 Khodr Terro
Khodr Terro Layal Sharrouf
Layal Sharrouf Jean El Cheikh
Jean El Cheikh
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 16 February 2022
Sec. Hematologic Malignancies
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.832428
This article is part of the Research Topic NK/T-Cell Lymphoma: Biology, Prognostics, Prediction, and Treatment View all 8 articles
Extranodal Natural Killer/T-cell lymphoma (ENKTL) is an extremely rare type of lymphoma which is highly lethal. It mainly affects the midline area unfolding as a necrotic granulomatous and extremely disfiguring lesion. There are two subtypes of (NKTL); the most common one is nasal which appears in the nasal cavity including the nasopharynx, oropharynx, parts of the aero digestive tract and Waldeyer’s ring. While the other rarer subtype, appears in sites like the skin, testis, gastrointestinal tract, salivary glands and muscle. ENKTL is popular for the expression of multidrug resistance-associated P-glycoprotein, which not only plays the main role at exporting many antitumor agents outside tumor cells, but also makes the disease hard to treat. It is commonly associated with Epstein-Barr virus (EBV) infection and commonly occurs in Asian populations. However, there is no single unified consensus yet as to what is the standardized treatment for ENKTL. Radiotherapy alone treatment, has been considered as a first-line therapy for localized ENKTL, which later on was found to be insufficient for improving survival rates. Thus, the combination of chemotherapy and radiotherapy has been recommended as a therapeutic modality for localized ENKTL. Several combination modalities of radiotherapy and chemotherapy have been advised in clinical practice including concurrent, sequential and sandwich chemo radiotherapy. For the best treatment outcome, only patients with localized nasal ENKTL and low risk of treatment failure are eligible for radiotherapy. Both radiotherapy and hematopoietic stem cell transplantation (HSCT) have been used as treatment modalities in ENKTL patients. Upfront HSCT was performed for ENKTL, but it was associated with a very poor prognosis even for the limited-stage disease. The evidence supporting the use of HSCT to treat ENKTL was derived from the results of a series of phase 1 and 2 trials along with retrospective studies. The end result was a unified consensus that consolidative HSCT is not necessary in patients with newly diagnosed localized ENKTL who achieved complete response after treatment with any of the modern chemo radiotherapy regimens. Hence, HSCT is solely advised for advanced and relapsed NKTL. The main debate remains over which HSCT is the most suitable for patients with newly diagnosed advanced NKTL and relapsed NKTL.
Natural Killer/T-cell lymphoma (NKTL) had been previously known as lethal midline granuloma due to its aggressive nature and its preference to grow in the medial region of the face (1). Later on, it was labeled as polymorphic reticulosis since it was found to be lymphoid in origin but essentially different from the commonly known lymphomas. NKTL microscopically consisted of inflammatory cells, eosinophils and atypical lymphoid cells (2). Then it was classified in the REAL classification of lymphoid malignancies as angiocentric T-cell lymphoma due to its tendency to invade blood vessels leading to zonal necrosis (3). With the advancement of immunohistochemistry and the development of monoclonal antibodies, it was revealed that this lymphoid malignancy is NK-cell in origin. That was after detecting the cytoplasmic ϵ chain of CD3 which is characteristic of NK-cells (4). Finally, in the 2016 World Health Organization (WHO) classification of lymphoid malignancies this disease is referred to as extra nodal NK/T cell lymphoma (5). It is predominantly an extra nodal lymphoma where the nasal cavity is the most common (80%) site of involvement. The term nasal cavity includes nose, nasopharynx, oropharynx, parts of the aero digestive tract and Waldeyer’s ring. This subtype is referred to as nasal NK/T cell lymphoma (6, 7). On the other hand, the other subtypes are collectively referred to as non-nasal NK/T cell lymphoma involving sites such as the skin, testis, gastrointestinal tract, salivary glands and muscle (6). NK/T cell lymphoma can rarely develop into a disseminated and more aggressive form by spreading hematogenously, infiltrating the liver, spleen, lymph nodes and bone marrow. In this case, it would be referred to as NK/T cell leukemia (6). Extranodal NK/T cell lymphoma (ENKTL) is commonly associated with Epstein-Barr virus (EBV) infection and most commonly occurs in Asian populations (5, 8). EBV in NK/T cells was found to be clonal after terminal repeat sequences assessment. Thus, it is believed that EBV plays a crucial role in the lymphomagenesis of ENKTL, and the presence of EBV is a requirement now for the diagnosis of ENKTL along with presence of CD56 or the cytotoxic molecules such as (granzyme B, TIA1, perforin) (5). With the improvement of our understanding to the pathogenesis of ENKTL, the treatment regimen has faced drastic changes. The previously used anthracycline-containing regimens like CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) and CHOP-like chemotherapy combinations were found to be working poorly. This is attributed to the expression of multidrug resistance-associated P-glycoprotein, which played the role at exporting many antitumor agents outside tumor cells (9, 10). In addition, multiple studies performed discovered the benefit of Hematopoietic Stem Cell Transplantation (HSCT) and radiotherapy in the treatment of NKTL. Nevertheless, a consensus over a standardized therapy has not been established yet due to the rarity of the disease and the scarcity of prospective trials (11). In this review, we will be exploring the findings regarding the benefits of various devised protocols of HSCT and radiotherapy used in the treatment of NKTL in both the western and the eastern worlds.
