
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 26 April 2022
Sec. Head and Neck Cancer
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.872130
This article is part of the Research Topic Improving Quality of Life in Patients with Differentiated Thyroid Cancer View all 20 articles
 Soo Young Kim1
Soo Young Kim1 Hyeok Jun Yun2
Hyeok Jun Yun2 Hojin Chang2
Hojin Chang2 Seok-Mo Kim2
Seok-Mo Kim2 Soyoung Jeon3Sujee Lee3Yong Sang Lee2*Hang-Seok Chang2Cheong Soo Park4
Soyoung Jeon3Sujee Lee3Yong Sang Lee2*Hang-Seok Chang2Cheong Soo Park4Background: The biological behavior of thyroid cancer in children has been known to be different from that in adults. We sought to understand the differences between DTC presentation in pediatric (<16 years) and adult patients, to guide better prognosis and clinical treatments.
Methods: This retrospective study included 48 pediatric patients younger than 16 years who underwent initial thyroid surgery and were diagnosed with DTC between January 1992 and December 2014 at Yonsei University in Seoul, South Korea. For a 1:4 propensity score-matched analysis, adult patients with matched sex and cancer size were included.
Results: The mean age was 12.54 ± 3.01 years. Total thyroidectomy (70.8%) without lateral lymph node dissection (47.9%) was the most commonly performed surgery. Central (73.9%) and lateral neck node metastases (62.5%) were common; distant metastasis was observed in 2 (4.2%) patients and recurrence occurred in 11 (22.9%). In propensity score-matched analysis, central lymph node metastasis and lateral neck node metastasis were significantly more frequent in pediatric patients. Symptoms were more common in the pediatric group than in the adult group (p < 0.001). In stratified cox regression, pediatric patients were more likely to experience recurrence [HR 5.339 (1.239–23.007)]. In stratified log-rank analysis, recurrence-free survival was significantly different between the adult and pediatric groups (p = 0.0209).
Conclusion: DTC in the pediatric group revealed more aggressive patterns than in the adult group with the same cancer size. Central lymph node metastasis and lateral neck node metastasis were more frequent. Stratified log-rank analysis revealed that recurrence was significantly higher in pediatric patients than in matched adult patients.
Among thyroid carcinomas, differentiated thyroid cancer (DTC) in childhood is one of the most common endocrine cancers in pediatric patients, accounting for 90%–95% of all pediatric thyroid carcinomas (1, 2). The most common histopathological diagnosis is papillary carcinoma, followed by follicular variant of papillary thyroid carcinoma. In 66% of the reports, multifocality has been reported (3). Since it only accounts for 1.8% of all thyroid malignancies, the treatment approaches historically have been extrapolated only from adult experiences (4, 5).
The incidence of pediatric DTC has been increasing gradually for the last few decades both in Korea and throughout the world (6–10). Its incidence is almost always higher in female patients (8). The increasing incidence has been reported to be associated with radiation exposure in children (11, 12). Many reports focused on the occurrence of papillary thyroid cancer (PTC) after the nuclear reactor accident in Chernobyl in 1986 (13–15). Treatment for a prior malignancy and a history of thyroiditis were identified as common features of pediatric thyroid cancer, suggesting thyroid cancer as a second malignancy in childhood cancer survivors (16).
The biological behavior of pediatric thyroid cancer is known to be different from that in adult patients; it has been suggested that it presents at a more advanced stage in prepuberty than in puberty (17). Younger pediatric patients are associated with a larger mean tumor size, more aggressive pathological features, and higher incidence of loco-regional and distant metastasis (18, 19). The patients first presented with symptoms such as neck swelling with a palpable mass or discomfort (3, 20).
Until now, the reported risk factors for poor prognosis are younger age, male sex, large primary tumor size, extrathyroidal tumor extension, palpable lymph nodes, distant metastases at diagnosis, and diffuse sclerosing pathology (19, 21). Despite the aggressive disease presentation and higher risk of recurrence, pediatric thyroid cancer is associated with an excellent prognosis (22–25).
Total thyroidectomy and radioactive iodine are recommended as the best management options to reduce the incidence of lung metastasis (22. One study also suggests more extensive cervical lymph node dissection with thyroid stimulating hormone (TSH) suppression therapy since young patients present with more lymph node metastasis (19). Treatment for pediatric thyroid cancer is still controversial because of these reasons.
Most previous studies on pediatric thyroid cancer also included adolescent patients; thus, we aimed to study DTC features in pediatric patients younger than 16 years.
