 Xinyi Zheng
Xinyi Zheng Hang Wang
Hang Wang Junyue Deng2
Junyue Deng2 Minghe Yao
Minghe Yao Xuelei Ma
Xuelei Ma
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 26 January 2023
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.907377
This article is part of the Research Topic Reviews in Genitourinary Oncology View all 19 articles
Objective: This review aimed to comprehensively analyze the safety and efficacy of erdafitinib in treating advanced and metastatic urothelial carcinoma and other solid tumors.
Methods: PubMed, Embase, and ClinicalTrials.gov were searched until 10 February 2022. The safety outcome as adverse events and efficacy outcomes, including objective response rate, stable disease rates, and progressive disease rates, were selected and analyzed by comprehensive meta-analysis version 3.0 and STATA 15.0.
Results: The most common all-grade adverse events were hyperphosphatemia, dry mouth, stomatitis, diarrhea, and dysgeusia. The occurrence of ≥3 adverse events was relatively low, and stomatitis and hyponatremia were the most common. Moreover, eye disorders could not be ignored. Efficacy in urothelial carcinoma patients was obviously better than in other solid tumor patients, with a higher objective response rate (0.38 versus 0.10) and lower progressive disease rate (0.26 versus 0.68). All responses occurred in patients with fibroblast growth factor receptor (FGFR) alteration. In those patients, a specific FGFR alteration (FGFR3-TACC3) was observed to have a maximum response.
Conclusion: Erdafitinib has satisfactory clinical activity for metastatic urothelial carcinoma and other solid tumors, while the toxicity is acceptable. With more RCTs and combination therapy trials published, erdafitinib will be applied widely.
Urothelial carcinoma (UC) refers to a transitional urothelial tumor of the urinary tract. It can be divided into upper and lower urothelial carcinoma according to the diseased region. Bladder cancer is the most common type of lower urothelial carcinoma, accounting for 90% of the total. Other types of urothelial carcinoma, such as renal pelvis and urethral carcinoma, are scarce. Generally, UC is the 10th most commonly diagnosed cancer worldwide, with approximately 573,000 new cases and 213,000 deaths in 2020 (1, 2). It has a predominance of male patients, with respective incidence and mortality rates of 9.5 and 3.3 per 100,000 among men, which are approximately four times those among women globally. For non-muscle-invasive bladder cancer, the present treatment is transurethral resection of bladder tumor (TURBT), intravesical chemotherapy, and intravesical BCG immunotherapy (3, 4). For unresectable or metastatic bladder tumor, platinum-based combination chemotherapies are the major therapy (5, 6). However, the efficacy of platinum-based drugs is not satisfactory, with a median survival of only 7.4 months. Since 2019, the application of FGFR inhibitors has innovated treatment options for advanced and metastatic UC, increasing the median survival by 3 months (7).
Erdafitinib is an ATP-competitive inhibitor of FGFR1–4. It is a small molecule inhibitor (SMi) that reversibly inhibits FGFR kinase autophosphorylation and decreases resultant downstream signaling (8). Under physiological conditions, fibroblast growth factor receptor 1–4 (FGFR1–4) bind to fibroblast growth factors (FGFs) to exert tyrosine kinase regulatory effects (9), which play a vital role in angiogenesis and damage repair. The FGFR molecule includes three extracellular immunoglobulin domains, one transmembrane domain, and one intracellular domain. The intracellular domain can activate the RAS-MAPK-ERK and PI3K-AKT pathways (10–14). However, gene amplification, mutation, rearrangement, or translocations occur and alter the signaling pathway, which leads to cell proliferation or migration (15–19).
The mechanism of erdafitinib inhibits these pathways from upstream, which can impede the growth of tumors. In a study, BLC2001(NCT02365597), those patients who had not responded to PD-1 treatment achieved an objective response with erdafitinib treatment. In other clinical trials (NCT01703481 and NCT01962532), erdafitinib resulted in prolonged progression-free survival and median duration of response. Therefore, the FDA granted approval to erdafitinib for metastatic urothelial carcinoma in patients with susceptible alterations in FGFR2 or FGFR3 who have progressed platinum-containing chemotherapy, including within neoadjuvant or adjuvant platinum-containing chemotherapy. It was also the first FGFR kinase inhibitor approved by FDA for urothelial carcinoma. However, erdafitinib causes adverse effects, such as increased serum phosphate, stomatitis, and central serous chorioretinopathy. These adverse events (AEs) may reduce medication compliance, which leads to reduced efficacy.
To our knowledge, there have not been any meta-analyses about the safety and efficacy of erdafitinib. To offer evidence-based references for physicians, we conducted this study to determine the most meaningful AEs and efficacy outcomes of erdafitinib.
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines were followed to complete this meta-analysis. PubMed, Embase, ClinicalTrials.gov, Cochrane Library, and China National Knowledge Infrastructure (CNKI) were searched for clinical trials and related articles until 10 February 2022. In addition, the references of reviews or trials related to erdafitinib were screened to avoid the omission of valuable articles. There was no restriction to language. The following words were used for searching: “erdafitinib” or “JNJ-42756493” or “Balversa.”
Two reviewers independently selected the search results according to PRISMA flow diagrams. Discrepancies were resolved by the third author. The inclusion criteria were as follows: (1) patients were confirmed to have carcinoma by pathology; (2) the gene alteration of patients was included in fusion, mutation, and amplification; (3) the interventions of studies included erdafitinib singly or combined with other drugs; and (4) relevant data of efficacy and safety were reported. Unrelated articles, case reports, retrospective studies, reviews, and studies that lacked necessary data or full text were excluded.
Data from the included articles were extracted independently by two reviewers while discussing disagreements with the third reviewers. Basic information, such as the first author’s name, publication year, clinical trial sequence number, study phase, study design, sample size, median age, median follow-up, carcinoma histology, and treatment regimens, was extracted. The efficacy indicators included the complete response rate (CRR), partial response rate (PRR), objective response rate (ORR, which referred to the presence of at least a confirmed complete response or confirmed partial response), stable disease (SD) rate, progressive disease rate (defined as >20% increase in the longest diameters of target lesions or the appearance of a new lesion), hazard ratio (HR), and risk ratio (RR). The data used for safety analyses were collected from all-grade and grade ≥3 AEs.
STATA was used to count the standard error of CR, PR, and ORR. We conducted a single-rate meta-analysis to draw a forest plot. Meanwhile, the odds ratio was calculated to compare erdafitinib with other treatments. Comprehensive Meta-Analysis (CMA) Version 3.0 was used to analyze all-grade and grade ≥3 AEs to calculate the event rate and 95% CI. STATA and CMA were used to analyze heterogeneity. I2 > 50% and p < 0.05 were considered as high heterogeneity. A fixed-effects model was used for I2 <50%; random-effects model analysis was used for I2 > 50%.
If we included 10 more studies, STATA 15.0 was used to analyze the heterogeneity of the included literature. If there was high heterogeneity, the METAREG command was used for meta-regression analysis. We discussed the sources of heterogeneity. At the same time, if 10 more articles were included, Begg’s and Egger’s funnel plots were conducted to investigate publication bias.
The risk of bias of randomized controlled trials was obtained by RevMan 5.4 (The Cochrane Collaboration). The articles were evaluated in the following processes: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and others. For the nonrandomized studies, the bias was assessed by the risk of bias in nonrandomized studies of interventions (ROBINS-I) tool (20, 21). ROBINS-I included seven domains: allocation bias, selection bias, observer bias, performance bias, attrition bias, detection bias, and analysis reporting bias. Meanwhile, ROBINS-I was used to assess the quality of non-randomized studies.
A total of 968 articles were produced through the search strategy. Five articles were searched through the references of previous reviews. After removing duplications, 557 were screened based on the title and abstract, and 546 unrelated articles were excluded. Eleven studies were selected, but five articles lacked the necessary data. Finally, six trials were included. The study selection procedure is shown in Figure 1.
