 Wei Lin1,2†
Wei Lin1,2† Weikang Huang2†Chaofan Mei2Chuyan Zhong2Leilei Zhu2,3Peiyi Liu2,4Shixin Yuan2,4Zhihua Liu2,3Yueyun Wang1,2,4*
Weikang Huang2†Chaofan Mei2Chuyan Zhong2Leilei Zhu2,3Peiyi Liu2,4Shixin Yuan2,4Zhihua Liu2,3Yueyun Wang1,2,4*- 1Department of Healthcare, Affiliated Shenzhen Maternity and Child Healthcare Hospital, Southern Medical University, Shenzhen, China
- 2Research Team of Cervical Cancer Prevention Project in Shenzhen, Affiliated Shenzhen Maternity and Child Healthcare Hospital, Southern Medical University, Shenzhen, China
- 3Department of Gynecology, Affiliated Shenzhen Maternity and Child Healthcare Hospital, Southern Medical University, Shenzhen, China
- 4Research Institute of Maternity and Child Healthcare, Affiliated Shenzhen Maternity and Child Healthcare Hospital, Southern Medical University, Shenzhen, China
Background: Research gaps exist in addressing the psychological harm related to the cervical cancer screening. Anxiety is the most common distress driven by the screening procedures, which may be affected by past screening experience (PSE) but with uncertainty. This study aimed to evaluate the pre-procedural anxiety in cervical cancer screening and to identify the influence attributed to PSE.
Methods: A cross-sectional survey targeted women seeking for cervical cancer screening services was conducted from June 5th to December 31st, 2020 in Shenzhen. The 20-item state anxiety scale of the State-Trait Anxiety Inventory (STAI-S) was applied to measure pre-procedural anxiety, in which a score of 40 or higher was regarded with anxiety symptom. Logistic regression models were established to explore potential associated factors of pre-procedural anxiety both for women with and without PSE.
Results: Overall, 3,651 women were enrolled, in which 36.1% had never been screened and the remaining 63.9% had been screened at least once before. Women without PSE demonstrated more prevalent pre-procedural anxiety (74.5% vs. 67.8%, P <0.001) than their experienced counterparts. Among women without PSE, having heard of cervical cancer screening was associated with a lower likelihood of pre-procedural anxiety (OR: 0.37, 95%CI: 0.25~0.56). Among experienced women, participating three or more times screening was negatively associated with anxiety symptom (OR: 0.67, 95%CI: 0.53~0.84), however, both receiving screening within three years (OR: 1.58, 95%CI: 1.27~1.97) and unknowing previous screening results (OR: 1.42, 95%CI: 1.11~1.82) increased the susceptibility of pre-procedural anxiety.
Conclusions: Women participating in cervical cancer screening commonly present pre-procedural anxiety. The association between PSE and pre-procedural anxiety may be influenced by past screening times, interval, and results. Psychological counseling according to women’s PSE before cervical cancer screening is warranted of necessity.
Introduction
Cervical cancer is the fourth frequent malignancy in females worldwide (1). Almost all cancers in the cervix were caused by the high-risk human papillomavirus (HPV) (2). Routine cervical screening is one of the most essential prevention strategies, leading to great success in reducing the disease burden. However, women are required to receive gynecological procedures for cervical examination and sampling, which can be regarded as an invasive operation performed by a healthcare provider. Screening related procedures may act as stressors and bring adverse psychological outcomes. Notably, evidence about the psychological harm of cervical screening is restricted to distress induced by switching screening methods, receiving abnormal results, and following colposcopy related procedures (3–5). Research gaps exist in addressing the psychological harm before and during the screening process.
Recent systematic reviews identified the psychological harm of cancer screening procedures, in which anxiety was the most commonly assessed construct (6, 7). Anxiety is thought to be a future-oriented affective status that reflects one’s preparation to cope with uncertainty but possibly negative situations without a triggering stimulus (8). Anxious feelings may be prevalent when women treat pain as the most important determinant of cervical screening participation (9). However, scant studies examined cervical screening related anxiety and only followed non-mainstream screening methods, like optical spectroscopy and visual inspection (10, 11). Anxiety driven by HPV or cytology based methods remain to be investigated.
Past screening experience (PSE) may impact on cervical cancer screening related anxiety. Anxious feelings could appear among those without PSE due to uncertainty of screening procedures. For women who have ever been screened, on one hand, they may prefer less frequent screening in order to avoid frequent anxiety, worry, or nervousness (12). On the other hand, anxiety may also be alleviated by repeated participation and fully understanding of screening procedures, as exposure to the feared situation helps to deal with specific anxiety (13). As more and more females are encouraged to receive cervical screening, there is a urgent need to understand screening related anxiety among women with and without PSE. Hence, based on a cross-sectional survey in Shenzhen, we evaluated the pre-procedural anxiety and associated factors among women seeking for cervical cancer screening services, in order to address the dearth of information about the psychological harm associated to cervical cancer screening and to identify the influence attributed to PSE.
Materials and Methods
Study Setting and Participants
A cross-sectional survey has been conducted from June 5th to December 31st, 2020 in Pinghu Maternity-child Healthcare and Family Planning Service Center of Longgang District, Shenzhen. It has been one of the most influential and public screening centers funded by the local government, offering free screening services of common diseases for nearly 8,000 women per year. Women could have access to cervical cancer screening services if they were engaged in sexual behavior, not pregnant, and at an age range from 20 to 65 years old. During the survey period, women who came to this screening site seeking for cervical cancer screening services and met above criteria were invited to participate in our survey. Here, we exclueded women without a smartphone or incapacitated women due to intellectual or other disability. They would be provided with a full explanation and invitation of the present survey by trained research assistants. With informed consent, women were asked to finish an online questionnaire before they received gynecological assessment and subsequent screening procedures. The questionnaire was available to access via scanning a unique quick response code with their smartphones, which was hosted by WenJuanXing (Changsha Haoxing Information Technology Co., Ltd., China). Totally, we collected 3717 questionnaires and excluded 66 questionnaires with unknown age information or out-of age range. Ethical approval was obtained from the medical ethics committee of Shenzhen Maternity and Child Healthcare Hospital.
