 Siyuan Zeng
Siyuan Zeng Yongai Yu
Yongai Yu Yuemei Cui
Yuemei Cui Bing Liu
Bing Liu Xianyu Jin1
Xianyu Jin1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol., 18 July 2022
Sec. Gynecological Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.900256
This article is part of the Research TopicThe Evolving Use of Neoadjuvant Treatment Paradigms in Gynecologic Malignancies: Early Insights into Pharmacodynamic and Clinical OutcomesView all 6 articles
Objective: The selection of minimally invasive surgery (MIS) or open laparotomy for ovarian cancer (OC) after neoadjuvant chemotherapy still remains controversial. This study aimed to assess the efficacy and safety of MIS versus open laparotomy following neoadjuvant chemotherapy for advanced OC, so as to provide another option to select optimal surgical procedures for patients with OC.
Methods: Relevant literature studies about the risks of progression or mortality between women receiving MIS and open laparotomy for interval debulking surgery (IDS) were searched in the online databases, including PubMed, Embase, and the Cochrane Library with the following keywords: “ovarian neoplasms”, “minimally invasive surgical procedures”, “laparotomy”, and “neoadjuvant therapy”. Eligible studies were screened out for further meta-analysis.
Results: Six eligible literature studies, with 643 patients in the MIS group and 2,885 patients in the open laparotomy group, were included in this meta-analysis. No significant differences were detected in the overall survival (OS) of patients with OC who were treated with MIS or open laparotomy [hazard ratio (HR) = 0.85; 95% confidence interval (CI) = 0.59–1.23; heterogeneity: P = 0.051, I2 = 57.6%]. However, the progression-free survival (PFS) was significantly higher in patients with OC treated with MIS than those treated with laparotomy (HR = 0.73; 95% CI = 0.57 to 0.92; heterogeneity: P = 0.276, I2 = 22.4%). The completeness of debulking removal (R0 rate) in the open laparotomy group was not statistically higher compared with the control group (RR = 1.07; 95% CI = 0.93 to 1.23; heterogeneity: P = 0.098, I2 = 52.3%), and no significant differences in residual disease of ≤1 cm (R1) (RR = 1.08; 95% CI = 0.91 to 1.28; heterogeneity: P = 0.330, I2 = 12.6%) and postoperative complications were found between the two groups (RR = 0.72; 95% CI = 0.34 to 1.54; heterogeneity: P = 0.055, I2 = 60.6%). Furthermore, the length of stays in hospital was significantly shorter in patients with OC treated with MIS than those treated with open laparotomy (Standard Mean Difference (SMD) = −1.21; 95% CI = −1.78 to −0.64; heterogeneity: P < 0.001, I2 = 92.7%].
Conclusions: For IDS after NACT in patients with advanced OC, complete cytoreductive surgery with MIS is another feasible and effective choice
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022298519, identifier CRD42022298519
Ovarian cancer (OC) is one of the most fatal gynecologic cancers in women (1). Epithelial OC is difficult to be detected early, and nearly 75% of patients with OC are detected at advanced stage (2, 3).
Traditionally, in patients with advanced OC, the standard treatment relied on laparotomy-based primary debulking surgery (PDS), followed by adjuvant platinum-based chemotherapy. Another recently emerged and developed treatment strategy is neoadjuvant chemotherapy (NACT) and interval debulking surgery (IDS), particularly in patients with high perioperative risk or limited likelihood of achieving adequate cytoreduction at PDS (4). According to two phase III clinical trials, patients with advanced OC receiving NACT and IDS have equivalent survival to those who received PDS and adjuvant chemotherapy (5, 6), as well as lower incidence of related morbidity and mortality.
However, in patients with advanced OC with large tumor lesions and/or complicated medical conditions, sophisticated surgical treatments may increase the risks of severe postoperative morbidity and mortality (M/M) (7). With the advancement of diagnostic and therapeutic technologies, minimally invasive surgery (MIS) is gradually recognized across gynecological debulking surgery (8). In patients with OC with complete response to NACT, a phase II clinical trial demonstrated that MIS is a feasible, effective, safe, and alternative procedure for IDS (9). According to the most recent OC guidelines (10), MIS is of great importance in debulking surgery of OC. Despite the fact that several studies have assessed the efficacy and safety of MIS and laparotomy in patients with OC after NACT (11–18), the results are still controversial.
To investigate the feasibility of MIS, this study systematically analyzed the comprehensive studies and compared the efficacy and safety of MIS and laparotomy in advanced patients with OC after NACT.
This meta-analysis was performed by following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) criteria (19). The following keywords were searched in the online databases, such as PubMed, Embase, and Cochrane Library: “neoadjuvant therapy”, “minimally invasive surgery”, “open laparotomy”, and “interval debulking surgery”. Selection criteria are as follows: 1) patients with advanced OC; 2) MIS versus open laparotomy in patients with OC who were treated with IDS after NACT; 3) the overall survival (OS), progression-free survival (PFS), completeness of debulking removal (R0), residual disease of ≤1 cm (R1), postoperative complications, and length of stays in hospital were reported; and 4) English-language published literature studies. Exclusion criteria: 1) abstracts without full text; 2) duplicates; and 3) IDS for advanced OC after non-neoadjuvant chemotherapy.
Two investigators were independently responsible for data extraction, and any disagreements were solved by a third contributor. The following data were extracted using a previously formulated data extraction table: (1) basic information of the literature: title, first author, publication journal, time, etc.; (2) baseline characteristics of subjects: age, case number, follow-up time, International Federation of Gynecology and Obstetrics (FIGO) stage, etc.; (3) chemotherapy cycles, American Society of Anesthesiologists physical status classification system (ASA) score, Response Evaluation Criteria in Solid Tumors (RECIST) response, study types, and key elements of quality evaluation; and (4) outcomes and the measurement data. To assess the quality of retrospective investigations, the nine-star Newcastle-Ottawa scale (NOS) was used, and those with a minimum of six stars were considered as high-quality (20).
The directly reported outcomes are rare. Therefore, log-rank p-values or Kaplan–Meier survival curves were used to extract the hazard ratio (HR) and the variance of the text (21); the combined risk ratio (RR) or HR and the corresponding 95% confidence interval (CI) were calculated using Stata 14.0; The Q-test was used to assess heterogeneity. If I2 < 50%, the fixed-effect model was used to combine the HR or RR of each study; otherwise, the random-effect model was utilized. By removing each study and calculating, the sensitivity analysis was used to determine the related effects of individual studies on the combined results. Begg’s funnel plots were depicted to assess publication bias. P < 0.05 was considered to be statistically significant.