Different studies have shown resistance of NKTL tumor cells to anthracycline-containing combination chemotherapy, with 5-year survival rates of less than 30% (7). Since then, efforts were shifted towards studying the effectivity of radiotherapy in treating NKTL (12–14). Many retrospective analysis and prospective clinical trials were published in the Far East supporting the use of radiotherapy as the primary treatment (13, 15–18). Radiotherapy has been found to be the most important modality for treating ENKTL since the 1990s when NKTL was still referred to as angiocentric lymphoma (13). This was supported by the western studies which also appreciated the importance of radiotherapy by acknowledging the negative impact of the omission or delivery of inadequate doses of radiotherapy on the overall survival (OS) of patients with NKTL (19). Radiotherapy alone treatment has been considered as a first-line therapy for localized ENKTL. Several retrospective studies, mostly from the Far East, suggested that the appropriate radiotherapy dose in radiotherapy alone treatment of limited NKTL is 50-55 Gy (18, 20). The upfront use of radiotherapy alone has been reported to improve local control rate of localized NKTL especially the Nasal subtype (13, 21–23). Unfortunately, radiotherapy alone is found to be insufficient for improving survival due to a considerable number of patients experiencing local and systemic relapse after radiotherapy (24–26).
Thus, the combination of chemotherapy and radiotherapy became a recommended therapeutic modality for localized ENKTL (27). Several combination modalities of radiotherapy and chemotherapy have been advised in clinical practice including concurrent, sequential and sandwich chemo radiotherapy (28). Technically, those three modalities stemmed from the ongoing debate of whether to employ radiotherapy as an upfront therapy or as a sequential therapy preceded by chemotherapy in limited stage ENKTL. Employing radiotherapy as an upfront therapy, achieves high treatment response rates and reduces the risk of chemo resistance. However, initiating chemotherapy followed by radiotherapy has shown to reduce the risk of systemic failure and distant metastasis (28).
Starting with concurrent chemo radiotherapy, a phase II trial in Japan tested the 3 cycles DeVIC (dexamethasone, etoposide, ifosfamide, and carboplatin) chemotherapy regimen simultaneously with 50 Gy radiotherapy over a period of 6-8 weeks (Table 1). It has shown a complete response (CR) rate of 77%, an overall response (OR) rate of 81%, 5-year OR of 70% and a 5-year progression free survival (PFS) of 63% (17, 29). Despite this regimen positive results, it has shown that the simultaneous administration of chemotherapy and radiotherapy increases the risk of hematological and non-hematological toxicities regardless of chemotherapy regimen. Therefore, changing the chemotherapy regimen to other regimens such as ESHAP (etoposide, steroid, high-dose Ara-C and cisplatin) and DEP (dexamethasone, etoposide and cisplatin) did not reduce toxicity rates (16, 30). Hence, another concurrent chemo radiotherapy regimen emerged consisting of 4 weeks of radiotherapy + cisplatin followed by an adjunct 3 cycles of VIPD (etoposide, ifosfamide, cisplatin, and dexamethasone), showed a CR rate of 80% and a 3-year PFS of 85%. In this regimen, the radiation dose has been reduced to around 40 Gy due to the radio-sensitizing quality of cisplatin. Many similar regimens have been employed in various trials with pretty close outcomes, but all have shown a significant potential risk of systemic disease progression during the period of radiotherapy (16, 31, 32). The latter issue led to two other chemo radiotherapy regimens (sequential and sandwich chemo radiotherapy) which start with chemotherapy as an upfront therapy.
