
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 08 July 2022
Sec. Radiation Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.954747
 Robert L. Foote1*
Robert L. Foote1* Hirohiko Tsujii2
Hirohiko Tsujii2 Reiko Imai3
Reiko Imai3 Hiroshi Tsuji4
Hiroshi Tsuji4 Eugen B. Hug5Tatsuaki Kanai6
Eugen B. Hug5Tatsuaki Kanai6 Jiade J. Lu7Juergen Debus8Rita Engenhart-Cabillic9
Jiade J. Lu7Juergen Debus8Rita Engenhart-Cabillic9 Anita Mahajan1
Anita Mahajan1As of December 31, 2020, there were 12 facilities located in Asia and Europe which were treating cancer patients with carbon ion radiotherapy (CIRT). Between June 1994 and December 2020, 37,548 patients were treated with CIRT worldwide. Fifteen of these patients were United States (U.S.) citizens. Using the Surveillance, Epidemiology, and End Results cancer statistics database, the Mayo Clinic in Rochester, MN has conservatively estimated that there are approximately 44,340 people diagnosed each year in the U.S. with malignancies that would benefit from treatment with CIRT. The absence of CIRT facilities in the U.S. not only limits access to CIRT for cancer care but also prevents inclusion of U.S. citizens in phase III clinical trials that will determine the comparative effectiveness and cost effectiveness of CIRT for a variety of malignancies for FDA approval and insurance coverage. Past and present phase III clinical trials have not been able to enroll U.S. citizens due to their unwillingness or inability to travel abroad for CIRT for an extended period. These barriers could be overcome with a limited number of CIRT facilities in the U.S.
Carbon ion radiotherapy (CIRT) is a more physically targeted form of radiotherapy compared to photon (X-ray) or proton radiotherapy due to a sharper lateral beam penumbra and end of range Bragg Peak (1–4). One of the advantages of this more targeted therapy is a lower risk for radiation-induced malignancies (5). It also has the biologic advantages of high linear energy transfer (LET), low oxygen enhancement ratio (OER) and increased relative biological effectiveness (RBE) resulting in more irreparable, clustered DNA double strand breaks (1–4).
A series of dose-escalating phase I/II and phase II clinical trials conducted at QST Hospital (National Institutes for Quantum and Radiological Science and Technology) in Chiba, Japan since 1994 have demonstrated that CIRT is safe and effective in the treatment of a number of recurrent, previously irradiated, photon-based radiation-resistant, and/or hypoxic malignancies including prostate cancer, salivary gland cancer, bone and soft tissue sarcoma, paranasal sinus mucosal melanoma, recurrent rectal cancer, non-small cell lung cancer, and liver cancer (6). These initial findings are being confirmed in Europe (7). Phase III clinical trials are underway in Asia and Europe (clinical trials.gov: NCT04592861, NCT02838602, NCT01182779, NCT01182753, NCT02986516, NCT04536649), yet CIRT is currently not available in the United States (U.S.).
This original evaluation was conducted to determine the number of U.S. citizens who have traveled abroad to receive CIRT. In addition, we present a case series describing the types of malignancies which have been treated in U.S. patients, and patient outcomes including survival, tumor control, and toxicity.
The Particle Therapy Co-Operative Group (PTCOG) website (www.ptcog.ch) was used to identify all CIRT facilities in the world treating patients as of December 31, 2020. The CIRT facilities were contacted to determine if they have treated U.S. citizens who have traveled abroad for CIRT from the date their facility opened and treated their first patient through December 31, 2020. U.S. citizens who had traveled abroad were verified by passport information. U.S. citizens living abroad and non-U.S. citizens living within the U.S. were not included.
The facilities having treated U.S. citizens were invited to provide demographic and outcomes information for their patients according to the policies and regulations of their local institutional review board or ethics committee including informed consent when required. No patient identifying information was shared. A data use agreement was instituted between the participating institutions. The data shared are shown in Table 1.