This retrospective cohort study initially included 48 pediatric patients (<16 years of age) who underwent initial thyroid surgery and were diagnosed with DTC between January 1992 to December 2014 at Yonsei University in Seoul, South Korea. Four patients were excluded from the study since they had missing information regarding pathology and clinical characteristics, i.e., a total of 48. Since the electronic chart system was introduced only in 2003, adult patients were enrolled from January 2003 to December 2014 for propensity score-matched analysis. To minimize the bias from differences in follow-up duration, for the matched analysis, data of only pediatric patients from January 2003 to December 2014 were analyzed, amounting to 37 patients in total.
Written informed consent by the patients was waived due to the retrospective nature of the study. The study protocol was approved by the Institutional Review Board of Yonsei University (IRB 3-2019-0281), Seoul, South Korea.
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and R statistics 4.0.2 (http://www.r-project.org). We conducted 1:4 matching using propensity score, selecting adult patients with the same tumor size and sex.
Continuous variables included mean and standard deviation, and categorical variables included frequency and percentage. To compare continuous and categorical variables between two groups, a generalized estimated equation was used. Recurrence-free survival curves were plotted using the Kaplan-Meier method, and the stratified log-rank test was performed to compare the recurrence rate between pediatric and adult patients. To evaluate risk factors for recurrence, stratified Cox regression was performed and are presented as hazard ratio (HR) and 95% confidence interval (CI). P-values of <0.05 were deemed to indicate statistical significance.
The baseline clinical characteristics of the 48 included patients are shown in Table 1. The incidence of DTC was higher in female patients (77.1%), and the mean age was 12.54 ± 3.01 years. The most common presenting symptom was a neck mass (60.4%). Most of the patients (85.4%) did not have a family history of thyroid cancer. Total thyroidectomy (70.8%) without lateral lymph node dissection (47.9%) was the most commonly performed surgery. Papillary thyroid cancer (87.5%) followed by follicular cancer (12.5%) were the most common diagnoses. Central (73.9%) and lateral neck node metastases (62.5%) were common. Further, distant metastasis was observed in 2 (4.2%) patients and recurrence occurred in 11 (22.9%) patients.
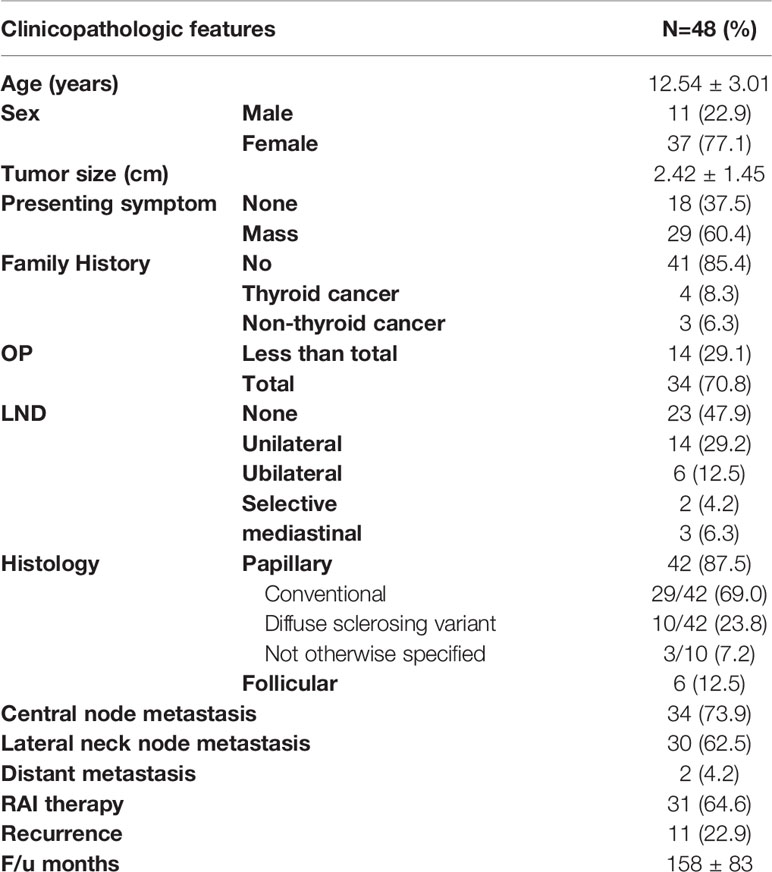
Table 1 The baseline clinical characteristics of 48 pediatric patients.
