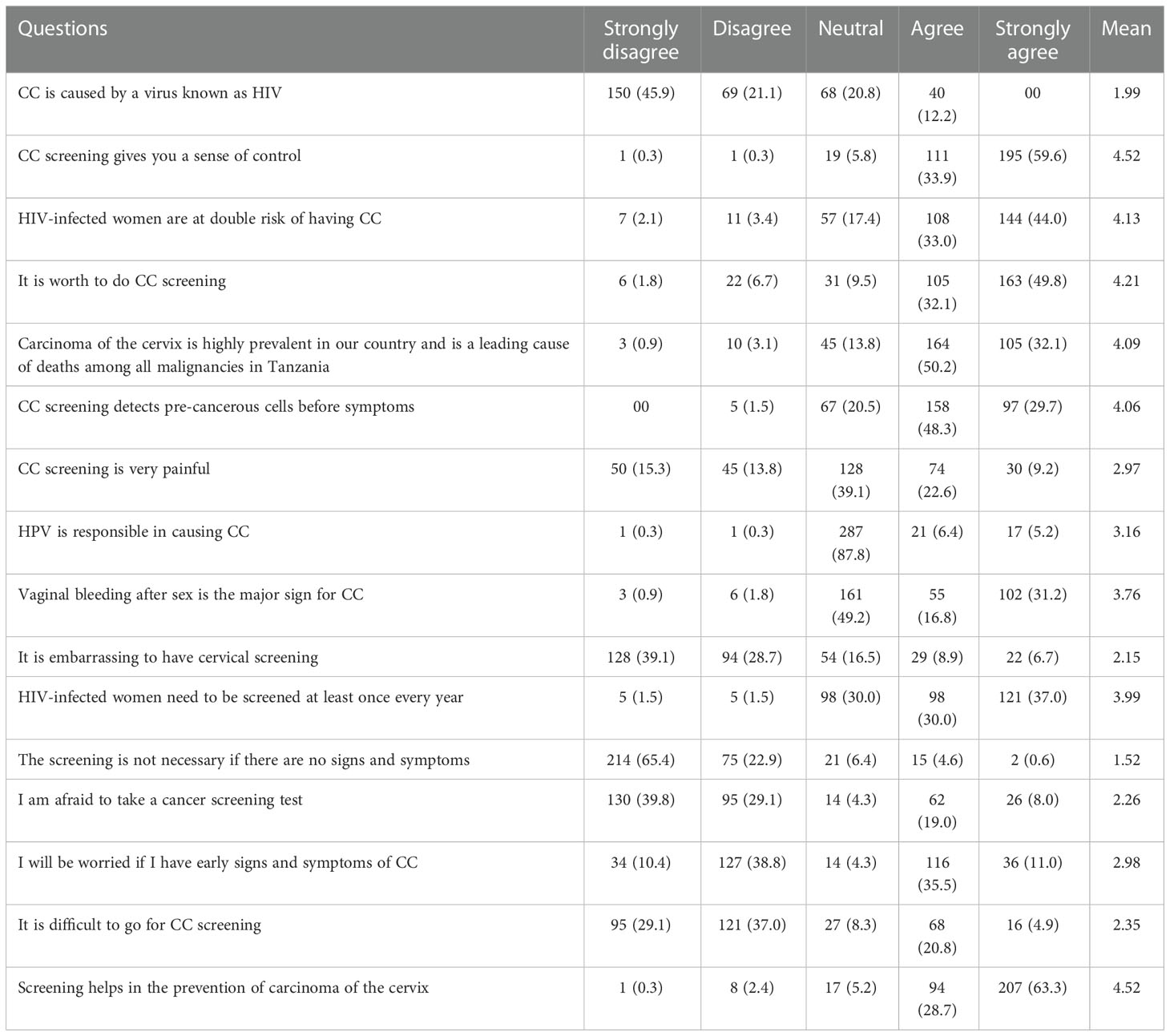
Table 3 Beliefs of CC and its screening services among WLHIV (N = 327).
