 Guangmin Guan
Guangmin Guan Zhemin Li
Zhemin Li Qi Wang
Qi Wang Xiangji Ying
Xiangji Ying Fei Shan
Fei Shan Ziyu Li
Ziyu Li
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol., 28 October 2022
Sec. Gastrointestinal Cancers: Gastric and Esophageal Cancers
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.955181
This article is part of the Research TopicReviews in Gastrointestinal CancersView all 35 articles
Background: The optimal indications of staging laparoscopy in gastric cancer to detect peritoneal carcinomatosis are still controversial. We performed this systematic review and meta-analysis to quantify the relevance of the preoperative factors with peritoneal carcinomatosis to explore the indications of staging laparoscopy.
Materials and methods: Systematic searches were conducted using Medline, Embase, and the Cochrane Library in December 2021. On the basis of calculating the odds ratio (OR) of each factor, we quantified the association between the risk factors and peritoneal carcinomatosis such as clinical T/N stage, Borrmann type, and tumor markers, using meta-analysis with a random-effects model.
Results: A total of 21 case-control studies and one cohort study were obtained. T stage, N stage, and differentiation degree were most widely studied, with OR values of 2.96 (95% CI: 1.87–4.69), 1.22 (95% CI: 0.86–1.73), and 1.91 (95% CI: 1.42–2.56), respectively. Among all the factors, elevated CA125 (OR = 19.45, 95% CI: 4.71–80.30), Borrmann type IV (OR = 7.68, 95% CI: 3.62–16.27), and large tumor diameter (OR = 5.12, 95% CI: 2.55–10.31) had the highest OR. In particular, CA125 had the best predictability for peritoneal carcinomatosis but was only mentioned by three articles.
Conclusions: There was a cognitive gap between the awareness and importance of risk factors for peritoneal carcinomatosis. In addition to T4 stage, patients with factors with high OR, such as Borrmann type IV, large tumor diameter, and elevated CA125, should undergo staging laparoscopy.
There were nearly 1.07 million new cases of gastric cancer in 2020, with incidence ranking fifth and mortality ranking fourth among malignant tumors (1). Peritoneal carcinomatosis (PC), including macroscopic carcinomatosis (P1) and positive cytology (CY1), is the most common metastasis of gastric cancer (2, 3). Current examination methods, such as CT and MRI, are not effective in detecting PC. It was reported that the sensitivity of CT in diagnosing PC changed from 25% to 50.9% and often at a relatively advanced stage (4–6). There is no evidence that PC could be diagnosed effectively by MRI.
The guidelines for gastric cancer recommend staging laparoscopy (SL) combined with peritoneal cytology as the best method for detecting PC (7–9). Its sensitivity changes from 85% to 98% and its specificity is close to 100% (10, 11). However, SL needs to be carried out under general anesthesia, which will increase the cost to patients, and SL could be more cost-effective if used selectively (12). However, the indications for SL of the guidelines are inconsistent. Japanese institutions chose patients with a more advanced stage like bulky lymph nodes or large Borrmann type III to undergo SL (7), whereas Western countries tend to apply SL to all patients with resectable tumors (13). This study aims to summarize the preoperative risk factors of PC to screen patients that are suitable for SL.
The study was performed following the PRISMA statements for systematic reviews and meta-analyses including observational studies. We searched the databases of PubMed, Embase, MEDLINE, and the Cochrane Library for studies that were published before December 2021 using the search strategy “((gastric [Title/Abstract]) OR (stomach [Title/Abstract]) OR (gastroesophageal [Title/Abstract])) AND ((staging laparoscopy [Title/Abstract]) OR (diagnostic laparoscopy [Title/Abstract]))”. In addition, the references cited in the publications were manually searched to identify additional relevant studies. Only studies published in English were included. No institutional review board approval was required for this literature review. This review was not registered.
Studies included in this systematic review and meta-analysis were required to meet the following criteria: 1. patients were pathologically diagnosed with gastric cancer; 2. PC was diagnosed by SL or open surgery; and 3. PC was diagnosed before any anti-tumor treatment. Studies were excluded on the basis of the following criteria: 1. patients were diagnosed with recurrent gastric cancer; 2. patients were diagnosed clearly as stage IV or with distant metastasis by CT or other non-invasive methods; 3. patients suffered from other malignant tumors at the same time; and 4. patients had a history of malignant tumors.
Two investigators (GMG and ZML) independently screened titles, abstracts, and full texts of the studies for eligibility. Disagreement was resolved between the two reviewers through discussion or, if needed, adjudication by a third reviewer (ZYL). The following information from the included studies were collected in the same way: first author, year of publication, country of patients, duration of study, inclusion and exclusion criteria, sample size, median or mean age, gender, the definition of PC, diagnostic methods of PC, and OR values of risk factors. We would extract the original data to calculate it when feasible, if needed. More specifically, in the latest Japanese guideline for gastric cancer, both P1 and CY1 were defined as M1 stage, so we did the same (7).
We quantified the association between risk factors and PC such as age and gender, using meta-analysis with a random-effects model, and presented the results with forest plots. Heterogeneity was tested with Cochran’s Q-test, with P-value < 0.1 indicating heterogeneity, and quantified by the I² statistic with values of <25%, 25%–50%, and >50% corresponding to low, moderate, and high degrees of heterogeneity, respectively. Then, we examined publication bias with the funnel plot and Egger’s test. All analyses were conducted in the statistical software Review Manager (RevMan version 5.3; The Nordic Cochrane Center, Copenhagen, Denmark). P-value < 0.05 was considered to be statistically significant.
PRISMA flow chart is shown in Figure 1. There were 520 potentially relevant studies initially identified through the database according to the predefined search strategy. In addition, five studies were obtained manually. Five studies were excluded by duplicate checking. A total of 443 studies were excluded after scanning the title and abstract, and the remaining 77 studies were further reviewed by the full-text view. Of these 77 studies, 50 studies were removed because of the lack of clinical information of patients. Five studies were removed because the objects were not PC (one study about chemotherapy, one study about complications, and three studies focusing on other malignant tumors). Finally, 22 studies were included in the meta-analysis.