As shown in Figure 1, 471 literature studies were initially searched, and 352 remained after excluding duplicates. Through reviewing the titles and abstracts based on the inclusion and exclusion criteria, 344 literature studies were excluded. Finally, six retrospective studies involving 3,528 patients with OC were recruited by reviewing the full text. The basic information of eligible literature studies was listed in Table 1. Three studies were performed in America, two in Europe, and one in Asia. The sample size was from 21 to 3,071. The information of chemotherapy cycles was reported in four articles (two reported patients underwent six cycles of NACT and two reported patients underwent less than six cycles of NACT). Two literature studies reported patients’ ASA score. The RECIST response to NACT was investigated in three articles, and there were no significant differences in NACT response between the MIS group and the laparotomy group in the original studies (Table 1). Moreover, all the studies were assessed as high-quality on the basis of the NOS (Supplementary Table 1).
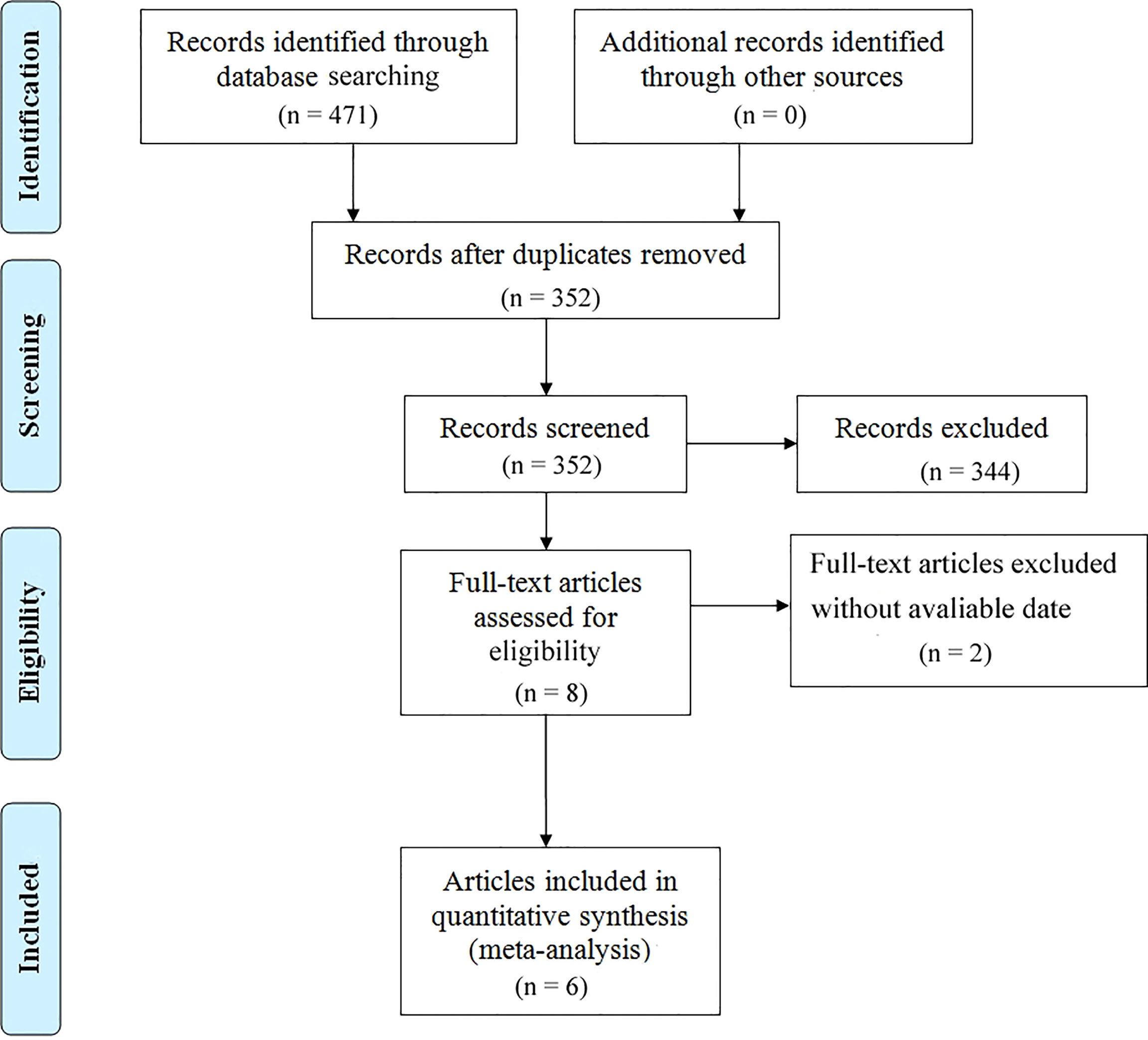
Figure 1 Flow chart of the meta-analysis.
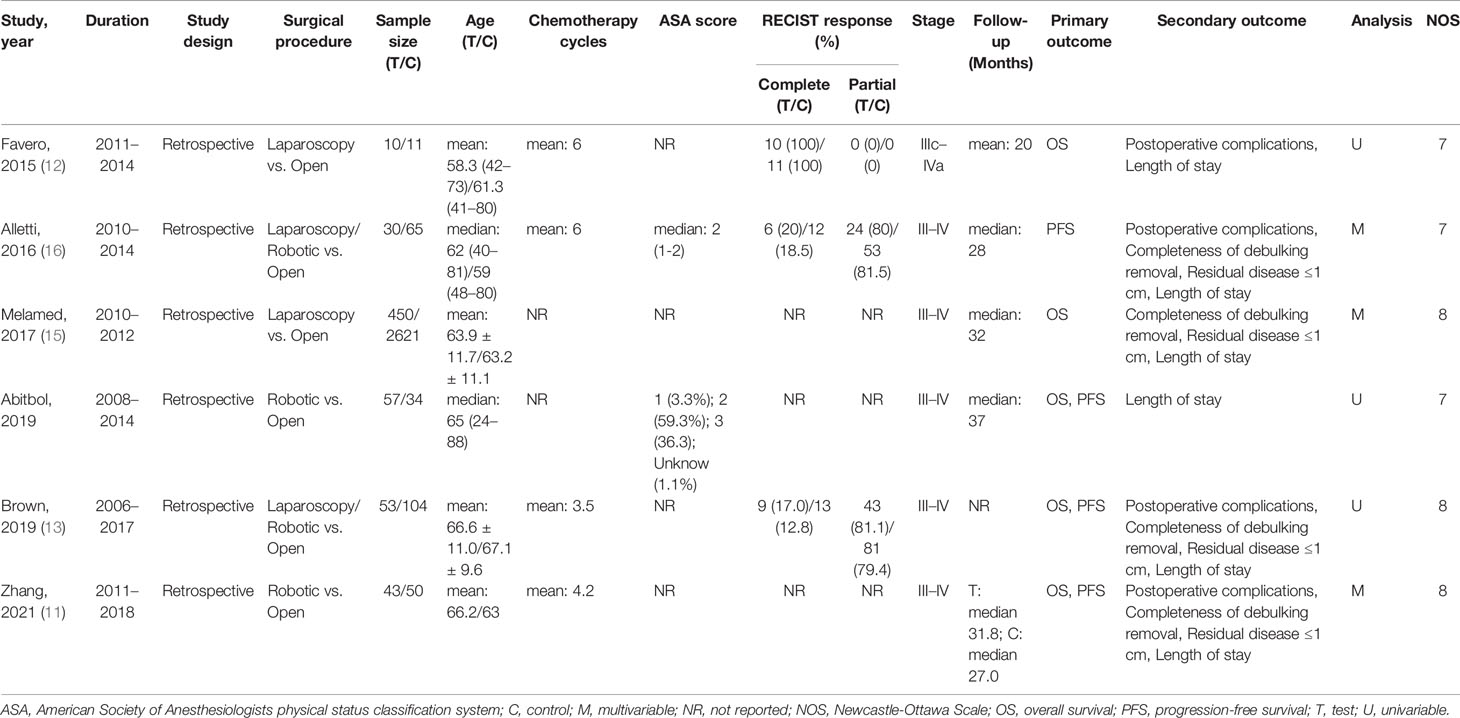
Table 1 Characteristics of studies included in this meta-analysis.
