
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 13 April 2022
Sec. Gynecological Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.859071
 Fulvio Borella1,2*†
Fulvio Borella1,2*† Stefano Cosma1,2†
Stefano Cosma1,2† Domenico Ferraioli3Mario Preti1,2
Domenico Ferraioli3Mario Preti1,2 Niccolò Gallio1,2
Niccolò Gallio1,2 Giorgio Valabrega4Giulia Scotto4
Giorgio Valabrega4Giulia Scotto4 Alessandro Rolfo2
Alessandro Rolfo2 Isabella Castellano5
Isabella Castellano5 Paola Cassoni5
Paola Cassoni5 Luca Bertero5‡Chiara Benedetto1,2‡
Luca Bertero5‡Chiara Benedetto1,2‡In this review, we provide the state of the art about brain metastases (BMs) from gestational trophoblastic neoplasia (GTN), a rare condition. Data concerning the epidemiology, clinical presentation, innovations in therapeutic modalities, and outcomes of GTN BMs are comprehensively presented with particular attention to the role of radiotherapy, neurosurgery, and the most recent chemotherapy regimens. Good response rates have been achieved thanks to multi-agent chemotherapy, but brain involvement by GTNs entails significant risks for patients’ health since sudden and extensive intracranial hemorrhages are possible. Moreover, despite the evolution of treatment protocols, a small proportion of these patients ultimately develops a resistant disease. To tackle this unmet clinical need, immunotherapy has been recently proposed. The role of this novel option for this subset of patients as well as the achieved results so far are also discussed.
The term gestational trophoblastic disease (GTD) encompasses a spectrum of clinical-pathological disorders of abnormal placental development that include both non-malignant lesions and invasive tumors arising from placental villous and extravillous trophoblasts. In Europe, North and South America the estimated incidence of GTD is 1 per 500-1000 pregnancies, with an overall decline reported in recent years. However, in Asian women, the incidence of GTD remains significantly higher: 1 per 120 pregnancies (1–3). In this context, gestational trophoblastic neoplasia (GTN) is a group of rare tumors that includes invasive mole, choriocarcinoma, placental site trophoblastic tumors (PSTT), and epithelioid trophoblastic tumors (ETT). The incidence of choriocarcinoma is low and is estimated to 1–9 cases per 40,000 pregnancies, while PSTT and ETT account for 2–3% of all trophoblastic neoplasms (1). Occasionally non-pregnant and post-menopausal women may develop GTN (non-gestational choriocarcinoma). High-risk GTNs can develop distant metastases and the most common metastatic sites are lung (80%), vagina (30%), brain (10%), and liver (10%) (2–5). The purpose of this paper is to provide an overview and an update of the clinical-pathological features and treatments of GTN brain metastasis (BMs).
BMs represent the most common adult intracranial malignancy, and it is estimated that approximately 20–30% of adult patients with a solid neoplasm. will develop this complication during the course of their disease. However, data from autopsy studies performed on cancer patients showed a prevalence of solid BMs of up to 40% suggesting that many cases are asymptomatic and undiagnosed (6, 7). The most common solid tumors associated with the development of BMs are in order lung, breast, colorectal cancer, and melanoma, while in other tumor types, including gynecological ones, BMs are very rare (6–13). In this context, the prevalence of BMs from GTN is very low, although variations occurred over the years mainly due to the development of new diagnostic and therapeutic approaches. Historically, a large autopsy study performed in 1963 (14, 15) on 1096 patients with solid cancers identified 200 BMs and only one case derived from choriocarcinoma, while in 1968 an analysis of 393 autopsies of patients with BMs did not reveal any case from GTN. Autopsy studies performed in the 1980s (16, 17) and 1990s (18, 19) reported similar results, suggesting an extremely low prevalence of GTN origin in the general population of patients with BMs. Due to this rarity, the true prevalence of BMs in GTN patients is difficult to determine. In a literature review, Piura E (20). described the clinical-pathological features of 222 patients with BMs from GTN reported between 1980 and 2011, suggesting an overall prevalence of 11.4% with variations across the analyzed time periods. However, it should be noted that most of these data derive from case reports or very heterogeneous small series, thus overestimation of the prevalence rate is possible. Savage et al (21) suggest an incidence of BMs from GTN of 1 case per 22,000 molar pregnancies with brain involvement in about 20% of non-molar choriocarcinoma cases. These authors estimate a comprehensive risk of developing BMs from GTN of 2-3 cases per million pregnancies. Overall, based on the most significant case series published since 1980 we have observed a BMs prevalence ranging from 6.4% to 21.4% among the GTNs (Table 1) (21–35).