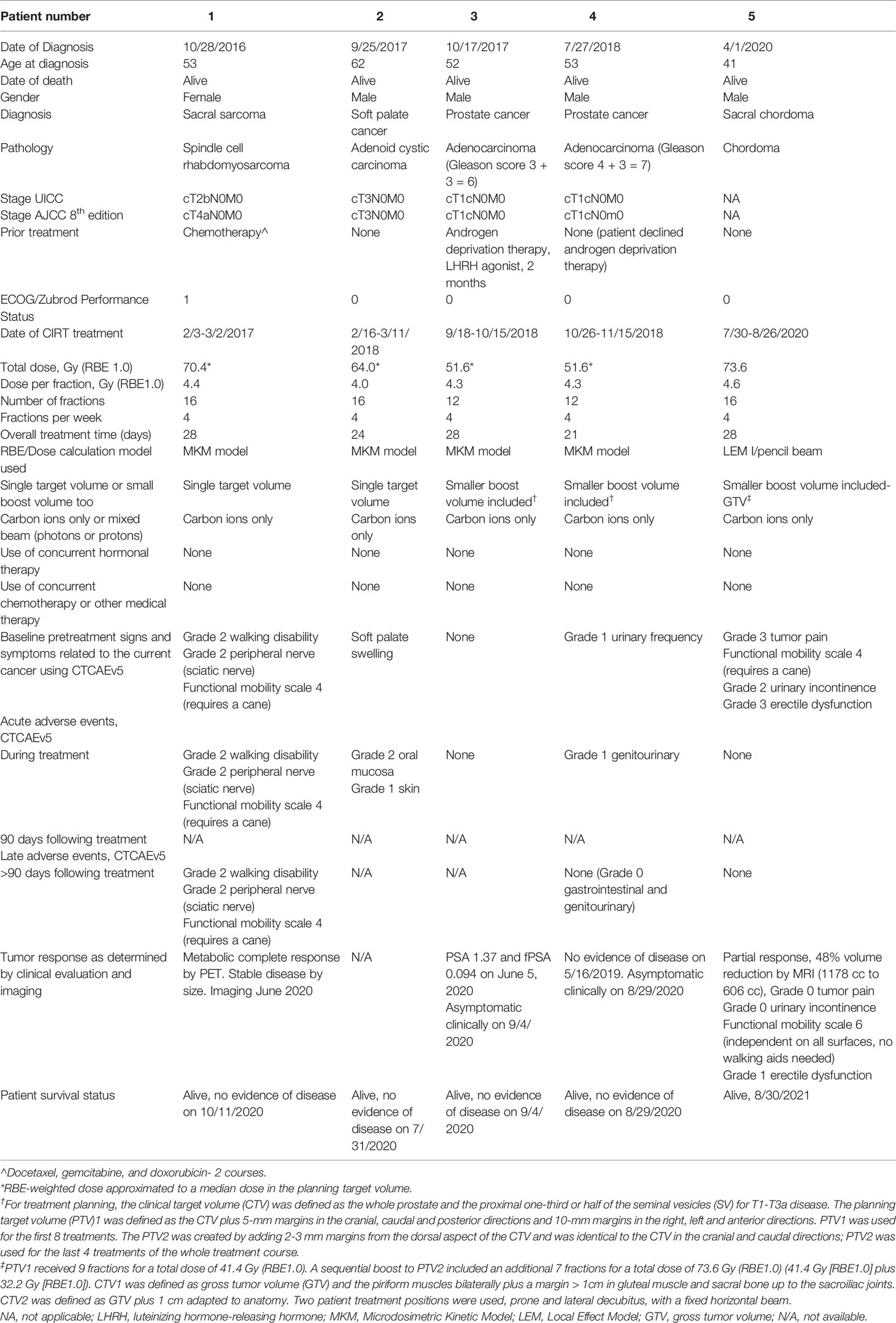
Table 1 Patient demographics, diagnosis, staging, treatment, and outcomes.
As of December 31, 2020, there were 12 facilities located in Asia and Europe which were treating cancer patients with CIRT (Table 2). Four facilities have treated U.S. citizens. Two facilities agreed to provide patient data. Between June 1994 and December 2020, 37,548 patients were treated with CIRT worldwide (Table 2). Fifteen of these patients were U.S. citizens (Table 2).
