
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 02 May 2022
Sec. Gastrointestinal Cancers: Gastric and Esophageal Cancers
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.877493
This article is part of the Research Topic Multimodal management of advanced gastric cancer. View all 27 articles
 Sunil Kumar1
Sunil Kumar1 Naveen Kumar1
Naveen Kumar1 Suryanarayana Deo1*Sandeep Bhoriwal1Amitabha Mandal1Atul Sharma2Sushmita Pathy3
Suryanarayana Deo1*Sandeep Bhoriwal1Amitabha Mandal1Atul Sharma2Sushmita Pathy3 Prasenjit Das4Sanjay Thulkar5Sushma Bhatnagar6
Prasenjit Das4Sanjay Thulkar5Sushma Bhatnagar6Introduction: Worldwide gastric cancer is the 5th most commonly diagnosed cancer and the leading cause of gastrointestinal cancer-related deaths. Alone surgery provides long-term survival improvements in 20% of the patients with local advanced gastric cancer. The results can be improved considering multimodal management including chemotherapy and radiotherapy. However, in low middle-income countries like India, multimodal management is challenging. Herein, we evaluated the experience of multimodal management of gastric cancer and the long-term outcome.
Methods: Retrospective analysis of the data of 372 patients was done from a prospectively maintained computerized database from 1994 to 2021. Records were analyzed for demographic details, treatment patterns, recurrences, and long-term outcomes (DFS and OS). Statistical analysis was done with the package SPSS version 26 (IBM Corp, Chicago, Illinois, USA).
Results: This study included 372 patients. The mean age of the patients was 54.07. A total of 307 patients (82.5%) were operated upfront, 45 (12%) received NACT, and 20 (5.5%) underwent the palliative procedure. A total of 53.2% underwent curative resection. R0 resection rate was achieved in 95% of patients. A total of 72.58% of patients required adjuvant treatment, and the majority of the patients underwent chemoradiotherapy. The most common site of metastasis was the liver. Median follow-up was 50.16 months. The 3-year disease-free survival and overall survival were 36.28% and 67.8%, and the 5-year disease-free survival and overall survival were 30.15% and 37.7%, respectively.
Conclusion: Our study suggested that multimodal management is required in locally advanced gastric cancer to achieve good long-term outcomes. The treatment sequence can be tailored based on the available resources.
Worldwide gastric cancer is the 5th most commonly diagnosed cancer and ranks 3rd in cancer-related death (1). Although gastric cancer was the leading cause of cancer death till the 1980s, the incidence has declined rapidly since the last few decades in most parts of the world (2–4). The decline in gastric cancer incidence was due to identifying Helicobacter pylori as a risk factor and modifying dietary factors. The rate of decline of gastric cancer is more profound in the United Kingdom, whereas in a country like Japan with a very high incidence of gastric cancer, the decline rate is slower. Almost two-thirds of the gastric patients are found with advanced stage, whereas 50% of patients are detected at the early stage in East Asian countries like Japan and Korea because of the endoscopic screening program (5, 6).
Gastric cancer is a lethal disease with persistently high mortality due to its presence in the advanced stage and change in the distribution of tumor location from pylorus and antrum to body and cardia (7). Despite the aggressive nature of the disease, the prognosis of gastric cancer had improved significantly in the last two decades due to improvement in surgical management and multimodal therapy. If it is diagnosed in the early stage, very good survival outcomes can be achieved with multimodal management (8). Multimodal management includes surgical management, ranging from endoscopic mucosal resection to gastrectomy, lymph node dissection, neoadjuvant chemotherapy (NACT), perioperative chemotherapy, adjuvant chemoradiation, and adjuvant chemotherapy. Advanced stage disease has a very dismal prognosis; multimodal treatment approach may prolong the survival. This study aims to evaluate the basic demographic characteristic, multimodal approach to gastric cancer, resectability rate, the response of neoadjuvant therapy, recurrence pattern, and long-term survival of gastric cancer in a high-volume tertiary cancer care center in North India.
Retrospective analysis of the data of 372 patients was done from a prospectively maintained computerized database from 1994 to 2021. All the gastric patients were registered in the gastrointestinal cancer clinic. Multimodal management was planned. Upper gastrointestinal endoscopy (UGIE) and biopsy were done in all patients for diagnosis and extent of intraluminal disease. Contrast-enhanced computed tomography (CECT) of the chest, abdomen, and pelvis was done for the staging of the disease.
Before the neoadjuvant era, upfront surgery was offered in all potentially operable cases and neoadjuvant chemotherapy was only offered to the patients who were initially unresectable or locally advanced without evidence of distant metastasis. Adjuvant therapy was given to patients with a pathological T3 or above and node-positive disease.
