
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 05 April 2022
Sec. Radiation Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.861127
This article is part of the Research TopicStereotactic Body Radiotherapy for Prostate CancerView all 15 articles
 Una Ryg1
Una Ryg1 Therese Seierstad1
Therese Seierstad1 Line Brennhaug Nilsen2
Line Brennhaug Nilsen2 Taran Paulsen Hellebust2,3
Taran Paulsen Hellebust2,3 Linda Holth Djupvik2
Linda Holth Djupvik2 Hilde Gustafson4Jørgen Hydal4
Hilde Gustafson4Jørgen Hydal4 Amar U. Kishan5,6Knut Håkon Hole1,7†
Amar U. Kishan5,6Knut Håkon Hole1,7† Wolfgang Lilleby4*†
Wolfgang Lilleby4*†Background: Up to half of patients with localized prostate cancer experience biochemical relapse within 10 years after definitive radiotherapy. The aim of this prospective study was to investigate the toxicity, dose to the organs at risk (OARs), and efficacy of dose-intensified focal salvage radiotherapy.
Methods and Material: Thirty-three patients (median age 68.8 years) with histologically confirmed relapse after primary definitive radiotherapy were enrolled between 2012 and 2019. No patients had metastases at imaging or in bone marrow aspiration. Twenty-three patients were treated with high dose-rate brachytherapy to the recurrent tumor, defined at multiparametric MRI, with 3 fractions of 10 Gy with two weeks interval, and 10 patients by stereotactic body radiotherapy with 35 Gy to the local recurrence and 25 Gy to the whole prostate in 5 fractions. We used the RTOG-scoring system to grade genitourinary (GU) and gastrointestinal toxicity (GI) at three months (acute), and at 12, 24, and 36 months (late). Dose-volume histogram parameters to the local recurrence and the OARs were obtained and 2 Gy equivalent (EQD2) total dose was calculated using the linear-quadratic model with α/β = 3 Gy. Efficacy was assessed by the progression-free interval and overall survival.
Results: Median follow-up time was 81 months (range 21–115). The cumulative moderate to severe GI and GU toxicities were 3.0% (1/33) and 15.2% (5/33). Six patients had grade 1 acute GI toxicity, none had grade 2 or 3. One patient had grade 3 acute GU toxicity, two had grade 2, and fourteen had grade 1. One patient had late GI toxicity grade 2 and eight had grade 1. Four patients had late GU toxicity grade 2 and eight had grade 1. No patients had grade 3 late toxicity. The mean total D90 to the recurrent tumor was 77.7 ± 17.0 Gy. The mean total rectum D2cc was 17.0 ± 7.9 Gy and the mean total urethra D0.1cc was 29.1 ± 8.2 Gy. Twenty-eight patients had re-irradiation without androgen deprivation therapy (ADT). Nine of these are still relapse-free and 10 had a recurrence-free interval longer than 2 years.
Conclusion: The toxicity of salvage radiotherapy was mild to moderate. One-third of the patients achieved long-term stable disease without ADT and one-third had a recurrence-free interval longer than 2 years. Some patients progressed rapidly and probably did not benefit from re-irradiation.
The primary treatment options for localized prostate cancer are radiotherapy and radical prostatectomy. Biochemical relapse occurs in up to half of the patients (1–5). In contrast to the management of recurrence after prostatectomy, optimal management of recurrence after radiotherapy remains unclear due to the lack of large prospective studies in this setting (6). Even the management of a true local recurrence after definitive radiotherapy is controversial and consensus recommendation is limited (6).
Androgen deprivation therapy (ADT) is often used for radio-recurrence, but is non-curative and is associated with impaired quality of life. Local treatment could postpone the onset of ADT and thereby the development of castration-resistant disease, and potentially cure the patient (7).
Salvage prostatectomy has the longest history of use for local treatment of intra-prostatic recurrence but suffers from significant side effects. Re-irradiation has been considered to induce serious toxicity. However, more focal radiotherapies such as brachytherapy (BT) and stereotactic body radiotherapy (SBRT) are less invasive compared to prostatectomy and may circumvent the problem of overdosage to critical structures (6). This can be achieved by applying inhomogeneous dose patches that lower the dose to the whole gland and preferably re-irradiate the local recurrent tumor only. One major concern of applying salvage irradiation is that the tolerance dose to the urothelium and rectal mucosa may limit the sufficient dose delivered to the tumor. To avoid unacceptable toxicity one can use technical strategies that spare the urethra and the rectum.
A recent Delphi consensus paper investigated the expert opinion on salvage re-irradiation and reported increasing interest (8). A recent large meta-analysis reported that the genitourinary toxicity rate for re-irradiation, particularly for SBRT and high dose-rate (HDR)-BT, were significantly less than those reported after salvage prostatectomy, high-intensity focused ultrasound (HIFU), and cryotherapy (6, 9). To establish re-irradiation as a treatment option results from prospective studies with sufficient long follow-up is highly warranted (6, 7, 9–11).
Herein we report prospectively recorded acute and late gastrointestinal (GI) and genitourinary (GU) toxicity and long-term clinical outcome after re-irradiation with HDR-BT and SBRT.
The Regional Committee for Medical Research Ethics southeast Norway approved this prospective study of focal salvage re-irradiation (2011/954) and all patients provided written informed consent.
The main inclusion criteria were local recurrence after primary curative intended external beam radiotherapy (EBRT), defined as prostate-specific antigen (PSA) >nadir + 2 ng/ml, and no metastases neither at imaging nor in bone marrow aspiration samples. Further inclusion criteria were PSA <10 ng/ml, PSA doubling time >6 months, more than 2 years recurrence-free interval since primary radiotherapy, and ECOG 0–1 with a life expectancy >5 years.
Between 2012 and 2019, we included 33 patients previously treated with conformal RT of 70–78 Gy to the prostate and seminal vesicles (Table 1). At primary treatment, the patients were diagnosed with intermediate (n = 13) or high-risk disease (n = 20) according to the D’Amico risk classification system (12). At recurrence, all patients had multiparametric MRI of the pelvis and lower lumbar spine, 24 had FACBC PET/CT (trans-1-amino-3-18F-fluorocyclobutanecarboxylic-acid positron emission tomography/computed tomography) and two had PSMA PET/CT (prostate-specific membrane antigen) to localize the recurrence and exclude metastatic disease. Intra-prostatic tumor recurrence was histologically verified in all but one patient.
