
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 12 July 2022
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.904800
This article is part of the Research Topic Optimizing Outcomes and Addressing Adversities of Immunotherapy in Lung Cancer View all 17 articles
 Luis E. Raez1†
Luis E. Raez1† Oscar Arrieta2†
Oscar Arrieta2† Diego F. Chamorro3,4†
Diego F. Chamorro3,4† Pamela Denisse Soberanis-Piña2†
Pamela Denisse Soberanis-Piña2† Luis Corrales5
Luis Corrales5 Claudio Martín6
Claudio Martín6 Mauricio Cuello7
Mauricio Cuello7 Suraj Samtani8
Suraj Samtani8 Gonzalo Recondo9
Gonzalo Recondo9 Luis Mas10
Luis Mas10 Zyanya Lucia Zatarain-Barrón2
Zyanya Lucia Zatarain-Barrón2 Alejandro Ruíz-Patiño3,4
Alejandro Ruíz-Patiño3,4 Juan Esteban García-Robledo11
Juan Esteban García-Robledo11 Camila Ordoñez-Reyes3,4
Camila Ordoñez-Reyes3,4 Elvira Jaller3,4
Elvira Jaller3,4 Franco Dickson1Leonardo Rojas12
Franco Dickson1Leonardo Rojas12 Christian Rolfo13Rafael Rosell14
Christian Rolfo13Rafael Rosell14 Andrés F. Cardona3,4,15*† on behalf of CLICaP
Andrés F. Cardona3,4,15*† on behalf of CLICaPObjectives: To compare the rate disparity between outcomes (overall survival (OS), progression-free survival (PFS), and safety) of concurrent chemoradiation (cCRT) followed by durvalumab in two patient cohorts with locally advanced (LA) stage III non-small cell lung cancer (NSCLC), one non-Hispanic White (NHW), and the other Latin-American.
Methods: A multicenter retrospective study was performed, including 80 Hispanic and 45 NHW LA stage III NSCLC patients treated with cCRT followed by durvalumab. Both cohorts were analyzed in terms of main outcomes (OS, PFS, and safety) and compared between them and with the PACIFIC trial population outcomes. The efficacy-effectiveness gap was assessed using an efficacy-effectiveness (EE) factor that was calculated by dividing each cohort median overall survival by the corresponding reference OS from the PACIFIC trial. In both cohorts, results of PD-L1 testing were recorded, and the main outcomes were compared according to PD-1 expression levels (≥50%, 1–49%, and <1%).
Results: For the entire population (N=125), the overall response rate (ORR) was 57.6% (N=72), and 18.4% (N=25) achieved stable disease. OS was 26.3 months (95%CI 23.9-28.6), and PFS was 20.5 months (95%CI 18.0-23.0). PFS assessed by ethnicity showed a median for the Hispanic population of 19.4 months (95%CI 16.4-22.5) and 21.2 months (95%CI 17.2-23.3; p=0.76) for the NHW group. OS by race showed a significant difference in favor of the NHW group, with a median OS of 27.7 months (95%CI 24.6-30.9) vs. 20.0 months (95%CI 16.4-23.5) for Hispanics. (P=0.032). Unadjusted 12-month and 24-month OS was 86.6% (95%CI 79.9–88.0) and 46.6% (95%CI 40.2–48.3) for NHW compared to 82.5% (95%CI 77.1–84.2) and 17.5% (95%CI 15.6-24.5) in Hispanics. NHW had an EE factor of 0.78 and Hispanics had 0.58, showing a reduction in survival versus NHW and PACIFIC of 20% and 42%, respectively. HR for the OS among NHWs and Hispanics was 1.53 (95%CI 1.12-1.71; P=0.052) and 2.31 (95%CI 1.76-2.49; P=0.004). Fifty-six patients (44.8%) had some degree of pneumonitis due to cCRT plus durvalumab. There was no difference in the proportion of pneumonitis according to race (P=0.95), and the severity of pneumonitis was not significantly different between Hispanics and NHWs (P=0.41).
Conclusions: Among patients with LA stage III NSCLC, NHW had better survival outcomes when compared to Hispanics, with an OS that seems to favor the NHW population and with an EE factor that shows a shorter survival in Hispanics compared with NHW and with the PACIFIC trial group.
• Chemoradiation followed by durvalumab is the standard of care in locally advanced stage III NSCLC.
• Outcomes of this treatment are not evaluated in Hispanic patients and could be inferior compared with non-Hispanic whites and even more with the results shown in the registry trial (PACIFIC).
• Reasons for inferior results in Hispanic patients must be evaluated and analyzed in prospective trials and could be related to delays in starting durvalumab after chemoradiation treatment.
Lung cancer (LC) has been one of the leading causes of cancer-related deaths during the last years in the United States, and it continues to be one of the leading causes of cancer-related deaths in men and women worldwide (1). Among LC, non-small cell lung cancer (NSCLC) accounts for 85% of all cases, with 1.28 million diagnoses made between 2007 and 2017 (2, 3). In the US, nearly 30% of patients with NSCLC are diagnosed with locally advanced disease (Stage III). This stage represents a complex group of patients with diverse characteristics regarding the extension of the disease, prognosis, and possible management that goes from resectable to unresectable lesions (4, 5). In patients with unresectable disease, platinum-based chemotherapy with concurrent chemotherapy has been the standard of care (6).
However, in 2017, the PACIFIC trial changed the treatment paradigm for locally advanced NSCLC. This study demonstrated a significant improvement in progression-free survival (PFS) and overall survival (OS) among patients who received durvalumab (anti-PD-L1) in addition to concurrent chemoradiotherapy (cCRT) (7). The updated 5-year analysis of the PACIFIC trial remained consistent with the current outcomes and showed a PFS of 33.1% and an OS of 42.9% in the durvalumab arm (8). In addition, durvalumab has been demonstrated to be safe, with pneumonitis as the main adverse effect (4.4%) (9).
Despite the clear evidence of benefits with immunotherapy in locally advanced NSCLC, most clinical trials have been done in Non-Hispanic Whites (NHW), leaving aside other population groups such as Hispanics. There are many disparities in the outcomes of Hispanic patients compared with NHW when they are treated with immunotherapy. These disparities begin with differential access to optimal cancer care and treatment, molecular profiling, or follow-up (10, 11).