Following bivariate analysis, variables that were significantly associated with knowledge of CC included married women (COR: 3.26, 95% CI: 1.64–6.46) as compared to unmarried or single; duration on ART of 2 years or more (COR: 3.37, 95% CI: 1.21–9.37); and ever being screened for CC (COR: 1.81, 95% CI: 1.15–2.85). After adjusting for covariates and confounders in multivariate analysis, married women were almost four times more likely to have knowledge of CC compared to their counterparts who were not married (AOR: 3.66, 95% CI: 1.84–7.28). Those who were widowed/divorced were twice more likely to have knowledge of CC compared to single women (AOR: 1.89, 95% CI: 0.95–3.75). Women who had a long duration on ART (more than 2 years) were four times more likely to understand CC compared to those with a shorter duration (less than 2 years) on ART (AOR: 4.08, 95% CI: 1.36–12.21). Furthermore, women who had ever screened for CC were almost two times more likely to be knowledgeable on CC compared to WLHIV who had never been screened for CC (AOR: 1.6295% CI: 1.01–2.59) (Table 4).
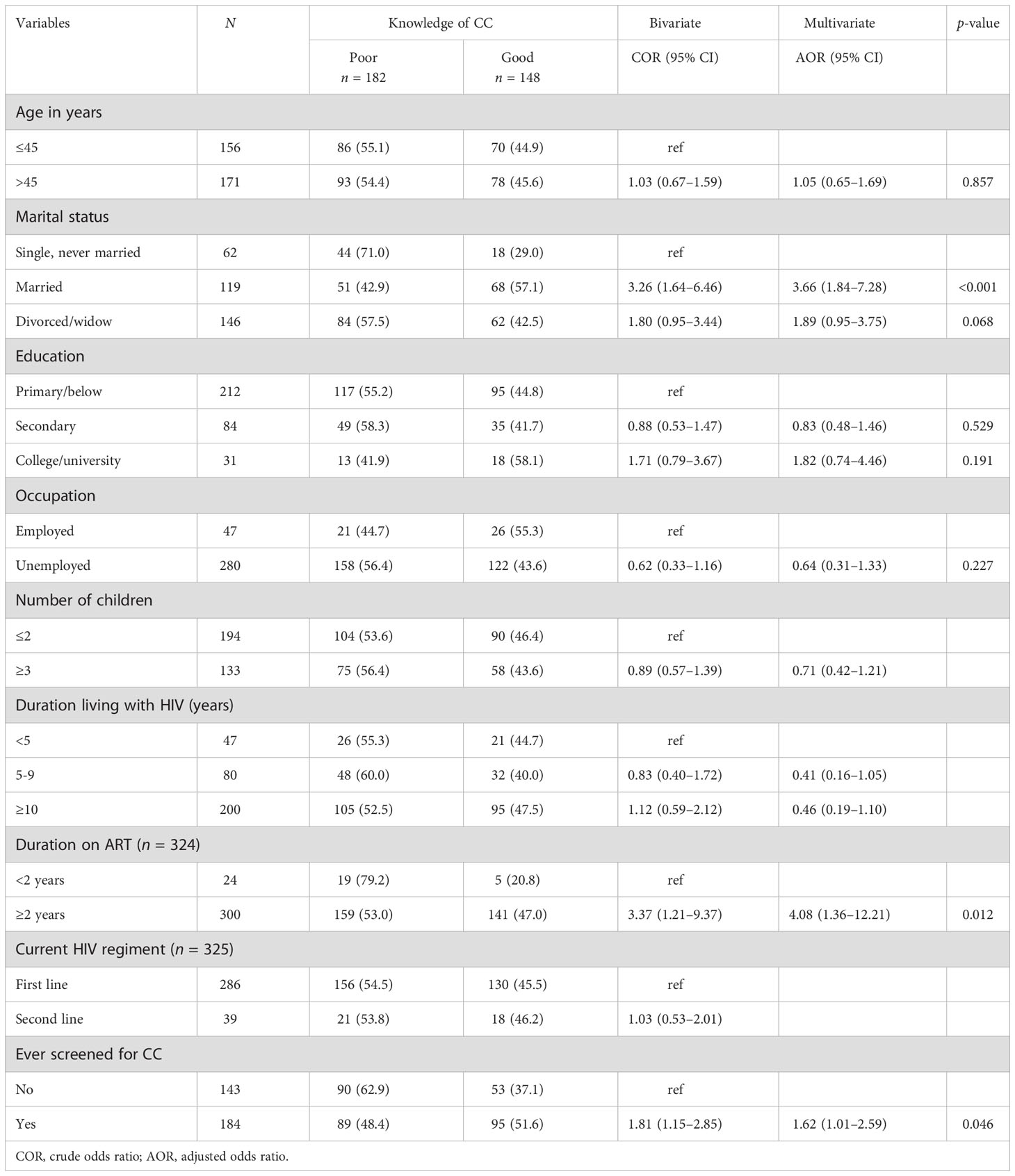
Table 4 Factors associated with knowledge of CC among women living with HIV (N = 327).