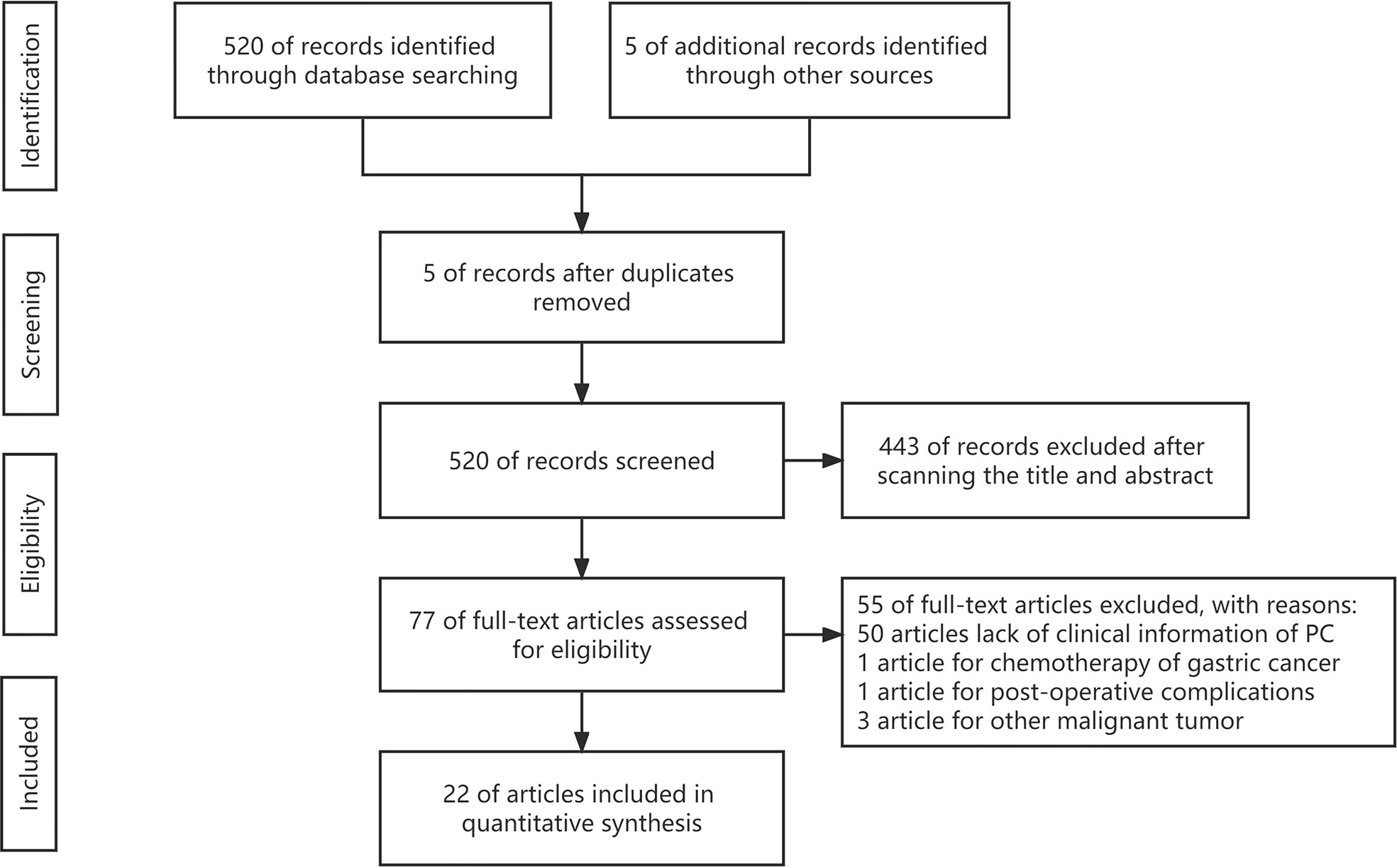
Figure 1 Flow diagram.
The characteristics of all studies are summarized in Table 1. The risk factors mentioned in the studies that may be related to PC and the number of studies for each factor are shown in Table 2. PC was defined as P1 and/or CY1 in nine studies, as only P1 in nine and only CY1 in four. The funnel charts of all results can be found in the supplementary materials.
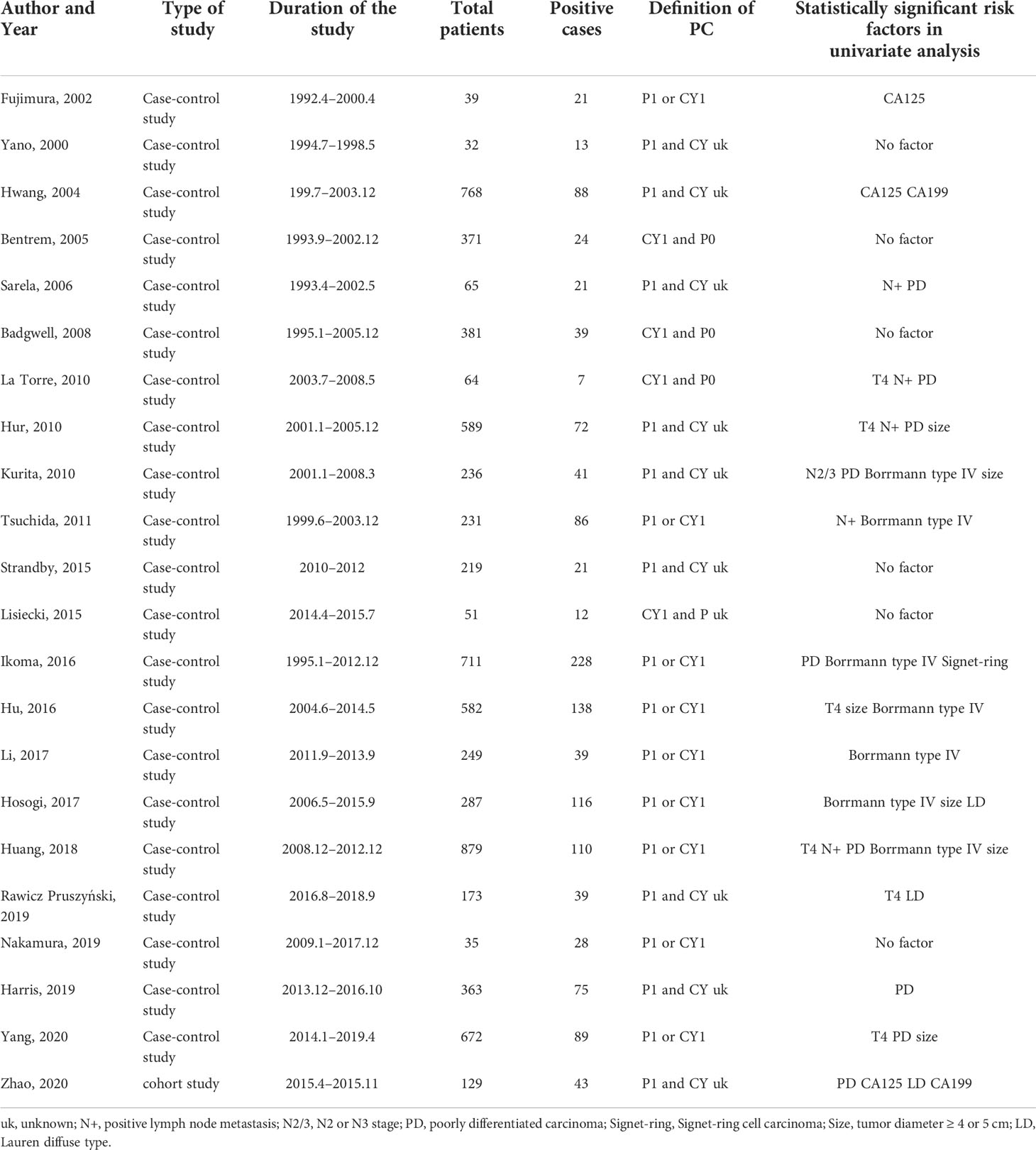
Table 1 Baseline characteristics of the included studies.
