
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 16 January 2023
Sec. Radiation Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1092875
This article is part of the Research Topic Stereotactic Body Radiotherapy for Lung Cancer View all 7 articles
 Rodolfo Chicas-Sett1*
Rodolfo Chicas-Sett1* Juan Castilla Martinez1Abrahan Hernández Blanquisett2Juan Zafra3,4,5Jorge Pastor-Peidro1
Juan Castilla Martinez1Abrahan Hernández Blanquisett2Juan Zafra3,4,5Jorge Pastor-Peidro1The advent of targeted therapy has transformed the treatment paradigm and survival of patients with metastatic non-small cell lung cancer (NSCLC) with driver mutations. The development of acquired resistances during treatment with tyrosine kinase inhibitors (TKIs) impedes a prolonged survival in many patients. This fact is leading to the use of locally ablative therapies such as stereotactic ablative radiotherapy (SABR) to counter these resistances. SABR is a non-invasive treatment that can be delivered in multiple locations and has already proven effective in oligometastatic disease. Clinical evidence suggests that the combination of SABR with TKIs prolongs progression-free survival (PFS) in metastatic NSCLC patients with mutations in epidermal growth factor receptor (EGFR), with international guidelines recommending their use in unfavorable scenarios such as oligoprogressive disease. In this publication, we have reviewed the available evidence on EGFR-TKIs resistance mechanisms and the combination of SABR with TKI in metastatic NSCLC with EGFR mutations. We also describe the utility and clinical recommendations of this combination in oligometastatic and oligoprogressive disease.
Historically, stage IV non-small cell lung cancer (NSCLC) has been considered an incurable disease, only candidate for palliative treatments. Chemotherapy (CT), the standard treatment, offered survival rates of less than a year (1). More recently, the identification of several genetic variants with a predomination of mutations in the oncogene for epidermal growth factor receptor (EGFR) has transformed the therapeutic landscape in this subset of patients (2–5). Targeted therapy (TT) with tyrosine kinase inhibitors (TKIs) has reported median overall survivals (OS) of 22-36 months in patients with an EGFR mutation (6). However, the onset of primary and acquired resistances continue to be the main obstacle to further improve these results (7). The main example is the T790M mutation, which is responsible for 60% of TKI resistance in this setting (8). Moreover, third-generation TKIs are also affected by the C797S mutation, causing resistance in 10-26% of patients receiving osimertinib as second-line and 7% when used as first-line (9).
Stereotactic ablative radiotherapy (SABR) is an effective treatment for oligometastatic disease (10). Recently, several studies have reported results on its promising combination with immunotherapy and TT (11–13). Various clinical guidelines recommend the use of SABR in oligometastatic or oligoprogressive patients with driver mutations (14). This has garnered a special interest in the potentially decisive role of SABR in the eradication tumor clones that are resistant to systemic therapy by extending clinical benefit. In this review, we aim to present the clinical data that justify the use of SABR as a therapeutic agent that may counteract the resistance to EGFR-TKI in patients with metastatic NSCLC.
EGFR mutations occur in 12% of NSCLC cases, although Asian patients have a higher prevalence at 47% (15). The majority of these patients have no prior history of smoking, and the most common activating mutations are deletions in exon 19 and the L858R point mutation in exon 20.
Currently, EGFR testing is recommended for all patients with stage IB-IV adenocarcinoma-type NSCLC and stage IV squamous cell carcinoma. EGFR inhibitors are the preferred treatment for NSCLC patients with somatic EGFR mutations. Those stage IB-IIIA EGFR+ patients initially treated with surgery and achieving a complete resection (R0) may benefit from adjuvant treatment with osimertinib 80 mg daily for 3 years following the results of the phase 3 ADAURA trial, which showed a substantial benefit in terms of disease-free survival. This benefit was most evident in stage IIIA patients. In this group, at 24 months, 88% of patients treated with adjuvant osimertinib were alive and disease-free compared to 32% in the placebo group. This trial reported that osimertinib had an acceptable safety profile with serious adverse events occurring in 16% of patients versus 13% in the placebo group (16).
Stage IV disease remains incurable, but EGFR inhibitors have shown consistent clinical and statistically significant benefits for the EGFR+ population compared with standard CT. Erlotinib, gefitinib, afatinib, dacomitinib and osimertinib are effective as monotherapy, while combination regimens such as erlotinib plus ramucirumab or erlotinib plus bevacizumab have emerged as alternative treatments for selected patients (17–23). Subsequently, the FLAURA trial has reported better results for osimertinib compared to gefitinib or erlotinib in terms of PFS and OS (21). It should be noted that these EGFR inhibitors are also effective in patients with less common EGFR mutations, such as S7681, L861Q and G719X, because these mutations are also sensitive to these treatments (24). However, recent real-world data suggest that osimertinib has better outcomes in patients with common EGFR mutations compared to patients harboring these rare mutations (25).