CC screening information is vital to facilitate the procedure and women’s willingness to screen (23). CC screening in Tanzania includes visual inspection with acetic acid (VIA), pap smear, and, for some women, an HPV test. Both pap smear and HPV tests use cells taken from the cervix. Participants from the current study had a limited knowledge on pap smear and HPV test while few were aware of VIA. This is different from the study done by Fatima Ahmed AL-Hammad et al., which shows that 85% of participants were aware of the pap smear (24) and from the study conducted on Saudi Arabian women (25).
Knowledge of CC is important in reducing the risks, and increases the ability to prevent and control CC. Having adequate knowledge of CC was reported to increase the utilization of CC screening services among WLHIV (26). We found that 8 out of 10 women could name at least three risk factors for CC and knew it was avoidable, but they had little knowledge of symptoms and screening options. Similar findings reported the deficiency of knowledge about CC in the general population (27) with additional findings in Ethiopia (20). The inadequate grasp of CC symptoms and prevention in this study may be related to a lack of awareness among study participants, especially about the natural history of CC and the belief of CC screening. Understanding CC risk factors, causes, and prevention is crucial for women to make behavior changes.
WLHIV in this study had limited information on CC and its screening methods. The other study backs this up by reporting that WLHIV had trouble recognizing the early signs of CC (28). Similar to Shiferaw et al., who found limited understanding of CC screening methods among WLHIV, it noted that majority of participants were not able to correctly determine when women should seek care for CC screening (29). Similar findings were reported by Faustini Kimondo et al. (30). Wanyenze from Uganda identified that about half of WLHIV had limited awareness of CC screening (31). Lacking awareness of CC screening methods among WLHIV might be a result of unfriendly protocols used to educate women during their appointment visits at CTCs. This implies that WLHIV are merely informed to go for CC screening without proper information regarding CC and HIV-related risks, which causes some to have misconceptions and underlines the value of CC screening. In the research carried out by Ghufran Jassim, the difference was noticed where most of the participants were able to recognize CC and the screening methods particularly VIA and pap smear (32).
Regarding beliefs of CC screening, the majority of WLHIV felt that CC screening gives a sense of control, that it is worth doing, that it finds pre-cancerous cells before symptoms, and that it prevents cervix cancer. However, according to several women, it was reported that CC screening is uncomfortable, painful, and unnecessary if there are no symptoms. Some were afraid of a CC screening for fear of early indications and symptoms; it is hard to go. The results from the current study resemble those reported in a study from Kenya, which reported that negative beliefs of CC screening are high among WLHIV (33). These results indicate the importance of proper interventions to improve the screening technology, and it seems that the current technology, particularly the VIA method, is not user-friendly and is less appealing to the majority of women.
Married women have better CC knowledge than single ones. This can be explained by the probability of sexually transmitted signs and symptoms that cause women to seek medical attention. We suspect that married women shared CC knowledge with their spouses, which facilitate the follow up. This is different from the study conducted in Bangladesh that revealed that unmarried women were more knowledgeable on CC compared to their counterparts (34).
Having more than 2 years of ART was associated with better CC knowledge. This implies that long-time CTC attendees have heard CC information multiple times. This differs from a study conducted in Gurage zone, Southern Ethiopia, which found that individuals with plans to screen for CC and those with a family history of CC knew more about CC (35). This implies that knowledge of CC and screening procedures varies depending on various factors, and no single element explains the difference. We conducted a quantitative study, and the results do not convince us that there are other, more important aspects to consider than training and discouraging negative beliefs and misperceptions about CC screening in order to achieve the intended outcomes. For future interventions, a qualitative study could provide in-depth examinations of CC and the screening repercussions among WLHIV.
