 Tomas Buchler
Tomas Buchler
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 28 April 2022
Sec. Cancer Genetics
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.888181
This article is part of the Research Topic Current Understanding of Genomic and Chromosomal Instabilities in Solid Malignancies View all 9 articles
Approximately 4-5% of patients with metastatic colorectal cancer (mCRC) have mismatch repair deficient (dMMR)/microsatellite instability-high (MSI-H) tumours. These tumours present challenges in the clinical practice due to variant response to fluoropyrimidine-based chemotherapy and, perhaps, also non-immunologic targeted therapies. Recently, a breakthrough in the treatment of dMMR/MSI-H mCRC has been achieved with several clinical trials showing dramatic long-term benefit of immunotherapy using checkpoint inhibitors. Nevertheless, several questions remain regarding the optimisation of immunotherapy regimens and the use of biomarkers to identify populations set to derive the greatest benefit from immunotherapy. Combination regimens and/or the use of immunotherapy as a maintenance after induction non-immunologic systemic therapy may be the way forward to improve outcomes.
Colorectal cancer (CRC) is one of the main causes of morbidity and mortality, representing approximately 10% of all cancers diagnosed worldwide (1). Mismatch repair deficient (dMMR)/microsatellite instability-high (MSI-H) colorectal tumours are identified in approximately 15% of CRC patients. Due to relatively favourable prognosis in comparison to the mismatch repair proficient (pMMR) CRC, the proportion of these tumours decreases to approximately 4-5% in patients with metastatic CRC (mCRC) (2).
Deficiency in protein products of MSH2, MLH1 and MSH6 genes results in impaired detection of mismatched and unpaired bases, leading to the expression of abnormal proteins that may be recognized as neoantigens by the immune system. Additionally, most likely due to Darwinian selection pressure, the deficiency causes failure of apoptosis upon detection of critical DNA damage (2, 3).
dMMR/MSI-H status has been associated with the lack of benefit from fluoropyrimidines in stage II and III CRC (4–6). Nevertheless, the benefit from oxaliplatin-containing regimens remains unchanged making them the standard of care in patients with CRC requiring adjuvant chemotherapy (6–8). In mCRC the prognosis and response to chemotherapy in patients with dMMR/MSI-H tumours is significantly influenced by the presence of somatic BRAF mutations which are associated with poor prognosis (9, 10). BRAF V600E mutations are causally linked to MLH1 promoter hypermethylation leading to deficiency in MLH1 and PMS2 proteins, the most common cause of dMMR/MSI-H phenotype in patients without Lynch syndrome (11–13).
Monoclonal antibodies against the vascular endothelial growth factor (VEGF) or, in patients with KRAS/NRAS wild-type tumours, against the epidermal growth factor receptor (EGFR) are commonly added to chemotherapy in mCRC. dMMR/MSI-H patients receiving the VEGF antagonist bevacizumab achieved longer overall survival (OS) compared to patients treated with the EGFR inhibitor cetuximab in the CALGB/SWOG 80405 clinical trial (14). Similar findings were recently reported in a retrospective study (15).
Due to the abundance and diversity of neoantigens generated in the absence of functional mismatch repair, immunotherapy using antagonists of the programmed death-1 (PD-1) receptor or its ligand PD-L1), with or without antagonists of the CTLA4 receptor, is an attractive option for patients with dMMR/MSI-H tumours. The pivotal phase 2 study establishing the efficacy of immunotherapy for dMMR/MSI-H tumours was published in 2015 by Le and collaborators and included 10 evaluable patients with colorectal cancer (16). Pembrolizumab was given at a dose of 10 mg/kg biweekly. At 20 weeks, the progression-free survival (PFS) rate in these patients was 78%. The overall response rate (ORR) reached 40% while no responses were seen in patients with pMMR mCRC. In an expanded cohort of 40 patients with mCRC, 2-year PFS and OS were 59 months (95% CI 44 ‐ 78 months) and 72 months respectively (95% confidence interval [CI] 58 ‐ 89 months). Five patients (12%) achieved complete responses (17).