The OS of patients with OC who were treated with MIS versus laparotomy was examined in five studies. It was found that heterogeneity is substantial (P = 0.051, I2 = 57.6%), so a random-effect model was used. No significant differences in OS were found between patients with OC in the laparotomy group and the MIS group (HR = 0.85, 95% CI = 0.59 to 1.23) (Figure 2). In addition, PFS of patients with OC treated with MIS versus open laparotomy was examined in four studies. The fixed-effect model was adopted to examine the pooled findings due to the non-significant heterogeneity (P = 0.276, I2 = 22.4%). In patients with OC after NACT, the MIS group significantly enhanced PFS, compared with the open laparotomy group (HR = 0.73, 95% CI = 0.57 to 0.92) (Figure 3).
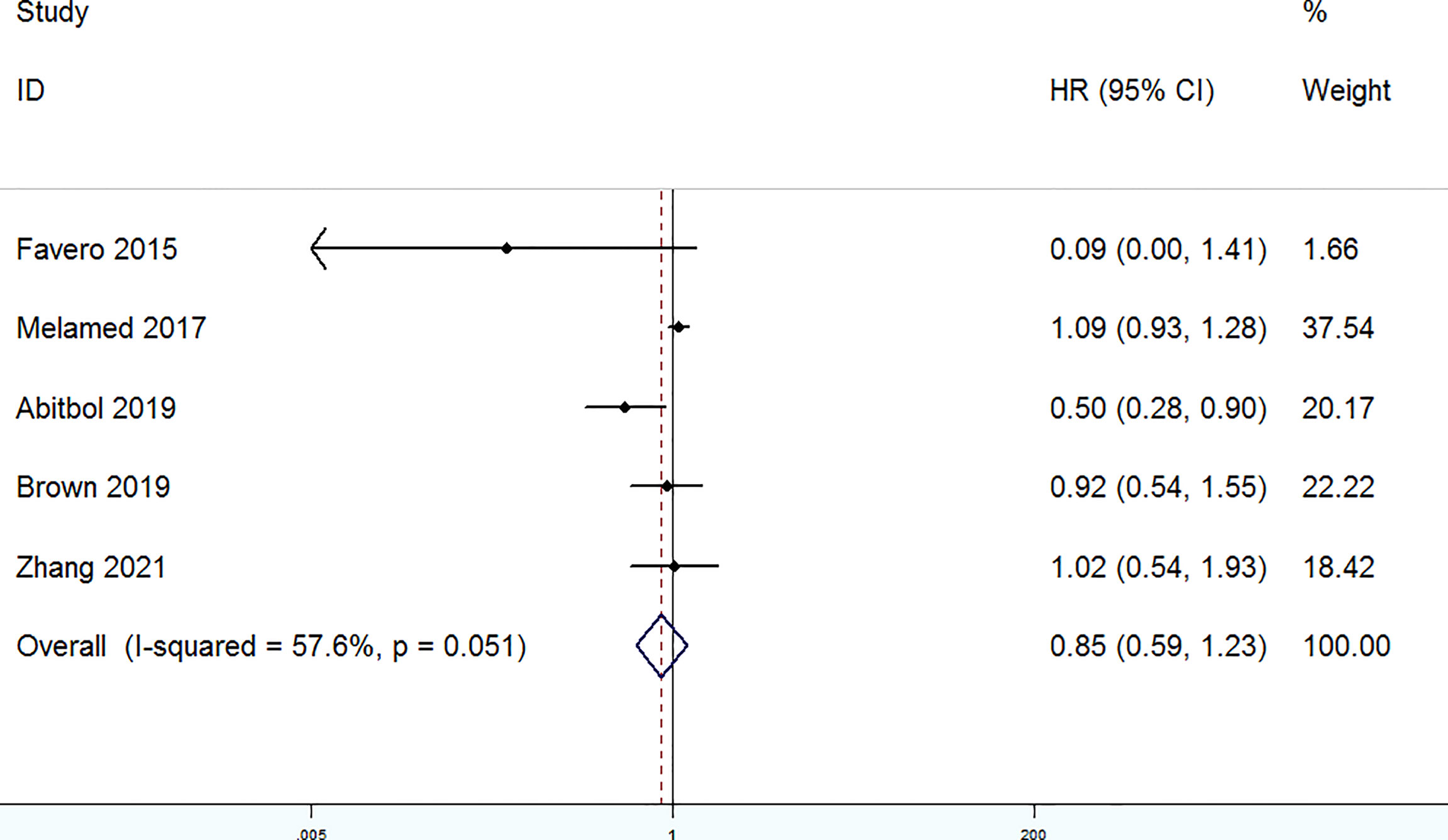
Figure 2 Forest plots for overall survival (OS).