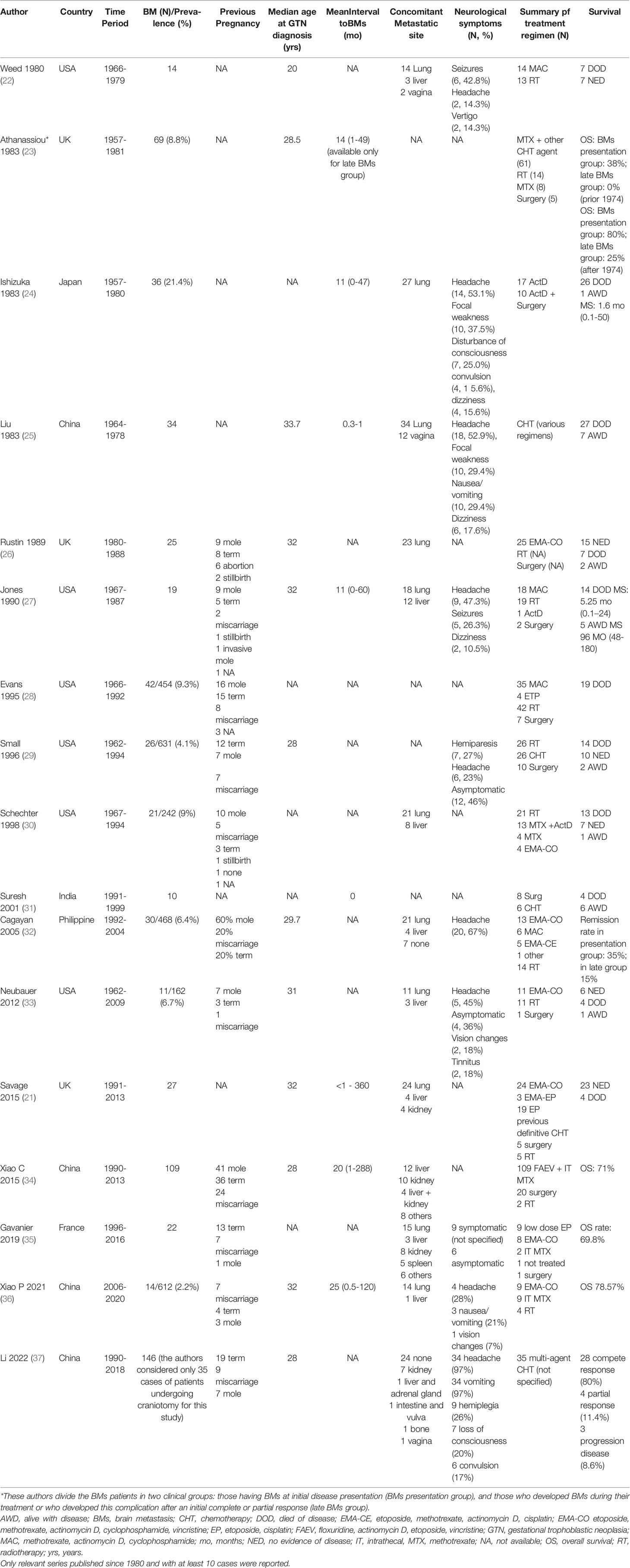
Table 1 Overview of clinical-pathological features, treatments, and outcomes of patients with BMs from GTN.
The median age at diagnosis of BMs ranged from 20 to 33.7 years (Table 1). The interval time from previous pregnancy to BMs detection ranged from <1 to 360 months (Table 1), furthermore, some authors have distinctly considered patients who presented BMs at diagnosis versus those who developed brain disease during chemotherapy or after the end of treatment, as the latter had a worse prognosis (23, 32, 34).
Regarding the clinical presentation, overall, the symptoms of patients affected by BMs depend on the location, number, and size of the lesions, similarly to any lesion causing an intracranial mass effect. Mild or strong headache represents the most common presenting symptom occurring in up to 50% of multiple metastases or in the case of posterior fossa involvement. Up to 40% of patients show focal neurological deficits and 15-20% of cases develop seizures (8), however, BMs can also be found in asymptomatic patients (Table 1).
A specific manifestation of BMs from GTN is a suddenly and extensive intracranial hemorrhage associated or not with oncotic aneurysm because neoplastic cells derived from trophoblast retain the innate capacity to penetrate and erode blood vessels. In the literature, 30 cases of oncotic aneurysms secondary to BMs have been reported, most of them involving the middle cerebral artery and in 17% of cases more than 3 aneurysms were detected. The pathogenesis of an oncotic aneurysm is due to neoplastic vascular embolization with obstruction of distal cerebral vessels or with infiltration of the vasa vasorum followed by focal destruction of the intima, internal elastic lamina, and medial layers, leading to the development of an aneurysm. Brain angiography can be useful to study the characteristics of oncotic aneurysms, but identification of these lesions can be challenging in the case of cerebral hemorrhage (38, 39).
Brain computer tomography (CT) scan and/or magnetic resonance imaging (MRI) are the diagnostic choice to study cerebral lesions. As a general rule, brain MRI with or without intravenous gadolinium contrast is the gold standard for the assessment of BMs and shows a better sensitivity over contrast-enhanced CT for metastasis located in the posterior fossa where bone artifact can hide small metastases and/or leptomeningeal disease (8).
BMs from GTN may appear as single or multiple lesions and in most cases are located in the gray-white matter junction of the cerebral hemispheres (20, 34, 40). BMs are characterized by avid enhancement after administration of contrast due to the high vascularity of neoplastic tissue. BMs show high attenuation at non-enhanced computer tomography, and, at brain MRI, they are characterized by variable signal intensity depending on the chronicity of the intralesional hemorrhage (40).
Positron emission tomography (PET) does not play a relevant role in the diagnosis and staging of low-risk GTNs but it can be usefully associated with CT in patients with high-risk GTN and/or who have previously undergone multiple chemotherapy lines in order to monitor/detect primary and/or metastatic disease (41, 42). It should be noted that 18F‐fluorodeoxyglucose PET alone can have non-negligible false negative and positive results, so it is always advisable to associate this investigation with other diagnostic techniques (43).
BMs may be associated with other metastatic sites and in particular, brain involvement is often synchronous with lung metastasis (Table 1). Therefore in the case of detection of lung metastasis, a potential brain involvement should be considered and promptly investigated even without neurological symptoms (44). The extremely low incidence of BMs in post-molar pregnancy GTN would suggest that in the absence of neurological symptoms performing brain imaging is not indicated; however, for patients with non-molar choriocarcinoma, it is recommended to exclude brain involvement in all patients (21).
The detection of high serum and cerebrospinal fluid levels of β-hCG may also be helpful if a BM from GTN is suspected (45).
The staging system currently used for GTN has been developed by the FIGO (International Federation of Gynecology and Obstetrics) and includes four categories: 1) the tumor is limited to the uterus, 2) the tumor extends outside the uterus with local involvement of other genital structures (vagina, adnexa), 3) presence of lung metastases with or without local extra-uterine extension 4) brain, liver, kidneys and/or gastrointestinal tract involvement (46–48). In addition to tumor stage, several prognostic risk factors have been defined including patient’s age, antecedent pregnancy, interval months from index pregnancy, pretreatment serum hCG, largest tumor size, site and number of metastases and, the previous number of chemotherapy regimens. Women presenting a FIGO score of 0-6 should be considered low risk and a regimen with a single agent (methotrexate - MTX or dactinomycin) should be proposed. A high FIGO score (> 6) is predictive for chemoresistance in the case of single agent therapy, therefore combination chemotherapy should be used for these patients (46–48). Indeed, most patients with scores 0-4 are successfully treated with a single chemotherapy agent, while about 40% of women with a score of 5–6 need a polychemotherapy regimen after the first therapy (49). Patients with ultra high-risk (FIGO score ≥ 12) GTN have a 5-years OS rate of 67.9% and the presence of BMs is associated with a worse prognosis (RR 2.280, 95% CI 1.248–4.163, p-value = 0.007) (50).