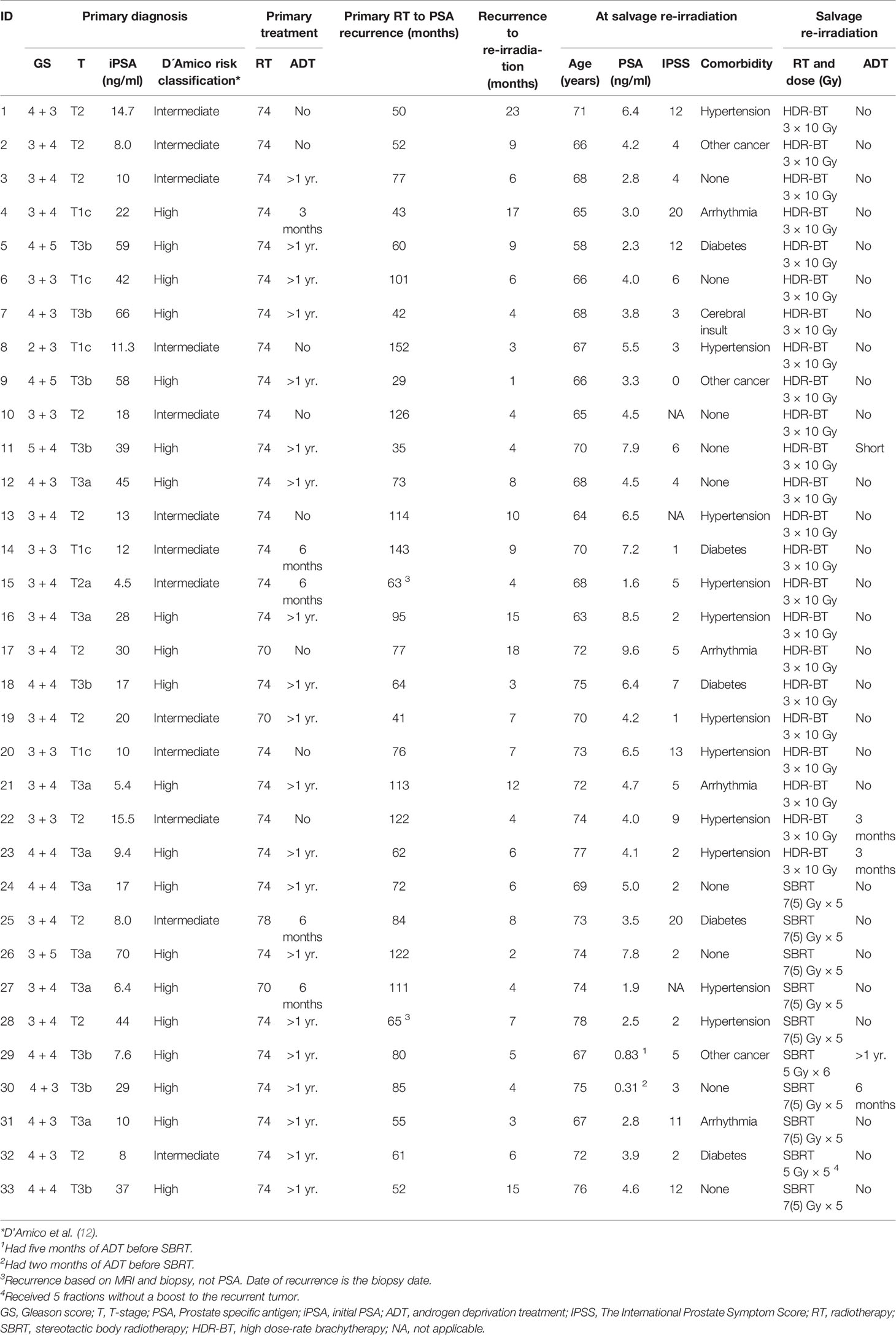
Table 1 Detailed overview of patient characteristics and treatment.
The median age of the study population was 69.8 years (interquartile range (IQR) 6.8), and the median PSA was 4.1 ng/ml (IQR 3.8). The median time from primary radiotherapy to biochemical recurrence was 73.0 months (IQR 52.5). Twenty-eight patients were eugonadal at salvage re-irradiation while five patients received either ongoing or concomitant ADT (Figure 1). The first 23 patients received HDR-BT, and the last 10 patients received SBRT. A detailed overview of the study population and treatment is shown in Table 1.
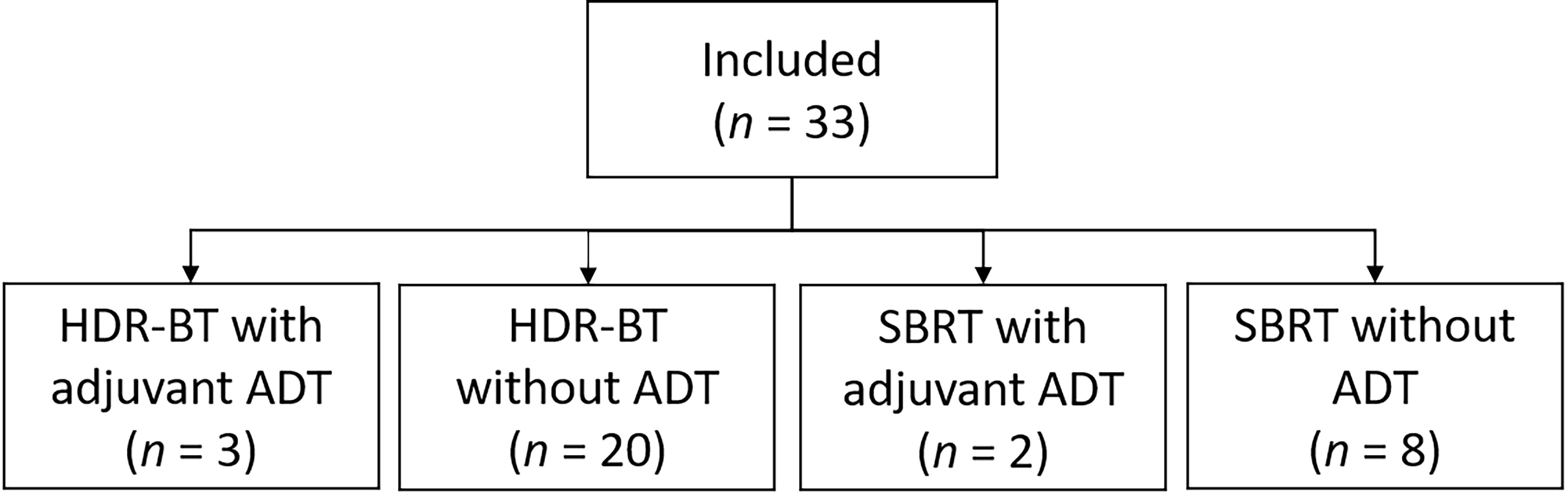
Figure 1 Overview of the salvage treatment. HDR-BT, high dose-rate brachytherapy; ADT, androgen deprivation therapy; SBRT, stereotactic body radiotherapy.
Multiparametric MRI prior to salvage re-irradiation included morphological T2-weighted, diffusion-weighted (DW), and dynamic contrast enhanced (DCE) sequences of the prostate. The acquisition protocol is described in detail in Tulipan et al. (13). The technical standard of the imaging protocol was in accordance with current technical requirements for prostate MRI (14). One radiologist with more than nine years of experience in prostate cancer MRI (KH) prospectively interpreted the examinations for study inclusion and biopsy guidance. The other radiologist (UR) with four years of experience retrospectively reviewed all the MRI examinations both from primary diagnosis, if available, and from the time of recurrence, with the purpose of comparing the site of the primary and recurrent tumor.
