 Lachlan McDowell
Lachlan McDowell Danny Rischin
Danny Rischin Karla Gough4,5
Karla Gough4,5- 1Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, VIC, Australia
- 2Sir Peter MacCallum Department of Oncology, The University of Melbourne, Melbourne, VIC, Australia
- 3Department of Medical Oncology, Peter MacCallum Cancer Centre, Melbourne, VIC, Australia
- 4Department of Health Services Research, Peter MacCallum Cancer Centre, Melbourne, VIC, Australia
- 5Department of Nursing, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Carlton, VIC, Australia
- 6Department of Radiation Oncology, Stephenson Cancer Center, University of Oklahoma, Oklahoma City, OK, United States
Head and neck squamous cell carcinoma (HNSCC) is the most common cancer involving the mucosal surfaces of the head and neck and is associated with a number of etiological factors, including cigarette smoking, alcohol and betel nut consumption and exposure to high-risk human papillomavirus. The risk of HNSCC increases with age, peaking in the seventh and eighth decade, but this varies by anatomical and histological subtype. While several advancements have been made in the treatment of head and neck cancer (HNC) in recent decades, undertaking curative treatment still subjects the majority of HNSCC patients to substantial treatment-related toxicity requiring patients to tolerate a gamut of physical, psychological, and emotional demands on their reserves. In conjunction with other patient-related factors, clinicians involved in treating patients with HNSCC may incorporate advancing chronological age into their decision-making process when determining treatment recommendations. While advancing chronological age may be associated with increased concerns regarding physical treatment tolerability, clinicians may also be concerned about heightened vulnerability in various health and wellbeing outcomes. The available literature, however, does not provide evidence of this vulnerability in patients with advancing age, and, in many instances, older patients self-report greater resilience compared to their younger counterparts. While this data is reassuring it is limited by selection bias and heterogeneity in trial and study design and the absence of a consistent definition of the elderly patient with HNSCC. This narrative review article also includes a review of the measures used to assess HRQL, psychosocial outcomes and unmet needs in elderly or older patients with HNSCC.
Introduction
Worldwide, head and neck cancer (HNC) accounts for more than 650,000 cases and 330,000 deaths annually and the majority of these are squamous cell carcinomas (HNSCC) (1). Treatment recommendations depend on many factors, including tumor subsite, stage, and pathologic findings, but typically involves surgery and radiation therapy (with or without systemic therapy) either alone or in combination (2). Proceeding along a curative course of treatment for any HNC exposes survivors to the possibility of permanent impairment, including those required for basic human functioning such as chewing, swallowing, tasting and communicating, and loss in these and other domains may also impose significant psychological and emotional challenges (3). It is therefore incumbent upon the HNC physician to weigh the benefits and risks of all therapeutic options, balancing the chance of cure and cost of suboptimal locoregional treatment against the potential toxicity and negative health and wellbeing impacts of curative-intent treatment. Numerous factors weigh into this decision, including performance status, perceived frailty, social supports, individual preferences for pursuing curative treatment and the individual’s physical and mental reserve, among others. Age, whether chronological or the individuals’ perceived biological age, is but one of a host of factors that clinicians may consider during this process.
There is no readily accepted or reliable threshold for defining an “older” HNC patient to incorporate into clinical decision-making, an observation reflecting the degree of variation in ability, functioning and capacity in older adults. As a consequence, tailored treatment recommendations for older patients have been lacking due to an underrepresentation in clinical trials (4). Defining the optimal treatment strategies for these patients, if they differ at all, should be considered a priority for our specialty given the advancing age of the average HNC patient. In the United States for example, the proportion of HNC patients over the age of 65 years is expected to increase from 54% in 2010 to 66% in 2030 (5). In addition, while much attention has been placed on an epidemic of younger patients presenting with human papillomavirus-associated oropharyngeal cancer (HPV+ OPC) the projected increased number of HPV+ OPC cases in the United States from 2016 to 2029 will be driven almost exclusively by patients over 65 years of age (6, 7). Aggressive treatment is definitely feasible for selected older patients with HNC, but reliance on chronological age in isolation may result in over- or under-treatment, and while functional measures may provide superior discrimination in predicting survival and the tolerability of therapy (8–14), they are time intensive and require considerable multidisciplinary expertise (15).
But what other factors do we need to consider for the older HNC patient? And where is the patient’s voice within this complex decision-making process? Do preferences for pursuing radical treatment and cure change with age? Do priorities and preferences for different oncological and functional outcomes change with increasing age? Do older patients demonstrate increased vulnerability to adverse health and wellbeing outcomes when aggressive treatment strategies are employed? Do older HNC patients have more unmet needs following completion of treatment? This narrative review will draw on published research incorporating patient-reported outcomes to examine these questions. Where possible, we have narrowed the scope to focus on studies reporting outcomes in HNSCC; however, many of the studies were very broad in their selection criteria (tumour subsite and histology) and treatment received including any treatment modifications that may have been made to improve treatment tolerance in older patients. Out of necessity, where suitable data was otherwise lacking, some mixed studies have been included in this review. It should also be acknowledged that specific details about patients’ baseline functional performance were lacking, and the presented studies largely included older patients considered fit for a radical course of treatment, introducing a degree of selection bias. Hence, these results cannot be extrapolated to poorly performing older patients.
Defining “Elderly” Head and Neck Cancer Patients
There is no strict chronological boundary for defining “elderly” patients with cancer. The United Nations and World Health Organization have defined elderly patients as those above 60 (16), while in many developed countries, the designation is tied to retirement, which varies between jurisdictions from 55 to 70 years of age (17). Further refinement of old, including young old (65–74), older old (75–84) and oldest old (≥85) have been proposed and adopted by the National Institute on Aging (18). The European Organization for Research and Treatment of Cancer (EORTC) recommended a cut-off of 70 years of age for their elderly HRQL module, the EORTC QLQ-ELD14 (19). Specifically in HNC, 70 years of age would be considered the most common clinically utilized threshold for decision-making available (4) based on the reported reduction in efficacy of concurrent chemotherapy observed in patients above this threshold (20). However, older patients have typically been underrepresented in HNC and HNSCC clinical trials (4), and caution should be observed in drawing too firm a conclusion given the significant improvement yielded in younger cohorts and the catastrophic complications of treatment failure. While the additional benefit of chemotherapy to locoregional treatment in the elderly remains an unresolved issue, it remains a fertile area of research, one where future studies, in particular, secondary analyses from phase II and III studies, could address questions of efficacy while also providing prospective and high quality data on patient-reported toxicity, HRQL and distress. Such data may provide clinically useful information to aid shared-decision making in older patients with HNSCC.
While there is conjecture and variation surrounding an exact age-related definition of elderly, it is somewhat arbitrary; instead, clarifying core variables such as biological age, medical co-morbidity and frailty lie at the heart of what the clinician is trying to ascertain – whether the patient has sufficient reserve to tolerate the physiological insults of radical treatment. While there has been some tantalizing preliminary work focusing on methods to determine an individuals’ epigenetic clock in HNC patients, it is currently difficult, if not impossible, to measure biological age reliably. This will be discussed in more detail in a subsequent section (21, 22). We acknowledge the limitations of chronological age as a predictor for treatment tolerance, particularly when used in isolation; however, it is a parameter that is commonly used both in clinical and research settings and the purpose of this review was to address variations in health and wellbeing outcomes based on chronological age, rather than other variables, which may provide useful additional data.
Treatment and Outcome Preferences in Older Patients With HNC and HNSCC
Do older patients with HNC prioritize oncologic outcomes, such as cure, survival and functional outcomes like preserving swallow and communicating, differently than younger patients with HNC? The Chicago Priority Scale is one of the most frequently used instruments in the HNC cancer literature to characterize treatment outcome priorities (23, 24). Patients (or controls) are asked to rank their disease and functional outcome goals in order from first to last for 12 different outcomes; these are listed in Table 1. In the first of these studies, which included newly diagnosed HNC patients (n=131) from nine institutions, older patients less frequently prioritized oncological outcomes, such as cure and survival (“living as long as possible) in the top three items. The median age in this study was 59 years (range 29-87 years). In those patients aged <55 years, 55-64 years and >65 years, the frequency of ranking the cure item in the highest three priorities was 98%, 96% and 84%, respectively. While this difference was statistically significant (p<0.05), it is clear that the vast majority of older patients place a high value on being cured of their cancer. Interestingly, the older patients did less frequently prioritize length of life or survival, with the “living as long as possible” outcome showing a more notable drop off in the top three ranked items across the same three age groups (73%, 48% and 43%, respectively, p=0.01).
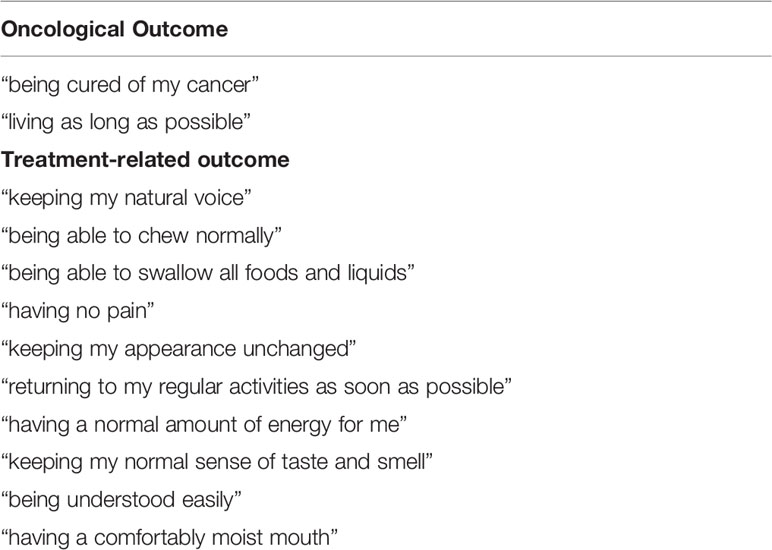
Table 1 Chicago priorities scale.
List et al. subsequently reported results for a larger sample of recently diagnosed, but untreated HNC patients (n=247) in parallel to a control sample (n=131) of non-cancer patients with no personal experience of HNC in close friends or relatives. Similar findings were observed, with most of the “older” group of patients in this series (older was defined by the median split at >58 years) placing the cure outcome in the top three outcomes (≤58: 93% vs >58: 87%). However, older patients also prioritized the “keeping appearances unchanged” item in the top three items more frequently than younger patients (13% vs 5%). Similar observations for both cure, length of life and appearances were observed in the control group.
The Chicago Priority Scale was also used to assess preferences in a more contemporary cohort of patients from John Hopkins, which importantly included many patients with HPV+ OPC (88/150, 59%) (25). Investigators conducted a one-time interview of patients with a mix of HNSCC tumor sites and treatments (surgery ± adjuvant therapy 70%, primary CRT/RT 30%), and the time since treatment completion also varied (median 7 months, IQR 1.5-23.5 months). The median age in this study was lower than in both prior studies (median 54, IQR 54-67, range 26-90). Cure was considered the highest priority at all ages with no differences reported with increasing decade of life. Like both studies by List and colleagues, survival (“living as long as possible”) was less important with increasing age, a finding unchanged after adjustment for HPV status, disease stage and HRQL scores. In the full cohort, the survival outcome was ranked the second most important outcome after cure (median rank 2.5, IQR 2-9), in those aged 75 or over the median rank of the survival outcome was only 6 (IQR 2-11). Nonetheless, there was wider variability in the ranking of the survival item in older patients. In this study, treatment regret using the Ottawa Decision Regret Scale also did not vary by age. In a smaller series of 37 HPV+ OPC patients also from John Hopkins which included patients aged <60 years (23/37,62%), 60-69 years (7/37, 19%) and ≥70 years (7/37, 19%), Windon et al. noted few changes in treatment priorities from baseline (median 1 month after diagnosis, IQR 1-2 months) to post-treatment (median 8 months after treatment, IQR 7-10 months) with the exception that the chewing normally item was increasingly prioritized with older age in the post-treatment setting compared to its initial ranking.
Patient preferences have been appraised in other settings, for instance, where survival may be traded for reduced toxicity or organ preservation. In a Canadian study, Brotherston et al. reported that 51 previously-treated (≥3 months earlier) oropharyngeal cancer patients were willing to accept very little reduction in survival for a reduction in toxicity (which, in this case, was omitting chemotherapy), and when analyzed by age (median age 58 years; 60-69 years: 19/51, 37%, ≥70 years 4/51, 8%) there were no differences in cure sacrifice thresholds (26). In patients treated for advanced laryngeal cancers, at least one study has shown that age was not significantly associated with variations in the willingness to trade laryngeal preservation for survival (27).
In the studies reviewed, cure remains a high priority for HNC patients irrespective of age. Treatment outcome priorities and preferences studies provide some useful broad concepts to guide clinicians but are not a surrogate for eliciting preferences from patients at an individual level, which must remain first and foremost in any shared decision-making model.
Health-Related Quality of Life
A large number of studies have examined age-related variations in health-related quality of life (HRQL) outcomes; however, these reports vary in design (longitudinal or cross-sectional) and how age has been included as a variable (categorical or continuous) in the analysis. Relevant studies have been tabulated for ease of reference, including longitudinal (Table 2) and cross-sectional studies (Table 3) that have modeled age as a categorical variable, single-arm studies enrolling only elderly patients (Table 4) and those that have modeled age as a continuous variable (Table 5). Yet another strategy in the literature has been to compare the outcomes of elderly patients to age-matched population controls, allowing the authors to account for changes expected with normal aging.
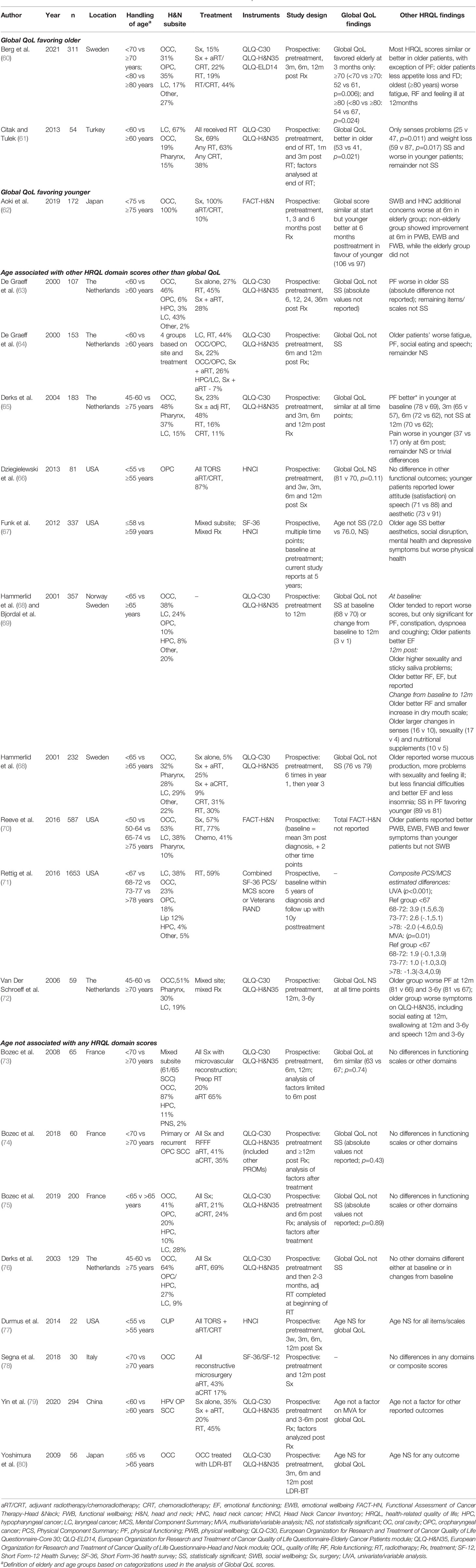
Table 2 Prospective studies reporting health-reported quality of life in elderly patientsa.
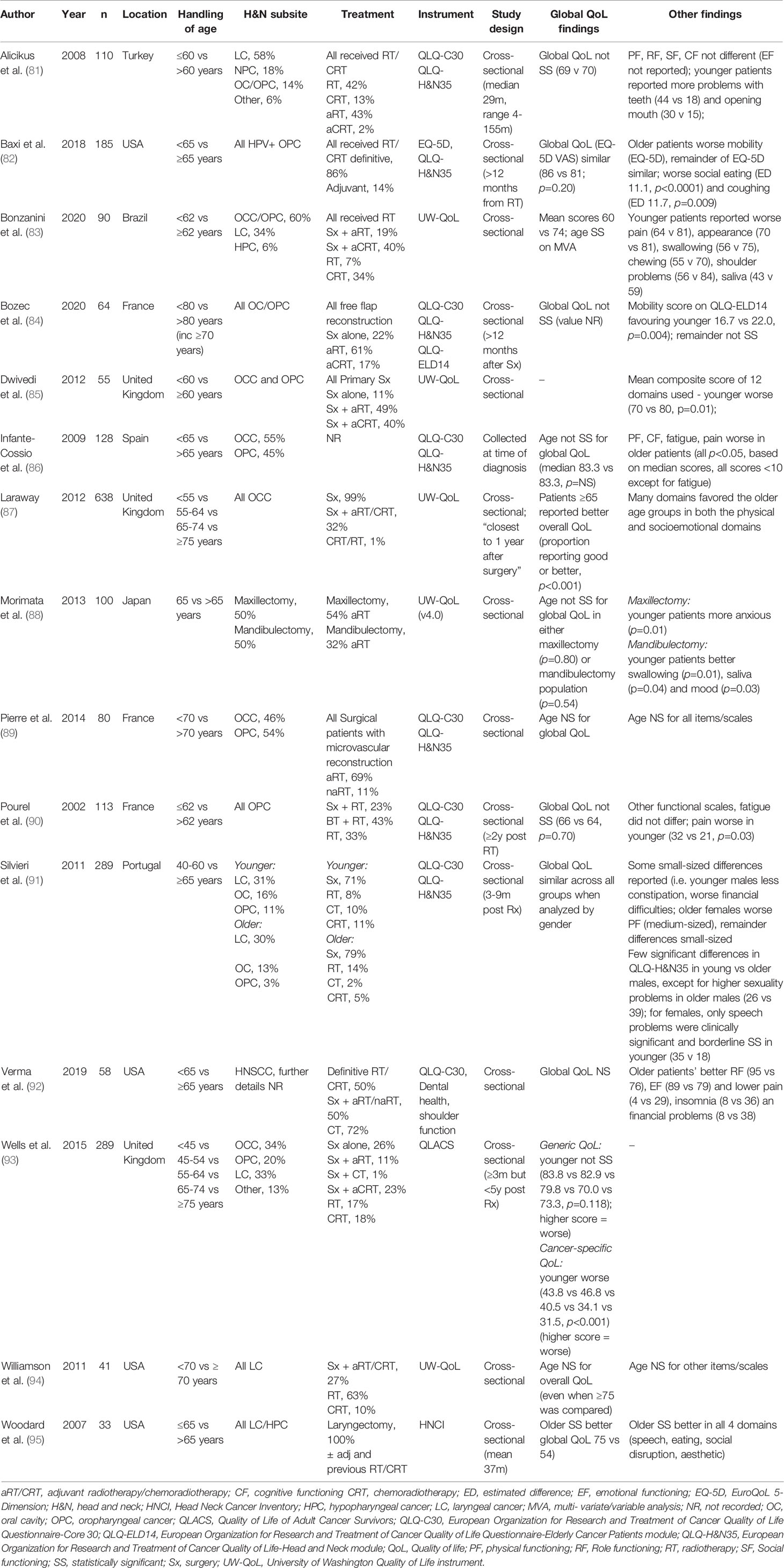
Table 3 Cross-sectional studies reporting health-reported quality of life in elderly HNSCC cohorts. .