In the last decade, neoadjuvant chemotherapy has gained ground significantly and now it is a standard treatment in locally advanced gastric cancer after the results of several randomized trials (9, 10). We followed the same treatment protocol. In all locally advanced tumors (T3/T4 or node positive), neoadjuvant chemotherapy followed by surgery was done. Upfront surgery was performed in only emergency indications like bleeding or gastric outlet obstruction.
We used epirubicine, cisplatin, and 5-FU (ECF); folinic acid, fluorouracil, and oxaliplatin (FOLFOX); and capecitabine and oxaliplatine (CAPOX) before FLOT era. After the FLOT4-AIO trial, 5-fluorouracile, leucovorin, oxaliplatin, and docetaxel (FLOT) regimen was an integral part of our NACT schedule for patients with good performance status (ECOG 0 or 1), and FOLFOX for poor performance status patients (2 or 3).
Adjuvant treatment was offered to patients with pathological T3/T4 or node-positive disease. Adjuvant chemotherapy alone was given to the patients with adequate lymph node dissection (D2 lymphadenectomy), and optimum lymph node was evaluated in histopathological examination (16 nodes). Adjuvant chemoradiation as per McDonald’s protocol (chemotherapy: fluorouracil and leucovorin; radiotherapy: 45 Gy of radiation at 1.80 Gy per day, 5 days per week for 5 weeks, with intensity-modulated radiation therapy technique) was given to those patients who had inadequate lymph node dissection (less than D2 dissection) and less than 16 nodes evaluated in the pathological examination.
Categorical variables were expressed in percentages and frequencies. A chi-square test was used for group comparison of categorical variables. The software package SPSS version 26 (IBM Corp, Chicago, Illinois, USA) was used for the statistical analysis. All values of p < 0.05 were taken as statistical significance. Disease-free