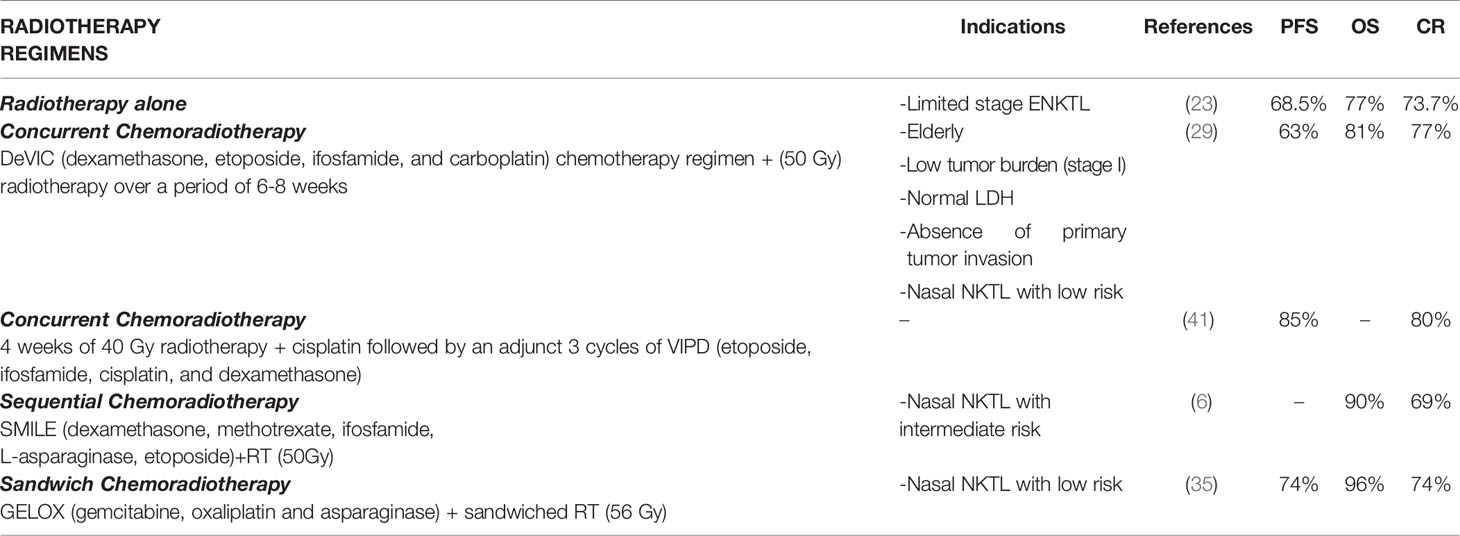
Table 1 Radiotherapy in NKTL.
The sequential chemo radiotherapy with 2-4 cycles of SMILE (dexamethasone, methotrexate, ifosfamide, L-asparaginase, and etoposide) followed by radiotherapy was demonstrated in a phase II clinical trial on stage IV NKTL. The results portrayed a CR rate of 69% and an OR rate of 90% (33). The SMILE has shown to commonly inflict severe hematologic toxicities which were intolerable in elderly and frail patients (6). Therefore, this therapy was advised as a treatment regimen for young low comorbid patients with localized nasal NKTL (6).
Finally, concerning the sandwich chemo radiotherapy regimen, a phase II trial has studied the employment of 2 cycles of GELOX (gemcitabine, L-asparaginase, and oxaliplatin) followed by radiotherapy of 56 Gy, then after a week 2-4 cycles of GELOX were added. Patients who experienced hypersensitivity to L-asparaginase were given pegaspargase instead. The outcome of this trial has shown a CR rate of 74% and an OR rate of 96% with an 85% 5-year PFS and 74% 5-year OS (34, 35). Despite the fact that this regimen is the most time consuming, it has shown the least levels of toxicities rendering it the most suitable for localized nasal NKTL in elderly and frail patients (36, 37).
More efforts have been exerted to decrease the toxicities induced by radiotherapy through implementing intensity modulated radiotherapy (IMRT) and volumetric modulated arc therapy (VMAT). Both of which are designed to use different types of boluses providing the patients with higher individuation and improved conformity and uniformity of the planning target volume. In other words, all these efforts are striving to make radiotherapy more effective which would permit the decrease of doses received by patients and consequently decrease the toxicity levels due to radiotherapy (37–40).
Furthermore, in order to achieve the best treatment outcome, radiotherapy should only be offered to patients with localized nasal ENKTL and low risk of treatment failure. Hence, a risk evaluation index (prognostic index of natural killer lymphoma (PINK)) was proposed to help identify people with advanced disease where radiotherapy is not effective (41).
Both upfront autologous and allogenic HSCT were performed for NKTL when the disease had not yet received its finalized nomenclature and was associated with poor prognosis even for the limited-disease stage (42). The evidence supporting the use of HSCT to treat ENKTL was derived from the results of a series of phase 1 and 2 trials along with retrospective studies. The studies reached a unified consensus that consolidative HSCT is not necessary in patients with newly diagnosed localized ENKTL who achieved CR after treatment with any of the modern chemo radiotherapy regimens previously discussed (29, 43, 44). The main debate remains over which HSCT is the most suitable for patients with newly diagnosed advanced NKTL and relapsed NKTL.
