
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 17 August 2022
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.939838
This article is part of the Research Topic Reviews in Thoracic Oncology View all 17 articles
 Siyuan Chen1,2†
Siyuan Chen1,2† Yu Qiao3†
Yu Qiao3† Juan Chen4†Yanan Li1,2
Juan Chen4†Yanan Li1,2 Jianlian Xie5Pengfei Cui1,2Ziwei Huang1,2Di Huang1,2Yiming Gao1,2
Jianlian Xie5Pengfei Cui1,2Ziwei Huang1,2Di Huang1,2Yiming Gao1,2 Yi Hu1*Zhefeng Liu1*
Yi Hu1*Zhefeng Liu1*Objective: The study was designed to explore the evolution of non-small cell lung cancer (NSCLC) management in the last 20 years.
Methods: The top 100 most-cited papers on NSCLC treatment were retrieved from the Web of Science Core Collection database. R and VOSviewer were used to extract bibliographic information, including the year of publication, countries/regions, institutions, authors, journals, keywords, impact factor, and total citations. The topic and type of papers were checked independently by authors. Bibliometric analysis was conducted and visualized with R, CiteSpace, Excel and VOSviewer to identify output dynamics, research forces, topics, hotspots, and frontiers in the field.
Results: The average citation of each retrieved top 100 most-cited NSCLC management papers was 1,725 (range: 615-7,340). Fifty-seven corresponding authors were from the United States. This country contributed the most papers (n=76), followed by Germany (n=34), France (n=33), and South Korea (n=32). The top contributors were Paz-Ares L. (n=12) and Reck M. (n=12). The Memorial Sloan Kettering Cancer Center published the largest number of papers (n=20). There were two significant citation paths, indicating publications in medicine/medical/clinical journals primarily cited journals in molecular/biology/genetics fields, partly cited health/nursing/medicine fields. Top-cited papers mainly came from the New England Journal of Medicine (n=33, citations=80,427), followed closely by the Journal of Clinical Oncology (n=28, citations=32,408). “Chemotherapy” (n=36) was the keyword with the greatest frequency of co-occurrence. “Open-label” was the keyword with the strongest burst strength (=4.01), followed by “nivolumab” (=3.85), “blockade” (=2.86), and “efficacy” (=2.85).
Conclusions: The United States as a nation and the Memorial Sloan Kettering Cancer Center as an institute contributed the most to this field. The New England Journal of Medicine is the most eye-catching journal. Hotspots of NSCLC management have almost undergone an evolution from chemotherapy and radiotherapy to targeted therapy to immunotherapy. Molecular/biological/genetic fields become the main research base for NSCLC treatment. Immunotherapy and combination therapy are research frontiers.
Lung cancer is the second most prevalent cancer and the most common cause of cancer-related deaths, with approximately 2.2 million new cases and 1.8 million deaths each year, accounting for one-tenth of diagnosed cancers and one-fifth of cancer deaths globally. This cancer has become the leading burden on worldwide health care (1). Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, accounting for approximately 85% of all lung cancer cases, which is further subdivided into three types: adenocarcinoma, squamous carcinoma, and large cell lung carcinoma (2, 3). The most common type is adenocarcinoma, which occurs in the peripheral bronchi and accounts for approximately 40% of all lung cancers. This is followed by squamous carcinoma, which arises in the main bronchi and comprises 25-30% of all diagnosed lung cancers. Large cell carcinoma accounts for 10%, occurring in the proximal part within the thorax (3, 4). NSCLC is a heterogeneous malignancy harboring a wide variety of driver genetic mutations. Over the past few decades, tremendous advances in NSCLC treatment, especially the advent of targeted and immunotherapy, have changed the landscape of NSCLC management. Individualized precision medicine based on genetic characteristics is gaining popularity. Currently, the options for NSCLC management mainly include surgery, radiotherapy, chemotherapy, targeted therapy, and immunotherapy. Among them, surgery has become a greatly recommended choice for resectable NSCLC, stereotactic ablative radiotherapy (SABR) techniques make radiotherapy more precise and less damaging, platinum-based chemotherapy remains the standard regimen for some advanced NSCLC patients, while small molecular tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs) have brought unprecedented benefit in particular patients (5–7). The emergence of new technologies and the obsolescence of old ones have been ongoing.
However, the evolution of NSCLC treatment over the last 20 years is not well defined previously. Textbook-style chapter summaries and systematic reviews fail to fully demonstrate a time-based research progress and to effectively analyze a large amount of data. In fact, it is difficult for scholars to perform an exhaustive analysis in the face of the vast amount of NSCLC treatment research findings over the last 20 years. It is even more challenging to assess the evolution of the subject according to its temporal dynamics. Bibliometric analysis is one of the best tools for studying temporal trends in a certain area, which offers more comprehensive and objective results (8–11). Therefore, bibliometrics may provide meaningful insight into NSCLC management. We have innovatively applied this approach in the field of NSCLC treatment. The volume of citations in a paper signifies the significance of the study, indicating the impact it has had on the understanding and treatment of the disease (12). To make the study representative, we filtered the 100 most-cited articles in NSCLC treatment based on bibliometric citation analysis. These articles stand for the most impressive achievements in NSCLC treatment. In the 21st century, when the treatment of NSCLC is rapidly evolving, all research is inseparable from the foundation of previous generations. We can gain a lot of inspiration and experience from the evolution of NSCLC treatment. The study may help clinicians and researchers quickly understand the evolution of NSCLC management and grasp research status quo. The data visualization can help them to have a more intuitive understanding of the 100 most-cited NSCLC papers. To our knowledge, this is the first comprehensive bibliometric study about the evolution of NSCLC treatment in the last 2 decades.
The relevant data used in this study were downloaded from the Science Citation Index Expanded (SCI-EXPANDED) of Clarivate Analytics Web of Science Core Collection (WoSCC). The WoSCC is the most commonly used database for various bibliometric studies (8, 13). As the most prestigious global database, it can provide detailed information needed for bibliometric software and ensure the quality of research (14).
Literature in WoSCC published from January 2000 to December 2021 was systematically searched. The search terms were partly selected from the Medical Subject Headings (MeSHs) offered by the PubMed. We mainly refer to papers to expand the search terms (8). In addition, we consulted experts and physicians to add supplementary concept. The search topic terms were “non-small cell lung cancer” and “treatment”. The summary of the search strategy is presented in Supplementary Table S1. Guidelines, editorials, and statements were all excluded. Only original articles and reviews with full manuscripts regarding the management of NSCLC were reserved, and no language restrictions were applied. It has been demonstrated that bibliometric analysis using original articles and reviews is effective (15). To select the papers with the highest academic impact in the field, two authors (S.C. and Y.Q.) identified the top 100 articles based on total citation (TC) independently. If there was any dissensus, it was discussed with a corresponding expert (Y.H.) until a consensus was reached. To avoid errors caused by the database update, all data acquisition was completed on December 2, 2021. We download the 100 most influential articles’ records, in the “Full Record and Cited References” form from WoSCC in.txt format (Figure 1).
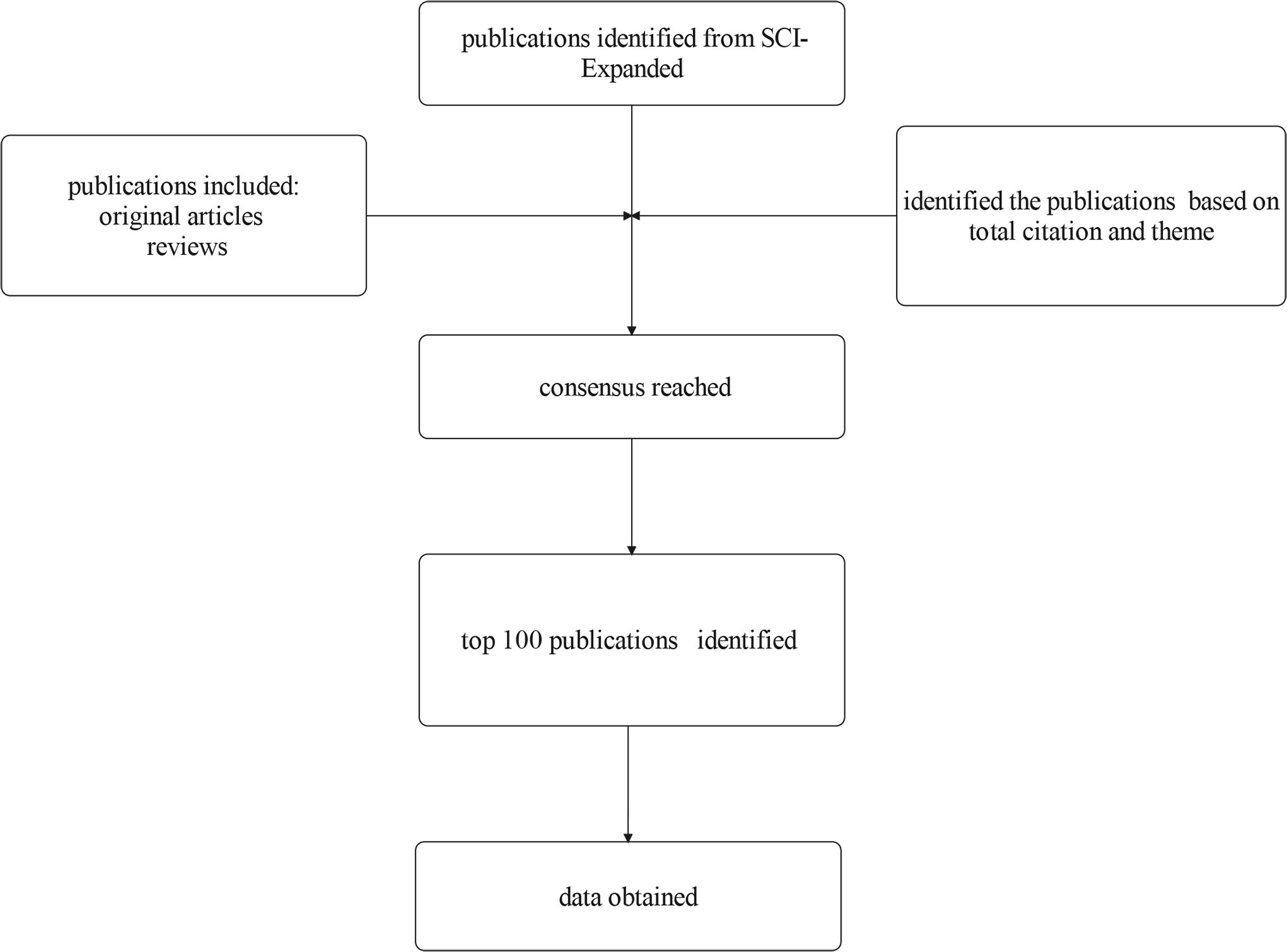
Figure 1 Flow chart of literature screening.