survival (DFS) was calculated from the date of completion of the treatment to recurrence or death, whichever comes earlier. Overall survival (OS) was calculated from the date of registration to death or lost to follow up, whichever comes earlier. Kaplan–Meier estimate was used for survival analysis.
This study included 372 patients. The mean age of the patients was 54.07 (range 17–84 years), with male predominance. Pain in the abdomen was the most common presenting symptom followed by anorexia and weight loss. The antropyloric region was the most common site of tumor occurrence. The majority of the patients were presented with locally advanced stages (stage II and stage III). The demographic profile of the patients is shown in Table 1. Among all the patients, 63 (16.9%), 39 (10.5%), and 36 patients (9.7%) were smokers, alcoholics, and tobacco chewers, respectively. Most of the patients were presented with good performance status (Table 1).
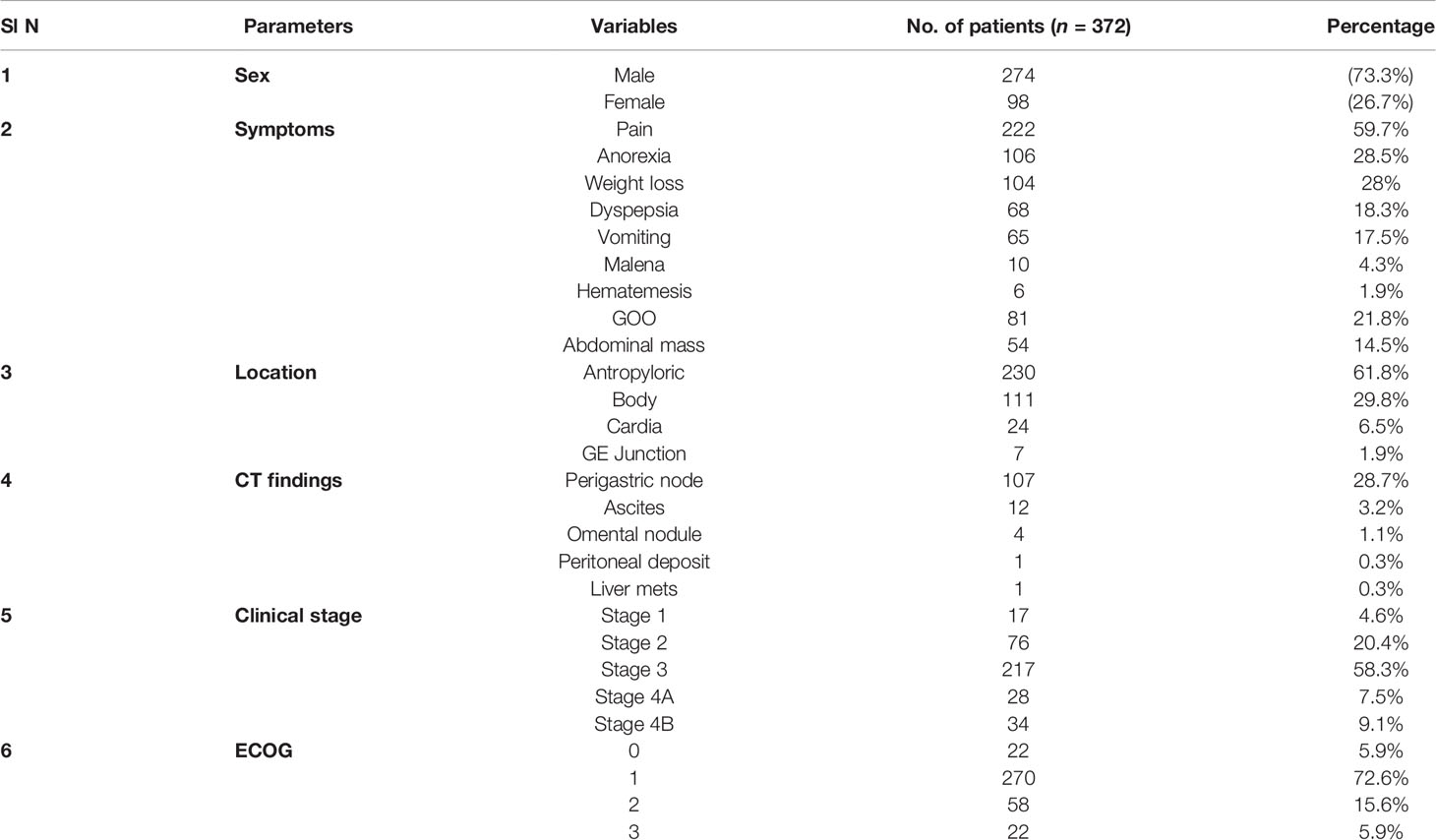
Table 1 Demographic profile and baseline characteristics of the patients.
A total of 307 patients (82.5%) were operated upfront, 45 (12%) patients were planned for neoadjuvant chemotherapy (NACT) followed by reassessment for surgery, and 20 (5.5%) cases underwent the palliative procedure. Among NACT patients, complete response (CR) and partial response (PR) were noted in 1 (0.5%) and 24 (6.5%) respectively; 17 (4.6%) patients had stable disease and 2 (0.5%) had progressive disease. Curative resection was done in 19 patients (42.2%) after NACT, and the rest of the 26 patients were unresectable on exploration and underwent palliative surgery.