We performed 1:4 propensity score matching with adult patients with matched sex and tumor size; the results are shown in Table 2. Pediatric patients were more likely to be symptomatic than adult patients (p < 0.001). There were no differences regarding family history and surgical extent. Histology was not significantly different when distinguished into papillary and follicular cancer. However, further dividing into histological variants of papillary thyroid cancer showed significant difference. Diffuse sclerosing variant of papillary thyroid carcinoma was more frequent in pediatric thyroid cancer [9/34 (26.5%) vs 6/145 (4.1%)]. Central lymph node metastasis [27 (73.0%) vs 69 (46.6%)] and lateral neck node metastasis were significantly more frequent in pediatric patients than in matched adult patients. There were no significant differences in distant metastasis and use of RAI therapy. Recurrence was significantly more frequent in pediatric patients than in adult patients (13.5% vs 2%, p = 0.0131).
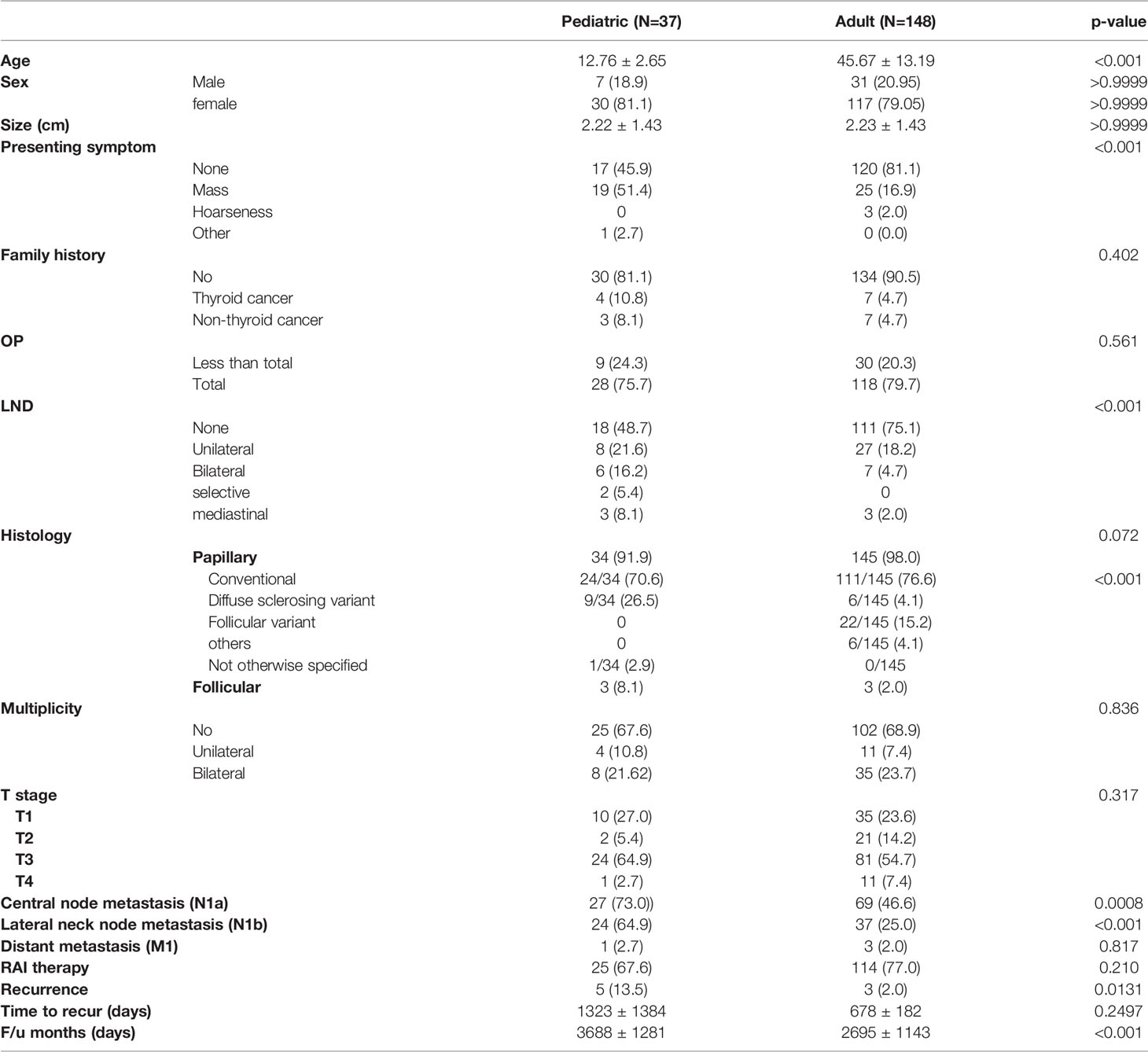
Table 2 1:4 Propensity score-matched GEE analysis.