R is a unique language and environment for statistical calculation and plotting (16). It offers a wide diversity of statistical and charting techniques and is highly extensible and useful in ever-changing fields, such as bibliometrics (11, 17). The “bibliometrix” R-package provides a range of flexible tools for quantitative research in bibliometrics and scientometrics while it can also be integrated with other R packages (11). We mainly rely on the “bibliometrix” package in the R software to convert, analyze, and visualize data.
VOSviewer, a computer program developed by Leiden University, used to build and view bibliometric maps, has exceptional capabilities in exploring and visualizing network-based data (18). It was chosen because it delivers concise, information-rich charts that meet the research needs.
CiteSpace, a JavaScript-based application developed by Drexel University, was designed as a powerful tool for identifying and mapping potential trends and dynamics of a scientific field over time (19). The program has been commonly applied for bibliometric analysis in numerous subjects, such as oncology, immunology, and regenerative medicine (9, 13, 20, 21).
The results of the bibliometric analysis are always manifested through science mapping, which is complex and frequently requires a combination of various software for the creation (11). The above applications were utilized in combination to achieve enriched results. We used the “bibliometrix” package (Version 3.1.4) in R software (Version 4.1.1) and VOSviewer (Version 1.6.17) to extract the bibliographic information of the selected papers, including the year of publication, countries/regions, institutions, authors, journals, keywords, impact factor (IF, from Web of Science InCites Journal Citation Reports, JCR Year 2020), and TC. To ensure the accuracy of the data, we also finalized the papers’ topic and type by reading titles, abstracts, and even the full texts. After that, we combine R and Microsoft Office Excel (Version 2019) to create the map concerning the annual distribution of publications, the proportion of international cooperation, the annual output of the top 10 authors, and the annual growth trends of the journals. VOSviewer was also used for graph generation of the overlay visualization map of the top-cited publications, the cooperation relationships of countries/regions, the item density visualization map of major institutions, the cooperation relationships of major authors, and the overlay visualization map of keywords co-occurrence. CiteSpace (Version 5.8.R3) was adopted to draw the dual-map overlay of journals and to identify the keywords with the strongest burst strength. Excel was used to manage the database.
More than 300,000 articles (published between January 2000 and December 2021) related to the treatment of NSCLC were retrieved from WoSCC. The result shows that the TC varied from 615 to 7,340 and the average citations per publication were 1,725. These papers, including 97 original articles and 3 reviews, were published by a sum of 1,940 authors, with an average of 19.7 authors per publication, and none of the papers were solely authored.
As is displayed in Figure 2A, the selected most influential papers were published from 2000 to 2019, with annual output ranging from 1 to 10. The high-yield years were 2005 (n=10), 2015 (n=9) and 2018 (n=9) and the lowest yield year was 2001 (n=1).
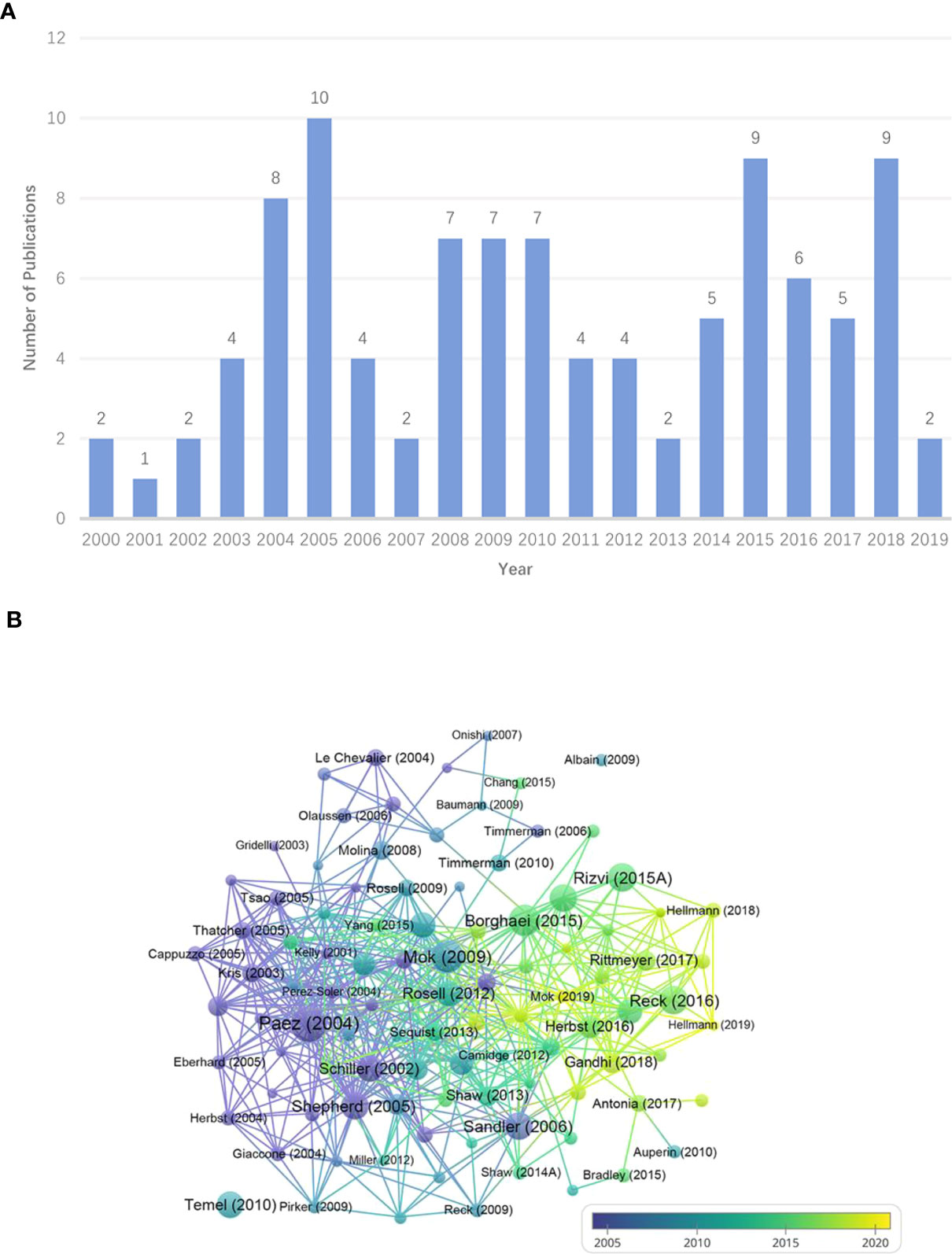
Figure 2 (A) Annual distribution of publications. (B) The overlay visualization map of the top-cited publications. Each node means an article. The size of circles and fonts is proportional to TC. The more purple the node, the earlier the year of publication, and the yellower the node, the more recent the publication date. The node name shows the first author and the publication year of a paper. The connecting line suggests that there is a citation relationship between the papers.
Figure 2B reflects that the single papers published by Paez JG, Mok TS, and Borghaei H had the top 3 TC, with 7,340, 5,931, and 5,453 respectively. In addition, there was a wide citation relationship between the top papers. The detailed information about the 100 most influential publications was recorded in Supplementary Table S2.
As is shown in Figure 3A, the 100 top-cited articles were from 44 countries/regions. Among these countries/regions, the United States possesses the largest weight (n=76), meaning the number of papers involving authors from the United States was 76. The densest connecting lines surrounding “Unites States” suggests the strongest cooperation between the United States and other countries/regions. The highly cooperative countries/regions also include Germany (n=34), France (n=33), South Korea (n=32), Spain (n=29), Italy (n=27), Japan (n=27), United Kingdom (n=25), Canada (n=24), Australia (n=22) and China (n=21) (shown in the Supplementary Table S3).

Figure 3 (A) The cooperation relationships of countries/regions. Each node represents a country/region. The size of circles and fonts symbolizes the number of articles in certain countries/regions, and the thickness of the linking line between countries/regions indicates the frequency of collaborations. The distance between the two circles demonstrates the relatedness of their link. (B) The proportion of international cooperation. The length of the bar is determined by the number of corresponding authors in the country/region. MCP is intercountry collaboration indices, denoting the number of papers issued collaboratively by multiple countries/regions. SCP is intra-country collaboration indices, indicating the number of papers published independently by a single country/region.
Figure 3B demonstrates the distribution of corresponding authors. The level of scientific research in a country/region depends to a large extent on the number of experts in the field. Generally, the corresponding author is the leader in charge of the research and the gatekeeper of the final quality of academic papers. To further explore leading countries/regions in the area, we analyze the distribution of corresponding authors. The majority of the article’s corresponding authors are from the United States (n=57), followed by China (n=10), Japan (n=7), France(n=5), Italy (n=4), Canada (n=4), Spain (n=3), Germany (n=3) and Korea (n=2).
