
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Oncol., 25 July 2022
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.934426
This article is part of the Research TopicUpdates on Current Protocols for the Management of Brain and Spine MalignanciesView all 15 articles
 Jordina Rincon-Torroella1,2
Jordina Rincon-Torroella1,2 Maureen Rakovec1
Maureen Rakovec1 Josh Materi1
Josh Materi1 Divyaansh Raj1
Divyaansh Raj1 Tito Vivas-Buitrago3
Tito Vivas-Buitrago3 Abel Ferres2William Reyes Serpa3Kristin J. Redmond4Matthias Holdhoff5Chetan Bettegowda1*
Abel Ferres2William Reyes Serpa3Kristin J. Redmond4Matthias Holdhoff5Chetan Bettegowda1* José Juan González Sánchez2*
José Juan González Sánchez2*Oligodendrogliomas are a subtype of adult diffuse glioma characterized by their better responsiveness to systemic chemotherapy than other high-grade glial tumors. The World Health Organization (WHO) 2021 brain tumor classification highlighted defining molecular markers, including 1p19q codeletion and IDH mutations which have become key in diagnosing and treating oligodendrogliomas. The management for patients with oligodendrogliomas includes observation or surgical resection potentially followed by radiation and chemotherapy with PCV (Procarbazine, Lomustine, and Vincristine) or Temozolomide. However, most of the available research about oligodendrogliomas includes a mix of histologically and molecularly diagnosed tumors. Even data driving our current management guidelines are based on post-hoc subgroup analyses of the 1p19q codeleted population in landmark prospective trials. Therefore, the optimal treatment paradigm for molecularly defined oligodendrogliomas is incompletely understood. Many questions remain open, such as the optimal timing of radiation and chemotherapy, the response to different chemotherapeutic agents, or what genetic factors influence responsiveness to these agents. Ultimately, oligodendrogliomas are still incurable and new therapies, such as targeting IDH mutations, are necessary. In this opinion piece, we present relevant literature in the field, discuss current challenges, and propose some studies that we think are necessary to answer these critical questions.
Oligodendrogliomas are a subtype of adult diffuse glioma characterized by isocitrate dehydrogenase (IDH) mutation and the codeletion of the short arm of chromosome 1 (1p) and the long arm of chromosome 19 (19q) (1). They are rare primary brain tumors that present with variable outcomes and for which curative therapy does not exist. Oligodendrogliomas have evoked much interest given their favorable prognosis and better response to treatment compared to astrocytomas and glioblastomas, their more malignant counterparts. Historically, the diagnosis of oligodendrogliomas was purely histological, based on the characteristic “fried-egg” appearance of oligodendroglial cells, which was subject to considerable interobserver variation (2, 3). Exhaustive research led to discovering the 1p/19q codeletion, a molecular marker that has come to define oligodendroglioma (4–6). Hence, the diagnosis of oligodendroglioma became molecular instead of histological.
The WHO 2021 brain tumor classification reinforced this requirement and included 1p/19q codeletion and IDH mutation as defining traits of oligodendroglioma (1). Given that this change became official in relatively recent times, it is not surprising that pivotal prospective trials that guide current clinical decisions were based on the histological diagnosis of oligodendroglioma (7, 8). Retrospective research conducted before or even after that critical change studied a mix of histological and molecularly diagnosed oligodendrogliomas with the risk of including tumors that may not be classified as oligodendrogliomas now (9–15). There is a paucity of studies on purely molecularly defined oligodendrogliomas and those usually have a small number of patients or limited follow-up time (16–22).
Technological developments over the past decade allowed the implementation of genomic studies to our current standard of care for brain tumors, including complex next-generation sequencing (NGS) to decipher their genomic features. Consequently, patients may receive detailed results of NGS panels that describe several tumor-associated mutations. Although many advances have been made, we do not fully understand the clinical implications of those mutations and how a specific genomic signature affects an individual patient’s outcome. This is especially true for oligodendrogliomas, where follow-up lasting 10-20 years may be required to understand the impact on prognosis.
Here, we summarize the scientific basis of current management decisions, pose critical questions that remain unanswered, and highlight ongoing or future studies that can improve the management of patients with oligodendrogliomas.
Oligodendrogliomas represent only 5%-10% of all glial tumors in population-based studies (23, 24). Although they typically occur in younger adults, they can appear at any age, have a higher incidence in men, and are rare in children (24, 25). More than 70% of oligodendrogliomas are WHO grade 2, and approximately 20% are WHO grade 3 (1, 24).