Measurement
Demographic Characteristics and Reproductive Health Condition
A structured questionnaire containing different aspects was employed in this study. Demographic characteristics were firstly collected based on self-report, containing age, ethnicity, local household registration, marital status, education level, occupation types, and monthly income level. Information on women’s reproductive health was also required, such as age at menarche and first sexual intercourse (coitarche), the number of sexual partners in recent one year, condom and oral contraceptive use, parity, age at first delivery, malignancy diagnosis of first-degree relatives, and previous diagnosis of vaginitis. Detailed division of above-mentioned variables were listed in Table 1.

Table 1 Characteristics of the participants varied by PSE (N=3651).
Past Cervical Screening Experience
All women were asked to recall previous experience of cervical cancer screening. The past participation of screening was evaluated by asking “Before the survey time, approximately how many times have you ever participated in cervical cancer screening? (none/once/twice/three or more times)”. Women without PSE were assessed with the awareness of cervical cancer screening service via asking “Before the survey time, have you ever heard of cervical cancer screening? (yes/no)”. Specific questions was developed to query past screening experience, containing “When did you receive previous screening? (within/over 3 years)” and “What was the result of previous screening? (normal/abnormal/unknown)”.
Health Habit
We further gathered variables of health habits in their daily routines. Women needed to recall specific life events, including active and passive exposure to smoking, the duration of sitting per day, the number of walking steps per day, and the frequency of physical exercise per week. Here, active smoking was defined as ever or currently smoking at least one cigarette per day on average. In addition, women exposed to tobacco smoke more than 15 minutes, at least one day per week were regarded with passive smoking. Walking steps were calculated according to the pedometer function of their smart-phones. Physical exercise referred to common exercise forms, including sports, running, swimming, dancing, mountain climbing, rope skipping, etc.
Psychological Health Status
Recent psychological health of the participants was measured through an ultra-brief screening scale named the Patient Health Questionnaire-4 (PHQ-4). It consists of a 2-item anxiety scale and a 2-item depression scale, assessing the frequency of psychological distress in recent two weeks. Each item was rated in four response options (not at all=0, several days=1, more than half of the days=2, and almost every day=3). Therefore, a total score of the four items was ranged from 0 to 12. Suggested by previous validation (14), those who scored ≥3 on PHQ-4 were considered to have psychological distress. In the present study, the internal consistency reliability of the PHQ-4 was found to be acceptable (Cronbach’s α: 0.86).
Pre-Procedural Anxiety