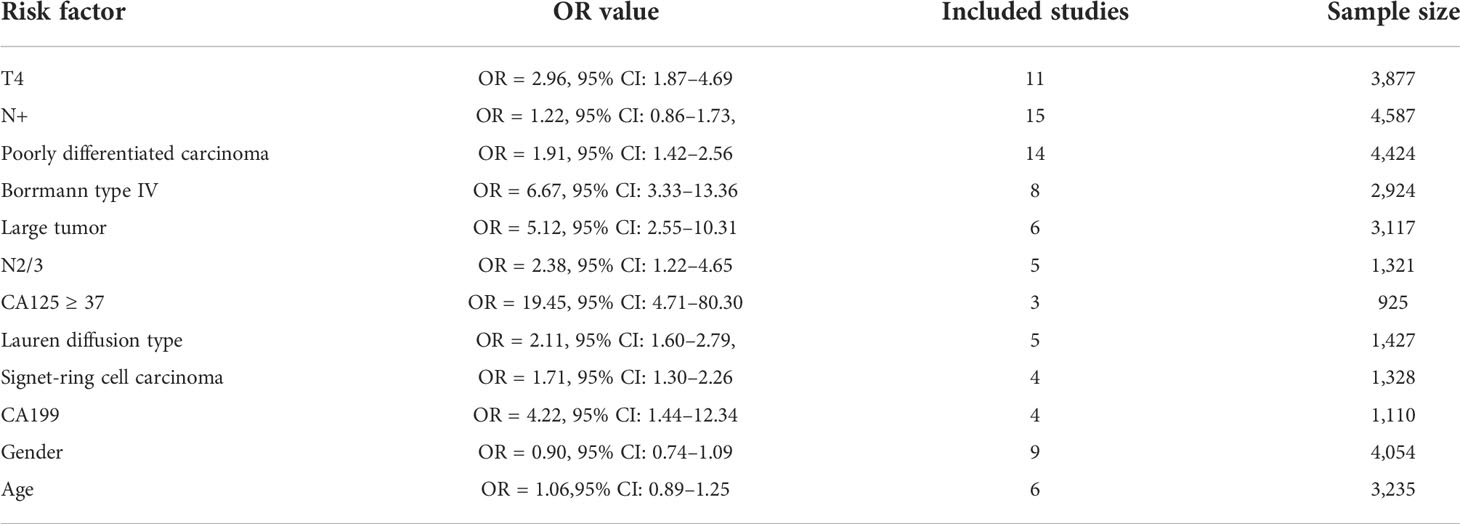
Table 2 Risk factors and OR value of the pooled results.
Eleven studies, with 3,877 patients, from 2008 to 2020 were included (10, 14–23). The sample size of the studies varied from 49 to 879.
The pooled results revealed that patients with T4 stage had a higher proportion in the PC group compared with the ones in the non-PC group; the difference was statistically significant; OR = 2.96, 95% CI: 1.87–4.69, P < 0.0001; I² = 73% (Figure 2).
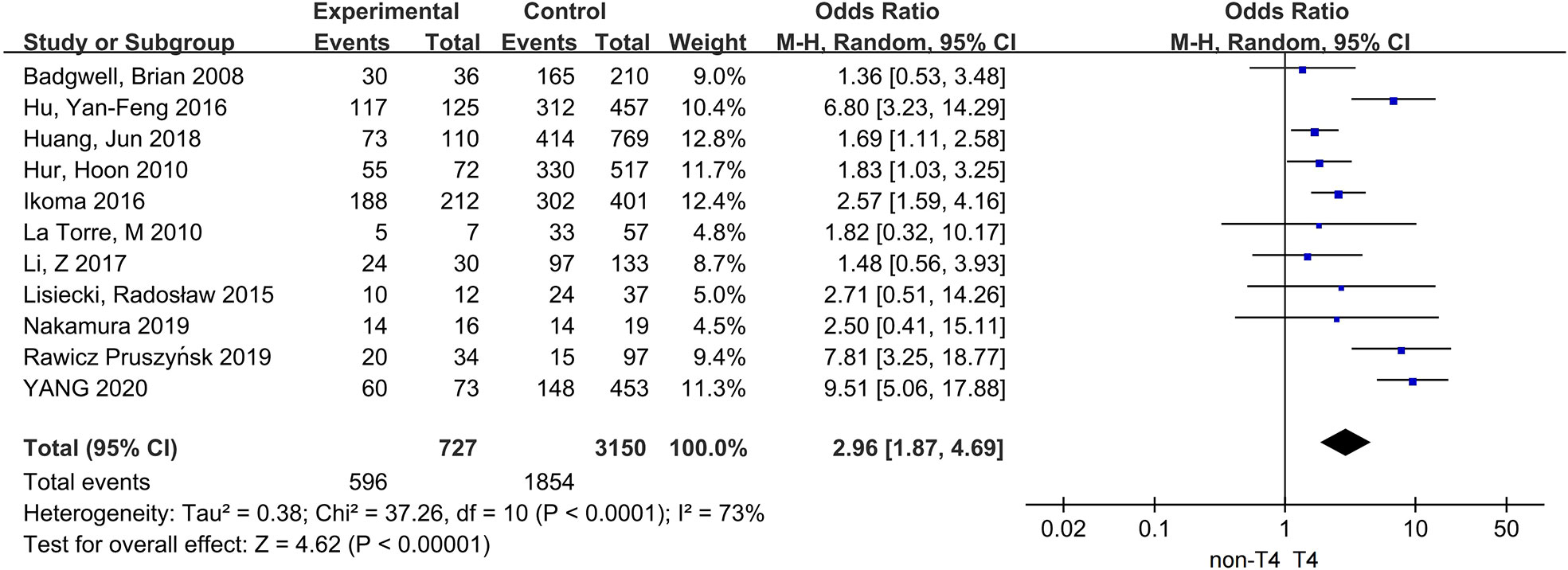
Figure 2 The correlation between T4 stage and PC.