Conversely to BMs derived by other types of tumors, which are predominantly treated with neurosurgical and radiation therapy approaches (8), in most cases BMs from GTNs are treated with cytotoxic chemotherapy (the most common protocols used are reported in Table 2). The proposed chemotherapy regimens have changed over the years, significantly improving the prognosis. Choriocarcinoma BMs series reported in the 1980s referring to cases from previous decades showed disappointing survival outcomes: Ishizuka et al (24) reported data regarding 27 patients treated with actinomycin D or actinomycin D plus neurosurgery resulting in 26 deaths, suggesting that this single-agent approach is not suitable. Probably, the poor efficacy of this drug lies in the difficulty of passing the blood-brain barrier (BBB). Furthermore, currently, actinomycin-D alone is indicated as a possible alternative to MTX in the treatment of low-risk, according to the FIGO score, GTN but not for high-risk GTN. Survival outcomes of 69 cases of choriocarcinoma BMs were reported in another series (23). These patients were mainly treated with systemic or intrathecal MTX alone or in combination with other unspecified chemotherapeutic agents. The authors reported worse survival outcomes in patients who developed BMs during treatment or after completing treatment compared to those who presented with BMs at first diagnosis, suggesting a progressive development of chemoresistance. Interestingly, they report an improvement in prognosis after 1974 for both the group that had early BMs diagnosis (38% vs 80%) and the group that developed BMs during or after treatment (0% vs 25%). These survival improvements were explained thanks to i) use of MTX in patients with lung metastases (often concomitant with brain metastases); ii) early detection of central nervous system lesions and iii) use of A combination of systemic and intrathecal therapy. Liu et al (25) reported the outcomes of 34 patients with metastatic brain disease treated with heterogeneous regimens mainly based on 6-mercaptopurine, 5-fluorouracil, and MTX also suggesting a complementary role of unspecified Chinese herbs, but most of the patients of this series died less than a month after diagnosis. Savage et al (21) reported a good overall survival (OS) rate (85%) treating most patients with EMA-CO (Table 2) preceded by low dose etoposide and cisplatin. Interestingly, none of these patients was subjected to whole-brain radiation therapy, and only 5 cases required brain stereotactic radiotherapy (RT) for residual tumor at the end of chemotherapy. Xiao et al (34) reported the outcomes of 109 GTN patients with BMs using a combination of systemic chemotherapy (FAEV regimen, Table 2) (51) plus intrathecal injection of MTX. Also in this series, only 2 patients received brain RT. The 5-year OS was 71.1%, rising to 85.5% for patients receiving primary chemotherapy in dedicated referral GTN centers. The authors also report as independent poor prognostic indicators for survival: FIGO score > 12 (Hazard ratio-HR 1.279, 95% CI 1.061-1.541, p-value = 0.010), failure of previous multidrug chemotherapy (HR 3.177, 95% CI 1.277-7.908, p-value = 0.013), and concomitant renal involvement (HR: 2.654, 95% CI 1.125-6.261, p-value = 0.026). The use of MTX-based intrathecal therapy is controversial: an early and intensive therapy with high doses of MTX can induce sudden necrosis of the BM and cause cerebral hemorrhage[ (23). Response rates of over 80% were achieved when intrathecal MTX was used alongside EMA-CO or EMA-EP (21, 26), however, a recent study reported a higher response rate in patients who underwent systemic chemotherapy without intrathecal MTX, therefore, the role of this therapeutic approach remains to be defined (35). The proposed regimen of intrathecal MTX is reported in Table 2 (52).
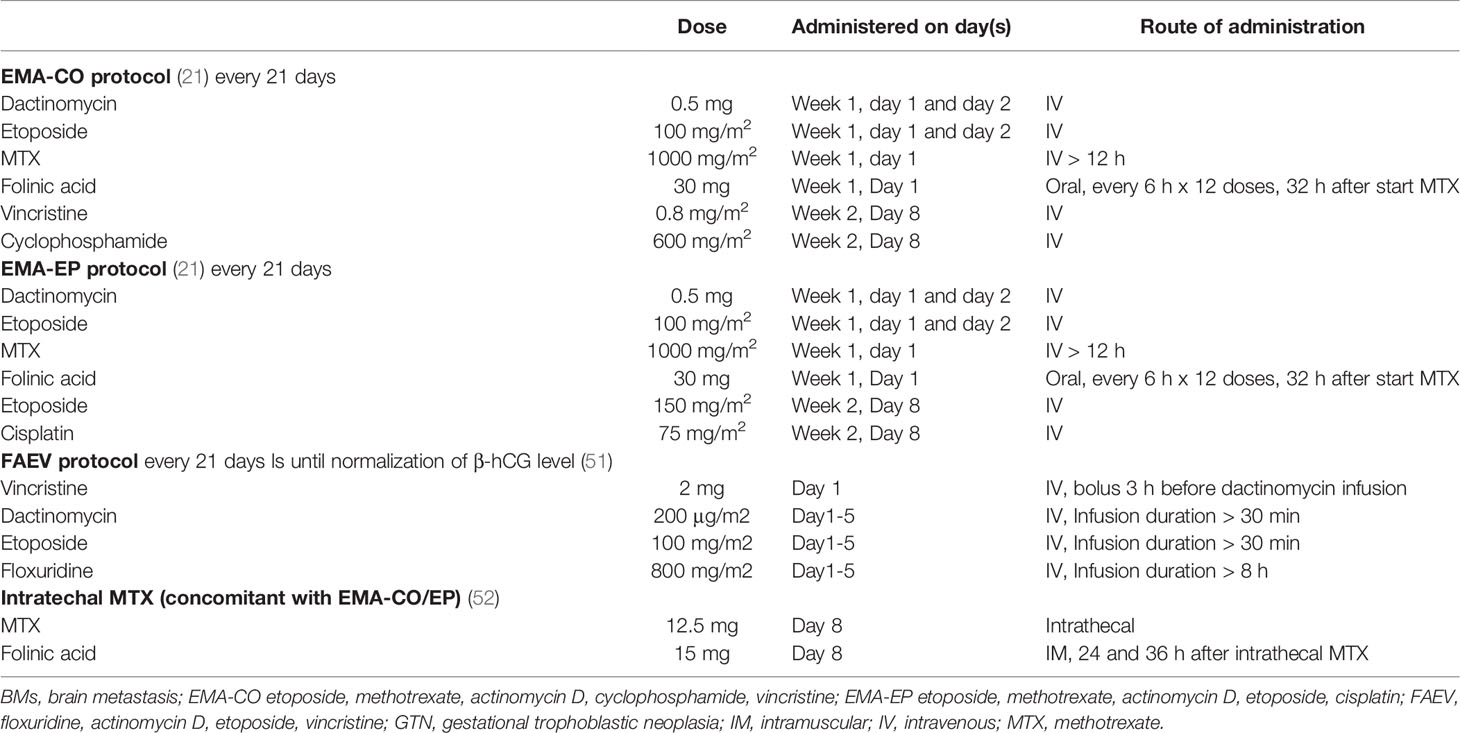
Table 2 most common multidrug regimens used for treating BMs from GTN.