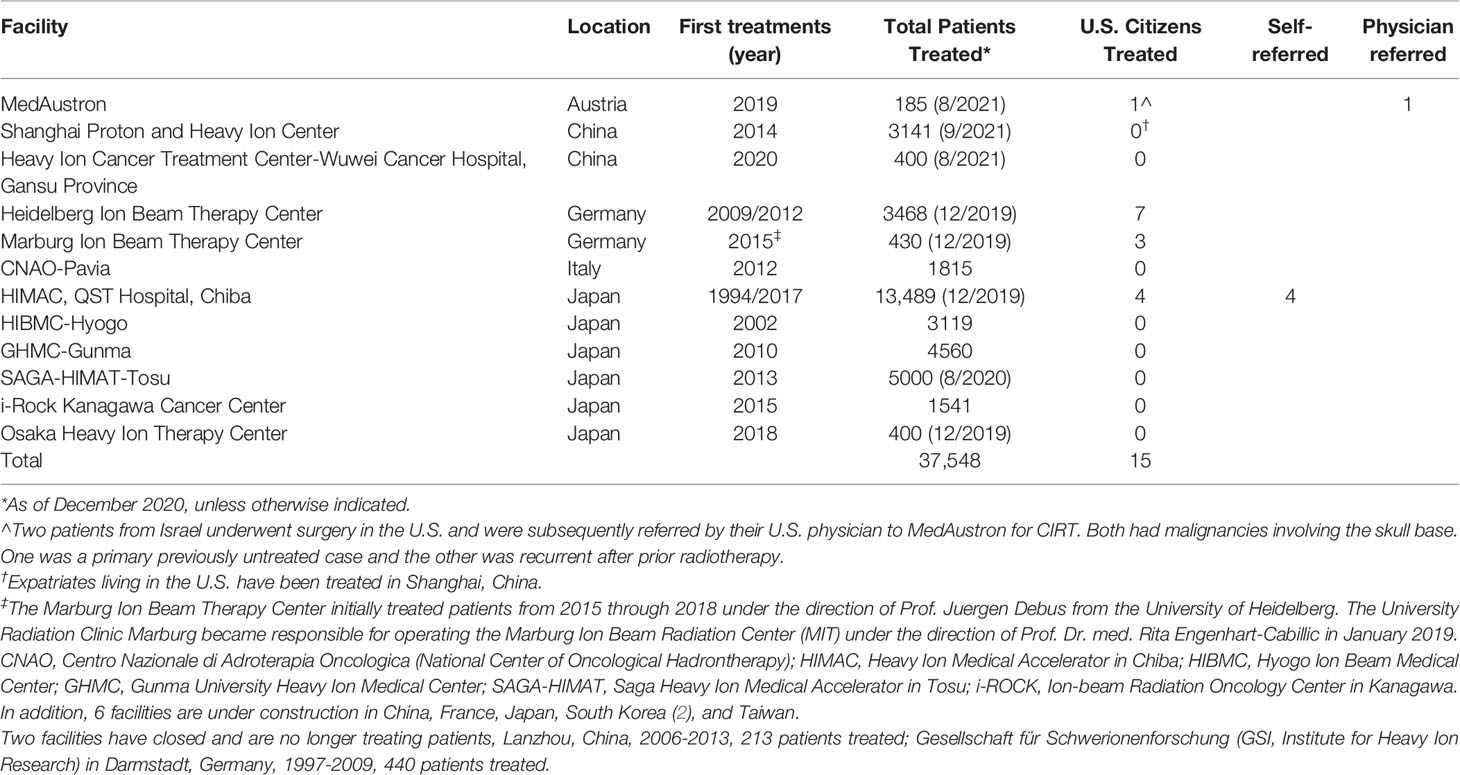
Table 2 Number of U.S. Citizens Treated with CIRT.
Demographic, diagnostic, pathologic, staging, treatment, toxicity, tumor response, and survival data were made available for 5 patients (Table 1). The median age was 53 years (41-62 years). 4 patients were male. Two patients had prostate cancer, one patient had adenoid cystic carcinoma of the soft palate, one patient had a rhabdomyosarcoma of the sacrum and one patient had a sacral chordoma. All patients were ECOG or Zubrod performance status 0 or 1. There was no grade 3 or higher acute or late toxicity associated with CIRT. All patients remain alive with no evidence of disease 12 to 43 months (median 24 months) since completing CIRT.