As is noted in Figure 4, The Memorial Sloan Kettering Cancer Center holds the largest weight (n = 20), which signifies that the institution was involved in publishing 20 papers, followed by the Massachusetts General Hospital, the AstraZeneca, the Dana-Farber Cancer Institute, and the Sungkyunkwan University, with 16, 12, 12 and 12 respectively. TC/publication is the ratio of TC to number of publications and is equal to the average TC per paper, reflecting the average impact of papers in the journal.
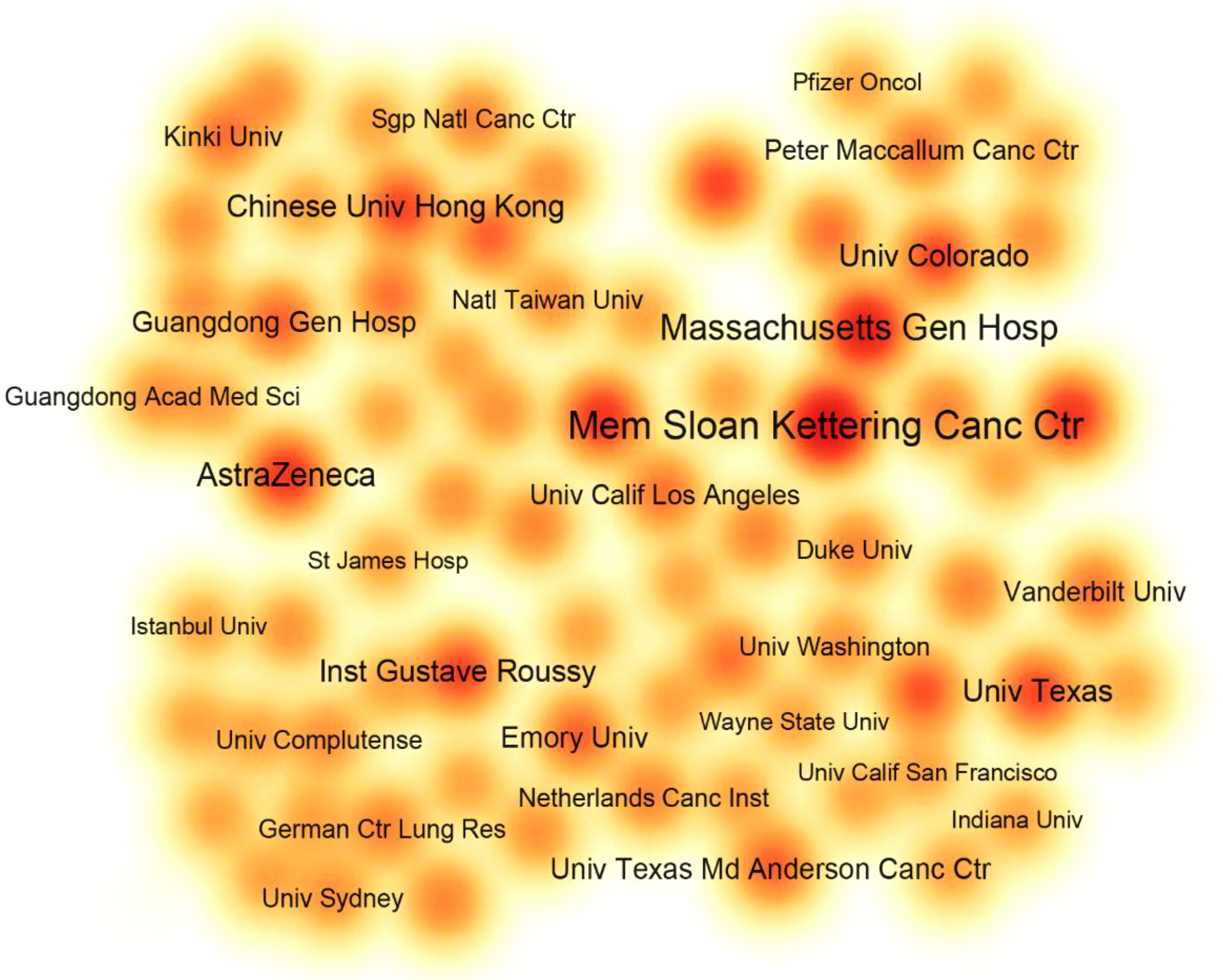
Figure 4 The item density visualization map of major institutions. Each node represents an institution. The larger the size of the fonts and the closer the color around the node to red, the more papers the institution is involved in.
As is listed in Table 1, the Dana-Farber Cancer Institute had the highest TC/publication (2,635.00), followed by the AstraZeneca (1,909.00), the Chinese University of Hong Kong (1,760.20), and the Memorial Sloan Kettering Cancer Center (1,747.15).

Table 1 Top 10 institutions with the most articles.
In Figure 5A, major authors were divided into 4 clusters, which can help us identify the core research teams. The researchers formed a collaborative network with Paz-Ares L., Reck M., Wu Yl., Von Pawel J., and Felip E. as the core, each publishing 12, 12, 11, 10, and 9 articles.
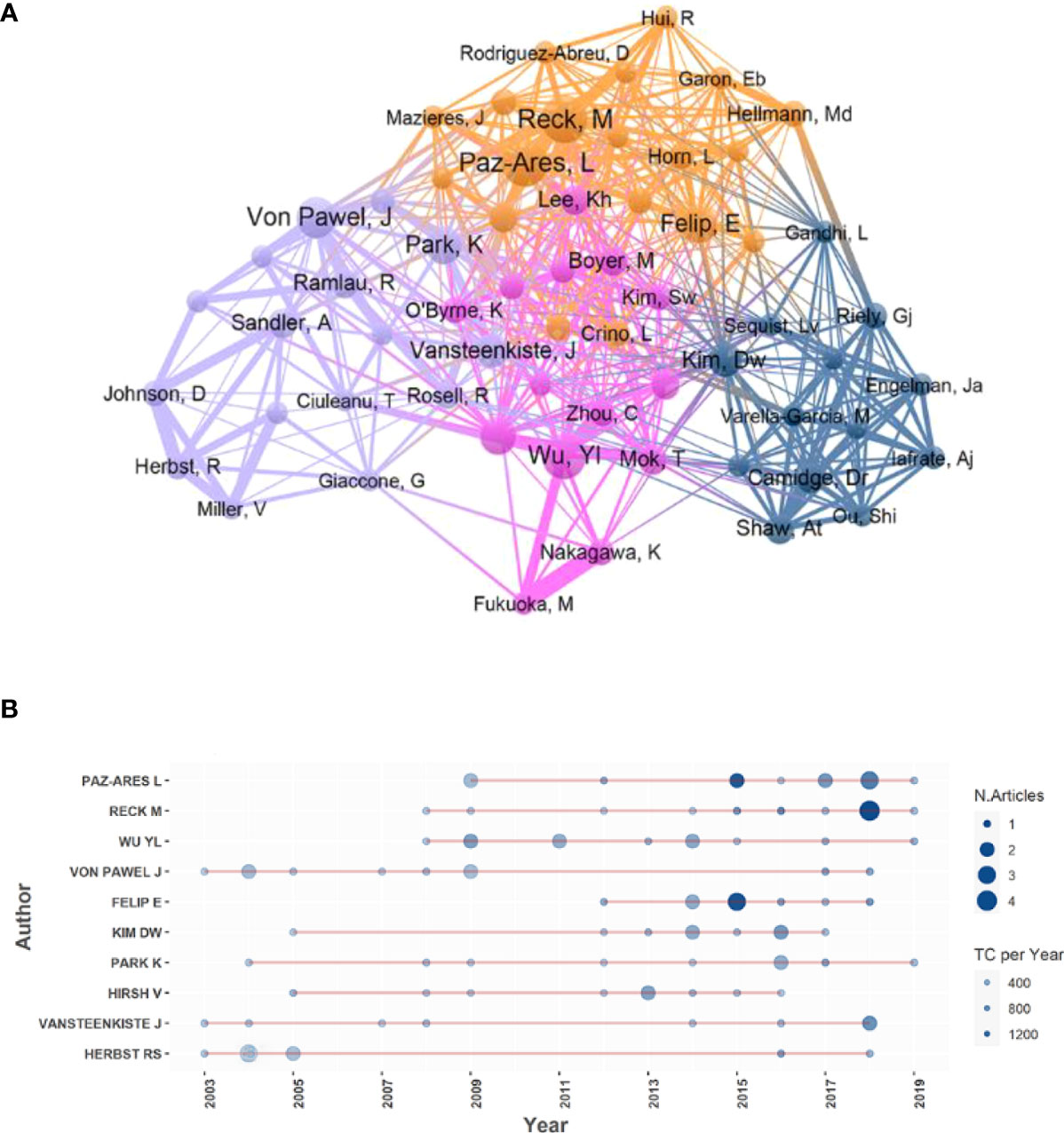
Figure 5 (A) The cooperation relationships of major authors. Each node stands for an author. The size of circles and fonts means the articles’ counts of the author. The colors of the nodes represent clusters. The thickness of the connecting line between authors shows the frequency of collaborations. The distance between the two circles expressed the relatedness of their link. (B) Annual output distribution of the top 10 authors. The bigger the node, the more papers published in that year, and the bluer the node, the more annual average TC of the authors’ papers in that year.
As is shown in Figure 5B, there was a large gap (nearly 10 years) between the two top articles published by Herbst R. whereas some authors, like Paz-Ares L. and Reck M., had been publishing articles for years in a row.