To provide some insights into the disparities between Hispanics and NHW in the outcomes of NSCLC treatment, we designed a multicenter retrospective study that included both populations and compared the outcomes after treatment with durvalumab in addition to cCRT.
This multicenter retrospective study included 80 Hispanic patients with histologically and/or cytologically confirmed unresectable stage III NSCLC who received at least one cycle of consolidative durvalumab post-cCRT, after reaching stable disease. All were treated in fourth-level centers in Florida (United States), Mexico, Central America, and Colombia between February 2018 and December 2021. To compare the rate of disparity in outcomes, the results of Hispanic patients were compared to a cohort of non-Hispanic white (NHW) patients (N=45) treated in the United States (at Memorial Cancer Institute, part of Memorial Healthcare System, Miami, FL), assuming that their results were homogeneous with those presented in the PACIFIC study (12) (Supplementary Figure S1). An independent review board approved the study in Bogotá Colombia (Kayre/FICMAC IRB 2018-14-021), and institutional approval of each linked site was subsequently obtained. In addition, the study was conducted in accordance with the Declaration of Helsinki. In each case, cCRT was administered with curative intent (54-66 Gy) concurrently with platinum-based chemotherapy for at least two cycles, followed by immunotherapy with durvalumab for one year (10 mg/kg intravenously every 2 weeks). Radiotherapy administered to patients was homogeneous, and all patients were treated with radiation in reference centers of main cities in Latin America using intensity-modulated radiation therapy (IMRT) (13). Furthermore, all participating radiotherapy centers have radiation protocols under ASTRO/ESTRO recommendations (14). Treatment patients with EGFR mutations (N=6) or ALK translocations (N=1) were allowed to be included, and each treating physician chose the concurrent chemotherapeutic regimen. The simulation procedure for RT planning and the definitions of target volumes followed previous recommendations and descriptions (15, 16). Follow-up chest CT was performed 1 month after cCRT, positron emission tomography (PET)-CT was done at diagnosis (92% of cases) and 3-4 months after the completion of cCRT (when available), and chest CT was repeated every 3 months after completion of CCRT as follow-up.
Globally, information was collected on tumor status, age, sex, Eastern Cooperative Oncology Group (ECOG) performance status, smoking history, number of pack-year, baseline lung comorbidities (asthma, chronic obstructive pulmonary disease, interstitial lung disease), histology subtype, cancer stage, PD-L1 expression status, platinum type, and time from cCRT completion to ICI start date. Information regarding the main adverse effects, with particular emphasis on post-cCRT pneumonitis, was also collected. The study estimated progression-free survival (PFS), overall response rate (ORR), overall survival (OS), and the primary outcomes obtained with the second line. The analysis of the results was stratified according to the expression of PD-L1 and according to RECIST-1.1 (17).
The PFS was defined as the last date of cCRT until radiographically confirmed progression or death. OS was defined as the time from treatment to death or loss to follow-up. Radiation pneumonitis was diagnosed clinically based on the presence of classic symptoms, timing, history of radiation therapy, imaging findings, and exclusion of alternative causes, such as infection, cardiogenic edema, pulmonary embolism, drug-induced pneumonitis, and other causes. Radiation pneumonitis may be graded using the Common Toxicity Criteria for Adverse Events (Version 5.0) (Common Terminology Criteria for Adverse Events (CTCAE) |, Protocol Development |, CTEP (2000). Retrieved from, https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.) (18).
PD-L1 expression was determined by immunohistochemistry using the Dako 22C3 pharmDx kit, with more than 100 tumor cells present in the slide section for accurate PD-L1 readings. PD-L1 testing was completed on biopsies taken at diagnoses. Patients were grouped according to PD-L1 status (i.e., ≥50%, 1–49%, and <1% subgroups) for survival analyses. Patients with unknown PD-L1 expression status were also included in this study to reflect real-world durvalumab use.
All analyses were conducted on IBM SPSS Statistics software version 25.0 (SPSS Inc. Chicago, IL, USA). Descriptive analyses were utilized to provide an overview of the characteristics of the study population. Categorical variables were assessed via the Chi-Square test or, whenever appropriate, Fisher’s Exact test. OS and PFS were reported as Kaplan Meier survival curves. Multivariable Cox regression models were generated to assess potential confounders. Two-sided P-Value was set to determine statistically significant outcomes. There were no adjustments made for multiple comparisons, and in all cases, the significance level was P=0.05. The efficacy-effectiveness gap was assessed using an efficacy-effectiveness (EE) factor that was calculated by dividing each cohort’s median overall survival by the corresponding reference OS from the most recent report from PACIFIC (12). This factor was used to estimate the presence of an EE gap and compare the real-world population’s survival relative to the clinical trial population. An EE factor of 0.60 indicates that median survival is 40% shorter in clinical practice than in the reference clinical trial (19).
Eighty Hispanic patients and 45 NHW were included. Baseline patient and treatment characteristics are summarized in Table 1. To establish the comparability of clinical variables between Hispanic patients treated in the US and Latin American countries, a stratified analysis was performed for age (P=0.53), gender (P=0.71), baseline performance status (P=0.22), and place of origin (P=0.57) without finding statistically significant differences. This allowed consideration of a balanced intervention for both populations to carry out a correct analysis of the disparities between groups. At the time of diagnosis, 52% of the patients were ≥65 years old, the majority were women (52.8%), and the most frequent histology was adenocarcinoma (80%). Two-thirds of the non-smoking patients were women (14/21), and six of them had EGFR mutations (four with exon 19 deletions and two with the L858R mutation). Overall, 19 (15.2%), 35 (28.0%), and 65 (52.0%) patients had PD-L1 expression ≥50%, <1%, and between 1%-49%, respectively. Most patients had a good ECOG performance status; 60% received carboplatin as part of the cCRT regimen, especially in combination with paclitaxel (40%) or pemetrexed (20%). The mean time from cCRT completion to durvalumab initiation was 37.3 days (SD ±23.7, range 7-133 days). There were no statistically significant imbalances between PD-L1 subgroups. Still, a significant difference was found in Hispanics regarding using the cisplatin/pemetrexed combination, while NHW were more exposed to cisplatin/etoposide (P=0.002). Similarly, the mean time interval between cCRT and the start of durvalumab was significantly shorter in NHW (difference of 10 days less, P=0.02). The median follow-up for the entire cohort of included patients was 19.6 months (95%CI 8.1-39.2).