Pre-procedural anxiety was assessed by the state anxiety scale of the State-Trait Anxiety Inventory (STAI-S). The STAI-S is composed of 20 items that reflect the transient emotional response to a stressful situation. It measures the anxious symptom at the moment of scoring, which has been widely adopted to identify anxiety in the Chinese population (15). Hence, the participants in our survey were all required to finish the STAI-S prior to gynecological procedures, in order to figure out their present feelings. All items of the STAI-S were responded on a 4-point Likert-type scale, contributing to a total score of 20 to 80. The score of the STAI-S positively correlates with the severity of anxiety. A total score of 40 or higher was applied to reflect anxious symptom in the present study, in line with past investigations (15–17). The Cronbach’s α of STAI-S in this study was 0.88.
Statistical Analyses
All data were analyzed descriptively by means of the SPSS 21.0 software (IBM Corp., Armonk, NY). Categorical variables were presented with numbers and frequencies, and continuous data were presented with means and standard deviations. For women with different characteristics (demographics, reproductive health condition, health habits, etc), the chi-square test was applied to detect the difference of anxiety level across subgroups, while the t-test and one way ANOVA were used to compare the distributed difference of STAI-S score. Logistic regression models were established to explore potential associated factors of pre-procedural anxiety both for women with and without PSE. Variables with P ≤0.10 in the uni-variate analysis were included in the multi-variate logistic regression models. Associated factors were identified with the stepwise procedure. Odds ratios (OR) and 95% confident intervals (CI) were calculated to estimate the strength of associations. Statistical significance was set to be less than 0.05 with a two-tailed test.
Results
Characteristics of All Participants
In total, 3,651 women were included in analysis (Figure 1), with an average age of 40.65 years (standard deviation: 7.56). Of all participants, 36.1% had never been screened before, while the remaining women had been screened at least once (once: 27.8%, twice: 17.5%, and three times or more: 18.6%) (Figure 2). Moreover, 302 women never heard of cervical cancer screening, accounted for 22.9% of non-experienced women. Among women with PSE, approximately three quarters received screening services within recent three years and reported normal screening results.
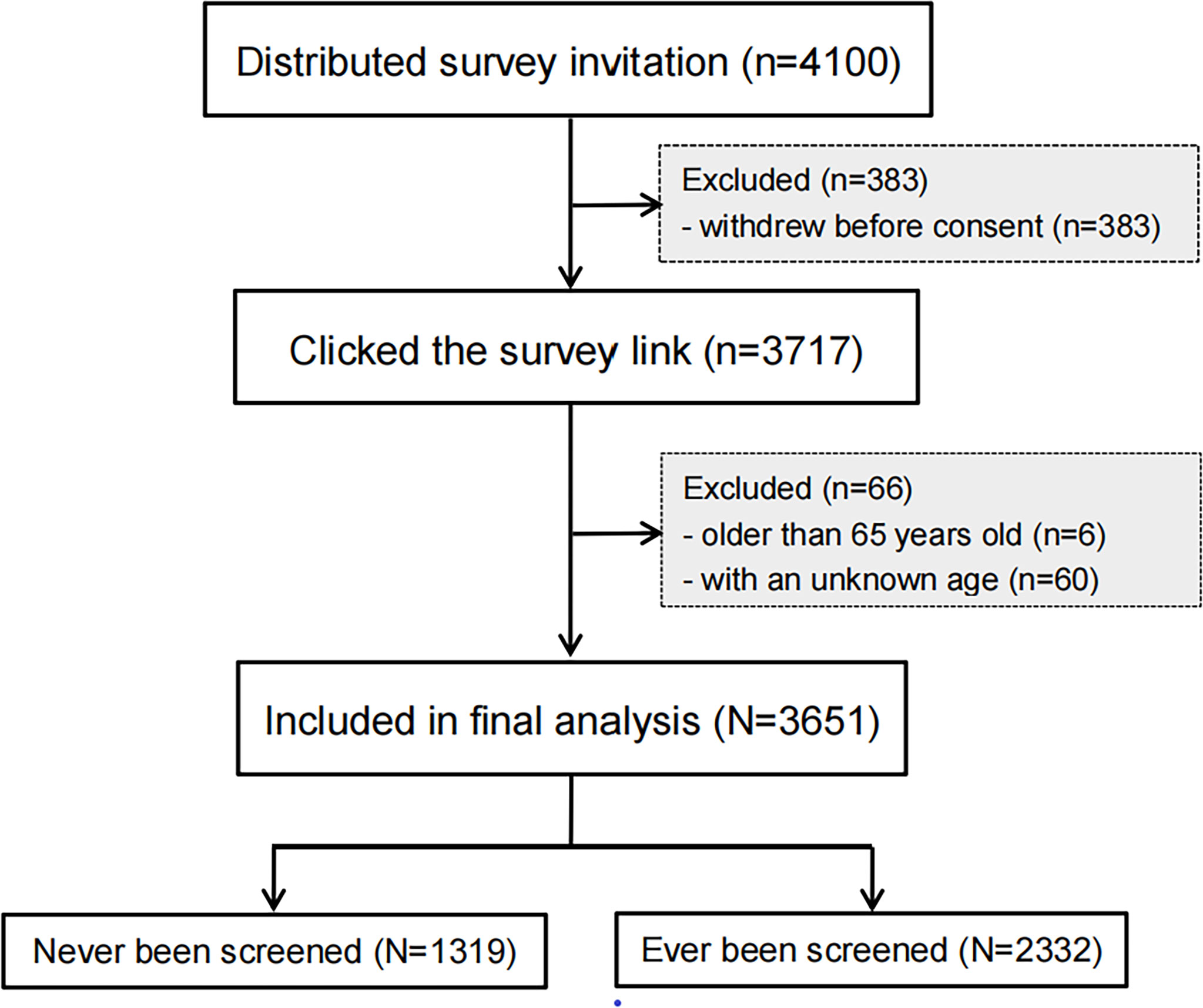
Figure 1 Flow chart diagram of the study population.
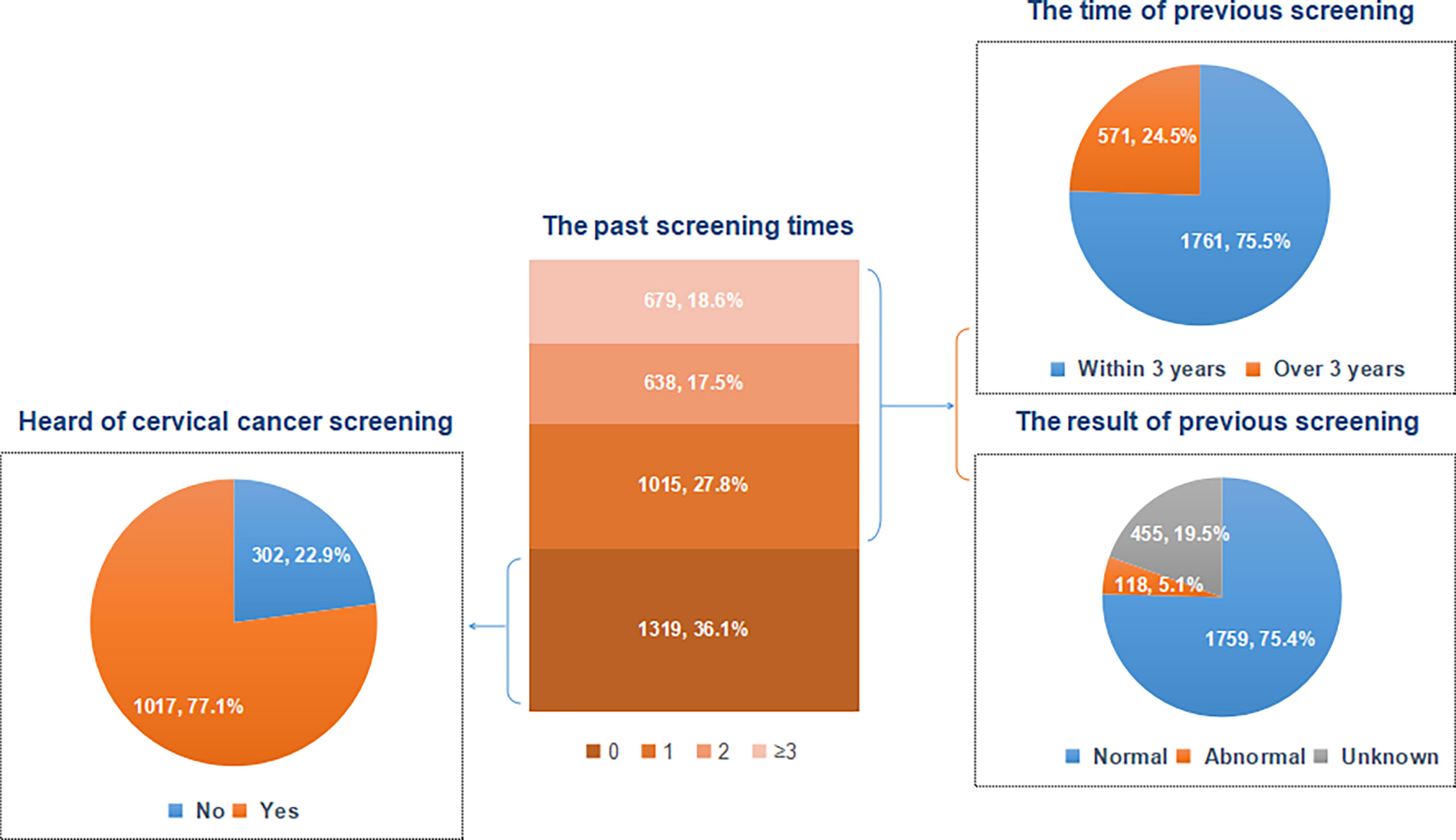
Figure 2 Past cervical cancer screening experience of all participants.
Characteristics of the participants varied by PSE (Table 1). Compared to those without PSE, experienced women were likely to be older, Han ethnic, local household registered, married, and well-educated (all P <0.05). These two groups also varied in occupation types, age at coitarche, the number of sexual partners, parity, malignancy diagnosis of first-degree relatives, and previous diagnosis of vaginitis (all P <0.05). Furthermore, experienced women tended to have healthier habits, such as no smoking, walking more steps, and more frequent physical exercise (all P <0.05).