Figure 6A conveys the category distribution of the journals (22). Two significant citation paths were identified and marked in green. The first green path indicates publications in medicine/medical/clinical journals primarily cited journals in molecular/biology/genetics fields and the second means publications in medicine/medical/clinical journals partly cited health/nursing/medicine journals. Immunology and computer-related journals also appear in the citation path marked in yellow and green.
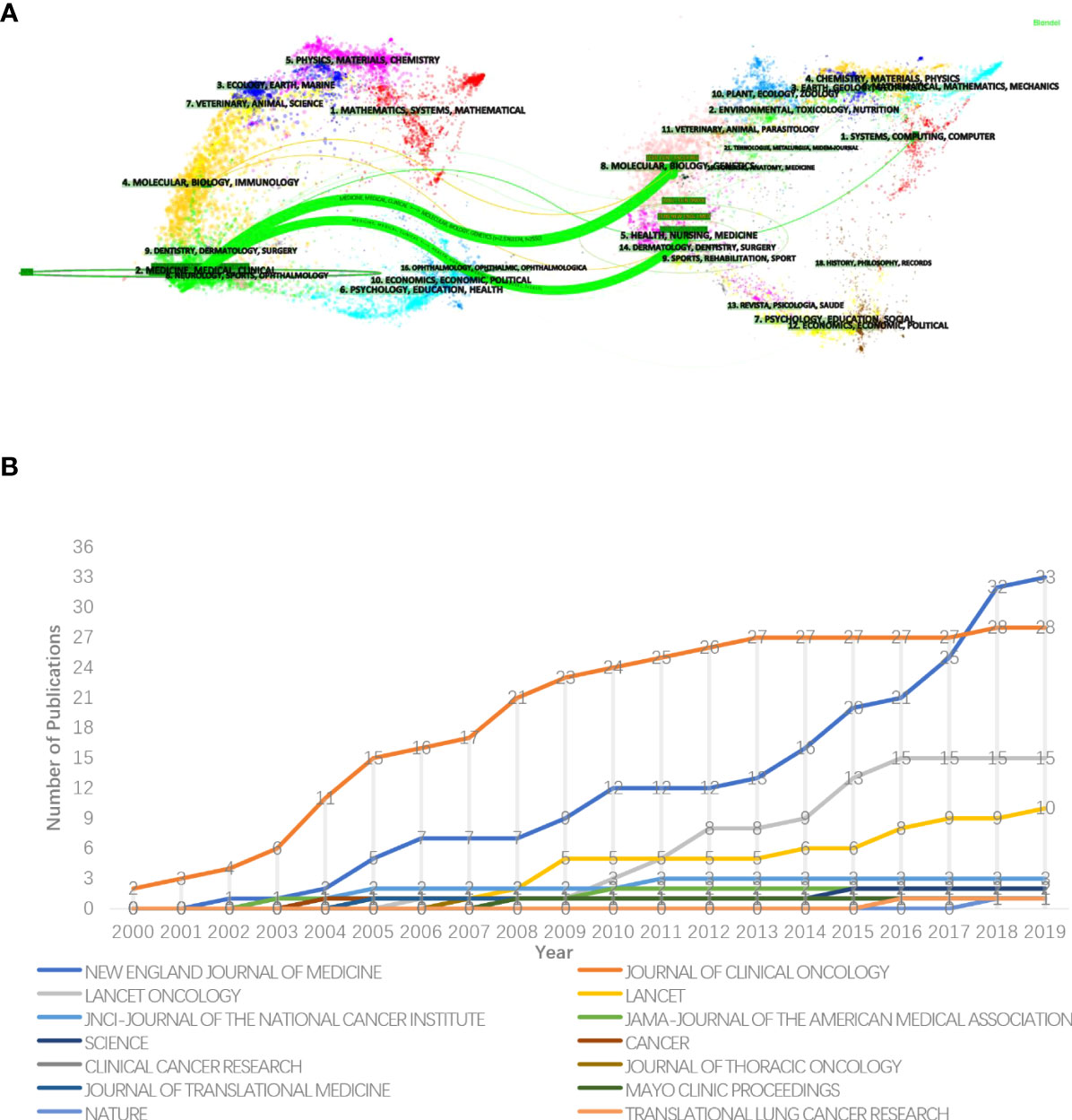
Figure 6 (A) The dual-map overlay of journals. The citing papers are listed on the left while the cited papers are laid on the right, between them was the curve that presents the citation relationship. Different colors denote journals from different subjects. The length of the vertical axis of the ellipse is proportional to the papers’ counts published in the journal and the horizontal length is to authors. (B) The annual growth trends of the journals.
From Figure 6B, the 100 most impactful papers were published in 14 journals. Source dynamics show that most of relevant papers (n=33) were published in the New England Journal of Medicine and had an exponential-like growth in recent years (2012–2019), followed by the Journal of Clinical Oncology (n=28), the Lancet Oncology (n=15) and the Lancet (n=10).
The details are listed in Table 2. The New England Journal of Medicine had the highest IF (=91.253) and TC (=80,427). The 3 journals with the ratio of TC to publication over 2,000 were the Science (=5,933.00), the New England Journal of Medicine (=2,437.18), and the Mayo Clinic Proceedings (=2,049.00).
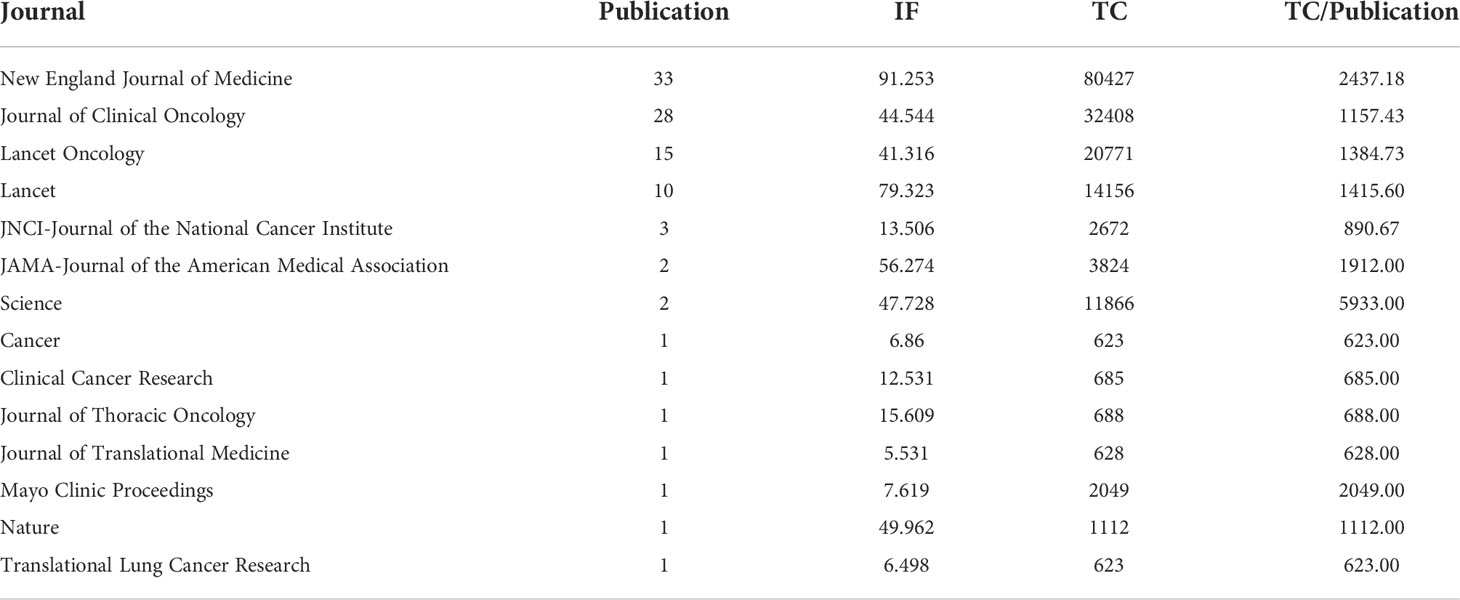
Table 2 Journals that published the most-cited 100 publications.
The theme of a paper is reflected in the keywords, and by analyzing them, researchers can get an idea of the topic of the article (23). The presence of two keywords from a certain field in the same article, called co-occurrence, reflected that there is some internal relationship between them, and the more they appear, the closer the relatedness is (24).
The keyword co-occurrence network (Figure 7A), based on the above principles, can detect the research dynamic and structure of the discipline (25). Keyword plus terms of WoS are effective and more broadly descriptive (26). We chose it to perform keyword analysis. The densest connecting lines around the keyword “chemotherapy” indicate that it is most closely related to other keywords.