In univariable stratified cox regression analysis, pediatric patients were more likely to experience recurrence. Pediatric patients had approximately 5.4 times the risk of recurrence than adult patients [HR 5.339 (1.239–23.007)]. Multiplicity of disease was associated with recurrence compared with a single disease [HR 264.171 (3.219–21678.05)]. In multivariable analysis, only multiplicity was associated with recurrence (Table 3).
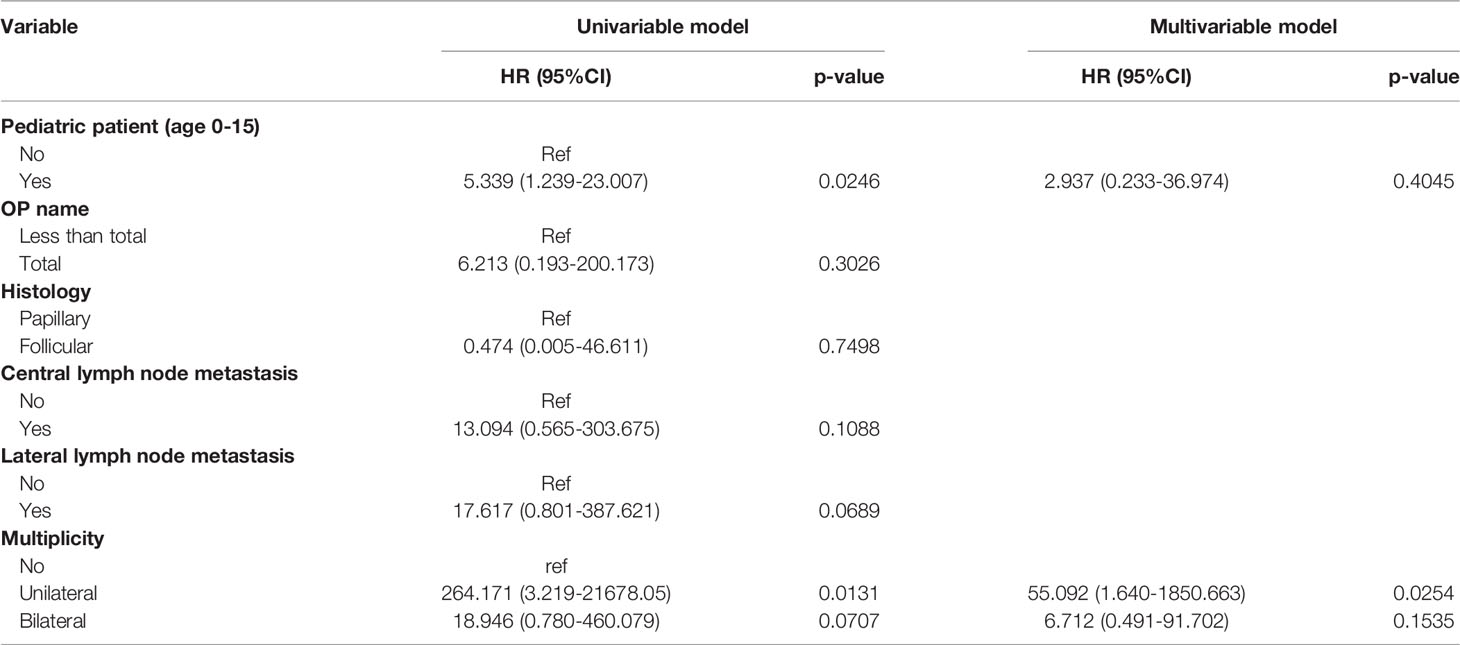
Table 3 Stratified Cox regression to evaluate risk factors for recurrence.
In stratified log-rank analysis, recurrence-free survival was significantly different between the adult and pediatric groups (p = 0.0209; Figure 1).