Prevalence of Pre-Procedural Anxiety in Cervical Cancer Screening
The average score of STAI-S was 42.72 (standard deviation: 8.64) in this survey. Women without PSE demonstrated significantly higher score of STAI-S than those with PSE (43.64 vs. 42.28, P <0.001). When using a cut-off value of 40, the overall prevalence of pre-procedural anxiety was 70.3%. Compared to the experienced counterparts, a higher prevalence of anxious symptom was reported among women without PSE (74.5% vs. 67.8%, P <0.001). The prevalence of anxious symptom decreased with the increased times of past screening participation (P for trend <0.001) (Figure 3). Regardless of whether women had been screened before, distinct STAI-S scores and prevalence of anxiety were detected across subgroups of varied characteristics (Tables 2, 3).
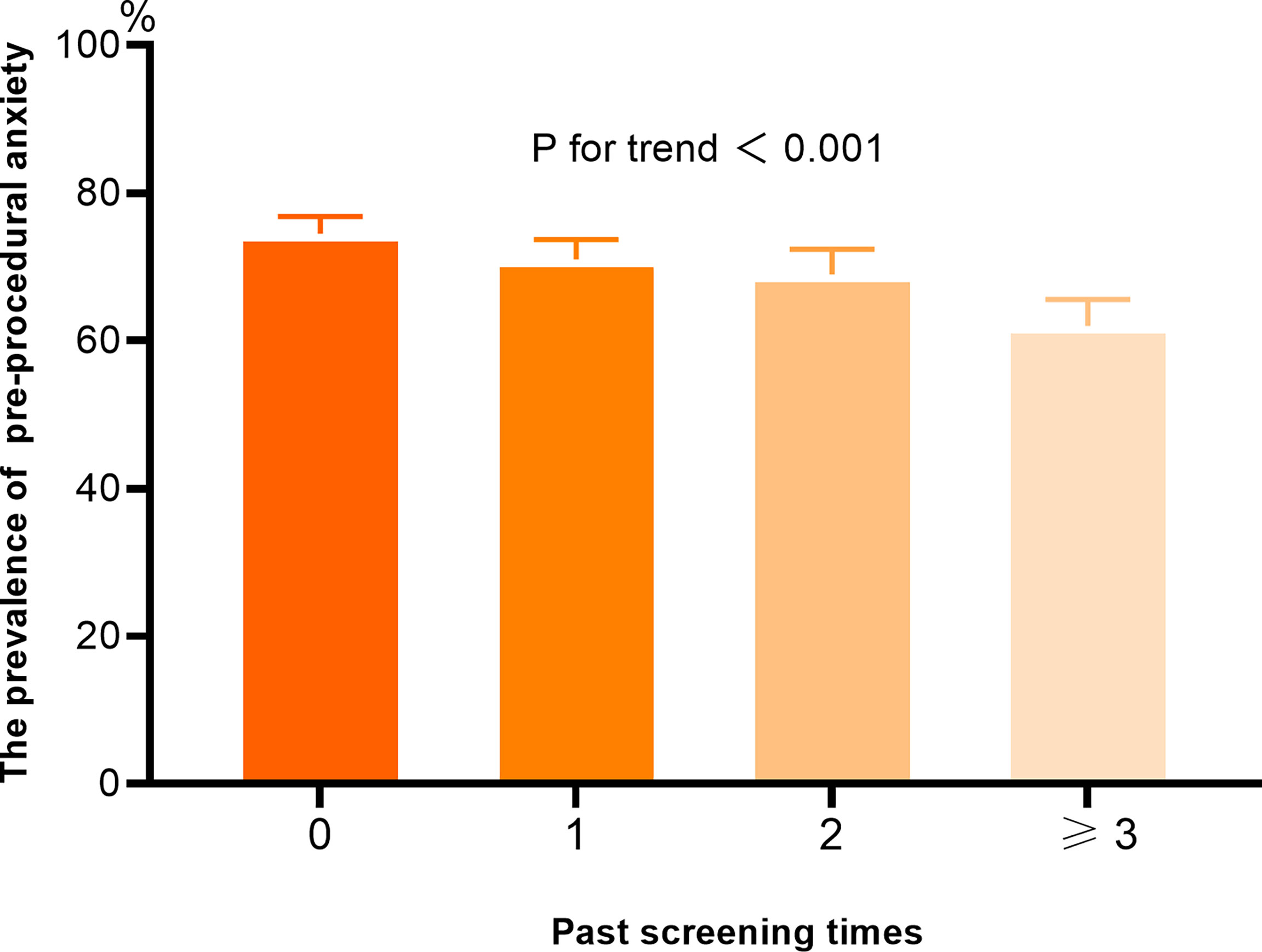
Figure 3 The prevalence of pre-procedural anxiety according to the past screening times.