The curative resection rate in this study was 53.4% (199 patients). The most commonly performed surgical procedure was distal radical gastrectomy followed by total gastrectomy. Clavien Dindo grade 3–4 was seen in 16 (7.5%) patients. R0 resection rate was achieved in 95% of the patients. The mean node harvested was 15, ranging from 6 to 32, and the mean pathological node involvement was 3 (range 1–16). Surgical details are shown in Table 2. After palliative surgery, 51 (13.3%) patients did not receive any form of palliative therapy, 102 (27.4%) patients received palliative chemotherapy, 2 (0.5%) patients received palliative radiotherapy, and the remaining 18 patients (4.8%) received the best supportive care.
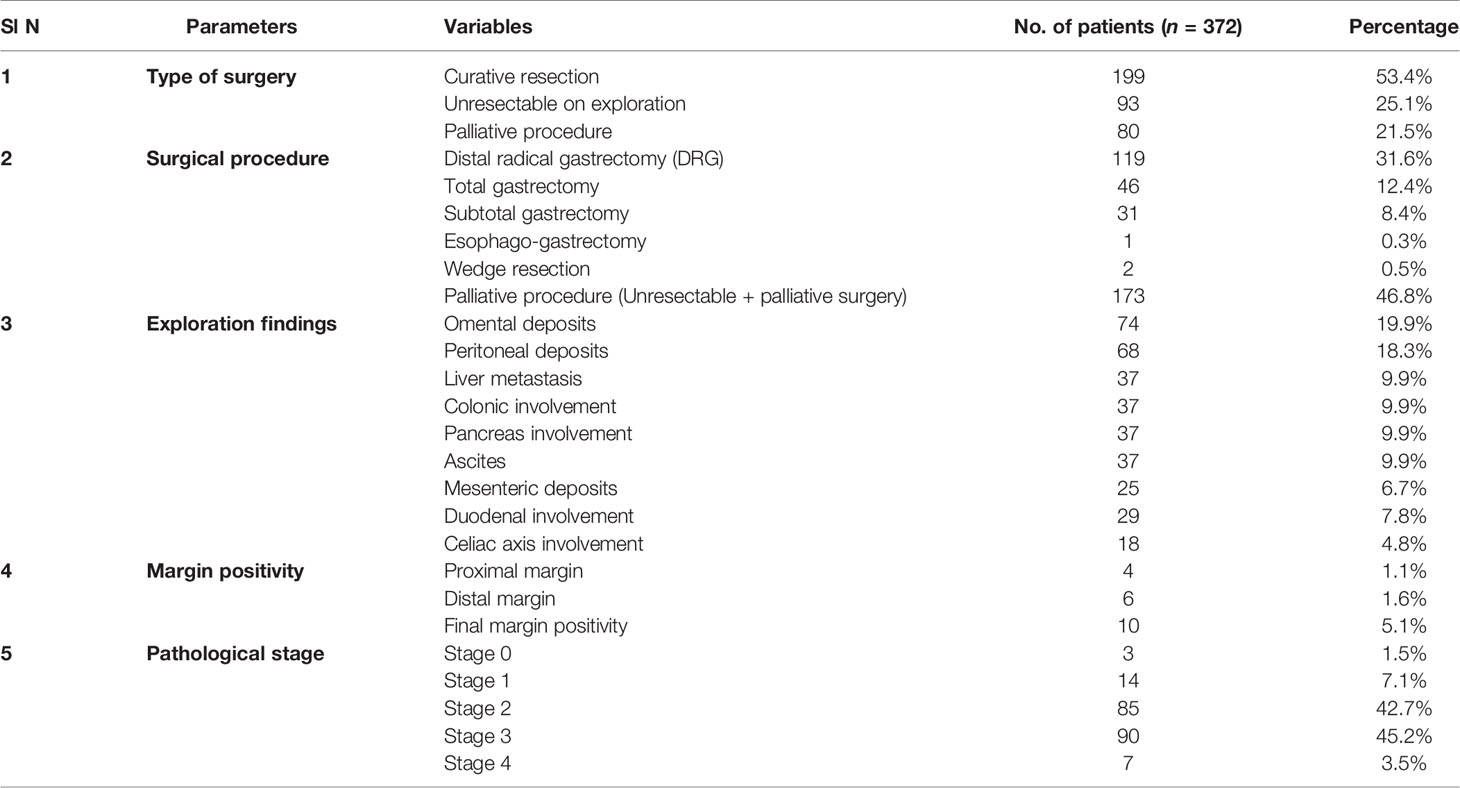
Table 2 Surgical details and pathological parameters.
After curative resection, 143 (72.58%) patients received adjuvant therapy, and 54 (27.4%) did not receive any adjuvant therapy. Out of 143 patients, 30 (15.2%) patients received adjuvant chemotherapy and 103 (52.3%) patients received adjuvant chemoradiotherapy. Palliative RT and palliative chemotherapy were offered to 3 (1.5%) patients each, whereas 1 patient went for the best supportive therapy; the remaining 18 patients (9.13%) lost their follow-up. The majority of the patients developed systemic recurrence, and the liver was the most common site of systemic recurrence. Systemic, local, and locoregional recurrence occurred in 72 patients (36.2%), 16 patients (8%), and 13 patients (6.5%), respectively. Among all systemic recurrences, 33 (16.6%) patients had liver metastasis followed by peritoneum in 29 (14.6%) patients.
Survival analysis was done for only those patients who underwent curative resection. The median follow-up was 50.166 months. The 3-year DFS and OS were 36.28% and 67.8%, respectively. The 3-year median DFS and OS were 61 (95% CI, 46.6–75.3) and 84 (95% CI, 85.1–103.1) months (Figure 1). The 5-year DFS and OS were 30.15% and 37.7%, respectively, and the 5-year median DFS and OS were 63 months (95% CI, 96.2–119.7) and (95% CI, 52.7–73.2) (Figure 2).