Ultimately, there is strong evidence from phase 3 randomized trials to support the use of EGFR inhibitors as first-line treatment for stage IV disease, and as adjuvant treatment after complete resection for stage IB-IIIA, being osimertinib the currently preferred option. Questions about the best regimen after failure to osimertinib in both settings warrant future research.
Although EGFR inhibitors have represented a turning point in the treatment of EGFR-mutated lung cancer, most stage IV patients will suffer from disease progression and eventually die from it. Lung cancer is a heterogeneous disease and sensitivity to treatment is not the same for all EGFR mutations. The best example is EGFR exon 20 insertion mutations, as most variants do not respond to EGFR inhibitors. Amivantamab (a bispecific EGFR-MET) and mobocertinib (an irreversible kinase inhibitor), are under investigation for these patients. Both have shown promising results in recent trial and expected to the widely available in the future (26, 27).
On the other hand, many patients who initially respond to EGFR inhibitors will develop secondary resistances through different mechanisms. The first-generation drugs erlotinib and gefitinib are reversible inhibitors, while second and third generation agatinib, dacomitinib and osimertinib are irreversible inhibitors. For first and second-generation inhibitors most cases will develop a new mutation in EGFR, the most frequent being T790M. This mutation produces a biochemical change in the ATP levels required to achieve a half-maximal reaction rate, ultimately resulting in a sensitivity to inhibitors which is similarly low as in EGFR wild–type (28). Osimertinib provides clinical and statistical benefit for patients who develop this resistance and is the preferred option for this subgroup (29). Another resistance mechanism called “bypass” is based on alternative molecular pathways that activate proliferation and survival independent of EGFR activation, the most frequent being the amplification of the ERBB2 and MET genes. Mutations in other genes such as BRAF, PIK3CA, KRAS, PTEN, NF-1 have also been described but are less frequent (28). Ongoing trials are testing several drugs (capmatinib, sotarasib, trastuzumab-deruxtecan and trastuzumab-emtasine) that are already used in clinical practice as a second line option for lung cancer and their benefit is not limited to the population with EGFR mutation (29–33).
A great challenge for oncologists nowadays is the acquired resistance to the third-generation inhibitor Osimertinib. The mutation in C797S is the most frequent in this context and most patients retain the T790M mutation after progression (6). There is currently no consensus on the standard treatment after failure to osimertinib. Rebiopsy is recommended at the time of relapse, either in tissue or liquid biopsy. Combinations of immunotherapy with CT, antiangiogenic agents or combinations of TT can be employed, with no choice being clearly superior. Clinical trials will hopefully establish the standard therapy for these progressing patients in the coming years.
The standard treatment for patients with metastatic NSCLC is systemic therapy based on CT and/or immunotherapy. In the case of NSCLC with driver mutations, TT is the treatment of choice. However, although improved from only CT regimes, median survival is still limited. When analyzing the relapse patterns of these patients, most recurrences occur at the same sites of the initial metastatic disease. Considering this fact, the addition of SABR in oligometastatic patients or those with low tumor burden with ECOG ≤2 could improve PFS and OS (34).
Even though no phase III trials that validate these results have been published, the use of SABR in clinical practice is increasing, with even international guidelines such as the National Comprehensive Cancer Network (NCCN) recommending the addition of ablative therapy in de novo oligometastatic patients to try to improve survival and in oligoprogressive disease to prolong the benefit of systemic therapy (35).
These recommendations are based on the results of different retrospective and prospective studies. As for retrospective data, a meta-analysis published in 2014 including 757 oligometastatic patients (1-5 lesions but 96.5% ≤2 metastases) treated with local therapy (surgery +/- radiotherapy/SABR). Median PFS was 11 months, with a two-year PFS of 25%. Furthermore, Median OS was 26 months and two-year OS was 51.1%. These are relevant numbers, especially considering that CT was part of the first-line treatment in only 17.7% of cases (36). A more recent meta-analysis of 693 NSCLC patients (78% oligometastatic) compared local consolidative treatment (surgery or radiotherapy) vs systemic therapy. In the oligometastatic subgroup, hazard ratio (HR) for PFS was 0.30 (p<0.001) and 0.41 (p<0.001) for OS, which shows the benefit of local therapy in these patients (37).
Moreover, several phase II studies have presented results that further show the effectivity of SABR in oligometastatic NSCLC:
● A phase II study conducted in Belgium analyzed 26 patients with ≤5 metastases diagnosed by positron emission tomography (PET) receiving CT, or SABR (5 Gy in 10 fractions) in patients who were not candidates for CT. Seventy five percent of patients presented synchronous oligometastases. With a median follow-up of 16.4 months, median PFS was 11.2 months and 1-year PFS was 45%. In terms of OS, median was 23 months and 67% at one year. Local failure in the irradiated sites was only 15% (38).