To our knowledge, this is the first study to explore knowledge, awareness, and beliefs on CC screening among WLHIV in this setting. Our findings have some limitations that should be taken into consideration when interpreting the results. This study was done in a referral hospital setting; therefore, the results might not resemble those of WLHIV who do not have access to a hospital. Furthermore, this study was completed at one site; therefore, results cannot be generalized to all HIV care and treatment centers in Tanzania.
There was a lack of CC knowledge among HIV-positive women receiving treatment at the study facility in Northern Tanzania (KCMC). While some individuals acknowledged being aware of the HPV vaccine as a means of avoiding CC, the majority were unable to name any of the clinical signs or symptoms associated with the CC. Only half of them were even aware that VIA is used in CC screening, indicating a widespread lack of knowledge about the topic. Positive attitudes toward CC and its screening services were displayed by the participants. Knowledge of CC was observed to increase with marital status, length of time on ART, and history of CC screening.
Posters on CTC clinic walls and fliers to WLHIV could increase CC knowledge. Using the ongoing Northern zone prevention effort to educate this specific group by empowering CTC HCPs to link CC and CTC services throughout care. Increase WLHIV awareness and screening. Future studies should examine the challenges to CC screening from the healthcare provider’s perspective using qualitative approaches.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The ethical approval was sought from Kilimanjaro Christian Medical University College research ethics committee prior to the commencement of this study. This was followed by permission from the KCMC authority to use the CTC clinic for study enrollment. The patients/participants provided their written informed consent to participate in this study.
DM: Conceived the research idea, designed the study, performed data analysis, prepared the manuscript and subsequent revisions. BTS, DT, and RS: Involved in data collection. EN: Participated in data entry management and manipulation for analysis. JA: Performed statistical analysis, and reviewed and edited the manuscript. JN, BCS, AM, MA, RM, EB, BS, SM, AKM, EL, and JB: Critically read and commented on the manuscript before submission to the journal. BM: Conceived the idea for the study and gave advice in designing the study, analysis, and revision of the manuscript. All authors contributed to the article and approved the submitted version.
Research reported in this publication was supported by the Fogarty International Centre of the National Institutes of Health under Award Number R25 TW011227. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors would like to thank the institutions KCMUCo, MUHAS, and CUHAS for the grant award and KCMUCo and KCMC for permitting DM to attend the Community of Young Research Peers (CYRP) fellowship. The authors also show their appreciation to the CYRP of three institutions (KCMUCo, MUHAS, and CUHAS) through THET for their valuable contributions during the development of this manuscript. The acknowledgement is also extended to the study participants for their valuable information and to data collectors and mentors for their commitment.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CC, cervical cancer; CTC, care and treatment clinic; HIV, human immunodeficiency virus; HCP, healthcare provider; HPV, human papilloma virus; KCMC , Kilimanjaro Christian Medical Centre; KCMUCo, Kilimanjaro Christian Medical University College; LMIC, low- and middle-income countries; SSA, sub-Saharan Africa; VIA, visual inspection with acetic acid; WHO, World Health Organization; WLHIV, women living with human immunodeficiency virus.
1. Bray F, Jacques F, Soerjomataram I. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018), 68394–424. doi: 10.3322/caac.21492
3. Arbyn M, Weiderpass E, Bruni L, De Sanjosé S, Saraiya M, Ferlay J, et al. Articles estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob Heal (2020) 8(2):191–203. doi: 10.1016/S2214-109X(19)30482-6
4. Chambuso RS, Shadrack S, Lidenge SJ, Mwakibete N, Medeiros RM. Influence of HIV/AID son cervical cancer: A retrospective study from Tanzania. J Glob Oncol (2017) 3(1):72–8. doi: 10.1200/JGO.2015.002964
5. ICO/IARC. Information center on HPV and cancer. Tanzania Hum Papillomavirus Related Cancers Fact Sheet 2018. (2018), 1–10.