As previously mentioned, the role of RT has progressively lost its importance in the treatment of GTN’s BMs. In 1980 Weed (22) et al. reported the survival outcomes of 14 patients affected by BMs from GTN. Of them, 13 were treated with whole brain RT plus systemic chemotherapy, but only 7 (50%) achieved a complete response. Athanassiou et al (23) also reported the survival outcomes of a series of patients treated with whole-brain RT: 6/6 patients who developed late BMs died, while out of 8 patients who developed early BMs only 2 survived. Other authors (26, 27, 32) also reported an overall poor efficacy of RT, while Schechter et al (30) reported a survival advantage in a small cohort of patients (N = 10) who received a dose greater than 2200 cGy compared to those who were subjected to lower doses (N = 11). Interestingly, the results of a recent study carried out at the French Trophoblastic Disease Reference Centre on 21 patients with BMs from GTN treated with multidrug chemotherapy without concomitant whole-brain RT showed a higher OS rate of 81.5% (excluding 3 cases of early death due to intracranial hemorrhage) compared with OS rates of 75% from studies combining whole-brain RT with multidrug chemotherapy (35). Based on these results, the authors of this study do not support the role of whole-brain RT in patients with BMs from GTN at initial diagnosis (35).
Furthermore, experiences in the treatment of BMs from other neoplasms suggest a decline in neurocognitive function (53, 54) and due to the mean young age of patients affected by BMs from GTN, this issue should also be taken into consideration.
The potential neurocognitive damage in patients with BM’s from GTN undergoing brain RT is poorly reported in the literature. Athanassiou et al (23) reported several side effects in patients who underwent whole-brain RT (N=14) for BMs from GTN including hemianopia, hemiparesis, epilepsy, episodes of amnesia, headache, aphasia, and cognitive deficits.
Recently, data from 35 patients treated with multi-agent chemotherapy regimens and craniotomy showed an OS of 80%, however, in 26 patients craniotomy was performed in critical condition for intracranial hemorrhage and hypertension (37).
The role of intracranial surgery is actually limited to salvage treatment in case of intracranial hypertension, hemorrhage, edema, or for resection of chemoresistant metastasis (23, 28, 38).
The introduction of immune checkpoint inhibitors (ICIs) constitutes a paradigm shift in cancer treatment, in particular for melanoma, non-small cell lung cancer, and renal cell cancer (55–59), but in other contexts, such as in the treatment of gynecological neoplasms their role is controversial and ICIs have been approved for treating only some specific subtypes of tumors (60–65).
The main ICIs targets include programmed cell death 1 (PD-1), programmed cell death 1 ligand 1 (PD-L1), and cytotoxic T lymphocyte antigen 4 (CTLA-4). PD-1 is a cell surface co-inhibitory receptor member of the CD28/CTLA-4 family. Normally, it is expressed on lymphocytes but it can also be found on other immune cells including monocytes and natural killer T cells. Following its activation, PD-1 receptor promotes the production of pro-inflammatory molecules such as interferon-γ (IFN-γ), tumor necrosis factor-α (TNF- α), and interleukin2 (IL-2), inhibits CD8+ T cell proliferation and activation and suppresses the activity of regulatory T lymphocytes. PD-1 may also target tumor cells and tumor-associated macrophages helping to maintain an immunosuppressive tumor environment (66, 67). CTLA-4 is another fundamental T cell protein associated with immune regulation. CTLA-4 is expressed by both CD4+ and CD8+ T cells and exerts its immunosuppressive effects through the modulation of regulatory T cells (68). The inhibition of the binding between PD-1 and CTLA-4 and their receptors by ICIs may improve the cytotoxic CD8+ T-cell effectiveness eliciting a higher antineoplastic effect.
Historically, already in the 1960s, immunotherapeutic approaches were used for the treatment of BMs from GTN, for example through skin graft from the patient’s husband with the rationale of stimulating immunity against paternal antigens or promoting nonspecific immunological stimuli through the Bacillus of Calmette-Guerin, but these methods were soon abandoned (23).
In recent years, the treatment of chemoresistant GTNs through ICIs has gained significant interest and has been actively investigated, even in patients with BMs. Zong et al (69) investigated the expression of molecules belonging to B7 family check-point proteins in 112 GTN: 68 choriocarcinomas, 33 PSTT.and 11 ETT. PD-L1 and B7-H3 were both highly expressed in all tumors, while PD-L2 was found in 87.5% of the samples. PD-L1, B7-H3, and VISTA expression were significantly higher in choriocarcinomas and PSTTs compared with ETTs. High expression of PD-L1 was also observed in GTNs in previous studies (70–72). These results suggest a strong rationale for the use of immunotherapy in these tumors.