The diagnosis of oligodendrogliomas requires the presence of both 1p/19q codeletion and IDH mutation (1). Two landmark papers in 2015 were pivotal to adopting this change. The first was a population-based study of 1087 diffuse gliomas that analyzed the mutation status of 1p/19q, IDH1 and 2, and TERT promoter. Classifying grade 2 and 3 gliomas based upon those mutations stratified the tumors into five molecular subgroups that were independently associated with clinical outcomes. This included the “triple positive” group, which harbored 1p/19q codeletion, IDH, and TERT promoter mutations. Triple-positive gliomas were most strongly associated with the oligodendroglial histologic type and better overall survival (4). This strengthened the importance of harboring an IDH mutation in addition to a 1p19q codeletion to confer a better prognosis, which was already described by Cairncross et al. and Jiao et al. in prior studies (26, 27). The second landmark paper was a genome-wide study of 293 low-grade gliomas by the TCGA Research Network. The group identified three molecular subtypes of lower-grade gliomas using a wide array of genomic, methylation, and protein expression analyses. The IDH-methylated, the IDH-wildtype, and the 1p/19q codeleted subgroups were found to be three prognostically significant and non-overlapping subtypes. Those two molecular markers (IDH mutation and 1p/19q codeletion) became critical in the current diagnosis of gliomas (5). This study also confirmed previous reports by our team and others identifying CIC and FUBP1 as potential oligodendroglioma tumor suppressor genes lost on chromosomes 1p and 19q, respectively (27, 28). Other molecular mutations frequently reported in gliomas, including chromosome 9p deletion and subsequent CDKN2A gene loss, have also been postulated to be involved in oligodendroglioma pathogenesis and malignant progression (29). Markers that drive an aggressive phenotype specifically in anaplastic oligodendroglioma have also been reported, including the transcription factor TCF12 (29). The specific role of these and other molecular markers and their effect on survival remain unclear.
Despite prior research, the optimal treatment paradigm for oligodendrogliomas is still in question (25). Management may start with surgery or observation. Many glioma studies have indicated that more extensive tumor resection with functional preservation is associated with prolonged survival (10–12, 30–33). Thus, although there is limited specific data on molecularly defined oligodendrogliomas, surgery for pathological diagnosis and maximal safe resection remains the favored initial therapeutic approach (31–34).
After surgical removal, upfront treatments for grade 2 oligodendrogliomas include observation (specifically in younger patients who underwent gross total resection [GTR]) or radiation with adjuvant chemotherapy. Grade 3 oligodendrogliomas are typically treated by surgical resection followed by radiation and chemotherapy, although observation may be an option in low-risk cases (35, 36). High-risk has been traditionally considered as being over 40 years of age or receiving less than GTR; however, this is controversial given the indolent biology of these tumors.
Current adjuvant treatment guidelines for oligodendrogliomas are based on two landmark clinical trials in anaplastic oligodendrogliomas and anaplastic oligoastrocytomas. These were the EORTC 26951 by the European Organization for Research and Treatment of Cancer and RTOG 9402 by the Radiation Therapy Oncology Group (7, 8). Both studies compared the role of Procarbazine, Lomustine - also known as CCNU, and Vincristine (PCV) in combination with radiotherapy with that of radiation therapy alone. However, the timing of radiotherapy was not evaluated. In addition, these trials were designed before discovering the prognostic implications of 1p/19q codeletion and IDH mutations. The 1p/19q codeletion was detected in 48% (126 of 263) of the cases in the RTOG and only 25% (80 of 316) in the EORTC trial (7, 8). In post-hoc analyses, both trials demonstrated that tumors with a 1p/19q codeletion benefitted from adding PCV to radiation therapy, markedly increasing the overall survival (OS) of patients with anaplastic oligodendroglioma. Specifically in RTOG 9402 the addition of PCV to RT improved OS from 7.3 to 14.7 years, and OS was not reached at the time of the EORTC 26951 data publication (7, 8). Studies attempting to identify the molecular determinants of survival from the RTOG 9402 were unsuccessful, largely due to a lack of sufficient samples (37).
The PCV regimen entails considerable side effects, including myelosuppression, hepatotoxicity, and neurotoxicity. Grade 3 or 4 hematologic toxicity was reported in more than 45% of the patients assigned to the experimental arm in the EORTC 26951 and RTOG 9402 trials (8, 38). Both studies were launched before the introduction of the oral alkylating agent temozolomide (TMZ) into neuro-oncology practice. TMZ has a more favorable toxicity profile than PCV and neuro-oncologists had become familiar with it in treating high-grade astrocytomas. With the RTOG 9402 and EORTC 26951 data pending, many neuro-oncologists started treating patients with the same regimen used for glioblastoma. TMZ resulted in considerable response rates and promising survival when used as “salvage” chemotherapy in oligodendroglioma relapse after the failure of PCV (39). However, retrospective studies of newly diagnosed oligodendrogliomas treated with TMZ alone revealed very variable outcomes with controversial conclusions (40, 41). The striking results of RTOG 9402 and EORTC 26951, two independently conducted, randomized studies with PCV, challenged the use of radiation and TMZ for oligodendrogliomas, as a comparable level of evidence did not exist for this regimen (25, 42, 43).