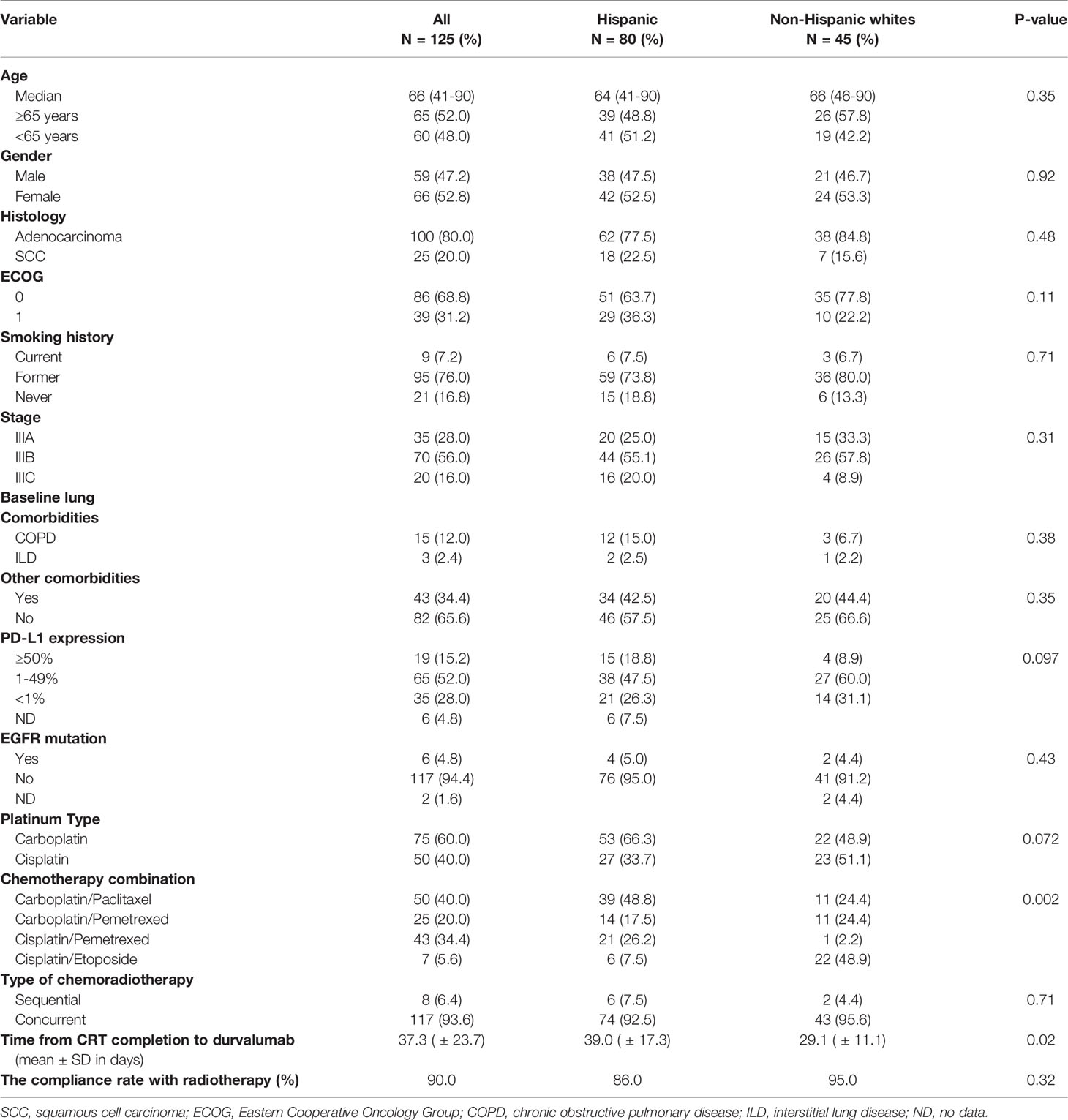
Table 1 Baseline patient and treatment characteristics.
For the 125 patients, the overall response rate (ORR) was 57.6% (N=72), and 18.4% (N=25) achieved stable disease (SD). OS was 26.3 months (95%CI 23.9-28.6) (Supplementary Figure S2A), and PFS was 20.5 months (95%CI 18.0-23.0) (Supplementary Figure S2B). When PFS was assessed by ethnicity, the median for the Hispanic population was 19.4 months (95%CI 16.4-22.5) and 21.2 months (95%CI 17.2-23.3; P=0.76) for the NHW group (Figure 1A). However, analysis of OS showed a significant difference in favor of the NHW group, given the median was 27.7 months (95%CI 24.6-30.9) versus 20.0 months (95%CI 16.4-23.5) for Hispanics. (P=0.032) (Figure 1B). Unadjusted 12-month and 24-month OS was 86.6% (95%CI 79.9–88.0) and 46.6% (95%CI 40.2–48.3) for NHW compared to 82.5% (95%CI 77.1–84.2) and 17.5% (95%CI 15.6-24.5) in Hispanics.