In a retrospective study for 62 patients, 50% of those had advanced stage NKTL and most of them received non-anthracycline-containing induction regimen. Around 65% had achieved CR pre auto-HSCT. After a 3-year follow-up the PFS and OS the came out to be 52.4% and 60% respectively. Patients with limited disease for sure did significantly better than the ones with advanced disease. Although 90% of patients with advanced NKTL were treated with non-anthracycline containing induction regimens, the 3-year PFS and OS came out to be 40.1% and 52.3% respectively. Unfortunately, all this did not show any difference compared to patients not receiving transplant from the previous studies (11). Another retrospective study from China had 20 patients mostly with advanced ENKTL who underwent upfront auto-HSCT following induction therapy with L-asparaginase-containing-chemotherapy with or without radiotherapy. The outcome of this group was compared to a control group consisting of 60 patients mostly with advanced ENKTL receiving the same chemotherapy and were eligible for auto-HSCT, but they declined. The 5-year OS of the auto-HSCT group came out to be 79.3% which is comparably higher than that of the control group which was 52.3%. While auto-HSCT group didn’t show a statistical significance in increasing the PFS rate compared to the control group (P=0.079). Based on the results of this retrospective study, the disease status and staging were found to be an important variable in giving the final verdict about the benefit of auto-HSCT in NKTL. Even though the auto-HSCT group showed a better OS than the control group, there was no additional benefit seen when comparing the outcomes of stage I/II NKTL patients from both groups (45). The European Society for Blood and Marrow Transplantation (EBMT) had a cohort of 28 patients who underwent auto-HSCT. The 2-year PFS and OS rates of the advanced-stage NKTL patients were 41% and 52% respectively. The outcome of those auto-HSCT patients, who received L-asparaginase-containing-induction therapy, was comparable to the outcomes in other similar studies (46). As a result, an official consensus was released by the American Society of Blood and Marrow Transplantation (ASBMT) to reserve auto-HSCT only for advanced-stage, relapsed or disseminated NKTL (43).
On the other hand, allo-HSCT has been evaluated in a retrospective analysis of 36 patients treated for NKTL where 10 patients were at an advanced stage. The 2-year PFS and OS were 30% and 40% respectively (Table 2). Most of the patients received L-asparaginase-containing induction regimen pre allo-HSCT. The main disadvantageous factors that played a role in decreasing OS rates were relapse, GVHD and infection (47). Another retrospective study, with patients receiving L-asparaginase-containing induction regimen pre allo-HSCT as well, was led by Center for International Bone Marrow Transplant Registry (CIBMTR) on 25 patients with 21 of them diagnosed with advanced stage NKTL. The 2-year PFS and OS rates were reported to be 20% and 24% respectively. The CR pre allo-HSCT was found to be the main predictor in achieving better survival rates (P< 0.001) (43). A multicenter retrospective analysis, led by the Asian Lymphoma Study Group with a total of 18 patients, studied allo-HSCT survival rates following L-asparaginase induction therapy as well. The 5-year PFS and OS were 51% and 57% respectively. It was noted that the use of SMILE as an induction regimen pre allo-HSCT showed a significant improvement in both PFS and OS. However, it should be noted that the last conclusion was made based on a limited cohort of patients. In this retrospective study both non-relapse-mortality and infection were the major contributors to mortality (48). Both infection and GVHD remain as main limitations in allo-HSCT, but multiple studies are being devised to improve this disadvantageous aspect of allo-HSCT. A very recent retrospective Spanish study, over a period of 25 years with a cohort of 201 patient undergone allo-HSCT for either NKTL or T-cell neoplasia, has shown that both post-transplant cyclophosphamide (PTCy) and haploidentical donor significantly decreased the risk for acute GVHD (49). Moreover, the Japanese Journal of Prosthodontic Research has highlighted in their very recent case report the importance of providing dental care with customized care plan before, during, and after HSCT for NKTL. The latter is based on their case report which demonstrated a significant decrease in risks of infections and oral function complications (50). As a result, the ASBMT reached a consensus on allo-HSCT in NKTL as well. They recommend allo-HSCT for disseminated NKTL in 1st CR, for localized NKTL with chemo sensitive relapsed disease, and for localized NKTL with primary refractory or relapsed/refractory disease (43).

Table 2 HSCT in NKTL.