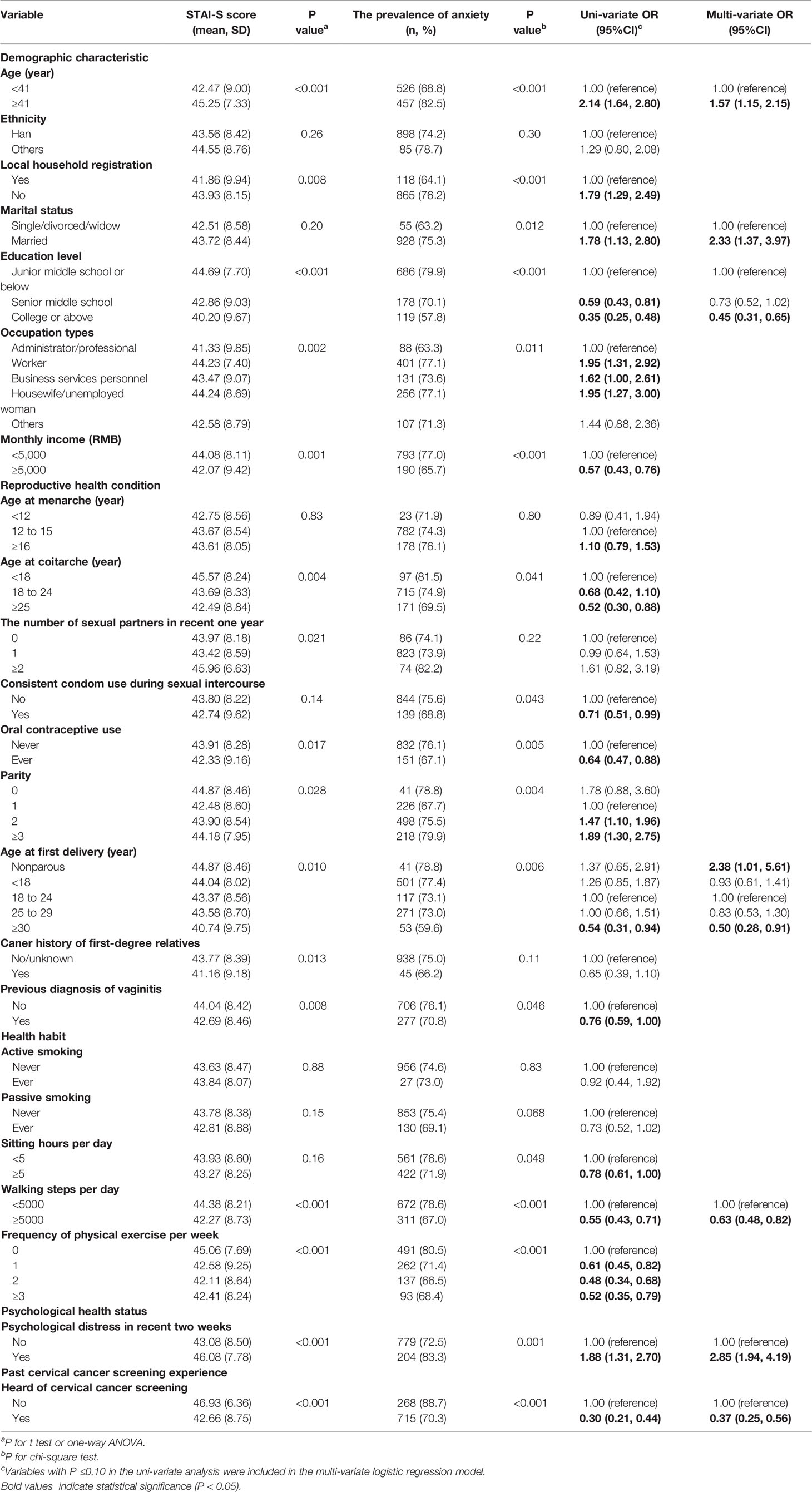
Table 2 Pre-procedural anxiety and associated factors among women without PSE (N=1319).
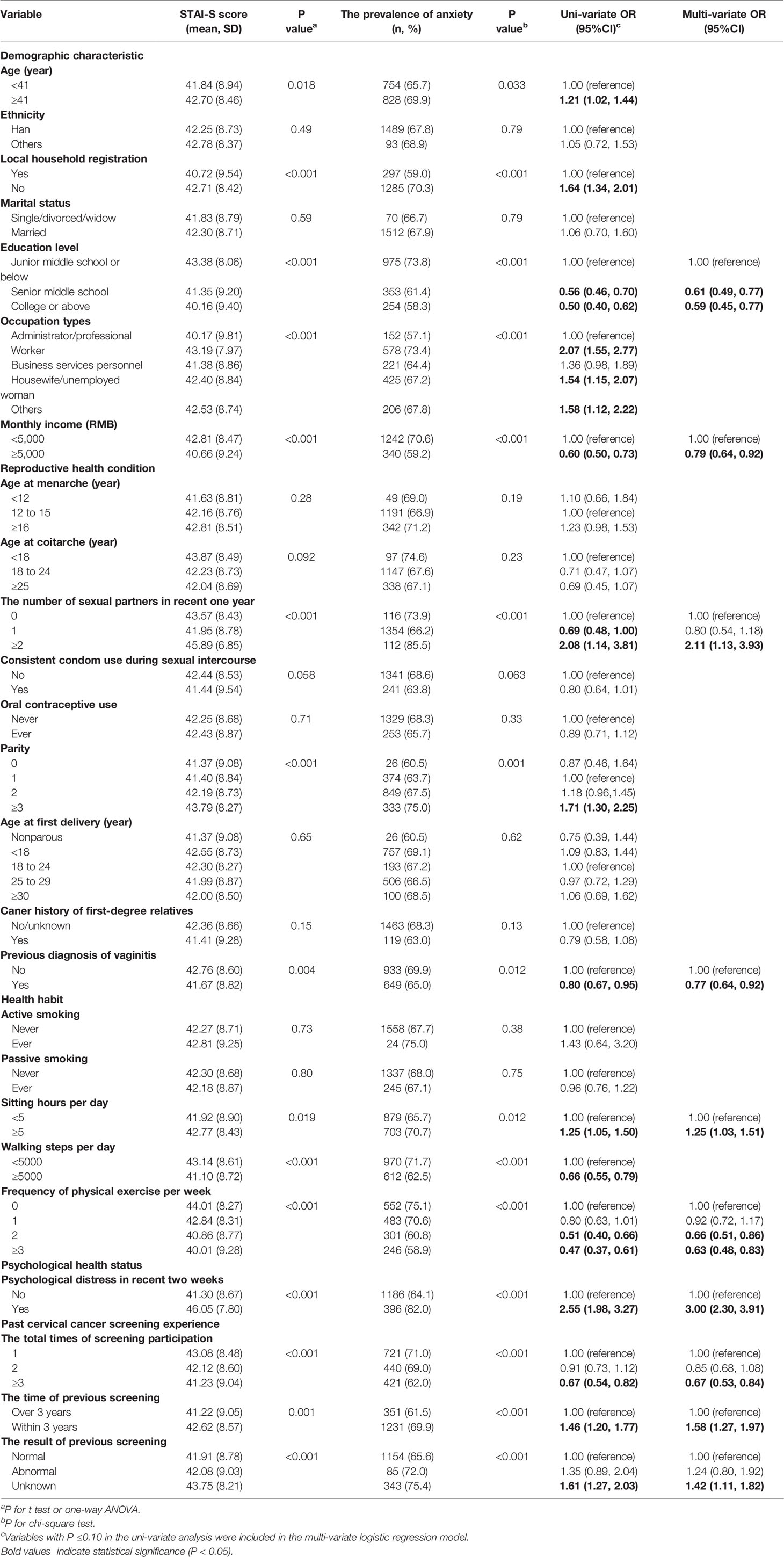
Table 3 Pre-procedural anxiety and associated factors among women with PSE (N=2332).