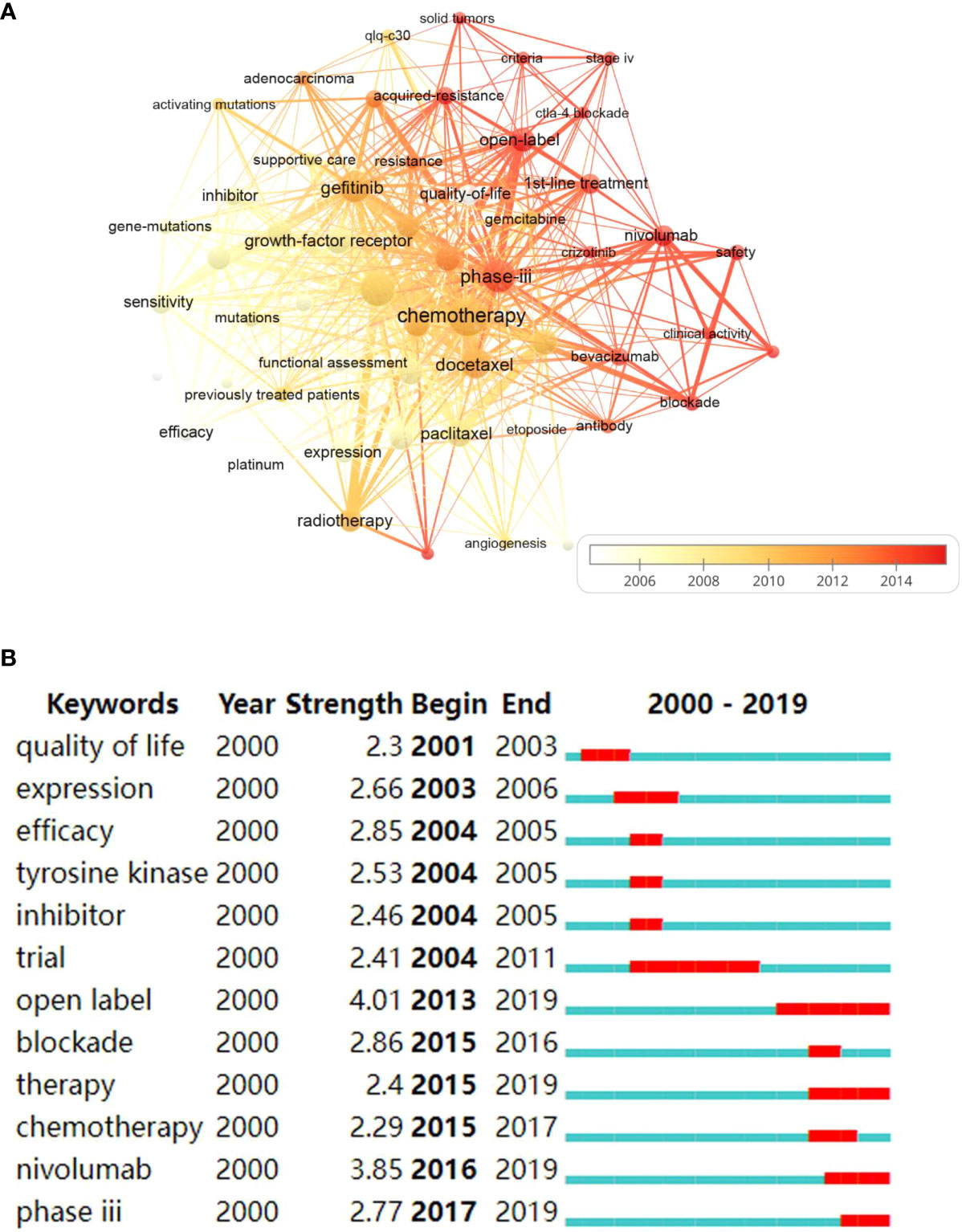
Figure 7 (A) The overlay visualization map of keywords co-occurrence. Each node represents a keyword. The size of circles and fonts is proportional to the frequency of keywords. The thickness of connecting lines stands for the co-occurrence frequency. The whiter the node is, the earlier the focus on this topic, and the redder is, the more attention it gets nowadays. (B) Keywords with strongest burst strength. The red bars indicate the sudden increase of occurrence frequency of the keyword in this period and the blue ones denote the unpopular period.
As is listed in Table 3, the keywords with the highest frequency were “chemotherapy” (n=36), followed by “clinical-trials” (n=28), “phase-iii” (n=24), and “gefitinib” (n=22).
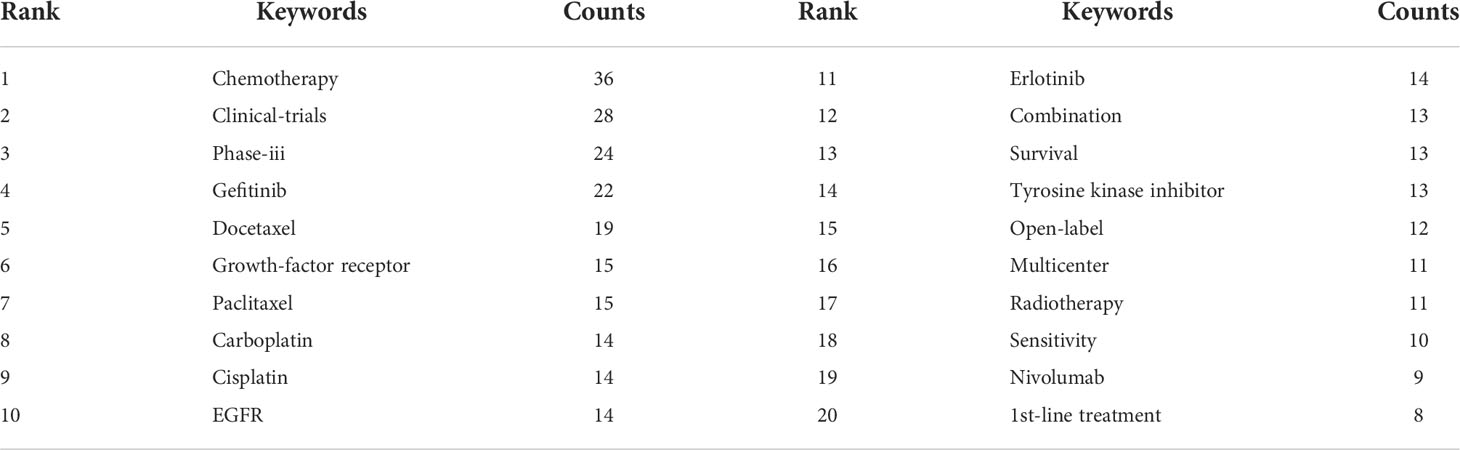
Table 3 Top 20 keywords with the most occurrence.
Figure 7B shows the keywords with the strongest burst strength. Burst-detection algorithms can recognize emerging terms regardless of the number of citations in the host articles, so that burst terms can sensitively and accurately capture the research frontiers (19). Keywords burst earlier indicate that researchers focused on this area in early years, while burst closer to the present denote the topic has suddenly attracted attention recently. The top 5 keywords identified are “open-label”, “nivolumab”, “blockade”, “efficacy” and “phase iii”, with the burst strength of 4.01, 3.85, 2.86, 2.85, and 2.77, respectively. “Quality of life” is the earliest keyword to burst, and the most recent burst keywords include “phase iii” and “nivolumab”. Keywords with the longest duration of burst are “trial” and “open label”.
Figure 8A exhibits the principles and landscape of NSCLC management. Chemotherapy, radiotherapy, surgery, targeted therapy and immunotherapy are the main regimens of current NSCLC treatment and have been widely used in clinical practice.
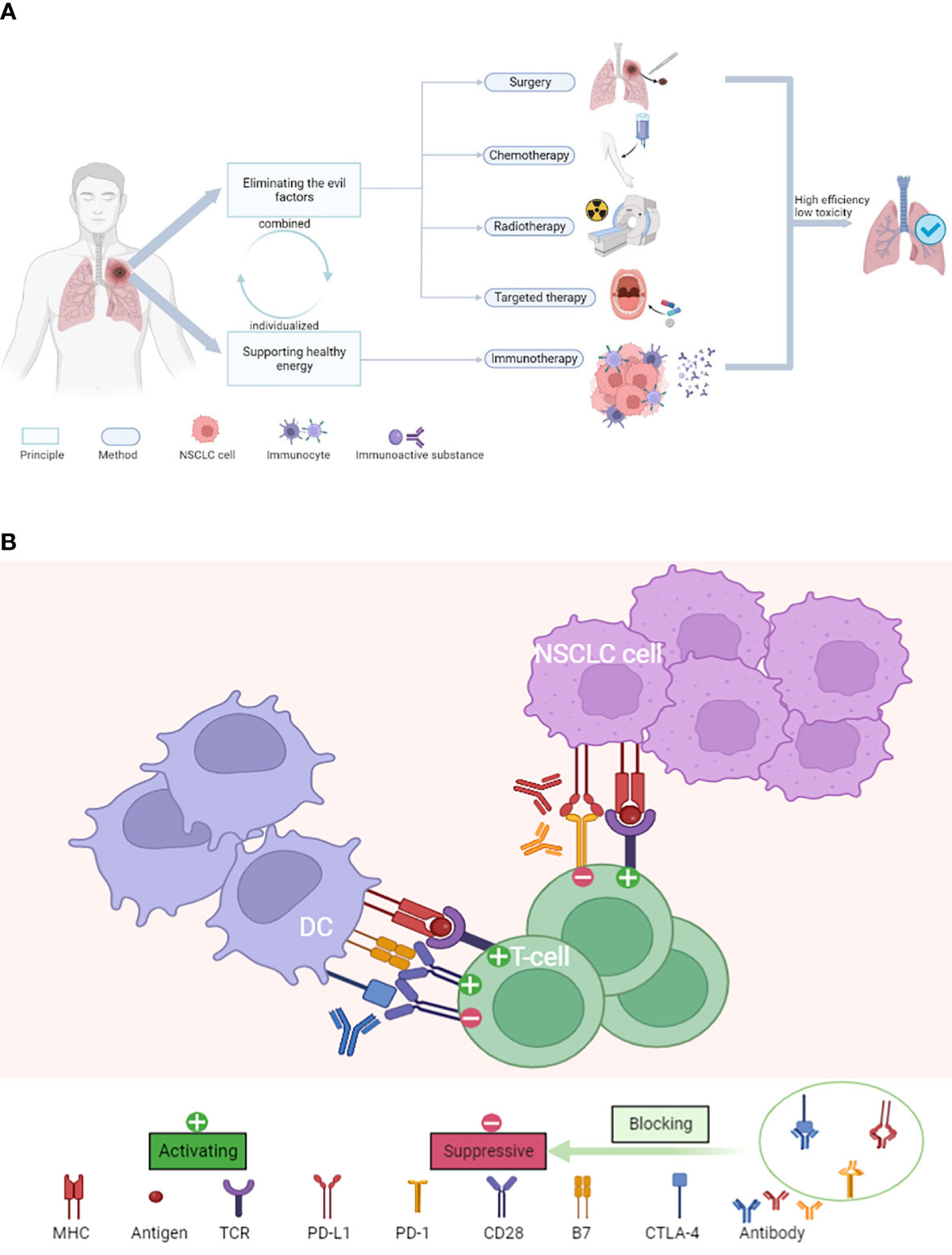
Figure 8 (A) The principles and landscape of NSCLC management. (B) The major mechanism of ICIs for the treatment of NSCLC.