After a thorough evaluation, to the best of our knowledge, 15 U.S. citizens have traveled abroad to receive CIRT. Using the Surveillance, Epidemiology, and End Results cancer statistics database, the Mayo Clinic in Rochester, MN has conservatively estimated that there are approximately 44,340 people diagnosed each year in the U.S. with malignancies that would benefit from treatment with CIRT. Approximately 780 patients with an indication for treatment with CIRT undergo evaluation at Mayo Clinic in Rochester, MN each year.
Despite this need, no CIRT facilities exist within the U.S. and barriers limit access to international facilities. Not all CIRT facilities accept international patients. Third-party medical coordinators are available to provide contracted services to patients seeking CIRT including review of medical records to determine eligibility for CIRT and arranging for international travel, housing, in-country transportation, insurance coverage and translation services as needed. Nevertheless, these remain substantial barriers to U.S. citizens seeking CIRT abroad. U.S. citizens face some of these same challenges even when seeking tertiary and quaternary medical care for complex illnesses within the U.S. with preference given to health care closer to home (8, 9), and insurance limitations on where they can receive care and which treatments are covered. Not all physicians or patients are aware of CIRT which may further limit referral. Referral outside of the provider’s network and associated revenue concerns may also be hurdles to referring patients for CIRT.
Additional barriers could include patient’s performance status and time away from family, friends, and work. A typical course of CIRT would require patients travel abroad for up to six weeks to complete a typical course of treatment of 4 days per week for 4 weeks with another week or two for treatment planning time. The global COVID-19 pandemic has introduced additional anxiety and barriers to travel over he past two years which could impact future international mobility.
Telemedicine has the potential to mitigate some, but not all, of the above barriers. Videoconferencing could be used to provide consultations to determine if the patient is eligible for CIRT prior to traveling abroad. This platform could also be used to provide patient education about the complexity of CIRT, introduce and engage the patient with their CIRT care team, and provide at home follow up care coordinated between the referring physician and the foreign CIRT care team limiting the number of trips and time abroad to the treatment planning and delivery time. Clinical trial information could also be obtained by electronic means.
Lazar, et al. have reported an increase in the number of trials investigating CIRT since 2010, and the number of countries and sites offering CIRT is slowly growing. They note, however, this progress has excluded other countries, including the U.S. They proposed several recommendations to study CIRT to accelerate progress in the field, including: 1) increasing the number of multinational randomized clinical trials, 2) leveraging the existing CIRT facilities to launch larger multinational trials directed at common cancers combined with high-level quality assurance; and 3) developing more compact and less expensive next-generation treatment systems integrated with radiobiologic research and preclinical testing (10). As noted above, barriers exist to U.S. citizens which limit benefits from successful implementation of recommendation 1 and 2. Implementation of recommendation 3 has the potential to improve the feasibility of construction of a limited number of CIRT facilities in the U.S. which would reduce many of the barriers.
The absence of U.S. CIRT facilities not only limits access to CIRT for cancer care but also prevents inclusion of U.S. citizens in phase III clinical trials that will determine the comparative effectiveness and cost effectiveness of CIRT for a variety of malignancies for FDA approval and insurance coverage. Past and present phase III clinical trials have not been able to enroll U.S. citizens due to their unwillingness or inability to travel abroad for an extended period due to the barriers noted above. These barriers could be overcome with a limited number of CIRT facilities in the U.S. with perhaps one located in the Eastern, Midwestern, and Western U.S.
The ideal CIRT facilities in the U.S. would have existing patient volumes to match the capacity of the facility, allow easy and rapid access to CIRT via responsive, respected radiation oncologists with particle therapy experience and subspecialty expertise in malignancies with indications for CIRT who will communicate openly and in a timely manner with referring physicians, patients and their families; radiation therapists, certified medical dosimetrists and medical physicists with particle therapy expertise; educational infrastructure to train the next generation of CIRT providers, research infrastructure to conduct basic science and clinical research, and a comprehensive cancer and medical center to provide surgery, medical therapy, rehabilitative services, social services, psychologic support, chaplain services and spiritual support, and concierge services to help patients and family members with transportation, food and housing, entertainment, and insurance coverage.