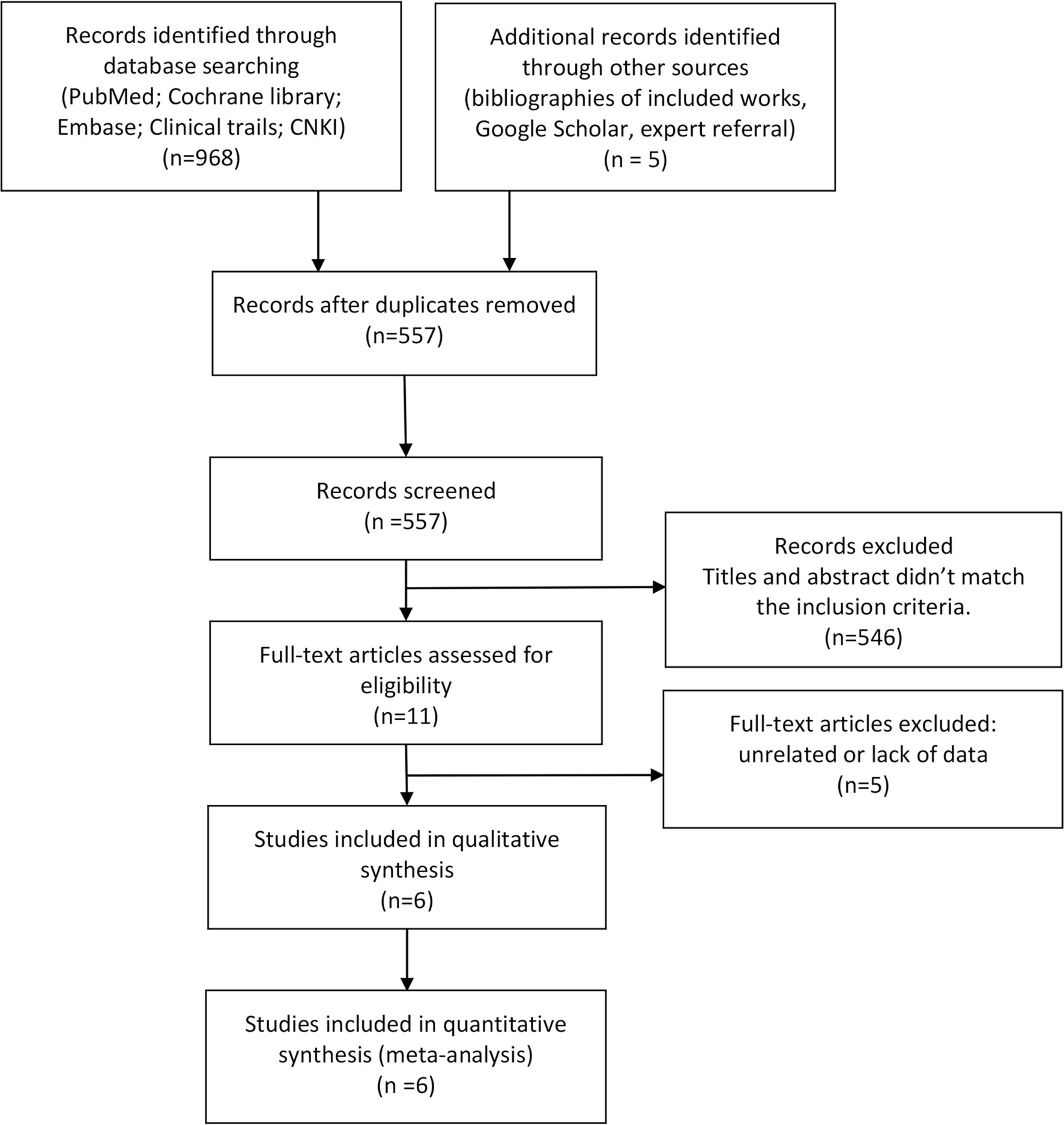
Figure 1 Flow diagram of literature selection for systemic reviews and meta-analyses (PRISMA).
The included studies were published from 2015 to 2022. There were three phase I and three phase II clinical trials, and all were nonrandomized. In phase I trials, patients with various kinds of solid tumors were included, in which some patients with UC were not being classified between other solid tumors. Meanwhile, every patient in phase II was suffering from urothelial carcinoma. Most of the included trials described FGFR alterations in patients except NCT01703481 (Tabernero,2015) and NCT01962532 (Nishina,2017). Mutations and fusions were the major gene alterations of FGFR. In NCT02365597 (Loriot,2019), the proportion of FGFR3 mutations was 74/99, while that of FGFR3 fusions was 25/99. In Bahleda’s research, the scale of FGFR mutations or fusions [mutation (+)/fusion (−) OR mutation (−)/fusion (+)] was 58/187, that of the amplifications was 45/187, and the ratio of co-alteration [mutation (+)/fusion (+)] was 5/187. In addition, all 12 patients in Monterio’s trial were found to have FGFR3 alterations. In NCT02365597 (Siefker-Radtke,2022), 70/101 were FGFR mutation (+)/fusion (−), 25/101 were mutation (−)/fusion (+), 6/101 were FGFR mutation (+)/fusion (+), and 5/101 were FGFR mutation/fusion co-alterations.
Erdafitinib was singly used for all six articles with constant, escalation, or intermittent doses. Most of the persistent doses ranged from 6 to 9 mg, while the intermittent dose was 10 or 12 mg. Notably, we found that in the latest trials, a constant dose of 8–9 mg was used more frequently, which might be related to the recommendation by the FDA. All the included articles used RECIST 1.1 (Response Evaluation Criteria in Solid Tumors) to assess the efficacy, while CTCAE 4.0–5.0 (Common Terminology Criteria for Adverse Events) was used for safety assessment. More basic information is displayed in Table 1.
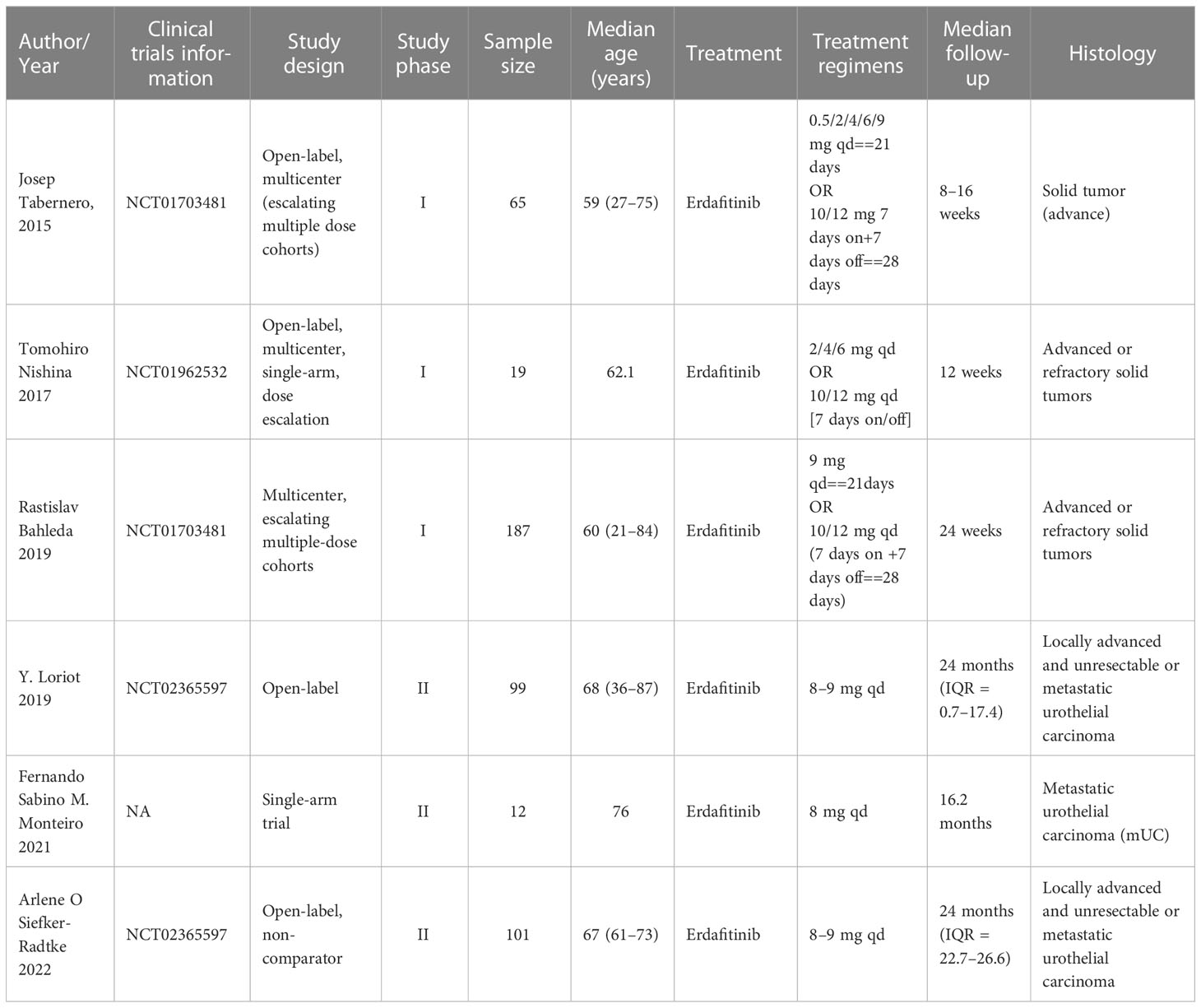
Table 1 Basic characteristics of the included trials.