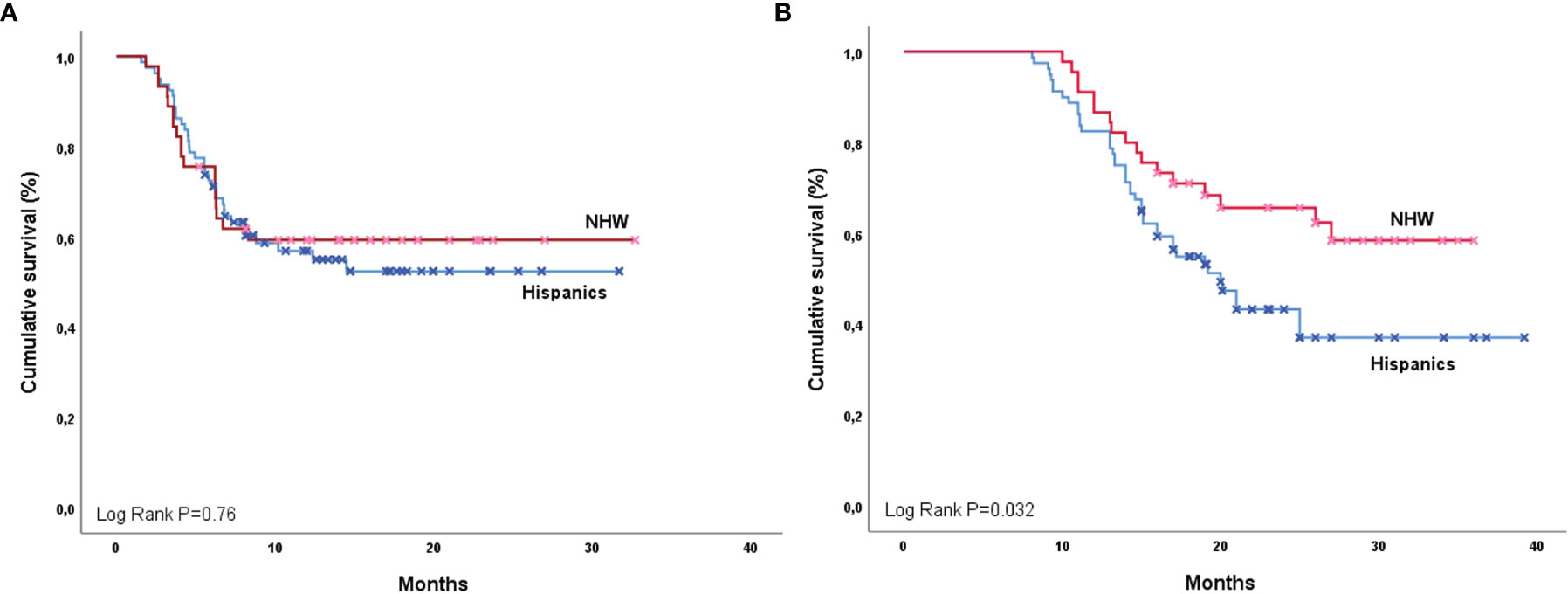
Figure 1 Progression-free survival (A) and overall survival (B) by ethnicity (Hispanic and NHW).
Among Hispanics, PFS was higher in those with better ECOG [ECOG 0: 21.4 months (95%CI 17.8-25.1) vs. ECOG 1: 10.2 months (95%CI 4.6-15.7); P=0.19] (Supplementary Figure S3), in patients with SCC [25.5 months (95%CI 20.2-30.8) vs. Adenocarcinomas 15.5 (CI95% 12.8-18.3); P=0.06] (Supplementary Figure S4) and in those with higher PD-L1 expression [PD-L1 ≥50% PFS NR, PD-L1 1-49% 14.5 months (95%CI 8.8-NR) and PD-L1 <1% 12.3 months (95%CI 6.8-13.6); P=0.001]. Neither history of tobacco exposure (P=0.67), tumor stage (P=0.10), nor presence of pneumonitis (P=0.51) influenced PFS among Hispanics. For the NHW group, the only variable that influenced PFS was the level of PDL-1 expression [PD-L1 ≥50% PFS NR, PD-L1 1%-49% 13.3 months (95%CI 11.9-NR) and PD-L1 <1% 10.4 months (95%CI 9.8-14.6); P=0.018)].
Univariate analysis for OS revealed that overall response to CRT positively impacted the survival in both Hispanics [OS responders 29.2 months (95%CI 25.8-37.7) vs. Non-responders 13.3 months (95%CI 10.3-16.2); P=0.0001] (Figure 2A) and NHW groups [OS responders 34.9 months (95%CI 33.6-36.3) vs. Non-responders 14.8 months (95%CI 13.1-16.4); P=0.0001] (Figure 3A). Similarly, Hispanic patients [PD-L1 ≥50% OS NR, PD-L1 1%-49% 25.0 months (95%CI 19.2-NR), and PD-L1 <1% 19.0 months (95%CI 13.0-16.1); P=0.0001] (Figure 2B) and NHW [PD-L1 ≥50% OS NR, PD-L1 1-49% 24.0 months (95%CI 14.7-NR) and PD-L1 <1% 19.0 months (95%CI 13.0- 16.8); P=0.04] (Figure 3B) with higher PD-L1 expression had better OS. Neither ECOG, smoking history, tumor staging, histology, nor pneumonitis influenced OS in either group. In the multivariate model for OS, the only predictor of increased mortality was lack of response after CRT (HR 7.8, 95%CI 3.1-19.4). In contrast, the only factor that positively impacted OS among Hispanics and NHW was PD-L1 expression ≥50% compared to the PD-L1 <1% group (HR 0.69, 95%CI 0.50-0.97). 08). In the model for PFS, the only predictor for a better outcome among Hispanics and NHW was PD-L1 expression ≥50% (HR 0.55, 95%CI 0.37-0.81). The OS (P=0.52) and PFS (P=0.40) of patients carrying EGFR mutations did not differ significantly from the Wt population.