Two ways of classification were applied for the N stage. First, patients were divided into positive regional lymph node (N+) and negative (N−) groups, separately. In addition, 15 studies, with 4,587 patients, were included (10, 14–22, 24–28). Then, we divided patients into N0/1 and N2/3 groups, separately. According to this criteria, five studies, with 1,321 patients, were included (14, 17, 20, 22, 29). The sample size varied from 35 to 589.
There was no statistical correlation between N+ and PC, with OR = 1.22, 95% CI: 0.86–1.73, P < 0.0001; I² = 66%. On contrary, patients with N2/3 stage had a higher proportion in the PC group, with OR = 2.38, 95% CI: 1.22–4.65, P = 0.01; I² = 53% (Figure 3).
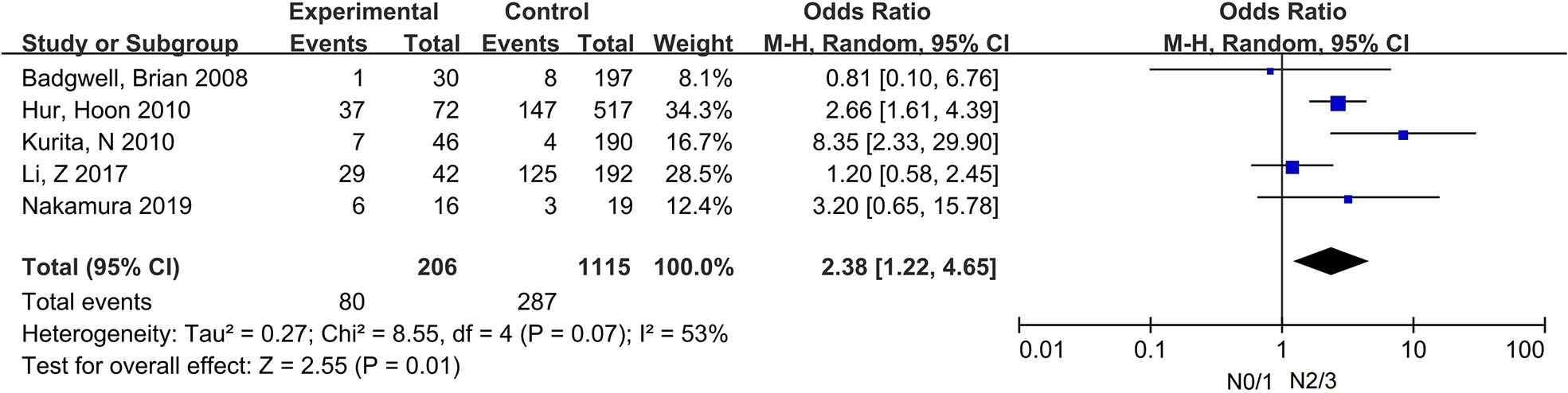
Figure 3 The correlation between N2/3 and PC.
Fourteen studies, with 4,424 patients, from 2006 to 2020 were included (15–23, 26, 27, 29–31). The sample size varied from 32 to 879.
The proportion of patients with poorly differentiated carcinoma was higher in the PC group, and the difference was statistically significant; OR = 1.91, 95% CI: 1.42–2.56, P < 0.0001; I² = 49% (Figure 4).
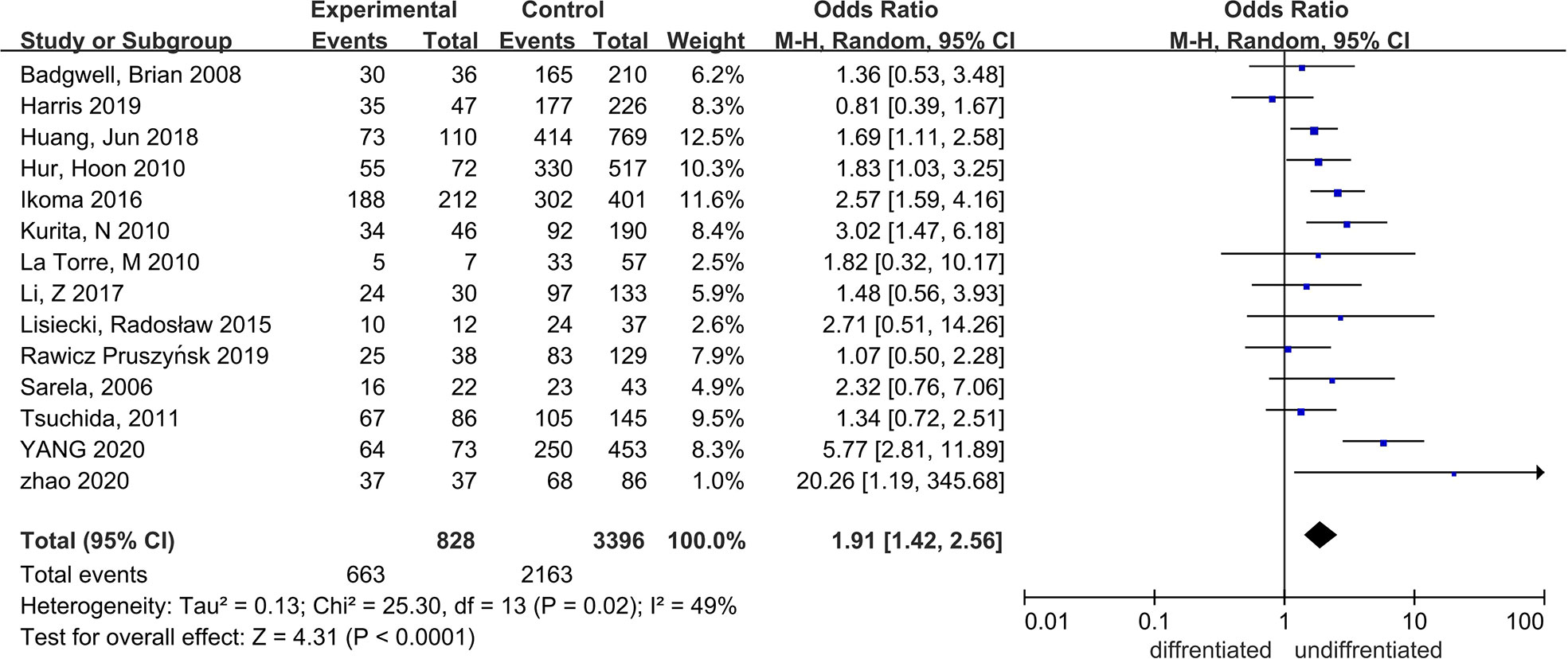
Figure 4 The correlation between differentiation degrees and PC.