Factors Associated With Pre-Procedural Anxiety Among Women Without PSE
Factors associated with pre-procedural anxiety among women without PSE were found in the multi-variate logistic regression model (Table 2). Higher odds of being anxious were shown if women were older (OR: 1.57, 95%CI: 1.15~2.15), married (OR: 2.33, 95%CI: 1.37~3.97), nonparous (OR: 2.38, 95%CI: 1.01~5.61), and having psychological distress (OR: 2.85, 95%CI: 1.94~4.19). Potential protective factors of anxiety included receiving higher education (OR: 0.45, 95%CI: 0.31~0.65), having older age at first delivery (OR: 0.50, 95%CI: 0.28~0.91), walking more steps per day (OR: 0.63, 95%CI: 0.48~0.82), and having heard of cervical cancer screening (OR: 0.37, 95%CI: 0.25~0.56).
Factors Associated With Pre-Procedural Anxiety Among Women With PSE
Distinct associated factors were detected among women with PSE (Table 3). Women who were susceptible to pre-procedural anxiety were identified as: having two or more sexual partners (OR: 2.11, 95%CI: 1.13~3.93), sitting longer per day (OR: 1.25, 95%CI: 1.03~1.51), having psychological distress(OR: 3.00, 95%CI: 2.30~3.91), receiving screening within three years (OR: 1.58, 95%CI: 1.27~1.97), and unknowing previous screening results (OR: 1.42, 95%CI: 1.11~1.82). Women that were less likely to be anxious tended to receive higher education (senior middle school: OR: 0.61, 95%CI: 0.49~0.77; college or above: OR: 0.59, 95%CI: 0.45~0.77), earn higher monthly income (OR: 0.79, 95%CI: 0.64~0.92), be diagnosed with vaginitis (OR: 0.77, 95%CI: 0.64~0.92), do physical exercise per week (two times: OR: 0.66, 95%CI: 0.51~0.86; three or more times: OR: 0.63, 95%CI: 0.48~0.83), and participating three or more times screening (OR: 0.67, 95%CI: 0.53~0.84).
Discussion
Negative psychological response to cervical cancer screening procedures has been considered to be a barrier to screening uptake. The present study explicitly investigated the prevalence of pre-procedural anxiety during cervical cancer screening among Chinese females using a cross-sectional design. Overall, nearly three quarters of the participants suffered pre-procedural anxiety, suggesting the substantial psychological harm derived by cervical cancer screening. To our knowledge, this study is a forerunner to explore the influence of PSE on the anxious symptom prior to the cervical cancer screening procedures. Notably, PSE may bring varied effects on the pre-procedural anxiety due to the difference of past screening times, interval and results. These novel findings help to develop proper guidance in reducing the psychological harm and promoting more uptake of cervical cancer screening.
Scant studies investigate the pre-procedural anxiety symptom in cervical cancer screening. This study reported a high level of the pre-procedural anxiety, with over 70% women rating a score above 40 in the STAI-S scale. The mean score (42.72) was much higher than that (30.2) in the USA (10). A relatively lower mean score (33.0) has also been detected before women underwent a Pap smear in the Netherlands (18). Despite of the ethnic, culture, and socio-economic differences, this disparity may also result from the distinct knowledge of HPV and cervical cancer. It has been revealed that better HPV knowledge was associated with lower anxiety and concerns during screening (19). Therefore, the prevalent pre-procedural anxiety in our survey may be partly explained by the knowledge gaps about HPV between China and other developed countries that we have previously found (20). Interestingly, the anxious level before screening was likely to be weaker than that in the diagnosis stage. Irish researchers observed a higher mean score of the STAI-S scale (45.31) prior to colposcopy (21). Colposcopy is usually applied for further diagnostic evaluation after receiving abnormal cervical cancer screening results. The fear of being diagnosed with malignancy along with complicated operations may bring more worries during colposcopy than screening procedures. Pre-procedural anxiety may associate with colposcopy-related pain and discomfort (22, 23). Nevertheless, our findings support the urgent need for the delivery of psychological assessment and support to the female population before screening procedures start.
Past participation of cervical cancer screening may help to reduce the anxiety or other negative psychological reactions in the current screening round. In our study, women without PSE had higher level of pre-procedural anxiety than their experienced counterparts. Similar findings have also been observed in other types of cancer screening. For colorectal cancer screening, patients without previous experience demonstrated greater anxiety when undergoing colonoscopy (24). For breast cancer screening, women who received mammogram at the first time tended to be more distressed than those having prior mammograms (25). However, the impact of PSE on screening-related anxiety may be obscured by a family history of cancer diagnosis. There was a inconsistent finding among women with a family history of breast cancer that women who had undergone mammography screening previously were vulnerable to longer-term distress (26). The possible explanation lies that a woman is more stressful to receive screening services regardless of having PSE if her relative has been diagnosed with or died from cancer. In addition, we noticed that the prevalence of pre-procedural anxiety decreased when the times of past screening participation increased in our study. This contrasted with another study in breast cancer screening, in which the anxiety level increased with the number of previous mammograms done (27). The difference in screening methods, medical apparatus and instruments, and body parts lead to these inconclusive findings to some extent, however, other screening-related factors may play a potential role in the link between PSE and anxiety, such as screening frequency, and past screening results.
In our study, distinct associated factors of pre-procedural anxiety between women with and without PSE were found, especially variables specific to PSE. Among women with PSE, we confirmed the impact of past screening times on pre-procedural anxiety that women participating three or more times screening had less likelihood of being anxious. A similar result were detected among women without PSE that having heard of cervical cancer screening was associated with less anxiety. Both more screening participation and heard of screening indicate a better understanding of the screening procedures, which may help women to reduce the psychological discomfort in cervical cancer screening. Notably, this protective effect may be counteracted by a short screening interval (within three years) and uncertainty of previous screening results as we observed in the present study. According to the screening guidelines, women can be screened every three or five years unless positive screening results for HPV testing or cytology appear (28). This means that screening repeatedly within three years is more likely to be owing to abnormal screening results, which may bring a heavier psychological burden (4, 29, 30). Furthermore, overscreening may present in these women, which can also result in significant anxiety (31). For women unknowing past screening results, less self-confidence and more worries in health status may become more salient when they engage in a new round of screening. Consedine et al. has proposed that there are different sources of anxiety in cancer screening, including fear of the screening process (e.g. pain, discomfort, embarrassment), fear of the screening outcomes, and undifferentiated fear of cancer (32). Hence, it can be inferred that PSE affects the sources of pre-procedural anxiety in different manners. Fear of the screening process may be alleviated by past participation of screening, while fear of the screening outcome or getting cancer may be aggravated by a short screening interval and previous uncertain results. Further population-based investigations are needed to verify the contribution of PSE to pre-procedural anxiety with different sources in cervical cancer screening.