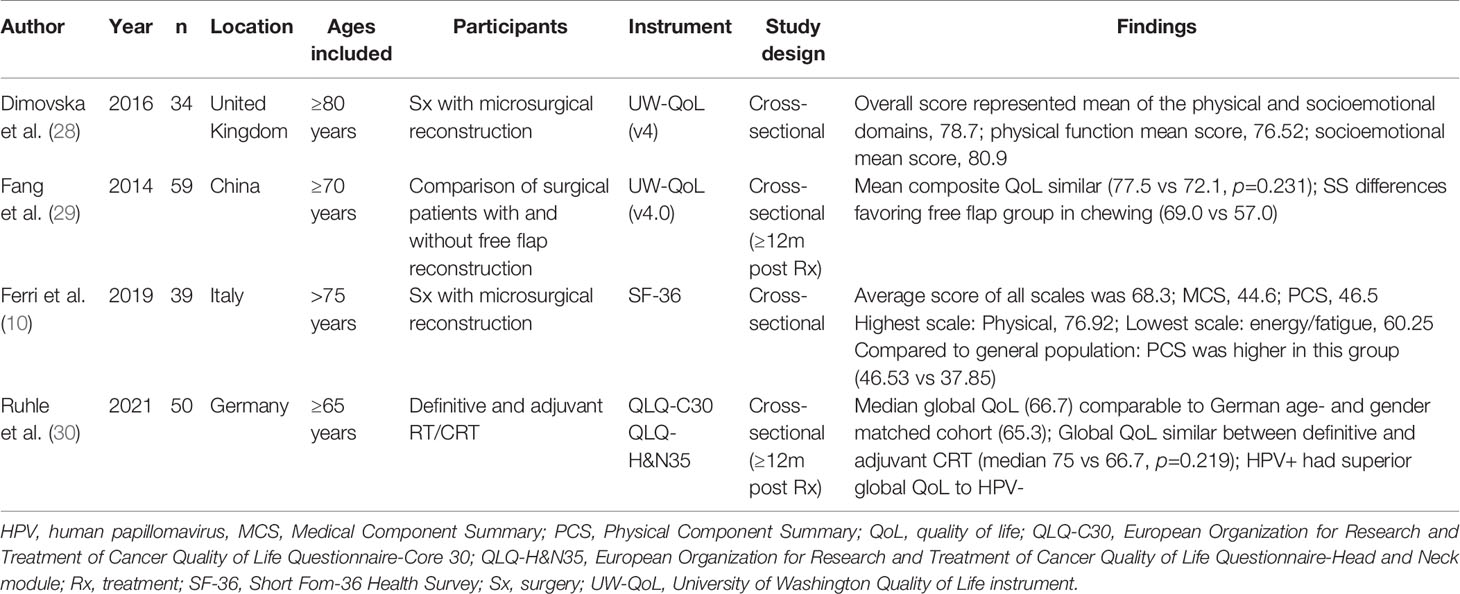
Table 4 Studies reporting health-related quality of life outcomes enrolling only elderly patients with HNSCC.
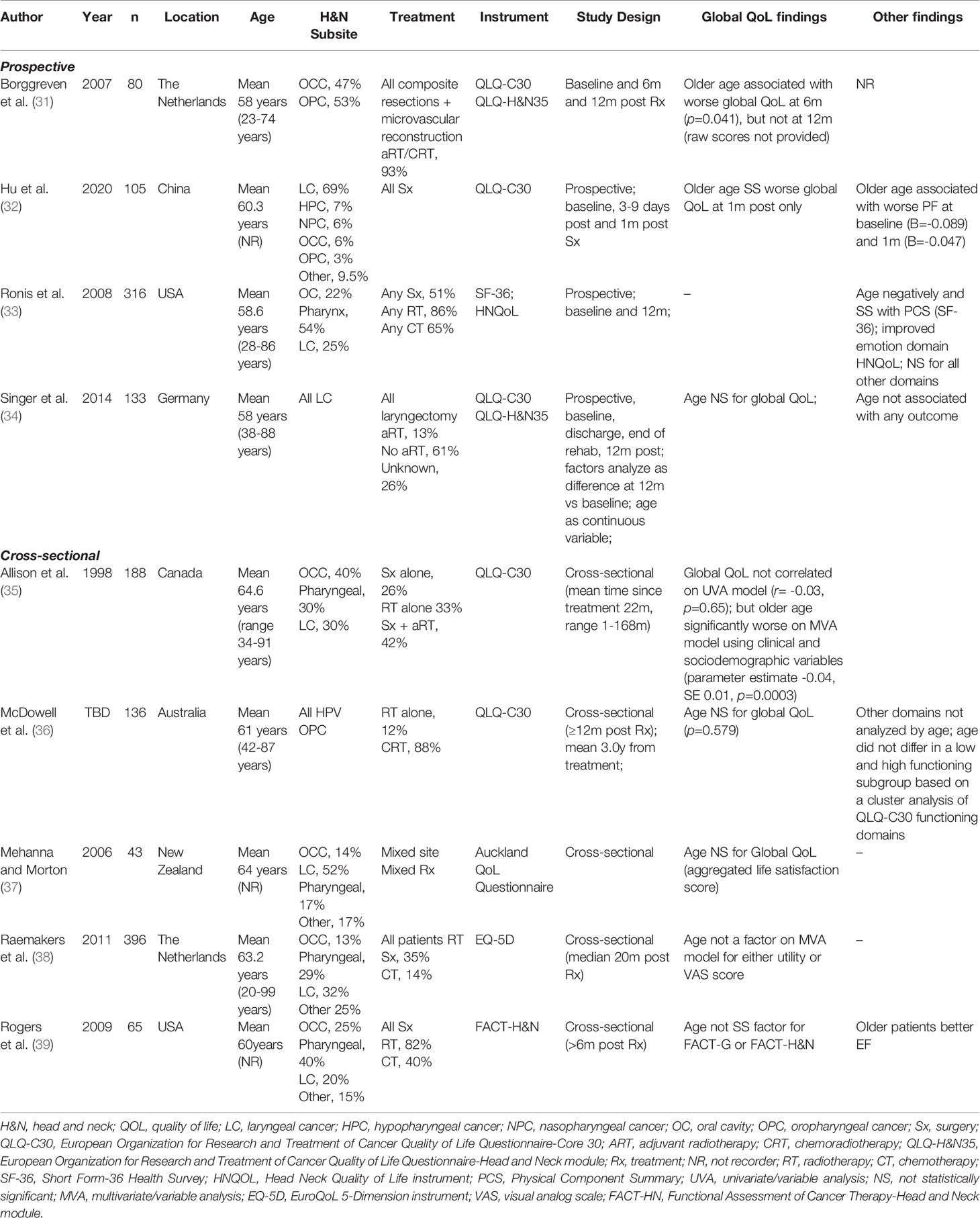
Table 5 Studies reporting age-related differences in health-related quality age in HNSCC (age analyzed as a continuous variable).
For this narrative report, we have focused and drawn attention to studies which have measured HRQL outcomes longitudinally with pretreatment assessments as their baseline, as of the numerous available studies, they are best placed to assess and report treatment-related differences across the age continuum. We have also drawn specific attention to those studies demonstrating significant age-based differences in HRQL, whether these differences have favored either the older or younger patients. However, it should be noted that these studies have also varied in study design from small underpowered studies to studies with very large numbers of patients while also using a variety of approaches to model age, including different age-based thresholds, hampering direct comparison. There is also variation in the instruments used and their assessment times. While the European Organization for Research and Treatment of Cancer (EORTC) modules, discussed below, have been the most frequently used measures in these studies, other instruments have been used, and cross-study comparisons are difficult given differences in their content, response options and the time frame with which individual instruments ask patients to consider how they have performed for a given item (i.e., “during the last week” or “during the past 4 weeks”). These are important differences to consider when comparing studies.
Health-Related Quality of Life Instruments
A variety of instruments are available to assess HRQL in HNC populations (Table 6). These include: (1) generic measures, which may also be used in non-cancer populations, such as the Short Form Health Surveys (SF-36, SF-12) (41, 42) or the EuroQoL modules (40); (2) generic cancer measures, such as the EORTC quality of life core questionnaire (QLQ-C30) (43) and the FACT-General (FACT-G) instrument (45); (3) head and neck cancer-specific instruments including the University of Washington Quality of Life Questionnaire (UW-QOL) (53), the EORTC Quality of Life Questionnaire Head and Neck Module (EORTC-QLQ-H&N35/43) (47, 48), and the Functional Assessment of Cancer Therapy Head and Neck (FACT-H&N), which includes the FACT-G and an additional HNC concerns module (49). Many of these HRQL tools are recommended and available for use in elderly HNC patients, but development and validation studies have not always included sufficient numbers of elderly patients (54). Many authors have recognized this problem, and while steps have been taken to develop psychometrically sound tools to measure HRQL in elderly cancer patients, such as the QLQ-ELD14/15 module developed by the EORTC (19, 55), often these tools do not address cancer-specific challenges faced by older HNC patients. For instance, HNC patients were not represented in the development phase of the QLQ-ELD14 (55). Thus, in selecting instruments for any given study investigating HRQL in elderly HNC patients, choices will largely depend on the clinical context and no single instrument is likely to assess all issues relevant to elderly HNC patients.
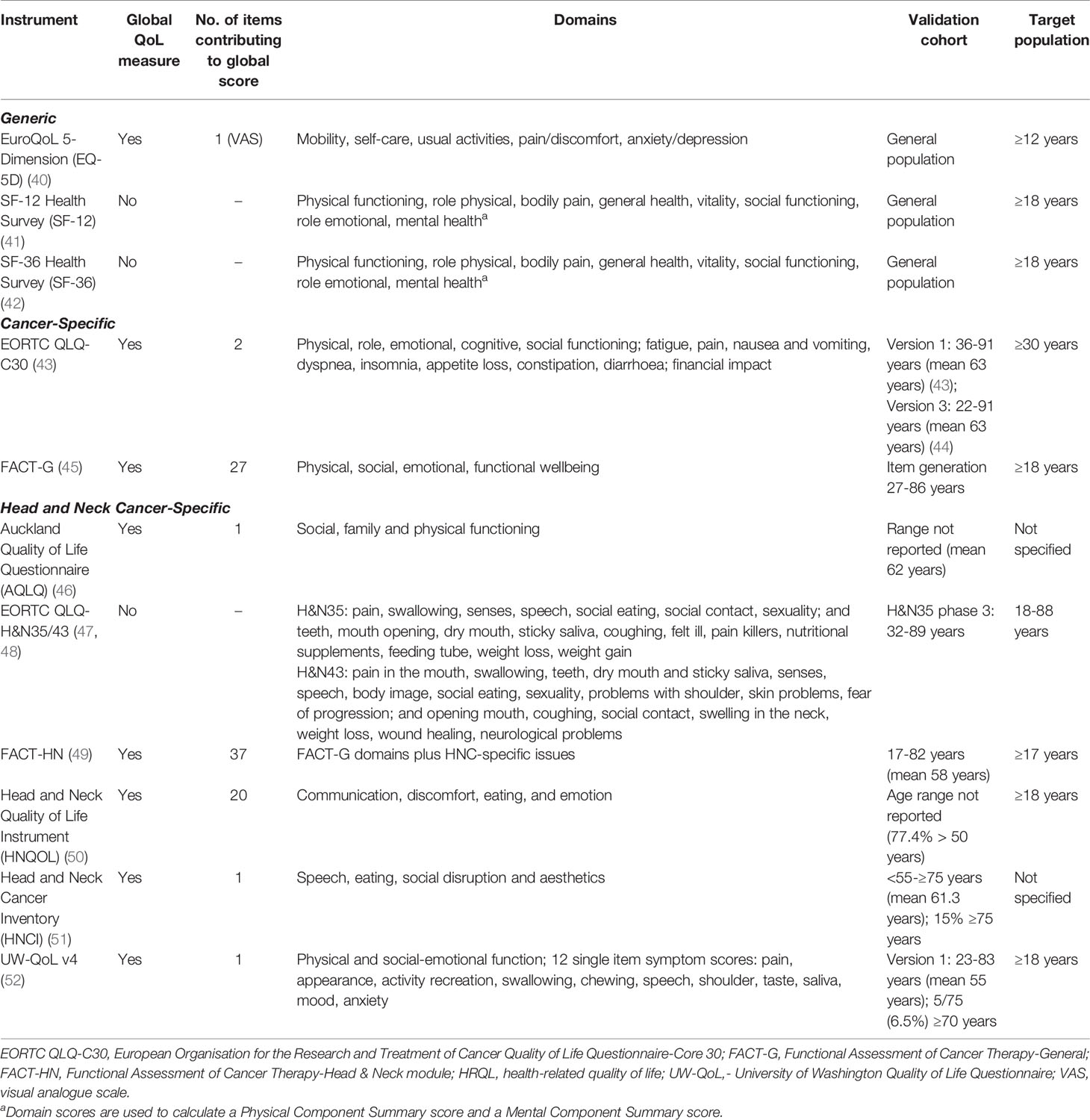
Table 6 Health-related quality of life instruments often used in HNC studies.
Global Quality of Life
Despite their limitations (56, 57), global measures of HRQL (referred to hereafter as global QoL) provide a straightforward means of assessing the overall impact of cancer and its treatment (56–59). Most prospective studies including measures of global QoL have found no significant differences between younger and older HNC patients (Table 2) (63, 64, 66–80) or have found significantly better self-reported global QoL in older patients (60–62). Findings from cross-sectional studies are similar (Table 3).
Berg et al. recently investigated longitudinal HRQL trajectories in 311 Swedish HNC patients. The sample included patients with various tumor sites, stages of disease and treatment; 37% had surgery and 85% received RT or CRT, either as definitive (63%) or adjuvant (22%) treatment (60). HRQL measures (EORTC QLQ-C30, QLQ-H&N35, QLQ-ELD14) were completed at diagnosis, then at three, six and 12 months from the commencement of treatment. The authors undertook two sets of analyses to compare younger and older patients. The first compared younger and older patients (<70 vs ≥ 70 years), the second compared younger and oldest patients (<80 vs ≥80 years). Despite similar global QoL at baseline, older patients reported better global QoL (<70 vs ≥70 years: 52 vs 61, p=0.006) three months after treatment, a difference of borderline clinical significance (96, 97); the oldest group (<80 vs ≥80 years: 54 vs 67, p=0.024) also fared better on global QoL at three months. Differences at three months were no longer evident at subsequent follow-ups. Citak et al. reported a prospective study of 54 Turkish patients, all of whom underwent radiotherapy (adjuvant treatment in 69%) (61). HRQL was captured with the EORTC QLQ-C30 and QLQ-H&N35 at baseline, at the end of RT, and one and three months after treatment. Global QoL was better in the older cohort (<60 vs ≥60 years: 53 vs 41, p=0.021) at the end of RT. While clinically relevant (96, 97), score differences at baseline were not described, so these results should be interpreted with caution.
Conversely, in a study reporting HRQL in elderly Japanese patients with oral cancer, Aoki et al. reported lower global QoL in older patients six months after treatment (62). In this study, 172 patients (≥75 years, n=43) completed the FACT-H&N at baseline, at treatment completion and one, three- and six-months post-treatment. While differences were small at the earlier time points, older patients reported worse global QoL scores at six months post-treatment (graphical interpretation, 106 vs 97, p=0.009), which falls into the range of a clinically meaningful difference (98). Interestingly, younger patients showed continued improvement from completion of treatment, whereas older patients plateaued at 1-month post-treatment.
Other Health-Related Quality of Life Outcomes
While considerable attention has been given to global QoL outcomes, other HRQL outcomes are highly relevant to older HNC patients and worth exploring in more detail. As with global QoL, most prospective studies fail to demonstrate consistent age-related differences in other self-reported HRQL outcomes (73–80), with some differences attributable to normal aging, irrespective of whether the patient has cancer.
In a prospective study of HNC patients from Sweden and Norway, Hammerlid et al. reported worse baseline (at the time of diagnosis) scores for older patients (≥75 years) on multiple scales/items of the QLQ-C30 and H&N35; however, these differences were only clinically relevant (≥10) for physical functioning, constipation, dyspnea and coughing. Older patients, however, reported better emotional functioning (99). At the 12-month follow-up, older patients (≥65 years) reported better role (difference = 11) and emotional functioning (difference = 10) but more significant problems with sexuality (difference = 18) and sticky saliva (difference = 15) than younger patients (69). Further, older patients reported less significant changes from baseline in role functioning and dryness of mouth. Nonetheless, changes from baseline in the senses (16 vs 10), sexuality (17 vs 4) and nutritional supplements (10 vs 5) were more severe.
In the previously mentioned Swedish study by Berg et al., the authors reported similar or better scores in the older cohorts with the exception of physical functioning, which was uniformly better in younger patients across the study. One exception was at the 3-month assessment. Here, differences in physical functioning were neither clinically nor statistically significant. This is largely explained by more significant declines in younger patients between baseline and 3 months. With further follow-up and recovery, however, the younger group regained its initial advantage. Older patients also reported less appetite loss and financial difficulties at various time points in this study (60). Notably, the oldest patients (≥80 years) reported worse fatigue, role functioning, and feeling ill at 12 months compared to those under 80 years. The Turkish study, which reported better global QoL at the end of RT, also found that older patients fared better with regards to senses problems and reported less weight loss, but scores were similar in other domains (61). Aoki et al., on the other hand, reported significantly worse social wellbeing and more HNC concerns in older patients (>75 years) at 6 months, as assessed by the FACT-H&N. Again, this appeared to be explained by younger patients showing better and ongoing recovery with further follow-up compared to the older patients.