An ongoing international phase III clinical trial (CODEL, NCT00887146) was designed to resolve this mystery (44). The CODEL trial compares the efficacy of concomitant radiotherapy with TMZ followed by adjuvant TMZ versus radiotherapy with adjuvant PCV. It is well known that radiotherapy provides an improved progression-free survival for oligodendroglioma patients. In fact, the CODEL trial was initially designed to compare TMZ alone, radiotherapy alone, and radiotherapy with concomitant and adjuvant TMZ. Because the TMZ-alone patients experienced significantly shorter progression-free survival when compared to the patients in the radiotherapy arms, CODEL was redesigned to its current paradigm (44). Radiotherapy has shown promising efficacy with oligodendrogliomas, but there is significant concern for its long-term neurocognitive effects, and the timing of radiotherapy is questioned (16, 25). An ongoing clinical trial (POLCA, NCT02444000) investigates the difference between upfront radiotherapy with PCV versus upfront PCV with deferred radiotherapy. Another active phase III clinical trial (NCT00978458) conducted by the Eastern Cooperative Oncology Group and the National Cancer Institute (NCI) is evaluating whether the addition of TMZ to adjuvant radiation therapy improves survival in patients with low grade glioma, including oligodendroglioma (45). These studies may provide some answers to those critical questions, but the final results will not be available for years. In fact, the expected completion time for primary outcome data collection since the initiation of the CODEL and POLCA trials is 16 and 9 years, respectively (46, 47).
In light of those challenges, both the European Association of Neuro-Oncology (EANO) and the joint American Society of Clinical Oncology (ASCO) and Society for Neuro-Oncology (SNO) recognized the need for clarification by publishing recent evidence-based guidelines on the management of diffuse gliomas, including oligodendrogliomas (35, 36). There have also been changes in the National Comprehensive Cancer Network (NCCN) guidelines for oligodendrogliomas (48). A comparison of those guidelines is presented in Table 1.
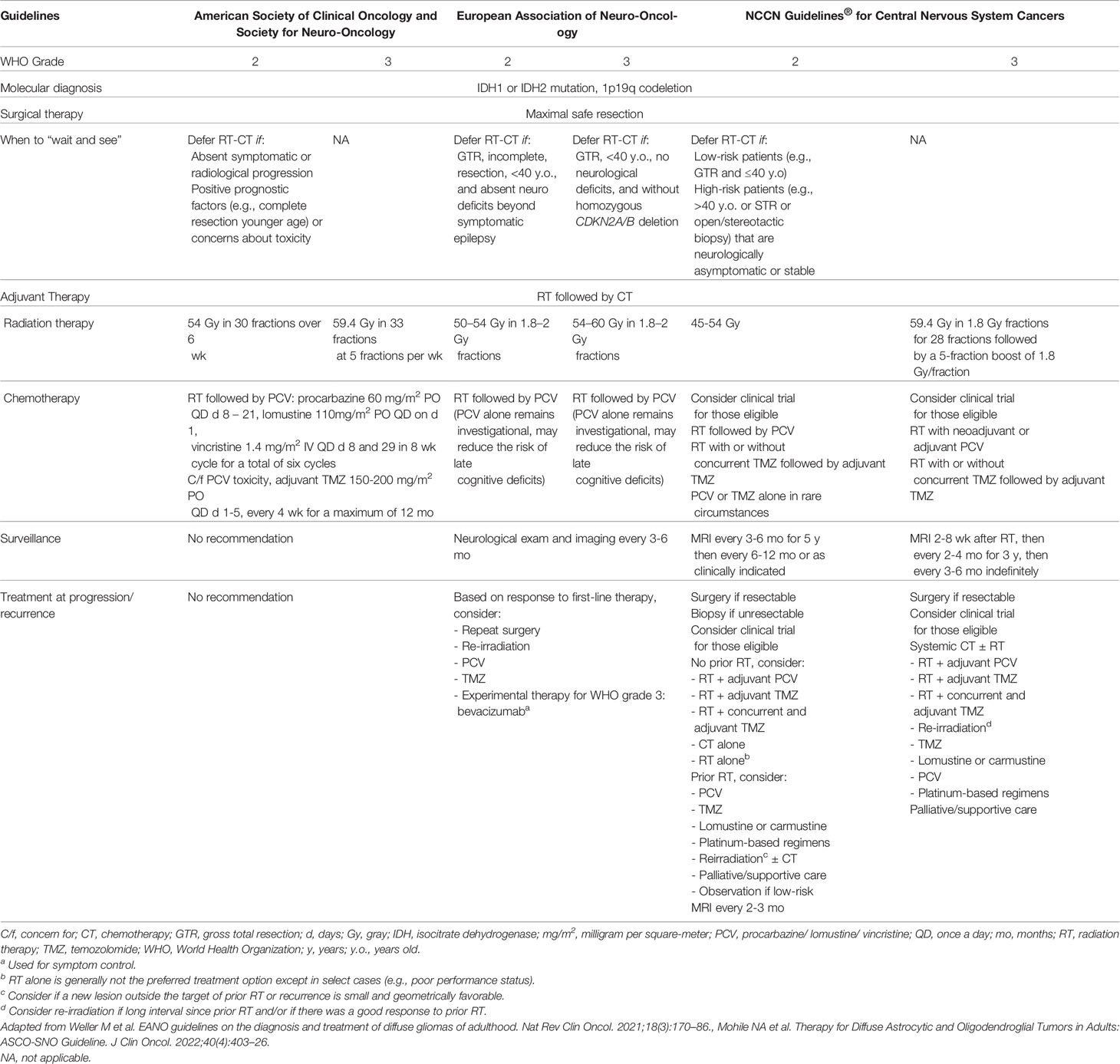
Table 1 Societal guidelines for oligodendroglioma management.
In summary, the current management for suspected oligodendroglioma consists of observation, surgery, radiation treatment, and chemotherapy. Observation is questionable given the strong evidence in favor of adjuvant therapy. Radiation treatment can be given after surgery and before chemotherapy, or chemotherapy can be given first, with radiation deferred to tumor progression. PCV is the chemotherapy of choice in the official guidelines, with TMZ reserved in those cases with PCV toxicity. In the past, both radiation and chemotherapy were usually delayed in the treatment of oligodendrogliomas. However, given the striking response to chemotherapy, the early use of adjuvant therapies has been favored in the past few years, especially in grade 3 oligodendrogliomas. For example, a 2019 study of the National Cancer