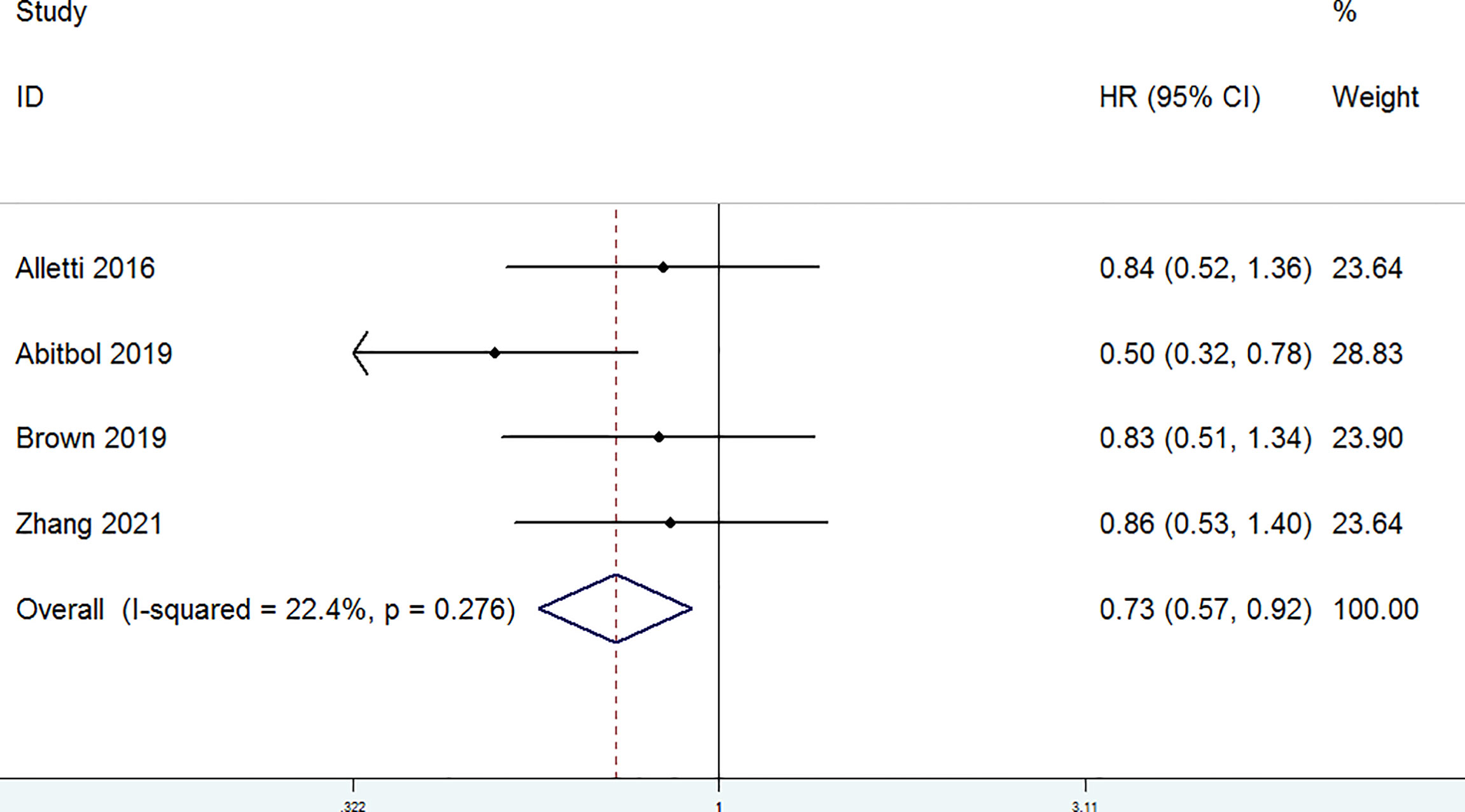
Figure 3 Forest plots for progression-free survival (PFS).
The completeness of debulking removal (R0) of patients with OC treated with MIS versus open laparotomy was examined in four studies. The random-effect model was selected for the significant heterogeneity (P = 0.098, I2 = 52.3%). There were no significant differences in the R0 rate between patients with OC in the laparotomy group and the MIS group (RR = 1.07, 95% CI = 0.93 to 1.23) (Figure 4). Residual disease ≤ 1 cm (R1) was evaluated in four studies. A fixed-effect model was adopted for the non-significant heterogeneity (P = 0.33, I2 = 12.6%). According to the combined data (RR = 1.08, 95% CI = 0.91 to 1.28), R1 was similar in the MIS group and the laparotomy group (Figure 5). Furthermore, postoperative complications were assessed in four studies. A random-effect model was adopted (P = 0.055, I2 = 60.6%), and no significant differences in the incidence of postoperative complications were detected between the MIS group and the open laparotomy group (RR = 0.72, 95% CI = 0.34 to 1.54) (Figure 6). All the studies reported the length of stays in hospital. The length of stays in hospital was significantly shorter in patients with OC treated with MIS than those treated with open laparotomy (SMD = −1.21, 95% CI = −1.78 to −0.64; heterogeneity: P < 0.001, I2 = 92.7%) with random-effect model (Figure 7).

Figure 4 Forest plots for completeness of debulking removal (R0).