CheckMate-142, a nonrandomised multiple cohort phase 2 study, enrolled patients with MSI-H/dMMR as well as pMMR colorectal cancer (18–20). The study comprised several treatment arms including nivolumab monotherapy, nivolumab with ipilimumab, nivolumab with ipilimumab plus cobimetinib (a MEK inhibitor), nivolumab plus relatlimab (a monoclonal antibody against lymphocyte activation gene-3), and nivolumab with daratumumab (a monoclonal antibody against CD38). Data from three cohorts enrolling patients with MSI-H/dMMR mCRC have been published so far.
The first reported cohort included 74 patients with previously treated mCRC (20). However, only 53 of these patients had centrally confirmed dMMR/MSI-H status. The treatment consisted of nivolumab 3 mg/kg every 2 weeks. In the population of 74 patients, PFS at 12 months was 50·4% (95% CI 38·1%–61·4%) and OS was 73·4% (95% CI 61·5%–82·1%). For the subgroups with BRAF mutation, KRAS mutation, and BRAFwt/KRASwt, the ORR was 41.4%, 26.9%, and 25.5%, respectively. The disease control rate was similar in patients with BRAF mutation and BRAFwt/KRASwt, but lower for patients with KRAS mutated tumours (20).
In another cohort of pre-treated patients, patients received nivolumab 3 mg/kg and ipilimumab 1 mg/kg every 3 weeks for four doses followed by biweekly nivolumab 3 mg/kg (18, 19). The majority of patients (76%) had received two or more previous systemic therapies. BRAF mutation was present in 25% and KRAS mutation in 37% of patients’ tumours. According to 4-year follow-up data, the overall response rate (ORR) reached 65%, with 13% of patients achieving complete response. The ORR was similar in patients with BRAFwt/KRASwt tumours and patients with tumours harbouring either mutation. As many as 53% of patients (95% CI 43-62%) were free of progression at 48 months. The OS rate at 48 months was excellent reaching 70.5% (95% CI 61.4-77.9%), far surpassing the expected results for conventional therapy where median OS would fluctuate around 19 months (10).
Finally, results of the cohort receiving nivolumab with ipilimumab as the first-line therapy were published recently (21). Here, 45 patients without previous systemic therapy for mCRC were treated with another combination regimen consisting of nivolumab 3 mg/kg once every 2 weeks and ipilimumab 1 mg/kg once every six weeks until progression or unacceptable toxicity. Interestingly, the 24-month PFS rate was higher for patients with KRAS mutated tumours compared to BRAFwt/KRASwt tumours, reaching 87.5% (95% CI, 38.7 to 98.1) and 68.4% (95% CI, 35.9 to 86.8), respectively. The 24-month OS rate was 79.4% (95% CI, 64.1 to 88.7).
KEYNOTE-177 is an ongoing open-label randomised multicentric phase 3 trial for patients without previous systemic treatment for mCRC (22, 23). So far, 307 patients with dMMR/MSI-H mCRC have been randomised to either pembrolizumab (200mg in 3-weekly cycle for a maximum of 35 cycles) or fluoropyrimidine-based chemotherapy with or without non-immunologic targeted agents including bevacizumab or cetuximab. Crossover was allowed for patients in the chemotherapy arm following disease progression. Treatment in the control arm consisted mostly of mFOLFOX6 with bevacizumab (44.8%) or FOLFIRI with bevacizumab (25.2%). Only 11.2% of control arm patients received first-line cetuximab with backbone chemotherapy.
Two-thirds of patients enrolled in the KEYNOTE -177 study had right-sided tumours. As expected, the proportion of patients with BRAF V600E mutation in the dMMR/MSI-H population was high (28.1% in the pembrolizumab arm). Unfortunately, molecular analysis data for KRAS/NRAS and BRAF V600E were not available for 23.8% patients in the study. The median PFS reached 16 months for patients allocated to pembrolizumab (95% CI 5.4-38.1 months) compared to 8.2 months in patients on chemotherapy (95% CI 6.1-10.2 months). The PFS curve seemed to plateau approximately 6 months after the treatment start and about 40% of patients experienced long-term responses. According to a subgroup analysis, patients over 70 years of age did not seem to derive as large benefit from immunotherapy as did younger patients. Of note, patients with KRAS/NRAS mutated tumours had numerically superior survival if allocated to the control arm. On the other hand, PFS benefit of immunotherapy was nearly identical for patients with BRAF wild-type tumours and those with BRAF V600E tumours, although arguably, the control arm regimens were inadequate for this subpopulation and a triplet chemotherapy with bevacizumab should be more effective (24).