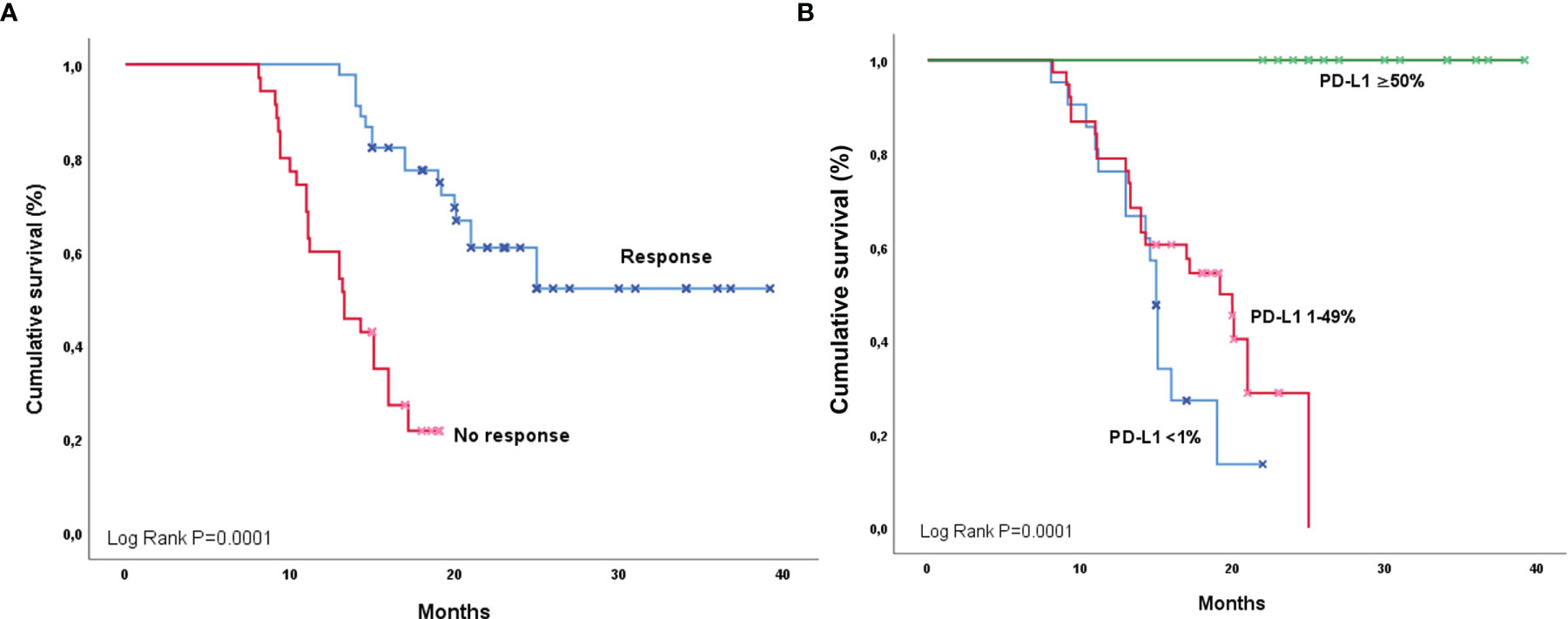
Figure 2 Overall survival among Hispanics according to response (A) and PD-L1 expression (B).
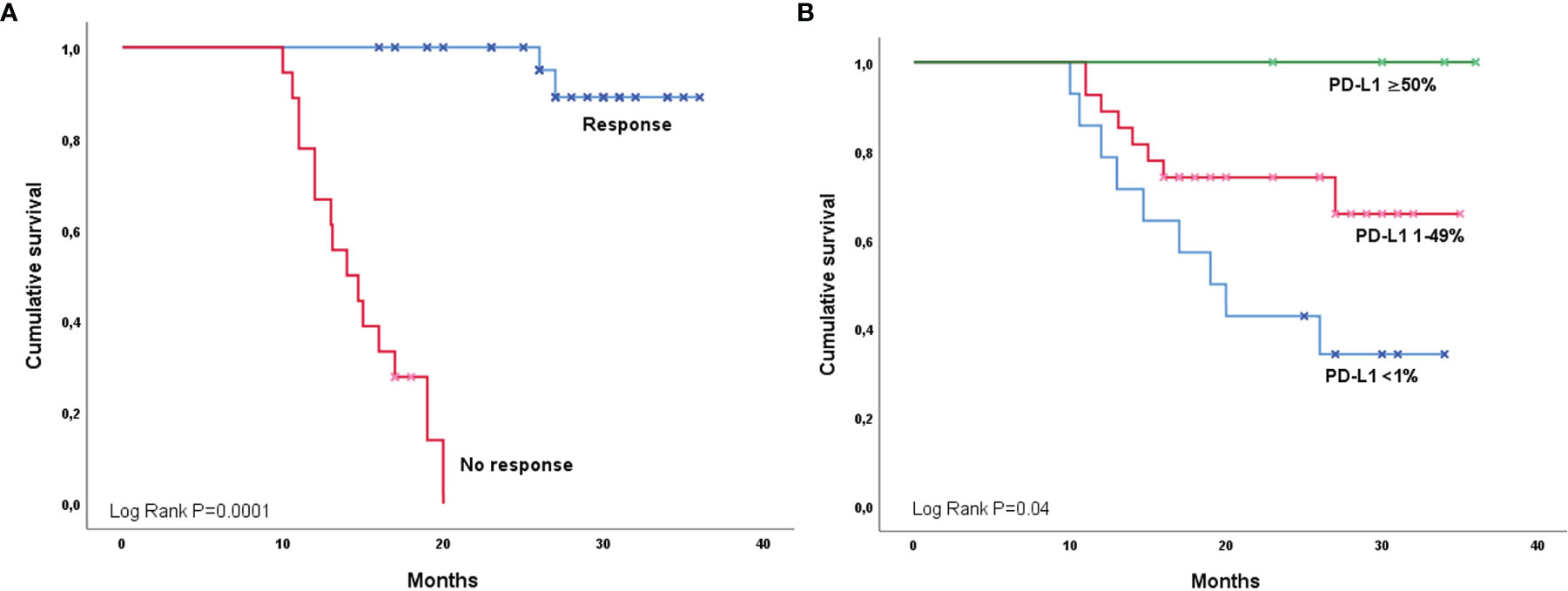
Figure 3 Overall survival among NHWs according to response (A) and PD-L1 expression (B).
To compare data derived from the PACIFIC study with real-life Hispanics and NHW treated with CRT and durvalumab in our research, the efficacy-effectiveness factor and hazard ratio for OS (between 24 and 36 months of follow-up) was estimated, comparing both groups to the durvalumab arm in the PACIFIC. NHW had an EE factor of 0.78, indicating that median OS was 22% shorter for those patients treated in clinical practice than median OS from the registered clinical trial receiving the same treatment. In addition, the EE factor for Hispanics was 0.58, showing a reduction in survival versus NHW and PACIFIC of 20% and 42%, respectively. The corresponding HR for the OS among NHW and Hispanics was 1.53 (95%CI 1.12-1.71; P=0.052) and 2.31 (95%CI 1.76-2.49; P=0.004), respectively.