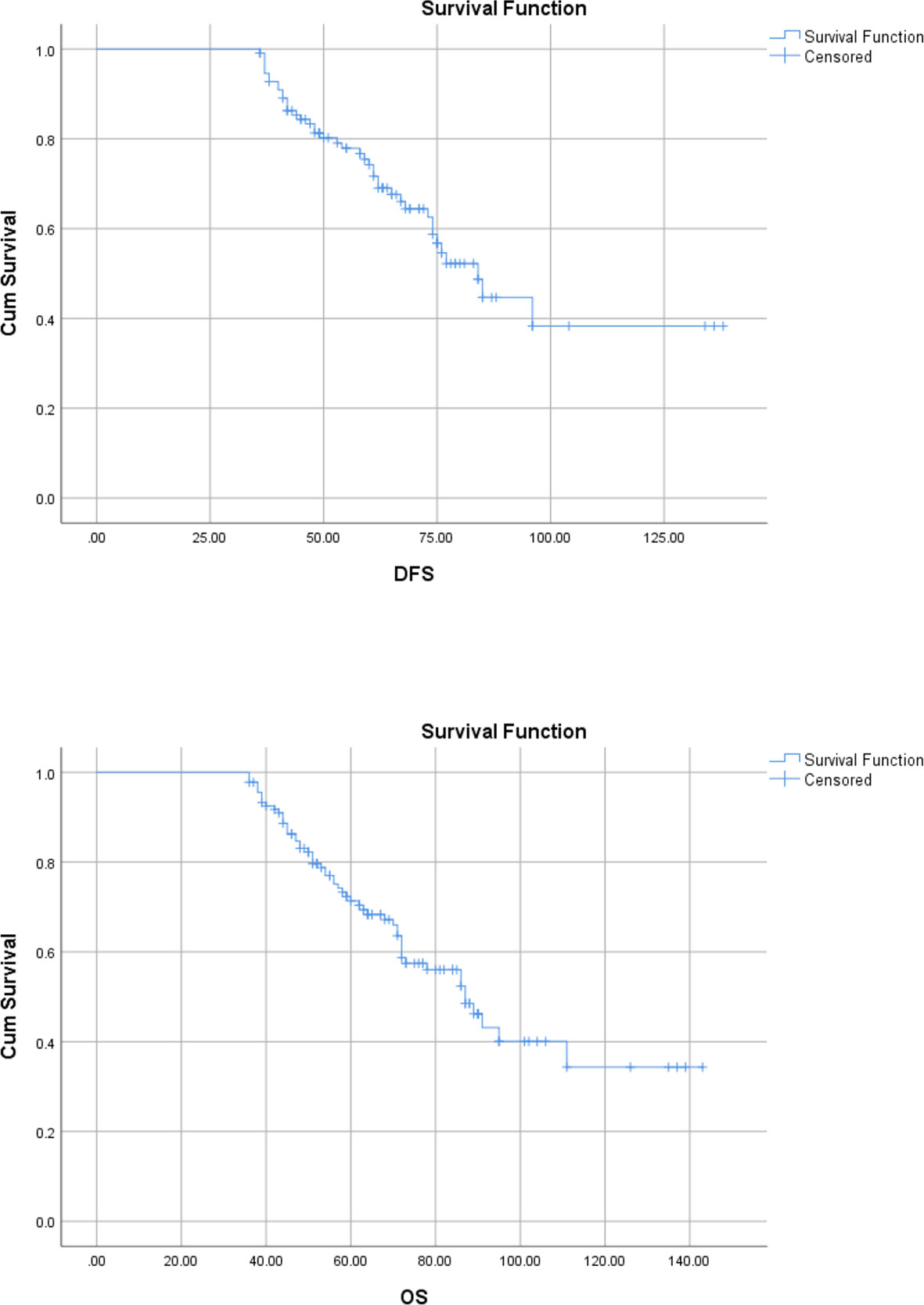
Figure 1 Kaplan–Meier curve showing 3-year disease-free and overall survival.

Figure 2 Kaplan–Meier curve showing 5-year disease-free and overall survival.
Although the incidence of gastric cancer has declined in most countries, it is still a major cause of cancer-related mortality (2, 7). The lethality of gastric cancer lies in its presentation in late stage, due to vague symptomatology. Until or unless there are features of gastric outlet obstruction, hematemesis, abdominal lump, or gross weight loss, the disease does not attract the attention of the patients (11, 12). In this study, the most common symptom was pain in the abdomen. Worldwide, the incidence of stomach cancer has declined significantly, mainly in European countries, due to modification in dietary factors and identification of H. pylori as a risk factor. Other risk factors are smoking, alcohol intake, and tobacco chewing (13). In our study, almost 35% of the patients were associated with predisposing factors.
In the last two decades, the trends of the location of the tumor in the stomach have shifted more proximally from the location in the distal stomach (14). In the current study, the distal stomach is the most common site of cancer.
Traditionally, the staging of gastric cancer is done with a CT scan; however, various studies have been conducted to see the role of 18-FDG PET scan. PET scan has certain limitations in diagnosing gastric cancer because the normal gastric mucosa and benign lesions take FDG uptake and are difficult to differentiate with pathological uptake. Few studies have reported a limited role in stage IV disease (peritoneal carcinomatosis) with low sensitivity (range: 9%–50%; median: 32.5%) and marginal higher specificity (63%–99%; median: 88.5%) (15). Thus, the role of PET scan is still evolving. At our center, a PET scan is advised only in recurrent or stage IV cases to prognosticate the disease.
The sequence of choice of the multimodal treatment depends on various factors like patient’s performance status (ECOG performance status), comorbidity, and site and stage of the disease. Treatment options for early gastric cancer are eradication of H. pylori, endoscopic therapy, gastrectomy, and adjuvant therapy (16). In developing countries, endoscopic resection expertise is still lesser, and gastrectomy is commonly preferred. In our study, only 4.6% of the patients presented with early gastric cancer and all patients underwent gastrectomies.