The response rate was higher in the pembrolizumab arm with 13.1% patients reaching complete response. Furthermore, responses were long-lasting in the immunotherapy arm with 83.5% of responses ongoing at 24 months.
The final survival analysis was presented at the 2021 American Society of Clinical Oncology (23). OS at 36 months was 61% in the pembrolizumab arm compared to 50% in the control arm (95% hazard ratio [HR] 0.74, 95% CI 0.53-1.03). There was, however, a massive crossover with 60.4% of patients from the control arm eventually receiving anti-PD-1/PD-L1 therapies, and some additional individuals receiving other checkpoint inhibitors (23).
The marked difference in the proportion of dMMR/MSI-H tumours between early and advanced CRC stages points to a strong role of immunoediting in the progression of these tumours. The activation of immunosuppressive pathways linked to PD-1 and CTLA4 protects these tumours from destruction by the immune system and could explain the high efficacy of checkpoint inhibitors in this setting (25). However, only 40-50% of patients with dMMR/MSI-H mCRC derive long-term benefit from the treatment. Possible mechanisms of intrinsic and acquired resistance have been comprehensively reviewed by Sahin et al. (26).
PD-L1 expression was not correlated with benefit from immunotherapy in patients with dMMR/MSI-H mCRC or in the tumour-agnostic trial by Le et al. (16, 18, 19).
The efficacy of checkpoint inhibitors in dMMR/MSI-H patients was not associated with BRAF V600E mutation which is present in approximately 30-40% of dMMR/MSI-H mCRC (19, 23). On the other hand, the apparent lower efficacy of immunotherapy in patients with KRAS/NRAS mutated tumours treated with anti-PD-1 monotherapy in the KEYNOTE -177 and CheckMate-142 studies, contrasted with a preserved benefit of combined immunotherapy in CheckMate-142, deserved further study as the subgroups were too small for a valid conclusion (19–21, 23).
Tumour mutation burden (TMB) was a better biomarker for the efficacy of immunotherapy than the absence of an MMR-related protein. It directly correlated with the number of neoantigens (27). Although the great majority of dMMR/MSI-H tumours had high TMB, some dMMR/MSI-H tumours with low TMB have been identified, and they exhibited resistance to therapy with checkpoint inhibitors (28, 29).
Salem et al. compared the TMB according to the type of MMR deficiency. In a heterogeneous cohort of cancers, the largest subgroups comprised endometrial and colorectal tumours. The loss of MSH2/MSH6 was associated with approximately double rate of mutations compared to loss of MLH1/PMS2 (30).
Approximately 3% of colorectal tumours classified as microsatellite stable (MSS) have high TMB, mostly associated with the mutation of polymerase epsilon (POLE) or variant MSH2 (28, 31, 32). These mutations resulted in a high sensitivity to checkpoint inhibitors. Clinical trials enrolling patients with POLE-mutated mCRC along those with dMMR/MSI-H mCRC are ongoing (NCT03150706 and NCT03435107, Table 1).