Longitudinal HRQL outcomes for 785 HNC patients were collected in a North Carolina study using the FACT-H&N, with questionnaires administered to newly diagnosed HNC patients who were then assessed again at two subsequent follow-ups (median 22- and 42-months post-treatment, respectively) (70). Like most prospective studies reviewed, this series contained patients with various HNC subsites and disease stages, and they were treated with any combination of surgery (57%) and/or radiation (77%), with many also receiving concurrent chemotherapy (41%). A linear mixed model incorporating time since follow-up was used on each of the wellbeing domains, but not the total score. Age was divided into four categories, <50 years (19%), 50-64 years (49%), 65-74 years (25%) and ≥75 years (7%). Older patients generally fared better, with superior scores across the physical, emotional and functional wellbeing domains and the HNC additional concerns subscale. No significant differences were observed on the social wellbeing domain.
Physical functioning has also been reported as worse in older patients in other series, sometimes as an isolated finding among all available items/scales/domains (63), or in conjunction with limited other differences (76). While many of these studies suggest that older patients are not more adversely affected, some studies, such as that by Van Der Schroeff et al. have shown worse outcomes (72). In this longitudinal study, 118 older (≥70 years) and 148 younger (45-60 years) patients were followed for three to six years. The QoL component of the study was limited to those who completed all HRQL questionnaires (n=24 and n=33 patients, respectively). Again, the study sample was quite heterogenous in terms of tumor site, disease stage and treatment received. In the QoL cohort, about half the patients had oral cavity cancers. Patients were enrolled at diagnosis and there were no differences in the baseline EORTC QLQ-C30 and H&N35 scores. A more significant decline in physical functioning was seen in the older patients by 12 months post-treatment and this difference persisted at follow-up (i.e. three to six years post-treatment). The older patients also tended to report worse HNC symptoms, including statistically and clinically significant worse social eating (43 vs 23), swallowing (32 v 19) and speech (30 vs 19) at 12 months. Score differences on the swallowing and speech measures remained statistically significantly and clinically worse in the older patients with longer follow-up.
Laryngectomy Patients
Singer et al. conducted a prospective study of patients undergoing laryngectomy in eight German centers (34). HRQL data was collected at prior to undergoing a laryngectomy, just before hospital discharge, during inpatient rehabilitation, and 12 months later (EORTC QLQ-C30 and QLQ-H&N35). In this study, 101/175 (58%) patients were aged <60 years, 51/174 (29%) were aged 60-69 years, and 22/174 (13%) were ≥70 years. A multivariable regression analysis was undertaken to explore variations in HRQL changes from baseline to 12 months. While several outcomes, such as physical, role and social functioning, and some of the symptom items from both the QLQ-C30 and H&N35 were significantly worse one year after laryngectomy, age (analyzed as a continuous variable) was not a significant ‘predictor of scale/item scores’. On the other hand, Woodard et al. conducted a cross-sectional study in laryngectomy survivors using the Head and Neck Cancer Inventory (HNCI). Analysis of HNCI scores was limited to 33/58 survivors at median follow-up of 37 months post laryngectomy. The study included patients who had received primary surgical treatment and those who had received salvage surgery, however, the final patient contributions to the HRQL data was not reported. Younger patients (<65 years, 15/33) fared far worse across all the functional and attitude domains, as well as the global QoL score (54 vs 75). Those patients needing a laryngectomy as a component of their cancer treatment represent a distinct survivorship cohort amongst HNC patients, one resulting in many HRQL challenges, including loss of communication, body image changes and, potentially, loss of functional employment. While all patients will no doubt struggle with the physical and psychological impacts of a laryngectomy, younger patients in the prime of their adult lives may be especially vulnerable to the consequence of this life changing event.
Comparison to Age- and Gender-Matched Populations
Several studies have contrasted the outcomes of elderly patients to age- and gender-matched cohorts to differentiate HRQL changes attributable to treatment vulnerability and those that may be expected as a consequence of aging alone. Ferri et al. reported the outcomes of patients aged >75 years who had undergone HNC surgery with microsurgical reconstruction. This multi-site cross-sectional study used the SF-36 to assess HRQL two years after surgery. Of the eligible patients, 76/115 had died, leaving 39/115 enrollees with an average age of 81 years at the time of surgery. Most patients had also received adjuvant treatment (26/39, 67%). While the Mental Component Summary scores were similar to an age-matched Italian cohort, the average Physical Component Summary scores for the treated cohort indicated better physical health (46.5 vs 37.9) compared to the age-matched population. In a series of 50 older patients (>65 at time of treatment) who were at least one year from curative-intent radiotherapy (definitive or adjuvant), Ruhle et al. contrasted cross-sectional HRQL outcomes to an age-matched German sample (30). Using the EORTC QLQ-C30, patients reported very similar global QoL to the matched group. However, social functioning (85 vs 71), appetite loss (8 vs 19) and constipation (7 vs 20) were worse in the treated group; conversely, pain scores were lower (22 vs 33).
In a larger study also from Germany, 817 patients were enrolled to a cross-sectional study which compared HRQL, emotional distress and fatigue in HNC patients to a gender- and aged-matched population (<65 years, n=476; and ≥65 years, n=341) (100). The study sample included all HNC subtypes and a mix of primary and adjuvant treatment. Younger treated patients were more adversely affected (larger negative impacts) compared to their age- and gender-matched peers across all measured outcomes. Even so, older patients (≥65 years) did report worse HRQL compared to their matched peers. Global QoL (EORTC QLQ-C30) was worse for both the older males (65 vs 54) and females (63 vs 54). Older patients also reported worse fatigue (males 45 vs 24, females 48 vs 25) compared to the non-cancer patients.
Psychosocial Distress
The term “distress”, in the context of cancer, was chosen by the NCCN because it is felt to be less stigmatizing than descriptors like “psychiatric” and “psychosocial” concerns. It is defined by the NCCN as “a multifactorial, unpleasant, emotional experience of a psychological (cognitive, behavioral, emotional), social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment (101)”. It encompasses both normal feelings such as vulnerability, sadness, and fears, as well as problems that can significantly impact a patient’s life such as depression, anxiety, panic, social isolation, and personal crisis (101).
This report has focused on multiple types of distress, including the more commonly appreciated forms anxiety, depression and suicidality, but also other measures including fear of cancer recurrence, post-traumatic stress disorder, coping strategies and body image distress. This section will also discuss what is known about pain, fatigue, and sleep in older patients with HNC. Where possible, this review has focused on longitudinal, prospective studies, but this was not always possible for some of the less frequently studied outcomes, and where cross-sectional studies have provided novel or additional information, they have been included. The variation in instrument selection in these reports is considerable, and as for the HRQL section, cross-comparison is limited by significant variations in their content and application.
Instruments Measuring Psychosocial Distress in HNC
Tools commonly used to measure distress in HNC research are listed in Table 7. While most HRQL measures include mental health and/or wellbeing scales, this section will focus on tools specifically designed to assess anxiety, depression and/or distress. These include: (1) generic measures which may also be used in a non-cancer population, such as the Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), Beck Depression Inventory (BDI), and Patient Health Questionnaire 9 (PHQ-9); (2) generic cancer measures, such as the Distress Thermometer (DT), Mini-Mental Adjustment to Cancer (Mini-MAC), and Distress Inventory for Cancer (DIC2); and (3) head and neck cancer specific instruments, such as the Patient Concerns Inventory (PCI). Additionally, there are tools for assessing other factors that directly impact patient distress levels, such as coping style, fear of cancer recurrence, fatigue and sleep, social support, pain, and body image. These will be discussed in their respective sections.
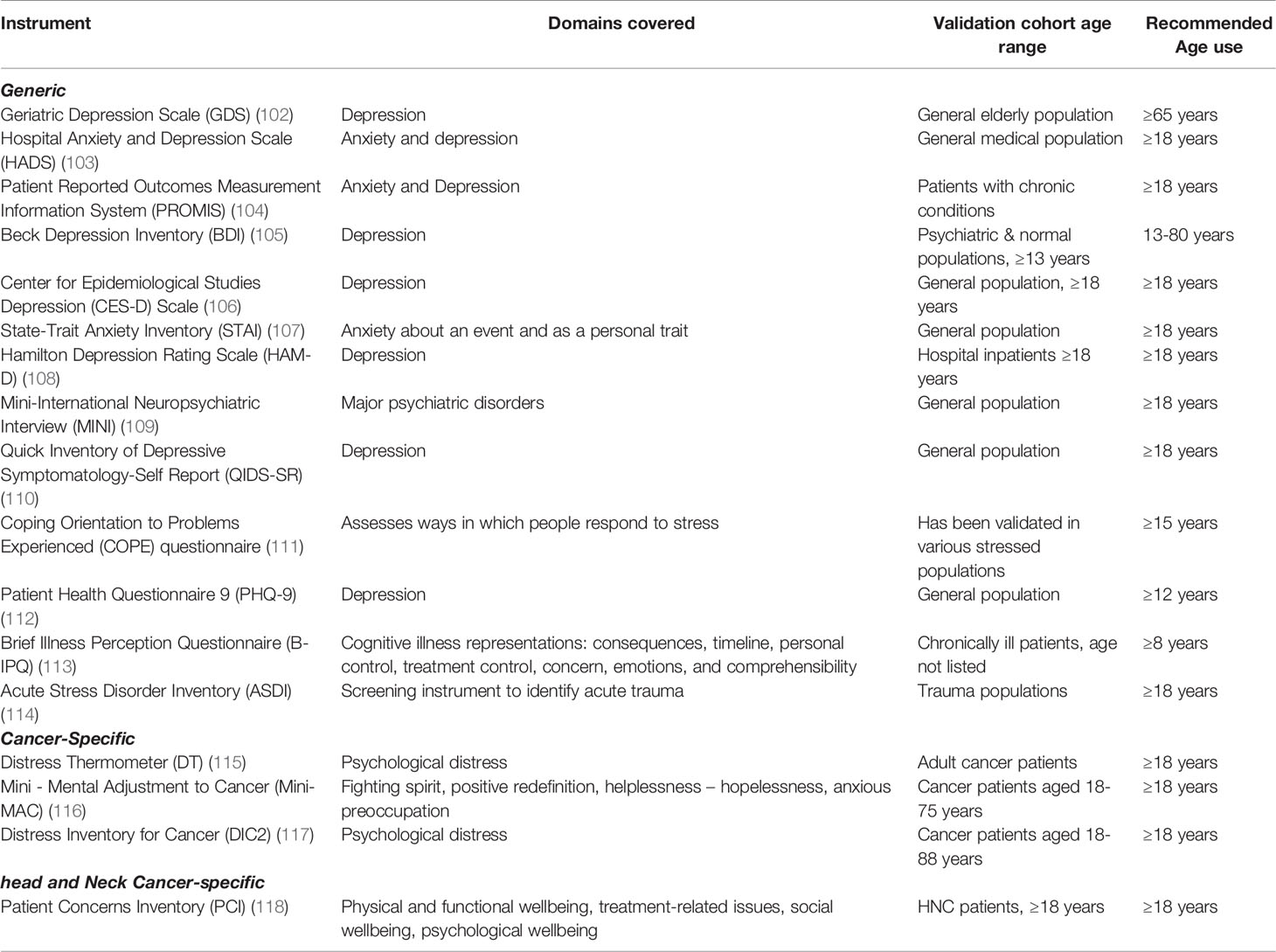
Table 7 Common Instruments used to capture distress in HNC studies.
Anxiety and Depression
Patients receiving HNC therapy self-report high levels of psychological distress, depression, and anxiety (119). Despite this awareness, psychological issues often remain unidentified or unassessed, albeit with significant effects on quality of life, functional status, and survival (8). Social isolation and lack of support have been linked to higher cancer mortality rates and poorer treatment tolerance (120). This is especially concerning in an older patient population because many elderly patients live alone (121). Literature on interventions to improve QOL and mood in patients with HNSCC have been summarized elsewhere (122).
Many studies have explored the relationship between age, and anxiety and depression in HNC patients. Due to the sheer volume of published studies, this paper will focus on results from prospective longitudinal studies (Table 8); results from cross-sectional studies are largely compatible. The overwhelming majority of prospective studies indicate that older HNC patients experience either similar rates of anxiety and depression (72, 74, 141–156), or less of one or both (123–138), than do their younger counterparts. Results from very few studies indicate worse distress among older HNC patients (139, 140).
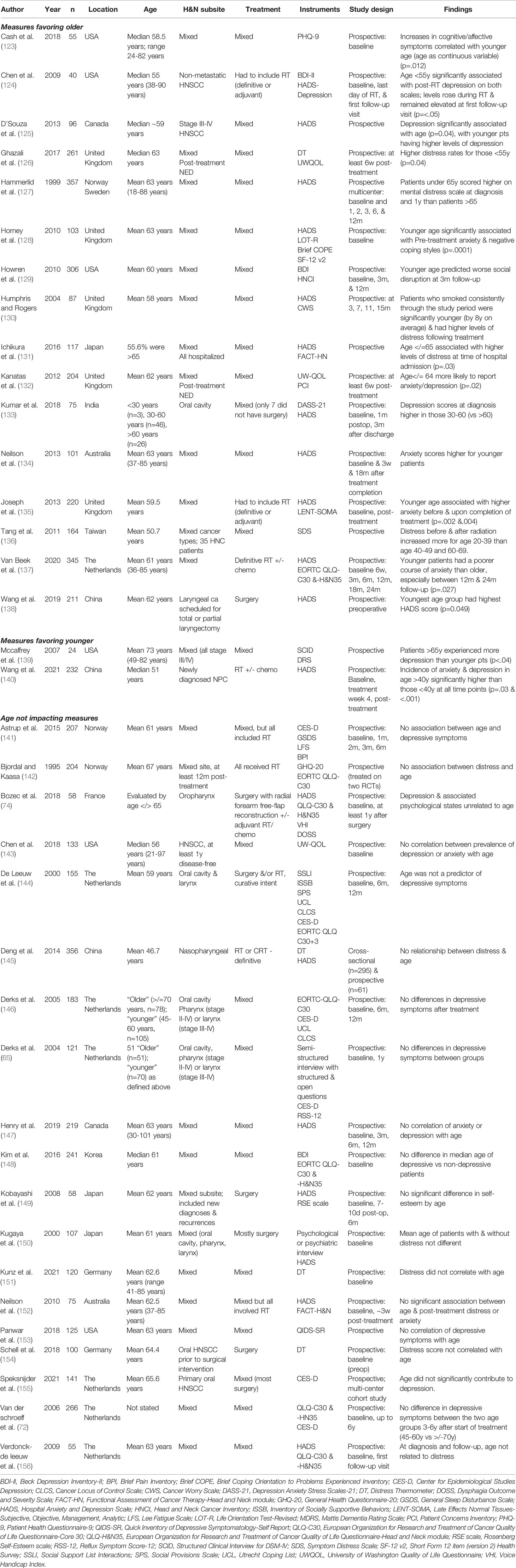
Table 8 Prospective studies reporting distress and age in elderly patients with HNSCC.
The largest prospective study to investigate the relationship between distress and age was reported by Hammerlid et al. in 1999 (127). The HADS was used to provide a measure of distress at baseline (after diagnosis but prior to initiating treatment) and one, two, three, six and 12 months after initiation of treatment in a mixed group of 357 HNC patients receiving various therapies. On average, patients <65 years reported higher levels of distress at diagnosis and at the one year follow up than did older patients. Another large prospective study evaluated a mixed group of 306 HNC patients from the US at their initial clinic appointment, and three- and twelve-months post-diagnosis, using the BDI and the Head and Neck Cancer Inventory. Younger age was associated with worse social disruption at three months (129). Prospective studies showing an association between distress and younger patient age have been reported from investigators in the UK, Japan, India, Australia, Taiwan, China, and the Netherlands (131, 133, 134, 136–138). In several studies, younger age is specifically linked to higher rates of anxiety, especially before and during treatment, which some speculate is due to increased fear of recurrence (126, 134, 135, 137).
There are only two prospective studies wherein older patients fared worse with regards to distress, and it is notable that the larger of the two reported on only nasopharyngeal cancer patients in China, with a median age of 51 years. In this study, rates of anxiety and depression in patients over the age of 40 was significantly higher than in those under 40 years at all timepoints; however, the interquartile range was 40-57, and this study is not representative of a broad elderly HNC population. The other prospective study reporting lower distress in younger patients is a very small study from the US reporting on preoperative distress in locally advanced HNC patients. Patients over 65 years were found to experience more depression than younger patients. This study did not utilize commonly utilized instruments and is far too small to draw any useful conclusions (139).
In summary, the preponderance of prospective evidence from a wide range of countries and across most head and neck disease sites and treatments suggests that elderly patients actually fare better with regards to distress as compared to their younger counterparts and that the reasoning for this is likely nuanced. Factors may include mid-life responsibilities more characteristic of younger patients, such as employment, childcare, greater perceived importance of social life, and less earned resilience. As discussed in the following sections, fear of cancer recurrence, pain, fatigue, sleep, body image issues, and post-traumatic stress may also be higher in younger patients. While most of these studies consist of self-reports based on screening tools rather than diagnostic interviews, which is a limitation, the results align with those from the general population; namely, that older people typically report lower levels of distress and anxiety than do younger people (157).
Fear of Cancer Recurrence
Fear of cancer recurrence (FCR) is a common concern reported by cancer survivors, including patients treated for HNC (Table 9). There are a number of methods used to gather information about FCR. FCR severity may be measured using standardized tools like the Fear of Cancer Recurrence Inventory (169, 170) or the Fear of Recurrence questionnaire (166). Concerns about FCR may also be gathered as part of various patient concerns inventories. Irrespective of the method used to gather information on FCR, older cancer survivors report lower levels/rates of FCR on average than younger patients (171). This observation has also been seen in HNC studies where variations in FCR have been analyzed by age (Table 9), with the majority showing an increased vulnerability to FCR in younger patients (158–164).