As shown in Figure 8B, ICIs, as new therapeutic agents, have unique advantages, and the mechanism of the ICIs is more in line with the future research direction.
With the significant advancements and rapid changes in NSCLC treatments in the last 20 years, it is crucial to understand the progress and evolution of NSCLC management in the new era where many therapies coexist (5). However, available textbooks and papers lack such information. We selected 100 most impactful papers in this field as research data and applied the bibliometric analysis to systematically explore the output dynamics, research forces, topics, hotspots, and frontiers in the field of NSCLC treatment. It can help scholars quickly learn the basics, clarify study ideas, and learn the research status quo.
As can be seen from Figure 3, top articles evidenced the merits of international cooperation and witnessed a multi-national cooperation network with the United States as the core. Half of the top 10 institutions are from the United States (rank 1, 2, 4, 9, 10 in Table 1). There are 57 corresponding authors belonging to the United States, reflecting the United States is the originator of most top papers and has the most specialists. Additionally, some European countries such as Germany, Britain, and Italy, Canada in North America, and China, Japan, and Korea in Asia, also have outstanding performance in the field In 2000, a phase III clinical trial conducted in the United States demonstrated for the first time that docetaxel monotherapy versus vinorelbine/ifosfamide could provide clinical benefit for patients with advanced NSCLC who had relapsed or progressed after receiving platinum-based chemotherapy (27). A phase II study performed in the United States in 2004 investigated the clinical efficacy of erlotinib and found that rash might be a clinical marker for efficacy prediction (28). About a decade ago, this country explored the toxicity and efficacy of stereotactic body radiation therapy in patients with early-stage inoperable NSCLC and concluded that the therapy had high local control rates and moderate adverse events (29). In recent years, the country has also made significant achievements in immunotherapy, such as a single-arm clinical trial covering 27 sites in the United States, France, Germany, and Italy, which revealed favorable efficacy and safety of nivolumab in previously treated patients with refractory advanced squamous NSCLC (30). The United States leads all areas of NSCLC treatment in the world.
As illustrated in Figure 4, the Memorial Sloan Kettering Cancer Center is the foremost research institution for NSCLC management, with the most top-notch papers and highest TC, followed closely by Massachusetts General Hospital. AstraZeneca, the Dana-Farber Cancer Institute, and the Sungkyunkwan University also with exceptional academic results. These institutions all have a long history of distinguished contributions to the field of NSCLC therapy. We found that the major studies in which the Memorial Sloan Kettering Cancer Center was involved were divided into two parts: before 2015 the theme of research was targeted therapy, and after 2015 the topic was immunotherapy. In 2003, the institution participated in a phase II clinical trial that further demonstrated the benefit of gefitinib in improving post-chemotherapy NSCLC symptoms and inducing radiographic cancer regressions (31). In 2015, it was involved in a randomized, open-label, international phase III study comparing the efficacy of nivolumab and docetaxel in patients with non-squamous NSCLC that progressed during or after platinum-based dual chemotherapy, proved that nivolumab had longer overall survival (32). The study has been cited more than 5,000 times.
The major contributors (shown in Figure 5), such as Paz-Ares L., Reck M., and Wu Yl., come from different countries and are affiliated with different institutions. It is their long-lasting efforts and closer global collaboration that have driven the development of NSCLC treatment. We found that the distribution of the authors’ top papers seemed no correlation with time. Interestingly, both Paz-Ares L. and Reck M. had published remarkable results in 2018, and the topics were both centered on immunotherapy for NSCLC (33, 34). It was also in 2018 that the Nobel Prize in Physiology or Medicine Prize was granted to scientists James P. Allison (United States) and Tasuku Honjo (Japan) for their pioneering work in tumor immunotherapy. Thus, we assume that 2018 was an important time-point for NSCLC immunotherapy.
The distribution of the journals (Figure 6A) demonstrates the treatment of NSCLC is increasingly reliant on molecular, biological, and genetic fields. Thanks to breakthroughs in targeted therapeutic pathways, different targeted regimens have been applied to patients with different genetic mutations, such as EGFR-positive and ALK-positive mutations. Furthermore, that advancement can predict efficacy, safety, and prognosis of targeted therapy (35–37). The molecular mechanism of immune checkpoint blockade has been partially elucidated. Tumor mutation burden and PD-l expression levels were utilized to predict the outcome of immunotherapy (38, 39). The citations in journals related to immunology and computer science indicate that the field has moved toward multidisciplinary integration. Increasingly routine clinical application of targeted next-generation sequencing technology, immunohistochemical techniques, and comprehensive genomic profiling enables more precise NSCLC management and makes personalized management possible (38, 40, 41). Clinical trials and basic experiments are becoming growingly inseparable today, inaugurating the century of rapid advancement in NSCLC management.
From Figure 6B, the most authoritative journal in the field is the New England Journal of Medicine, which has the most top-cited papers, the fastest papers growth rate, the highest IF and TC, followed by Journal of Clinical Oncology, Lancet Oncology, etc. Papers published in these journals are likely to be of higher academic quality. The most cited paper in the New England Journal of Medicine is about 6,000 times. The paper reported an open-label, phase III trial for non-smoking or formerly lightly smoking untreated patients with adenocarcinoma in East Asia. It demonstrated superior progression-free survival with gefitinib as initial treatment over carboplatin-paclitaxel in this population (42).
As is presented in Figure 7A, chemotherapy and targeted therapy have been studied in a lot of top papers, while the counts of immunotherapy-related keywords, such as nivolumab, were relatively small, probably because it as an emerging regimen has not been heavily cited yet. Of note, the earliest article was published in 2000 on the topic of chemotherapy in NSCLC (27), and the most recent 3 publications published in 2018 and 2019, all focused on immunotherapy (33, 43, 44). The timeline of the keywords illustrated that the hotspots of NSCLC management have evolved from chemotherapy and radiotherapy to targeted therapy and then to immunotherapy.
Surgery and cytotoxic drugs were introduced to treat NSCLC in the 1960 and 1970, making the first leap forward in NSCLC treatment. Surgery is currently the most recommended method for NSCLC patients with stage I-II, yet 70% of patients are in advanced stage III-IV at the time of diagnosis. Cytotoxic drugs, targeted therapy, and immunotherapy are critical for patients with advanced NSCLC (41). Among 100 highly cited papers, there is no research with the theme of surgery for NSCLC, which may be related to the high maturity and effectiveness of video-assisted thoracic surgery (VATS) (45, 46). SABR is considered as a standard care for inoperable peripheral type early-stage NSCLC, showing meaningful clinical benefit (47). Over the past 21 years, the common cytotoxic chemotherapy, such as paclitaxel and docetaxel, remains the predominant therapy for advanced NSCLC to some extent, but with the development of targeted therapy, TKIs have become the first-line treatment for some driver gene mutation-positive NSCLC patients.
TKIs such as gefitinib, and anti-angiogenic agents such as bevacizumab, were approved by the Food and Drug Administration (FDA) for NSCLC treatment. New targeted therapeutics are continually being approved by the FDA. In 2003, gefitinib was granted for treatment of second-line, unselected advanced NSCLC (48). Then in 2006, bevacizumab plus paclitaxel and carboplatin became the first-line regimen for non-squamous NSCLC, approved by the FDA. Using ALK-TKIs and EGFR-TKIs as first-line in the 2010 updates the options for the therapy of NSCLC (41). Third-generation targeted agents, such as osimertinib, and new combination regimens, for example EGFR-TKI erlotinib in combination with anti-angiogenic agent ramucirumab approved for EGFR-mutant NSCLC in 2020, were also gradually being used in the clinical practice (5, 41). Along with the application of targeted therapies, researchers were also more devoted to studying gene mutations and growth-factor receptors, which are inextricably linked to the effectiveness of targeted therapy (40). There is no doubt that targeted therapy is a milestone in the treatment of NSCLC.