Eight studies, with 2,924 patients, from 2000 to 2018 were included (10, 16–18, 24, 26, 29, 32). The sample size of the studies varied from 32 to 879.
After summing up all the results, we could find that patients with Borrmann type IV had a higher proportion in the PC group, with OR = 6.67, 95% CI: 3.33–13.36, P < 0.0001; I² = 85% (Figure 5).

Figure 5 The correlation between Borrmann type IV and PC.
Six studies recorded the diameters of the primary tumors, of which three studies used 4 cm as the cutoff value, and others used 5 cm. We put patients with tumor diameters ≥4 or ≥5 cm together as the large tumor size group. Finally, the number of the included patients was 3,117 (10, 16, 20, 23, 24, 29), with the sample size changing from 231 to 879.
The pooled results showed that patients with large tumor size had a higher proportion in the PC group; the difference was statistically significant; OR = 5.12, 95% CI: 2.55–10.31, P < 0.0001; I² = 83% (Figure 6).
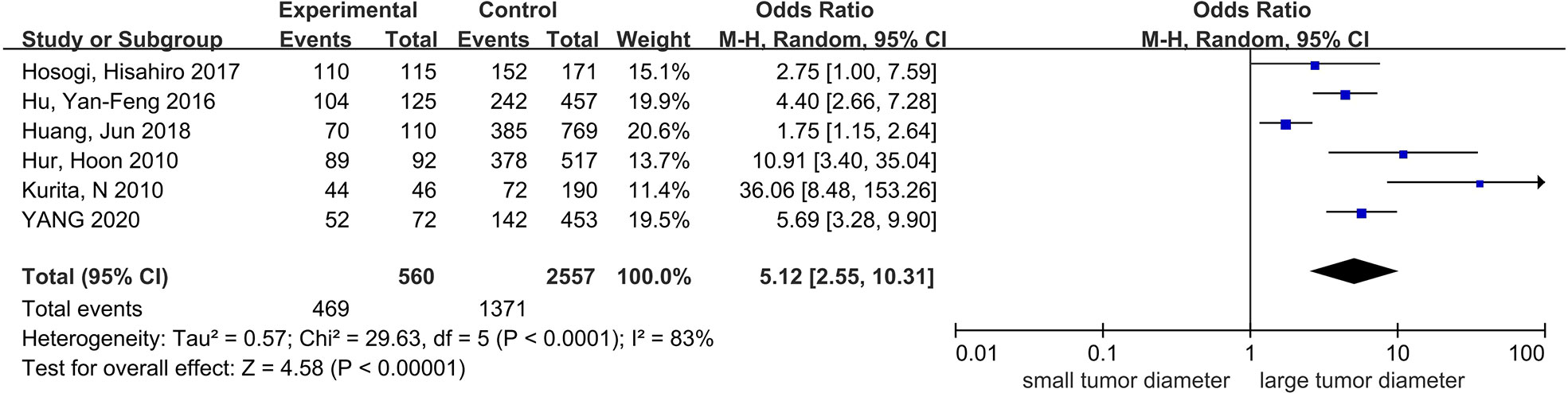
Figure 6 The correlation between tumor diameter and PC.
Three studies, with 925 patients, from 2002 to 2020 were included (11, 30, 33). All of the studies used 35 ng/ml as cutoff value. The sample size varied from 37 to 728.
The pooled results showed that patients with serum CA125 ≥ 35 ng/ml had a higher proportion in the PC group, with OR = 19.45, 95% CI: 4.71–80.30, P < 0.0001; I² = 73% (Figure 7).
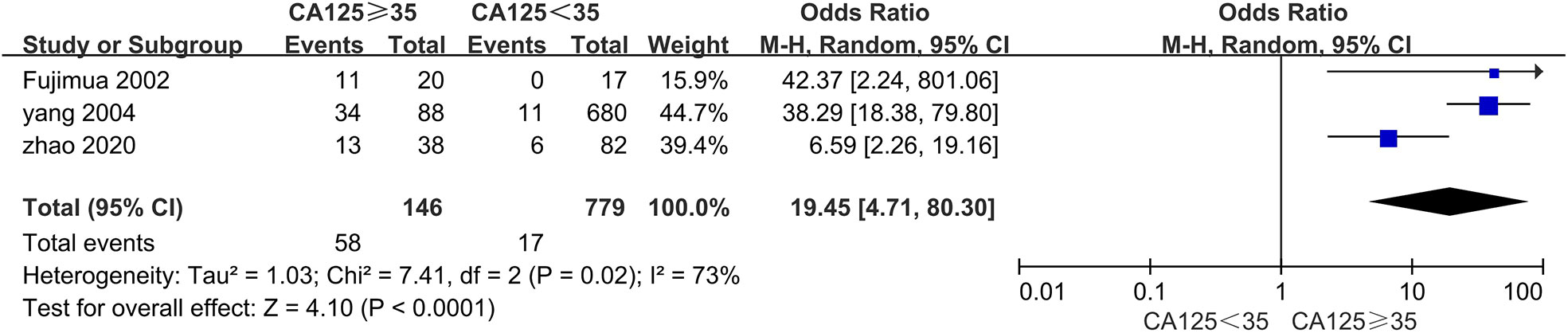
Figure 7 The correlation between serum CA125 and PC.