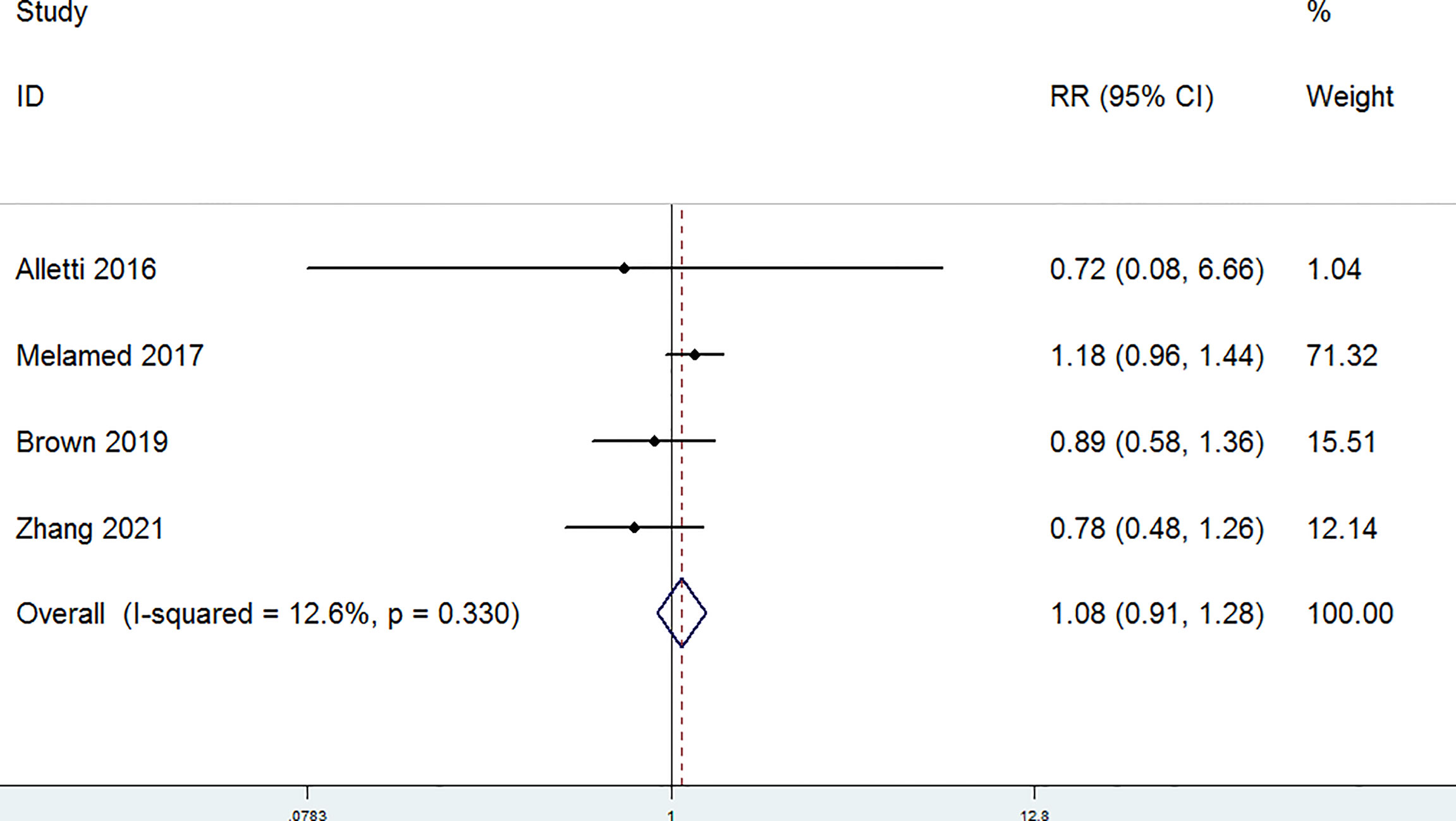
Figure 5 Forest plots for residual disease ≤1 cm (R1).
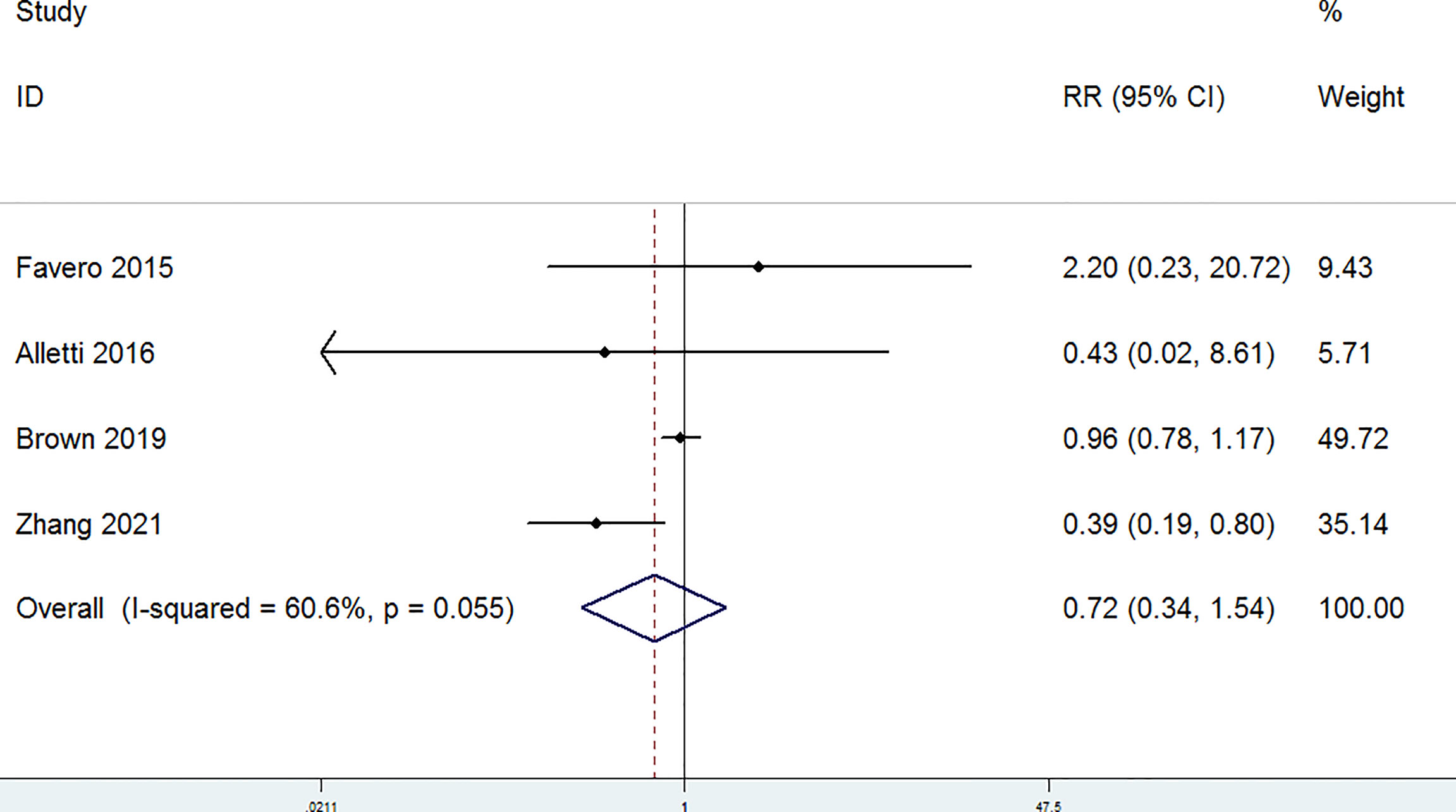
Figure 6 Forest plots for postoperative complications.