Encouraging results were obtained with the use of ICIs in the TROPHIMMUN Phase II Trial (73). This study included 15 patients who experienced progression disease from GTN and were treated with Avelumab (anti PD-L1 drug) 10 mg/kg intravenously every 2 weeks on monotherapy achieving a complete response in approximately 50% of patients. Unfortunately, this study considered the presence of BMs as an exclusion criterion. Furthermore, Ghorani et al (74) reported the outcomes of 4 patients with drug-resistant GTN treated with pembrolizumab, an anti PD-1 antibody. Of these 4 patients, 3 achieved a complete response to pembrolizumab, including one patient with metastatic brain disease. Good clinical results with pembrolizumab were also obtained in a 30-year-old patient with multiple GTN metastasis including within the central nervous system, refractory to classical chemotherapy regimens (75). Unfortunately, given the rarity of BMs from GTN, there are no trials on the specific use of ICIs for this disease.
GTN BMs remain a rare occurrence often associated with other metastatic sites and harboring a poorer prognosis, especially because of the complications such as rupture of an oncotic aneurysm. An immediate multidisciplinary approach is recognized as the best strategy for patient assessment and decision-making regarding the initial treatment of NTG with brain metastases. The multidisciplinary team should include a neuroradiologist, a neurosurgeon, and a radiotherapist led by a specialist with knowledge of all treatment modalities involved in the management of GTN (44).
Despite the rarity of this complication, excellent therapeutic results have been obtained through a progressive refinement of multi-agent chemotherapy regimens, achieving complete remissions in many cases. Nevertheless, some patients develop chemoresistant disease. In this subset of patients, some further progress has been recently made thanks to the use of ICIs, but further studies are needed to confirm the role of immunotherapy in GTN BMs resistant to classical chemotherapy regimens.
Conceptualization: FB, SC; Methodology: FB, SC; Resources: CB; Literature research: DF, MP, GV, GS, NG, AR; Data curation, FB, SC, DF, LB; Interpretation of data: all authors. Writing—original draft preparation: FB, SC, DF, LB; Writing—review and editing: all authors; Supervision: CB; Project administration: FB, SC, CB; All authors have read and agreed to the published version of the manuscript.
GV has received personal fees from Roche, AstraZeneca, Tesaro, PharmaMar and Amgen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lurain JR. Gestational Trophoblastic Disease I: Epidemiology, Pathology, Clinical Presentation and Diagnosis of Gestational Trophoblastic Disease, and Management of Hydatidiform Mole. Am J Obstet Gynecol (2010) 203:531–9. doi: 10.1016/j.ajog.2010.06.073
2. Sita-Lumsden A, Short D, Lindsay I, Sebire NJ, Adjogatse D, Seckl MJ, et al. Treatment Outcomes for 618 Women With Gestational Trophoblastic Tumours Following a Molar Pregnancy at the Charing Cross Hospital, 2000–2009. Br J Cancer (2012) 107:1810–4. doi: 10.1038/bjc.2012.462
3. Fülöp V, Szigetvári I, Szepesi J, Végh G, Bátorfi J, Nagymányoki Z, et al. 30 Years’ Experience in the Treatment of Low-Risk Gestational Trophoblastic Neoplasia in Hungary. J Reprod Med (2010) 55:253–7.
4. Duong J, Ghanchi H, Miulli D, Kahlon A. Metastatic Nongestational Choriocarcinoma to the Brain: Case Report and Proposed Treatment Recommendations. World Neurosurg (2018) 115:170–5. doi: 10.1016/j.wneu.2018.04.050
5. Soper JT. Gestational Trophoblastic Disease. Obstet Gynecol (2006) 108:176–87. doi: 10.1097/01.AOG.0000224697.31138.a1
6. Nayak L, Lee EQ, Wen PY. Epidemiology of Brain Metastases. Curr Oncol Rep (2012) 14:48–54. doi: 10.1007/s11912-011-0203-y
7. Suh JH, Kotecha R, Chao ST, Ahluwalia MS, Sahgal A, Chang EL. Current Approaches to the Management of Brain Metastases. Nat Rev Clin Oncol (2020) 17:279–99. doi: 10.1038/s41571-019-0320-3
8. Achrol AS, Rennert RC, Anders C, Soffietti R, Ahluwalia MS, Nayak L, et al. Brain Metastases. Nat Rev Dis Primer (2019) 5:5. doi: 10.1038/s41572-018-0055-y
9. Berghoff AS, Schur S, Füreder LM, Gatterbauer B, Dieckmann K, Widhalm G, et al. Descriptive Statistical Analysis of a Real Life Cohort of 2419 Patients With Brain Metastases of Solid Cancers. ESMO Open (2016) 1:e000024. doi: 10.1136/esmoopen-2015-000024
10. Borella F, Bertero L, Morrone A, Gambella A, Bovetti M, Cosma S, et al. Brain Metastases From Ovarian Cancer: Current Evidence in Diagnosis, Treatment, and Prognosis. Cancers (2020) 12:E2156. doi: 10.3390/cancers12082156
11. Hwang JH, Yoo HJ, Lim MC, Seo S-S, Kang S, Kim J-Y, et al. Brain Metastasis in Patients With Uterine Cervical Cancer. J Obstet Gynaecol Res (2013) 39:287–91. doi: 10.1111/j.1447-0756.2012.01927.x
12. Bhambhvani HP, Zhou O, Cattle C, Taiwo R, Diver E, Hayden Gephart M. Brain Metastases From Endometrial Cancer: Clinical Characteristics, Outcomes, and Review of the Literature. World Neurosurg (2021) 147:e32–9. doi: 10.1016/j.wneu.2020.11.087
13. Scotto G, Borella F, Turinetto M, Tuninetti V, Valsecchi AA, Giannone G, et al. Biomarkers of Central Nervous System Involvement From Epithelial Ovarian Cancer. Cells (2021) 10:3408. doi: 10.3390/cells10123408
14. Chason JL, Walker FB, Landers JW. Metastatic Carcinoma in the Central Nervous System and Dorsal Root Ganglia. A Prospective Autopsy Study. Cancer (1963) 16:781–7. doi: 10.1002/1097-0142(196306)16:6<781::aid-cncr2820160614>3.0.co;2-m
16. Zimm S, Wampler GL, Stablein D, Hazra T, Young HF. Intracerebral Metastases in Solid-Tumor Patients: Natural History and Results of Treatment. Cancer (1981) 48:384–94. doi: 10.1002/1097-0142(19810715)48:2<384::aid-cncr2820480227>3.0.co;2-8
17. Le Chevalier T, Smith FP, Caille P, Constans JP, Rouesse JG. Sites of Primary Malignancies in Patients Presenting With Cerebral Metastases. A Review of 120 Cases. Cancer (1985) 56:880–2. doi: 10.1002/1097-0142(19850815)56:4<880::aid-cncr2820560430>3.0.co;2-i
18. Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain Metastases. Histology, Multiplicity, Surgery, and Survival. Cancer (1996) 78:1781–8. doi: 10.1002/(SICI)1097-0142(19961015)78:8<1781::AID-CNCR19>3.0.CO;2-U
19. Lagerwaard FJ, Levendag PC, Nowak PJ, Eijkenboom WM, Hanssens PE, Schmitz PI. Identification of Prognostic Factors in Patients With Brain Metastases: A Review of 1292 Patients. Int J Radiat Oncol Biol Phys (1999) 43:795–803. doi: 10.1016/s0360-3016(98)00442-8
20. Piura E, Piura B. Brain Metastases From Gestational Trophoblastic Neoplasia: Review of Pertinent Literature. Eur J Gynaecol Oncol (2014) 35:359–67.