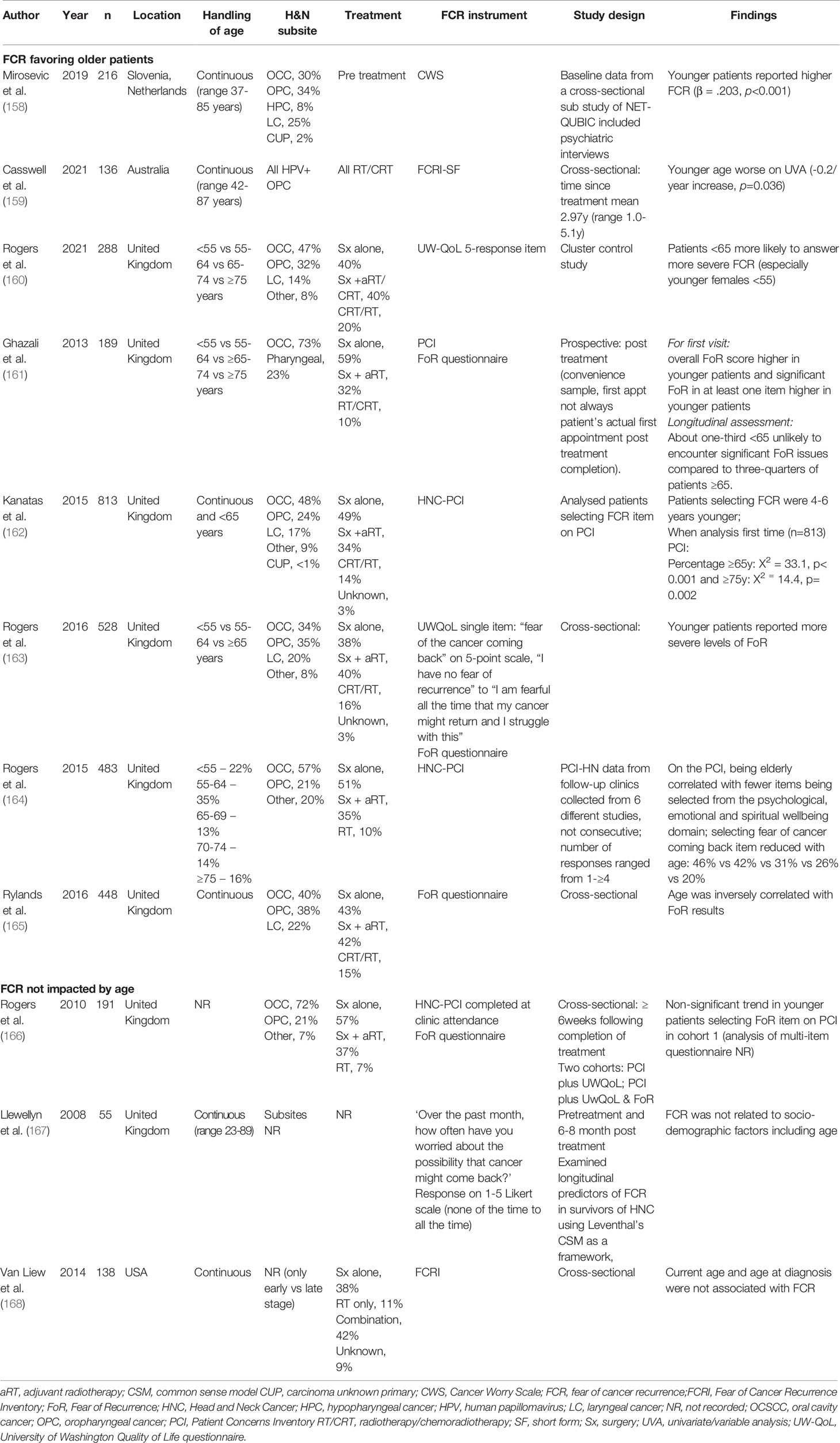
Table 9 Head and neck cancer studies reporting variations in fear of cancer recurrence measures by age.
Concerns about cancer recurrence (perhaps fear of progression) may begin early on the cancer journey, and age-related differences may be observed even before treatment has commenced. Mirosevic et al. reported FCR outcomes in 216 newly diagnosed HNC patients using the 8-item Cancer Worry Scale (158). FCR scores were higher in younger patients, and age, along with baseline HADS anxiety scores were the strongest predictors of baseline FCR. As shown in Table 9, many studies have included substantial proportions of patients treated for oral cavity cancer with surgery alone. Irrespective of study design, younger patients appear more vulnerable, with the oldest patients (≥75 years) reporting low or lower rates of FCR (162, 164). In a cross-sectional cohort of 136 patients with HPV-associated oropharyngeal cancer treated with definitive (chemo)radiotherapy Casswell et al. measured FCR using the FCRI-short form (which assesses the severity domain of the larger FCRI version). In this study, age was analyzed as a continuous variable, and it is interesting to note that even with this favorable HNC cohort harboring a typically low risk of recurrence (given most had had a complete response to treatment and the mean time since treatment completion was 3 years) that older patients continued to report lower rates of FCR.
Body Image Distress in Older Patients With HNSCC
Body image studies in HNC have mostly been undertaken in samples of patients undergoing major surgery for their cancer, as detailed in Table 10. In summary, evidence of an association between age and body image distress is weak but limited cross-sectional and retrospective data suggest similar or less severe body image distress in older HNC patients (172–175). Further high-quality research is needed in this area.
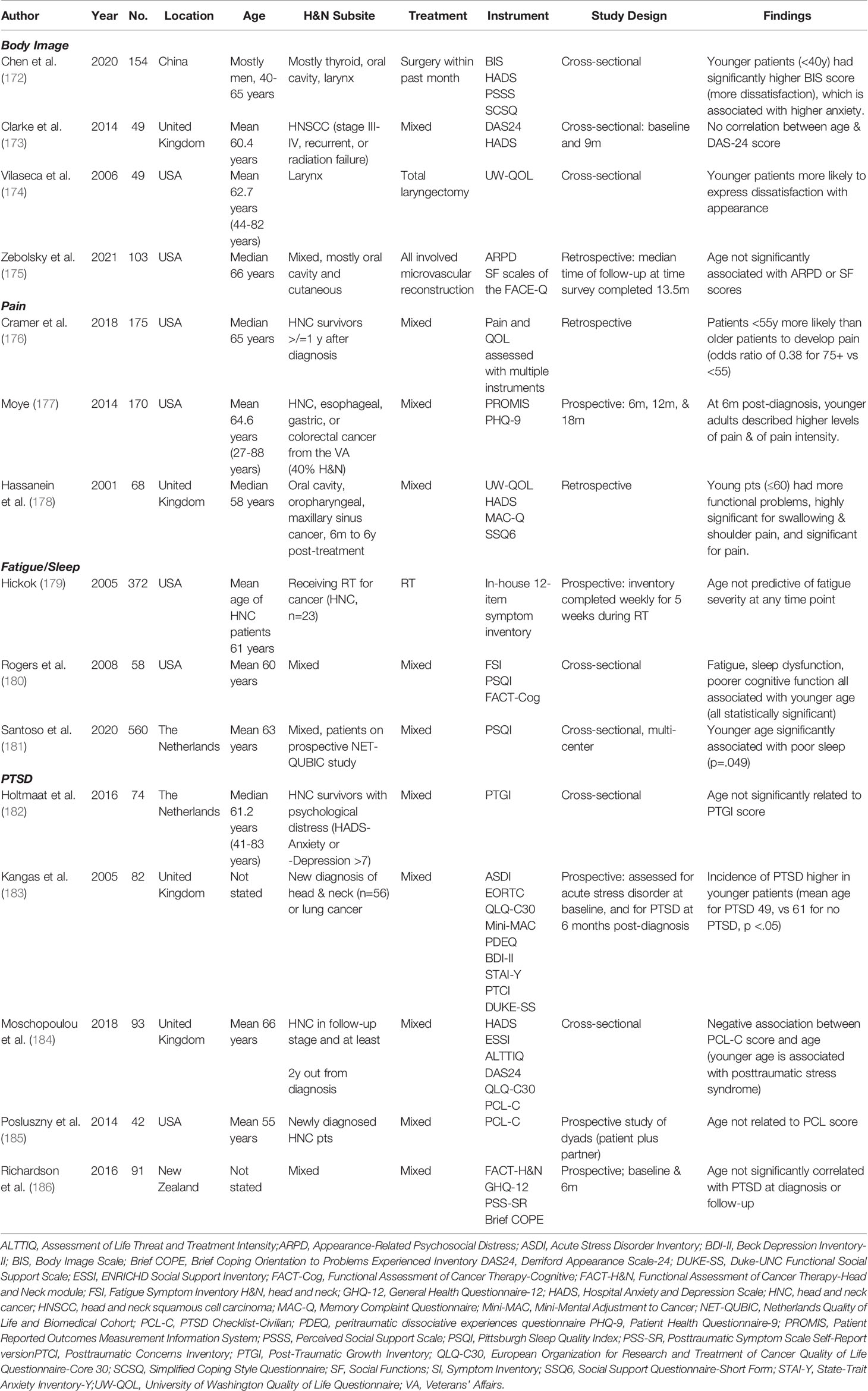
Table 10 Studies reporting on body image, pain, fatigue/sleep, and post-traumatic stress.
Fatigue and Sleep in Older Patients With HNSCC
There is a paucity of data on sleep quality in HNC patients; however, insight into sleep quality would likely help healthcare providers better support their patients. Sleep disturbance and fatigue have been shown to contribute significantly to depressive symptoms, and sleep is unique as it is an often treatable risk factor (141). Tools used to assess sleep and fatigue in HNC patients include the Pittsburgh Sleep Quality Inventory (PSQI), Fatigue Symptom Inventory, Lee Fatigue Scale, and General Sleep Disturbance Scale (GSDS).
Table 10 outlines studies reporting on fatigue and sleep in head and neck cancer patients. Hickok et al. prospectively administered a one-page symptom inventory to 372 patients weekly for five weeks during radiotherapy. Of note, this included patients with all types of cancer and only 23 had HNC. Mean age of the HNC patients was 61 years, and age was not predictive of fatigue severity at any time in this study (179). Other studies are cross-sectional in design but have the advantage of being limited to head and neck cancer and, like most of the other domains reviewed, they appear to show an association between younger age and poor sleep quality and fatigue (180, 181). As with body image distress, more high-quality research would be helpful in investigating this relationship further.
Pain in Older Patients With HNSCC
Pain is experienced as one of the most impactful sources of distress in cancer survivors and has been linked to poorer outcomes and decreased QoL (177). Most of the literature on pain and HNC indicates that younger patients experience higher levels of pain than older patients. Relevant studies are reported in Table 10. In summary, one prospective trial conducted using the PROMIS scale in a Veterans Administration Hospital population showed that at six months post-diagnosis, younger adults (64 years and younger) described significantly higher levels of pain and of pain intensity as compared to older adults (≥65). It is notable that this was a mixed population of cancer patients, with 40% having HNC (177).
Two retrospective papers show similar trends, with younger patients experiencing more pain. Interesting findings from these studies include that the incidence of pain among survivors was as high as 45.1% at a median of 6.3 years since treatment completion, and that pain was the third-most important issue identified by survivors, after swallowing and saliva. Additionally, patients with pain were significantly more likely to report issues with anxiey and mood (176). The findings also suggest that younger patinets may have more functional problems, including dysphagia and shoulder function (178).
This is an interesting observation with many possible confounders, and future research efforts may look to focus on understanding this association and strategies to help support younger patients affected by HNC.
Post-Traumatic Stress in Elderly HNC Patients
As with other factors influencing distress, the literature evaluating the relationship between PTSD and age in HNC patients is mixed, with some showing no difference in rates, and some showing higher incidence in younger patients (Table 10). There have been two similarly powered prospective studies, with contradictory findings regarding an asssociation between PTSD and age (183, 186). Cross-sectional studies, as well as one small prospective study of patient-partner dyads, have shown mixed results (182, 184, 185). In summary, the literature suggests either no association between age and PTSD, or a trend toward higher rates in younger patients.
Differences in Coping Styles
Coping refers to the ways in which people respond to and behave during stressful events, and it is likely to influence how one evaluates his or her quality of life (146). Research suggests older people adapt better to cancer because serious illness is more common and expected with increasing age and their experience of physical decline may be less dramatic. Younger people also often have more stage of life-related stressors like child-rearing and employment (146).
Pre- and post-treatment depression and anxiety have been linked to ineffective coping styles such as helplessness/hopelessness, fatalism, and avoidant coping (128). Some authors have noted that although depression and anxiety are more easily measured than coping styles, patient coping strategies may be more amenable to intervention (128). Notably, coping styles seem to vary quite predictably with age in samples of HNC patients (Table 11).
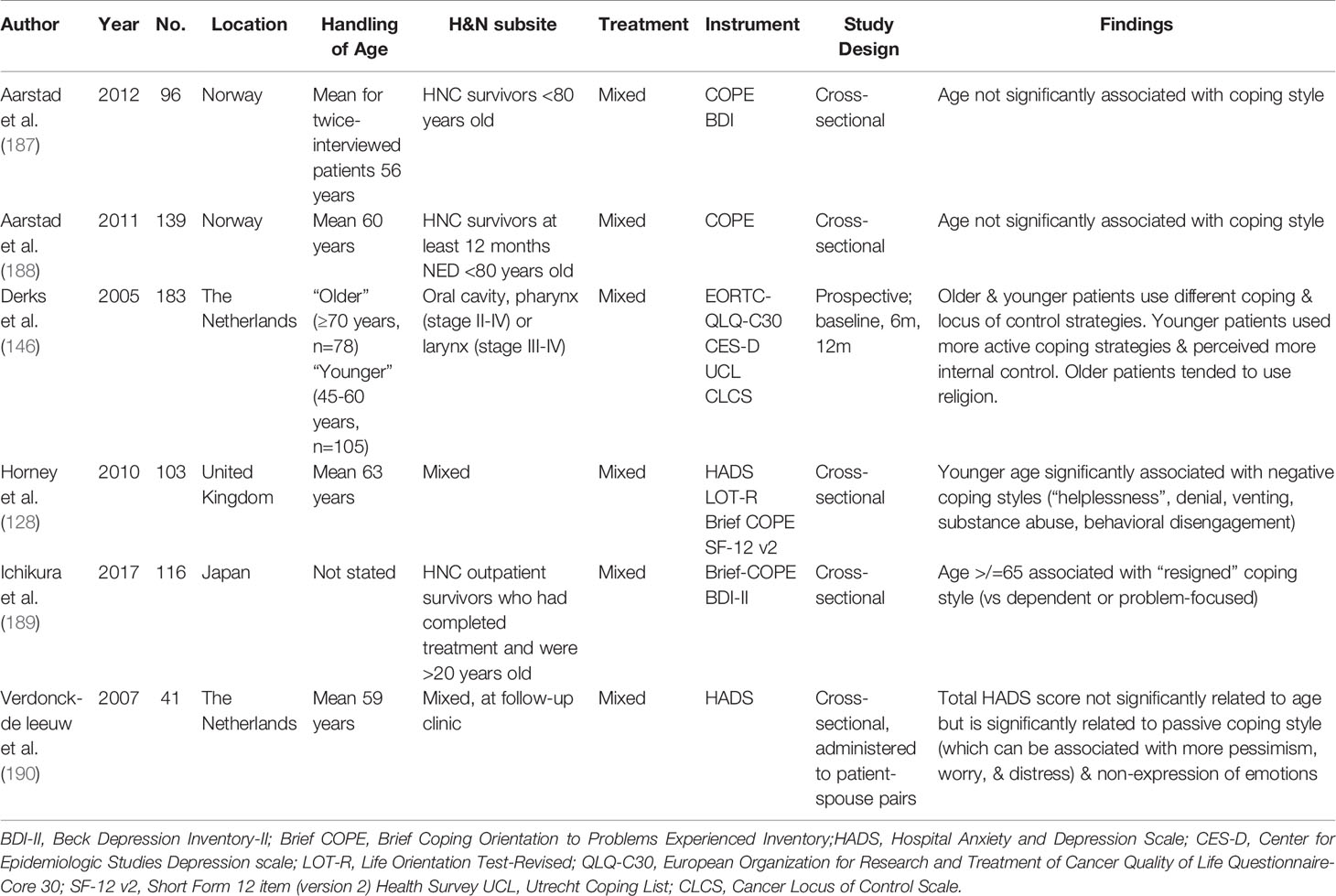
Table 11 Studies reporting on coping styles.
One prospective study showed that older and younger patients use different coping and locus of control strategies, with younger patients using more active coping strategies and perceiving more internal control, and older patients tending to use religion. These differences in coping styles did not significantly impact QoL or depressive symptoms, but avoidant coping style was associated with worse depressive symptoms and QoL regardless of age group (146).
One retrospective study showed that younger age is significantly associated pretreatment anxiety and with negative coping styles such as helplessness, denial, venting, substance abuse, and behavioral disengagement (128). Another showed that older patients tended to use a “resigned” coping style (versus dependent or problem-focused). The dependent-coping pattern, which includes smoking, drinking, seeking support and engaging self-distraction, was found to be the most common style and was also the most likely to be associated with depression (189).
There are other studies, in contrast, that have shown no association between age and coping style, most notably, the Norweigan studies by Aarstad et al. (187, 188). Again, this area would benefit from further exploration.
Suicidality in Older Patients With HNSCC
At the extreme end of unrecognized or poorly managed psychosocial distress are self-inflicted injuries including suicide. Patients with any cancer diagnosis have been reported to have higher risks of suicide (191–193) or non-fatal self-injury (NFSI) compared to the general population, and patients with HNC may harbour even higher rates compared to most other types of cancer (191, 193–196). Other factors such as increasing age, social supports and a history of mental health have also been associated with an increased suicide risk (197).
Zaorsky et al. compared rates of suicide outcomes in cancer patients via the US-based SEER database from 1973 to 2014 (191). Compared to the general population, the relative risk of suicide was highest for those patients diagnosed with head and neck, lung, and testicular cancer, as well as Hodgkin lymphoma. The standardized mortality ratio (SMR) for HNC patients was highest in the first year after diagnosis and decreased with time from the initial diagnosis. Across the entire cancer cohort, elderly, white men with localized cancer who were not married were at highest risk. In a SEER study focusing primarily on patients with HNC (including thyroid), Kam et al. reported an adjusted (age, sex, race) suicide rate of 37.9 per 100 000 person-years, corresponding to a SMR of 3.21 (95% CI 2.18-4.23). Across all HNC subsites, older patients (60-79 years and >80 years) had the highest SMR. All of the HNC subsites, except for thyroid, had a higher risk of suicide than the general population, with those patients diagnosed with hypopharynx having the highest risk (SMR 13.91, 95% CI, 11.78-16.03). There was a decline in SMR over time for most of the subsites, though for all but thyroid and nasal cavity/sinuses, the risk exceeded that of the general population, while those with NPC had a persistently elevated and high risk even 15 to 30 years after their diagnosis.