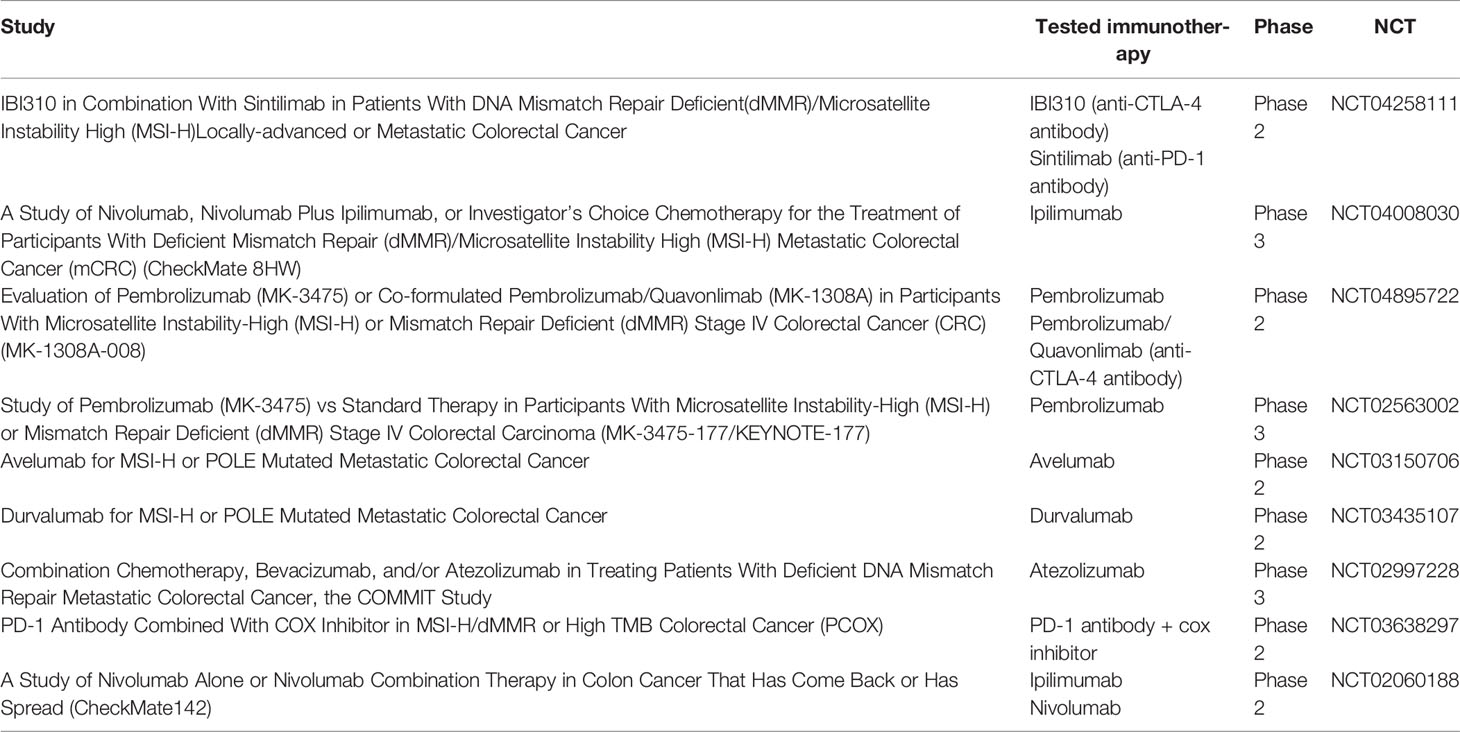
Table 1 Ongoing clinical trials for dMMR/MSI-H mCRC using immunotherapy.
There is growing evidence that the genomic instability in tumours with mismatch-repair deficiency may result in the formation of gene fusions. Cocco and collaborators found that potentially targetable fusions of oncogenes such as NTRK, BRAF, RET, FGFR, ROS1 and ALK were present in 5% of dMMR/MSI-H CRC as compared to only 0.4% of MSS CRC cases. Particular enrichment was seen in the subgroup of dMMR/MSI-H BRAFwt/RASwt CRC cases with MLH1 promoter hypermethylation where the occurrence of these aberrations was as high as 42% (13). Vaňkova et al. confirmed these findings identifying oncogenic gene fusions in as many as 9 of 23 colorectal tumours that were dMMR/MSI-H due to MLH1 promoter hypermethylation and simultaneously BRAFwt/KRASwt. The fusions involved NTRK, ALK and BRAF genes (33). These studies suggest that BRAFwt/KRASwt tumours with MLH1 promoter hypermethylation should also be tested for the presence of oncogene fusions.
It has been shown that dMMR-MSI-H colorectal cancer was associated with specific changes in gut microbiome. Fusobacterium nucleatum was enriched in dMMR/MSI-H CRC and associated with lower number of tumour-infiltrating lymphocytes while the opposite has been suggested for MSS colorectal cancer (34). However, somewhat counterintuitively, F. nucleatum has been found to be positively associated with response to checkpoint inhibitors, enhancing the expression of PD-1 and PD-L1 and activating the stimulator of interferon genes (STING) signalling (35). The activity of interferon-γ pathway was also associated with response in dMMR/MSI-H CRC in a recent transcriptomics study while VEGF-A expression characterised poor responders (36).