Database showed that radiation followed by chemotherapy is the favored sequence of adjuvant therapy for grade 3 oligodendrogliomas in the US (13). Beyond current treatment, new therapeutic avenues are necessary and underway. Exciting work has been done targeting mutant IDH or related pathways. An important example is INDIGO (NCT04164901), an ongoing randomized phase III study of vorasidenib, a promising oral inhibitor of IDH1/2 mutations that has shown a 30.8% objective response rate in non-enhancing glioma patients (49). Other drugs that target molecular markers including abemaciclib, a CDK inhibitor selective for CDK4 and CDK6, are also being investigated for use in oligodendroglioma patients in ongoing clinical trials (NCT03969706) (50).
As described, many questions remain unanswered regarding the management of oligodendrogliomas, and a comprehensive understanding of current practices is not known. This was stressed in the oligodendroglioma workshop organized by the National Cancer Institute’s NCI-CONNECT in 2018 (25). However, in part due to the low incidence and high complexity of oligodendroglioma management, few of those questions have been clarified. In addition, available prospective data on the management of molecularly defined oligodendrogliomas are either indirect or from post-hoc subgroup analysis with potential risk of bias. More definitive answers may be provided by ongoing long-lasting multi-institutional clinical trials based on molecular criteria. In our opinion, intermediate answers are required to shed light on the current management of this type of tumor and standardize practices. First, it is paramount that any future oligodendroglioma study is based on the current molecular definition of oligodendroglioma, confirming 1p19q codeletion and IDH mutation. Second, we believe that surveying the oncological and neurosurgical societies would clarify if current treatment trends, especially adjuvant therapy utilization and chemotherapy regimen selection, differ between geographical regions given the current lack of universal and standardized worldwide guidelines. Although not definitive, an exhaustive study of the clinical features, management, genetic profile, and outcomes of purely molecularly defined oligodendrogliomas in a large retrospective cohort would potentially unveil characteristic features and provide updated management guidance based on current diagnostic standards. This can also help improve risk stratification to extend beyond age and extent of resection. Changes in medical practice are complex and require widespread dissemination of information. In the long run, a worldwide task force in charge of revising and implementing the CODEL and POLCA trial results will be essential to translate high-quality data into daily practices. Finally, oligodendrogliomas are still not curable, and new therapeutic avenues are imperative. Whether IDH inhibitors become integral to treating this disease remains to be evaluated. These and other important clinical trials are desperately needed to improve outcomes for patients with oligodendroglioma.