In a Korean study, Choi et al. reported higher suicide risk amongst cancer patients older than 60 years of age compared to sampled population data (includes ~10% of the entire population (193). Similar to the Zaorsky et al. study, the risk of suicide was highest in the first year after any cancer diagnosis, accounting for 34.9% of all cases (median time to suicide was 1.74 years). For those patients diagnosed with a HNC, the adjusted hazard ratio was 2.28 (95% CI 1.47-3.54) which was amongst the highest risk for any cancer type.
Unmet Needs in Elderly Patients With HNSCC
Although various unmet needs tools are available for use in cancer populations, their content and structure is highly variable. Individual items and needs domains covered may range from physical and psychological needs to informational needs. Needs domains may also include, but are not limited to, nutritional, dental, financial, and sexual needs. Shunmugasundaram et al. recently conducted a systematic review comparing the content of self-reported unmet needs instruments in head and neck cancer populations, concluding that the PCI was the most comprehensive of the available tools, covering all twelve specified needs included in the conceptual framework of unmet needs developed by the research team (198). This is perhaps not surprising given it was the only unmet needs instrument which was developed specifically in a head and neck cancer population and has undergone continual refinement since its initial development. Studies of HNC patients including unmet needs tools are summarized in Table 12.
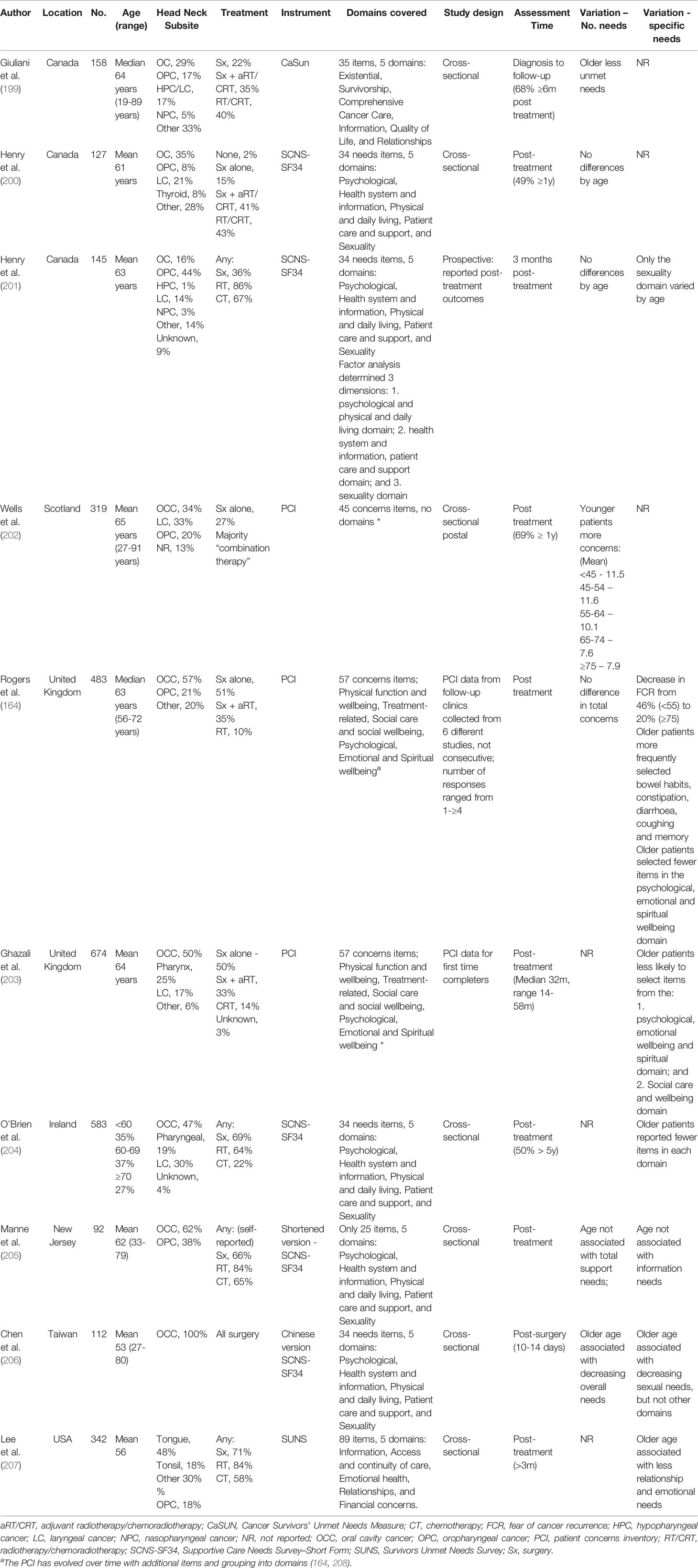
Table 12 Studies reporting variations in unmet needs by age in HNC patients.
Almost all of these studies focused on patients who had emerged from the acute post-treatment period with exception of the Canadian study by Giuliani et al. which included patients from diagnosis through to survivorship and that by Chen which evaluated patients shortly after they had undergone surgery (206). The survivors included in many of these studies are quite heterogenous, as has been seen in many of the QoL and psychosocial distress reports with only the study by Chen et al. focusing on patients with oral cavity cancer (206). Despite variability in the instruments used, the available evidence suggests that older patients report fewer unmet needs than younger patients. In those studies which report a summed overall assessment of unmet needs, most have shown a lower burden in older patients (199, 202, 206) or no age-related differences at all (164, 200, 201, 205). For individual domains, older patients generally report less unmet needs, including in the sexuality domain (201, 206), or domains assessing psychological/emotional or spiritual needs (164, 203, 204, 207).
Novel Approaches
Biological Age
Recently, Xiao et al. reported associations between epigenetic age acceleration (EAA), survival and HRQL in HNC patients (22). EAA )describes discordance between the chronological age of an individual and their “epigenetic age”; EAA’s can be both positive, where the epigenetic age is greater than the patients’ chronological age, or more simply where aging has been accelerated, and negative where the reverse is seen, indicating a slower aging process. In this sample, they identified clinical variables associated with increased EAA, which was associated with worse survival outcomes. However, they also analyzed longitudinal variations in the FACT-H&N. Using a multivariable generalized estimating equation, and controlling for covariates, patients with a negative EAA had higher FACT-H&N total score over, indicating better QoL, than those with a positive EAA. The estimated score difference was 10.6 points (p<0.001), which is in excess of a commonly cited MCID (98). These are intriguing results, but how best to utilize these measures in clinical practice and how to incorporate them into complex treatment decision-making pathways and counselling will require additional research.
Comprehensive Geriatric Assessment
Across the oncology landscape, interest is increasing in the use of comprehensive geriatric assessments (CGAs) to aid clinical decision making in older individuals with cancer. The CGA has been defined as “a multidimensional, interdisciplinary diagnostic process focusing on determining an older person’s medical, psychosocial, and functional capabilities to develop a coordinated and integrated plan for treatment and long-term follow-up” (209, 210). The International Society of Geriatric Oncology have recommended a core set of domains to assess in a CGA, including functional status, fatigue, medical comorbidities, cognitive capacity and underlying mental health issues, social status and the anticipated degree of social support, nutritional status and the presence of any geriatric syndromes, which is a term encompassing many issues of the elderly including falls, delirium and dementia, osteoporosis and polypharmacy, amongst others (210). In HNC populations, the CGA may be more adept at uncovering impairments beyond that of the multi-disciplinary team; it has also been associated with the length of post-operative inpatient stays and the rates of surgical complications and successful completion of radiotherapy (211–214). Deficits in some of the CGA domains may predict more significant declines in global QoL (215) or other HRQL domains (214) after treatment in HNC patients. The implementation and use of CGA in routine clinical practice is, however, resource intensive and while a comprehensive assessment of every older patient being considered for curative-intent HNC treatment would no doubt lead to many opportunities for pre-treatment optimization, how best to incorporate a CGA into routine practice would need considerable resource and multi-disciplinary investment at a local or institutional level.
Limitations
This narrative review provides an overview of findings from studies investigating health and wellbeing outcomes and unmet needs in older and elderly patients with HNC and HNSCC and contrasts them to outcomes reported in younger HNC patients. Of the available studies, there are several limitations hampering the ability to draw firm conclusions. Most notably the data is hindered by a lack of consensus in defining the threshold for an older HNC patient. These studies which largely included patients treated with radical treatment also represent the outcomes for a biased population of robust older patients and their outcomes are likely not generalizable to all older patients with HNC, particularly those who may be more frail. It is also worth considering that these studies did not include detailed information about the treatments received, and whether older patients may have undergone reduced intensity treatment to accommodate their age, such as alterations in surgical fields, radiation volumes or chemotherapy dosing. The available studies also vary widely in the different PROs used, the methodologies used in their application and the statistical methods with which they have been analyzed and interpreted. Future studies and high-quality research will hopefully add to our understanding and avoid some of the aforementioned limitations. Well-defined secondary analyses from prospective phase II or III studies where older patients are included would be a welcome addition to the literature. In this review, where possible we have focused on those studies including only HNSCC, however, this was not always possible particularly with the lesser-studied psychosocial distress outcomes. However, despite their histological similarities, HNSCC encompasses a diverse range of tumors, including tumors with different etiology (HPV or smoking-related), primary sites and treatment, factors which may all impart different HRQL and psychosocial challenges for individual HNC patients. Interpretation outcomes from the various studies included in this review was frequently hampered by a reliance on statistical inferences rather than focusing on differences that would be clinically relevant, a theme which echoes throughout most of the PRO literature. Future studies of age-related changes would benefit from taking into account what is already known about changes over the life course in the general population. This would further our understanding of cancer- and treatment-related issues in younger and older patients. Future research exploring variations in age-related outcomes in HNC populations will need to focus on these challenges to draw more meaningful conclusions for our patients.
Conclusions and Future Directions
While there are many limitations to the available data this review should be reassuring when considering intensive treatment in the older HNC and HNSCC population. In synthesizing the varied health and wellbeing outcomes included in this report, when undergoing curative intent protocols, older patients have tended to demonstrate more resilience in HRQL and psychosocial outcomes when compared to their younger counterparts, with the caveat the older patients included in most of these studies were considered robust enough to treat with radical treatment. While refining optimal survivorship models will remain across the continuum of patients presenting with HNC, these findings suggests that we should be in fact more aware of the support that younger HNC patients may need across multiple HRQL and psychosocial distress domains following HNC treatment, despite their perceived physical robustness. Future research efforts in reporting age-related variations in HRQL, psychosocial distress and unmet needs will need to work towards harmonizing the definition of the older HNC patient, narrow the research question in more homogenous HNC populations and investigate novel approaches to measure biological rather than chronological age.
Author Contributions
LM and CH designed the concept of the submitted manuscript, were responsible for data acquisition and wrote the first draft. All authors (LM, CH, KG, and DR) were involved in the interpretation of the data included and in drafting and revising the first draft. All authors have provided approval for publication of the included content.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
3. Hanasoge S, Magliocca KR, Switchenko JM, Saba NF, Wadsworth JT, El-Deiry MW, et al. Clinical Outcomes in Elderly Patients With Human Papillomavirus-Positive Squamous Cell Carcinoma of the Oropharynx Treated With Definitive Chemoradiation Therapy. Head Neck (2016) 38(6):846–51. doi: 10.1002/hed.24073
4. Szturz P, Vermorken JB. Treatment of Elderly Patients With Squamous Cell Carcinoma of the Head and Neck. Front Oncol (2016) 6:199. doi: 10.3389/fonc.2016.00199
5. Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of Cancer Incidence in the United States: Burdens Upon an Aging, Changing Nation. J Clin Oncol (2009) 27(17):2758–65. doi: 10.1200/JCO.2008.20.8983
6. Roman BR, Aragones A. Epidemiology and Incidence of HPV-Related Cancers of the Head and Neck. J Surg Oncol (2021) 124(6):920–2. doi: 10.1002/jso.26687
7. Tota JE, Best AF, Zumsteg ZS, Gillison ML, Rosenberg PS, Chaturvedi AK. Evolution of the Oropharynx Cancer Epidemic in the United States: Moderation of Increasing Incidence in Younger Individuals and Shift in the Burden to Older Individuals. J Clin Oncol (2019) 37(18):1538–46. doi: 10.1200/JCO.19.00370
8. Soto-Perez-de-Celis E, Li D, Yuan Y, Lau YM, Hurria A. Functional Versus Chronological Age: Geriatric Assessments to Guide Decision Making in Older Patients With Cancer. Lancet Oncol (2018) 19(6):e305–16. doi: 10.1016/S1470-2045(18)30348-6
9. Ørum M, Gregersen M, Jensen K, Meldgaard P, Damsgaard EMS. Frailty Status But Not Age Predicts Complications in Elderly Cancer Patients: A Follow-Up Study. Acta Oncol (2018) 57(11):1458–66. doi: 10.1080/0284186X.2018.1489144
10. Ferri A, Segna E, Varazzani A, Copelli C, Valsecchi S, Dell'Aversana Orabona G, et al. Free Flap Head and Neck Reconstruction in the Elderly: What is the Impact on Quality of Life? Acta Otorhinolaryngol Ital (2019) 39(3):145–9. doi: 10.14639/0392-100X-2149
11. Horsley PJ, Perera L, Veness MJ, Stevens MJ, Eade TN, Back M, et al. Outcomes for Elderly Patients 75 Years and Older Treated With Curative Intent Radiotherapy for Mucosal Squamous Cell Carcinomas of the Head and Neck. Head Neck (2020) 42(1):25–32. doi: 10.1002/hed.25969
12. Ward MC, Reddy CA, Adelstein DJ, Koyfman SA. Use of Systemic Therapy With Definitive Radiotherapy for Elderly Patients With Head and Neck Cancer: A National Cancer Data Base Analysis. Cancer (2016) 122(22):3472–83. doi: 10.1002/cncr.30214
13. Szturz P, Bossi P, Vermorken JB. Systemic Treatment in Elderly Head and Neck Cancer Patients: Recommendations for Clinical Practice. Curr Opin Otolaryngol Head Neck Surg (2019) 27(2):142–50. doi: 10.1097/MOO.0000000000000526
14. Amini A, Jones BL, McDermott JD, Serracino HS, Jimeno A, Raben D, et al. Survival Outcomes With Concurrent Chemoradiation for Elderly Patients With Locally Advanced Head and Neck Cancer According to the National Cancer Data Base. Cancer (2016) 122(10):1533–43. doi: 10.1002/cncr.29956
15. Santana-Davila R. Head and Neck Cancer in Elderly Patients: What to Do When Data Are Limited? J Oncol Pract (2018) 14(9):549–50. doi: 10.1200/JOP.18.00480
16. World Health Organisation. Ageing (2021). Available at: https://www.who.int/health-topics/ageing.
17. Wikipedia. Retirement Age (2021). Available at: https://en.wikipedia.org/wiki/Retirement_age.
18. Balducci L. Management of Cancer in the Elderly. Oncol (Williston Park) (2006) 20(2):135–43; discussion 44, 46, 51-2.