The rates of all-grade and grade ≥3 AEs were pooled from single-arm studies. The all-grade AEs are shown in Table 2 and Supplementary Material 1. Among them, the top five most frequent AEs were dry mouth (42.4%, 95% CI 38.0%–46.9%), dysgeusia (30.8%, 95% CI 26.3%–35.7%), dry skin (30.6%, 95% CI 26.5%–34.9%), abnormal hepatic function (21.5%, 95% CI 13.2%–33.2%), and nausea (20.5%, 95% CI 17.1%–24.5%) in the fixed-effects model. In the random-effects model, hyperphosphatemia ranked first in incidence (68.2%, 95% CI 59.4%–75.8%), followed by stomatitis (37.4%, 95% CI 27.0%–49.0%), diarrhea (30.9%, 95% CI 18.8%–46.4%), decreased appetite (30.6%, 95% CI 22.3%–40.4%), and asthenia (27.7%, 95% CI 15.4%–44.7%). Eye disorders that might be caused by central serous chorioretinopathy cannot be ignored.
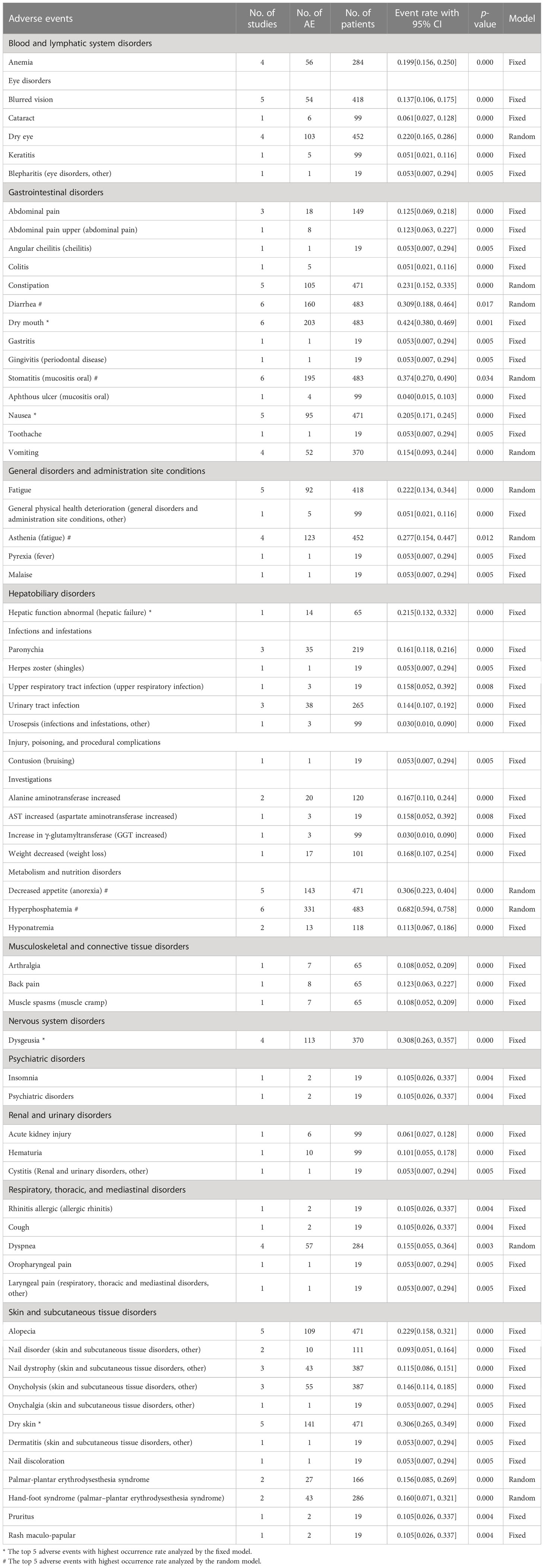
Table 2 The all-grade adverse events classified by CACTE 5.0 and the details.
When fixed-effects models were applied to grade ≥ 3 AEs analysis, hyponatremia was found to be the most common AE (8.3%, 95% CI 5.6%–12.2%), while abnormal hepatic function (7.7%, 95% CI 3.2%–17.2%), anemia (7.0%, 95% CI 4.9%–9.8%), asthenia (6.6%, 95% CI 4.5%–9.5%), and nail dystrophy (6.0%, 95% CI 3.4%–10.3%) were other major AEs. Regarding random-effects models, stomatitis (9.7%, 95% CI 6.1%–15.1%) and general physical health deterioration (7.0%, 95% CI 2.8%–16.5%) commonly occurred in grade ≥3 AEs, and these consequences are listed in Table 3 and Supplementary Material 2.
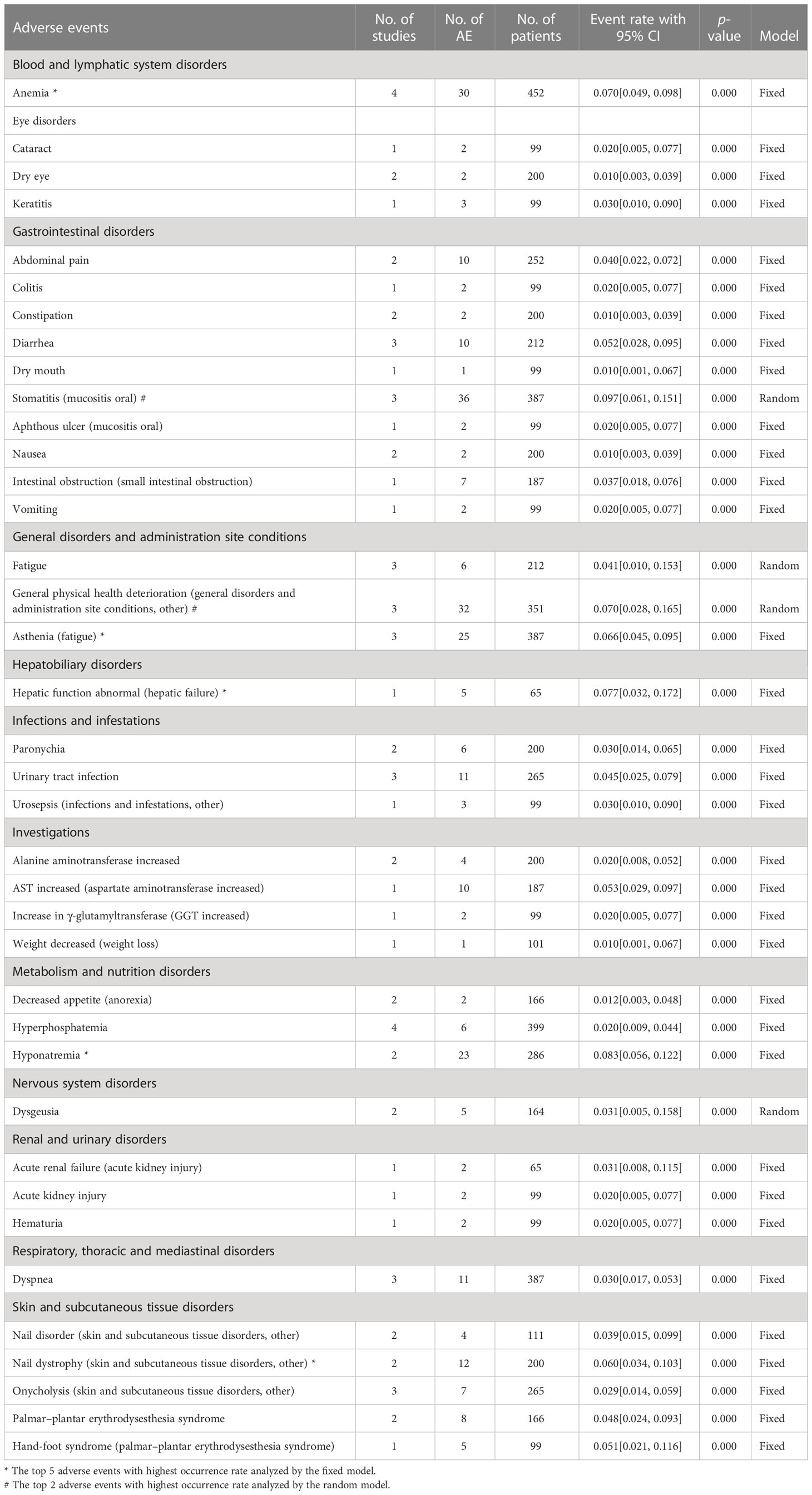
Table 3 The grade ≥3 adverse events classified by CAC Table 5.0 and the details.