Here, we have summarized the current advancements in the molecular characterization of oligodendrogliomas and reviewed adjuvant treatment modalities currently used in its treatment. The future directions in research we have outlined, including retrospective and clinical trials, have significant potential to further advance the management and prognosis of oligodendroglioma patients when effectively translated into clinical practice.
JR-T, CB, and JJGS devised the project, the main conceptual ideas, and the proof outline. JR-T, MR, JM, DR, TV-B, AF, WRS, KR, MH, CB, and JJGS contributed to the design and implementation of the research, the analysis of the results, and the writing of the manuscript. In addition, WRS, CB, and JJGS provided institutional support. All the authors approved and reviewed the submitted version of the manuscript.
JR-T is an NINDS R25 training grant awardee (5R25NS065729).
CB is a consultant for Depuy-Synthes, Bionaut Labs and Galectin Therapeutics and a co-founder of OrisDx. KR: Research support from Elekta AB, Accuray, Canon; Data Safety Monitoring Board for BioMimetix; Travel expenses from Brainlab, Elekta AB, Accuray, Icotec, RSS; Honorarium for speaking engagement NCCN, Accuray.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Universidad de Santander and Universitat de Barcelona for their administrative support.
1. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro Oncol (2021) 23(8):1231–51. doi: 10.1093/neuonc/noab106
2. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol (2007) 114(2):97–109. doi: 10.1007/s00401-007-0243-4
3. Kros JM, Gorlia T, Kouwenhoven MC, Zheng P-P, Collins VP, Figarella-Branger D, et al. Panel Review of Anaplastic Oligodendroglioma From European Organization For Research and Treatment of Cancer Trial 26951: Assessment of Consensus in Diagnosis, Influence of 1p/19q Loss, and Correlations With Outcome. J Neuropathol Exp Neurol (2007) 66(6):545–51. doi: 10.1097/01.jnen.0000263869.84188.72
4. Eckel-Passow JE, Lachance DH, Molinaro AM, Walsh KM, Decker PA, Sicotte H, et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. N Engl J Med (2015) 372(26):2499–508. doi: 10.1056/NEJMoa1407279
5. Brat DJ, Verhaak RGW, Aldape KD, Yung WKA, Salama SR, Cooper LAD, et al. Comprehensive, Integrative Genomic Analysis of Diffuse Lower-Grade Gliomas. N Engl J Med (2015) 372(26):2481–98. doi: 10.1056/NEJMoa1402121
6. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol (2016) 131(6):803–20. doi: 10.1007/s00401-016-1545-1
7. van den Bent MJ, Brandes AA, Taphoorn MJB, Kros JM, Kouwenhoven MCM, Delattre J-Y, et al. Adjuvant Procarbazine, Lomustine, and Vincristine Chemotherapy in Newly Diagnosed Anaplastic Oligodendroglioma: Long-Term Follow-Up of EORTC Brain Tumor Group Study 26951. J Clin Oncol Off J Am Soc Clin Oncol (2013) 31(3):344–50. doi: 10.1200/JCO.2012.43.2229
8. Cairncross G, Wang M, Shaw E, Jenkins R, Brachman D, Buckner J, et al. Phase III Trial of Chemoradiotherapy for Anaplastic Oligodendroglioma: Long-Term Results of RTOG 9402. J Clin Oncol Off J Am Soc Clin Oncol (2013) 31(3):337–43. doi: 10.1200/JCO.2012.43.2674
9. Berger MS, Rostomily RC. Low Grade Gliomas: Functional Mapping Resection Strategies, Extent of Resection, and Outcome. J Neurooncol (1997) 34(1):85–101. doi: 10.1023/A:1005715405413
10. McGirt MJ, Chaichana KL, Attenello FJ, Weingart JD, Than K, Burger PC, et al. Extent of Surgical Resection is Independently Associated With Survival in Patients With Hemispheric Infiltrating Low-Grade Gliomas. Neurosurgery (2008) 63(4):700–8. doi: 10.1227/01.NEU.0000325729.41085.73
11. Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha S, et al. Role of Extent of Resection in the Long-Term Outcome of Low-Grade Hemispheric Gliomas. J Clin Oncol Off J Am Soc Clin Oncol (2008) 26(8):1338–45. doi: 10.1200/JCO.2007.13.9337
12. Stupp R, Brada M, van den Bent MJ, Tonn J-C, Pentheroudakis G. High-Grade Glioma: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol Off J Eur Soc Med Oncol (2014) 25 Suppl 3:iii93–101. doi: 10.1093/annonc/mdu050
13. Ryckman JM, Surkar SM, Haque W, Butler EB, Teh BS, Verma V. Sequencing of Chemotherapy and Radiotherapy for Newly Diagnosed Anaplastic Oligodendroglioma and Oligoastrocytoma. Am J Clin Oncol (2019) 42(3):258–64. doi: 10.1097/COC.0000000000000511
14. Byrne E, Abel S, Yu A, Shepard M, Karlovits SM, Wegner RE. Trends in Radiation Dose for Low Grade Gliomas Across the United States. J Neurooncol (2022) 157(1):197–205. doi: 10.1007/s11060-022-03962-4
15. Buckner JC, Shaw EG, Pugh SL, Chakravarti A, Gilbert MR, Barger GR, et al. Radiation Plus Procarbazine, CCNU, and Vincristine in Low-Grade Glioma. N Engl J Med (2016) 374(14):1344–55. doi: 10.1056/NEJMoa1500925
16. Bush NAO, Young JS, Zhang Y, Dalle Ore CL, Molinaro AM, Taylor J, et al. A Single Institution Retrospective Analysis on Survival Based on Treatment Paradigms for Patients With Anaplastic Oligodendroglioma. J Neurooncol (2021) 153(3):447–54. doi: 10.1007/s11060-021-03781-z
17. Lin Y, Xing Z, She D, Yang X, Zheng Y, Xiao Z, et al. IDH Mutant and 1p/19q Co-Deleted Oligodendrogliomas: Tumor Grade Stratification Using Diffusion-, Susceptibility-, and Perfusion-Weighted MRI. Neuroradiology (2017) 59(6):555–62. doi: 10.1007/s00234-017-1839-6
18. Yeboa DN, Yu JB, Liao E, Huse J, Penas-Prado M, Kann BH, et al. Differences in Patterns of Care and Outcomes Between Grade II and Grade III Molecularly Defined 1p19q Co-Deleted Gliomas. Clin Transl Radiat Oncol (2019) 15:46–52. doi: 10.1016/j.ctro.2018.12.003
19. Weller J, Katzendobler S, Karschnia P, Lietke S, Egensperger R, Thon N, et al. PCV Chemotherapy Alone for WHO Grade 2 Oligodendroglioma: Prolonged Disease Control With Low Risk of Malignant Progression. J Neurooncol (2021) 153(2):283–91. doi: 10.1007/s11060-021-03765-z
20. Kavouridis VK, Boaro A, Dorr J, Cho EY, Iorgulescu JB, Reardon DA, et al. Contemporary Assessment of Extent of Resection in Molecularly Defined Categories of Diffuse Low-Grade Glioma: A Volumetric Analysis. J Neurosurg (2020) 133(5):1291–301. doi: 10.3171/2019.6.JNS19972
21. Mesny E, Barritault M, Izquierdo C, Poncet D, d’Hombres A, Guyotat J, et al. Gyriform Infiltration as Imaging Biomarker for Molecular Glioblastomas. J Neurooncol (2022) 157(3):511–521. doi: 10.1007/s11060-022-03995-9
22. Luks TL, Villanueva-Meyer JE, Weyer-Jamora C, Gehring K, Jakary A, Hervey-Jumper SL, et al. T2 FLAIR Hyperintensity Volume Is Associated With Cognitive Function and Quality of Life in Clinically Stable Patients With Lower Grade Gliomas. Front Neurol (2021) 12:769345. doi: 10.3389/fneur.2021.769345
23. Visser O, Ardanaz E, Botta L, Sant M, Tavilla A, Minicozzi P. Survival of Adults With Primary Malignant Brain Tumours in Europe; Results of the EUROCARE-5 Study. Eur J Cancer (2015) 51(15):2231–41. doi: 10.1016/j.ejca.2015.07.032
24. Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro Oncol (2020) 22(12 Supplement_2):iv1–iv96. doi: 10.1093/neuonc/noaa200
25. Penas-Prado M, Wu J, Cahill DP, Brat DJ, Costello JF, Kluetz PG, et al. Proceedings of the Comprehensive Oncology Network Evaluating Rare CNS Tumors (NCI-CONNECT) Oligodendroglioma Workshop. Neuro-oncol Adv (2020) 2(1):vdz048. doi: 10.1093/noajnl/vdz048