9. Simms KT, Steinberg J, Caruana M, Smith MA, Lew J, Soerjomataram I, et al. Articles impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020 – 99: A modelling study. Lancet Oncol (2019), 1–14. doi: 10.1016/s1470-2045(18)30836-2
10. Liu G, Sharma M, Tan N. HIV-Positive women have higher risk of HPV infection, precancerous lesions, and cervical cancer: A systematic review and meta-analysis. PMC. (2019) 32(6):795–808. doi: 10.1097/QAD.0000000000001765
11. Massad LS, Xie X, Burk R, Keller MJ, Minkoff H, Souza GD, et al. Long-term cumulative detection of human papillomavirus among HIV seropositive women. AIDS. (2014) 28(17):1–8. doi: 10.1097/QAD.0000000000000455
12. Mutambara J, Mutandwa P, Mahapa M, Chirasha V, Nkiwane S, Shangahaidonhi T. Knowledge, attitudes and practices of cervical cancer screening among women who attend traditional churches in Zimbabwe. J Cancer Res Pract (2017) 4(2):53–8. doi: 10.1016/j.jcrpr.2017.02.001
13. Ma GX, Gao W. Health beliefs associated with cervical cancer screening among Vietnamese americans. J WOMEN’S Heal (2013) 22(3):276–88. doi: 10.1089/jwh.2012.3587
14. Singer R, Henke A, Alloyce JP, Serventi F, Massawe A, Henke O. Repetitive cancer training for community healthcare workers: an effective method to strengthen knowledge and impact on the communities: Results from a pilot training at Kilimanjaro region, Tanzania. J Cancer Educ (2019), 1–8. doi: 10.1007/s13187-019-01648-6
15. Busolo DS, Woodgate RL. Cancer prevention in Africa: A review of the literature. Glob Health Promot. (2015) 22(2):31–9. doi: 10.1177/1757975914537094
16. Morhason-Bello IO, Odedina F, Rebbeck TR, Harford J, Dangou JM, Denny L, et al. Challenges and opportunities in cancer control in Africa: A perspective from the African organisation for research and training in cancer. Lancet Oncol (2013) 14(4):e142–51. doi: 10.1016/S1470-2045(12)70482-5
17. Peters LM, Soliman AS, Bukori P, Mkuchu J, Ngoma T. Evidence for the need of educational programs for cervical screening in rural Tanzania. J Cancer Educ (2012) 23(1):1–7. doi: 10.1007/s13187-009-0018-9
18. Moshi FV, Vandervort EB, Kibusi SM. Cervical cancer awareness among women in Tanzania : An analysis of data from the 2011-12 Tanzania HIV and malaria indicators survey. Int J of Chronic Dis (2018) 2018(5):1–7. doi: 10.1155/2018/2458232
19. Cornish PR. Statistics: An introduction to sample size calculations precision-based sample size calculations. (2006) 2:1–5.
20. Getahun F, Mazengia F, Abuhay M, Birhanu Z. Comprehensive knowledge about cervical cancer is low among women in Northwest Ethiopia. BMC Cancer [Internet]. (2013) 13(1):1. doi: 10.1186/1471-2407-13-2
21. Kisanga DH, Ireson G. Test of e-learning related attitudes (TeLRA) scale: Development, reliability and validity study. Int J Educ Dev using Inf Commun Technol (2016) 12(1):20–36.