In the general population, 56 patients (44.8%) had some degree of pneumonitis due to CRT plus durvalumab. Pneumonitis was grade 1, 2, and 3 in 51.8% (N=29), 35.7% (N=20), and 12.5% (N=7), respectively. There was no difference in the proportion of pneumonitis according to race (P=0.95), previous tobacco exposure (P=0.14), type of chemotherapy regimen (P=0.36), or history of pulmonary comorbidity (P=0.55). Similarly, the severity of pneumonitis was not significantly different between Hispanics and NHW (P=0.41) and was not response-dependent (P=0.24).
It is essential to do real-world studies with diverse ethnic populations to address cancer disparities, reduce the variability of the results among minorities, and promote global access oncology. In the original PACIFIC trial, a landmark study that changed the standard of care in Stage IIII NSCLC, less than 2% of enrolled patients were documented as a minority, and there was no information about Hispanic ethnicity. In our multicenter retrospective study, we reported the outcomes of cCRT in addition to durvalumab for stage III NSCLC in two populations, Hispanics and NHW. Some studies have shown that the Hispanic population might have worse immunotherapy outcomes, possibly due to a complex interaction of factors such as culture, genomic heritage, or social determinants of health. Compared with NHW, the median PFS among Hispanics was lower but not significant (P=0.76). Nevertheless, when we analyzed OS stratified by race, we found that NHW reached a higher OS than Hispanics. This finding contrasts with previous studies that found no statistical difference in OS between the two ethnic groups (20).
Interestingly, the PFS and OS were higher in the subgroups with increased expression of PD-L1 in both the Hispanic and NHW groups. This result is consistent with the observations done by Kartolo et al., who found that high expression of PD-L1 was associated with improved survival as an independent prognostic factor (21). However, the most evident benefit was observed in a patient with PD-L1 expression of >50%, with no impact in the groups of PD-L1 expression of 1-49% or <1% (21) and, for our study, the median was not reached for the PDL-1 >50% subgroup. Regardless of the expression, there is evidence that durvalumab has a positive impact on outcomes even with PD-L1 expression higher than 1 to 25% (22, 23). Some evidence suggests that among Hispanics, expression in stage IIIB/IV NSCLC is around 21.7% (24).
Our study reports that overall response to cCRT positively impacts the OS, and the benefit is higher for NHW than for Hispanics (34.9 months vs. 29.2 months, respectively). Previously, some studies documented that complete or partial response to the treatment relates directly to an increased OS (25, 26). In this scenario, the outcome is still better for NHW despite the grade of response.
The results demonstrate that the use of durvalumab consolidation among both Hispanics and NHW is associated with improvement in the OS. When we contrasted the results of our study with those of the PACIFIC trial, we found that among NHW, the OS was slightly inferior in clinical practice (EE gap 0.78). Still, for Hispanics, the median survival was significantly shorter than for NHW (20%) and with the PACIFIC intervention (42%). In real-life scenarios, it has been described that the OS tends to be lower (27). Besides the differences between Hispanics and NHW, the inferior survival in both groups could be attributed to a delayed durvalumab onset and a significantly shorter time in favor of NHW. Post hoc analysis of the PACIFIC trial suggests that starting the ICI within 14 days after cCRT is associated with a higher OS (28). Also, the follow-up of the patients was relatively short.
In the general population, 56 patients (44.8%) had some degree of pneumonitis due to cCRT plus durvalumab. Pneumonitis was grade 1, 2, and 3 in 51.8% (N=29), 35.7% (N=20), and 12.5% (N=7), respectively. There was no difference in the proportion of pneumonitis according to race (P=0.95), previous tobacco exposure (P=0.14), type of chemotherapy regimen (P=0.36), or history of pulmonary comorbidity (P=0.55). Similarly, the severity of pneumonitis was not significantly different between Hispanics and NHW (P=0.41) and was not response-dependent (P=0.24).
In terms of safety, pneumonitis represents the most severe and life-threatening adverse effect related to immunotherapy (26). We reported a higher pneumonitis incidence than the PACIFIC trial (44.8% in the general population) (7). However, most cases were mild to moderate, without any patients needing to stop immunotherapy. This study did not find any variables related to a higher incidence of pneumonitis among the subjects. Some studies failed to identify specific risk factors associated with the development of pneumonitis among patients treated with durvalumab (29).
As we exposed earlier, PFS did not differ between the populations; however, the OS did. This finding could be explained in light of multiple differences between Hispanics vs. NHW, including overall access to second-line therapy or follow-up. Unfortunately, our available data related to the treatment approach after initial therapy is scarce and unbalanced between the two groups in our cohort. Further analyses are required to find a possible impact of these new variables in the response to therapy. In addition, we would like to remark that due to the immortality bias, commonly present in lung cancer scenarios, it is frequent that many patients exposed to ICI have a measurable effect on the OS but not in the PFS (30). On the other hand, populations with EGFR mutations (among others) should be analyzed independently (31).
Limitations in our analysis include a relatively short follow-up period for patients; however, in the same period, we were able to distinguish the differences between the Hispanic and NHW groups compared to the PACIFIC trial results. Furthermore, we only considered patients treated with cCRT plus durvalumab, which could create a selection bias in the study because we did not compare our results with a control population. In addition, the analysis of basal characteristics of the Hispanic patients treated in Latin America and those treated in the US did not show any differences, and this could be a risk for the interpretation of the data. On the other hand, the specific dose of durvalumab was not actively recorded, and information about other immuno-mediated side effects besides pneumonitis was not homogeneous.
Among patients with stage III NSCLC, NHW have better survival outcomes when compared to Hispanics. With an OS that seems to favor the NHW population and an EE factor that shows a shorter survival in Hispanics in comparison with NHW and with the PACIFIC trial group. Further analyses must be done to identify factors that might lead to these differences between Hispanics and NHW, and large clinical trials must include more representation of Hispanics.