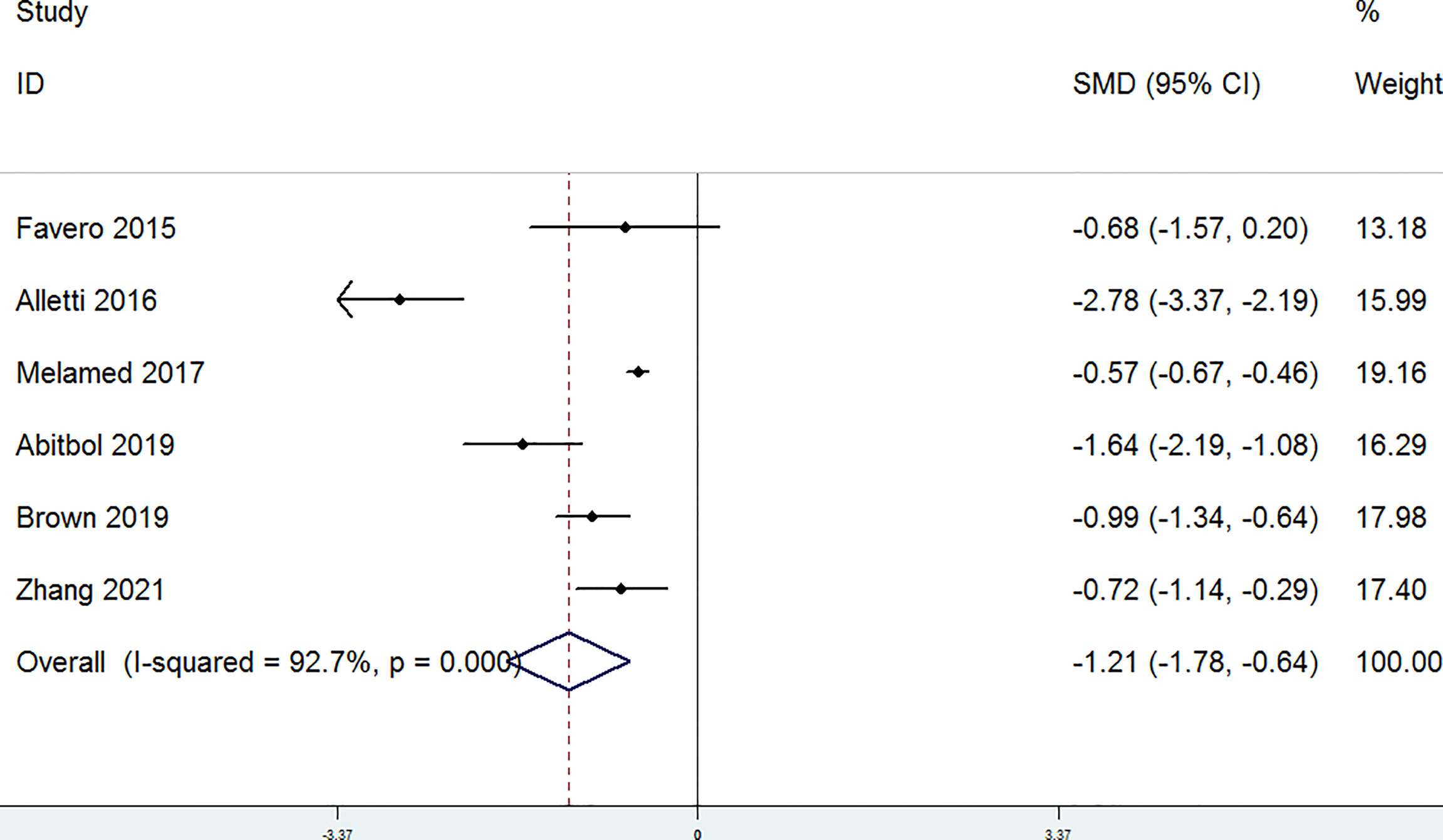
Figure 7 Forest plots for the length of stays in hospital.
As displayed in Supplementary Figures 1, 2, Begg’s funnel plot indicated that both the OS (P = 0.103) and PFS (P = 0.089) did not have publication bias. Sensitivity analysis was performed by removing one study each time and assessing the influence of the remaining pooled data on the overall results. No significant changes were observed in the remaining pooled data, which suggested that our results were robust (Supplementary Figures 3, 4).
In the present study, six studies, with 643 patients in the MIS group and 2,885 patients in the open laparotomy group, were analyzed to assess the efficacy and safety between MIS and laparotomy in IDS after NACT in patients with advanced OC. Our findings indicated that the MIS group seemed to have a better PFS than that in the open laparotomy group in patients with advanced OC, whereas no significant differences were detected in OS, completeness of debulking removal, residual disease of ≤1 cm, and postoperative complications between the two groups. Furthermore, the length of stays in hospital was significantly shorter in patients with OC who were treated with MIS than those treated with laparotomy. To our best knowledge, this was the most recent study with the largest sample size that compared the therapeutic benefits between MIS and laparotomy in patients with OC following NACT.
Although PDS was the standard treatment strategy for advanced OC, the application of NACT and IDS has increased substantially in the United States (22). It has been validated that MIS is a safe, technically practical, and appropriate procedure, as long as the optimal cytoreduction can be accomplished, not only in the case of pelvic diseases but also in the case of upper abdominal diseases (14, 16, 23). The last guideline recommends NACT and IDS for advanced patients with OC with high risk of perioperative M/M or low likelihood of attaining optimum cytoreduction at the PDS (10). In the last decade, MIS for IDS has gradually become an appealing alternative to traditional laparotomy among elderly and infirmed patients who were assessed and selected for neoadjuvant therapy. At present, assessing the feasibility of MIS for IDS after NACT have been reported in several studies (12–14, 24), but the results still remain controversial. Joel et al., for the first time, analyzed the therapeutic value of MIS and open laparotomy for IDS in patients with OC after NACT through the meta-analysis, in which the results showed that MIS appears to be a feasible and safe procedure for complete cytoreductive surgery in selected advanced patients with OC with NACT (25).
In the current study, it was also found that MIS had comparable feasibility with laparotomy for debulking OC after NACT with regarding to the OS, completeness of debulking removal, residual disease lesions, and postoperative complications, which was consistent with the previous study (11–16). At the Society of Gynecologic Oncology (SGO) conference in 2021, a retrospective study compared the surgical and tumor outcomes of MIS and open surgery in patients with advanced EOC who underwent IDS after NACT, and the results showed that MIS was a feasible and effective procedure of IDS after NACT in patients with advanced EOC (26). The proportion of reaching R0 (66% vs. 46%, P < 0.001) and optimal tumor cell reduction (93% vs. 84%, P = 0.02) was higher in MIS group. The 24-month PFS was higher in the MIS group (40% vs. 30%, P = 0.06). In addition, the ongoing prospective LANCE study would include 549 patients (27). The main purpose was to compare the PFS of MIS in IDS surgery with that in laparotomy.