26. Cairncross JG, Wang M, Jenkins RB, Shaw EG, Giannini C, Brachman DG, et al. Benefit From Procarbazine, Lomustine, and Vincristine in Oligodendroglial Tumors Is Associated With Mutation of IDH. J Clin Oncol Off J Am Soc Clin Oncol (2014) 32(8):783–90. doi: 10.1200/JCO.2013.49.3726
27. Jiao Y, Killela PJ, Reitman ZJ, Rasheed AB, Heaphy CM, de Wilde RF, et al. CIC, FUBP1 and IDH1 Mutations Refine the Classification of Malignant Gliomas. Oncotarget (2012) 3(7):709–22. doi: 10.18632/oncotarget.588
28. Bettegowda C, Agrawal N, Jiao Y, Sausen M, Wood LD, Hruban RH, et al. Mutations in CIC and FUBP1 Contribute to Human Oligodendroglioma. Science (2011) 333(6048):1453–5. doi: 10.1126/science.1210557
29. Bou Zerdan M, Assi HI. Oligodendroglioma: A Review of Management and Pathways. Front Mol Neurosci (2021) 14:722396. doi: 10.3389/fnmol.2021.722396
30. Almeida JP, Chaichana KL, Rincon-Torroella J, Quinones-Hinojosa A. The Value of Extent of Resection of Glioblastomas: Clinical Evidence and Current Approach. Curr Neurol Neurosci Rep (2015) 15(2):517. doi: 10.1007/s11910-014-0517-x
31. Garton ALA, Kinslow CJ, Rae AI, Mehta A, Pannullo SC, Magge RS, et al. Extent of Resection, Molecular Signature, and Survival in 1p19q-Codeleted Gliomas. J Neurosurg (2020) 134(5):1357–67. doi: 10.3171/2020.2.JNS192767
32. Snyder LA, Wolf AB, Oppenlander ME, Bina R, Wilson JR, Ashby L, et al. The Impact of Extent of Resection on Malignant Transformation of Pure Oligodendrogliomas. J Neurosurg (2014) 120(2):309–14. doi: 10.3171/2013.10.JNS13368
33. Thon N, Kreth F-W, Tonn J-C. The Role of Surgery in Grade II/III Oligodendroglial Tumors. CNS Oncol (2015) 4(5):317–23. doi: 10.2217/cns.15.26
34. Kinslow CJ, Garton ALA, Rae AI, Marcus LP, Adams CM, McKhann GM, et al. Extent of Resection and Survival for Oligodendroglioma: A U.S. Population-based Study J Neurooncol (2019) 144(3):591–601. doi: 10.1007/s11060-019-03261-5
35. Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat Rev Clin Oncol (2021) 18(3):170–86. doi: 10.1038/s41571-020-00447-z
36. Mohile NA, Messersmith H, Gatson NT, Hottinger AF, Lassman A, Morton J, et al. Therapy for Diffuse Astrocytic and Oligodendroglial Tumors in Adults: ASCO-SNO Guideline. J Clin Oncol (2022) 40(4):403–26. doi: 10.1200/JCO.21.02036
37. Holdhoff M, Cairncross GJ, Kollmeyer TM, Zhang M, Zhang P, Mehta MP, et al. Genetic Landscape of Extreme Responders With Anaplastic Oligodendroglioma. Oncotarget (2017) 8(22):35523–31. doi: 10.18632/oncotarget.16773
38. van den Bent MJ, Carpentier AF, Brandes AA, Sanson M, Taphoorn MJB, Bernsen HJJA, et al. Adjuvant Procarbazine, Lomustine, and Vincristine Improves Progression-Free Survival But Not Overall Survival in Newly Diagnosed Anaplastic Oligodendrogliomas and Oligoastrocytomas: A Randomized European Organisation for Research and Treatment of Cancer. J Clin Oncol Off J Am Soc Clin Oncol (2006) 24(18):2715–22. doi: 10.1200/JCO.2005.04.6078
39. Gwak H-S, Yee GT, Park C-K, Kim JW, Hong Y-K, Kang S-G, et al. Temozolomide Salvage Chemotherapy for Recurrent Anaplastic Oligodendroglioma and Oligo-Astrocytoma. J Korean Neurosurg Soc (2013) 54(6):489–95. doi: 10.3340/jkns.2013.54.6.489
40. Taliansky-Aronov A, Bokstein F, Lavon I, Siegal T. Temozolomide Treatment for Newly Diagnosed Anaplastic Oligodendrogliomas: A Clinical Efficacy Trial. J Neurooncol (2006) 79(2):153–7. doi: 10.1007/s11060-005-9020-1
41. Lassman AB, Iwamoto FM, Cloughesy TF, Aldape KD, Rivera AL, Eichler AF, et al. International Retrospective Study of Over 1000 Adults With Anaplastic Oligodendroglial Tumors. Neuro Oncol (2011) 13(6):649–59. doi: 10.1093/neuonc/nor040