In conclusion, the prognosis of NKTL has never been any better than today. The role of radiotherapy and HSCT continue to evolve and improve. As for radiotherapy, the combination of chemotherapy (non-anthracycline, platinum or L-asparaginase containing) and radiotherapy is now advised as a therapeutic modality for only localized ENKTL with low risk of treatment failure. As for HSCT, it should be reserved for advanced stages of NKTL. Both auto-HSCT and allo-HSCT have shown promising results in advanced NKTL patients. Auto-HSCT is preferred more for disseminated NKTL with 1st CR, while allo-HSCT for refractory NKTL. Moreover, multiple studies are being devised to improve the two main limitations of HSCT which are GVHD and infection. For us to better understand and treat such a highly fatal and rare disease, additional multi-institutional collaborations and prospective clinical trials are needed.
JC is the corresponding author. KT is the first author responsible for writing the manuscript. LS is the second author responsible for editing and finalizing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chim CS, Ooi GC, Shek TW, Liang R, Kwong YL. Lethal Midline Granuloma Revisited: Nasal T/Natural-Killer Cell Lymphoma. J Clin Oncol (1999) 17(4):1322–5. doi: 10.1200/JCO.1999.17.4.1322
2. Tse E, Kwong YL. Diagnosis and Management of Extranodal NK/T Cell Lymphoma Nasal Type. Expert Rev Hematol (2016) 9(9):861–71. doi: 10.1080/17474086.2016.1206465
3. Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A Revised European-American Classification of Lymphoid Neoplasms: A Proposal From the International Lymphoma Study Group. Blood (1994) 84(5):1361–92. doi: 10.1182/blood.V84.5.1361.1361
4. Chan JK, Tsang WY, Ng CS. Clarification of CD3 Immunoreactivity in Nasal T/natural Killer Cell Lymphomas: The Neoplastic Cells Are Often CD3 Epsilon+. Blood (1996) 87(2):839–41. doi: 10.1182/blood.V87.2.839.bloodjournal872839
5. Chan JK Q-ML, Ferry JA eds. Extranodal Nk/T-Cell Lymphoma, Nasal Type. Lyon, France: IARC (2017).
6. Tse E, Kwong YL. How I Treat NK/T-Cell Lymphomas. Blood (2013) 121(25):4997–5005. doi: 10.1182/blood-2013-01-453233
7. Vose J, Armitage J, Weisenburger D. International Peripheral T-Cell and Natural Killer/T-Cell Lymphoma Study: Pathology Findings and Clinical Outcomes. J Clin Oncol (2008) 26(25):4124–30. doi: 10.1200/JCO.2008.16.4558
8. Kwong YL, Chan AC, Liang R, Chiang AK, Chim CS, Chan TK, et al. CD56+ NK Lymphomas: Clinicopathological Features and Prognosis. Br J Haematol (1997) 97(4):821–9. doi: 10.1046/j.1365-2141.1997.1462962.x
9. Yamaguchi M, Kita K, Miwa H, Nishii K, Oka K, Ohno T, et al. Frequent Expression of P-Glycoprotein/MDR1 by Nasal T-Cell Lymphoma Cells. Cancer (1995) 76(11):2351–6. doi: 10.1002/1097-0142(19951201)76:11<2351::AID-CNCR2820761125>3.0.CO;2-1
10. Kimura H, Ito Y, Kawabe S, Gotoh K, Takahashi Y, Kojima S, et al. EBV-Associated T/NK-Cell Lymphoproliferative Diseases in Nonimmunocompromised Hosts: Prospective Analysis of 108 Cases. Blood (2012) 119(3):673–86. doi: 10.1182/blood-2011-10-381921
11. Yhim HY, Kim JS, Mun YC, Moon JH, Chae YS, Park Y, et al. Clinical Outcomes and Prognostic Factors of Up-Front Autologous Stem Cell Transplantation in Patients With Extranodal Natural Killer/T Cell Lymphoma. Biol Blood Marrow Transplant (2015) 21(9):1597–604. doi: 10.1016/j.bbmt.2015.05.003
12. Abouyabis AN, Shenoy PJ, Lechowicz MJ, Flowers CR. Incidence and Outcomes of the Peripheral T-Cell Lymphoma Subtypes in the United States. Leuk Lymphoma (2008) 49(11):2099–107. doi: 10.1080/10428190802455867