19. Wheelwright S, Darlington AS, Fitzsimmons D, Fayers P, Arraras JI, Bonnetain F, et al. International Validation of the EORTC QLQ-ELD14 Questionnaire for Assessment of Health-Related Quality of Life Elderly Patients With Cancer. Br J Cancer (2013) 109(4):852–8. doi: 10.1038/bjc.2013.407
20. Pignon JP, le Maitre A, Maillard E, Bourhis J, Group M-NC. Meta-Analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): An Update on 93 Randomised Trials and 17,346 Patients. Radiother Oncol J Eur Soc Ther Radiol Oncol (2009) 92(1):4–14. doi: 10.1016/j.radonc.2009.04.014
21. Xiao C, Beitler JJ, Peng G, Levine ME, Conneely KN, Zhao H, et al. Epigenetic Age Acceleration, Fatigue, and Inflammation in Patients Undergoing Radiation Therapy for Head and Neck Cancer: A Longitudinal Study. Cancer (2021) 127(18):3361–71. doi: 10.1002/cncr.33641
22. Xiao C, Miller AH, Peng G, Levine ME, Conneely KN, Zhao H, et al. Association of Epigenetic Age Acceleration With Risk Factors, Survival, and Quality of Life in Patients With Head and Neck Cancer. Int J Radiat Oncol Biol Phys (2021) 111(1):157–67. doi: 10.1016/j.ijrobp.2021.04.002
23. List MA, Rutherford JL, Stracks J, Pauloski BR, Logemann JA, Lundy D, et al. Prioritizing Treatment Outcomes: Head and Neck Cancer Patients Versus Nonpatients. Head Neck (2004) 26(2):163–70. doi: 10.1002/hed.10367
24. List MA, Stracks J, Colangelo L, Butler P, Ganzenko N, Lundy D, et al. How Do Head and Neck Cancer Patients Prioritize Treatment Outcomes Before Initiating Treatment? J Clin Oncol (2000) 18(4):877–84. doi: 10.1200/JCO.2000.18.4.877
25. Windon MJ, D'Souza G, Faraji F, Troy T, Koch WM, Gourin CG, et al. Priorities, Concerns, and Regret Among Patients With Head and Neck Cancer. Cancer (2019) 125(8):1281–9. doi: 10.1002/cncr.31920
26. Brotherston DC, Poon I, Le T, Leung M, Kiss A, Ringash J, et al. Patient Preferences for Oropharyngeal Cancer Treatment De-Escalation. Head Neck (2013) 35(2):151–9. doi: 10.1002/hed.22930
27. Otto RA, Dobie RA, Lawrence V, Sakai C. Impact of a Laryngectomy on Quality of Life: Perspective of the Patient Versus That of the Health Care Provider. Ann Otol Rhinol Laryngol (1997) 106(8):693–9. doi: 10.1177/000348949710600815
28. Dimovska EO, Clibbon JJ, Moncrieff MD, Heaton MJ, Figus A. Microsurgical Reconstructions for Head and Neck Cancers in Elderly Aged >80 Years: An Analysis of Surgical Outcomes and Quality of Life. Ann Surg Oncol (2016) 23(5):1684–92. doi: 10.1245/s10434-015-5049-3
29. Fang QG, Shi S, Li M, Zhang X, Liu FY, Sun CF. Free Flap Reconstruction Versus non-Free Flap Reconstruction in Treating Elderly Patients With Advanced Oral Cancer. J Oral Maxillofac Surg Off J Am Assoc Oral Maxillofacial Surgeons (2014) 72(7):1420–4. doi: 10.1016/j.joms.2014.01.010
30. Rühle A, Haehl E, Kalckreuth T, Stoian R, Spohn SKB, Sprave T, et al. Surviving Elderly Patients With Head-And-Neck Squamous Cell Carcinoma-What Is the Long-Term Quality of Life After Curative Radiotherapy? Cancers (Basel) (2021) 13(6):1275. doi: 10.3390/cancers13061275
31. Borggreven PA, Aaronson NK, Verdonck-de Leeuw IM, Muller MJ, Heiligers ML, Bree R, et al. Quality of Life After Surgical Treatment for Oral and Oropharyngeal Cancer: A Prospective Longitudinal Assessment of Patients Reconstructed by a Microvascular Flap. Oral Oncol (2007) 43(10):1034–42. doi: 10.1016/j.oraloncology.2006.11.017
32. Hu ZY, Feng XQ, Fu MR, Yu R, Zhao HL. Symptom Patterns, Physical Function and Quality of Life Among Head and Neck Cancer Patients Prior to and After Surgical Treatment: A Prospective Study. Eur J Oncol Nurs (2020) 46:101770. doi: 10.1016/j.ejon.2020.101770
33. Ronis DL, Duffy SA, Fowler KE, Khan MJ, Terrell JE. Changes in Quality of Life Over 1 Year in Patients With Head and Neck Cancer. Arch Otolaryngol Head Neck Surg (2008) 134(3):241–8. doi: 10.1001/archoto.2007.43
34. Singer S, Danker H, Guntinas-Lichius O, Oeken J, Pabst F, Schock J, et al. Quality of Life Before and After Total Laryngectomy: Results of a Multicenter Prospective Cohort Study. Head Neck (2014) 36(3):359–68. doi: 10.1002/hed.23305
35. Allison PJ, Locker D, Wood-Dauphinee S, Black M, Feine JS. Correlates of Health-Related Quality of Life in Upper Aerodigestive Tract Cancer Patients. Qual Life Res (1998) 7(8):713–22. doi: 10.1023/A:1008880816543
36. McDowell L, Casswell G, Bressel M, Drosdowsky A, Rischin D, Coleman A, et al. Symptom Burden, Quality of Life, Functioning and Emotional Distress in Survivors of Human Papillomavirus Associated Oropharyngeal Cancer: An Australian Cohort. Oral Oncol (2021) 122:105560. doi: 10.1016/j.oraloncology.2021.105560
37. Mehanna HM, Morton RP. Deterioration in Quality-of-Life of Late (10-Year) Survivors of Head and Neck Cancer. Clin Otolaryngol (2006) 31(3):204–11. doi: 10.1111/j.1749-4486.2006.01188.x
38. Ramaekers BL, Joore MA, Grutters JP, van den Ende P, Jong J, Houben R, et al. The Impact of Late Treatment-Toxicity on Generic Health-Related Quality of Life in Head and Neck Cancer Patients After Radiotherapy. Oral Oncol (2011) 47(8):768–74. doi: 10.1016/j.oraloncology.2011.05.012
39. Rogers LQ, Rao K, Malone J, Kandula P, Ronen O, Markwell SJ, et al. Factors Associated With Quality of Life in Outpatients With Head and Neck Cancer 6 Months After Diagnosis. Head Neck (2009) 31(9):1207–14. doi: 10.1002/hed.21084
40. EuroQoL Group. EuroQol–a New Facility for the Measurement of Health-Related Quality of Life. Health Policy (1990) 16(3):199–208. doi: 10.1016/0168-8510(90)90421-9
41. Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med Care (1996) 34(3):220–33. doi: 10.1097/00005650-199603000-00003
42. Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 Health Survey Questionnaire: New Outcome Measure for Primary Care. Bmj (1992) 305(6846):160–4. doi: 10.1136/bmj.305.6846.160
43. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
44. Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, Curran D, et al. A 12 Country Field Study of the EORTC QLQ-C30 (Version 3.0) and the Head and Neck Cancer Specific Module (EORTC QLQ-H&N35) in Head and Neck Patients. Eur J Cancer (2000) 36(14):1796–807. doi: 10.1016/s0959-8049(00)00186-6
45. Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. The Functional Assessment of Cancer Therapy Scale: Development and Validation of the General Measure. J Clin Oncol (1993) 11(3):570–9. doi: 10.1200/JCO.1993.11.3.570
46. Morton RP, Witterick IJ. Rationale and Development of a Quality-of-Life Instrument for Head-and-Neck Cancer Patients. Am J Otolaryngol (1995) 16(5):284–93. doi: 10.1016/0196-0709(95)90055-1
47. Bjordal K, Hammerlid E, Ahlner-Elmqvist M, de Graeff A, Boysen M, Evensen JF, et al. Quality of Life in Head and Neck Cancer Patients: Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-H&N35. J Clin Oncol (1999) 17(3):1008–19. doi: 10.1200/JCO.1999.17.3.1008
48. Singer S, Amdal CD, Hammerlid E, Tomaszewska IM, Castro Silva J, Mehanna H, et al. International Validation of the Revised European Organisation for Research and Treatment of Cancer Head and Neck Cancer Module, the EORTC QLQ-HN43: Phase Iv. Head Neck (2019) 41(6):1725–37. doi: 10.1002/hed.25609
49. List MA, D'Antonio LL, Cella DF, Siston A, Mumby P, Haraf D, et al. The Performance Status Scale for Head and Neck Cancer Patients and the Functional Assessment of Cancer Therapy-Head and Neck Scale. A Study of Utility and Validity. Cancer (1996) 77(11):2294–301. doi: 10.1002/(SICI)1097-0142(19960601)77:11<2294::AID-CNCR17>3.0.CO;2-S
50. Terrell JE, Nanavati KA, Esclamado RM, Bishop JK, Bradford CR, Wolf GT. Head and Neck Cancer-Specific Quality of Life: Instrument Validation. Arch Otolaryngol Head Neck Surg (1997) 123(10):1125–32. doi: 10.1001/archotol.1997.01900100101014
51. Funk GF, Karnell LH, Christensen AJ, Moran PJ, Ricks J. Comprehensive Head and Neck Oncology Health Status Assessment. Head Neck (2003) 25(7):561–75. doi: 10.1002/hed.10245
52. Hassan SJ, Weymuller EA Jr. Assessment of Quality of Life in Head and Neck Cancer Patients. Head Neck (1993) 15(6):485–96. doi: 10.1002/hed.2880150603
53. Rogers SN, Gwanne S, Lowe D, Humphris G, Yueh B, Weymuller EA Jr. The Addition of Mood and Anxiety Domains to the University of Washington Quality of Life Scale. Head Neck (2002) 24(6):521–9. doi: 10.1002/hed.10106
54. Fitzsimmons D, Gilbert J, Howse F, Young T, Arrarras JI, Brédart A, et al. A Systematic Review of the Use and Validation of Health-Related Quality of Life Instruments in Older Cancer Patients. Eur J Cancer (2009) 45(1):19–32. doi: 10.1016/j.ejca.2008.07.036
55. Johnson C, Fitzsimmons D, Gilbert J, Arrarras JI, Hammerlid E, Bredart A, et al. Development of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Module for Older People With Cancer: The EORTC QLQ-Eld15. Eur J Cancer (2010) 46(12):2242–52. doi: 10.1016/j.ejca.2010.04.014
56. Amdur RJ, Chera BS. Misuse of Quality of Life Evaluation in Oncology Studies: Reification, Adaptation, and the U-Shaped Curve. Pract Radiat Oncol (2019) 9(4):191–2. doi: 10.1016/j.prro.2018.05.002
57. Ringash J. Re: Misuse of Quality of Life Evaluation in Oncology Studies. Pract Radiat Oncol (2019) 9(6):503. doi: 10.1016/j.prro.2019.07.016
58. McDowell L, Gough K, King M, Corry J, Rischin D. Patient-Reported Quality of Life and Symptom Burden Measures in Human Papillomavirus Associated Oropharyngeal Cancer - A Review of the Literature and PRO Methodology. Oral Oncol (2021) 118:105309. doi: 10.1016/j.oraloncology.2021.105309
59. Sprangers MA, Schwartz CE. Integrating Response Shift Into Health-Related Quality of Life Research: A Theoretical Model. Soc Sci Med (1982) (1999) 48(11):1507–15. doi: 10.1016/S0277-9536(99)00045-3
60. Berg M, Silander E, Bove M, Johansson L, Nyman J, Hammerlid E. The Effect of Age on Health-Related Quality of Life for Head and Neck Cancer Patients Up to 1 Year After Curative Treatment. J Geriatr Oncol (2022) 13(1):60–6. doi: 10.1016/j.jgo.2021.06.009
61. Citak E, Tulek Z. Longitudinal Quality of Life in Turkish Patients With Head and Neck Cancer Undergoing Radiotherapy. Support Care Cancer (2013) 21(8):2171–83. doi: 10.1007/s00520-013-1774-y
62. Aoki T, Ota Y, Sasaki M, Suzuki T, Uchibori M, Nakanishi Y, et al. Quality of Life of Japanese Elderly Oral Cancer Patients During the Perioperative Period. Int J Oral Maxillofac Surg (2021) 50(9):1138–46. doi: 10.1016/j.ijom.2020.12.011
63. de Graeff A, de Leeuw JR, Ros WJ, Hordijk GJ, Blijham GH, Winnubst JA. Long-Term Quality of Life of Patients With Head and Neck Cancer. Laryngoscope (2000) 110(1):98–106. doi: 10.1097/00005537-200001000-00018
64. de Graeff A, de Leeuw JR, Ros WJ, Hordijk GJ, Blijham GH, Winnubst JA. Pretreatment Factors Predicting Quality of Life After Treatment for Head and Neck Cancer. Head Neck (2000) 22(4):398–407. doi: 10.1002/1097-0347(200007)22:4<398::AID-HED14>3.0.CO;2-V
65. Derks W, De Leeuw R, Winnubst J, Hordijk GJ. Elderly Patients With Head and Neck Cancer: Physical, Social and Psychological Aspects After 1 Year. Acta Otolaryngol (2004) 124(4):509–14. doi: 10.1080/00016480310000656
66. Dziegielewski PT, Teknos TN, Durmus K, Old M, Agrawal A, Kakarala K, et al. Transoral Robotic Surgery for Oropharyngeal Cancer: Long-Term Quality of Life and Functional Outcomes. JAMA Otolaryngol– Head Neck Surg (2013) 139(11):1099–108. doi: 10.1001/jamaoto.2013.2747
67. Funk GF, Karnell LH, Christensen AJ. Long-Term Health-Related Quality of Life in Survivors of Head and Neck Cancer. Arch Otolaryngol Head Neck Surg (2012) 138(2):123–33. doi: 10.1001/archoto.2011.234
68. Hammerlid E, Silander E, Hörnestam L, Sullivan M. Health-Related Quality of Life Three Years After Diagnosis of Head and Neck Cancer - A Longitudinal Study. Head Neck (2001) 23(2):113–25. doi: 10.1002/1097-0347(200102)23:2<113::AID-HED1006>3.0.CO;2-W
69. Bjordal K, Ahlner-Elmqvist M, Hammerlid E, Boysen M, Evensen JF, Biorklund A, et al. A Prospective Study of Quality of Life in Head and Neck Cancer Patients. Part II: Longitudinal Data. Laryngoscope (2001) 111(8):1440–52. doi: 10.1097/00005537-200108000-00022
70. Reeve BB, Cai J, Zhang H, Weissler MC, Wisniewski K, Gross H, et al. Factors That Impact Health-Related Quality of Life Over Time for Individuals With Head and Neck Cancer. Laryngoscope (2016) 126(12):2718–25. doi: 10.1002/lary.26073
71. Rettig EM, D'Souza G, Thompson CB, Koch WM, Eisele DW, Fakhry C. Health-Related Quality of Life Before and After Head and Neck Squamous Cell Carcinoma: Analysis of the Surveillance, Epidemiology, and End Results-Medicare Health Outcomes Survey Linkage. Cancer (2016) 122(12):1861–70. doi: 10.1002/cncr.30005
72. van der Schroeff MP, Derks W, Hordijk GJ, de Leeuw RJ. The Effect of Age on Survival and Quality of Life in Elderly Head and Neck Cancer Patients: A Long-Term Prospective Study. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2007) 264(4):415–22. doi: 10.1007/s00405-006-0203-y
73. Bozec A, Poissonnet G, Chamorey E, Casanova C, Vallicioni J, Demard F, et al. Free-Flap Head and Neck Reconstruction and Quality of Life: A 2-Year Prospective Study. Laryngoscope (2008) 118(5):874–80. doi: 10.1097/MLG.0b013e3181644abd
74. Bozec A, Demez P, Gal J, Chamorey E, Louis MY, Blanchard D, et al. Long-Term Quality of Life and Psycho-Social Outcomes After Oropharyngeal Cancer Surgery and Radial Forearm Free-Flap Reconstruction: A GETTEC Prospective Multicentric Study. Surg Oncol (2018) 27(1):23–30. doi: 10.1016/j.suronc.2017.11.005
75. Bozec A, Schultz P, Gal J, Chamorey E, Chateau Y, Dassonville O, et al. Evolution and Predictive Factors of Quality of Life in Patients Undergoing Oncologic Surgery for Head and Neck Cancer: A Prospective Multicentric Study. Surg Oncol (2019) 28:236–42. doi: 10.1016/j.suronc.2019.01.012
76. Derks W, De Leeuw JR, Hordijk GJ, Winnubst JA. Elderly Patients With Head and Neck Cancer: Short-Term Effects of Surgical Treatment on Quality of Life. Clin Otolaryngol Allied Sci (2003) 28(5):399–405. doi: 10.1046/j.1365-2273.2003.00718.x
77. Durmus K, Patwa HS, Gokozan HN, Kucur C, Teknos TN, Agrawal A, et al. Functional and Quality-of-Life Outcomes of Transoral Robotic Surgery for Carcinoma of Unknown Primary. Laryngoscope (2014) 124(9):2089–95. doi: 10.1002/lary.24705
78. Segna E, Bolzoni AR, Giannì AB, Baj A, Beltramini GA. Impact of Reconstructive Microsurgery on Patients With Cancer of the Head and Neck: A Prospective Study of Quality of Life, Particularly in Older Patients. Br J Oral Maxillofac Surg (2018) 56(9):830–4. doi: 10.1016/j.bjoms.2018.09.003
79. Yin X, Shan C, Wang J, Zhang H. Factors Associated With the Quality of Life for Hospitalized Patients With HPV-Associated Oropharyngeal Squamous Cell Carcinoma. Oral Oncol (2020) 103:104590. doi: 10.1016/j.oraloncology.2020.104590
80. Yoshimura R, Shibuya H, Miura M, Watanabe H, Ayukawa F, Hayashi K, et al. Quality of Life of Oral Cancer Patients After Low-Dose-Rate Interstitial Brachytherapy. Int J Radiat Oncol Biol Phys (2009) 73(3):772–8. doi: 10.1016/j.ijrobp.2008.05.001
81. Alicikus ZA, Akman F, Ataman OU, Dag N, Orcin E, Bakis B, et al. Importance of Patient, Tumour and Treatment Related Factors on Quality of Life in Head and Neck Cancer Patients After Definitive Treatment. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2009) 266(9):1461–8. doi: 10.1007/s00405-008-0889-0
82. Baxi SS, Cullen G, Xiao H, Atoria CL, Sherman EJ, Ho A, et al. Long-Term Quality of Life in Older Patients With HPV-Related Oropharyngeal Cancer. Head Neck (2018) 40(11):2321–8. doi: 10.1002/hed.25159
83. Bonzanini LIL, Soldera EB, Ortigara GB, Schulz RE, Antoniazzi RP, Ardenghi TM, et al. Clinical and Sociodemographic Factors That Affect the Quality of Life of Survivors of Head and Neck Cancer. Support Care Cancer (2020) 28(4):1941–50. doi: 10.1007/s00520-019-05008-4
84. Bozec A, Majoufre C, De Boutray M, Gal J, Chamorey E, Roussel LM, et al. Oral and Oropharyngeal Cancer Surgery With Free-Flap Reconstruction in the Elderly: Factors Associated With Long-Term Quality of Life, Patient Needs and Concerns. A GETTEC cross-sectional study. Surg Oncol (2020) 35:81–8. doi: 10.1016/j.suronc.2020.08.014
85. Dwivedi RC, St Rose S, Chisholm EJ, Youssefi P, Hassan MS, Khan AS, et al. Evaluation of Factors Affecting Post-Treatment Quality of Life in Oral and Oropharyngeal Cancer Patients Primarily Treated With Curative Surgery: An Exploratory Study. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2012) 269(2):591–9. doi: 10.1007/s00405-011-1621-z
86. Infante-Cossio P, Torres-Carranza E, Cayuela A, Gutierrez-Perez JL, Gili-Miner M. Quality of Life in Patients With Oral and Oropharyngeal Cancer. Int J Oral Maxillofac Surg (2009) 38(3):250–5. doi: 10.1016/j.ijom.2008.12.001
87. Laraway DC, Lakshmiah R, Lowe D, Roe B, Rogers SN. Quality of Life in Older People With Oral Cancer. Br J Oral Maxillofac Surg (2012) 50(8):715–20. doi: 10.1016/j.bjoms.2012.01.010
88. Morimata J, Otomaru T, Murase M, Haraguchi M, Sumita Y, Taniguchi H. Investigation of Factor Affecting Health-Related Quality of Life in Head and Neck Cancer Patients. Gerodontology (2013) 30(3):194–200. doi: 10.1111/j.1741-2358.2012.00662.x
89. Pierre CS, Dassonville O, Chamorey E, Poissonnet G, Ettaiche M, Santini J, et al. Long-Term Quality of Life and its Predictive Factors After Oncologic Surgery and Microvascular Reconstruction in Patients With Oral or Oropharyngeal Cancer. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2014) 271(4):801–7. doi: 10.1007/s00405-013-2592-z
90. Pourel N, Peiffert D, Lartigau E, Desandes E, Luporsi E, Conroy T. Quality of Life in Long-Term Survivors of Oropharynx Carcinoma. Int J Radiat Oncol Biol Phys (2002) 54(3):742–51. doi: 10.1016/S0360-3016(02)02959-0
91. Silveira AP, Gonçalves J, Sequeira T, Ribeiro C, Lopes C, Monteiro E, et al. Geriatric Oncology: Comparing Health Related Quality of Life in Head and Neck Cancer Patients. Head Neck Oncol (2011) 3(1):3. doi: 10.1186/1758-3284-3-3
92. Verma N, Tan X, Knowles M, Bernard S, Chera B. Patient-Reported Outcomes for Dental Health, Shoulder-Neck Dysfunction, and Overall Quality of Life After Treatment With Radiation for Head and Neck Cancer. Laryngoscope Investig Otolaryngol (2019) 4(3):300–6. doi: 10.1002/lio2.262
93. Wells M, Swartzman S, Lang H, Cunningham M, Taylor L, Thomson J, et al. Predictors of Quality of Life in Head and Neck Cancer Survivors Up to 5 Years After End of Treatment: A Cross-Sectional Survey. Support Care Cancer (2016) 24(6):2463–72. doi: 10.1007/s00520-015-3045-6
94. Williamson JS, Ingrams D, Jones H. Quality of Life After Treatment of Laryngeal Carcinoma: A Single Centre Cross-Sectional Study. Ann R Coll Surg Engl (2011) 93(8):591–5. doi: 10.1308/147870811X13137608455253
95. Woodard TD, Oplatek A, Petruzzelli GJ. Life After Total Laryngectomy: A Measure of Long-Term Survival, Function, and Quality of Life. Arch Otolaryngol Head Neck Surg (2007) 133(6):526–32. doi: 10.1001/archotol.133.6.526
96. Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the Significance of Changes in Health-Related Quality-of-Life Scores. J Clin Oncol (1998) 16(1):139–44. doi: 10.1200/JCO.1998.16.1.139
97. Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM. Evidence-Based Guidelines for Determination of Sample Size and Interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J Clin Oncol (2011) 29(1):89–96. doi: 10.1200/JCO.2010.28.0107
98. Ringash J, Bezjak A, O'Sullivan B, Redelmeier DA. Interpreting Differences in Quality of Life: The FACT-H&N in Laryngeal Cancer Patients. Qual Life Res (2004) 13(4):725–33. doi: 10.1023/B:QURE.0000021703.47079.46
99. Hammerlid E, Bjordal K, Ahlner-Elmqvist M, Boysen M, Evensen JF, Biörklund A, et al. A Prospective Study of Quality of Life in Head and Neck Cancer Patients. Part I: At Diagnosis. Laryngoscope (2001) 111(4 Pt 1):669–80. doi: 10.1097/00005537-200104000-00021
100. Hammermüller C, Hinz A, Dietz A, Wichmann G, Pirlich M, Berger T, et al. Depression, Anxiety, Fatigue, and Quality of Life in a Large Sample of Patients Suffering From Head and Neck Cancer in Comparison With the General Population. BMC Cancer (2021) 21(1):94. doi: 10.1186/s12885-020-07773-6
101. Holland JC, Andersen B, Breitbart WS, Compas B, Dudley MM, Fleishman S, et al. Distress Management. J Natl Compr Canc Netw (2010) 8(4):448–85. doi: 10.6004/jnccn.2010.0034
102. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and Validation of a Geriatric Depression Screening Scale: A Preliminary Report. J Psychiatr Res (1982) 17(1):37–49. doi: 10.1016/0022-3956(82)90033-4
103. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand (1983) 67(6):361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
104. Pilkonis PA, Choi SW, Reise SP, Stover AM, Riley WT, Cella D, et al. Item Banks for Measuring Emotional Distress From the Patient-Reported Outcomes Measurement Information System (PROMIS(R)): Depression, Anxiety, and Anger. Assessment (2011) 18(3):263–83. doi: 10.1177/1073191111411667