21. Savage P, Kelpanides I, Tuthill M, Short D, Seckl MJ. Brain Metastases in Gestational Trophoblast Neoplasia: An Update on Incidence, Management and Outcome. Gynecol Oncol (2015) 137:73–6. doi: 10.1016/j.ygyno.2015.01.530
22. Weed JC, Hammond CB. Cerebral Metastatic Choriocarcinoma: Intensive Therapy and Prognosis. Obstet Gynecol (1980) 55:89–94.
23. Athanassiou A, Begent RH, Newlands ES, Parker D, Rustin GJ, Bagshawe KD. Central Nervous System Metastases of Choriocarcinoma. 23 Years’ Experience at Charing Cross Hospital. Cancer (1983) 52:1728–35. doi: 10.1002/1097-0142(19831101)52:9<1728::aid-cncr2820520929>3.0.co;2-u
24. Ishizuka T, Tomoda Y, Kaseki S, Goto S, Hara T, Kobayashi T. Intracranial Metastasis of Choriocarcinoma. A Clinicopathologic Study. Cancer (1983) 52:1896–903. doi: 10.1002/1097-0142(19831115)52:10<1896::aid-cncr2820521021>3.0.co;2-b
25. Liu TL, Deppe G, Chang QT, Tan TT. Cerebral Metastatic Choriocarcinoma in the People’s Republic of China. Gynecol Oncol (1983) 15:166–70. doi: 10.1016/0090-8258(83)90071-9
26. Rustin GJ, Newlands ES, Begent RH, Dent J, Bagshawe KD. Weekly Alternating Etoposide, Methotrexate, and Actinomycin/Vincristine and Cyclophosphamide Chemotherapy for the Treatment of CNS Metastases of Choriocarcinoma. J Clin Oncol Off J Am Soc Clin Oncol (1989) 7:900–3. doi: 10.1200/JCO.1989.7.7.900
27. Jones WB, Wagner-Reiss KM, Lewis JL. Intracerebral Choriocarcinoma. Gynecol Oncol (1990) 38:234–43. doi: 10.1016/0090-8258(90)90048-p
28. Evans AC, Soper JT, Clarke-Pearson DL, Berchuck A, Rodriguez GC, Hammond CB. Gestational Trophoblastic Disease Metastatic to the Central Nervous System. Gynecol Oncol (1995) 59:226–30. doi: 10.1006/gyno.1995.0013
29. Small W, Lurain JR, Shetty RM, Huang CF, Applegate GL, Brand WN. Gestational Trophoblastic Disease Metastatic to the Brain. Radiology (1996) 200:277–80. doi: 10.1148/radiology.200.1.8657926
30. Schechter NR, Mychalczak B, Jones W, Spriggs D. Prognosis of Patients Treated With Whole-Brain Radiation Therapy for Metastatic Gestational Trophoblastic Disease. Gynecol Oncol (1998) 68:183–92. doi: 10.1006/gyno.1997.4920
31. Suresh TN, Santosh V, Shastry Kolluri VR, Jayakumar PN, Yasha TC, Mahadevan A, et al. Intracranial Haemorrhage Resulting From Unsuspected Choriocarcinoma Metastasis. Neurol India (2001) 49:231–6.
32. Cagayan MSFS, Lu-Lasala LR. Management of Gestational Trophoblastic Neoplasia With Metastasis to the Central Nervous System: A 12-Year Review at the Philippine General Hospital. J Reprod Med (2006) 51:785–92.
33. Neubauer NL, Latif N, Kalakota K, Marymont M, Small W, Schink JC, et al. Brain Metastasis in Gestational Trophoblastic Neoplasia: An Update. J Reprod Med (2012) 57:288–92.