13. Li YX, Yao B, Jin J, Wang WH, Liu YP, Song YW, et al. Radiotherapy as Primary Treatment for Stage IE and IIE Nasal Natural Killer/T-Cell Lymphoma. J Clin Oncol (2006) 24(1):181–9. doi: 10.1200/JCO.2005.03.2573
14. Au WY, Weisenburger DD, Intragumtornchai T, Nakamura S, Kim WS, Sng I, et al. Clinical Differences Between Nasal and Extranasal Natural Killer/T-Cell Lymphoma: A Study of 136 Cases From the International Peripheral T-Cell Lymphoma Project. Blood (2009) 113(17):3931–7. doi: 10.1182/blood-2008-10-185256
15. Wang ZY, Li YX, Wang WH, Jin J, Wang H, Song YW, et al. Primary Radiotherapy Showed Favorable Outcome in Treating Extranodal Nasal-Type NK/T-Cell Lymphoma in Children and Adolescents. Blood (2009) 114(23):4771–6. doi: 10.1182/blood-2009-07-235853
16. Kim SJ, Kim K, Kim BS, Kim CY, Suh C, Huh J, et al. Phase II Trial of Concurrent Radiation and Weekly Cisplatin Followed by VIPD Chemotherapy in Newly Diagnosed, Stage IE to IIE, Nasal, Extranodal NK/T-Cell Lymphoma: Consortium for Improving Survival of Lymphoma Study. J Clin Oncol (2009) 27(35):6027–32. doi: 10.1200/JCO.2009.23.8592
17. Yamaguchi M, Tobinai K, Oguchi M, Ishizuka N, Kobayashi Y, Isobe Y, et al. Phase I/II Study of Concurrent Chemoradiotherapy for Localized Nasal Natural Killer/T-Cell Lymphoma: Japan Clinical Oncology Group Study Jcog0211. J Clin Oncol (2009) 27(33):5594–600. doi: 10.1200/JCO.2009.23.8295
18. Yang Y, Zhu Y, Cao JZ, Zhang YJ, Xu LM, Yuan ZY, et al. Risk-Adapted Therapy for Early-Stage Extranodal Nasal-Type NK/T-Cell Lymphoma: Analysis From a Multicenter Study. Blood (2015) 126(12):1424–32; quiz 517. doi: 10.1182/blood-2015-04-639336
19. Vargo JA, Patel A, Glaser SM, Balasubramani GK, Farah RJ, Marks SM, et al. The Impact of the Omission or Inadequate Dosing of Radiotherapy in Extranodal Natural Killer T-Cell Lymphoma, Nasal Type, in the United States. Cancer (2017) 123(16):3176–85. doi: 10.1002/cncr.30697
20. Sakata K, Fuwa N, Kodaira T, Aratani K, Ikeda H, Takagi M, et al. Analyses of Dose-Response in Radiotherapy for Patients With Mature T/NK-Cell Lymphomas According to the WHO Classification. Radiother Oncol (2006) 79(2):179–84. doi: 10.1016/j.radonc.2006.03.014
21. You JY, Chi KH, Yang MH, Chen CC, Ho CH, Chau WK, et al. Radiation Therapy Versus Chemotherapy as Initial Treatment for Localized Nasal Natural Killer (NK)/T-Cell Lymphoma: A Single Institute Survey in Taiwan. Ann Oncol (2004) 15(4):618–25. doi: 10.1093/annonc/mdh143
22. Kim K, Chie EK, Kim CW, Kim IH, Park CI. Treatment Outcome of Angiocentric T-Cell and NK/T-Cell Lymphoma, Nasal Type: Radiotherapy Versus Chemoradiotherapy. Jpn J Clin Oncol (2005) 35(1):1–5. doi: 10.1093/jjco/hyi006
23. Huang MJ, Jiang Y, Liu WP, Li ZP, Li M, Zhou L, et al. Early or Up-Front Radiotherapy Improved Survival of Localized Extranodal NK/T-Cell Lymphoma, Nasal-Type in the Upper Aerodigestive Tract. Int J Radiat Oncol Biol Phys (2008) 70(1):166–74. doi: 10.1016/j.ijrobp.2007.05.073
24. Ribrag V, Ell Hajj M, Janot F, Girinsky T, Domenge C, Schwaab G, et al. Early Locoregional High-Dose Radiotherapy Is Associated With Long-Term Disease Control in Localized Primary Angiocentric Lymphoma of the Nose and Nasopharynx. Leukemia (2001) 15(7):1123–6. doi: 10.1038/sj.leu.2402148
25. Cheung MM, Chan JK, Lau WH, Ngan RK, Foo WW. Early Stage Nasal NK/T-Cell Lymphoma: Clinical Outcome, Prognostic Factors, and the Effect of Treatment Modality. Int J Radiat Oncol Biol Phys (2002) 54(1):182–90. doi: 10.1016/S0360-3016(02)02916-4
26. Kim GE, Lee SW, Chang SK, Park HC, Pyo HR, Kim JH, et al. Combined Chemotherapy and Radiation Versus Radiation Alone in the Management of Localized Angiocentric Lymphoma of the Head and Neck. Radiother Oncol (2001) 61(3):261–9. doi: 10.1016/S0167-8140(01)00428-5