Twenty-three patients received mainly focal HDR-BT in three fractions every second week using the microSelectron HDR 192Ir source (Nucletron B.V., Veenendaal, The Netherlands). The planning aim was 10 Gy to the gross tumor volume (GTV), which for the majority of the patients (n = 20) was defined as the recurrent tumor identified at imaging (Figure 2). The HDR-BT procedure has previously been described in detail in Raabe et al. (15). In short, the patients were under general anesthesia and in the lithotomy position. A Foley catheter was placed in the bladder. Guided by transrectal ultrasound (US) the needles were inserted into the gross tumor volume (GTV) through the perineum. The recurrent tumor, prostate gland, rectal wall, and the urethra (cylinder with a radius of 3 mm) were delineated by the oncologist on US images acquired both before and after needle insertion (Figure 3). The delineation of the recurrent tumor was guided by multiparametric MRI (Figure 2). Intra-operative treatment planning, namely, inverse plan optimization and consecutive graphical adjustments, was performed using Oncentra Prostate Vs.4.1.6 (Nucletron). Source positions 3 mm or closer to the urethra were not allowed to be used. Initial optimization settings and dose constraints are found in Supplementary Tables 1–3.
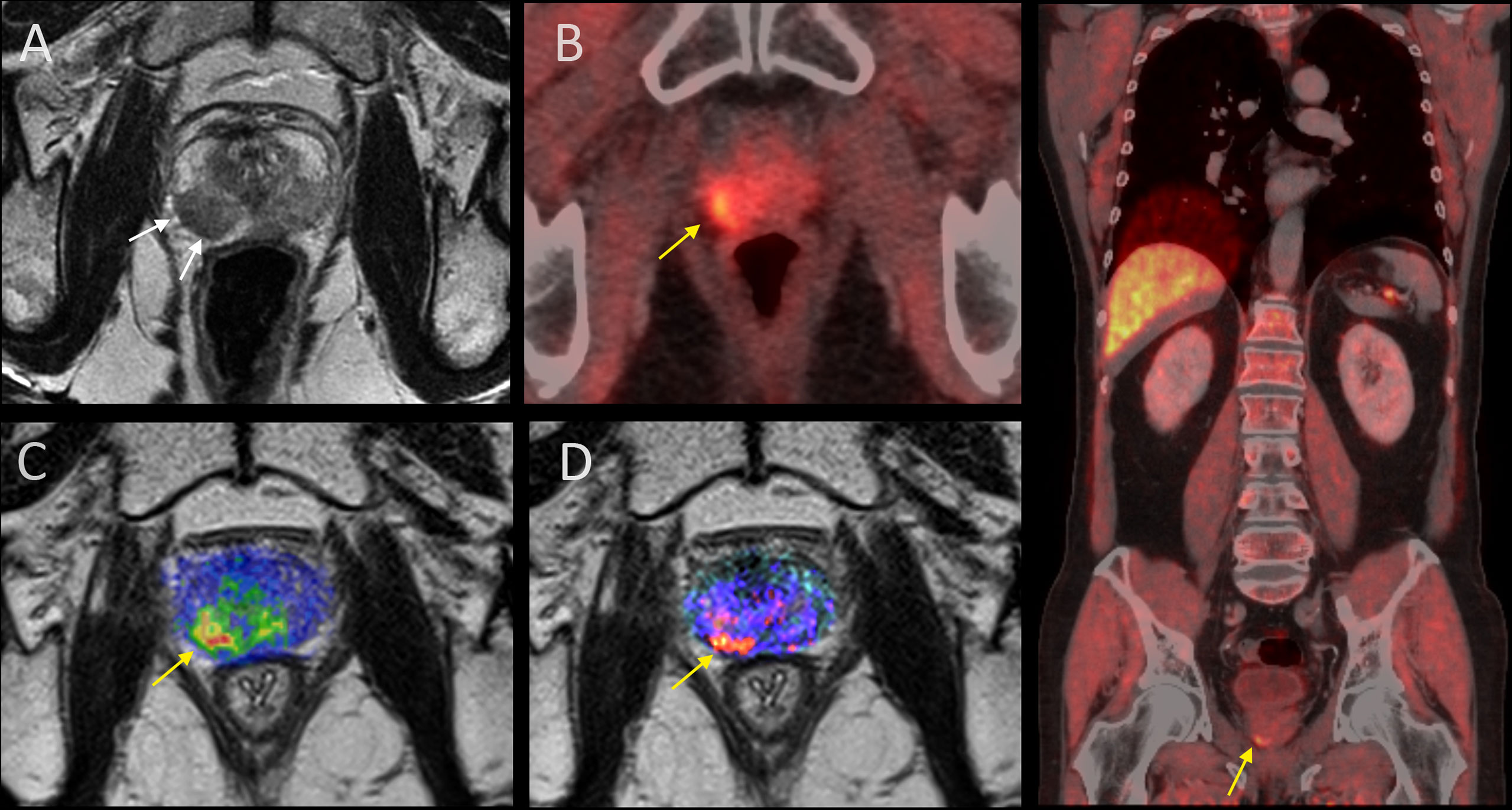
Figure 2 Primary and radio-recurrent prostate cancer at imaging. (A) Primary tumor at T2W MRI (white arrows). (B–D) Recurrent tumor (yellow arrow) at FACBC PET/CT, diffusion weighting overlaid on T2W MRI, and dynamic contrast-enhanced MRI overlaid on T2W MRI. To the right: Whole-body FACBC PET/CT to prove true local recurrence only (yellow arrow).