23. Kasraeian M, Hessami K, Vafaei H, Asadi N, Foroughinia L, Roozmeh S, et al. Gynecologic oncology reports patients ‘ self-reported factors in fl uencing cervical cancer screening uptake among HIV-positive women in low- and middle-income countries : An integrative review. Gynecol Oncol Rep (2020) 33(6):100596. doi: 10.1016/j.gore.2020.100596
24. Al-hammadi FA, Al-tahri F, Al-ali A, Nair SC. Limited understanding of pap smear testing among women, a barrier to cervical cancer screening in the United Arab Emirates. Asian Pac J Cancer Prev (2017) 18:3379–87. doi: 10.22034/APJCP.2017.18.12.3379
25. Id NAA. Knowledge and intentions regarding the pap smear test among Saudi Arabian women. PlosOne (2021) 1–9. doi: 10.1371/journal.pone.0253850
26. Assefa AA, Astawesegn FH, Eshetu B. Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, hawassa town, Ethiopia: A cross-sectional study. BMC Health Serv Res (2019) 19(1):1–11. doi: 10.1186/s12913-019-4718-5
27. Henke A, Kluge U, Borde T, Mchome B, Serventi F, Henke O. Tanzanian Women´s knowledge about cervical cancer and HPV and their prevalence of positive VIA cervical screening results. data from a prevention and awareness campaign in northern Tanzania, 2017–2019. Glob Health Action. (2021) 14(1):1–16. doi: 10.1080/16549716.2020.1852780
28. Nkurunziza C, Ghebre R, Magriples U, Ntasumbumuyange D, Bazzett-matabele L. Gynecologic oncology reports healthcare provider challenges to early detection of cervical cancer at primary healthcare level in Rwanda. Gynecol Oncol Rep (2021) 37:100810. doi: 10.1016/j.gore.2021.100810
29. Shiferaw N, Brooks MI, Salvador-davila G, Lonsako S, Kassahun K, Ansel J, et al. Knowledge and awareness of cervical cancer among HIV-infected women in Ethiopia. Hindawi Publ Corp Obstet Gynecol Int (2016) 2016:1–9. doi: 10.1155/2016/1274734
30. Kimondo FC, Kajoka HD, Mwantake MR, Amour C, Mboya IB. Knowledge, attitude, and practice of cervical cancer screening among women living with HIV in the Kilimanjaro region, northern Tanzania. Cancer Rep (2021) 2):1–8. doi: 10.1002/cnr2.1374
31. Wanyenze RK, Bwanika JB, Beyeza-kashesya J, Arinaitwe J, Matovu JKB, Gwokyalya V, et al. Uptake and correlates of cervical cancer screening among HIV-infected women attending HIV care in Uganda. Glob Health Action. (2017) 10(1):1–12. doi: 10.1080/16549716.2017.1380361
32. Jassim G, Obeid A, Nasheet HA Al. Knowledge , attitudes , and practices regarding cervical cancer and screening among women visiting primary health care centres in Bahrain. BMC Public Health (2018) 18:1–6. doi: 10.1186/s12889-018-5023-7
33. Heena H, Durrani S, Alfayyad I, Riaz M, Tabasim R, Parvez G, et al. Knowledge, attitudes, and practices towards cervical cancer and screening amongst female healthcare Professionals: A cross-sectional study. J Oncol (2019) 2019:1–9. doi: 10.1155/2019/5423130
34. Alam NE, Islam MS, Rayyan F, Ifa HN, Khabir MIU, Chowdhury K, et al. Lack of knowledge is the leading key for the growing cervical cancer incidents in Bangladesh: A population based, cross-sectional study. PloS Glob Public Heal (2022) 2(1):e0000149. doi: 10.1371/journal.pgph.0000149
Keywords: cervical cancer, WLHIV, knowledge, HIV infection, awareness and Tanzania
Citation: Mrema D, Ngocho JS, Mremi A, Amour M, Machange R, Shayo BC, Alloyce JP, Ndosi E, Shirima BT, Fande D, Shehoza R, Balandya E, Sunguya B, Mshana SE, Mteta AK, Lyamuya E, Bartlett J and Mmbaga BT (2023) Cervical cancer in Northern Tanzania—What do women living with HIV know. Front. Oncol. 12:957325. doi: 10.3389/fonc.2022.957325
Received: 31 May 2022; Accepted: 09 December 2022;
Published: 09 January 2023.
Edited by:
Philip Robert Debruyne, Kortrijk Cancer Centre, BelgiumReviewed by:
Donaldson Conserve, George Washington University, United StatesCopyright © 2023 Mrema, Ngocho, Mremi, Amour, Machange, Shayo, Alloyce, Ndosi, Shirima, Fande, Shehoza, Balandya, Sunguya, Mshana, Mteta, Lyamuya, Bartlett and Mmbaga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dorah Mrema, ZG9yYWhtcmVtYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.