Unexpectedly, our study revealed that MIS seemed to be linked with a better survival than laparotomy in patients with OC after NACT from the pooled HR for PFS. However, the sensitivity analysis showed that the PFS superiority effect was mitigated and even disappeared after removing the study of Abitbol et al. (14). In addition, almost all HRs and 95% CIs in the included study were extracted from the survival curve, which did not account for the confounding mediators between the two groups. The differences in the study design, the duration of median follow-up, and the differences in surgical techniques among gynecological oncologists do not allow to draw definitive conclusions regarding survival. For example, Alletti et al. showed that the Time to Chemo (TTC) and bevacizumab administration played independent prognostic role for PFS based on multivariable analysis, and thus, the PFS superiority effect should not erroneously ascribed to the MIS procedure only (16). On the other hand, the shorter TTC related to MIS might suggest a potential prognostic benefit of the procedure, because it ensured that the dose intensity of NACT regimens is properly maintained. In our study, there were no significant differences in NACT response between the MIS group and the laparotomy group in the original studies. Patients’ characteristics were similar among the studies. The number of neoadjuvant chemotherapy ranged from three to six cycles, and three studies reported at least a partial response before cytoreductive surgery. Because of the insufficient report on chemical cycles, ASA score, RECIST response, and other data, no detailed statistical analysis was conducted on these data. In fact, the purpose of this study was not to compare but to explore the security and effectiveness of IDS through MIS in advanced OC after NACT. Our meta-analysis suggested that MIS for IDS is feasible and safe for selecting advanced patients with OC (for partial response or complete response after NACT, optimal cytoreduction can be accomplished). This is consistent with the study on an important international multicenter experience published by Fagotti et al. They found that, for patients with AOC after NACT, MIS can be considered when the operation is limited to low complexity standard cytoreductive surgery. Meanwhile, MIS is associated with R0 recovery rate of 96%, and the median PFS and OS reported in this series seem reassuring (28). The SGO meeting in 2021 also reported the effects of laparoscopic prediction of minimally invasive IDS for advanced OC (MIID-SOC Test) with a clinical model, which calculated the total predictive index score (PIV) according to the location of pelvic and peritoneal lesions. The study showed that, when the PIV is less than 2, patients may achieve the best effects of minimally invasive IDS (29). However, whether this clinical prediction model can be used in clinical practice still needs to be verified by randomized controlled trials. Therefore, in this context, the finding of a better PFS in patients treated with MIS needs to be further clarified with large-scale randomized clinical trial with respect to standard laparotomy.
The secondary outcomes of the study proved that the length of stays in hospital was significantly shorter in patients with OC who were treated with MIS than those treated with laparotomy. In addition, although MIS did not reach a statistical significance, it had a trend to reduce postoperative complications, including bleeding, fever, infection, cardiac complications, ileus, lymphocyst formation, urinary retention, and wound complications (11–13, 30). This phenomenon might be explained as the following reasons: (1) small sample size; (2) heterogeneous literature; and (3) hynecologists have different surgical techniques.
Some limitations in our meta-analysis should be noted. First, the limited included studies had relatively small sample sizes. Second, the heterogeneity of study design, surgical procedure, and chemotherapy regimen in the included studies might result in potential biases. Third, only English-language published literature studies were included, which may lead to missing data. Fourth, there are insufficient data to evaluate the chemotherapy response, chemical cycles, and ASA score. Fifth, our literature only confirmed the results of current literature studies and provided another option for traditional IDS. This study did not add specific value to the scientific knowledge about the role of MIS in IDS.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: PubMed, Embase, and the Cochrane Library.
SZ, Conceptualization, Methodology, Data curation, Writing- Original draft preparation, Visualization, Software, investigation, writing - review and editing. YY, YC, BL and ZL conceptualization, investigation, ,writing-review and editing. LL and XJ, final approval of the version, writing- review and editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.900256/full#supplementary-material
Supplementary Figure 1 | Publication bias detected by Begg’s funnel plots for OS.
Supplementary Figure 2 | Publication bias detected by Begg’s funnel plots for PFS.
Supplementary Figure 3 | Sensitivity analysis for the meta-analysis (OS).
Supplementary Figure 4 | Sensitivity analysis for the meta-analysis (PFS).
1. Kurman RJ, Carcangiu ML, Herrington CS, Young RH. WHO Classification of Tumours of Female Reproductive Organs. (2014). Lyon: IARC Publications.
2. Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2020. CA: A Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: Cancer J Clin (2018) 68:394–424. doi: 10.3322/caac.21492
4. Wright AA, Bohlke K, Armstrong DK, Bookman MA, Cliby WA, Coleman RL, et al. Neoadjuvant Chemotherapy for Newly Diagnosed, Advanced Ovarian Cancer: Society of Gynecologic Oncology and American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol Off J Am Soc Clin Oncol (2016) 143:3–15. doi: 10.1016/j.ygyno.2016.05.022
5. Dungan JS. Neoadjuvant Chemotherapy or Primary Surgery in Stage Iiic or Iv Ovarian Cancer. Yearbook Obstet (2011) 2011:507–8. doi: 10.1016/j.yobg.2011.05.172
6. Onda T, Satoh T, Saito T, Kasamatsu T, Nakanishi T, Nakamura K, et al. Comparison of Treatment Invasiveness Between Upfront Debulking Surgery Versus Interval Debulking Surgery Following Neoadjuvant Chemotherapy for Stage III/IV Ovarian, Tubal, and Peritoneal Cancers in a Phase III Randomised Trial: Japan Clinical Oncology Group Study Jcog0602. Eur J Cancer (Oxford Engl 1990) (2016) 64:22–31. doi: 10.1016/j.ejca.2016.05.017
7. Armstrong DK, Alvarez RD, Bakkum-Gamez JN, Barroilhet L, Behbakht K, Berchuck A, et al. Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Network: JNCCN (2021) 19(2):191–226. doi: 10.6004/jnccn.2021.0007
8. Corrado G, Mancini E, Cutillo G, Baiocco E, Vizza E. Laparoscopic Debulking Surgery in the Management of Advanced Ovarian Cancer After Neoadjuvant Chemotherapy. Int J Gynecol Cancer (2015) 25(7):1253. doi: 10.1097/IGC.0000000000000491
9. Alletti SG, Bottoni C, Fanfani F, Gallotta V, Fagotti A. Minimally Invasive Interval Debulking Surgery in Ovarian Neoplasm (Mission Trial - Nct02324595): A Feasibility Study. Am J Obstet Gynecol (2015) 214(4):1340–1. doi: 10.1016/j.ajog.2015.10.922
10. National Comprehensive Cancer Networks. Practice Guidelines in Oncology: Ovarian Cancer (2022). Available at: https://www.nccn.org/patients.Version1.