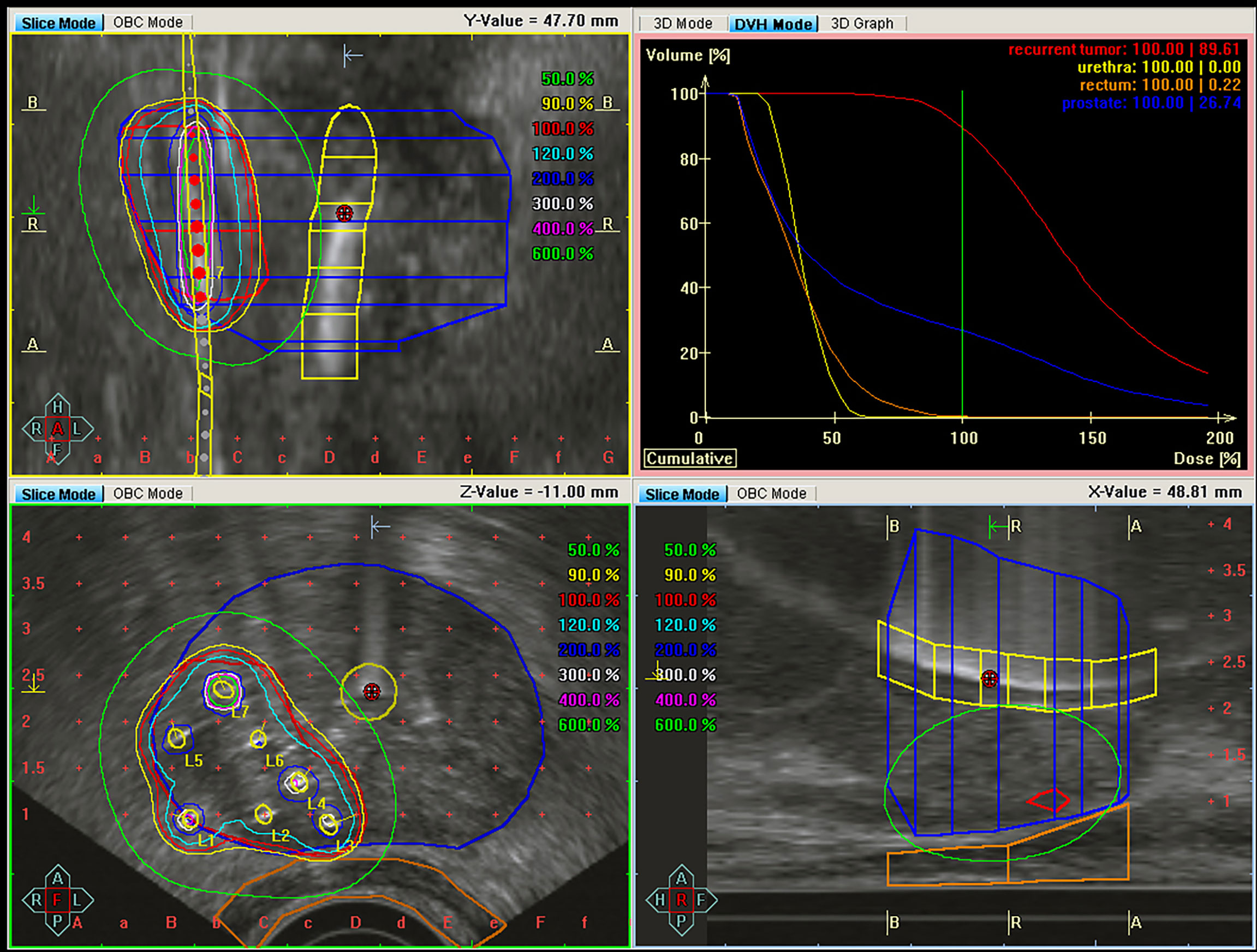
Figure 3 Dose distribution for high dose-rate brachytherapy of the same patient as in Figure 2 showing the coronal (upper left), transversal (lower left), and sagittal (lower right) plane. The recurrent tumor (red), prostate (blue), urethra (yellow), and rectum wall (brown) are delineated. Air-filled gel has been inserted in the urethra catheter to visualize the urethra in the ultrasound images. The dose-volume histograms (upper right quadrant) show the highly conformal dose distribution, sparing the rectum and urethra, achieved by brachytherapy.
For patients 9, 11, and 23 (Table 1), the whole prostate gland, excluding the urethra, was defined as the GTV. For patient 23, the GTV included only the recurrent tumor on the two last fractions.
Ten patients received SBRT with 6MV flattening filter-free volumetric arc therapy (VMAT) delivered on a linear accelerator (Varian TrueBeam ™ STx, Varian Medical Systems, Palo Alto, USA). Fiducial gold markers implanted as strands along the urethra and as cubes in the prostate prior to treatment planning assisted the image-guided RT (daily cone-beam CT for target positioning and verification). The SBRT was delivered in five fractions as a simultaneous integrated boost with a planning aim of 35 Gy to the recurrent tumor and 25 Gy to the prostate gland (n = 8) or in six fractions with a planning aim of 30 Gy to the whole prostate gland (n = 1). One patient (patient 32) received only five fractions without an integrated boost to the tumor. The fractions were delivered every other day. The delineation of target volumes (recurrent tumor and/or prostate gland) and organs at risk (OARs) (urethra, bladder, rectum, anal canal, and femoral heads), and treatment planning was performed using Raystation 5 (RaySearch Laboratories, Stockholm, Sweden). An isotropic planning target volume (PTV) margin of 3 mm was used for both the recurrent tumor and the prostate. The treatment plans were optimized with a steep dose gradient to the urethra and normalized to a prescription volume that excluded the urethra with a margin of 3–5 mm. Clinical goals and dose constraints are found in Supplementary Tables 4, 5. Patient-specific quality assurance of the SBRT plans was performed prior to the onset of treatment using the ArcCheck® phantom (Sun Nuclear Corporation, Melbourne, USA).
Dose to 90% (D90) of the target volumes (recurrent tumor/prostate) were found from the dose volume histograms. Also, the minimum dose to the most exposed 2 and 0.1 cubic centimeter (D2cc and D0.1cc) were recorded for the rectum and urethra, respectively. The linear-quadratic model was used to calculate 2 Gy equivalent (EQD2) total dose, assuming α/β = 3 Gy for both the recurrent tumor/prostate and for the OARs.
We used the toxicity criteria of the Radiation Therapy Oncology Group (RTOG) (16) to grade gastrointestinal (GI) and genitourinary (GU) toxicity at three months (acute), and at 12, 24, and 36 months (late). RTOG-grading ceased if patients received additional treatment such as HIFU, prostatectomy, or chemotherapy.
Patients were followed every three months for the first two years, and every six months for the following years. The clinical outcome was measured as the recurrence-free interval from re-irradiation to the second recurrence, defined as PSA >2 ng/ml above nadir after salvage re-irradiation (8).
Data are presented with descriptive statistics. We calculated Kaplan–Meier estimates for recurrence-free and overall survival after re-irradiation. To assess the association between dose and late toxicity, we selected the highest RTOG-scoring of the three reported late time points. We performed subgroup analyses to investigate parameters that could identify the patients who had the highest benefit from salvage re-irradiations. Data were analyzed and figures created using Prism 6 for Mac OS X version 6.0f (GraphPad Software Inc., San Diego, CA).
Figure 4 shows the course of RTOG-graded toxicity for each patient prior to, and 3, 12, 24, and 36 months after salvage re-irradiation. The cumulative moderate to severe GI and GU toxicities were 3.0% (1/33) and 15.2% (5/33). Before re-irradiation, 8 had grade 1 GI toxicity, and 7 had grade 1 GU toxicity. At 3 months, six patients had grade 1 acute GI toxicity while none had grade 2 or 3. Fourteen patients had grade 1 acute GU toxicity, two had grade 2, and one had grade 3. At later time points, eight patients had late GI toxicity grade 1, and one had grade 2. Eight had grade 1 late GU toxicity and four had grade 2. No patients had grade 3 late GI or GU toxicity.