Five studies, with 1,427 patients, from 2015 to 2020 were included (15, 16, 19, 24, 30). The sample size of the studies changed from 51 to 804.
The proportion of patients with Lauren diffusion type was higher in the PC group, with OR = 2.11, 95% CI: 1.60–2.79, P < 0.0001; I² = 71% (Supplementary Figure 8).
Four studies, with 1,328 patients, from 2008 to 2017 were included (17, 18, 22, 25). The sample size changed from 185 to 662.
The pooled results showed that patients with Signet-ring cell carcinoma had a higher proportion in the PC group, with OR = 1.71, 95% CI: 1.30–2.26, P = 0.0001; I² = 0% (Supplementary Figure 9).
Four studies, with 1,110 patients, from 2002 to 2020, which used 37 ng/ml as cutoff value, were included (11, 17, 30, 33). The sample size of the studies varied from 37 to 768.
The pooled results showed that patients with the serum CA199 ≥ 37 ng/ml had a higher proportion in the PC group, with OR = 4.22, 95% CI: 1.44–12.34, P = 0.001; I² = 81% (Supplementary Figure 10).
Nine studies, with 4,054 patients, from 2005 to 2019 were included (10, 15–18, 20, 26, 28, 31). The sample size varied from 173 to 889.
The pooled results showed that the gender of patients was not statistically associated with PC, OR = 1.06, 95% CI: 0.89–1.25, P = 0.51; I² = 63% (Supplementary Figure 11).
Five studies used 65 years old as the cutoff value and one for 60 years old. We put patients elder than 60 or 65 together as one group. Finally, six studies, with 3,235 patients, from 2005 to 2019 were included (10, 16, 18, 20, 28). The sample size varied from 153 to 878.
The pooled results showed that the age of patients was not statistically associated with PC, OR = 0.90, 95% CI: 0.74–1.09, P = 0.26; I² = 0% (Supplementary Figure 12).
The guidelines provide different indications of SL for patients with advanced gastric cancer. The NCCN (National Comprehensive Cancer Network) guideline recommends that all locoregional patients undergo SL with cytology (8). However, the JGCA (Japan Gastric Cancer Association) guideline recommends that only patients with large Borrmann type III or IV or bulky lymph nodes require SL (7). In between, the CSCO (Chinese Society of Clinical Oncology) guideline sets the indication as CT suspected PC or T3−4/N+ patients ready for neoadjuvant therapy (9). The conflict between the guidelines raised the need for further research on the risk factors of PC to select patients suitable for SL.
In this meta-analysis, we found that there was a cognitive gap between awareness and importance of risk factors of PC, which could partly explain the reasons for the current divergence. In addition to the clinical stage mentioned by the guidelines, there were also factors significantly statistically related to PC but with low concern, such as tumor size and CA125.
T stage is one of the most discussed factors, and our data support its relevance with PC. The majority of the included studies used T4 as a criterion, and T4’s relevance with PC is also consistent with the “seed and soil” hypothesis, which states that more free cancer cells exfoliated from the tumor penetrating serosa could lead to PC (34). However, if all three studies with CY1 only were included in the analysis, then OR (95% CI) was 1.65 (0.79–3.44), which means that there is no statistical difference (19, 21, 22). Yoshida et al. found the occurrence of CY1 or P1 in five of the 1,509 patients with early gastric cancer, and pathological analysis revealed that the primary tumor invaded the submucosa and metastasized to the regional lymph nodes through the lymph vessels; they speculated that tumor cells may metastasize to the peritoneal cavity through the lymphatic system rather than by breaking through the plasma (35). This could be the reason for this subgroup analysis. The analysis of the remaining eight studies involving P1 showed a stronger statistical correlation between T4 and P1. We prefer to recommend SL to patients with T4 stage to avoid missing PC, although the relationship between T4 and CY1 still needs to be explored.
N stage is another most mentioned factor in the studies and guidelines, but the statistical relevance is not obvious. An alternative approach is for N0/1 and N2/3 groups. Although with fewer studies and increased publication bias, there is a significant increase in OR (95% CI) of 2.38 (1.22–4.65). Yoshida et al. proposed that PC can occur through the lymphatic system (35). According to this hypothesis, the more regional lymph nodes that metastasize, the greater likelihood that tumor cells initiate PC by lymph vessels. We cannot propose a definitive SL strategy based on the N stage with insufficient evidence. It may be appropriate to analyze the relationship between the N1–3 stage and PC, separately.
Tumor size is often omitted in the guidelines, with only the Japanese guideline recommending SL for patients with Borrmann type III tumor with diameter ≥ 8 cm (7). However, multiple studies have confirmed the dependency between tumor diameter and PC. Although different lengths were used as the standard of classification, such as 4 or 5 cm, the results indicated that larger tumor diameter was independent risk factor of PC. However, there was no detailed description of how to measure tumor size in the studies. We suggest that patients with large tumor size undergo SL, but the method of measuring the diameter and the cutoff value of tumor size needs to be further clarified.
Several studies have concluded that Borrmann type IV is risk factor for PC, similarly to the JGCA guideline (10, 16–18, 24, 26, 29). In addition, the results of studies indicated that Borrmann type III is also risk factor for PC (10, 16, 26). This may be because Bormann type IV and large Borrmann type III tumors are usually accompanied by larger tumor size and more advanced stage. As discussed previously, patients with risk factors of PC, such as T4 and N+, are more likely to develop PC. Therefore, we recommend that patients with Bormann type IV and large Borrmann type III gastric cancer receive SL.