For the ORR, stable disease rate, and progressive disease rate, STATA 15.0 was used to conduct a single-rate analysis. For solid tumors and urothelial carcinoma, we calculated their response rates separately, as shown in Figures 2–4. In the study of urothelial carcinoma, a random-effects model was used to analyze stable disease and progressive disease rates, which were 0.36 (0.26–0.46) and 0.26 (0.04–0.48), respectively. For urothelial carcinoma, the ORR was 0.38 (0.31–0.44) for the fixed model. Similarly, the ORR of solid tumors was 0.10 (0.07–0.14), while the overall stable disease and progressive disease rates of solid tumors were 0.16 (0.06–0.26) and 0.68 (0.41–0.95), respectively. Other details are shown in Table 4.
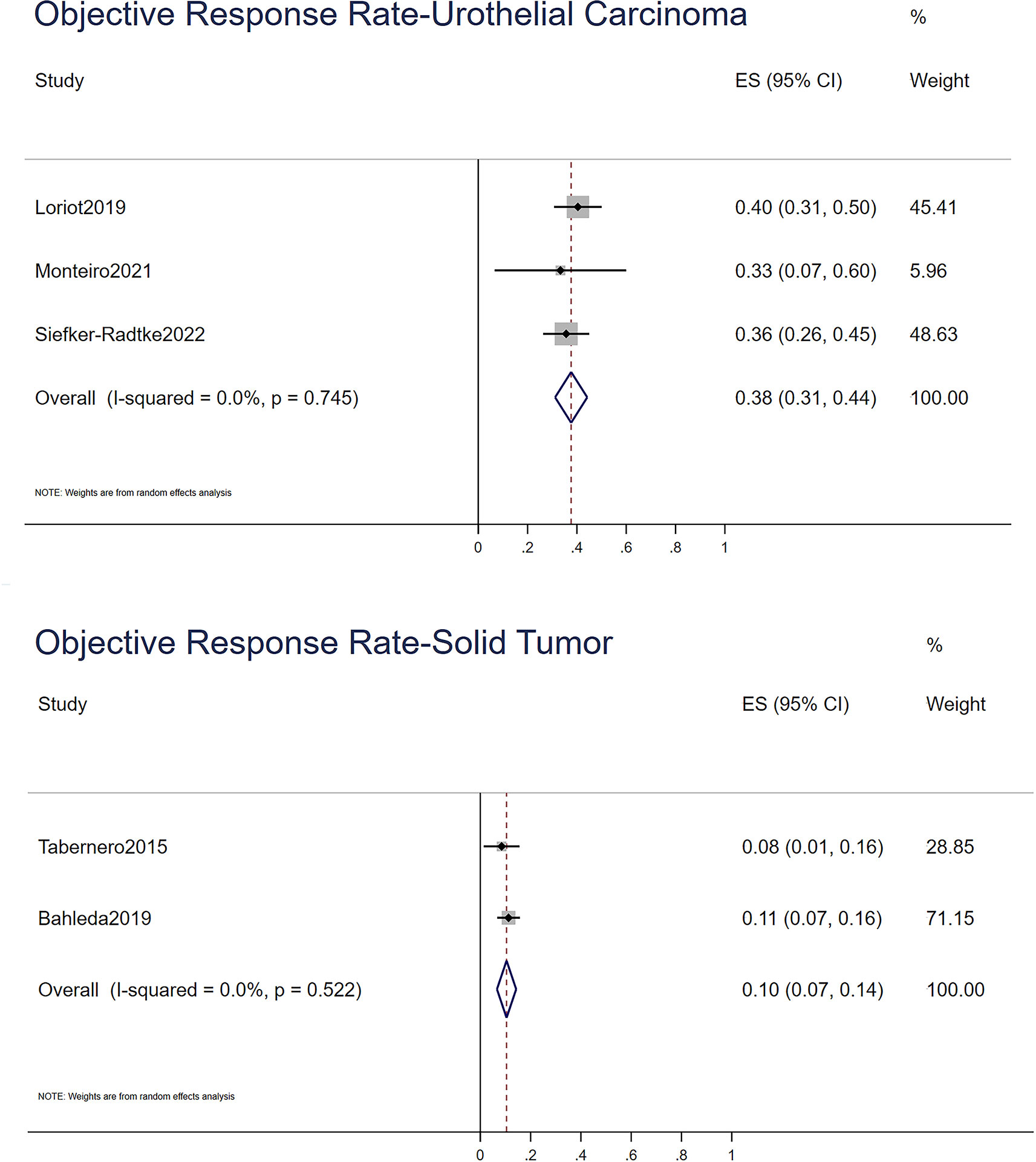
Figure 2 The objective response rate of urothelial carcinoma and solid tumor.
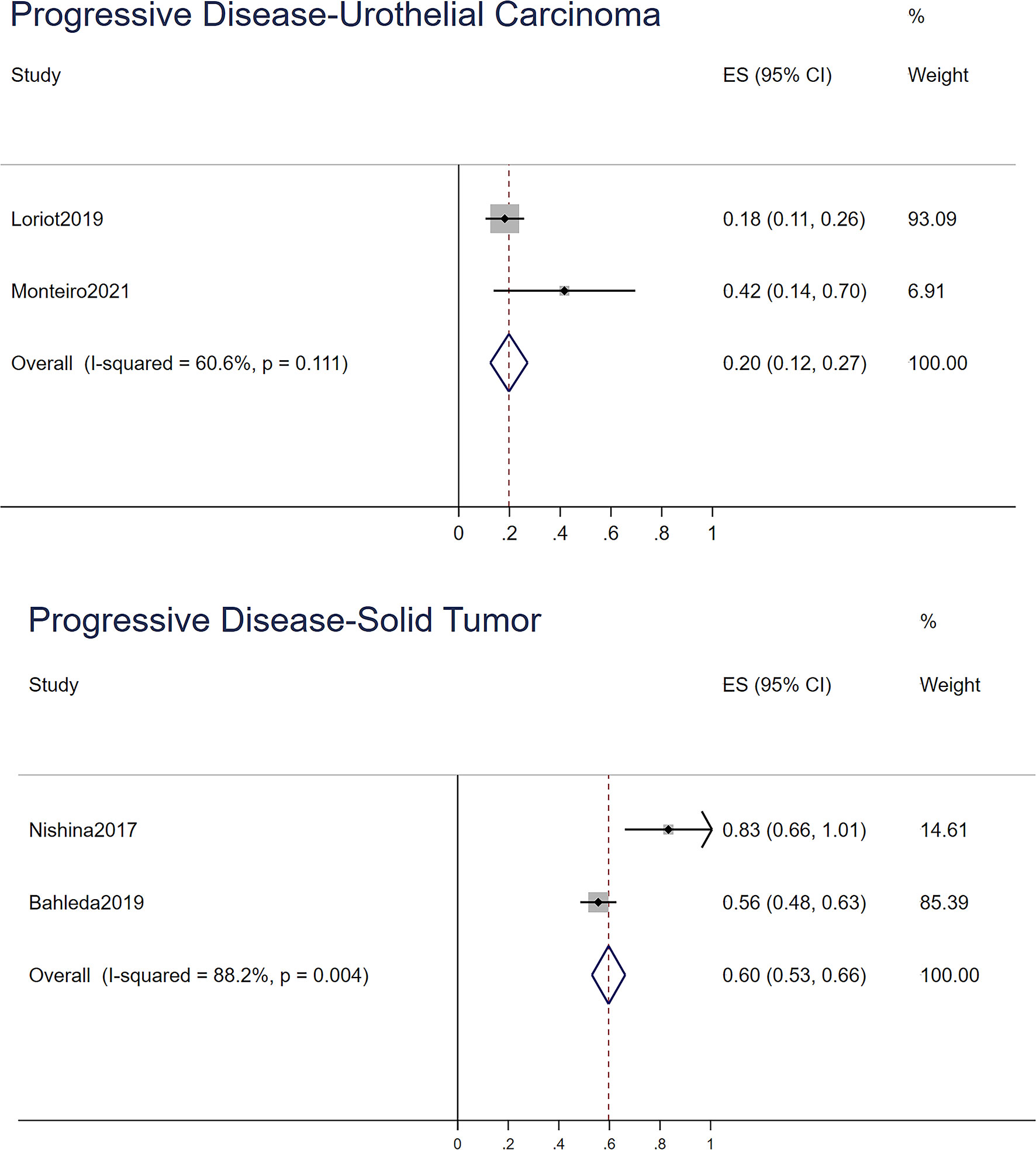
Figure 3 The progressive disease of urothelial carcinoma and solid tumor.