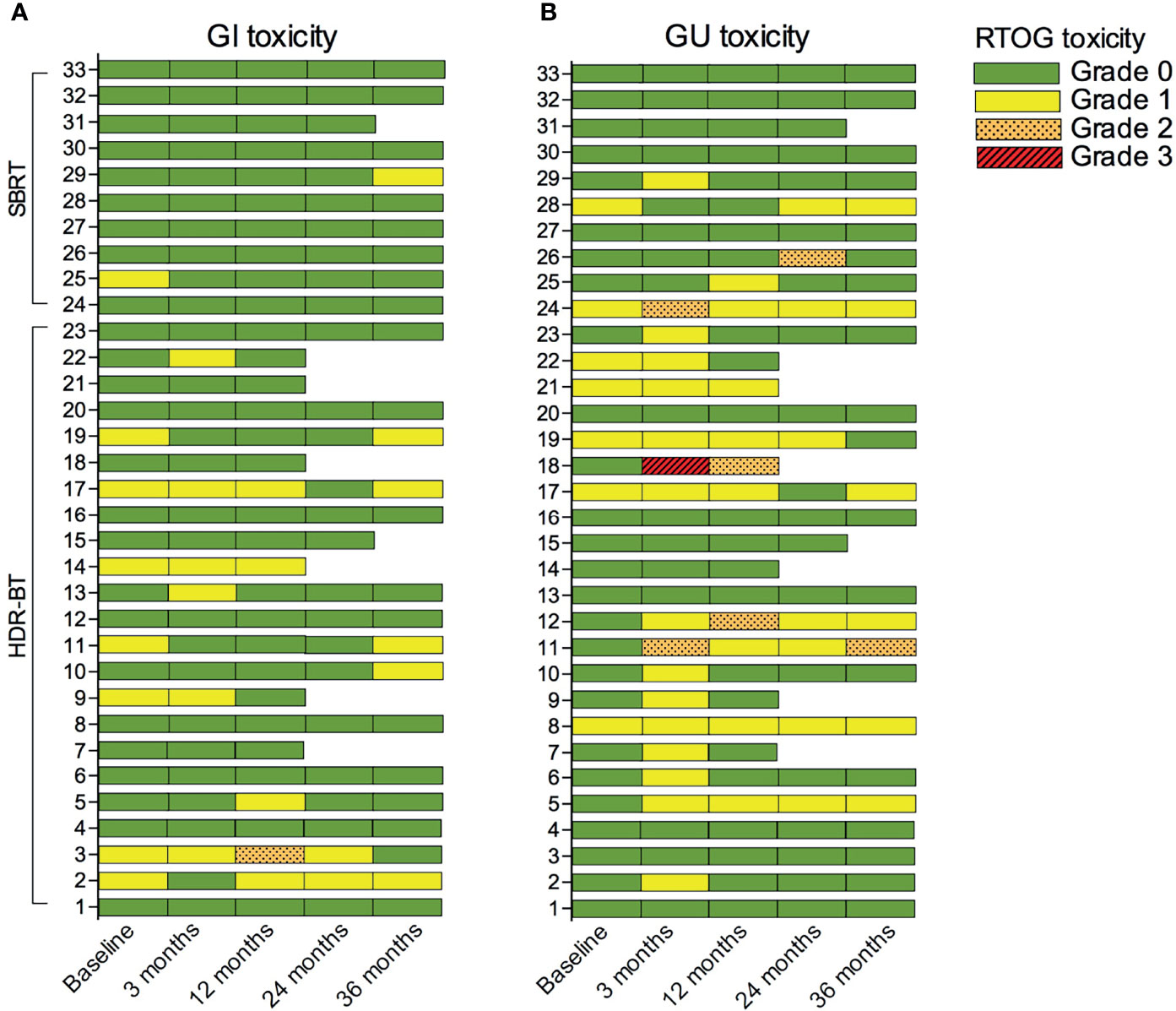
Figure 4 RTOG-graded gastrointestinal (GI) (A) and genitourinary (GU) (B) toxicity before (baseline) and following salvage re-irradiation. RTOG grading ceased if patients received additional local treatment such as HIFU, prostatectomy, or chemotherapy. HDR-BT, High dose-rate brachytherapy; SBRT, Stereotactic body radiotherapy.
Eight patients received additional treatment after re-irradiation. The remaining 25 patients had toxicity scored at 36 months. Compared to baseline, only two (patients 10 and 29) reported increased GI toxicity, and three (patients 5, 11, and 12) reported increased GU toxicity. Patient 18, who experienced severe toxicity, had poorly regulated diabetes.
The mean total D90 to the local recurrence was 77.7 ± 17.0 Gy. The mean total D2cc for the rectum was 17.0 Gy (SD 7.9), and the mean total D0.1cc for the urethra was 29.1 Gy (SD 8.2). Only the contribution from the re-irradiation is included in these figures. We found no association between doses to rectum and urethra from the re-irradiation, and toxicity (Figure 5).
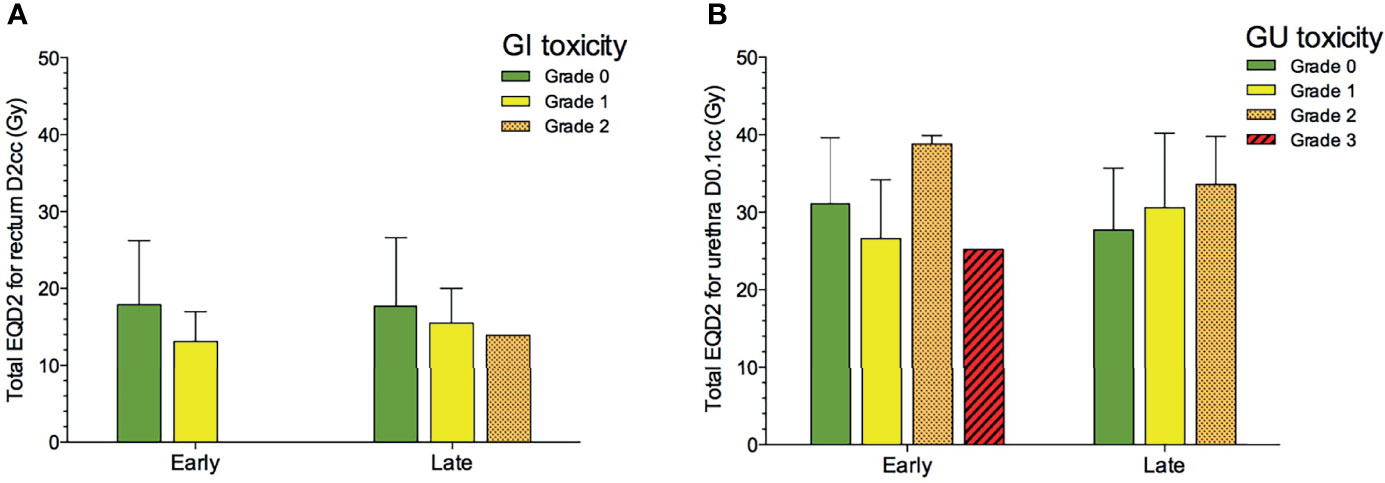
Figure 5 Total EQD2 for rectum D2cc (A) and urethra D0.1cc (B) from the re-irradiation and RTOG-graded gastrointestinal (GI) and genitourinary (GU) toxicity after salvage re-irradiation (n = 33). Bars represent mean values, and whiskers SD.
During the median follow-up after re-irradiation of 81 months (range 21–115), two patients died, one of prostate cancer and one of complications following aortic dissection (Figure 6A). For the entire cohort, the median biochemical progression-free survival after re-irradiation was 40 months. For the 22 patients who relapsed, the median time to secondary recurrence was 24 months (range 7–85). Data for individual patients are reported in Figure 7. Eleven patients, including the patient who died of complications, did not relapse, whereas 22 had a second recurrence, four within one year and six within the second year. Twelve patients had a recurrence-free interval longer than two years.