Although differentiation degrees have been widely studied, no definite conclusion has been made about its relationship with PC. The pooled results suggested that poorly differentiated carcinoma is a risk factor for PC, but the OR was only 1.91 and eight of the 14 studies had opposite results, with a weight of 45.2%. These diminish the confidence of the conclusion. Furthermore, the result of subgroup analysis showed that poorly differentiated carcinoma was not risk factor for CY1 but a risk factor for P1. This suggests that the relationship between poorly differentiated carcinoma and P1 and CY1 may be investigated, separately.
Regarding CA125, CA199, Signet-ring cell carcinoma, and Lauren’s diffuse type, the insufficient studies in the meta-analysis and heterogeneity between results reduce the confidence of the conclusion. We believe that only a system review of their relationship with PC can be made on the base of the current finding. In particular, the OR of elevated CA125 was 19.45, significantly higher than other factors. Moreover, all three studies indicated that elevated CA125 was a risk factor for PC (11, 30, 33). Tumor cells can cause CA125 elevation, and the mesothelial cells in the abdomen and pelvis stimulated by tumors can also increase CA125 secretion. Therefore, we suggest that patients with elevated CA125 should undergo SL and more attention should be paid to its relationship with PC.
There are still limitations in this study. The included studies used different definitions of PC. Four studies defined CY1 as PC and the remaining studies involved P1, of which the conclusions were generally consistent with the overall results. However, no similar relationship was observed in the subgroup analysis of CY1. For example, the relationship between T4 and CY1 was different from between T4 and PC or P1. Moreover, part of the conclusions was based on insufficient evidence, for instance, the relationship between CA125 and PC. In addition, there is heterogeneity and publication bias among the results of the included studies. Meanwhile, the absence of randomized controlled trials has led to the inclusion of only retrospective studies in this article.
In conclusion, this meta-analysis raised the potential conflict between current indications of SL and their actual relevance with PC. We think that patients with T4 stage, Borrmann type IV, large tumor size, and elevated CA125 are more likely to have PC and should undergo SL. In particular, the relationship between CA125 and PC deserves further investigation.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Conception and design of the research: ZYL, GG, and ZML. Analysis and interpretation of the data: GG, ZML, XY, and QW. Writing of the manuscript: GG and ZML. Critical revision of the manuscript for intellectual content: ZYL, GG, and ZML. Final review: ZYL, GG, ZML, and FS. All authors contributed to the article and approved the submitted version.
This work was funded by Beijing Municipal Administration of Hospitals Incubating Program (PX2022047), Beijing Municipal Health Commission (DFL20181103 and ZYLX201701), and Clinical Medicine Plus X – Young Scholars Project, Peking University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.955181/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2020) 71:209–49. doi: 10.3322/caac.21660
2. Fujitani K, Yang H, Mizusawa J, Kim Y, Terashima M, Han S, et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): A phase 3, randomised controlled trial. Lancet Oncol (2016) 17:309–18. doi: 10.1016/S1470-2045(15)00553-7
3. Coccolini F, Cotte E, Glehen O, Lotti M, Poiasina E, Catena F, et al. Intraperitoneal chemotherapy in advanced gastric cancer. meta-analysis of randomized trials. Eur J Surg Oncol (EJSO) (2014) 40:12–26. doi: 10.1016/j.ejso.2013.10.019
4. Burbidge S, Mahady K, Naik K. The role of CT and staging laparoscopy in the staging of gastric cancer. Clin Radiol (2013) 68:251–55. doi: 10.1016/j.crad.2012.07.015
5. Kim SJ, Kim HH, Kim YH, Hwang SH, Lee HS, Park DJ, et al. Peritoneal metastasis: detection with 16- or 64-detector row CT in patients undergoing surgery for gastric cancer. Radiology (2009) 253:407–15. doi: 10.1148/radiol.2532082272
6. Yajima K, Kanda T, Ohashi M, Wakai T, Nakagawa S, Sasamoto R, et al. Clinical and diagnostic significance of preoperative computed tomography findings of ascites in patients with advanced gastric cancer. Am J Surg (2006) 192:185–90. doi: 10.1016/j.amjsurg.2006.05.007
7. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer (2021) 24:1–21. doi: 10.1007/s10120-020-01042-y
8. Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C, et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2022) 20:167–92. doi: 10.6004/jnccn.2022.0008
9. Wang FH, Zhang XT, Li YF, Tang L, Qu XJ, Ying JE, et al. The Chinese Society of Clinical Oncology (CSCO): Clinical guidelines for the diagnosis and treatment of gastric cancer, 2021. Cancer Commun (Lond) (2021) 41:747–95. doi: 10.1002/cac2.12193
10. Hu Y, Deng Z, Liu H, Mou T, Chen T, Lu X, et al. Staging laparoscopy improves treatment decision-making for advanced gastric cancer. World J Gastroenterol WJG (2016) 22:1859–68. doi: 10.3748/wjg.v22.i5.1859
11. Fujimura T, Kinami S, Ninomiya I, Kitagawa H, Fushida S, Nishimura G, et al. Diagnostic laparoscopy, serum CA125, and peritoneal metastasis in gastric cancer. Endoscopy (2002) 34:569–74. doi: 10.1055/s-2002-33228
12. Li K, Cannon JGD, Jiang SY, Sambare TD, Owens DK, Bendavid E, et al. Diagnostic staging laparoscopy in gastric cancer treatment: A cost-effectiveness analysis. J Surg Oncol (2018) 117:1288–96. doi: 10.1002/jso.24942
13. Fukagawa T. Role of staging laparoscopy for gastric cancer patients. Ann Gastroenterol Surg (2019) 3:496–505. doi: 10.1002/ags3.12283