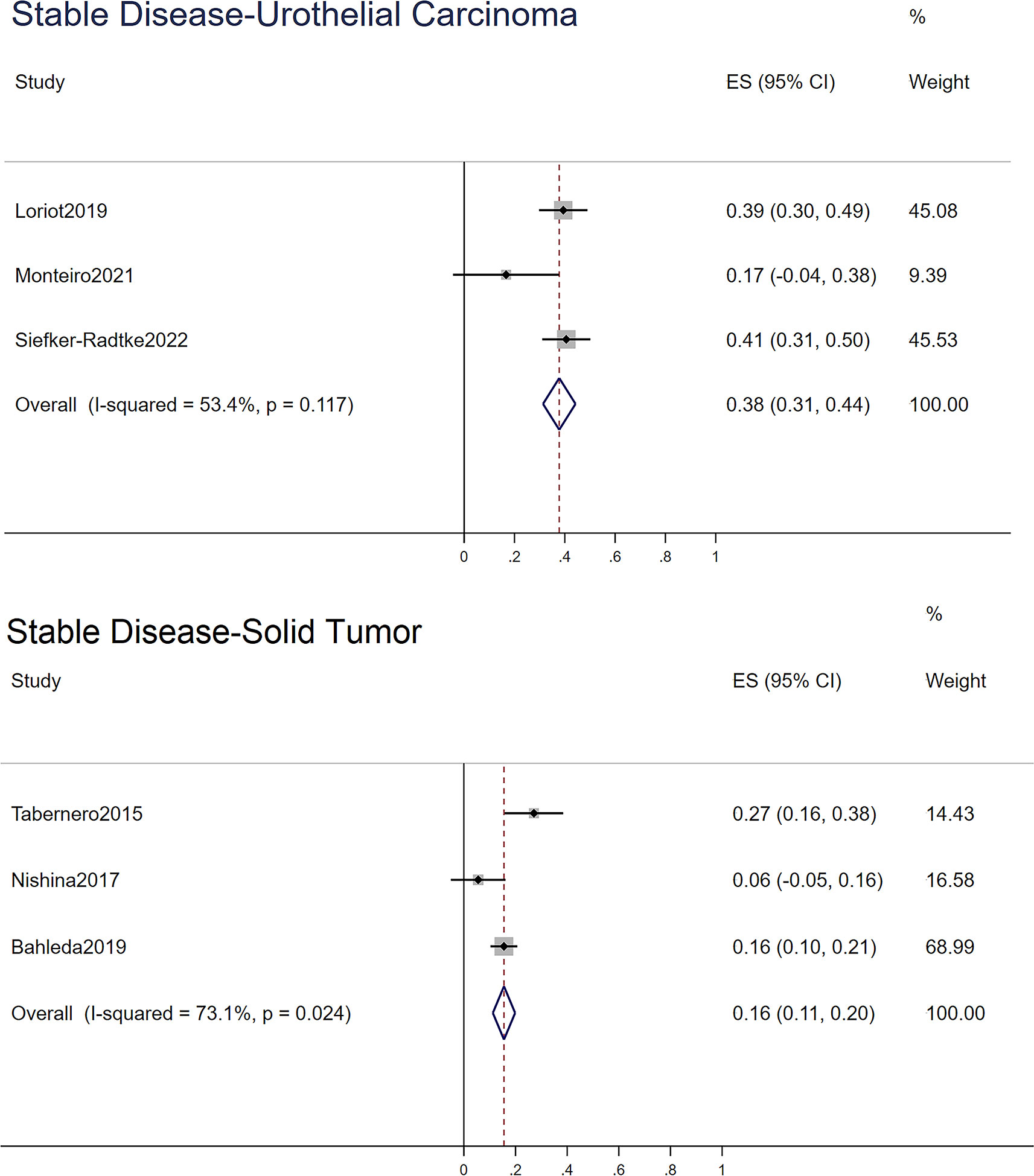
Figure 4 The stable disease of urothelial carcinoma and solid tumor.
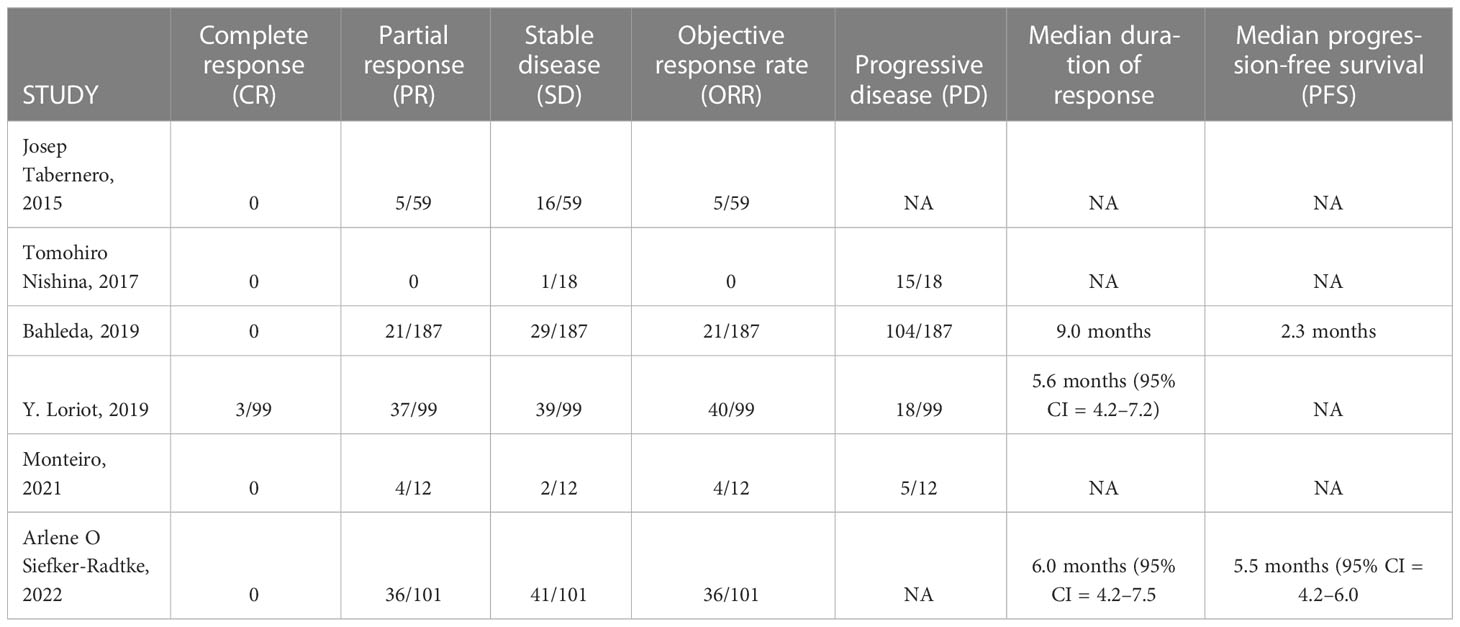
Table 4 Efficacy profile of erdafitinib.
Only three trials provided data on the median duration of response and median progression-free survival (PFS). The most prolonged duration occurred in studies published in 2022, which had a median duration of response of 6.0 months, while the median PFS was 5.5 months. A continuous dose of 8 mg or 8 to 9 mg was used for treatment.
In Siefker-Radtke’s trial, the median PFS of FGFR mutation was longer than that of FGFR fusion. For the patients who presented both FGFR mutation and fusion, the median PFS was 6.9 months, while mutation (−)/fusion (+) was 2.8 months, and mutation (+)/fusion (−) was 5.6 months.