27. Yamaguchi M, Suzuki R, Oguchi M. Advances in the Treatment of Extranodal NK/T-Cell Lymphoma, Nasal Type. Blood (2018) 131(23):2528–40. doi: 10.1182/blood-2017-12-791418
28. Hu S, Zhou D, Zhang W. The Optimal Timing of Radiotherapy in the Combined Modality Therapy for Limited-Stage Extranodal NK/T Cell Lymphoma (ENKTL): A Systematic Review and Meta-Analysis. Ann Hematol (2018) 97(12):2279–87. doi: 10.1007/s00277-018-3479-2
29. Yamaguchi M, Tobinai K, Oguchi M, Ishizuka N, Kobayashi Y, Isobe Y, et al. Concurrent Chemoradiotherapy for Localized Nasal Natural Killer/T-Cell Lymphoma: An Updated Analysis of the Japan Clinical Oncology Group Study JCOG0211. J Clin Oncol (2012) 30(32):4044–6. doi: 10.1200/JCO.2012.45.6541
30. Michot JM, Mazeron R, Danu A, Lazarovici J, Ghez D, Antosikova A, et al. Concurrent Etoposide, Steroid, High-Dose Ara-C and Platinum Chemotherapy With Radiation Therapy in Localised Extranodal Natural Killer (NK)/T-Cell Lymphoma, Nasal Type. Eur J Cancer (2015) 51(16):2386–95. doi: 10.1016/j.ejca.2015.07.009
31. Kim SJ, Yang DH, Kim JS, Kwak JY, Eom HS, Hong DS, et al. Concurrent Chemoradiotherapy Followed by L-Asparaginase-Containing Chemotherapy, VIDL, for Localized Nasal Extranodal NK/T Cell Lymphoma: CISL08-01 Phase II Study. Ann Hematol (2014) 93(11):1895–901. doi: 10.1007/s00277-014-2137-6
32. Yoon DH, Kim SJ, Jeong SH, Shin DY, Bae SH, Hong J, et al. Phase II Trial of Concurrent Chemoradiotherapy With L-Asparaginase and MIDLE Chemotherapy for Newly Diagnosed Stage I/II Extranodal NK/T-Cell Lymphoma, Nasal Type (CISL-1008). Oncotarget (2016) 7(51):85584–91. doi: 10.18632/oncotarget.11319
33. Kwong YL, Kim WS, Lim ST, Kim SJ, Tang T, Tse E, et al. SMILE for Natural Killer/T-Cell Lymphoma: Analysis of Safety and Efficacy From the Asia Lymphoma Study Group. Blood (2012) 120(15):2973–80. doi: 10.1182/blood-2012-05-431460
34. Wang L, Wang ZH, Chen XQ, Li YJ, Wang KF, Xia YF, et al. First-Line Combination of Gemcitabine, Oxaliplatin, and L-Asparaginase (GELOX) Followed by Involved-Field Radiation Therapy for Patients With Stage IE/IIE Extranodal Natural Killer/T-Cell Lymphoma. Cancer (2013) 119(2):348–55. doi: 10.1002/cncr.27752
35. Wang L, Wang ZH, Chen XQ, Wang KF, Huang HQ, Xia ZJ. First-Line Combination of GELOX Followed by Radiation Therapy for Patients With Stage IE/IIE ENKTL: An Updated Analysis With Long-Term Follow-Up. Oncol Lett (2015) 10(2):1036–40. doi: 10.3892/ol.2015.3327
36. Bi XW, Xia Y, Zhang WW, Sun P, Liu PP, Wang Y, et al. Radiotherapy and PGEMOX/GELOX Regimen Improved Prognosis in Elderly Patients With Early-Stage Extranodal NK/T-Cell Lymphoma. Ann Hematol (2015) 94(9):1525–33. doi: 10.1007/s00277-015-2395-y
37. Li JW, Li YJ, Zhong MZ, Liu XL, Li J, Li KL, et al. Efficacy and Tolerance of GELOXD/P-GEMOXD in Newly Diagnosed Nasal-Type Extranodal NK/T-Cell Lymphoma: A Multicenter Retrospective Study. Eur J Haematol (2018) 100(3):247–56. doi: 10.1111/ejh.13004
38. Su S, Moran K, Robar JL. Design and Production of 3D Printed Bolus for Electron Radiation Therapy. J Appl Clin Med Phys (2014) 15(4):4831. doi: 10.1120/jacmp.v15i4.4831
39. Canters RA, Lips IM, Wendling M, Kusters M, van Zeeland M, Gerritsen RM, et al. Clinical Implementation of 3D Printing in the Construction of Patient Specific Bolus for Electron Beam Radiotherapy for Non-Melanoma Skin Cancer. Radiother Oncol (2016) 121(1):148–53. doi: 10.1016/j.radonc.2016.07.011
40. Kong Y, Yan T, Sun Y, Qian J, Zhou G, Cai S, et al. A Dosimetric Study on the Use of 3D-Printed Customized Boluses in Photon Therapy: A Hydrogel and Silica Gel Study. J Appl Clin Med Phys (2019) 20(1):348–55. doi: 10.1002/acm2.12489