14. Nakamura N, Kinami S, Fujii Y, Miura S, Fujita J, Kaida D, et al. The neutrophil/lymphocyte ratio as a predictor of peritoneal metastasis during staging laparoscopy for advanced gastric cancer: A retrospective cohort analysis. World J Surg Oncol (2019) 17:108. doi: 10.1186/s12957-019-1651-3
15. Rawicz Pruszyński K, Mielko J, Pudło K, Lisiecki R, Skoczylas T, Murawa D, et al. Yield of staging laparoscopy in gastric cancer is influenced by laurén histologic subtype. J Surg Oncol (2019) 120:1148–53. doi: 10.1002/jso.25711
16. Huang J, Luo H, Zhou C, Zhan J, Rao X, Zhao G, et al. Yield of staging laparoscopy for incurable factors in Chinese patients with advanced gastric cancer. J Laparoendosc Adv S (2018) 28:19–24. doi: 10.1089/lap.2017.0170
17. Li Z, Li Z, Jia S, Bu Z, Zhang L, Wu X, et al. Depth of tumor invasion and tumor-occupied portions of stomach are predictive factors of intra-abdominal metastasis. Chin J Cancer Res (2017) 29:109–17. doi: 10.21147/j.issn.1000-9604.2017.02.03
18. Ikoma N, Blum M, Chiang Y, Estrella JS, Roy-Chowdhuri S, Fournier K, et al. Yield of staging laparoscopy and lavage cytology for radiologically occult peritoneal carcinomatosis of gastric cancer. Ann Surg Oncol (2016) 23:4332–37. doi: 10.1245/s10434-016-5409-7
19. Lisiecki R, Spychała A, Pater K, Murawa D. Analysis of risk factors of positive peritoneal cytology in patients treated for gastric cancer – preliminary report*. Polish J Surg (2015) 87:506–12. doi: 10.1515/pjs-2015-0096
20. Hur H, Lee HH, Jung H, Song KY, Jeon HM, Park CH. Predicting factors of unexpected peritoneal seeding in locally advanced gastric cancer: Indications for staging laparoscopy. J Surg Oncol (2010) 102:753–57. doi: 10.1002/jso.21685
21. La Torre M, Ferri M, Giovagnoli MR, Sforza N, Cosenza G, Giarnieri E, et al. Peritoneal wash cytology in gastric carcinoma. prognostic significance and therapeutic consequences. Eur J Surg Oncol (EJSO) (2010) 36:982–86. doi: 10.1016/j.ejso.2010.06.007
22. Badgwell B, Cormier JN, Krishnan S, Yao J, Staerkel GA, Lupo PJ, et al. Does neoadjuvant treatment for gastric cancer patients with positive peritoneal cytology at staging laparoscopy improve survival? Ann Surg Oncol (2008) 15:2684–91. doi: 10.1245/s10434-008-0055-3
23. Yang C, Yang Y, Huang X, Li H, Cheng H, Tong S, et al. A nomogram based on clinicopathologic features and preoperative hematology parameters to predict occult peritoneal metastasis of gastric cancer: A single-center retrospective study. Dis Markers (2020) 2020:1–10. doi: 10.1155/2020/1418978
24. Hosogi H, Shinohara H, Tsunoda S, Hisamori S, Sumida H, Hida K, et al. Staging laparoscopy for advanced gastric cancer: Significance of preoperative clinicopathological factors. Langenbeck's Arch Surg (2017) 402:33–9. doi: 10.1007/s00423-016-1536-7
25. Strandby RB, Svendsen LB, Fallentin E, Egeland C, Achiam MP. The multidisciplinary team conference’s decision on m-staging in patients with gastric- and gastroesophageal cancer is not accurate without staging laparoscopy. Scand J Surg (2015) 105:104–08. doi: 10.1177/1457496915598760
26. Tsuchida K, Yoshikawa T, Tsuburaya A, Cho H, Kobayashi O. Indications for staging laparoscopy in clinical T4M0 gastric cancer. World J Surg (2011) 35:2703–09. doi: 10.1007/s00268-011-1290-5
27. Sarela AI, Lefkowitz R, Brennan MF, Karpeh MS. Selection of patients with gastric adenocarcinoma for laparoscopic staging. Am J Surg (2006) 191:134–38. doi: 10.1016/j.amjsurg.2005.10.015
28. Bentrem D, Wilton A, Mazumdar M, Brennan M, Coit D. The value of peritoneal cytology as a preoperative predictor in patients with gastric carcinoma undergoing a curative resection. Ann Surg Oncol (2005) 12:347–53. doi: 10.1245/ASO.2005.03.065
29. Kurita N, Shimada M, Utsunomiya T, Iwata T, Nishioka M, Yoshikawa K, et al. Predictive factors of peritoneal metastasis in gastric cancer. Hepatogastroenterology (2010) 57:980–83.
30. Zhao J, Qin R, Chen H, Yang Y, Qin W, Han J, et al. A nomogram based on glycomic biomarkers in serum and clinicopathological characteristics for evaluating the risk of peritoneal metastasis in gastric cancer. Clin Proteom (2020) 17:34. doi: 10.1186/s12014-020-09297-4
31. Harris C, Ostwal V, Vallathol DH, Dusane R, Mandavkar S, Patkar S, et al. Calculation of a clinical predictive factors identifying peritoneal disease on a staging laparoscopy in gastric cancers. South Asian J Cancer (2019) 8:166–67. doi: 10.4103/sajc.sajc_182_18
32. Yano M, Tsujinaka T, Shiozaki H, Inoue M, Sekimoto M, Doki Y, et al. Appraisal of treatment strategy by staging laparoscopy for locally advanced gastric cancer. World J Surg (2000) 24:1130–36. doi: 10.1007/s002680010183
33. Hwang GI, Yoo CH, Sohn BH, Shin JH, Park YL, Kim HD, et al. Predictive value of preoperative serum CEA, CA19-9 and CA125 levels for peritoneal metastasis in patients with gastric carcinoma. Cancer Res Treat (2004) 36:178. doi: 10.4143/crt.2004.36.3.178
34. Akhtar M, Haider A, Rashid S, Al-Nabet ADMH. Paget’s “Seed and soil” theory of cancer metastasis: An idea whose time has come. Adv Anat Pathol (2019) 26:69–74. doi: 10.1097/PAP.0000000000000219
Keywords: gastric cancer, peritoneal carcinomatosis, risk factors, staging laparoscopy, indications
Citation: Guan G, Li Z, Wang Q, Ying X, Shan F and Li Z (2022) Risk factors associated with peritoneal carcinomatosis of gastric cancer in staging laparoscopy: A systematic review and meta-analysis. Front. Oncol. 12:955181. doi: 10.3389/fonc.2022.955181
Received: 28 May 2022; Accepted: 26 September 2022;
Published: 28 October 2022.
Edited by:
Emilio Francesco Giunta, Università degli Studi della Campania Luigi Vanvitelli, ItalyReviewed by:
Pedro Villarejo Campos, University Hospital Fundación Jiménez Díaz, SpainCopyright © 2022 Guan, Li, Wang, Ying, Shan and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ziyu Li, eml5dV9saUBoc2MucGt1LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.