Locally advanced gastric cancer requires multimodal management. Many randomized trials and one meta-analysis proved that using NACT or perioperative chemotherapy has a survival advantage over upfront surgery for potentially resectable gastric cancer (9, 17). In our study, more than 50% of patients had a locally advanced stage and required multimodal management. The resectability rate after NACT was 42.2%, which is a bit lower than other studies. The pathological CR rate is lower (0.5%) in this study as compared to literature (5%–15%) (18, 19). This difference was seen because of the advanced stage at the presentation.
Gastrectomy with adequate lymph node dissection (at least 16 nodes) is the surgical procedure of choice for operable gastric cancer with good quality of life. Proximal tumors involving cardia, fundus, and GE junction are treated with total gastrectomy and distal tumors (body, antropyloric area) with subtotal or distal gastrectomy. In our series, most of the patients underwent distal radical gastrectomy since the majority of the patients had distal gastric cancer and total gastrectomy was only performed for proximal tumors or involvement of the whole stomach. In the literature, two major trials compared subtotal with total gastrectomy for distal gastric cancer without any significant survival advantage in favor of total gastrectomy (20, 21). In this study, distant metastasis, involvement of celiac axis, hepatic artery, and aorta were considered as unresectable diseases, and require palliative surgery (56%) in the form of feeding jejunostomy or gastrojejunostomy.
The extent of lymphadenectomy is an area of active debate for a long time. Various types of lymph node dissection is described in the literature, D1 (Station 1-6), D1+ (Station 1-6, and 8a, 9, 11), D2 (Station 1-12a), and D3 (Station 1-16 or D2+ paraaortic node dissection). Japanese and Korean surgeons preferred more aggressive lymph node dissection, whereas according to current NCCN guidelines, spleen and pancreas preserving D2 lymphadenectomy with at least 15 nodes for histopathological examination is the standard of care (22–24). In the current study, all the patients underwent D2 lymph node dissection and the complication rate is comparable. Most of the prospective randomized trials have failed to demonstrate the survival advantage of D2 over D1 lymphadenectomy. The two largest prospective randomized trials (MRC, Dutch), which are debated the most, also did not find any significant survival advantage of D2 over D1 lymphadenectomy; however, long-term analysis of these studies had shown disease-specific survival benefits (25–28).
Targeted therapy such as trastuzumab has been established for unresectable and metastatic HER2 positive gastric cancer. Many trials like ToGA, LOGiC, and TyTNHA showed an improvement in survival after using the HER2-targeted therapy. Various phase III trials are ongoing to explore other targeted therapies based on epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF)/vascular endothelial growth factor receptor (VEGFR), MET, or the mechanistic target of rapamycin (mTOR) (29).
Systemic and locoregional recurrence are the two forms of recurrence in gastric cancer, where systemic is common. In one study, systemic and locoregional recurrences were 60% and 40%, respectively (30). Another study quoted locoregional recurrence rate in 15% of cases; peritoneal, 49%; nonperitoneal distant recurrence, 54%; and liver metastasis, 20% (31). Another study evaluated the recurrence pattern in proximal gastric cancer and found a recurrence rate of 85.9% within 2 years, where locoregional recurrence was the most common pattern followed by hematogenous. Among them, liver was the most common organ for systemic recurrence followed by the peritoneum (32). In this current study, systemic recurrence (36.2%) was the most common form of relapse and liver was the most common site.
Survival after curative resection depends on stage, location, and ethnicity. The Asian population has better survival than the Western population (32). In the literature, 5-year survival of locally advanced gastric cancer is reported with a range of 40%–60% after multimodal management (25, 26, 33). Our study has shown almost similar outcomes.
Although the incidence of gastric cancer has been decreased in the Indian population, it is still a deadly disease, because of its aggressive biology and late presentation. Our study suggested that optimal outcomes of gastric cancer in low middle-income countries can be achieved based on the best available resources using a multimodal treatment approach.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
SD started the surgical program and provided extensive guidance in making the manuscript. NK and AM analyzed the data and wrote the manuscript. SK and SBho reviewed the manuscript and added their inputs. AS were the lead medical oncologist and added the inputs. SP was a lead radiation oncologist and PD was the lead pathologist and they added their inputs. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Pisani P, Parkin DM, Ferlay J. Estimates of the Worldwide Mortality From Eighteen Major Cancers in 1985. Implications for Prevention and Projections of Future Burden. Int J Cancer (1993) 55(6):891–903. doi: 10.1002/ijc.2910550604
3. Zhu AL, Sonnenberg A. Is Gastric Cancer Again Rising? J Clin Gastroenterol (2012) 46(9):804–6. doi: 10.1097/MCG.0b013e3182604254
4. Fitzsimmons D, Osmond C, George S, Johnson CD. Trends in Stomach and Pancreatic Cancer Incidence and Mortality in England and Wales, 1951-2000. Br J Surg (2007) 94(9):1162–71. doi: 10.1002/bjs.5751
5. Ahn HS, Lee H-J, Yoo M-W, Jeong S-H, Park D-J, Kim H-H, et al. Changes in Clinicopathological Features and Survival After Gastrectomy for Gastric Cancer Over a 20-Year Period. Br J Surg (2011) 98(2):255–60. doi: 10.1002/bjs.7310
6. Rausei S, Boni L, Rovera F, Dionigi G. Locally Advanced Gastric Cancer: A New Definition to Standardise. J Clin Pathol (2013) 66(2):164–5. doi: 10.1136/jclinpath-2012-201176
7. Fuchs CS, Mayer RJ. Gastric Carcinoma. N Engl J Med (1995) 333(1):32–41. doi: 10.1056/NEJM199507063330107
8. Cellini F, Morganti AG, Di Matteo FM, Mattiucci GC, Valentini V. Clinical Management of Gastroesophageal Junction Tumors: Past and Recent Evidences for the Role of Radiotherapy in the Multidisciplinary Approach. Radiat Oncol (2014) 9(1):45. doi: 10.1186/1748-717X-9-45
9. Perioperative Chemotherapy Versus Surgery Alone for Resectable Gastroesophageal Cancer | NEJM. Available at: https://www.nejm.org/doi/full/10.1056/nejmoa055531.