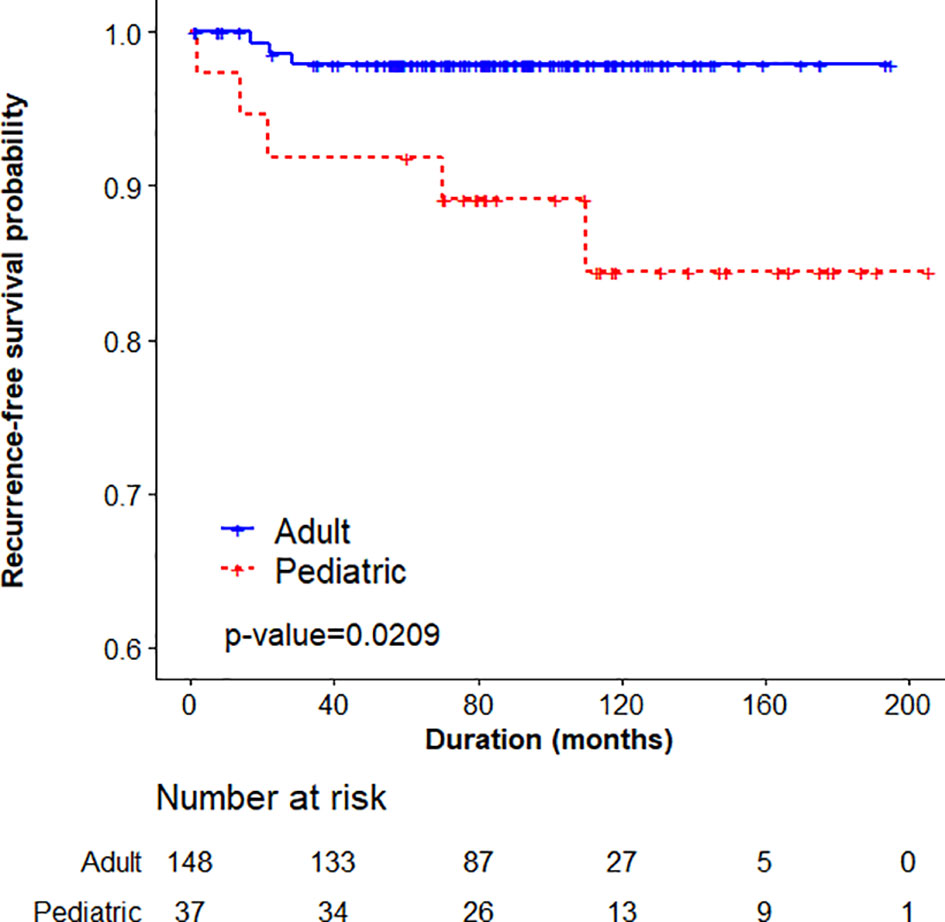
Figure 1 Stratified log-rank analysis comparing adult and pediatric patients.
To the best of our knowledge, this is the first study to examine such a large number of young pediatric patients under the age of 16 years with propensity score matching. Previous studies also included adolescent patients and did not consist of pediatric patients solely (8, 16, 20, 26, 27).
Pediatric DTC is an uncommon malignancy. Although the disease is more aggressive and presents at more advanced stages in this group, the overall prognosis is known to be excellent. Our results show that pediatric patients younger than 16 years have a higher risk of recurrence than adult patients with the same tumor size and matched sex. Pediatric patients showed significantly more central node metastasis and lateral neck node metastasis, which could have had an impact on the higher recurrence probability.
Pediatric patients were reported to have larger lesions than adult patients (median 23.6 vs 19.3 mm), with more frequent lymph node metastases (67.8% vs 42.1%) and distant metastases (19, 28). In this study, pediatric patients were matched to adult patients with the same tumor size to overcome this difference. Young patients were significantly more likely to undergo second treatment such as surgery and radiotherapy. The rate of mutations in the proto-oncogene BRAF was significantly higher in adult patients than that in pediatric patients with PTC (28).
Sherman et al. (29) noted the significance of tumor size; the small size of the thyroid gland in children can lead to earlier extrathyroidal spread of the disease. However, extrathyroidal extension was not more frequent in our study. Reports have shown that although DTC presented more aggressively at the time of diagnosis in children, intensive management elicits a similar clinical outcome in both children and young adults (18, 22). A study comparing patients younger than 10 years, and pediatric patients older than 10 and younger than 18 years, noted no significant differences in tumor size or aggressiveness; they suggested that younger children are more likely to have lymph node metastasis at presentation as well as subsequent metastases (16, 25). Our study showed that pediatric patients showed more aggressive patterns than adult patients with the same cancer size with more frequent central node and lateral node metastasis. More than half of the pediatric patients presented with cervical lymph node metastasis.
Lee et al. showed that the younger the patient at diagnosis, the higher the percentage of PTC, multifocality, ETE, LN metastasis, and lung metastasis. The age at diagnosis was not a predictor of recurrence-free survival, suggesting that multifocality rather than age at diagnosis is an important predictor for recurrence (20). Chaukar et al. suggested a correlation between hormonal influence during puberty and an increased risk of thyroid carcinoma. They observed a near equal distribution of female and male patients in the prepubertal age group (1.5:1), whereas the ratio in patients of 13 to 17 years of age was 3:1, which could suggest a hormonal influence. Since thyroid carcinoma is known to be TSH-dependent, any condition leading to an increase in circulating TSH level in the blood may be associated with an increased risk of thyroid cancer (22). Another study showed that female patients predominantly presented with DTC, although the ratio in the young group was higher, suggesting an association with sex hormone factors (19).