Study limitations were shown in the present study. As the study sample came from only one screening center as well as smartphone users, the prevalence of pre-procedural anxiety might be not able to generalize to the whole population in cervical cancer screening. Recall bias on PSE and other key information could not be avoided due to self-reported answers. Moreover, we conducted psychological assessment prior to the screening process rather than during the screening procedure, which might lead to underestimation of anxious feeling. The sources of anxiety could not be distinguished in our study as well. Thus, precise classification evaluation of screening related anxiety should be considered in further investigations. In addition, Women’s psychological health status may be influenced by the COVID-19 pandemic to some extent. However, there was no difference of psychological distress in recent two weeks between women with and without PSE. Simultaneously, no local COVID-19 cases had been detected in Shenzhen during the survey time period. The impacts of the COVID-19 pandemic could be limited.
In conclusion, the current study lends to support that women participating in cervical cancer screening commonly present pre-procedural anxiety. Importantly, PSE may help to alleviate pre-procedural anxiety, which is influenced by past screening times, interval, and results. Even if women have not been screened before, having heard of cervical cancer screening is associated a lower likelihood of pre-procedural anxiety. Psychological counseling according to women’s PSE before cervical cancer screening is warranted of necessity.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by the medical ethics committee of Shenzhen Maternity and Child Healthcare Hospital. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
WL wrote and presented the original draft. WL, WH, CZ, and LZ were involved in data curation and visualization. WL, WH, CM, PL, ZL, and YW were involved in methodology, software, analysis, review and editing. WL, WH, and CM revised the manuscript and polished the language. SY and YW were involved in supervision. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Shenzhen Healthcare Research Project (Grant No. SZGW2018005) and the Sanming Project of Medicine in Shenzhen (Grant No. SZSM201612042).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank all the participants for their time and efforts. Special thanks go to Dr. Hong Yu and Dr. Yuedi Liu from Pinghu Maternity-child Healthcare and Family Planning Service Center of Longgang District, Shenzhen for providing strong support in this survey.
References
1. Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical Cancer. Lancet (2019) 393:169–82. doi: 10.1016/S0140-6736(18)32470-X
2. Schiffman M, Castle PE, Jeronimo J, Rodriguez AC, Wacholder S. Human Papillomavirus and Cervical Cancer. Lancet (2007) 370:890–907. doi: 10.1016/S0140-6736(07)61416-0
3. Andreassen T, Hansen BT, Engesaeter B, Hashim D, Støer NC, Tropé A, et al. Psychological Effect of Cervical Cancer Screening When Changing Primary Screening Method From Cytology to High-Risk Human Papilloma Virus Testing. Int J Cancer (2019) 145:29–39. doi: 10.1002/ijc.32067
4. Dodd RH, Mac O, Brotherton J, Cvejic E, McCaffery KJ. Levels of Anxiety and Distress Following Receipt of Positive Screening Tests in Australia's HPV-Based Cervical Screening Programme: A Cross-Sectional Survey. Sex Transm Infect (2020) 96:166–72. doi: 10.1136/sextrans-2019-054290
5. O'Connor M, Gallagher P, Waller J, Martin CM, O'Leary JJ, Sharp L. Adverse Psychological Outcomes Following Colposcopy and Related Procedures: A Systematic Review. BJOG (2016) 123:24–38. doi: 10.1111/1471-0528.13462
6. Chad-Friedman E, Coleman S, Traeger LN, Pirl WF, Goldman R, Atlas SJ, et al. Psychological Distress Associated With Cancer Screening: A Systematic Review. Cancer-Am Cancer Soc (2017) 123:3882–94. doi: 10.1002/cncr.30904
7. Kim A, Chung KC, Keir C, Patrick DL. Patient-Reported Outcomes Associated With Cancer Screening: A Systematic Review. BMC Cancer (2022) 22:223. doi: 10.1186/s12885-022-09261-5
8. Giacobbe P, Flint A. Diagnosis and Management of Anxiety Disorders. Continuum (Minneap Minn) (2018) 24:893–919. doi: 10.1212/CON.0000000000000607
9. Basen-Engquist K, Fouladi RT, Cantor SB, Shinn E, Sui D, Sharman M, et al. Patient Assessment of Tests to Detect Cervical Cancer. Int J Technol Assess Health Care (2007) 23:240–7. doi: 10.1017/S0266462307070171
10. Basen-Engquist K, Shinn EH, Warneke C, de Moor C, Le T, Richards-Kortum R, et al. Patient Distress and Satisfaction With Optical Spectroscopy in Cervical Dysplasia Detection. Am J Obstet Gynecol (2003) 189:1136–42. doi: 10.1067/s0002-9378(03)00540-4
11. Camail R, Kenfack B, Tran PL, Viviano M, Tebeu PM, Temogne L, et al. Benefit of Watching a Live Visual Inspection of the Cervix With Acetic Acid and Lugol Iodine on Women's Anxiety: Randomized Controlled Trial of an Educational Intervention Conducted in a Low-Resource Setting. JMIR Cancer (2019) 5:e9798. doi: 10.2196/cancer.9798
12. Gerend MA, Shepherd MA, Kaltz EA, Davis WJ, Shepherd JE. Understanding Women's Hesitancy to Undergo Less Frequent Cervical Cancer Screening. Prev Med (2017) 95:96–102. doi: 10.1016/j.ypmed.2016.11.028
13. Swedish Council on Health Technology Assessment. Treatment of Anxiety Disorders: A Systematic Review. Stockholm: SBU Yellow Report (2005).