RevMan 5.4 was used to assess the risk of bias. However, they were all single-arm studies. In Loriot’s study, except for performance bias, which was assessed as high risk because of open label, the other aspects were assessed as low risk. Five nonrandomized studies were evaluated as low to moderate risk in the ROBINS-I assessment. Overall, the quality of the studies was satisfactory. Because there were fewer than 10 included articles, the meta-regression and funnel plot were not made.
Based on the present findings, we conducted a meta-analysis to summarize six published clinical trials (22–27), comprehensively investigating the safety and efficacy of erdafitinib. Our review analyzed the ORR, stable disease rate, and progressive disease rate of UC and other solid tumors separately. As mentioned in the Characteristics of studies section, some articles reported the outcomes regardless of UC and other solid tumors. Thus, we calculated the efficacy of UC and solid tumors separately by the trials that were specific to UC and the rest. Finally, we indicated that erdafitinib had a more satisfactory effect in UC than in solid tumors, with a higher ORR and lower progression rate.
Based on the development of next-generation DNA sequencing, it is now easy to determine the genetic alteration type of tumors. The effect of erdafitinib is surprising in some specific categories of FGFR gene alteration like FGFR3-TACC3. In Loriot’s trial, 4 of 11 patients responded to erdafitinib. All four patients had FGFR3:TACC3v1 gene alteration (a specific kind of gene fusion). In Tabernero’s article, patients with FGFR3-TACC3 tended to have greater response or tumor shrinkage than patients with other gene alterations. This phenomenon can be explained by a fusion of FGFR3 and TACC3, which contributed to constitutive tyrosine kinase activation and disruption of mitotic activity (28). Nevertheless, in addition to mutation and fusion, amplification may also occur. The trial (25) indicated that patients with FGFR mutations/fusion/co-alterations had significantly higher ORRs (12/27) than those with FGFR amplification (only 2/23 patients responded). Previous reviews have also found that for FGFR inhibitors, qualitative FGFR1–3 alterations such as mutation and rearrangement are more sensitive to drugs, and quantitative alterations like gene amplification rarely exhibit clinical activity (29). This might be because amplification leads to oncogene redundancy, which can lead to the overexpression of related proteins and initiate downstream signaling that promotes carcinoma proliferation and survival. Some studies have demonstrated that redundant oncogenes were associated with immune escape, which reduced or nullified the effect of FGFR SMi (30, 31).
In the study of AEs, we indicated that the most common all-grade AEs were hyperphosphatemia, stomatitis, dry mouth, dysgeusia, and diarrhea. Hyperphosphatemia occurred in more than half of the patients; however, all of them were grade 1–2. The most common grade ≥3 AEs were stomatitis, hyponatremia, and abnormal hepatic function. Generally, severe AEs were relatively rare.
For gastrointestinal AEs such as diarrhea, stomatitis, dry mouth, decreased appetite, nausea, vomiting, and abdominal pain, most can be controlled with symptomatic treatments (32). There have been no trials that reported drug withdrawal because of gastrointestinal AEs.
In the remaining AEs, hyperphosphatemia needed to be noted for its high occurrence and the possibility of causing reduction or withdrawal of erdafitinib. Hyperphosphatemia is the most common all-grade AE, occurring at 68.2%, related to fibroblast growth factor 23 (FGF-23) in bone metabolism (33, 34). FGF23 is a bone-derived mediator that maintains phosphate homeostasis, which inhibits the synthesis of 1,25-dihydroxyvitamin D3. Meanwhile, FGF-23 interacts with Klotho (which is the main structure of FGF receptor complex) to suppress renal phosphate reabsorption by decreasing the expression of the sodium-phosphate cotransporters NPT2A and NPT2C in the brush-border membrane of proximal tubule epithelial cells (35–37). FGFR1 co-expresses with Klotho, which increases the affinity of FGF23 for FGFR1 (38). A previous study suggested that Klotho was regulated by phosphaturia and that FGFR1 expression was modulated by FGF23. In a trial with a pan-FGFR inhibitor (PD173074), researchers found that the biologic activity of FGF-23 was counteracted, leading to hyperphosphatemia and high 1,25(OH)2 D3 (39). Therefore, the decrease in FGF-23 contributed to hyperphosphatemia and increased the production of calcitriol. In two phase I trials (NCT0103481 and NCT01962532), hyperphosphatemia appeared with 4 mg of erdafitinib. However, they both noted no dose-related changes in FGF23 values and vitamin D. Since no raw data on FGF23 content were provided, we did not perform a comprehensive analysis of FGF23. We suspected that the inconspicuous changes in FGF23 may be due to the following reasons. First, the sample size was small (the total number of patients was 82), and second, in NCT0103481, some patients reduced the dose of medication while others were given intermittent administration (27). These therapies may alleviate the inhibition of FGF23 by FGFR inhibitors. Therefore, FGFR23 did not show significant changes (40). Thus, the mechanism of erdafitinib-induced hyperphosphatemia needs further study. In patients with hyperphosphatemia, phosphate binders like sevelamer, acetazolamide, and sevelamer carbonate can be taken (25). Satisfactorily, the use of sevelamer has no significant effect on the pharmacokinetic parameters of erdafitinib.
In addition to hyperphosphatemia, central serous chorioretinopathy (CSC) was another AE mentioned in FDA NEWS RELEASE: FDA approves first targeted therapy for metastatic bladder cancer. In BLC2001, CSC occurred in 27 of 101 patients. A case report noticed that patients’ visual acuity changed from 20/25 OD and 20/15 OD to 20/20 OU after using erdafitinib (41). Meanwhile, in Tabernero’s study, one patient reported visual spots. As Jung et al. mentioned, this symptom might be caused by drug-induced pseudo-central serous chorioretinopathy (pCSC). However, it is worth noting though that primary CSC and paraneoplastic retinopathy (PNR, a retinopathy that occurs in patients with carcinomas) have the same symptoms (42). Therefore, a differential diagnosis is necessary for targeted treatment and appropriate prognosis prediction. For pCSC, retinopathy is often self-limited. The symptom disappears simultaneously or shortly after discontinuation of therapy, which is the most significant feature. The main difference of pathology between true CSC and PNR is that the former has typical features for lipofuscin irregularities, and the latter has progressive lesion (42). The included trials in this review showed that the dose of erdafitinib had no noticeable difference in the occurrence rate of retinopathy disease, with rates of 15/60 (25%) in the 8-mg QD group and 12/41 (29%) in the 9-mg QD group. After dose interruption, reduction, or shutoff, 17 of 27 patients were solved. After resolving detachment of retinal pigment epithelium (RPE), a grade 3 retinopathy patient recurred as grade 2. A similar phenomenon also occurred in Bahelda’s article, which indicated that after dose interruption, the pathological changes of the retina reversed except for the patients who had grade 1–2 retinopathy. However, grade 1–2 retinopathy events have not been solved in some patients. We have no accurate conclusions about why mild retinal damage still exists.
We suspected that this is related to other pathways downstream of FGFR, like MAPK. Some studies have indicated that MEK inhibitors have a toxic effect on RPE (43, 44), which leads to retinal-related AEs. Other studies have formulated some hypotheses. For instance, the Wnt/β-catenin signaling pathway can promote the proliferation of RPE and the accumulation of extracellular matrix. If the signaling pathway is impacted, RPE will become pathological (45). The pathological contraction and traction of the fibrocellular membranes cause retinal detachment (46). Another hypothesis states that FGFR-1 and FGFR-2 increase L-type Ca2+ channel activity in retinal pigment epithelial cells, and consequently promote the secretion of vascular endothelial growth factor A (VEGF-A), which plays a critical role in neovascularization. Decreasing visual acuity might cause that (47).
Nevertheless, this hypothesis for mild retinal damage requires further evidentiary support. Because pCSCs are self-limited, we do not suggest physicians use additional drugs other than closely observing and reducing the dose accordingly.
Presently, erdafitinib is being used with other drugs for clinical treatments, for example, combined with the PD-1 inhibitor cetrelimab (NCT03473743). More RCTs comparing erdafitinib to intravesical chemotherapy in non-muscle-invasive bladder cancer are ongoing. The unsatisfactory effect caused by FGFR gene amplification might be solved during new therapy, while AEs are alleviated by adjusting erdafitinib dosing.