Fifteen U.S. citizens have been treated with CIRT. Substantial barriers to traveling abroad for CIRT exist. A limited number of CIRT facilities in the U.S. would improve access to CIRT and enhance accrual to phase III clinical trials. U.S. patients deserve more practical access to life saving cancer treatments which are available elsewhere in the world.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was reviewed and approved by QST Hospital. Written informed consent for participation was not required for this study in accordance with national legislation in the United States and institutional requirements of Mayo Clinic.
All authors have made substantial contributions to conception and design, acquisition of data, analysis, and interpretation of data; and have been involved in drafting the manuscript or revising it critically for important intellectual content; and given final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Schulz-Ertner D, Jakel O, Schlegel W. Radiation Therapy With Charged Particles. Semin Radiat Oncol (2006) 16:249–59. doi: 10.1016/j.semradonc.2006.04.008
2. Pompos A, Durante M, Choy H. Heavy Ions in Cancer Therapy. JAMA Oncol (2016) 2:1539–40. doi: 10.1001/jamaoncol.2016.2646
3. Mohamad O, Sishc BJ, Saha J, Pompos A, Rahimi A, Story MD, et al. Carbon Ion Radiotherapy: A Review of Clinical Experiences and Preclinical Research, With an Emphasis on DNA Damage/Repair. Cancers (2017) 9:66. doi: 10.3390/cancers9060066
4. Mohamad O, Makishima H, Kamada T. Evolution of Carbon Ion Radiotherapy at the National Institute of Radiological Sciences in Japan. Cancers (2018) 10:66. doi: 10.3390/cancers10030066
5. Mohamad O, Tabuchi T, Nitta Y, Nomoto A, Sato A, Kasuya G, et al. Risk of Subsequent Primary Cancers After Carbon Ion Radiotherapy, Photon Radiotherapy, or Surgery for Localised Prostate Cancer: A Propensity Score-Weighted, Retrospective, Cohort Study. Lancet Oncol (2019) 20:674–85. doi: 10.1016/S1470-2045(18)30931-8
6. Kamada T, Tsujii H, Blakely EA, Debus J, De Neve W, Durante M, et al. Carbon Ion Radiotherapy in Japan: An Assessment of 20 Years of Clinical Experience. Lancet Oncol (2015) 16:e93–100. doi: 10.1016/S1470-2045(14)70412-7
7. Eichkorn T, König L, Held T, Naumann P, Harrabi S, Ellerbrock M, et al. Carbon Ion Radiation Therapy: One Decade of Research and Clinical Experience at Heidelberg Ion Beam Therapy Center. Intl J Rad Onc Bio Phys (2021) 111(3):597–609. doi: 10.1016/j.ijrobp.2021.05.131
8. Finlayson SRG, Birkmeyer JD, Tosteson ANA, Nease RF Jr. Patient Preferences for Location of Care. Implications for Regionalization. Med Care (1999) 37(2):204–9. doi: 10.1097/00005650-199902000-00010
9. Ellis RJ, Yuce TK, Hewitt DB, Merkow RP, Kinnier CV, Johnson JK, et al. National Evaluation of Patient Preferences in Selecting Hospitals and Health Care Providers. Med Care (2020) 58(2):867–73. doi: 10.1097/MLR.0000000000001374
Keywords: radiation therapy, carbon ion radiotherapy, US citizens, clinical trial accrual, heavy particle therapy, access
Citation: Foote RL, Tsujii H, Imai R, Tsuji H, Hug EB, Kanai T, Lu JJ, Debus J, Engenhart-Cabillic R and Mahajan A (2022) The Majority of United States Citizens With Cancer do not Have Access to Carbon Ion Radiotherapy. Front. Oncol. 12:954747. doi: 10.3389/fonc.2022.954747
Received: 27 May 2022; Accepted: 13 June 2022;
Published: 08 July 2022.
Edited by:
Marco Durante, Helmholtz Association of German Research Centres (HZ), GermanyReviewed by:
Ester Orlandi, National Center of Oncological Hadrontherapy, ItalyCopyright © 2022 Foote, Tsujii, Imai, Tsuji, Hug, Kanai, Lu, Debus, Engenhart-Cabillic and Mahajan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert L. Foote, Zm9vdGUucm9iZXJ0QG1heW8uZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.