105. Beck AT SR, Brown GK. BDI®-II Manual. San Antonio, TX, USA: The Psychological Corporation (1996).
106. Radloff LS. The CES-D Scale:A Self-Report Depression Scale for Research in the General Population. Appl psychol Meas (1977) 1(3):385–401. doi: 10.1177/014662167700100306
107. Ramanaiah NV, Franzen M, Schill T. A Psychometric Study of the State-Trait Anxiety Inventory. J Pers Assess (1983) 47(5):531–5. doi: 10.1207/s15327752jpa4705_14
108. Hamilton M. Development of a Rating Scale for Primary Depressive Illness. Br J Soc Clin Psychol (1967) 6(4):278–96. doi: 10.1111/j.2044-8260.1967.tb00530.x
109. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J Clin Psychiatry (1998) 59 Suppl 20:22–33;quiz 4-57.
110. Lenderking WR, Hu M, Tennen H, Cappelleri JC, Petrie CD, Rush AJ. Daily Process Methodology for Measuring Earlier Antidepressant Response. Contemp Clin Trials (2008) 29(6):867–77. doi: 10.1016/j.cct.2008.05.012
111. Carver CS, Scheier MF, Weintraub JK. Assessing Coping Strategies: A Theoretically Based Approach. J Pers Soc Psychol (1989) 56(2):267–83. doi: 10.1037/0022-3514.56.2.267
112. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a Brief Depression Severity Measure. J Gen Intern Med (2001) 16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
113. Broadbent E, Petrie KJ, Main J, Weinman J. The Brief Illness Perception Questionnaire. J Psychosom Res (2006) 60(6):631–7. doi: 10.1016/j.jpsychores.2005.10.020
114. Kertz S, Bigda-Peyton J, Bjorgvinsson T. Validity of the Generalized Anxiety Disorder-7 Scale in an Acute Psychiatric Sample. Clin Psychol Psychother (2013) 20(5):456–64. doi: 10.1002/cpp.1802
115. Roth AJ, Kornblith AB, Batel-Copel L, Peabody E, Scher HI, Holland JC. Rapid Screening for Psychologic Distress in Men With Prostate Carcinoma: A Pilot Study. Cancer (1998) 82(10):1904–8. doi: 10.1002/(SICI)1097-0142(19980515)82:10<1904::AID-CNCR13>3.0.CO;2-X
116. Watson M, Greer S, Young J, Inayat Q, Burgess C, Robertson B. Development of a Questionnaire Measure of Adjustment to Cancer: The MAC Scale. psychol Med (1988) 18(1):203–9. doi: 10.1017/S0033291700002026
117. Thomas BC, Mohan VN, Thomas I, Pandey M. Development of a Distress Inventory for Cancer: Preliminary Results. J Postgrad Med (2002) 48(1):16–20.
118. Rogers SN, El-Sheikha J, Lowe D. The Development of a Patients Concerns Inventory (PCI) to Help Reveal Patients Concerns in the Head and Neck Clinic. Oral Oncol (2009) 45(7):555–61. doi: 10.1016/j.oraloncology.2008.09.004
119. Badr H, Gupta V, Sikora A, Posner M. Psychological Distress in Patients and Caregivers Over the Course of Radiotherapy for Head and Neck Cancer. Oral Oncol (2014) 50(10):1005–11. doi: 10.1016/j.oraloncology.2014.07.003
120. Kroenke CH, Kubzansky LD, Schernhammer ES, Holmes MD, Kawachi I. Social Networks, Social Support, and Survival After Breast Cancer Diagnosis. J Clin Oncol (2006) 24(7):1105–11. doi: 10.1200/JCO.2005.04.2846
121. Caillet P, Canoui-Poitrine F, Vouriot J, Berle M, Reinald N, Krypciak S, et al. Comprehensive Geriatric Assessment in the Decision-Making Process in Elderly Patients With Cancer: ELCAPA Study. J Clin Oncol (2011) 29(27):3636–42. doi: 10.1200/JCO.2010.31.0664
122. Senchak JJ, Fang CY, Bauman JR. Interventions to Improve Quality of Life (QOL) and/or Mood in Patients With Head and Neck Cancer (HNC): A Review of the Evidence. Cancers Head Neck (2019) 4:2. doi: 10.1186/s41199-019-0041-4
123. Cash E, Duck CR, Brinkman C, Rebholz W, Albert C, Worthen M, et al. Depressive Symptoms and Actigraphy-Measured Circadian Disruption Predict Head and Neck Cancer Survival. Psychooncology (2018) 27(10):2500–7. doi: 10.1002/pon.4862
124. Chen AM, Jennelle RL, Grady V, Tovar A, Bowen K, Simonin P, et al. Prospective Study of Psychosocial Distress Among Patients Undergoing Radiotherapy for Head and Neck Cancer. Int J Radiat Oncol Biol Phys (2009) 73(1):187–93. doi: 10.1016/j.ijrobp.2008.04.010
125. D'Souza V, Blouin E, Zeitouni A, Muller K, Allison PJ. An Investigation of the Effect of Tailored Information on Symptoms of Anxiety and Depression in Head and Neck Cancer Patients. Oral Oncol (2013) 49(5):431–7. doi: 10.1016/j.oraloncology.2012.12.001
126. Ghazali N, Roe B, Lowe D, Tandon S, Jones T, Brown J, et al. Screening for Distress Using the Distress Thermometer and the University of Washington Quality of Life in Post-Treatment Head and Neck Cancer Survivors. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2017) 274(5):2253–60. doi: 10.1007/s00405-017-4474-2
127. Hammerlid E, Ahlner-Elmqvist M, Bjordal K, Biorklund A, Evensen J, Boysen M, et al. A Prospective Multicentre Study in Sweden and Norway of Mental Distress and Psychiatric Morbidity in Head and Neck Cancer Patients. Br J Cancer (1999) 80(5-6):766–74. doi: 10.1038/sj.bjc.6690420
128. Horney DJ, Smith HE, McGurk M, Weinman J, Herold J, Altman K, et al. Associations Between Quality of Life, Coping Styles, Optimism, and Anxiety and Depression in Pretreatment Patients With Head and Neck Cancer. Head Neck (2011) 33(1):65–71. doi: 10.1002/hed.21407
129. Howren MB, Christensen AJ, Karnell LH, Funk GF. Health-Related Quality of Life in Head and Neck Cancer Survivors: Impact of Pretreatment Depressive Symptoms. Health Psychol (2010) 29(1):65–71. doi: 10.1037/a0017788
130. Humphris GM, Rogers SN. The Association of Cigarette Smoking and Anxiety, Depression and Fears of Recurrence in Patients Following Treatment of Oral and Oropharyngeal Malignancy. Eur J Cancer Care (Engl) (2004) 13(4):328–35. doi: 10.1111/j.1365-2354.2004.00479.x
131. Ichikura K, Yamashita A, Sugimoto T, Kishimoto S, Matsushima E. Persistence of Psychological Distress and Correlated Factors Among Patients With Head and Neck Cancer. Palliat Support Care (2016) 14(1):42–51. doi: 10.1017/S1478951515000711
132. Kanatas A, Ghazali N, Lowe D, Rogers SN. The Identification of Mood and Anxiety Concerns Using the Patients Concerns Inventory Following Head and Neck Cancer. Int J Oral Maxillofac Surg (2012) 41(4):429–36. doi: 10.1016/j.ijom.2011.12.021
133. Kumar K, Kumar S, Mehrotra D, Tiwari SC, Kumar V, Khandpur S, et al. Prospective Evaluation of Psychological Burden in Patients With Oral Cancer. Br J Oral Maxillofac Surg (2018) 56(10):918–24. doi: 10.1016/j.bjoms.2018.09.004
134. Neilson K, Pollard A, Boonzaier A, Corry J, Castle D, Smith D, et al. A Longitudinal Study of Distress (Depression and Anxiety) Up to 18 Months After Radiotherapy for Head and Neck Cancer. Psychooncology (2013) 22(8):1843–8. doi: 10.1002/pon.3228
135. Joseph LA, Routledge JA, Burns MP, Swindell R, Sykes AJ, Slevin NJ, et al. Value of the Hospital Anxiety and Depression Scale in the Follow Up of Head and Neck Cancer Patients. J Laryngol Otol (2013) 127(3):285–94. doi: 10.1017/S0022215113000078
136. Tang PL, Wang C, Hung MF, Lin HS. Assessment of Symptom Distress in Cancer Patients Before and After Radiotherapy. Cancer Nurs (2011) 34(1):78–84. doi: 10.1097/NCC.0b013e3181f04ac8
137. van Beek FE, Jansen F, Mak L, Lissenberg-Witte BI, Buter J, Vergeer MR, et al. The Course of Symptoms of Anxiety and Depression From Time of Diagnosis Up to 2 Years Follow-Up in Head and Neck Cancer Patients Treated With Primary (Chemo)Radiation. Oral Oncol (2020) 102:104576. doi: 10.1016/j.oraloncology.2020.104576
138. Wang Y, Lu W, Shen X. Assessment of Preoperative Psychologic Distress in Laryngeal Cancer Patients. Acta Otolaryngol (2019) 139(2):184–6. doi: 10.1080/00016489.2018.1523555
139. McCaffrey JC, Weitzner M, Kamboukas D, Haselhuhn G, Lamonde L, Booth-Jones M. Alcoholism, Depression, and Abnormal Cognition in Head and Neck Cancer: A Pilot Study. Otolaryngol Head Neck Surg (2007) 136(1):92–7. doi: 10.1016/j.otohns.2006.06.1275
140. Wang C, Chen J, Su L, Hua Y, Ye J, Song X, et al. The Psychological Status in Patients With Nasopharyngeal Carcinoma During Radiotherapy. Eur Arch Otorhinolaryngol (2022) 279(2):1035–42. doi: 10.1007/s00405-021-06892-5
141. Astrup GL, Rustoen T, Miaskowski C, Paul SM, Bjordal K. A Longitudinal Study of Depressive Symptoms in Patients With Head and Neck Cancer Undergoing Radiotherapy. Cancer Nurs (2015) 38(6):436–46. doi: 10.1097/NCC.0000000000000225
142. Bjordal K, Kaasa S. Psychological Distress in Head and Neck Cancer Patients 7-11 Years After Curative Treatment. Br J Cancer (1995) 71(3):592–7. doi: 10.1038/bjc.1995.115
143. Chen AM, Hsu S, Felix C, Garst J, Yoshizaki T. Effect of Psychosocial Distress on Outcome for Head and Neck Cancer Patients Undergoing Radiation. Laryngoscope (2018) 128(3):641–5. doi: 10.1002/lary.26751
144. de Leeuw JR, de Graeff A, Ros WJ, Blijham GH, Hordijk GJ, Winnubst JA. Prediction of Depressive Symptomatology After Treatment of Head and Neck Cancer: The Influence of Pre-Treatment Physical and Depressive Symptoms, Coping, and Social Support. Head Neck (2000) 22(8):799–807. doi: 10.1002/1097-0347(200012)22:8<799::AID-HED9>3.0.CO;2-E
145. Deng YT, Zhong WN, Jiang Y. Measurement of Distress and its Alteration During Treatment in Patients With Nasopharyngeal Carcinoma. Head Neck (2014) 36(8):1077–86. doi: 10.1002/hed.23412
146. Derks W, Leeuw JR, Hordijk GJ, Winnubst JA. Differences in Coping Style and Locus of Control Between Older and Younger Patients With Head and Neck Cancer. Clin Otolaryngol (2005) 30(2):186–92. doi: 10.1111/j.1365-2273.2004.00938.x
147. Henry M, Fuehrmann F, Hier M, Zeitouni A, Kost K, Richardson K, et al. Contextual and Historical Factors for Increased Levels of Anxiety and Depression in Patients With Head and Neck Cancer: A Prospective Longitudinal Study. Head Neck (2019) 41(8):2538–48. doi: 10.1002/hed.25725
148. Kim SA, Roh JL, Lee SA, Lee SW, Kim SB, Choi SH, et al. Pretreatment Depression as a Prognostic Indicator of Survival and Nutritional Status in Patients With Head and Neck Cancer. Cancer (2016) 122(1):131–40. doi: 10.1002/cncr.29693
149. Kobayashi M, Sugimoto T, Matsuda A, Matsushima E, Kishimoto S. Association Between Self-Esteem and Depression Among Patients With Head and Neck Cancer: A Pilot Study. Head Neck (2008) 30(10):1303–9. doi: 10.1002/hed.20868
150. Kugaya A, Akechi T, Okuyama T, Nakano T, Mikami I, Okamura H, et al. Prevalence, Predictive Factors, and Screening for Psychologic Distress in Patients With Newly Diagnosed Head and Neck Cancer. Cancer (2000) 88(12):2817–23. doi: 10.1002/1097-0142(20000615)88:12<2817::AID-CNCR22>3.0.CO;2-N
151. Kunz V, Wichmann G, Lehmann-Laue A, Mehnert-Theuerkauf A, Dietz A, Wiegand S. Screening for Distress, Related Problems and Perceived Need for Psycho-Oncological Support in Head and Neck Squamous Cell Carcinoma (HNSCC) Patients: A Retrospective Cohort Study. BMC Cancer (2021) 21(1):478. doi: 10.1186/s12885-021-08236-2
152. Neilson KA, Pollard AC, Boonzaier AM, Corry J, Castle DJ, Mead KR, et al. Psychological Distress (Depression and Anxiety) in People With Head and Neck Cancers. Med J Aust (2010) 193(S5):S48–51. doi: 10.5694/j.1326-5377.2010.tb03928.x
153. Panwar A, Rieke K, Burke WJ, Sayles H, Lydiatt WM, Prevention of Depression in Patients Being Treated for H, et al. Identification of Baseline Characteristics Associated With Development of Depression Among Patients With Head and Neck Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Otolaryngol– Head Neck Surg (2018) 144(11):1004–10. doi: 10.1001/jamaoto.2018.2228
154. Schell JT, Petermann-Meyer A, Kloss-Brandstatter A, Bartella AK, Kamal M, Holzle F, et al. Distress Thermometer for Preoperative Screening of Patients With Oral Squamous Cell Carcinoma. J Craniomaxillofac Surg (2018) 46(7):1111–6. doi: 10.1016/j.jcms.2018.04.022
155. Speksnijder CM, Lankhorst PJM, de Bree R, de Haan AFJ, Koole R, Merkx MAW. Depression and Related Factors After Oral Oncological Treatment: A 5-Year Prospective Cohort Study. Support Care Cancer (2021) 29(6):2907–16. doi: 10.1007/s00520-020-05795-1
156. Verdonck-de Leeuw IM, de Bree R, Keizer AL, Houffelaar T, Cuijpers P, van der Linden MH, et al. Computerized Prospective Screening for High Levels of Emotional Distress in Head and Neck Cancer Patients and Referral Rate to Psychosocial Care. Oral Oncol (2009) 45(10):e129–33. doi: 10.1016/j.oraloncology.2009.01.012
157. Thomas ML, Kaufmann CN, Palmer BW, Depp CA, Martin AS, Glorioso DK, et al. Paradoxical Trend for Improvement in Mental Health With Aging: A Community-Based Study of 1,546 Adults Aged 21-100 Years. J Clin Psychiatry (2016) 77(8):e1019–25. doi: 10.4088/JCP.16m10671
158. Mirosevic S, Thewes B, van Herpen C, Kaanders J, Merkx T, Humphris G, et al. Prevalence and Clinical and Psychological Correlates of High Fear of Cancer Recurrence in Patients Newly Diagnosed With Head and Neck Cancer. Head Neck (2019) 41(9):3187–200. doi: 10.1002/hed.25812
159. Casswell G, Gough K, Drosdowsky A, Bressel M, Coleman A, Shrestha S, et al. Fear of Cancer Recurrence in Survivors of Human Papillomavirus-Associated Oropharyngeal Carcinoma. Int J Radiat Oncol Biol Phys (2021) 111(4):890–9. doi: 10.1016/j.ijrobp.2021.07.006
160. Rogers SN, Monssen C, Humphris GM, Lowe D, Kanatas A. Which Head and Neck Cancer Patients Are Most at Risk of High Levels of Fear of Cancer Recurrence. Front Psychol (2021) 12:671366. doi: 10.3389/fpsyg.2021.671366
161. Ghazali N, Cadwallader E, Lowe D, Humphris G, Ozakinci G, Rogers SN. Fear of Recurrence Among Head and Neck Cancer Survivors: Longitudinal Trends. Psychooncology (2013) 22(4):807–13. doi: 10.1002/pon.3069
162. Kanatas A, Humphris G, Lowe D, Rogers SN. Further Analysis of the Emotional Consequences of Head and Neck Cancer as Reflected by the Patients' Concerns Inventory. Br J Oral Maxillofac Surg (2015) 53(8):711–8. doi: 10.1016/j.bjoms.2015.02.026