Race was identified as an independent predictor in multivariate analysis, suggesting that non-Caucasian patients are at higher risk of recurrence than Caucasians. Pediatric PTC was associated with lateral node involvement (30). This could somehow explain the higher incidence of recurrent pediatric cancer in our study since our study population only comprised Korean patients, and pediatric patients showed frequent lateral lymph node involvement.
In our study, central lymph node metastasis and lateral neck node metastasis were more frequent. An aggressive operative approach to lymph node resection in experienced hands may be safer when considering complication and recurrence rates compared with less complete resection at a lower volume center (30).
In young children, more stable and progressive disease forms were noted, showing higher cure rates in adolescents (19). Disease-free survival was significantly shorter in the children group than that in the adolescent group, but no significant difference was found in cancer-specific survival between these two groups (25). A previous study on the initial and dynamic risk stratification of pediatric patients showed that reflecting the extent of disease by tumor size, localized invasion, and the number and size of cervical LN metastases was useful for predicting the risk of structurally persistent or recurrent disease (31). Using the Kaplan-Meier analysis, we observed that the incidence of recurrence was significantly higher in the pediatric group than in the matched adult group.
According to the ATA management guidelines for children, total thyroidectomy remains the treatment of choice for pediatric patients with thyroid cancer (32). A study reported that comparable surgical outcome was seen with lobectomy instead of total thyroidectomy in patients with limited disease, such as those with tumors smaller than 2 cm, no lymph node metastasis, and no multifocal disease (27). Considering our results wherein the mean tumor size was 2.33 ± 1.39 cm and the fact that the central node metastasis (73.9%) and lateral neck node metastasis (64.6%) rates were quite high, patients suitable for lobectomy may be rare. Our results suggest that young patients should undergo more thorough preoperative analysis to decide the extent of surgery since loco-regional and distant metastasis may be more frequent.
This study has several limitations, including small sample size, single institution and limitations inherent to retrospective nature of the study. Molecular analysis should be included in future studies.
Pediatric patients showed more aggressive patterns than adult patients with the same cancer size. Central lymph node metastasis and lateral neck node metastasis were more frequent. Recurrence was more significantly observed in stratified log-rank analysis in pediatric patients than in matched adult patients.
There is a need for prospective, collaborative multicenter studies. Future prospective multicenter pediatric studies are required to answer questions regarding the natural history of this condition in pediatric patients.
The data analyzed in this study is subject to the following licenses/restrictions: personal data. Requests to access these datasets should be directed to a2ltc3V5QGF1bWMuYWMua3I=.
The studies involving human participants were reviewed and approved by Institutional Review Board of Yonsei University (IRB 3-2019-0281), Seoul, South Korea. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
SYK, YSL, SMK, HSC, CSP contributed to the conception and design of the study. SYK, HJY and HC organized the database. SL and SJ performed the statistical analyses. SYK wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
This research was supported by faculty research fund of Yonsei University College of Medicine (6-2019-0092) and by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (2017R1E1A1A03070345).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Park S, Jeong JS, Ryu HR, Lee CR, Park JH, Kang SW, et al. Differentiated Thyroid Carcinoma of Children and Adolescents: 27-Year Experience in the Yonsei University Health System. J Korean Med Sci (2013) 28(5):693–9. doi: 10.3346/jkms.2013.28.5.693