10. Al-Batran S-E, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative Chemotherapy With Fluorouracil Plus Leucovorin, Oxaliplatin, and Docetaxel Versus Fluorouracil or Capecitabine Plus Cisplatin and Epirubicin for Locally Advanced, Resectable Gastric or Gastro-Oesophageal Junction Adenocarcinoma (FLOT4): A Randomised, Phase 2/3 Trial. Lancet Lond Engl (2019) 393(10184):1948–57. doi: 10.1016/S0140-6736(18)32557-1
11. Quadri HS, Smaglo BG, Morales SJ, Phillips AC, Martin AD, Chalhoub WM, et al. Gastric Adenocarcinoma: A Multimodal Approach. Front Surg (2017) 4:42. doi: 10.3389/fsurg.2017.00042
12. Dicken BJ, Bigam DL, Cass C, Mackey JR, Joy AA, Hamilton SM. Gastric Adenocarcinoma: Review and Considerations for Future Directions. Ann Surg (2005) 241(1):27–39. doi: 10.1097/01.sla.0000149300.28588.23
13. Rawla P, Barsouk A. Epidemiology of Gastric Cancer: Global Trends, Risk Factors and Prevention. Przeglad Gastroenterol (2019) 14(1):26–38. doi: 10.5114/pg.2018.80001
14. Crew KD, Neugut AI. Epidemiology of Gastric Cancer. World J Gastroenterol (2006) 12(3):354–62. doi: 10.3748/wjg.v12.i3.354
15. Dascălu R-I, Păduraru DN, Bolocan A, Ion D, Andronic O. The Role of PET-CT in Gastric Cancer – A Narrative Review. Sudan J Med Sci (SJMS) (2020) 15(3):332–44. doi: 10.18502/sjms.v15i3.7749
16. Espinel J, Pinedo E, Ojeda V, del Rio MG. Treatment Modalities for Early Gastric Cancer. World J Gastrointest Endosc (2015) 7(12):1062–9. doi: 10.4253/wjge.v7.i12.1062
17. Xiong B-H, Cheng Y, Ma L, Zhang C-Q. An Updated Meta-Analysis of Randomized Controlled Trial Assessing the Effect of Neoadjuvant Chemotherapy in Advanced Gastric Cancer. Cancer Invest (2014) 32(6):272–84. doi: 10.3109/07357907.2014.911877
18. Gallardo-Rincón D, Oñate-Ocaña LF, Calderillo-Ruiz G. Neoadjuvant Chemotherapy With P-ELF (Cisplatin, Etoposide, Leucovorin, 5-Fluorouracil) Followed by Radical Resection in Patients With Initially Unresectable Gastric Adenocarcinoma: A Phase II Study. Ann Surg Oncol (2000) 7(1):45–50. doi: 10.1007/s10434-000-0045-6
19. Yoshikawa T, Sasako M, Yamamoto S, Sano T, Imamura H, Fujitani K, et al. Phase II Study of Neoadjuvant Chemotherapy and Extended Surgery for Locally Advanced Gastric Cancer. Br J Surg (2009) 96(9):1015–22. doi: 10.1002/bjs.6665
20. Robertson CS, Chung SC, Woods SD, Griffin SM, Raimes SA, Lau JT, et al. A Prospective Randomized Trial Comparing R1 Subtotal Gastrectomy With R3 Total Gastrectomy for Antral Cancer. Ann Surg (1994) 220(2):176. doi: 10.1097/00000658-199408000-00009
21. Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Gennari L. Subtotal Versus Total Gastrectomy for Gastric Cancer: Five-Year Survival Rates in a Multicenter Randomized Italian Trial. Italian Gastrointestinal Tumor Study Group. Ann Surg (1999) 230(2):170–8. doi: 10.1097/00000658-199908000-00006
22. Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2018 (5th Edition). Gastric Cancer (2021) 24(1):1–21. doi: 10.1007/s10120-020-01042-y
23. Degiuli M, De Manzoni G, Di Leo A, D'Ugo D, Galasso E, Marrelli D, et al. Gastric Cancer: Current Status of Lymph Node Dissection. World J of Gastroenterol (2016) 22(10):2875–93. doi: 10.3748/wjg.v22.i10.2875