In Figure 7A, the large number of lines between treatment modalities implied combination application to different degrees, and the density of the lines did not decrease over time, pointing that combination medication has always been a concern for researchers and remains a hot academic topic, based on which we recommend scholars make more attempts on combination therapy for NSCLC. Keywords with higher burst strength may become the new turning point (49, 50), which can lead us to find emerging hotspots and frontiers of the field. Figure 7B show that after the research boom of targeted therapy represented by TKIs, immune checkpoint blockade represented by programmed cell death-1 (PD1) and programmed cell death ligand-1 (PD-L1) blockade, such as “nivolumab” with the burst strength of 3.85, may become turning points in NSCLC treatment. Actually, cytotoxic T-lymphocyte antigen-4 (CTLA-4) and PD-1/PD-L1 blockade are research frontiers. In 2015, the FDA authorized nivolumab for the treatment of patients whose tumor had progressed on or after platinum-based regimens, a dramatic breakthrough in the treatment of advanced NSCLC that foreshadowed an immune era in lung cancer treatment (5, 51). In 2016, pembrolizumab was approved as monotherapy for first-line treatment of NSCLC with PD-L1 ≥ 50%. Pembrolizumab combined with chemotherapy as first-line treatment for advanced non-squamous NSCLC, granted in 2017, provides survival benefit for patients without target gene mutations (41). Furthermore, durvalumab became a new treatment option for adjuvant therapy in 2018. In 2020, first-line treatment using nivolumab plus ipilimumab and double-platinum chemotherapy for advanced NSCLC also proved the effectiveness of ICIs therapy (52). Another PD-1 inhibitor, such as cemiplimab-rwlc, was approved for first-line treatment in 2021, further confirming the rise of immunotherapy (41). Immunotherapy is perhaps the most significant breakthrough in NSCLC treatment in the last 20 years. It has profoundly changed our treatment landscape and research outlook. More immunologic agents will be available for NSCLC management, while the comparison between different immunologic agents may be worth the attention of researchers. Indeed, immunotherapy has shown excellent anti-tumor effects and a better prognosis than conventional therapy for patients with advanced NSCLC without EGFR or ALK mutations. Although patients can benefit from ICIs, most of patients may develop resistance after use, and combination therapy is considered a viable approach to overcome acquired resistance (53, 54). At present, ICIs are being explored as combination or monotherapy in neoadjuvant or adjuvant settings for NSCLC management and the results were promising (34, 39, 44). New immunotherapies, such as tumor vaccines, are being developed (3, 55). Researchers are also paying more attention to issues such as drug safety and resistance (30, 56). In terms of trial design, “open label” trials with the burst strength of 4.01, and “phase iii” clinical trials, 2.77, were widely used in the top articles. The large sample size, multicenter, international collaborative RCTs and experiments are necessary to derive reliable studies. Top researchers preferred to explore the efficacy of the combination of various regimens in different types of NSCLC while are more passionate about seeking effective first-line treatment alternatives. Recently, in top-cited papers, immunotherapy and chemotherapy were often combined to treat NSCLC patients or used separately to compare clinical value (33, 43), which is also consistent with Figure 7B, where “chemotherapy” and “nivolumab” red bars overlap in some years.
As shown in Figure 8, the treatment principles of diseases can be divided into two parts: eliminating the evil factors and supporting healthy energy, which is complementary to each other. We think that the management of lung cancer may also be divided based on this principle. Traditional therapy methods (surgery, chemotherapy, radiotherapy, targeted therapy) (54) kill tumor cells directly, in keeping with the principle of eliminating harmful factors. On the other hand, immunotherapy destroys tumor cells indirectly by triggering or improving the immune function of the body, supporting healthy energy. The search for more effective, safer, and sustainable first-line treatment options using a combination of chemotherapy, radiotherapy, surgery, targeted therapy, and immunotherapy is the focus of researchers and clinicians in nowadays. The potential of immunotherapy has not yet been fully explored, and a new therapeutic leap after it is yet to come. Nevertheless, researchers should actively consider what the next epoch-making breakthrough after immunotherapy will be and conceive the future landscape of NSCLC treatment. We speculate that this breakthrough should be based on genetic and molecular technology, relying on the body’s inherent anti-tumor ability rather than the direct killing of tumors, in line with the principle of supporting healthy energy.
This study has certain limitations. First, although we identified the most influential papers in NSCLC management based on bibliometric citation analysis and the broad search terms we have formulated, there is still a possibility of missing articles, such as recently published papers that may be widely cited at a future date but do not currently accumulate enough citations to be included in our data. To minimize information omission caused by publication time, we discussed the latest papers to derive the new research progress in NSCLC treatment. Second, our data are all from the WoSCC, so some publications indexed in other databases may be omitted. Databases such as Scopus or PubMed can be used in further research. Third, bibliometric tools inevitably exclude some secondary topics when mapping despite our combination of multiple tools to counteract this effect, and this information probably is also important. Nonetheless, unlike most papers using single tools, we innovatively combined R software, CiteSpace, VOSviewer, and Excel, which may help us achieve comprehensive insights from multiple viewpoints. To our knowledge, the study is the first comprehensive bibliometric assessment of the evolution of NSCLC treatment in the 21st century.
We found that the United States is the strongest research nation and the Memorial Sloan Kettering Cancer Center is the most prominent institution over the last 20 years. Core authors, such as Paz-Ares L. and Reck M., have developed extensive international collaborations. The New England Journal is the most authoritative journal in the field. Molecular, biological, and genetic research plays a progressively important role in the treatment of NSCLC, while immunology and computer science have also been widely applied to this field. Hotspots of NSCLC management have almost undergone an evolution from chemotherapy and radiotherapy to targeted therapy to immunotherapy, while the exploration of combination therapy has never stopped. Immunotherapy and combination therapy are research frontiers. Encouraging progress has been made in the management of NSCLC in the last 2 decades, and more breakthroughs are sure to be explored in the future.
Overall, our study revealed leading countries, core institutions, distinguished authors, authoritative journals, citation relationships, topic dynamics, and research frontiers in the field of NSCLC management. That information may help researchers quickly sort out the historical progress of NSCLC treatment, provide insight into the future advancement of the field, and guide future research practice.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
ZL and SC designed the study. SC wrote the manuscript. SC, YH, and YQ selected the 100 most impactful papers and did the bibliometric analysis. YQ and JC guided the use of the software. SC, YQ, and JC framed the article. YL, JX, and PC proposed constructive opinions. ZH, DH, and YG helped retrieve data. ZL and YH led the team and revised the paper. All authors conducted the literature search and analyzed the data. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.939838/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA-Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc (2008) 83(3):355–67. doi: 10.4065/83.3.355
3. Zappa C, Mousa SA. Non-small cell lung cancer: Current treatment and future advances. Transl Lung Cancer Res (2016) 5(3):288–300. doi: 10.21037/tlcr.2016.06.07
4. Singh T, Hassanabad MF, Hassanabad AF. Non-small cell lung cancer: Emerging molecular targeted and immunotherapeutic agents. Biochim Biophys Acta-Rev Cancer (2021) 1876(2):34. doi: 10.1016/j.bbcan.2021.188636
5. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature (2018) 553(7689):446–54. doi: 10.1038/nature25183
6. Ricciuti B, Awad MM. What is the standard first-line treatment for advanced non-small cell lung cancer? Cancer J (2020) 26(6):485–95. doi: 10.1097/ppo.0000000000000489
7. Baumann P, Nyman J, Hoyer M, Wennberg B, Gagliardi G, Lax I, et al. Outcome in a prospective phase ii trial of medically inoperable stage I non-Small-Cell lung cancer patients treated with stereotactic body radiotherapy. J Clin Oncol (2009) 27(20):3290–6. doi: 10.1200/jco.2008.21.5681
8. Xu G, Jin B, Xian XM, Yang HY, Zhao HT, Du SD, et al. Evolutions in the management of hepatocellular carcinoma over last 4 decades: An analysis from the 100 most influential articles in the field. Liver Cancer (2021) 10(2):137–50. doi: 10.1159/000513412
9. Zhang J, Song LX, Xu LY, Fan YX, Wang T, Tian WD, et al. Knowledge domain and emerging trends in ferroptosis research: A bibliometric and knowledge-map analysis. Front Oncol (2021) 11:686726. doi: 10.3389/fonc.2021.686726
10. Da W, Tao ZB, Meng Y, Wen KC, Zhou SM, Yang KD, et al. A 10-year bibliometric analysis of osteosarcoma and cure from 2010 to 2019. BMC Cancer (2021) 21(1):15. doi: 10.1186/s12885-021-07818-4
11. Aria M, Cuccurullo C. Bibliometrix: An r-tool for comprehensive science mapping analysis. J Informetr (2017) 11(4):959–75. doi: 10.1016/j.joi.2017.08.007
12. Brooke BS, Nathan H, Pawlik TM. Trends in the quality of highly cited surgical research over the past 20 years. Ann Surg (2009) 249(1):162–7. doi: 10.1097/SLA.0b013e31819291f9
13. Wang YX, Zhao N, Zhang XW, Li ZH, Liang Z, Yang JR, et al. Bibliometrics analysis of butyrophilins as immune regulators 1992-2019 and implications for cancer prognosis. Front Immunol (2020) 11:1187. doi: 10.3389/fimmu.2020.01187
14. Mulet-Forteza C, Genovart-Balaguer J, Mauleon-Mendez E, Merigo JM. A bibliometric research in the tourism, leisure and hospitality fields. J Bus Res (2019) 101:819–27. doi: 10.1016/j.jbusres.2018.12.002
15. Chen CM, Hu ZG, Liu SB, Tseng H. Emerging trends in regenerative medicine: A scientometric analysis in citespace. Expert Opin Biol Ther (2012) 12(5):593–608. doi: 10.1517/14712598.2012.674507
16. Grunsky EC. R: A data analysis and statistical programming environment - an emerging tool for the geosciences. Comput Geosci (2002) 28(10):1219–22. doi: 10.1016/s0098-3004(02)00034-1
17. Matloff N. The art of r programming: A tour of statistical software design. (San Francisco, California, USA: No Starch Press) (2011).