There were some limitations in our article. For instance, the patients’ characteristics, the dose of erdafitinib, and FGFR gene alterations differ, which result in unavoidable heterogeneity. Moreover, restricted to the small number of included studies, we did not conduct meta-regression and funnel plots to assess the publication bias. Last but not least, all of the included articles are single-arm trials and lacked comparisons to other therapies.
As the first FDA-approved FGFR inhibitor to treat urothelial cancer, erdafitinib has a more satisfactory effect than traditional therapy. The most common AE is hyperphosphatemia, which occurs in grade 1–2 and can be controlled with sevelamer. Another AE worth discussing is pCSC. pCSC is caused by inhibiting the MAPK pathway, which needs to be distinguished from true CSC and PNR. Moreover, erdafitinib has rare severe AEs. In efficacy analysis, erdafitinib can increase the PFS significantly, among which, patients with FGFR mutations have a better response than those with fusions, while in FGFR gene fusion, FGFR3-TACC3 is the most sensitive gene alteration. Further studies on single-use and combined therapy of erdafitinib are ongoing, such as the phase III PROOF 302 trial (NCT04197986), which evaluates the efficacy of the FGFR1–3 inhibitor infigratinib in invasive urothelial carcinoma, which provides evidence for FGFR inhibitors in clinical decisions (48). After more clinical trials are published, the discoveries will be further improved.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
XYZ, HW, and JD wrote the original manuscript, and XLM designed and supervised this study. MHY made the major contribution to the data extracted. XHZ and FZ edited the language and improved figures and tables. All authors analyzed the data and edited the manuscript. All authors contributed to the article and approved the submitted version.
The authors thank JZ for providing language help. The first author also expresses heartfelt gratitude to Peng T, for T's constant encouragement and guidance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.907377/full#supplementary-material
UC, Urothelial carcinoma; SMi, Small molecule inhibitor; CRR, Complete response rate; PRR, Partial response rate; ORR, Objective response rate; SD, Stable disease; HR, Hazard ratio; RR, Risk ratio; PFS, Progression-free survival; AE, Adverse events; CMA, Comprehensive meta-analysis; ROBINS-I, Risk of bias in nonrandomized studies of interventions; pCSC, Pseudo-central serous chorioretinopathy; CSC, Central serous chorioretinopathy; RPE, Retinal pigment epithelium.
1. Cumberbatch MGK, Jubber I, Black PC, Esperto F, Figueroa JD, Kamat AM, et al. Epidemiology of bladder cancer: A systematic review and contemporary update of risk factors in 2018. Eur Urol (2018) 74:784–95. doi: 10.1016/j.eururo.2018.09.001
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
3. Chang SS, Bochner BH, Chou R, Dreicer R, Kamat AM, Lerner SP, et al. Treatment of nonmetastatic muscle-invasive bladder cancer: American urological Association/American society of clinical Oncology/American society for radiation Oncology/Society of urologic oncology clinical practice guideline summary. J Oncol Pract (2017) 13:621–5. doi: 10.1200/jop.2017.024919
4. Babjuk M, Burger M, Capoun O, Cohen D, Compérat EM, Dominguez Escrig JL, et al. European Association of urology guidelines on non-muscle-invasive bladder cancer (Ta, T1, and carcinoma in situ). Eur Urol (2022) 81:75–94. doi: 10.1016/j.eururo.2021.08.010
5. von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol Off J Am Soc Clin Oncol (2000) 18:3068–77. doi: 10.1200/jco.2000.18.17.3068
6. Sternberg CN, de Mulder P, Schornagel JH, Theodore C, Fossa SD, van Oosterom AT, et al. Seven year update of an EORTC phase III trial of high-dose intensity m-VAC chemotherapy and G-CSF versus classic m-VAC in advanced urothelial tract tumours. Eur J Cancer (Oxford Engl 1990) (2006) 42:50–4. doi: 10.1016/j.ejca.2005.08.032
7. Bellmunt J, de Wit R, Vaughn DJ, Fradet Y, Lee JL, Fong L, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. New Engl J Med (2017) 376:1015–26. doi: 10.1056/NEJMoa1613683
8. Perera TPS, Jovcheva E, Mevellec L, Vialard J, De Lange D, Verhulst T, et al. Discovery and pharmacological characterization of JNJ-42756493 (Erdafitinib), a functionally selective small-molecule FGFR family inhibitor. Mol Cancer Ther (2017) 16:1010–20. doi: 10.1158/1535-7163.Mct-16-0589
9. Mohammadi M, Olsen SK, Ibrahimi OA. Structural basis for fibroblast growth factor receptor activation. Cytokine Growth factor Rev (2005) 16:107–37. doi: 10.1016/j.cytogfr.2005.01.008
10. Gotoh N. Regulation of growth factor signaling by FRS2 family docking/scaffold adaptor proteins. Cancer Sci (2008) 99:1319–25. doi: 10.1111/j.1349-7006.2008.00840.x
11. Kouhara H, Hadari YR, Spivak-Kroizman T, Schilling J, Bar-Sagi D, Lax I, et al. A lipid-anchored Grb2-binding protein that links FGF-receptor activation to the Ras/MAPK signaling pathway. Cell (1997) 89:693–702. doi: 10.1016/s0092-8674(00)80252-4
12. Goetz R, Mohammadi M. Exploring mechanisms of FGF signalling through the lens of structural biology. Nat Rev Mol Cell Biol (2013) 14:166–80. doi: 10.1038/nrm3528
13. Turner N, Grose R. Fibroblast growth factor signalling: from development to cancer. Nat Rev Cancer (2010) 10:116–29. doi: 10.1038/nrc2780
14. Roskoski R Jr. The role of fibroblast growth factor receptor (FGFR) protein-tyrosine kinase inhibitors in the treatment of cancers including those of the urinary bladder. Pharmacol Res (2020) 151:104567. doi: 10.1016/j.phrs.2019.104567
15. Helsten T, Elkin S, Arthur E, Tomson BN, Carter J, Kurzrock R. The FGFR landscape in cancer: Analysis of 4,853 tumors by next-generation sequencing. Clin Cancer Res an Off J Am Assoc Cancer Res (2016) 22:259–67. doi: 10.1158/1078-0432.Ccr-14-3212
16. Li F, Huynh H, Li X, Ruddy DA, Wang Y, Ong R, et al. FGFR-mediated reactivation of MAPK signaling attenuates antitumor effects of imatinib in gastrointestinal stromal tumors. Cancer Discovery (2015) 5:438–51. doi: 10.1158/2159-8290.Cd-14-0763
17. Tomlinson DC, Lamont FR, Shnyder SD, Knowles MA. Fibroblast growth factor receptor 1 promotes proliferation and survival via activation of the mitogen-activated protein kinase pathway in bladder cancer. Cancer Res (2009) 69:4613–20. doi: 10.1158/0008-5472.Can-08-2816
18. Baselga J. Targeting the phosphoinositide-3 (PI3) kinase pathway in breast cancer. Oncologist (2011) 16 Suppl 1:12–9. doi: 10.1634/theoncologist.2011-S1-12
19. Chen Y, Li X, Eswarakumar VP, Seger R, Lonai P. Fibroblast growth factor (FGF) signaling through PI 3-kinase and Akt/PKB is required for embryoid body differentiation. Oncogene (2000) 19:3750–6. doi: 10.1038/sj.onc.1203726
20. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Clinical Res ed.) (2016) 355:i4919. doi: 10.1136/bmj.i4919
21. Schünemann HJ, Cuello C, Akl EA, Mustafa RA, Meerpohl JJ, Thayer K, et al. GRADE guidelines: 18. how ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J Clin Epidemiol (2019) 111:105–14. doi: 10.1016/j.jclinepi.2018.01.012