24. Sasako M, Sano T, Yamamoto S, Kurokawa Y, Nashimoto A, Kurita A, et al. D2 Lymphadenectomy Alone or With Para-Aortic Nodal Dissection for Gastric Cancer. N Engl J Med (2008) 359(5):453–62. doi: 10.1056/NEJMoa0707035
25. Cuschieri A, Weeden S, Fielding J, Bancewicz J, Craven J, Joypaul V, et al. Patient Survival After D1 and D2 Resections for Gastric Cancer: Long-Term Results of the MRC Randomized Surgical Trial. Surgical Co-Operative Group. Br J Cancer (1999) 79(9–10):1522–30. doi: 10.1038/sj.bjc.6690243
26. Songun I, Putter H, Kranenbarg EM-K, Sasako M, van de Velde CJH. Surgical Treatment of Gastric Cancer: 15-Year Follow-Up Results of the Randomised Nationwide Dutch D1D2 Trial. Lancet Oncol (2010) 11(5):439–49. doi: 10.1016/S1470-2045(10)70070-X
27. Degiuli M, Sasako M, Ponti A, Vendrame A, Tomatis M, Mazza C, et al. Randomized Clinical Trial Comparing Survival After D1 or D2 Gastrectomy for Gastric Cancer. Br J Surg (2014) 101(2):23–31. doi: 10.1002/bjs.9345
28. Information NC for B, Pike USNL of M 8600 R, MD B, Usa 20894. A Meta-Analysis of D1 Versus D2 Lymph Node Dissection. In: Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews. UK: Centre for Reviews and Dissemination (2012). Available at: https://www.ncbi.nlm.nih.gov/books/NBK127357/.
29. Kiyozumi Y, Iwatsuki M, Yamashita K, Koga Y, Yoshida N, Baba H. Update on Targeted Therapy and Immune Therapy for Gastric Cancer, 2018. J Cancer Metastasis Treat (2018) 4:31. doi: 10.20517/2394-4722.2017.77
30. Wanebo HJ, Kennedy BJ, Chmiel J, Steele G, Winchester D, Osteen R. Cancer of the Stomach. A Patient Care Study by the American College of Surgeons. Ann Surg (1993) 218(5):583–92. doi: 10.1097/00000658-199321850-00002
31. Elimova E, Slack RS, Chen H-C, Planjery V, Shiozaki H, Shimodaira Y, et al. Patterns of Relapse in Patients With Localized Gastric Adenocarcinoma Who Had Surgery With or Without Adjunctive Therapy: Costs and Effectiveness of Surveillance. Oncotarget (2017) 8(46):81430–40. doi: 10.18632/oncotarget.19226
32. Cao L, Selby LV, Hu X, Zhang Y, Janjigian YY, Tang L, et al. Risk Factors for Recurrence in T1-2n0 Gastric Cancer in the United States and China. J Surg Oncol (2016) 113(7):745–9. doi: 10.1002/jso.24228
33. Stomach (Gastric) Cancer Survival Rates. Available at: https://www.cancer.org/cancer/stomach-cancer/detection-diagnosis-staging/survival-rates.html.
Keywords: gastric cancer, multimodal, outcomes, survival, India
Citation: Kumar S, Kumar N, Deo S, Bhoriwal S, Mandal A, Sharma A, Pathy S, Das P, Thulkar S and Bhatnagar S (2022) Patterns of Multimodality Management of Gastric Cancer—Single Institutional Experience of 372 Cases From a Tertiary Care Center in North India. Front. Oncol. 12:877493. doi: 10.3389/fonc.2022.877493
Received: 16 February 2022; Accepted: 25 March 2022;
Published: 02 May 2022.
Edited by:
Pankaj Kumar Garg, Shri Guru Ram Rai Institute of Medical and Health Sciences, IndiaReviewed by:
Ajeet Kumar Tiwari, Sir Ganga Ram Hospital, IndiaCopyright © 2022 Kumar, Kumar, Deo, Bhoriwal, Mandal, Sharma, Pathy, Das, Thulkar and Bhatnagar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suryanarayana Deo, c3ZzZGVvQHlhaG9vLmNvLmlu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.