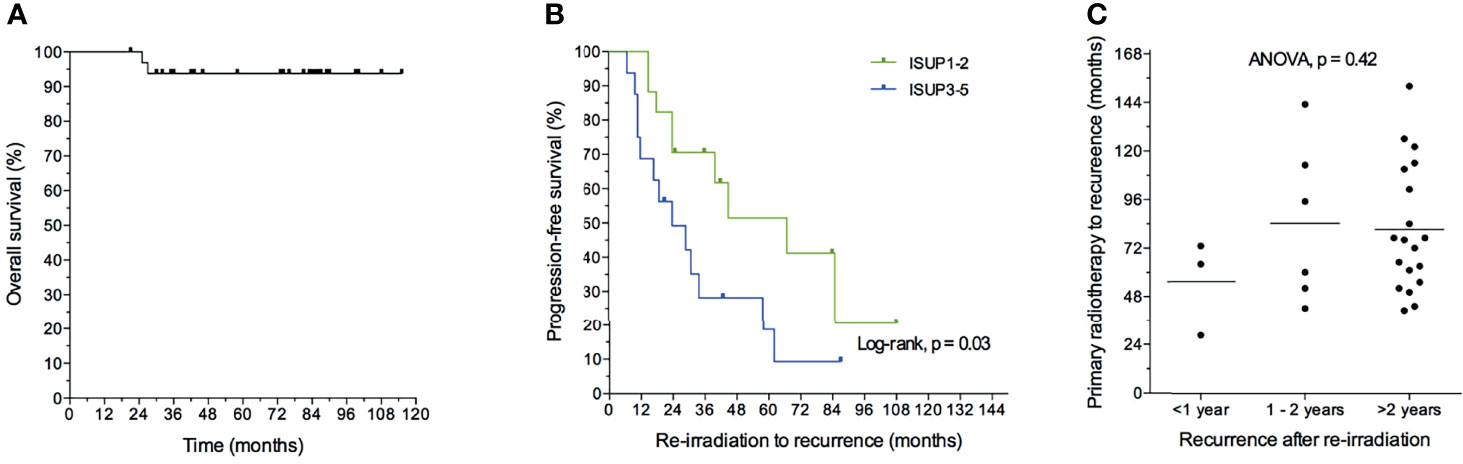
Figure 6 Kaplan–Meier estimate of overall survival (A) and progression-free survival (B) after re-irradiation without androgen deprivation treatment (n = 28). Time to first recurrence for patients recurring within one, two, or more than two years after re-irradiation (C).
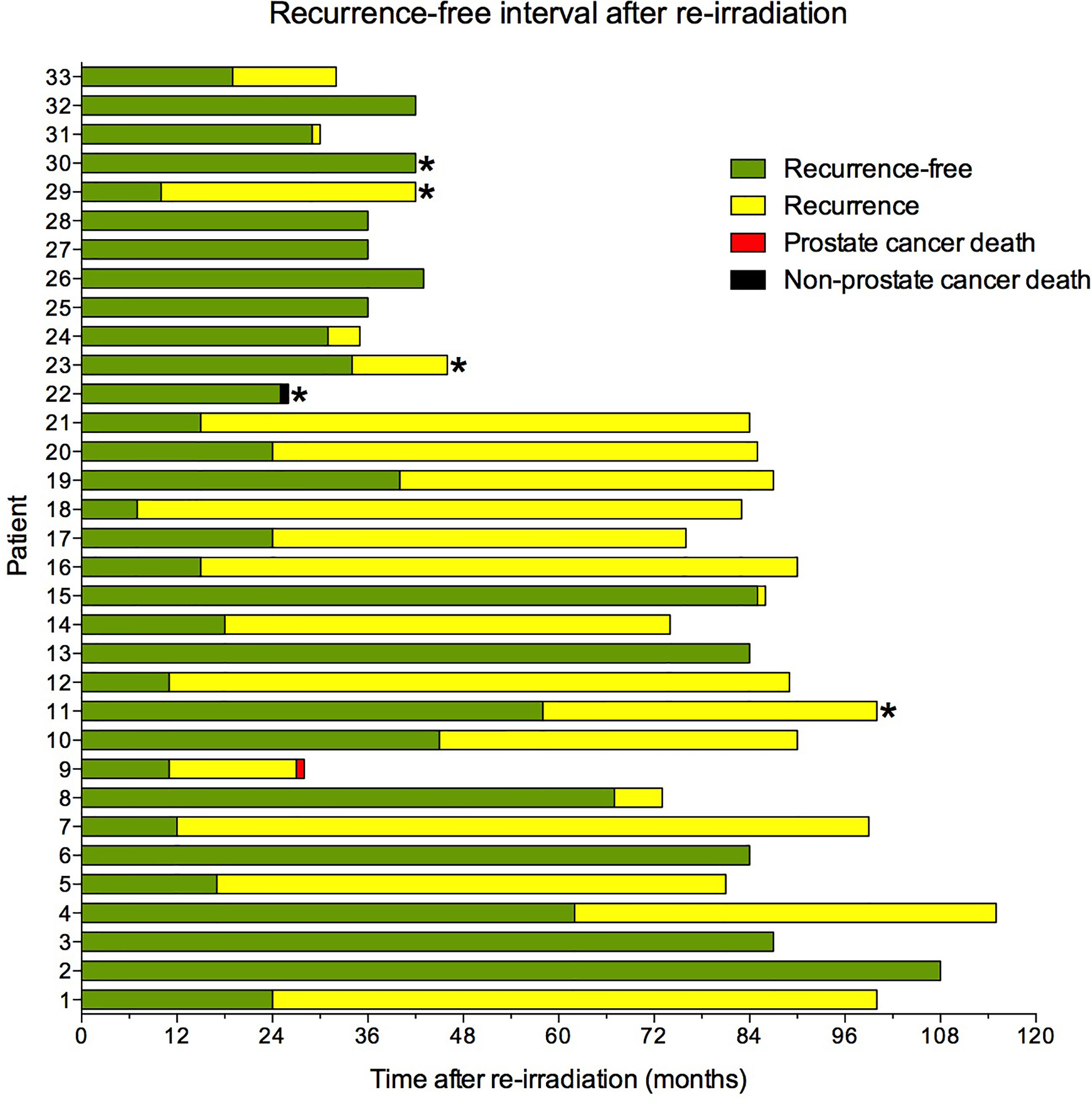
Figure 7 Recurrence-free interval after re-irradiation. *Patients who received androgen deprivation treatment at salvage re-irradiation.
Twenty-eight patients (85%) had salvage radiotherapy without ADT. Nine of these 28 (32%) are still relapse-free, 10 (36%) had a recurrence-free interval longer than two years, and nine (32%) patients relapsed within the two years.
The clinical goal of re-irradiation is to eradicate the recurrent tumor and/or to postpone the onset of ADT. Some patients had a short recurrence-free interval after re-irradiation and probably limited clinical benefit. We sought to identify predictive parameters and hypothesized that less aggressive tumors would benefit the most. We therefore investigated whether the short time from primary radiotherapy to recurrence and low ISUP (International Society of Urological Pathology) grade groups, were markers of a long-term effect of salvage re-irradiation. No other clinical parameters were significant.