22. Siefker-Radtke AO, Necchi A, Park SH, García-Donas J, Huddart RA, Burgess EF, et al. Efficacy and safety of erdafitinib in patients with locally advanced or metastatic urothelial carcinoma: long-term follow-up of a phase 2 study. Lancet Oncol (2022) 23:248–58. doi: 10.1016/s1470-2045(21)00660-4
23. Loriot Y, Necchi A, Park SH, Garcia-Donas J, Huddart R, Burgess E, et al. Erdafitinib in locally advanced or metastatic urothelial carcinoma. New Engl J Med (2019) 381:338–48. doi: 10.1056/NEJMoa1817323
24. Monteiro FSM, Silva AGE, Gomes AJPS, Dutra C, Ferreira NO, Mariano RC, et al. Erdafitinib treatment in Brazilian patients with metastatic urothelial carcinoma (mUC): real-world evidence from an expanded access program 13. (2021) 13:17588359211015499. doi: 10.1177/17588359211015499
25. Rastislav B, Antoine I, Cinta H, Alain M, Andres C, Nancy C, et al. Multicenter phase I study of erdafitinib (JNJ-42756493), oral pan-fibroblast growth factor receptor inhibitor, in patients with advanced or refractory solid tumors. %J Clin Cancer Res an Off J Am Assoc Cancer Res 25 (2019) 25(16):4888-4897. doi: 10.1158/1078-0432.CCR-18-3334
26. Tabernero J, Bahleda R, Dienstmann R, Infante JR, Mita A, Italiano A, et al. Phase I dose-escalation study of JNJ-42756493, an oral pan-fibroblast growth factor receptor inhibitor, in patients with advanced solid tumors. J Clin Oncol (2015) 33:3401–8. doi: 10.1200/JCO.2014.60.7341
27. Nishina T, Takahashi S, Iwasawa R, Noguchi H, Aoki M, Doi T. Safety, pharmacokinetic, and pharmacodynamics of erdafitinib, a pan-fibroblast growth factor receptor (FGFR) tyrosine kinase inhibitor, in patients with advanced or refractory solid tumors %J investigational new drugs. (2018) 36(3):424-434. doi: 10.1007/s10637-017-0514-4
28. Costa R, Carneiro BA, Taxter T, Tavora FA, Kalyan A, Pai SA, et al. FGFR3-TACC3 fusion in solid tumors: mini review. Oncotarget (2016) 7:55924–38. doi: 10.18632/oncotarget.10482
29. Kim SB, Meric-Bernstam F, Kalyan A, Babich A, Liu R, Tanigawa T, et al. First-in-Human phase I study of aprutumab ixadotin, a fibroblast growth factor receptor 2 antibody-drug conjugate (BAY 1187982) in patients with advanced cancer. Target Oncol (2019) 14:591–601. doi: 10.1007/s11523-019-00670-4
30. Kim RD, Sarker D, Meyer T, Yau T, Macarulla T, Park JW, et al. First-in-Human phase I study of fisogatinib (BLU-554) validates aberrant FGF19 signaling as a driver event in hepatocellular carcinoma. Cancer Discovery (2019) 9:1696–707. doi: 10.1158/2159-8290.Cd-19-0555
31. Chan SL, Yen C-J, Schuler M, Lin C-C, Choo SP, Weiss K-H, et al. Abstract CT106: Ph I/II study of FGF401 in adult pts with HCC or solid tumors characterized by FGFR4/KLB expression. Cancer Res (2017) 77:CT106–6. doi: 10.1158/1538-7445.AM2017-CT106%JCancerResearch
32. Chandana SR, Babiker HM, Mahadevan D. Clinical complexity of utilizing FGFR inhibitors in cancer therapeutics. Expert Opin Investigational Drugs (2020) 29:1413–29. doi: 10.1080/13543784.2020.1838484
33. Razzaque MS. The FGF23-klotho axis: endocrine regulation of phosphate homeostasis. Nat Rev Endocrinol (2009) 5:611–9. doi: 10.1038/nrendo.2009.196
34. Meng F, Bertucci C, Gao Y, Li J, Luu S, LeBoff MS, et al. Fibroblast growth factor 23 counters vitamin d metabolism and action in human mesenchymal stem cells. J Steroid Biochem Mol Biol (2020) 199:105587. doi: 10.1016/j.jsbmb.2020.105587
35. Wohrle S, Bonny O, Beluch N, Gaulis S, Stamm C, Scheibler M, et al. FGF receptors control vitamin d and phosphate homeostasis by mediating renal FGF-23 signaling and regulating FGF-23 expression in bone. J Bone Miner Res (2011) 26:2486–97. doi: 10.1002/jbmr.478
36. Shimada T, Urakawa I, Yamazaki Y, Hasegawa H, Hino R, Yoneya T, et al. FGF-23 transgenic mice demonstrate hypophosphatemic rickets with reduced expression of sodium phosphate cotransporter type IIa. Biochem Biophys Res Commun (2004) 314:409–14. doi: 10.1016/j.bbrc.2003.12.102
37. Baum M, Schiavi S, Dwarakanath V, Quigley R. Effect of fibroblast growth factor-23 on phosphate transport in proximal tubules. Kidney Int (2005) 68:1148–53. doi: 10.1111/j.1523-1755.2005.00506.x
38. Muñoz-Castañeda JR, Herencia C, Pendón-Ruiz de Mier MV, Rodriguez-Ortiz ME, Diaz-Tocados JM, Vergara N, et al. Differential regulation of renal klotho and FGFR1 in normal and uremic rats. FASEB J Off Publ Fed Am Societies Exp Biol (2017) 31:3858–67. doi: 10.1096/fj.201700006R
39. Mohammadi M, Froum S, Hamby JM, Schroeder MC, Panek RL, Lu GH, et al. Crystal structure of an angiogenesis inhibitor bound to the FGF receptor tyrosine kinase domain. EMBO J (1998) 17:5896–904. doi: 10.1093/emboj/17.20.5896
40. Isakova T, Wolf MS. FGF23 or PTH: which comes first in CKD? Kidney Int (2010) 78:947–9. doi: 10.1038/ki.2010.281
41. Parikh D, Eliott D, Kim LA. Fibroblast growth factor receptor inhibitor-associated retinopathy. JAMA Ophthalmol (2020) 138:1101–3. doi: 10.1001/jamaophthalmol.2020.2778
42. Jung SM, Valmaggia C, Jörger M, Todorova M. Drug-induced pseudo-central serous chorioretinopathy in carcinoma patients. Klinische Monatsblatter fur Augenheilkunde (2021) 238:403–9. doi: 10.1055/a-1403-3068
43. van Dijk EH, van Herpen CM, Marinkovic M, Haanen JB, Amundson D, Luyten GP, et al. Serous retinopathy associated with mitogen-activated protein kinase kinase inhibition (Binimetinib) for metastatic cutaneous and uveal melanoma. Ophthalmology (2015) 122:1907–16. doi: 10.1016/j.ophtha.2015.05.027
44. Weber ML, Liang MC, Flaherty KT, Heier JS. Subretinal fluid associated with MEK inhibitor use in the treatment of systemic cancer. JAMA Ophthalmol (2016) 134:855–62. doi: 10.1001/jamaophthalmol.2016.0090
45. Pastor JC, Rojas J, Pastor-Idoate S, Di Lauro S, Gonzalez-Buendia L, Delgado-Tirado S. Proliferative vitreoretinopathy: A new concept of disease pathogenesis and practical consequences. Prog retinal eye Res (2016) 51:125–55. doi: 10.1016/j.preteyeres.2015.07.005
46. Zhang Y, Wang R, Zhang H, Liu L, An J, Hao J, et al. Plumbagin inhibits proliferation, migration, and invasion of retinal pigment epithelial cells induced by FGF-2. Tissue Cell (2021) 72:101547. doi: 10.1016/j.tice.2021.101547
47. Rosenthal R, Malek G, Salomon N, Peill-Meininghaus M, Coeppicus L, Wohlleben H, et al. The fibroblast growth factor receptors, FGFR-1 and FGFR-2, mediate two independent signalling pathways in human retinal pigment epithelial cells. Biochem Biophys Res Commun (2005) 337:241–7. doi: 10.1016/j.bbrc.2005.09.028
Keywords: erdafitinib, urothelial carcinoma, FGFR, hyperphosphatemia, central serous chorioretinopathy
Citation: Zheng X, Wang H, Deng J, Yao M, Zou X, Zhang F and Ma X (2023) Safety and efficacy of the pan-FGFR inhibitor erdafitinib in advanced urothelial carcinoma and other solid tumors: A systematic review and meta-analysis. Front. Oncol. 12:907377. doi: 10.3389/fonc.2022.907377
Received: 26 April 2022; Accepted: 13 December 2022;
Published: 26 January 2023.
Edited by:
Gianluca Ingrosso, University of Perugia, ItalyReviewed by:
Matthias Ocker, Charité Universitätsmedizin Berlin, GermanyCopyright © 2023 Zheng, Wang, Deng, Yao, Zou, Zhang and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiuhe Zou, em91eGl1aGUxOTg2QDE2My5jb20=; Fan Zhang, NDU3MDE3NTlAcXEuY29t
†These authors have contributed equally to this work
‡These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.