11. Zhang Y, Grant MS, Zhang X, Paraghamian SE, Clark LH. Comparing Laparotomy With Robot-Assisted Interval Debulking Surgery for Patients With Advanced Epithelial Ovarian Cancer Receiving Neoadjuvant Chemotherapy. J Minimally Invasive Gynecol (2020) 28(6):1237–43. doi: 10.1016/j.jmig.2020.11.015
12. Favero G, Macerox N, Pfiffer T, Köhler C, da Costa Miranda V, Estevez Diz Mdel P, et al. Oncologic Concerns Regarding Laparoscopic Cytoreductive Surgery in Patients With Advanced Ovarian Cancer Submitted to Neoadjuvant Chemotherapy. Oncology (2015) 89(3):159–16. doi: 10.1159/000381462
13. Brown J, Drury L, Crane EK, Anderson WE, Tait DL, Higgins RV, et al. When Less is More: Minimally Invasive Surgery Compared With Laparotomy for Interval Debulking After Neoadjuvant Chemotherapy in Women With Advanced Ovarian Cancer. J Minimally Invasive Gynecol (2018) 26:902–9. doi: 10.1016/j.jmig.2018.09.765
14. Abitbol J, Gotlieb W, Zeng Z, Ramanakumar A, Kessous R, Kogan L, et alIncorporating Robotic Surgery Into the Management of Ovarian Cancer After Neoadjuvant Chemotherapy. Int J Gynecol Cancer (2019) 29(9):1341–7. doi: 10.1136/ijgc-2019-000413
15. Melamed A, Rauh-Hain J. Laparoscopy Compared With Laparotomy for Debulking Ovarian Cancer After Neoadjuvant Chemotherapy Reply. Obstet Gynecol J Am Coll Obstet Gynecol (2017) 129:861–9. doi: 10.1097/AOG.0000000000001851
16. Alletti SG, Petrillo M, Vizzielli G, Bottoni C, Nardelli F, Costantini B, et al. Minimally Invasive Versus Standard Laparotomic Interval Debulking Surgery in Ovarian Neoplasm: A Single-Institution Retrospective Case-Control Study. Gynecol Oncol (2016) 516:516–20. doi: 10.1016/j.ygyno.2016.10.017
17. Ditto A, Bogani G, Martinelli F, Signorelli M, Chiappa V, Scaffa C, et al. Minimally Invasive Surgical Staging for Ovarian Carcinoma: A Propensity-Matched Comparison With Traditional Open Surgery. J Minimally Invasive Gynecol (2016) 98:98–102. doi: 10.1016/j.jmig.2016.09.018
18. Gouy S, Belghiti J, Uzan C, Canlorbe G, Gauthier T, Morice P. Accuracy and Reproducibility of the Peritoneal Cancer Index in Advanced Ovarian Cancer During Laparoscopy and Laparotomy. Int J Gynecol Cancer (2013) 23(9):1699–703. doi: 10.1097/IGC.0b013e3182a616a7
19. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement (Reprinted From Annals of Internal Medicine). Phys Ther (2009) 89(9):873–80. doi: 10.1093/ptj/89.9.873
20. Stang A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
21. Parmar MK, Torri V, Stewart L. Extracting Summary Statistics to Perform Meta-Analyses of the Published Literature for Survival Endpoints. Stat Med (1998) 17(24):2815–34. doi: 10.1002/(SICI)1097-0258(19981230)17:24<2815::AID-SIM110>3.0.CO;2-8
22. Melamed A, Hinchcliff EM, Clemmer JT, Bregar AJ, Uppal S, Bostock I, et al. Trends in the Use of Neoadjuvant Chemotherapy for Advanced Ovarian Cancer in the United States. Gynecol Oncol (2016) 143:236–40. doi: 10.1016/j.ygyno.2016.09.002
23. Tozzi R, Majd HS, Campanile RG, Ferrari F. Feasibility of Laparoscopic Diaphragmatic Peritonectomy During Visceral-Peritoneal Debulking (Vpd) in Patients With Stage Iiic-Iv Ovarian Cancer. J Gynecol Oncol (2020) 31(5):1–12. doi: 10.3802/jgo.2020.31.e71
24. Ceccaroni M, Roviglione G, Bruni F, Clarizia R, Ruffo G, Salgarello M, et al. Laparoscopy for Primary Cytoreduction With Multivisceral Resections in Advanced Ovarian Cancer: Prospective Validation. "the Times They are a-Changin"? Surg Endoscopy Other Interventional Techniques (2017). doi: 10.1007/s00464-017-5899-9
25. Joel CG, Wang Y, Susan MG, Saleem MD, Carbajal M, Pomputius AF, et al. Minimally Invasive Interval Cytoreductive Surgery in Ovarian Cancer: Systematic Review and Meta-Analysis. J Robotic Surg (2018) 13(1):1–11. DOI: 10.1007/s11701-018-0838-x
26. Brown J, Barr A, Zhang Y, Davidson B, Secord AA, Drury L, et al. A Multi-Institutional Study of Minimally Invasive Surgery Compared to Laparotomy for Interval Debulking After Neoadjuvant Chemotherapy in Women With Advanced Ovarian Cancer. Gynecol Oncol (2021) 162:S20. doi: 10.1016/S0090-8258(21)00684-3
27. Nitecki R, Rauh-Hain JA, Melamed A, Scambia G, Fagotti A. Laparoscopic Cytoreduction After Neoadjuvant Chemotherapy (Lance). Int J Gynecol Cancer (2020) 30(9):1450–4. doi: 10.1136/ijgc-2020-001584
28. Fagotti A, Alletti SG, Corrado G, Cola E, Scambia G. The International Mission Study: Minimally Invasive Surgery in Ovarian Neoplasms After Neoadjuvant Chemotherapy. Int J Gynecol Cancer (2019) 29(1):5–9. doi: 10.1136/ijgc-2018-000012
29. Costales A, Crane E, Chambers L, Debernardo R, Ricci S, Rose P, et al. Laparoscopic Predictability of Minimally Invasive Interval Debulking in Advanced Ovarian Cancer: The Miid-Soc Trial. Gynecol Oncol (2021) 162:19–20. doi: 10.1016/S0090-8258(21)00683-1
Keywords: Advanced ovarian cancer (AOC), neo-adjuvant chemotherapy (NACT), minimally invasive surgery (MIS), laparotomy, interval debulking surgery (IDS)
Citation: Zeng S, Yu Y, Cui Y, Liu B, Jin X, Li Z and Liu L (2022) Efficacy and Safety of Minimally Invasive Surgery Versus Open Laparotomy for Interval Debulking Surgery of Advanced Ovarian Cancer After Neoadjuvant Chemotherapy: A Systematic Review and A Meta-Analysis. Front. Oncol. 12:900256. doi: 10.3389/fonc.2022.900256
Received: 20 March 2022; Accepted: 22 June 2022;
Published: 18 July 2022.
Edited by:
Valerio Gallotta, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Federico Ferrari, University of Brescia, ItalyCopyright © 2022 Zeng, Yu, Cui, Liu, Jin, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lifeng Liu, bGl1bGlmZW5nMjAwOEBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.