14. Xu Y, Zhang R, Zhou Z, Fan J, Liang J, Cai L, et al. Parental Psychological Distress and Attitudes Towards COVID-19 Vaccination: A Cross-Sectional Survey in Shenzhen, China. J Affect Disord (2021) 292:552–8. doi: 10.1016/j.jad.2021.06.003
15. Lin Y, Hu Z, Alias H, Wong LP. Knowledge, Attitudes, Impact, and Anxiety Regarding COVID-19 Infection Among the Public in China. Front Public Health (2020) 8:236. doi: 10.3389/fpubh.2020.00236
16. Wu Y, Lu YC, Jacobs M, Pradhan S, Kapse K, Zhao L, et al. Association of Prenatal Maternal Psychological Distress With Fetal Brain Growth, Metabolism, and Cortical Maturation. JAMA Netw Open (2020) 3:e1919940. doi: 10.1001/jamanetworkopen.2019.19940
17. Wangmar J, von Vogelsang AC, Hultcrantz R, Fritzell K, Wengström Y, Jervaeus A. Are Anxiety Levels Associated With the Decision to Participate in a Swedish Colorectal Cancer Screening Programme? A Nationwide Cross-Sectional Study. BMJ Open (2018) 8:e25109. doi: 10.1136/bmjopen-2018-025109
18. Korfage IJ, van Ballegooijen M, Wauben B, Looman CW, Habbema JD, Essink-Bot ML. Having a Pap Smear, Quality of Life Before and After Cervical Screening: A Questionnaire Study. BJOG (2012) 119:936–44. doi: 10.1111/j.1471-0528.2012.03344.x
19. Markovic-Denic L, Djuric O, Maksimovic N, Popovac S, Kesic V. Effects of Human Papillomavirus Awareness and Knowledge on Psychological State of Women Referred to Cervical Cancer Screening. J Low Genit Tract Dis (2018) 22:178–83. doi: 10.1097/LGT.0000000000000397
20. Lin W, Wang Y, Liu Z, Chen B, Yuan S, Wu B, et al. Awareness and Attitude Towards Human Papillomavirus and Its Vaccine Among Females With and Without Daughter(s) Who Participated in Cervical Cancer Screening in Shenzhen, China. Trop Med Int Health (2019) 24:1054–63. doi: 10.1111/tmi.13283
21. Kola S, Walsh JC. Determinants of Pre-Procedural State Anxiety and Negative Affect in First-Time Colposcopy Patients: Implications for Intervention. Eur J Cancer Care (Engl) (2012) 21:469–76. doi: 10.1111/j.1365-2354.2011.01317.x
22. Baser E, Togrul C, Ozgu E, Esercan A, Caglar M, Gungor T. Effect of Pre-Procedural State-Trait Anxiety on Pain Perception and Discomfort in Women Undergoing Colposcopy for Cervical Cytological Abnormalities. Asian Pac J Cancer Prev (2013) 14:4053–6. doi: 10.7314/apjcp.2013.14.7.4053
23. Handelzalts JE, Krissi H, Levy S, Broitman M, Binyamin L, Peled Y. Multidimensional Associations of Pain and Anxiety Before and After Colposcopy. Int J Gynaecol Obstet (2015) 131:297–300. doi: 10.1016/j.ijgo.2015.05.038
24. Yang C, Sriranjan V, Abou-Setta AM, Poluha W, Walker JR, Singh H. Anxiety Associated With Colonoscopy and Flexible Sigmoidoscopy: A Systematic Review. Am J Gastroenterol (2018) 113:1810–8. doi: 10.1038/s41395-018-0398-8
25. Mainiero MB, Schepps B, Clements NC, Bird CE. Mammography-Related Anxiety: Effect of Preprocedural Patient Education. Women Health Iss (2001) 11:110–5. doi: 10.1016/s1049-3867(00)00071-2
26. Brain K, Henderson BJ, Tyndel S, Bankhead C, Watson E, Clements A, et al. Predictors of Breast Cancer-Related Distress Following Mammography Screening in Younger Women on a Family History Breast Screening Programme. Psychooncology (2008) 17:1180–8. doi: 10.1002/pon.1355
27. Bölükbaş N, Erbil N, Kahraman AN. Determination of the Anxiety Level of Women Who Present for Mammography. Asian Pac J Cancer Prev (2010) 11:495–8.
28. Fontham E, Wolf A, Church TR, Etzioni R, Flowers CR, Herzig A, et al. Cervical Cancer Screening for Individuals at Average Risk: 2020 Guideline Update From the American Cancer Society. CA Cancer J Clin (2020) 70:321–46. doi: 10.3322/caac.21628
29. McBride E, Marlow L, Forster AS, Ridout D, Kitchener H, Patnick J, et al. Anxiety and Distress Following Receipt of Results From Routine HPV Primary Testing in Cervical Screening: The Psychological Impact of Primary Screening (PIPS) Study. Int J Cancer (2020) 146:2113–21. doi: 10.1002/ijc.32540
30. Markovic-Denic L, Popovac S, Djuric O, Perisic Z, Rakic S. Psychological Effects of Concurrent Cytology and Colposcopy Testing in Women Referred to Cancer Counseling Outpatient Clinic in Belgrade. J Buon (2017) 22:214–23.
31. Practice Bulletin No. 168: Cervical Cancer Screening and Prevention. Obstet Gynecol (2016) 128:e111–30. doi: 10.1097/AOG.0000000000001708
Keywords: cervical cancer, past screening experience, pre-procedural anxiety, psychological harm, associated factor
Citation: Lin W, Huang W, Mei C, Zhong C, Zhu L, Liu P, Yuan S, Liu Z and Wang Y (2022) Pre-Procedural Anxiety and Associated Factors Among Women Seeking for Cervical Cancer Screening Services in Shenzhen, China: Does Past Screening Experience Matter? Front. Oncol. 12:857138. doi: 10.3389/fonc.2022.857138
Received: 18 January 2022; Accepted: 03 June 2022;
Published: 06 July 2022.
Edited by:
Marine Hovhannisyan, Yerevan State Medical University, ArmeniaReviewed by:
Komsun Suwannarurk, Thammasat University, ThailandLeila Allahqoli, Iran University of Medical Sciences, Iran
Copyright © 2022 Lin, Huang, Mei, Zhong, Zhu, Liu, Yuan, Liu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yueyun Wang, d2FuZ3l1ZXl1bkAxMjYuY29t
†These authors have contributed equally to this work