The median PFS after re-irradiation was 67 months for patients with ISUP grade groups 1–2 compared to 24 months for ISUP grade groups 3–5. Patients with ISUP grade groups 1–2 had significantly longer time from re-irradiation to recurrence and thus longer progression-free survival (Figure 6B, log-rank test; p = 0.03). However, time from primary radiotherapy to recurrence was not a significant marker of early recurrence after re-irradiation (Figure 6C).
Sixteen patients had MRI both at primary diagnosis and at first recurrence. For 15 of these patients, the recurrent tumor occurred within the extent of the primary tumor (Figure 2). The extent of the primary tumor for the last patient could not be assessed due to artifacts from air in the rectum.
This prospective study reports toxicity and long-term clinical outcome after salvage re-irradiation of localized intra-prostatic recurrence. The study cohort consisted of 33 patients who initially were treated with primary EBRT (70–78 Gy). All had a true local recurrence verified by biopsy and no metastases at imaging or in bone marrow samples. For most patients (28/33) salvage re-irradiation was delivered without androgen deprivation therapy. Overall, the GU and GI toxicity was mild to moderate. One-third of the patients had a biochemical relapse within the first two years, one third relapsed later than two years, and one-third of the patients are still relapse-free.
There are several studies that have reported results from salvage re-irradiation (6, 7, 10, 11, 17). However, there is a large heterogeneity among the reported studies: different primary treatment (prostatectomy, cryotherapy, HIFU, low dose-rate (LDR) brachytherapy, EBRT, and combinations), limited follow-up time, peri-salvage use and inconsistent reporting of ADT, and retrospective study design. The limited GU/GI toxicity in our patients is in line with the reasonable toxicity reported in the prospective phase II RTOG-0526 trial (17) and two recent large systematic reviews and meta-analyses (6, 7).
In the RTOG-0526 applying salvage LDR-BT 14% had grade 3 GU toxicity compared to 3% in our study. Because only one patient in our study had grade 3 GU toxicity, the data is too sparse to assess if this was associated with primary and salvage treatments. The patients in the RTOG-0526 study received 78 Gy/39 fractions or 81 Gy/45 fractions, a slightly higher dose than in our cohort. Nearly all patients in the RTOG-0526 study had whole-gland salvage LDR brachytherapy, whereas we used focal HDR-BT/SBRT and delivered a boosted dose to the recurrent tumor with pre-specified low tolerance dose to the urethra (Supplementary Tables 3, 5).
The 2-year biochemical recurrence-free survival was 68% (19 of 28 patients). In the review from Valle et al. 2-year recurrence-free survival was 62% for SBRT and 77% for HDR-BT, however, about 40% of these patients received peri-salvage ADT (6). Corkum et al. (7) reported the random effect of biochemical recurrence-free survival (BRFS) to be 60% with a significant heterogeneity (50–70%). Crook et al. have recently published their long-term clinical outcome of the RTOG-0526 trial and found a 5-year disease-free survival of 61%. Their results seem in line with ours, but they had longer follow-up time, excluded high-risk patients, and permitted up to six months of peri-salvage ADT. The majority of our patients had high-risk disease.
In the setting of radio-recurrence, salvage prostatectomy and ADT are the guideline-recommended standard options. A longstanding principle in radiation oncology is that after EBRT, re-irradiation will exceed normal tissue tolerances leading to potentially serious toxicity (7–9). A recent ESTRO ACROP consensus paper agrees that re-irradiation is a feasible therapeutic option for selected patients (8). The meta-analyses from Valle et al. reported significantly less GU toxicity rates for SBRT and BT than after prostatectomy, HIFU, and cryotherapy (6, 9). In the current study, we demonstrate that re-irradiation, without rectal spacer devices, is feasible and tolerable provided stringent dose constraints to the urethra and rectum (Supplementary Tables 3, 5). In the future, the assessment of germline variants that predict clinical radio-sensitivity could be implemented to improve patient selection and further reduce toxicity (18).
The therapeutic goal of re-irradiation is the eradication of the recurrence or substantial delay of onset of ADT and subsequent development of castration-resistant disease. One-third of the patients in our study had an early second biochemical relapse within two years, indicating that not all patients will benefit from re-irradiation. The only marker of poor clinical outcome was the high ISUP grade group of the primary tumor. Two-thirds of the patients saw clinical benefits, more than 2-years BFS, probably because the patients were carefully selected by strict inclusion criteria and thorough imaging to localize the site and extent of the recurrence and exclude metastatic disease. The ESTRO APCO Delphi consensus also agrees on and highlights the need for strict inclusion criteria and state-of-the-art imaging (8).
All recurrences occurred within the extent of the primary tumor for the 15 patients in which we had MRI with sufficient image quality at primary diagnosis. Jalloh et al. (19) also found that nearly all recurrences were within the extent of the primary index tumor. These findings indicate that the radiotherapy of primary prostate cancer could be improved by dose escalation (20). Modern dose painting techniques may deliver increased dose selectively to the radio-persisting intra-prostatic lesion without increasing the dose to the OARs (21).
The major limitations of our study are the limited sample size and the lack of a control group. The minor limitations are that not all patients had the same treatment, some had HDR-BT, some had SBRT, and five patients received peri-salvage ADT. The major strengths are the prospective design, clearly defined inclusion criteria, modern ultra-hypofractionated image-guided radiotherapy, a long follow-up time, and state-of-the-art imaging. Furthermore, most of the patients (28/33) did not have ADT. As such, our prospective study does not provide a high level of evidence but adds to the body of knowledge.
Re-irradiation of intra-prostatic recurrence with HDR-BT and SBRT is feasible and resulted in mild to moderate GU or GI toxicity. Two-thirds of the patients experienced more than 2-years BFS, one-third are still recurrence-free without ADT. Some patients progressed rapidly and may not have benefitted from salvage radiotherapy. Careful selection of patients is needed.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by The Regional Committee for Medical Research Ethics South East Norway. The patients/participants provided their written informed consent to participate in this study.