41. Kim SJ, Yoon DH, Jaccard A, Chng WJ, Lim ST, Hong H, et al. A Prognostic Index for Natural Killer Cell Lymphoma After Non-Anthracycline-Based Treatment: A Multicentre, Retrospective Analysis. Lancet Oncol (2016) 17(3):389–400. doi: 10.1016/S1470-2045(15)00533-1
42. Suzuki R, Nakamura S, Suzumiya J, Ichimura K, Ichikawa M, Ogata K, et al. Blastic Natural Killer Cell Lymphoma/Leukemia (CD56-Positive Blastic Tumor): Prognostication and Categorization According to Anatomic Sites of Involvement. Cancer (2005) 104(5):1022–31. doi: 10.1002/cncr.21268
43. Kharfan-Dabaja MA, Kumar A, Ayala E, Hamadani M, Reimer P, Gisselbrecht C, et al. Clinical Practice Recommendations on Indication and Timing of Hematopoietic Cell Transplantation in Mature T Cell and NK/T Cell Lymphomas: An International Collaborative Effort on Behalf of the Guidelines Committee of the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant (2017) 23(11):1826–38. doi: 10.1016/j.bbmt.2017.07.027
44. Yamaguchi M, Suzuki R, Oguchi M, Asano N, Amaki J, Akiba T, et al. Treatments and Outcomes of Patients With Extranodal Natural Killer/T-Cell Lymphoma Diagnosed Between 2000 and 2013: A Cooperative Study in Japan. J Clin Oncol (2017) 35(1):32–9. doi: 10.1200/JCO.2016.68.1619
45. Wang J, Wei L, Ye J, Yang L, Li X, Cong J, et al. Autologous Hematopoietic Stem Cell Transplantation may Improve Long-Term Outcomes in Patients With Newly Diagnosed Extranodal Natural Killer/T-Cell Lymphoma, Nasal Type: A Retrospective Controlled Study in a Single Center. Int J Hematol (2018) 107(1):98–104. doi: 10.1007/s12185-017-2324-z
46. Fox CP, Boumendil A, Schmitz N, Finel H, Luan JJ, Sucak G, et al. High-Dose Therapy and Autologous Stem Cell Transplantation for Extra-Nodal NK/T Lymphoma in Patients From the Western Hemisphere: A Study From the European Society for Blood and Marrow Transplantation. Leuk Lymphoma (2015) 56(12):3295–300. doi: 10.3109/10428194.2015.1037764
47. Jeong SH, Song HN, Park JS, Yang DH, Koh Y, Yoon SS, et al. Allogeneic Stem Cell Transplantation for Patients With Natural Killer/T Cell Lymphoid Malignancy: A Multicenter Analysis Comparing Upfront and Salvage Transplantation. Biol Blood Marrow Transplant (2018) 24(12):2471–8. doi: 10.1016/j.bbmt.2018.07.034
48. Tse E, Chan TS, Koh LP, Chng WJ, Kim WS, Tang T, et al. Allogeneic Haematopoietic SCT for Natural Killer/T-Cell Lymphoma: A Multicentre Analysis From the Asia Lymphoma Study Group. Bone Marrow Transplant (2014) 49(7):902–6. doi: 10.1038/bmt.2014.65
49. Novelli S, Bento L, Garcia I, Prieto L, López L, Gutierrez G, et al. Allogeneic Stem Cell Transplantation in Mature T Cell and Natural Killer/T Neoplasias: A Registry Study From Spanish GETH/GELTAMO Centers. Transplant Cell Ther (2021) 27(6):493.e1–.e8. doi: 10.1016/j.jtct.2021.03.014
Keywords: extranodal natural killer/t cell lymphoma, autologous hematopoietic stem cell transplantation, allogenic hematopoietic stem cell transplantation, radiotherapy, chemo radiotherapy
Citation: Terro K, Sharrouf L and El Cheikh J (2022) Progress of Hematopoietic Stem Cell Transplantation and Radiotherapy in the Treatment of Extranodal NK/T Cell Lymphoma. Front. Oncol. 12:832428. doi: 10.3389/fonc.2022.832428
Received: 09 December 2021; Accepted: 25 January 2022;
Published: 16 February 2022.
Edited by:
Onder Alpdogan, Thomas Jefferson University, United StatesReviewed by:
Govind Babu Kanakasetty, HCG Cancer Hospital, IndiaCopyright © 2022 Terro, Sharrouf and El Cheikh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean El Cheikh, amU0NkBhdWIuZWR1Lmxi
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.