The datasets presented in this article are not readily available because of the Colombian organic law of data protection that limits access to raw genetic information in an open format. Requests to access the datasets should be directed to the corresponding author, who will release it upon formal request to the Ministry of Health of Colombia following the requirements of Law 1581 of 2012, paragraph 201811601170851 of 2018.
The studies involving human participants were reviewed and approved by Kayre/FICMAC IRB 2018-14-021. The patients/participants provided their written informed consent to participate in this study.
Conception and study design: LER, OA, CR, RR, AC, LC, CM, and LR. Data acquisition: LR, AC, DC, FD, JG-R, EJ, CO, and AR-P. Analysis and Data interpretation: AR-P, AC, LR, OA, DC, CM, MC, SS, GR, LZ-B, and LM. Article Draft: AFC, DFC, LR, OA, LC, CM, MC, SS, GR, LM, LZB, CR, and RR. Manuscript preparation and approval: All authors.
Supported by The CLICaP and The Foundation for Clinical and Applied Cancer Research- FICMAC (Bogotá, Colombia) research grant 037-2021.
LR discloses research support from Merck Sharp & Dohme, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, Pfizer, Novartis, LOXO Pharmaceuticals, Guardant Health, Natera, Syndax, Eli Lilly, and Astra Zeneca. AC discloses financial research support from Merck Sharp & Dohme, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, and The Foundation for Clinical and Applied Cancer Research – FICMAC. Additionally, he was linked and received honoraria as an advisor, participated in speakers’ bureau, and gave expert testimony to Merck Sharp & Dohme, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, Pfizer, Novartis, Celldex Therapeutics, Foundation Medicine, Eli Lilly, and Foundation for Clinical and Applied Cancer Research – FICMAC. OA reports personal fees from Pfizer, grants and individual fees from Astra Zeneca, grants and individual fees from Boehringer-Ingelheim, personal fees from Lilly, individual fees from Merck, and personal fees from Bristol Myers Squibb, grants and personal fees from Roche, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.904800/full#supplementary-material
1. Barta JA, Powell CA, Wisnivesky JP. Global Epidemiology of Lung Cancer. Ann Glob Heal (2019) 85(1):8. doi: 10.5334/aogh.2419
2. Inamura K. Lung Cancer: Understanding its Molecular Pathology and the 2015 WHO Classification. Front Oncol (2017) 7:193(AUG). doi: 10.3389/fonc.2017.00193
3. Ganti A, Klein A, Cotarla I, Seal B, Chou E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non–Small Cell Lung Cancer in the US. JAMA Oncol (2021) 7(12):1824–32. doi: 10.1001/jamaoncol.2021.4932
4. Morgensztern D, Ng SH, Gao F, Govindan R. Trends in Stage Distribution for Patients With non-Small Cell Lung Cancer: A National Cancer Database Survey. J Thorac Oncol (2010) 5(1):29–33. doi: 10.1097/JTO.0b013e3181c5920c
5. Casal-Mouriño A, Ruano-Ravina A, Lorenzo-González M, Rodríguez-Mártinez A, Giraldo-Osorio A, Varela-Lema L, et al. Epidemiology of Stage III Lung Cancer: Frequency, Diagnostic Characteristics, and Survival Review Articles on Multimodal Management of Locally Advanced N2 Non-Small Cell Lung Cancer. Transl Lung Cancer Res (2021) 10(1):506–18. doi: 10.21037/tlcr.2020.03.40
6. Aupérin A, Le Péchoux C, Rolland E, Curran W, Furuse K, Forunel P, et al. Meta-Analysis of Concomitant Versus Sequential Radiochemotherapy in Locally Advanced Non - Small-Cell Lung Cancer. J Clin Oncol (2010) 28(13):2181–90. doi: 10.1200/JCO.2009.26.2543
7. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Durvalumab After Chemoradiotherapy in Stage III Non–Small-Cell Lung Cancer. N Engl J Med (2017) 377(20):1919–29. doi: 10.1056/nejmoa1709937
8. Spigel DR, Faivre-Finn C, Gray JE, Vicente D, Planchard D, Paz-Ares L, et al. Five-Year Survival Outcomes From the PACIFIC Trial: Durvalumab After Chemoradiotherapy in Stage III Non–Small-Cell Lung Cancer. J Clin Oncol (2022) 40(12):1301–11. doi: 10.1200/jco.21.01308
9. Shibata Y, Murakami S. Safety Evaluation of Durvalumab for the Treatment of Non-Small-Cell Lung Cancer. Expert Opin Drug Saf (2020) 0(0):1. doi: 10.1080/14740338.2020.1764936
10. Cardona F, Arrieta O, Lopes G. Lung Cancer Disparities in Hispanics: Molecular Diagnosis and Use of Immunotherapy. JCO Glob Oncol (2020) 6:784–8. doi: 10.1200/GO.20.00004
11. Zheng R, Yin Z, Alhatem A, Lyle D, You B, Jiang AS, et al. Epidemiologic Features of NSCLC Gene Alterations in Hispanic Patients From Puerto Rico. Cancers (Basel) (2020) 12(12):3492. doi: 10.3390/cancers12123492
12. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Overall Survival With Durvalumab After Chemoradiotherapy in Stage III NSCLC. N Engl J Med (2018) 379(24):2342–50. doi: 10.1056/nejmoa1809697
13. Taylor A, Powell MEB. Intensity-Modulated Radiotherapy - What is it? Cancer Imaging (2004) 4(2):68–73. doi: 10.1102/1470-7330.2004.0003
14. Nestle U, De Ruysscher D, Ricardi U, Geets X, Belderbos J, Pottgen C, et al. ESTRO ACROP Guidelines for Target Volume Definition in the Treatment of Locally Advanced non-Small Cell Lung Cancer. Radiother Oncol (2018) 127(1):1–5. doi: 10.1016/j.radonc.2018.02.023