163. Rogers SN, Cross B, Talwar C, Lowe D, Humphris G. A Single-Item Screening Question for Fear of Recurrence in Head and Neck Cancer. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2016) 273(5):1235–42. doi: 10.1007/s00405-015-3585-x
164. Rogers SN, Audisio RA, Lowe D. Do the Elderly Raise Different Issues When Using the Patient Concerns Inventory in Routine Head and Neck Cancer Follow-Up Clinics? Eur J Cancer Care (Engl) (2015) 24(2):189–97. doi: 10.1111/ecc.12289
165. Rylands J, Lowe D, Rogers SN. Influence of Deprivation on Health-Related Quality of Life of Patients With Cancer of the Head and Neck in Merseyside and Cheshire. Br J Oral Maxillofac Surg (2016) 54(6):669–76. doi: 10.1016/j.bjoms.2016.03.030
166. Rogers SN, Scott B, Lowe D, Ozakinci G, Humphris GM. Fear of Recurrence Following Head and Neck Cancer in the Outpatient Clinic. Eur Arch Otorhinolaryngol Off J Eur Fed Otorhinolaryngol Societies (2010) 267(12):1943–9. doi: 10.1007/s00405-010-1307-y
167. Llewellyn CD, Weinman J, McGurk M, Humphris G. Can We Predict Which Head and Neck Cancer Survivors Develop Fears of Recurrence? J Psychosomatic Res (2008) 65(6):525–32. doi: 10.1016/j.jpsychores.2008.03.014
168. Van Liew JR, Christensen AJ, Howren MB, Hynds Karnell L, Funk GF. Fear of Recurrence Impacts Health-Related Quality of Life and Continued Tobacco Use in Head and Neck Cancer Survivors. Health Psychol Off J Division Health Psychology Am psychol Assoc (2014) 33(4):373–81. doi: 10.1037/a0032680
169. Simard S, Savard J. Fear of Cancer Recurrence Inventory: Development and Initial Validation of a Multidimensional Measure of Fear of Cancer Recurrence. Support Care Cancer (2009) 17(3):241–51. doi: 10.1007/s00520-008-0444-y
170. Simard S, Savard J. Screening and Comorbidity of Clinical Levels of Fear of Cancer Recurrence. J Cancer Surviv (2015) 9(3):481–91. doi: 10.1007/s11764-015-0424-4
171. Simard S, Thewes B, Humphris G, Dixon M, Hayden C, Mireskandari S, et al. Fear of Cancer Recurrence in Adult Cancer Survivors: A Systematic Review of Quantitative Studies. J Cancer Surviv (2013) 7(3):300–22. doi: 10.1007/s11764-013-0272-z
172. Chen C, Cao J, Wang L, Zhang R, Li H, Peng J. Body Image and its Associated Factors Among Chinese Head and Neck Cancer Patients Undergoing Surgical Treatment: A Cross-Sectional Survey. Support Care Cancer (2020) 28(3):1233–9. doi: 10.1007/s00520-019-04940-9
173. Clarke SA, Newell R, Thompson A, Harcourt D, Lindenmeyer A. Appearance Concerns and Psychosocial Adjustment Following Head and Neck Cancer: A Cross-Sectional Study and Nine-Month Follow-Up. Psychol Health Med (2014) 19(5):505–18. doi: 10.1080/13548506.2013.855319
174. Chang DC, Chen AW, Lo YS, Chuang YC, Chen MK. Factors Associated With Suicidal Ideation Risk in Head and Neck Cancer: A Longitudinal Study. Laryngoscope (2019) 129(11):2491–5. doi: 10.1002/lary.27843
175. Zebolsky AL, Ochoa E, Badran KW, Heaton C, Park A, Seth R, et al. Appearance-Related Distress and Social Functioning After Head and Neck Microvascular Reconstruction. Laryngoscope (2021) 131(7):E2204–11. doi: 10.1002/lary.29548
176. Cramer JD, Johnson JT, Nilsen ML. Pain in Head and Neck Cancer Survivors: Prevalence, Predictors, and Quality-Of-Life Impact. Otolaryngol Head Neck Surg (2018) 159(5):853–8. doi: 10.1177/0194599818783964
177. Moye J, June A, Martin LA, Gosian J, Herman LI, Naik AD. Pain is Prevalent and Persisting in Cancer Survivors: Differential Factors Across Age Groups. J Geriatr Oncol (2014) 5(2):190–6. doi: 10.1016/j.jgo.2013.12.006
178. Hassanein KA, Musgrove BT, Bradbury E. Functional Status of Patients With Oral Cancer and its Relation to Style of Coping, Social Support and Psychological Status. Br J Oral Maxillofac Surg (2001) 39(5):340–5. doi: 10.1054/bjom.2001.0652
179. Hickok JT, Roscoe JA, Morrow GR, Mustian K, Okunieff P, Bole CW. Frequency, Severity, Clinical Course, and Correlates of Fatigue in 372 Patients During 5 Weeks of Radiotherapy for Cancer. Cancer (2005) 104(8):1772–8. doi: 10.1002/cncr.21364
180. Rogers LQ, Courneya KS, Robbins KT, Rao K, Malone J, Seiz A, et al. Factors Associated With Fatigue, Sleep, and Cognitive Function Among Patients With Head and Neck Cancer. Head Neck (2008) 30(10):1310–7. doi: 10.1002/hed.20873
181. Santoso AMM, Jansen F, Lissenberg-Witte BI, Baatenburg de Jong RJ, Langendijk JA, Leemans CR, et al. Poor Sleep Quality Among Newly Diagnosed Head and Neck Cancer Patients: Prevalence and Associated Factors. Support Care Cancer (2021) 29(2):1035–45. doi: 10.1007/s00520-020-05577-9
182. Holtmaat K, van der Spek N, Cuijpers P, Leemans CR, Verdonck-de Leeuw IM. Posttraumatic Growth Among Head and Neck Cancer Survivors With Psychological Distress. Psychooncology (2017) 26(1):96–101. doi: 10.1002/pon.4106
183. Kangas M, Henry JL, Bryant RA. Predictors of Posttraumatic Stress Disorder Following Cancer. Health Psychol (2005) 24(6):579–85. doi: 10.1037/0278-6133.24.6.579
184. Moschopoulou E, Hutchison I, Bhui K, Korszun A. Post-Traumatic Stress in Head and Neck Cancer Survivors and Their Partners. Support Care Cancer (2018) 26(9):3003–11. doi: 10.1007/s00520-018-4146-9
185. Posluszny DM, Dougall AL, Johnson JT, Argiris A, Ferris RL, Baum A, et al. Posttraumatic Stress Disorder Symptoms in Newly Diagnosed Patients With Head and Neck Cancer and Their Partners. Head Neck (2015) 37(9):1282–9. doi: 10.1002/hed.23760
186. Richardson AE, Morton RP, Broadbent E. Coping Strategies Predict Post-Traumatic Stress in Patients With Head and Neck Cancer. Eur Arch Otorhinolaryngol (2016) 273(10):3385–91. doi: 10.1007/s00405-016-3960-2
187. Aarstad AK, Beisland E, Aarstad HJ. Personality, Choice of Coping and T Stage Predict Level of Distress in Head and Neck Cancer Patients During Follow-Up. Eur Arch Otorhinolaryngol (2012) 269(9):2121–8. doi: 10.1007/s00405-011-1884-4
188. Aarstad AK, Beisland E, Osthus AA, Aarstad HJ. Distress, Quality of Life, Neuroticism and Psychological Coping are Related in Head and Neck Cancer Patients During Follow-Up. Acta Oncol (2011) 50(3):390–8. doi: 10.3109/0284186X.2010.504227
189. Ichikura K, Yamashita A, Sugimoto T, Kishimoto S, Matsushima E. Patterns of Stress Coping and Depression Among Patients With Head and Neck Cancer: A Japanese Cross-Sectional Study. Psychooncology (2018) 27(2):556–62. doi: 10.1002/pon.4549
190. Verdonck-de Leeuw IM, Eerenstein SE, van der Linden MH, Kuik DJ, de Bree R, Leemans CR. Distress in Spouses and Patients After Treatment for Head and Neck Cancer. Laryngoscope (2007) 117(2):238–41. doi: 10.1097/01.mlg.0000250169.10241.58
191. Zaorsky NG, Zhang Y, Tuanquin L, Bluethmann SM, Park HS, Chinchilli VM. Suicide Among Cancer Patients. Nat Commun (2019) 10(1):207. doi: 10.1038/s41467-018-08170-1
192. Anguiano L, Mayer DK, Piven ML, Rosenstein D. A Literature Review of Suicide in Cancer Patients. Cancer Nurs (2012) 35(4):E14–26. doi: 10.1097/NCC.0b013e31822fc76c
193. Choi JW, Park EC. Suicide Risk After Cancer Diagnosis Among Older Adults: A Nationwide Retrospective Cohort Study. J Geriatr Oncol (2020) 11(5):814–9. doi: 10.1016/j.jgo.2019.11.006
194. Osazuwa-Peters N, Simpson MC, Zhao L, Boakye EA, Olomukoro SI, Deshields T, et al. Suicide Risk Among Cancer Survivors: Head and Neck Versus Other Cancers. Cancer (2018) 124(20):4072–9. doi: 10.1002/cncr.31675
195. Noel CW, Eskander A, Sutradhar R, Mahar A, Vigod SN, Isenberg-Grzeda E, et al. Incidence of and Factors Associated With Nonfatal Self-Injury After a Cancer Diagnosis in Ontario, Canada. JAMA Netw Open (2021) 4(9):e2126822. doi: 10.1001/jamanetworkopen.2021.26822
196. Fang F, Fall K, Mittleman MA, Sparén P, Ye W, Adami HO, et al. Suicide and Cardiovascular Death After a Cancer Diagnosis. N Engl J Med (2012) 366(14):1310–8. doi: 10.1056/NEJMoa1110307
197. Klaassen Z, Wallis CJD, Chandrasekar T, Goldberg H, Sayyid RK, Williams SB, et al. Cancer Diagnosis and Risk of Suicide After Accounting for Prediagnosis Psychiatric Care: A Matched-Cohort Study of Patients With Incident Solid-Organ Malignancies. Cancer (2019) 125(16):2886–95. doi: 10.1002/cncr.32146
198. Shunmugasundaram C, Rutherford C, Butow PN, Sundaresan P, Dhillon HM. Content Comparison of Unmet Needs Self-Report Measures Used in Patients With Head and Neck Cancer: A Systematic Review. Psychooncology (2019) 28(12):2295–306. doi: 10.1002/pon.5257
199. Giuliani M, McQuestion M, Jones J, Papadakos J, Le LW, Alkazaz N, et al. Prevalence and Nature of Survivorship Needs in Patients With Head and Neck Cancer. Head Neck (2016) 38(7):1097–103. doi: 10.1002/hed.24411
200. Henry M, Habib LA, Morrison M, Yang JW, Li XJ, Lin S, et al. Head and Neck Cancer Patients Want Us to Support Them Psychologically in the Posttreatment Period: Survey Results. Palliat Support Care (2014) 12(6):481–93. doi: 10.1017/S1478951513000771
201. Henry M, Alias A, Cherba M, Woronko C, Rosberger Z, Hier M, et al. Immediate Post-Treatment Supportive Care Needs of Patients Newly Diagnosed With Head and Neck Cancer. Support Care Cancer (2020) 28(11):5557–67. doi: 10.1007/s00520-020-05368-2
202. Wells M, Cunningham M, Lang H, Swartzman S, Philp J, Taylor L, et al. Distress, Concerns and Unmet Needs in Survivors of Head and Neck Cancer: A Cross-Sectional Survey. Eur J Cancer Care (2015) 24(5):748–60. doi: 10.1111/ecc.12370
203. Ghazali N, Roe B, Lowe D, Rogers SN. Patients Concerns Inventory Highlights Perceived Needs and Concerns in Head and Neck Cancer Survivors and its Impact on Health-Related Quality of Life. Br J Oral Maxillofac Surg (2015) 53(4):371–9. doi: 10.1016/j.bjoms.2015.01.022
204. O'Brien KM, Timmons A, Butow P, Gooberman-Hill R, O'Sullivan E, Balfe M, et al. Associations Between Neighbourhood Support and Financial Burden With Unmet Needs of Head and Neck Cancer Survivors. Oral Oncol (2017) 65:57–64. doi: 10.1016/j.oraloncology.2016.12.019
205. Manne S, Hudson SV, Baredes S, Stroup A, Virtue SM, Paddock L, et al. Survivorship Care Experiences, Information, and Support Needs of Patients With Oral and Oropharyngeal Cancer. Head Neck (2016) 38 Suppl 1(Suppl 1):E1935–46. doi: 10.1002/hed.24351
206. Chen SC, Liao CT, Lin CC, Chang JT, Lai YH. Distress and Care Needs in Newly Diagnosed Oral Cavity Cancer Patients Receiving Surgery. Oral Oncol (2009) 45(9):815–20. doi: 10.1016/j.oraloncology.2009.01.001
207. Lee MS, Nelson AM, Thompson LM, Donovan KA. Supportive Care Needs of Oral Cancer Survivors: Prevalence and Correlates. Oral Oncol (2016) 53:85–90. doi: 10.1016/j.oraloncology.2015.11.007
208. Ghazali N, Roe B, Lowe D, Rogers SN. Uncovering Patients′ Concerns in Routine Head and Neck Oncology Follow Up Clinics: An Exploratory Study. Br J Oral Maxillofacial Surg (2013) 51(4):294–300. doi: 10.1016/j.bjoms.2012.08.002
209. Rubenstein LZ, Stuck AE, Siu AL, Wieland D. Impacts of Geriatric Evaluation and Management Programs on Defined Outcomes: Overview of the Evidence. J Am Geriatrics Soc (1991) 39(9 Pt 2):8S–16S; discussion 7S-8S. doi: 10.1111/j.1532-5415.1991.tb05927.x
210. Wildiers H, Heeren P, Puts M, Topinkova E, Janssen-Heijnen ML, Extermann M, et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients With Cancer. J Clin Oncol (2014) 32(24):2595–603. doi: 10.1200/JCO.2013.54.8347
211. Neve M, Jameson MB, Govender S, Hartopeanu C. Impact of Geriatric Assessment on the Management of Older Adults With Head and Neck Cancer: A Pilot Study. J Geriatr Oncol (2016) 7(6):457–62. doi: 10.1016/j.jgo.2016.05.006
212. Raab G, Restifo D, McBride SM, Wong RJ, Lee NY, Shahrokni A, et al. Outcomes Following Head and Neck Cancer Surgery Among Older Adults as Determined by an Electronic Geriatric Assessment. J Geriatr Oncol (2021) S1879-4068(21):00242–3. doi: 10.1016/j.jgo.2021.10.010
213. Bras L, de Vries J, Festen S, Steenbakkers R, Langendijk JA, Witjes MJH, et al. Frailty and Restrictions in Geriatric Domains are Associated With Surgical Complications But Not With Radiation-Induced Acute Toxicity in Head and Neck Cancer Patients: A Prospective Study. Oral Oncol (2021) 118:105329. doi: 10.1016/j.oraloncology.2021.105329
214. VanderWalde NA, Deal AM, Comitz E, Stravers L, Muss H, Reeve BB, et al. Geriatric Assessment as a Predictor of Tolerance, Quality of Life, and Outcomes in Older Patients With Head and Neck Cancers and Lung Cancers Receiving Radiation Therapy. Int J Radiat Oncol Biol Phys (2017) 98(4):850–7. doi: 10.1016/j.ijrobp.2016.11.048
215. de Vries J, Bras L, Sidorenkov G, Festen S, Steenbakkers R, Langendijk JA, et al. Association of Deficits Identified by Geriatric Assessment With Deterioration of Health-Related Quality of Life in Patients Treated for Head and Neck Cancer. JAMA Otolaryngol– Head Neck Surg (2021) 147(12):1089–99. doi: 10.1001/jamaoto.2021.2837
Keywords: radiation therapy, head neck cancer, surgery, chemotherapy, quality of life, psychosocial distress, sleep, unmet need
Citation: McDowell L, Rischin D, Gough K and Henson C (2022) Health-Related Quality of Life, Psychosocial Distress and Unmet Needs in Older Patients With Head and Neck Cancer. Front. Oncol. 12:834068. doi: 10.3389/fonc.2022.834068
Received: 12 December 2021; Accepted: 24 January 2022;
Published: 15 February 2022.
Edited by:
Jan Baptist Vermorken, University of Antwerp, BelgiumReviewed by:
Marshall Posner, Icahn School of Medicine at Mount Sinai, United StatesPaul Swiecicki, University of Michigan, United States
Copyright © 2022 McDowell, Rischin, Gough and Henson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lachlan McDowell, TGFjaGxhbi5tY2Rvd2VsbEBwZXRlcm1hYy5vcmc=