18. van Eck NJ, Waltman L. Software survey: Vosviewer, a computer program for bibliometric mapping. Scientometrics (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
19. Chen CM. Citespace ii: Detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol (2006) 57(3):359–77. doi: 10.1002/asi.20317
20. Ding H, Wu C, Liao N, Zhan Q, Sun W, Huang Y, et al. Radiomics in oncology: A 10-year bibliometric analysis. Front Oncol (2021) 11:689802. doi: 10.3389/fonc.2021.689802
21. Chen CM, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: A scientometric update (2000 - 2014). Expert Opin Biol Ther (2014) 14(9):1295–317. doi: 10.1517/14712598.2014.920813
22. Chen CM, Leydesdorff L. Patterns of connections and movements in dual-map overlays: A new method of publication portfolio analysis. J Assoc Inf Sci Technol (2014) 65(2):334–51. doi: 10.1002/asi.22968
23. Jin YC, Li JW, Li JY, Zhang N, Guo KL, Zhang QI, et al. Visualized analysis of heavy ion radiotherapy: Development, barriers and future directions. Front Oncol (2021) 11:634913. doi: 10.3389/fonc.2021.634913
24. Lee PC, Su HN. Investigating the structure of regional innovation system research through keyword Co-occurrence and social network analysis. Innov-Manag Policy Pract (2010) 12(1):26–40. doi: 10.5172/impp.12.1.26
25. Li HJ, An HZ, Wang Y, Huang JC, Gao XY. Evolutionary features of academic articles Co-keyword network and keywords Co-occurrence network: Based on two-mode affiliation network. Physica A (2016) 450:657–69. doi: 10.1016/j.physa.2016.01.017
26. Zhang J, Yu Q, Zheng FS, Long C, Lu ZX, Duan ZG. Comparing keywords plus of wos and author keywords: A case study of patient adherence research. J Assoc Inf Sci Technol (2016) 67(4):967–72. doi: 10.1002/asi.23437
27. Fossella FV, DeVore R, Kerr RN, Crawford J, Natale RR, Dunphy F, et al. Randomized phase iii trial of docetaxel versus vinorelbine or ifosfamide in patients with advanced non-Small-Cell lung cancer previously treated with platinum-containing chemotherapy regimens. J Clin Oncol (2000) 18(12):2354–62. doi: 10.1200/jco.2000.18.12.2354
28. Perez-Soler R, Chachoua A, Hammond LA, Rowinsky EK, Huberman M, Karp D, et al. Determinants of tumor response and survival with erlotinib in patients with non-Small-Cell lung cancer. J Clin Oncol (2004) 22(16):3238–47. doi: 10.1200/jco.2004.11.057
29. Timmerman R, Paulus R, Galvin J, Michalski J, Straube W, Bradley J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA-J Am Med Assoc (2010) 303(11):1070–6. doi: 10.1001/jama.2010.261
30. Rizvi NA, Mazieres J, Planchard D, Stinchcombe TE, Dy GK, Antonia SJ, et al. Activity and safety of nivolumab, an anti-Pd-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-Small-Cell lung cancer (Checkmate 063): A phase 2, single-arm trial. Lancet Oncol (2015) 16(3):257–65. doi: 10.1016/s1470-2045(15)70054-9
31. Kris MG, Natale RB, Herbst RS, Lynch TJ, Prager D, Belani CP, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer - a randomized trial. JAMA-J Am Med Assoc (2003) 290(16):2149–58. doi: 10.1001/jama.290.16.2149
32. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non-Small-Cell lung cancer. N Engl J Med (2015) 373(17):1627–39. doi: 10.1056/NEJMoa1507643
33. Gandhi L, Rodriguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-Small-Cell lung cancer. N Engl J Med (2018) 378(22):2078–92. doi: 10.1056/NEJMoa1801005
34. Hellmann MD, Ciuleanu TE, Pluzanski A, Lee JS, Otterson GA, Audigier-Valette C, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med (2018) 378(22):2093–104. doi: 10.1056/NEJMoa1801946
35. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated egfr-mutated advanced non-Small-Cell lung cancer. N Engl J Med (2018) 378(2):113–25. doi: 10.1056/NEJMoa1713137
36. Camidge DR, Bang YJ, Kwak EL, Iafrate AJ, Varella-Garcia M, Fox SB, et al. Activity and safety of crizotinib in patients with alk-positive non-Small-Cell lung cancer: Updated results from a phase 1 study. Lancet Oncol (2012) 13(10):1011–9. doi: 10.1016/s1470-2045(12)70344-3
37. Eberhard DA, Johnson BE, Amler LC, Goddard AD, Heldens SL, Herbst RS, et al. Mutations in the epidermal growth factor receptor and in kras are predictive and prognostic indicators in patients with non-Small-Cell lung cancer treated with chemotherapy alone and in combination with erlotinib. J Clin Oncol (2005) 23(25):5900–9. doi: 10.1200/jco.2005.02.857
38. Rizvi H, Sanchez-Vega F, La K, Chatila W, Jonsson P, Halpenny D, et al. Molecular determinants of response to anti-programmed cell death (Pd)-1 and anti-programmed death-ligand 1 (Pd-L1) blockade in patients with non-Small-Cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol (2018) 36(7):633–+. doi: 10.1200/jco.2017.75.3384
39. Forde PM, Chaft JE, Smith KN, Anagnostou V, Cottrell TR, Hellmann MD, et al. Neoadjuvant pd-1 blockade in resectable lung cancer. N Engl J Med (2018) 378(21):1976–86. doi: 10.1056/NEJMoa1716078
40. Tsao MS, Sakurada A, Cutz JC, Zhu CQ, Kamel-Reid S, Squire J, et al. Erlotinib in lung cancer - molecular and clinical predictors of outcome. N Engl J Med (2005) 353(2):133–44. doi: 10.1056/NEJMoa050736
41. Cheng Y, Zhang T, Xu Q. Therapeutic advances in non-small cell lung cancer: Focus on clinical development of targeted therapy and immunotherapy. MedComm (2021) 2(4):692–729. doi: 10.1002/mco2.105
42. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med (2009) 361(10):947–57. doi: 10.1056/NEJMoa0810699
43. Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho BC, Turna HZ, et al. Pembrolizumab versus chemotherapy for previously untreated, pd-L1-Expressing, locally advanced or metastatic non-Small-Cell lung cancer (Keynote-042): A randomised, open-label, controlled, phase 3 trial. Lancet (2019) 393(10183):1819–30. doi: 10.1016/s0140-6736(18)32409-7
44. Hellmann MD, Paz-Ares L, Caro RB, Zurawski B, Kim SW, Costa EC, et al. Nivolumab plus ipilimumab in advanced non-Small-Cell lung cancer. N Engl J Med (2019) 381(21):2020–31. doi: 10.1056/NEJMoa1910231
45. Cao C, Manganas C, Ang SC, Peeceeyen S, Yan TD. Video-assisted thoracic surgery versus open thoracotomy for non-small cell lung cancer: A meta-analysis of propensity score-matched patients. Interact Cardiovasc Thorac Surg (2013) 16(3):244–9. doi: 10.1093/icvts/ivs472
46. Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ, Wu YL, et al. Lung cancer: Current therapies and new targeted treatments. Lancet (2017) 389(10066):299–311. doi: 10.1016/s0140-6736(16)30958-8
47. Senthi S, Lagerwaard FJ, Haasbeek CJA, Slotman BJ, Senan S. Patterns of disease recurrence after stereotactic ablative radiotherapy for early stage non-Small-Cell lung cancer: A retrospective analysis. Lancet Oncol (2012) 13(8):802–9. doi: 10.1016/s1470-2045(12)70242-5
48. Blackhall F, Ranson M, Thatcher N. Where next for gefitinib in patients with lung cancer? Lancet Oncol (2006) 7(6):499–507. doi: 10.1016/s1470-2045(06)70725-2
49. Chen CM. Searching for intellectual turning points: Progressive knowledge domain visualization. Proc Natl Acad Sci U.S.A. (2004) 101:5303–10. doi: 10.1073/pnas.0307513100
50. Kleinberg J. Bursty and hierarchical structure in streams. Data Min Knowl Discovery (2003) 7(4):373–97. doi: 10.1023/a:1024940629314
51. Kazandjian D, Suzman DL, Blumenthal G, Mushti S, He K, Libeg M, et al. Fda approval summary: Nivolumab for the treatment of metastatic non-small cell lung cancer with progression on or after platinum-based chemotherapy. Oncologist (2016) 21(5):634–42. doi: 10.1634/theoncologist.2015-0507
52. Paz-Ares L, Ciuleanu TE, Cobo M, Schenker M, Zurawski B, Menezes J, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-Small-Cell lung cancer (Checkmate 9la): An international, randomised, open-label, phase 3 trial. Lancet Oncol (2021) 22(2):198–211. doi: 10.1016/s1470-2045(20)30641-0
53. Blach J, Wojas-Krawczyk K, Nicos M, Krawczyk P. Failure of immunotherapy-the molecular and immunological origin of immunotherapy resistance in lung cancer. Int J Mol Sci (2021) 22(16):16. doi: 10.3390/ijms22169030
54. Kong FM, Wang ZW, Liao DY, Zuo JH, Xie HX, Li XJ, et al. Non-small cell lung cancer: Challenge and improvement of immune drug resistance. Front Oncol (2021) 11:739191. doi: 10.3389/fonc.2021.739191
55. Pateras IS, Kotsakis A, Avgeris M, Baliou E, Kouroupakis P, Patsea E, et al. Clinical activity of an htert-specific cancer vaccine (Vx-001) in "Immune desert" NSCLC. Cancers (2021) 13(7):13. doi: 10.3390/cancers13071658
Keywords: non-small cell lung cancer (NSCLC), management, treatment, bibliometric, R, VOSviewer, Citespace
Citation: Chen S, Qiao Y, Chen J, Li Y, Xie J, Cui P, Huang Z, Huang D, Gao Y, Hu Y and Liu Z (2022) Evolutions in the management of non-small cell lung cancer: A bibliometric study from the 100 most impactful articles in the field. Front. Oncol. 12:939838. doi: 10.3389/fonc.2022.939838
Received: 09 May 2022; Accepted: 01 August 2022;
Published: 17 August 2022.
Edited by:
Mohamed Rahouma, NewYork-Presbyterian, United StatesReviewed by:
Chunxia Su, Shanghai Pulmonary Hospital, ChinaCopyright © 2022 Chen, Qiao, Chen, Li, Xie, Cui, Huang, Huang, Gao, Hu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhefeng Liu, bHpmMTIyMEBzaW5hLmNvbQ==; Yi Hu, aHV5aTMwMXpseGJAc2luYS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.