34. Xiao C, Yang J, Zhao J, Ren T, Feng F, Wan X, et al. Management and Prognosis of Patients With Brain Metastasis From Gestational Trophoblastic Neoplasia: A 24-Year Experience in Peking Union Medical College Hospital. BMC Cancer (2015) 15:318. doi: 10.1186/s12885-015-1325-7
35. Gavanier D, Leport H, Massardier J, Abbas F, Schott A-M, Hajri T, et al. Gestational Trophoblastic Neoplasia With Brain Metastasis at Initial Presentation: A Retrospective Study. Int J Clin Oncol (2019) 24:153–60. doi: 10.1007/s10147-018-1337-9
36. Xiao P, Guo T, Luo Y, Zhang M, Yin R. Real-World Data of 14 Cases of Brain Metastases From Gestational Trophoblastic Neoplasia and a Literature Review. Arch Gynecol Obstet (2021) 305(4):929–35. doi: 10.1007/s00404-021-06238-w
37. Li Y, Wang W, Wan X, Feng F, He Y-L, Yang J, et al. Effectiveness of Craniotomy and Long-Term Survival in 35 Patients With Gestational Trophoblastic Neoplasia With Brain Metastases: A Clinical Retrospective Analysis. J Gynecol Oncol (2022) 33:e33. doi: 10.3802/jgo.2022.33.e33
38. Kim S-U, Huh J, Kim D-S, Huh C-W. Recurrent Cerebral Hemorrhage With Brain Metastasis of Choriocarcinoma Presenting as Initially Absent and Later Identified as Oncotic Aneurysms: A Case Report and Literature Review. Interdiscip Neurosurg (2021) 24:101043. doi: 10.1016/j.inat.2020.101043
39. Yeo CJJ, Britz GW, Powell SZ, Smith RG, Zhang YJ. Recurrent Cerebral Hemorrhage in Normal Pregnancy Secondary to Mycotic Pseudoaneurysms Related to Choriocarcinoma. World Neurosurg (2018) 109:247–50. doi: 10.1016/j.wneu.2017.09.187
40. Shaaban AM, Rezvani M, Haroun RR, Kennedy AM, Elsayes KM, Olpin JD, et al. Gestational Trophoblastic Disease: Clinical and Imaging Features. Radiogr Rev Publ Radiol Soc N Am Inc (2017) 37:681–700. doi: 10.1148/rg.2017160140
41. Mapelli P, Mangili G, Picchio M, Gentile C, Rabaiotti E, Giorgione V, et al. Role of 18F-FDG PET in the Management of Gestational Trophoblastic Neoplasia. Eur J Nucl Med Mol Imaging (2013) 40:505–13. doi: 10.1007/s00259-012-2324-4
42. Mangili G, Bergamini A, Giorgione V, Picchio M, Petrone M, Mapelli P, et al. [18f]Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography and Trophoblastic Disease: The Gynecologist Perspective. Q J Nucl Med Mol Imaging (2016) 60:103–16. Off. Publ. Ital. Assoc. Nucl. Med. AIMN Int. Assoc. Radiopharmacol. IAR Sect. Soc. Of.
43. Dhillon T, Palmieri C, Sebire NJ, Lindsay I, Newlands ES, Schmid P, et al. Value of Whole Body 18fdg-PET to Identify the Active Site of Gestational Trophoblastic Neoplasia. J Reprod Med (2006) 51:879–87.
44. Soper JT. Gestational Trophoblastic Disease: Current Evaluation and Management. Obstet Gynecol (2021) 137:355–70. doi: 10.1097/AOG.0000000000004240
45. Fujimaki T. Levels of Beta-Human Chorionic Gonadotropin in Cerebrospinal Fluid of Patients With Malignant Germ Cell Tumor Can Be Used to Detect Early Recurrence and Monitor the Response to Treatment. Jpn J Clin Oncol (2000) 30:291–4. doi: 10.1093/jjco/hyd076
46. Kohorn EI. The New FIGO 2000 Staging and Risk Factor Scoring System for Gestational Trophoblastic Disease: Description and Critical Assessment. Int J Gynecol Cancer Off J Int Gynecol Cancer Soc (2001) 11:73–7. doi: 10.1046/j.1525-1438.2001.011001073.x
47. Ngan HY, Bender H, Benedet JL, Jones H, Montruccoli GC, Pecorelli S, et al. Gestational Trophoblastic Neoplasia, FIGO 2000 Staging and Classification. Int J Gynaecol Obstet (2003) 83 Suppl 1:175–7. doi: 10.1016/s0020-7292(03)90120-2. Off. Organ Int. Fed. Gynaecol. Obstet.
48. Ngan HYS. The Practicability of FIGO 2000 Staging for Gestational Trophoblastic Neoplasia. Int J Gynecol Cancer (2004) 14:202–5. doi: 10.1111/j.1048-891X.2004.014236.x. Off. J. Int. Gynecol. Cancer Soc.
49. Braga A, Paiva G, Ghorani E, Freitas F, Velarde LGC, Kaur B, et al. Predictors for Single-Agent Resistance in FIGO Score 5 or 6 Gestational Trophoblastic Neoplasia: A Multicentre, Retrospective, Cohort Study. Lancet Oncol (2021) 22:1188–98. doi: 10.1016/S1470-2045(21)00262-X
50. Kong Y, Yang J, Jiang F, Zhao J, Ren T, Li J, et al. Clinical Characteristics and Prognosis of Ultra High-Risk Gestational Trophoblastic Neoplasia Patients: A Retrospective Cohort Study. Gynecol Oncol (2017) 146:81–6. doi: 10.1016/j.ygyno.2017.04.010
51. Yang J, Xiang Y, Wan X, Feng F, Ren T. Primary Treatment of Stage IV Gestational Trophoblastic Neoplasia With Floxuridine, Dactinomycin, Etoposide and Vincristine (FAEV): A Report Based on Our 10-Year Clinical Experiences. Gynecol Oncol (2016) 143:68–72. doi: 10.1016/j.ygyno.2016.07.099
52. Braga A, Elias KM, Horowitz NS, Berkowitz RS. Treatment of High-Risk Gestational Trophoblastic Neoplasia and Chemoresistance/Relapsed Disease. Best Pract Res Clin Obstet Gynaecol (2021) 74:81–96. doi: 10.1016/j.bpobgyn.2021.01.005
53. Tallet AV, Azria D, Barlesi F, Spano J-P, Carpentier AF, Gonçalves A, et al. Neurocognitive Function Impairment After Whole Brain Radiotherapy for Brain Metastases: Actual Assessment. Radiat Oncol (2012) 7:77. doi: 10.1186/1748-717X-7-77
54. McTyre E, Scott J, Chinnaiyan P. Whole Brain Radiotherapy for Brain Metastasis. Surg Neurol Int (2013) 4:236. doi: 10.4103/2152-7806.111301
55. Steininger J, Gellrich FF, Schulz A, Westphal D, Beissert S, Meier F. Systemic Therapy of Metastatic Melanoma: On the Road to Cure. Cancers (2021) 13:1430. doi: 10.3390/cancers13061430