2. Holmes L Jr., Hossain J, Opara F. Pediatric Thyroid Carcinoma Incidence and Temporal Trends in the USA (1973-2007): Race or Shifting Diagnostic Paradigm? ISRN Oncol (2012) 2012:906197. doi: 10.5402/2012/906197
3. Kiratli PO, Volkan-Salanci B, Gunay EC, Varan A, Akyuz C, Buyukpamukcu M. Thyroid Cancer in Pediatric Age Group: An Institutional Experience and Review of the Literature. J Pediatr Hematol Oncol (2013) 35(2):93–7. doi: 10.1097/MPH.0b013e3182755d9e
4. Howlader N, Ries LA, Stinchcomb DG, Edwards BK. The Impact of Underreported Veterans Affairs Data on National Cancer Statistics: Analysis Using Population-Based SEER Registries. J Natl Cancer Inst (2009) 101(7):533–6. doi: 10.1093/jnci/djn517
5. Rapkin L, Pashankar FD. Management of Thyroid Carcinoma in Children and Young Adults. J Pediatr Hematol Oncol (2012) 34 Suppl 2:S39–46. doi: 10.1097/MPH.0b013e31824e37a6
6. Millman B, Pellitteri PK. Thyroid Carcinoma in Children and Adolescents. Arch Otolaryngol Head Neck Surg (1995) 121(11):1261–4. doi: 10.1001/archotol.1995.01890110037007
7. Halac I, Zimmerman D. Thyroid Nodules and Cancers in Children. Endocrinol Metab Clin North Am (2005) 34(3):725–44, x. doi: 10.1016/j.ecl.2005.04.007
8. Vaccarella S, Lortet-Tieulent J, Colombet M, Davies L, Stiller CA, Schuz J, et al. Global Patterns and Trends in Incidence and Mortality of Thyroid Cancer in Children and Adolescents: A Population-Based Study. Lancet Diabetes Endocrinol (2021) 9(3):144–52. doi: 10.1016/S2213-8587(20)30401-0
9. Hogan AR, Zhuge Y, Perez EA, Koniaris LG, Lew JI, Sola JE. Pediatric Thyroid Carcinoma: Incidence and Outcomes in 1753 Patients. J Surg Res (2009) 156(1):167–72. doi: 10.1016/j.jss.2009.03.098
10. Moon EK, Park HJ, Oh CM, Jung KW, Shin HY, Park BK, et al. Cancer Incidence and Survival Among Adolescents and Young Adults in Korea. PloS One (2014) 9(5):e96088. doi: 10.1371/journal.pone.0096088
11. Pacini F, Vorontsova T, Demidchik EP, Molinaro E, Agate L, Romei C, et al. Post-Chernobyl Thyroid Carcinoma in Belarus Children and Adolescents: Comparison With Naturally Occurring Thyroid Carcinoma in Italy and France. J Clin Endocrinol Metab (1997) 82(11):3563–9. doi: 10.1210/jc.82.11.3563
12. Demidchik YE, Demidchik EP, Reiners C, Biko J, Mine M, Saenko VA, et al. Comprehensive Clinical Assessment of 740 Cases of Surgically Treated Thyroid Cancer in Children of Belarus. Ann Surg (2006) 243(4):525–32. doi: 10.1097/01.sla.0000205977.74806.0b
13. Tronko MD, Bogdanova TI, Komissarenko IV, Epstein OV, Oliynyk V, Kovalenko A, et al. Thyroid Carcinoma in Children and Adolescents in Ukraine After the Chernobyl Nuclear Accident: Statistical Data and Clinicomorphologic Characteristics. Cancer (1999) 86(1):149–56. doi: 10.1002/(SICI)1097-0142(19990701)86:1<149::AID-CNCR21>3.0.CO;2-A
14. Antonelli A, Miccoli P, Derzhitski VE, Panasiuk G, Solovieva N, Baschieri L. Epidemiologic and Clinical Evaluation of Thyroid Cancer in Children From the Gomel Region (Belarus). World J Surg (1996) 20(7):867–71. doi: 10.1007/s002689900132
15. Baverstock K, Egloff B, Pinchera A, Ruchti C, Williams D. Thyroid Cancer After Chernobyl. Nature (1992) 359(6390):21–2. doi: 10.1038/359021b0
16. O'Gorman CS, Hamilton J, Rachmiel M, Gupta A, Ngan BY, Daneman D. Thyroid Cancer in Childhood: A Retrospective Review of Childhood Course. Thyroid (2010) 20(4):375–80. doi: 10.1089/thy.2009.0386
17. Lazar L, Lebenthal Y, Steinmetz A, Yackobovitch-Gavan M, Phillip M. Differentiated Thyroid Carcinoma in Pediatric Patients: Comparison of Presentation and Course Between Pre-Pubertal Children and Adolescents. J Pediatr (2009) 154(5):708–14. doi: 10.1016/j.jpeds.2008.11.059
18. Kim SS, Kim SJ, Kim IJ, Kim BH, Jeon YK, Kim YK. Comparison of Clinical Outcomes in Differentiated Thyroid Carcinoma Between Children and Young Adult Patients. Clin Nucl Med (2012) 37(9):850–3. doi: 10.1097/RLU.0b013e318262c5d6