42. Nguyen SA, Stechishin ODM, Luchman HA, Lun XQ, Senger DL, Robbins SM, et al. Novel MSH6 Mutations in Treatment-Naïve Glioblastoma and Anaplastic Oligodendroglioma Contribute to Temozolomide Resistance Independently of MGMT Promoter Methylation. Clin Cancer Res Off J Am Assoc Cancer Res (2014) 20(18):4894–903. doi: 10.1158/1078-0432.CCR-13-1856
43. Ahluwalia MS, Xie H, Dahiya S, Hashemi-Sadraei N, Schiff D, Fisher PG, et al. Efficacy and Patient-Reported Outcomes With Dose-Intense Temozolomide in Patients With Newly Diagnosed Pure and Mixed Anaplastic Oligodendroglioma: A Phase II Multicenter Study. J Neurooncol (2015) 122(1):111–9. doi: 10.1007/s11060-014-1684-y
44. Jaeckle KA, Ballman KV, van den Bent M, Giannini C, Galanis E, Brown PD, et al. CODEL: Phase III Study of RT, RT + TMZ, or TMZ for Newly Diagnosed 1p/19q Codeleted Oligodendroglioma. Analysis from the initial study design Neuro Oncol (2021) 23(3):457–67. doi: 10.1093/neuonc/noaa168
45. NIH US National Library of Medicine. Radiation Therapy With or Without Temozolomide in Treating Patients With Low-Grade Glioma (NCT00978458) . Available at: https://clinicaltrials.gov/ct2/show/NCT00978458. Accessed May 2, 2022.
46. NIH US National Library of Medicine. Radiation Therapy With Concomitant and Adjuvant Temozolomide Versus Radiation Therapy With Adjuvant PCV Chemotherapy in Patients With Anaplastic Glioma or Low Grade Glioma (NCT00887146) . Available at: https://clinicaltrials.gov/ct2/show/NCT00887146. Accessed May 2, 2022.
47. NIH US National Library of Medicine. A Randomized Trial of Delayed Radiotherapy in Patients With Newly Diagnosed 1p/19q Codeleted Anaplastic Oligodendroglial Tumors: The POLCA Trial (NCT02444000). Available at: https://clinicaltrials.gov/ct2/show/NCT02444000. Accessed May 2, 2022.
48. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology - Central Nervous System Cancers (Version 2.2021). Available at: http://www.nccn.org/professionals/physician_gls/pdf/CNS_cancers.pdf. Accessed May 2, 2022.
49. Mellinghoff IK, Van Den Bent MJ, Clarke JL, Maher EA, Peters KB, Touat M, et al. INDIGO: A Global, Randomized, Double-Blind, Phase III Study of Vorasidenib (VOR; AG-881) vs Placebo in Patients (Pts) With Residual or Recurrent Grade II Glioma With an Isocitrate Dehydrogenase 1/2 (IDH1/2) Mutation. J Clin Oncol (2020) 38(15\_suppl):TPS2574–TPS2574. doi: 10.1200/JCO.2020.38.15_suppl.TPS2574
50. NIH US National Library of Medicine. Abemaciclib in Patients With Oligodendroglioma (NCT03969706). Available at: https://clinicaltrials.gov/ct2/show/NCT03969706. Accessed May 2, 2022.
Keywords: oligodendroglioma, diffuse glioma, 1p19q codeletion, EORTC, RTOG, POLCA, CODEL, NCCN
Citation: Rincon-Torroella J, Rakovec M, Materi J, Raj D, Vivas-Buitrago T, Ferres A, Reyes Serpa W, Redmond KJ, Holdhoff M, Bettegowda C and González Sánchez JJ (2022) Current and Future Frontiers of Molecularly Defined Oligodendrogliomas. Front. Oncol. 12:934426. doi: 10.3389/fonc.2022.934426
Received: 02 May 2022; Accepted: 13 June 2022;
Published: 25 July 2022.
Edited by:
Luca Ricciardi, Sapienza University of Rome, ItalyReviewed by:
Nicola Montemurro, Azienda Ospedaliera Universitaria Pisana, ItalyCopyright © 2022 Rincon-Torroella, Rakovec, Materi, Raj, Vivas-Buitrago, Ferres, Reyes Serpa, Redmond, Holdhoff, Bettegowda and González Sánchez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chetan Bettegowda, Y2JldHRlZzFAamhtaS5lZHU=; José Juan González Sánchez, ampnb256YWxAY2xpbmljLmNhdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.