56. Hah Y-S, Koo K-C. Immunology and Immunotherapeutic Approaches for Advanced Renal Cell Carcinoma: A Comprehensive Review. Int J Mol Sci (2021) 22:4452. doi: 10.3390/ijms22094452
57. Lavacchi D, Pellegrini E, Palmieri VE, Doni L, Mela MM, Di Maida F, et al. Immune Checkpoint Inhibitors in the Treatment of Renal Cancer: Current State and Future Perspective. Int J Mol Sci (2020) 21:4691. doi: 10.3390/ijms21134691
58. Mencoboni M, Ceppi M, Bruzzone M, Taveggia P, Cavo A, Scordamaglia F, et al. Effectiveness and Safety of Immune Checkpoint Inhibitors for Patients With Advanced Non Small-Cell Lung Cancer in Real-World: Review and Meta-Analysis. Cancers (2021) 13:1388. doi: 10.3390/cancers13061388
59. Pathak R, Amini A, Hill A, Massarelli E, Salgia R. Immunotherapy in Non-Small Cell Lung Cancer Patients With Brain Metastases: Clinical Challenges and Future Directions. Cancers (2021) 13:3407. doi: 10.3390/cancers13143407
60. Borella F, Ghisoni E, Giannone G, Cosma S, Benedetto C, Valabrega G, et al. Immune Checkpoint Inhibitors in Epithelial Ovarian Cancer: An Overview on Efficacy and Future Perspectives. Diagn Basel Switz (2020) 10(3):146. doi: 10.3390/diagnostics10030146
61. Musacchio L, Boccia SM, Caruso G, Santangelo G, Fischetti M, Tomao F, et al. Immune Checkpoint Inhibitors: A Promising Choice for Endometrial Cancer Patients? J Clin Med (2020) 9:E1721. doi: 10.3390/jcm9061721
62. Attademo L, Tuninetti V, Pisano C, Cecere SC, Di Napoli M, Tambaro R, et al. Immunotherapy in Cervix Cancer. Cancer Treat Rev (2020) 90:102088. doi: 10.1016/j.ctrv.2020.102088
63. Borella F, Preti M, Bertero L, Collemi G, Castellano I, Cassoni P, et al. Is There a Place for Immune Checkpoint Inhibitors in Vulvar Neoplasms? A State of the Art Review. Int J Mol Sci (2020) 22.(1):190 doi: 10.3390/ijms22010190
64. Ferrall L, Lin KY, Roden RBS, Hung C-F, Wu T-C. Cervical Cancer Immunotherapy: Facts and Hopes. Clin Cancer Res (2021) 27:4953–73. doi: 10.1158/1078-0432.CCR-20-2833. Off. J. Am. Assoc. Cancer Res.
65. Voelker R. Immunotherapy Approved for Endometrial Cancer. JAMA (2021) 325:2143. doi: 10.1001/jama.2021.8319
66. Buchbinder EI, Desai A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am J Clin Oncol (2016) 39:98–106. doi: 10.1097/COC.0000000000000239
67. Seidel JA, Otsuka A, Kabashima K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front Oncol (2018) 8:86. doi: 10.3389/fonc.2018.00086
68. Walker LSK, Sansom DM. The Emerging Role of CTLA4 as a Cell-Extrinsic Regulator of T Cell Responses. Nat Rev Immunol (2011) 11:852–63. doi: 10.1038/nri3108
69. Zong L, Zhang M, Wang W, Wan X, Yang J, Xiang Y. PD-L1, B7-H3 and VISTA Are Highly Expressed in Gestational Trophoblastic Neoplasia. Histopathology (2019) 75:421–30. doi: 10.1111/his.13882
70. Veras E, Kurman RJ, Wang T-L, Shih I-M. PD-L1 Expression in Human Placentas and Gestational Trophoblastic Diseases. Int J Gynecol Pathol (2017) 36:146–53. doi: 10.1097/PGP.0000000000000305. Off. J. Int. Soc. Gynecol. Pathol.
71. Bolze P-A, Patrier S, Massardier J, Hajri T, Abbas F, Schott AM, et al. PD-L1 Expression in Premalignant and Malignant Trophoblasts From Gestational Trophoblastic Diseases Is Ubiquitous and Independent of Clinical Outcomes. Int J Gynecol Cancer (2017) 27:554–61. doi: 10.1097/IGC.0000000000000892. Off. J. Int. Gynecol. Cancer Soc.
72. Inaguma S, Wang Z, Lasota J, Sarlomo-Rikala M, McCue PA, Ikeda H, et al. Comprehensive Immunohistochemical Study of Programmed Cell Death Ligand 1 (PD-L1): Analysis in 5536 Cases Revealed Consistent Expression in Trophoblastic Tumors. Am J Surg Pathol (2016) 40:1133–42. doi: 10.1097/PAS.0000000000000653
73. You B, Bolze P-A, Lotz J-P, Massardier J, Gladieff L, Joly F, et al. Avelumab in Patients With Gestational Trophoblastic Tumors With Resistance to Single-Agent Chemotherapy: Cohort A of the TROPHIMMUN Phase II Trial. J Clin Oncol (2020) 38:3129–37. doi: 10.1200/JCO.20.00803. Off. J. Am. Soc. Clin. Oncol.
74. Ghorani E, Kaur B, Fisher RA, Short D, Joneborg U, Carlson JW, et al. Pembrolizumab Is Effective for Drug-Resistant Gestational Trophoblastic Neoplasia. Lancet (2017) 390:2343–5. doi: 10.1016/S0140-6736(17)32894-5
Keywords: gestational trophoblastic neoplasia, brain metastases (BMs), choriocarcinoma, chemotherapy, immunotherapy, treatment outcomes
Citation: Borella F, Cosma S, Ferraioli D, Preti M, Gallio N, Valabrega G, Scotto G, Rolfo A, Castellano I, Cassoni P, Bertero L and Benedetto C (2022) From Uterus to Brain: An Update on Epidemiology, Clinical Features, and Treatment of Brain Metastases From Gestational Trophoblastic Neoplasia. Front. Oncol. 12:859071. doi: 10.3389/fonc.2022.859071
Received: 20 January 2022; Accepted: 17 March 2022;
Published: 13 April 2022.
Edited by:
Elena Ioana Braicu, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Amanda E. D. Van Swearingen, Duke University, United StatesCopyright © 2022 Borella, Cosma, Ferraioli, Preti, Gallio, Valabrega, Scotto, Rolfo, Castellano, Cassoni, Bertero and Benedetto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fulvio Borella, ZnVsdmlvLmJvcmVsbGFAdW5pdG8uaXQ=
†These authors share first authorship
‡These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.