19. Motazedian M, Shafiei B, Vatankhah P, Hoseinzadeh S, Mirzababaee M, Fathollahi L, et al. Differentiated Thyroid Carcinoma: Comparison of Histopathologic Characteristics, Clinical Course, and Outcome Between Young Children and Adolescents. Med Oncol (2013) 30(2):506. doi: 10.1007/s12032-013-0506-y
20. Lee YA, Jung HW, Kim HY, Choi H, Kim HY, Hah JH, et al. Pediatric Patients With Multifocal Papillary Thyroid Cancer Have Higher Recurrence Rates Than Adult Patients: A Retrospective Analysis of a Large Pediatric Thyroid Cancer Cohort Over 33 Years. J Clin Endocrinol Metab (2015) 100(4):1619–29. doi: 10.1210/jc.2014-3647
21. Rachmiel M, Charron M, Gupta A, Hamilton J, Wherrett D, Forte V, et al. Evidence-Based Review of Treatment and Follow Up of Pediatric Patients With Differentiated Thyroid Carcinoma. J Pediatr Endocrinol Metab (2006) 19(12):1377–93. doi: 10.1515/JPEM.2006.19.12.1377
22. Chaukar DA, Rangarajan V, Nair N, Dcruz AK, Nadkarni MS, Pai PS, et al. Pediatric Thyroid Cancer. J Surg Oncol (2005) 92(2):130–3. doi: 10.1002/jso.20339
23. Papendieck P, Gruneiro-Papendieck L, Venara M, Acha O, Maglio S, Bergada I, et al. Differentiated Thyroid Carcinoma: Presentation and Follow-Up in Children and Adolescents. J Pediatr Endocrinol Metab (2011) 24(9-10):743–8. doi: 10.1515/JPEM.2011.241
24. Alzahrani AS, Alkhafaji D, Tuli M, Al-Hindi H, Sadiq BB. Comparison of Differentiated Thyroid Cancer in Children and Adolescents (</=20 Years) With Young Adults. Clin Endocrinol (Oxf) (2016) 84(4):571–7. doi: 10.1111/cen.12845
25. Enomoto Y, Enomoto K, Uchino S, Shibuya H, Watanabe S, Noguchi S. Clinical Features, Treatment, and Long-Term Outcome of Papillary Thyroid Cancer in Children and Adolescents Without Radiation Exposure. World J Surg (2012) 36(6):1241–6. doi: 10.1007/s00268-012-1558-4
26. Nam KH LC, Lee J, Chang HS, Chung WY, Choi SH, Park CS. Differentiated Thyroid Carcinoma in Patients Less Than 20 Years of Age at Diagnosis: Clinicopathologic Characteristics and Prognostic Factors. J Korean Surg Soc (2005) 69(6):443–9.
27. Kim K, Lee CR, Kang SW, Lee J, Jeong JJ, Nam KH, et al. Clinical Assessment of Pediatric Patients With Differentiated Thyroid Carcinoma: A 30-Year Experience at a Single Institution. World J Surg (2020) 44(10):3383–92. doi: 10.1007/s00268-020-05598-9
28. Galuppini F, Vianello F, Censi S, Barollo S, Bertazza L, Carducci S, et al. Differentiated Thyroid Carcinoma in Pediatric Age: Genetic and Clinical Scenario. Front Endocrinol (Lausanne) (2019) 10:552. doi: 10.3389/fendo.2019.00552
29. Sherman SI, Angelos P, Ball DW, Byrd D, Clark OH, Daniels GH, et al. Thyroid Carcinoma. J Natl Compr Canc Netw (2007) 5(6):568–621. doi: 10.6004/jnccn.2007.0052
30. Rubinstein JC, Herrick-Reynolds K, Dinauer C, Morotti R, Solomon D, Callender GG, et al. Recurrence and Complications in Pediatric and Adolescent Papillary Thyroid Cancer in a High-Volume Practice. J Surg Res (2020) 249:58–66. doi: 10.1016/j.jss.2019.12.002
31. Sung TY, Jeon MJ, Lee YH, Lee YM, Kwon H, Yoon JH, et al. Initial and Dynamic Risk Stratification of Pediatric Patients With Differentiated Thyroid Cancer. J Clin Endocrinol Metab (2017) 102(3):793–800. doi: 10.1210/jc.2016-2666
Keywords: thyroid cancer, pediatric thyroid cancer, differentiated thyroid cancer, propensity score matched analysis, papillary thyroid cancer
Citation: Kim SY, Yun HJ, Chang H, Kim S-M, Jeon S, Lee S, Lee YS, Chang H-S and Park CS (2022) Aggressiveness of Differentiated Thyroid Carcinoma in Pediatric Patients Younger Than 16 years: A Propensity Score-Matched Analysis. Front. Oncol. 12:872130. doi: 10.3389/fonc.2022.872130
Received: 09 February 2022; Accepted: 28 March 2022;
Published: 26 April 2022.
Edited by:
Ottavio Piccin, University of Bologna, ItalyReviewed by:
Carlotta Giani, University of Pisa, ItalyCopyright © 2022 Kim, Yun, Chang, Kim, Jeon, Lee, Lee, Chang and Park. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Sang Lee, bWVkaWx5c0B5dWhzLmFj
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.