15. Park SE, Noh JM, Kim YJ, Lee HS, Cho JH, Lim SW, et al. EGFR Mutation Is Associated With Short Progression-Free Survival in Patients With Stage III Non-Squamous Cell Lung Cancer Treated With Concurrent Chemoradiotherapy. Cancer Res Treat (2019) 51(2):493–501. doi: 10.4143/crt.2018.125
16. Noh JM, Kim JM, Ahn YC, Pyo H, Kim B, Oh D, et al. Effect of Radiation Therapy Techniques on Outcome in N3-Positive IIIB Non-Small Cell Lung Cancer Treated With Concurrent Chemoradiotherapy. Cancer Res Treat (2016) 48(1):106–14. doi: 10.4143/crt.2014.131
17. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur J Cancer (2009) 45(2):228–47. doi: 10.1016/j.ejca.2008.10.026
18. National Cancer Intistute. Common Terminology Criteria for Adverse Events (CTCAE) | Protocol Development |CTEP (2017). Available at: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
19. Liu N, Zhou Y, Lee JJ. IPDfromKM: Reconstruct Individual Patient Data From Published Kaplan-Meier Survival Curves. BMC Med Res Methodol (2021) 21(1):1–22. doi: 10.1186/s12874-021-01308-8
20. Price SN, Flores M, Hamann HA, Ruiz JM. Ethnic Differences in Survival Among Lung Cancer Patients: A Systematic Review. JNCI Cancer Spect (2021) 5(5):pkab062. doi: 10.1093/jncics/pkab062
21. Kartolo A, Shah H, Hopman W, Fung A, Wheatley-Price P, Robinson A. Consolidative Durvalumab Outcomes in Stage III Non-Small Cell Lung Cancer in a Multi-Centre Study. Cancer Treat Res Commun (2021) 29:100496. doi: 10.1016/j.ctarc.2021.100496
22. Botticella A, Mezquita L, Le Pechoux C, Planchard D. Durvalumab for Stage III Non-Small-Cell Lung Cancer Patients : Clinical Evidence and Real-World Experience. Ther Adv Respir Dis (2019) 13:1753466619885530. doi: 10.1177/1753466619885530
23. Bruni A, Scotti V, Borghetti P, Vagge S, Cozzi S, D'Angelo E, et al. A Real-World, Multicenter, Observational Retrospective Study of Durvalumab After Concomitant or Sequential Chemoradiation for Unresectable Stage III Non-Small Cell Lung Cancer. Front Oncol (2021) 11:744956(September). doi: 10.3389/fonc.2021.744956
24. Gelatti ACZ, De Lima VCC, Freitas H, Werutsky G, Gaiger AM, Klock C, et al. Real-World Prevalence of PD-L1 Expression Among Tumor Samples From Patients With Non E Small-Cell Lung Cancer. Clin Lung Cancer (2020) 21(6):e511–5. doi: 10.1016/j.cllc.2020.04.007
25. Arrieta OG, Cardona AF, Martin C, Raez L, Zatarain-Barón ZL, Barrón F, et al. Characterization of Hispanic Patients Who Experienced Hyperprogression During Treatment for Advanced NSCLC With Immunotherapy Toxicity as a Clinical Marker for Efficacy of Immunotherapy in NSCLC: A Multicentric Experience F. J Thorac Oncol (2019) 14(10):S474. doi: 10.1016/j.jtho.2019.08.984
26. Patel P, Alrifai D, McDonald F, Forster M. Beyond Chemoradiotherapy: Improving Treatment Outcomes for Patients With Stage III Unresectable non-Small-Cell Lung Cancer Through Immuno-Oncology and Durvalumab (Imfinzi®▼, AstraZeneca UK Limited). Br J Cancer (2020) 123(December):18–27. doi: 10.1038/s41416-020-01071-5
27. Sankar K, Bryant AK, Strohbehn GW, Zhao L, Elliot D, Moghanaki D, et al. Real World Outcomes Versus Clinical Trial Results of Durvalumab Maintenance in Veterans With Stage III Non-Small Cell Lung Cancer. Cancers (Basel) (2022) 14(3):614–24. doi: 10.3390/cancers14030614
28. Faivre-Finn C, Spigel DR, Senan S, Langer C, Perez BA, Özgüroğlu M, et al. Impact of Prior Chemoradiotherapy-Related Variables on Outcomes With Durvalumab in Unresectable Stage III NSCLC (PACIFIC). Lung Cancer (2021) 151:30–8. doi: 10.1016/j.lungcan.2020.11.024
29. Leclair JN, Merl MY, Cohenuram M, Luon D, Leclair JN. Real-World Incidence of Pneumonitis in Patients Receiving Durvalumab. Clin Lung Cancer (2022) 23(1):34–42. doi: 10.1016/j.cllc.2021.08.006
30. Suissa S. Immortal Time Bias in Pharmacoepidemiology. Am J Epidemiol (2008) 167(4):492–9. doi: 10.1093/aje/kwm324
Keywords: durvalumab, non-small cell lung cancer, hispanics, survival, health equity, immunotherapy
Citation: Raez LE, Arrieta O, Chamorro DF, Soberanis-Piña PD, Corrales L, Martín C, Cuello M, Samtani S, Recondo G, Mas L, Zatarain-Barrón ZL, Ruíz-Patiño A, García-Robledo JE, Ordoñez-Reyes C, Jaller E, Dickson F, Rojas L, Rolfo C, Rosell R and Cardona AF (2022) Durvalumab After Chemoradiation for Unresectable Stage III Non-Small Cell Lung Cancer: Inferior Outcomes and Lack of Health Equity in Hispanic Patients Treated With PACIFIC Protocol (LA1-CLICaP). Front. Oncol. 12:904800. doi: 10.3389/fonc.2022.904800
Received: 25 March 2022; Accepted: 23 May 2022;
Published: 12 July 2022.
Edited by:
Idris Bahce, Academic Medical Center, NetherlandsReviewed by:
Yee Ung, University of Toronto, CanadaCopyright © 2022 Raez, Arrieta, Chamorro, Soberanis-Piña, Corrales, Martín, Cuello, Samtani, Recondo, Mas, Zatarain-Barrón, Ruíz-Patiño, García-Robledo, Ordoñez-Reyes, Jaller, Dickson, Rojas, Rolfo, Rosell and Cardona. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrés F. Cardona, YWNhcmRvbmFAZmN0aWMub3Jn
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.