Other putative molecular markers of response to checkpoint inhibitors have been proposed, in particular β2-microglobulin mutations (37). Nevertheless, a recent study failed to corroborate their association with treatment outcomes (38).
Finally, peritoneal involvement manifesting with ascites is associated with resistance to immune checkpoint blockade in dMMR/MSI-H gastrointestinal cancers and markedly inferior patient outcomes, even compared to peritoneal disease without ascites (39).
The search for reliable predictors is ongoing and detailed reviews of potential biomarkers for immunotherapy of colorectal cancer are available (40, 41).
Immunotherapy is the preferred treatment option for dMMR/MSI-H CRC resulting in long-term treatment responses in approximately 40-50% of patients. As most non-responders will experience progression within 6-8 months of the treatment initiation, the obvious clinical strategies that have been successfully applied in other tumours with similar early treatment characteristics include the combinations of checkpoint inhibitors with chemotherapy and the use of checkpoint inhibitors as a maintenance therapy in non-progressing patients after the induction (42, 43) In both situations, inclusion of a VEGF-targeted therapy in the regimen appears beneficial. Multiple clinical trials are ongoing and our knowledge on the use of immunotherapy in this setting will keep expanding in the following years (Table 1).
TB has designed and written the manuscript. The author confirms being the sole contributor of this work and has approved it for publication.
The work was supported by grant TN-00064190 from the Ministry of Health, Czech Republic to the Thomayer University Hospital. Publication fee was covered by unrestricted grants from Servier, Roche, AstraZeneca, and Bristol Myers Squibb to the First Faculty of Medicine, Charles University, Prague, Czech Republic. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
TB received research support and honoraria from Roche, Bristol Myers Squibb, Merck Sharp Dohme, Merck, and AstraZeneca, all unrelated to the present paper.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The author would like to thank Dr Alena Novakova for critical reading of the manuscript and helpful comments.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Sinicrope FA, Sargent DJ. Molecular Pathways: Microsatellite Instability in Colorectal Cancer: Prognostic, Predictive, and Therapeutic Implications. Clin Cancer Res an Off J Am Assoc Cancer Res (2012) 18(6):1506–12. doi: 10.1158/1078-0432.CCR-11-1469
3. Vodenkova S, Buchler T, Cervena K, Veskrnova V, Vodicka P, Vymetalkova V. 5-Fluorouracil and Other Fluoropyrimidines in Colorectal Cancer: Past, Present and Future. Pharmacol Ther (2020) 206:107447. doi: 10.1016/j.pharmthera.2019.107447
4. Sargent DJ, Marsoni S, Monges G, Thibodeau SN, Labianca R, Hamilton SR, et al. Defective Mismatch Repair as a Predictive Marker for Lack of Efficacy of Fluorouracil-Based Adjuvant Therapy in Colon Cancer. J Clin Oncol Off J Am Soc Clin Oncol (2010) 28(20):3219–26. doi: 10.1200/JCO.2009.27.1825
5. Ribic CM, Sargent DJ, Moore MJ, Thibodeau SN, French AJ, Goldberg RM, et al. Tumor Microsatellite-Instability Status as a Predictor of Benefit From Fluorouracil-Based Adjuvant Chemotherapy for Colon Cancer. N Engl J Med (2003) 349(3):247–57. doi: 10.1056/NEJMoa022289