Conceptualization, TS, KH, AK, and WL. Methodology, UR, TS, LN, TH, LD, HG, KH, and WL. Formal analysis, TS. Investigation, UR, TS, LN, TH, LD, HG, JH, KH, and WL. Resources, WL. Writing—Original Draft, UR, TS, KH, and WL. Writing—Review & Editing, UR, TS, LN, TH, LD, HG, JH, AK, KH, and WL. Visualization, TS and KH. Supervision, TS, KH, and WL. Funding Acquisition, WL. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
We would like to thank the Raagholt Foundation for their generous support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.861127/full#supplementary-material
1. Kupelian PA, Mahadevan A, Reddy CA, Reuther AM, Klein EA. Use of Different Definitions of Biochemical Failure After External Beam Radiotherapy Changes Conclusions About Relative Treatment Efficacy for Localized Prostate Cancer. Urology (2006) 68:593–8. doi: 10.1016/j.urology.2006.03.075
2. Cahlon O, Zelefsky MJ, Shippy A, Chan H, Fuks Z, Yamada Y, et al. Ultra-High Dose (86.4 Gy) IMRT for Localized Prostate Cancer: Toxicity and Biochemical Outcomes. Int J Radiat Oncol Biol Phys (2008) 71:330–7. doi: 10.1016/j.ijrobp.2007.10.004
3. Michalski J, Winter K, Roach M, Markoe A, Sandler HM, Ryu J, et al. Clinical Outcome of Patients Treated With 3D Conformal Radiation Therapy (3D-CRT) for Prostate Cancer on RTOG 9406. Int J Radiat Oncol Biol Phys (2012) 83:e363–370. doi: 10.1016/j.ijrobp.2011.12.070
4. Nomiya T, Tsuji H, Toyama S, Maruyama K, Nemoto K, Tsujii H, et al. Management of High-Risk Prostate Cancer: Radiation Therapy and Hormonal Therapy. Cancer Treat Rev (2013) 39:872–8. doi: 10.1016/j.ctrv.2013.04.003
5. Liesenfeld L, Kron M, Gschwend JE, Herkommer K. Prognostic Factors for Biochemical Recurrence More Than 10 Years After Radical Prostatectomy. J Urol (2017) 197:143–8. doi: 10.1016/j.juro.2016.07.004
6. Valle LF, Lehrer EJ, Markovic D, Elashoff D, Levin-Epstein R, Karnes RJ, et al. A Systematic Review and Meta-Analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur Urol (2021) 80:280–92. doi: 10.1016/j.eururo.2020.11.010
7. Corkum MT, Mendez LC, Chin J, D'souza D, Boldt RG, Bauman GS. A Novel Salvage Option for Local Failure in Prostate Cancer, Reirradiation Using External Beam or Stereotactic Radiation Therapy: Systematic Review and Meta-Analysis. Adv Radiat Oncol (2020) 5:965–77. doi: 10.1016/j.adro.2020.04.022
8. Jereczek-Fossa BA, Marvaso G, Zaffaroni M, Gugliandolo SG, Zerini D, Corso F, et al. Salvage Stereotactic Body Radiotherapy (SBRT) for Intraprostatic Relapse After Prostate Cancer Radiotherapy: An ESTRO ACROP Delphi Consensus. Cancer Treat Rev (2021) 98:102206. doi: 10.1016/j.ctrv.2021.102206
9. Zheng J, Crook J. Mastering the Landscape of Postradiation Local Prostate Salvage Therapy. Eur Urol (2021) 80:293–4. doi: 10.1016/j.eururo.2021.04.032
10. Crook J, Rodgers JP, Pisansky TM, Trabulsi EJ, Amin MB, Bice W, et al. Salvage Low-Dose-Rate Prostate Brachytherapy: Clinical Outcomes of a Phase 2 Trial for Local Recurrence After External Beam Radiation Therapy (NRG Oncology/Xxxx). Int J Radiat Oncol Biol Phys (2021) 112(5):1115–22. doi: 10.1016/j.ijrobp.2021.10.138
11. Munoz F, Fiorica F, Caravatta L, Rosa C, Ferella L, Boldrini L, et al. Outcomes and Toxicities of Re-Irradiation for Prostate Cancer: A Systematic Review on Behalf of the Re-Irradiation Working Group of the Italian Association of Radiotherapy and Clinical Oncology (AIRO). Cancer Treat Rev (2021) 95:102176. doi: 10.1016/j.ctrv.2021.102176
12. D'amico AV, Moul J, Carroll PR, Sun L, Lubeck D, Chen MH. Cancer-Specific Mortality After Surgery or Radiation for Patients With Clinically Localized Prostate Cancer Managed During the Prostate-Specific Antigen Era. J Clin Oncol (2003) 21:2163–72. doi: 10.1200/jco.2003.01.075
13. Tulipan AJ, Hole KH, Vlatkovic L, Revheim ME, Reijnen JS, Willoch F, et al. Localization of Radio-Recurrence Within the Prostate: Anti-3-18F-FACBC PET/CT Compared With Multiparametric MRI Using Histopathology as Reference Standard. Acta Radiol (2019) 60:1028–38. doi: 10.1177/0284185118810977
14. Barentsz JO, Richenberg J, Clements R, Choyke P, Verma S, Villeirs G, et al. ESUR Prostate MR Guidelines 2012. Eur Radiol (2012) 22:746–57. doi: 10.1007/s00330-011-2377-y
15. Raabe NK, Lilleby W, Tafjord G, Aström L. [High Dose Rate Brachytherapy in Prostate Cancer in Norway]. Tidsskr Nor Laegeforen (2008) 128:1275–8.
16. Cox JD, Stetz J, Pajak TF. Toxicity Criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys (1995) 31:1341–6. doi: 10.1016/0360-3016(95)00060-c
17. Crook JM, Zhang P, Pisansky TM, Trabulsi EJ, Amin MB, Bice W, et al. A Prospective Phase 2 Trial of Transperineal Ultrasound-Guided Brachytherapy for Locally Recurrent Prostate Cancer After External Beam Radiation Therapy (NRG Oncology/RTOG-0526). Int J Radiat Oncol Biol Phys (2019) 103:335–43. doi: 10.1016/j.ijrobp.2018.09.039
18. Kishan AU, Marco N, Schulz-Jaavall MB, Steinberg ML, Tran PT, Juarez JE, et al. Germline Variants Disrupting microRNAs Predict Long-Term Genitourinary Toxicity After Prostate Cancer Radiation. Radiother Oncol (2022) 167:226–32. doi: 10.1016/j.radonc.2021.12.040
19. Jalloh M, Leapman MS, Cowan JE, Shinohara K, Greene KL, Roach M 3rd, et al. Patterns of Local Failure Following Radiation Therapy for Prostate Cancer. J Urol (2015) 194:977–82. doi: 10.1016/j.juro.2015.04.111
20. Deek M, Lilleby W, Vaage V, Hole KH, Deweese T, Stensvold A, et al. Impact of Radiation Dose on Recurrence in High-Risk Prostate Cancer Patients. Prostate (2020) 80:1322–7. doi: 10.1002/pros.24059
21. Groen VH, Van Schie M, Zuithoff NPA, Monninkhof EM, Kunze-Busch M, De Boer JCJ, et al. Urethral and Bladder Dose-Effect Relations for Late Genitourinary Toxicity Following External Beam Radiotherapy for Prostate Cancer in the FLAME Trial. Radiother Oncol (2021) 167:127–32. doi: 10.1016/j.radonc.2021.12.027
Keywords: prostatic neoplasms, re-irradiation, image-guided radiotherapy, radiation dose hypofractionation, toxicity, treatment outcome
Citation: Ryg U, Seierstad T, Nilsen LB, Hellebust TP, Djupvik LH, Gustafson H, Hydal J, Kishan AU, Hole KH and Lilleby W (2022) A Prospective Study of High Dose-Rate Brachytherapy or Stereotactic Body Radiotherapy of Intra-Prostatic Recurrence: Toxicity and Long Term Clinical Outcome. Front. Oncol. 12:861127. doi: 10.3389/fonc.2022.861127
Received: 24 January 2022; Accepted: 08 March 2022;
Published: 05 April 2022.
Edited by:
Fiona Lyng, Technological University Dublin, IrelandReviewed by:
Suneil Jain, Queen’s University Belfast, United KingdomCopyright © 2022 Ryg, Seierstad, Nilsen, Hellebust, Djupvik, Gustafson, Hydal, Kishan, Hole and Lilleby. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfgang Lilleby, d2xsQG91cy1oZi5ubw==
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.