6. Cohen R, Taieb J, Fiskum J, Yothers G, Goldberg R, Yoshino T, et al. Microsatellite Instability in Patients With Stage III Colon Cancer Receiving Fluoropyrimidine With or Without Oxaliplatin: An ACCENT Pooled Analysis of 12 Adjuvant Trials. J Clin Oncol Off J Am Soc Clin Oncol (2021) 39(6):642–51. doi: 10.1200/JCO.20.01600
7. André T, de Gramont A, Vernerey D, Chibaudel B, Bonnetain F, Tijeras-Raballand A, et al. Adjuvant Fluorouracil, Leucovorin, and Oxaliplatin in Stage II to III Colon Cancer: Updated 10-Year Survival and Outcomes According to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(35):4176–87. doi: 10.1200/JCO.2015.63.4238
8. Gavin PG, Colangelo LH, Fumagalli D, Tanaka N, Remillard MY, Yothers G, et al. Mutation Profiling and Microsatellite Instability in Stage II and III Colon Cancer: An Assessment of Their Prognostic and Oxaliplatin Predictive Value. Clin Cancer Res an Off J Am Assoc Cancer Res (2012) 18(23):6531–41. doi: 10.1158/1078-0432.CCR-12-0605
9. Venderbosch S, Nagtegaal ID, Maughan TS, Smith CG, Cheadle JP, Fisher D, et al. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FOCUS Studies. Clin Cancer Res (2014) 20(20):5322–30. doi: 10.1158/1078-0432.CCR-14-0332
10. Shulman K, Barnett-Griness O, Friedman V, Greenson JK, Gruber SB, Lejbkowicz F, et al. Outcomes of Chemotherapy for Microsatellite Instable-High Metastatic Colorectal Cancers. JCO Precis Oncol (2018) 2:PO.17.00253. doi: 10.1200/PO.17.00253
11. Weisenberger DJ, Siegmund KD, Campan M, Young J, Long TI, Faasse MA, et al. CpG Island Methylator Phenotype Underlies Sporadic Microsatellite Instability and is Tightly Associated With BRAF Mutation in Colorectal Cancer. Nat Genet (2006) 38(7):787–93. doi: 10.1038/ng1834
12. Fang M, Ou J, Hutchinson L, Green MR. The BRAF Oncoprotein Functions Through the Transcriptional Repressor MAFG to Mediate The CpG Island Methylator Phenotype. Mol Cell (2014) 55(6):904–15. doi: 10.1016/j.molcel.2014.08.010
13. Cocco E, Benhamida J, Middha S, Zehir A, Mullaney K, Shia J, et al. Colorectal Carcinomas Containing Hypermethylated MLH1 Promoter and Wild-Type BRAF/KRAS Are Enriched for Targetable Kinase Fusions. Cancer Res (2019) 79(6):1047–53. doi: 10.1158/0008-5472.CAN-18-3126
14. Innocenti F, Ou F-S, Qu X, Zemla TJ, Niedzwiecki D, Tam R, et al. Mutational Analysis of Patients With Colorectal Cancer in CALGB/SWOG 80405 Identifies New Roles of Microsatellite Instability and Tumor Mutational Burden for Patient Outcome. J Clin Oncol Off J Am Soc Clin Oncol (2019) 37(14):1217–27. doi: 10.1200/JCO.18.01798
15. Tougeron D, Sueur B, Zaanan A, de la Fouchardiére C, Sefrioui D, Lecomte T, et al. Prognosis and Chemosensitivity of Deficient MMR Phenotype in Patients With Metastatic Colorectal Cancer: An AGEO Retrospective Multicenter Study. Int J Cancer (2020) 147(1):285–96. doi: 10.1002/ijc.32879
16. Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 Blockade in Tumors With Mismatch-Repair Deficiency. N Engl J Med (2015) 372(26):2509–20. doi: 10.1056/NEJMoa1500596
17. Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, et al. Mismatch Repair Deficiency Predicts Response of Solid Tumors to PD-1 Blockade. Science (2017) 357(6349):409–13. doi: 10.1126/science.aan6733
18. Overman MJ, Lonardi S, Wong KYM, Lenz H-J, Gelsomino F, Aglietta M, et al. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol Off J Am Soc Clin Oncol (2018) 36(8):773–9. doi: 10.1200/JCO.2017.76.9901
19. André T, Lonardi S, Wong K, Lenz H, Gelsomino F, Aglietta M, et al. SO-27 Nivolumab Plus Low-Dose Ipilimumab in Previously Treated Patients With Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: 4-Year Follow-Up From CheckMate 142. Ann Oncol (2021) 32:S213–4. doi: 10.1016/j.annonc.2021.05.051
20. Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in Patients With Metastatic DNA Mismatch Repair-Deficient or Microsatellite Instability-High Colorectal Cancer (CheckMate 142): An Open-Label, Multicentre, Phase 2 Study. Lancet Oncol (2017)18(9):1182–91. doi: 10.1016/S1470-2045(17)30422-9
21. Lenz H-J, Van Cutsem E, Luisa Limon M, Wong KYM, Hendlisz A, Aglietta M, et al. First-Line Nivolumab Plus Low-Dose Ipilimumab for Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: The Phase II CheckMate 142 Study. J Clin Oncol Off J Am Soc Clin Oncol (2022) 40(2):161–70. doi: 10.1200/JCO.21.01015
22. André T, Shiu K-K, Kim TW, Jensen BV, Jensen LH, Punt C, et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med (2020) 383(23):2207–18. doi: 10.1056/NEJMoa2017699
23. Andre T, Shiu K-K, Kim TW, Jensen BV, Jensen LH, Punt CJA, et al. Final Overall Survival for the Phase III KN177 Study: Pembrolizumab Versus Chemotherapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal Cancer (mCRC). J Clin Oncol (2021) 39(15_suppl):3500. doi: 10.1200/JCO.2021.39.15_suppl.3500
24. Cremolini C, Loupakis F, Antoniotti C, Lupi C, Sensi E, Lonardi S, et al. FOLFOXIRI Plus Bevacizumab Versus FOLFIRI Plus Bevacizumab as First-Line Treatment Of Patients With Metastatic Colorectal Cancer: Updated Overall Survival and Molecular Subgroup Analyses of the Open-Label, Phase 3 TRIBE Study. Lancet Oncol (2015) 16(13):1306–15. doi: 10.1016/S1470-2045(15)00122-9
25. Cho YA, Lee H, Kim DG, Kim H, Ha SY, Choi Y-L, et al. PD-L1 Expression Is Significantly Associated With Tumor Mutation Burden and Microsatellite Instability Score. Cancers (Basel) (2021) 13(18):4659. doi: 10.3390/cancers13184659
26. Sahin IH, Akce M, Alese O, Shaib W, Lesinski GB, El-Rayes B, et al. Immune Checkpoint Inhibitors for the Treatment of MSI-H/MMR-D Colorectal Cancer and A Perspective on Resistance Mechanisms. Br J Cancer (2019) 121(10):809–18. doi: 10.1038/s41416-019-0599-y
27. Schrock AB, Ouyang C, Sandhu J, Sokol E, Jin D, Ross JS, et al. Tumor Mutational Burden is Predictive of Response to Immune Checkpoint Inhibitors in MSI-High Metastatic Colorectal Cancer. Ann Oncol Off J Eur Soc Med Oncol (2019) 30(7):1096–103. doi: 10.1093/annonc/mdz134
28. Fabrizio DA, George TJJ, Dunne RF, Frampton G, Sun J, Gowen K, et al. Beyond Microsatellite Testing: Assessment of Tumor Mutational Burden Identifies Subsets of Colorectal Cancer Who may Respond to Immune Checkpoint Inhibition. J Gastrointest Oncol (2018) 9(4):610–7. doi: 10.21037/jgo.2018.05.06
29. Bielska AA, Chatila WK, Walch H, Schultz N, Stadler ZK, Shia J, et al. Tumor Mutational Burden and Mismatch Repair Deficiency Discordance as a Mechanism of Immunotherapy Resistance. J Natl Compr Canc Netw (2021) 19(2):130–3. doi: 10.6004/jnccn.2020.7680
30. Salem ME, Bodor JN, Puccini A, Xiu J, Goldberg RM, Grothey A, et al. Relationship Between MLH1, PMS2, MSH2 and MSH6 Gene-Specific Alterations and Tumor Mutational Burden in 1057 Microsatellite Instability-High Solid Tumors. Int J Cancer (2020) 147(10):2948–56. doi: 10.1002/ijc.33115
31. Domingo E, Freeman-Mills L, Rayner E, Glaire M, Briggs S, Vermeulen L, et al. Somatic POLE Proofreading Domain Mutation, Immune Response, and Prognosis in Colorectal Cancer: A Retrospective, Pooled Biomarker Study. Lancet Gastroenterol Hepatol (2016) 1(3):207–16. doi: 10.1016/S2468-1253(16)30014-0
32. Hu H, Cai W, Wu D, Hu W, Dong Wang L, Mao J, et al. Ultra-Mutated Colorectal Cancer Patients With POLE Driver Mutations Exhibit Distinct Clinical Patterns. Cancer Med (2021) 10(1):135–42. doi: 10.1002/cam4.3579
33. Vaňková B, Vaněček T, Ptáková N, Hájková V, Dušek M, Michal M, et al. Targeted Next Generation Sequencing of MLH1-Deficient, MLH1 Promoter Hypermethylated, and BRAF/RAS-Wild-Type Colorectal Adenocarcinomas is Effective in Detecting Tumors With Actionable Oncogenic Gene Fusions. Genes Chromosomes Cancer (2020) 59(10):562–8. doi: 10.1002/gcc.22861
34. Hamada T, Zhang X, Mima K, Bullman S, Sukawa Y, Nowak JA, et al. Fusobacterium Nucleatum in Colorectal Cancer Relates to Immune Response Differentially by Tumor Microsatellite Instability Status. Cancer Immunol Res (2018) 6(11):1327–36. doi: 10.1158/2326-6066.CIR-18-0174
35. Gao Y, Bi D, Xie R, Li M, Guo J, Liu H, et al. Fusobacterium Nucleatum Enhances the Efficacy of PD-L1 Blockade in Colorectal Cancer. Signal Transduct Target Ther (2021) 6(1):398. doi: 10.1038/s41392-021-00795-x
36. Chida K, Kawazoe A, Suzuki T, Kawazu M, Ueno T, Takenouchi K, et al. Transcriptomic Profiling of MSI-H/dMMR Gastrointestinal Tumors to Identify Determinants of Responsiveness to Anti-PD-1 Therapy. Clin Cancer Res an Off J Am Assoc Cancer Res (2022). doi: 10.1158/1078-0432.CCR-22-0041
37. Sade-Feldman M, Jiao YJ, Chen JH, Rooney MS, Barzily-Rokni M, Eliane J-P, et al. Resistance to Checkpoint Blockade Therapy Through Inactivation of Antigen Presentation. Nat Commun (2017) 8(1):1136. doi: 10.1038/s41467-017-01062-w
38. Middha S, Yaeger R, Shia J, Stadler ZK, King S, Guercio S, et al. Majority of B2M-Mutant and -Deficient Colorectal Carcinomas Achieve Clinical Benefit From Immune Checkpoint Inhibitor Therapy and Are Microsatellite Instability-High. JCO Precis Oncol (2019) 3:PO.18.00321. doi: 10.1200/PO.18.00321
39. Fucà G, Cohen R, Lonardi S, Shitara K, Elez ME, Fakih M, et al. Ascites and Resistance to Immune Checkpoint Inhibition in dMMR/MSI-H Metastatic Colorectal and Gastric Cancers. J Immunother Cancer (2022) 10(2):e004001. doi: 10.1136/jitc-2021-004001
40. Battaglin F, Naseem M, Lenz H-J, Salem ME. Microsatellite Instability in Colorectal Cancer: Overview of its Clinical Significance and Novel Perspectives. Clin Adv Hematol Oncol (2018) 16(11):735–45.
41. Carlsen L, Huntington KE, El-Deiry WS. Immunotherapy for Colorectal Cancer: Mechanisms and Predictive Biomarkers. Cancers (Basel) (2022) 14(4):1028. doi: 10.3390/cancers14041028
42. Powles T, Park SH, Voog E, Caserta C, Valderrama BP, Gurney H, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med (2020) 383(13):1218–30. doi: 10.1056/NEJMoa2002788
43. Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY-S, et al. Pembrolizumab Alone or Combined With Chemotherapy Versus Chemotherapy as First-Line Therapy for Advanced Urothelial Carcinoma (KEYNOTE-361): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol (2021) 22(7):931–45. doi: 10.1016/S1470-2045(21)00152-2
Keywords: colorectal cancer, mismatch repair, chemotherapy, nivolumab, pembrolizumab, ipilimumab
Citation: Buchler T (2022) Microsatellite Instability and Metastatic Colorectal Cancer – A Clinical Perspective. Front. Oncol. 12:888181. doi: 10.3389/fonc.2022.888181
Received: 02 March 2022; Accepted: 31 March 2022;
Published: 28 April 2022.
Edited by:
Rajiv Kumar, German Cancer Research Center (DKFZ), GermanyReviewed by:
Shuji Ogino, Brigham and Harvard Medical School, United StatesCopyright © 2022 Buchler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomas Buchler, dG9tYXMuYnVjaGxlckBmdG4uY3o=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.