● Iyengar et al. published in 2017 a single-institution cohort of patients with ≤6 metastases (including the primary tumor) treated with at 4-6 cycles of CT and who were not treatable with TT for driver mutations. Patients who did not progress after CT were randomized to SABR plus maintenance CT vs CT alone. After 29 patients and a median follow-up of 9.6 months, the study was closed due to the interim analysis showing positive results, with a median PFS of 9.6 months in the SABR group vs 3.5 months in the control group (p=0.01) (13).
● The OLIGOMEZ study (2019) is a multicenter randomized study of patients with up to three metastases (>90% synchronous) after induction systemic therapy (CT or TT in case of EGFR or ALK+). Forty-nine patients which did not progress after systemic therapy were randomized to receive local therapy (surgery and/or radiotherapy/SABR) or maintenance systemic therapy (17% received no treatment in this arm). After a median follow-up of 38.8 months, median PFS was 14.2 months in the local treatment group vs 4.4 months in the control group (p=0.022). Median OS was also significantly better in the experimental arm (41.2 months vs 18.9, p=0.017). An interesting endpoint analyzed in the study was the time until the diagnoses of new lesions, which showed a non-statistically significant tendency in favor of the local treatment group (14.2 vs 6 months). This could suggest that local treatment could even limit the dissemination potential of the disease (12, 13, 39).
● The final results of the SABR-COMET trial were published in 2020. This study included 99 patients with different primary tumors (18 patients had lung cancer) and with 1-5 metastases (93 ≤3 lesions) that were randomized 2:1 to receive SABR plus best palliative treatment vs palliative treatment alone). With a median follow-up of 51 months, median PFS was 11.6 months with SABR vs 5.4 in the control arm (p=0.001), and four-year PFS was 21.6% vs 3.2%. A favorable impact of SABR was also reported in terms of OS, with a median of 50 months vs 28 months. After excluding prostate cancer from the analysis, OS remained better for SABR (five-year OS 33.1% vs 16.2%, p=0.085) (10). In 2022, updated results have been published with a median follow-up of 5.7 years. Eight-year PFS was 21.3% in the SABR arm vs 0% in the control arm (p<0.001). The positive impact of SABR was also observed in eight-year OS: 27.2% vs 13.6% (p=0.008). These recent data supports the durability of the effect of SABR (34).
In terms of toxicity, all these studies confirm that SABR is a safe approach. Recently, a phase II multicenter study has analyzed toxicity in 381 patients treated with SABR, reporting grade ≥3 toxicity of 4% and grade ≥2 of 8% (40).
All the studies above justify the use of SABR in oligometastatic patients (≤5) with ECOG ≤2 that do not progress to systemic therapy. However, it must be noted that these are studies with few patients, with a heterogeneous systemic therapy and none of them include the use of immunotherapy, which currently has a key role in these patients. We are awaiting the results of phase III studies in oligometastatic NSCLC such as NRG-LU-002 (NCT03137771), SARON (NCT02417662), and SABR-COMET 3 (NCT03862911) and 10 (NCT03721341). Many of these are aiming to demonstrate the benefit in OS of the addition of SABR to systemic therapy. Moreover, the OMEGA (NCT03827577) study is comparing locally ablative treatment vs conventional systemic therapy (41).
Given these results, and while ongoing studies report their data, SABR may be recommended in oligometastatic patients (with up to 3-5 metastases) with ECOG ≤2 that do not progress to initial systemic therapy. The ESTRO-ASTRO consensus also adds that size is not a limiting factor and that, in fact, larger lesions can be treated with adequate constraints (42).
The biological effect of SABR differs from conventional radiotherapy. SABR unleashes additional microvascular damage through the activation of different cellular pathways, producing a higher rate of tumor cell death (43). Several studies have reported that the combination of SABR and TKIs could have a synergistic effect. This could be justified by the following ideas: a) EGFR-mutated patients present a higher sensitivity to radiation (44), b) TKIs inhibit DNA repair (45), c) there is a reduction in T790M mutations after irradiation (46).
EGFR+ patients tend to suffer from disease progression 1-2 years after the star of TKIs. In fact, 60% develop acquired resistance explained by the T790M mutation T790M (18, 20, 47), and 70% in the form of oligoprogression (48). Yajing Wu et al. found it a recent meta-analysis that adding local therapy to systemic treatment improves PFS and OS with no increase in grade ≥3 toxicity (37). These reasons have led to the considering SABR as a tool that may revert these resistances with the following objectives:
-Lower/maintain disease burden.
-Delay disease progression.
-Extend the duration of clinical Benefit from TKIs, mainly in the oligometastatic scenario (oligorrecurrence, oligopersistence and oligoprogression).
-Local control of symptomatic lesions.
Prospective studies evaluating the combination of SABR and TKIs are limited and focus on more unfavorable scenarios such as oligoprogressive disease. While most evidence comes from retrospective data, results are similar to those reported in controlled studies, showing a positive impact on PFS (Table 1). At present, clinical guidelines like the ones by NCCN recommend SABR in oligoprogressive EGFR+ NSCLC patients (35).
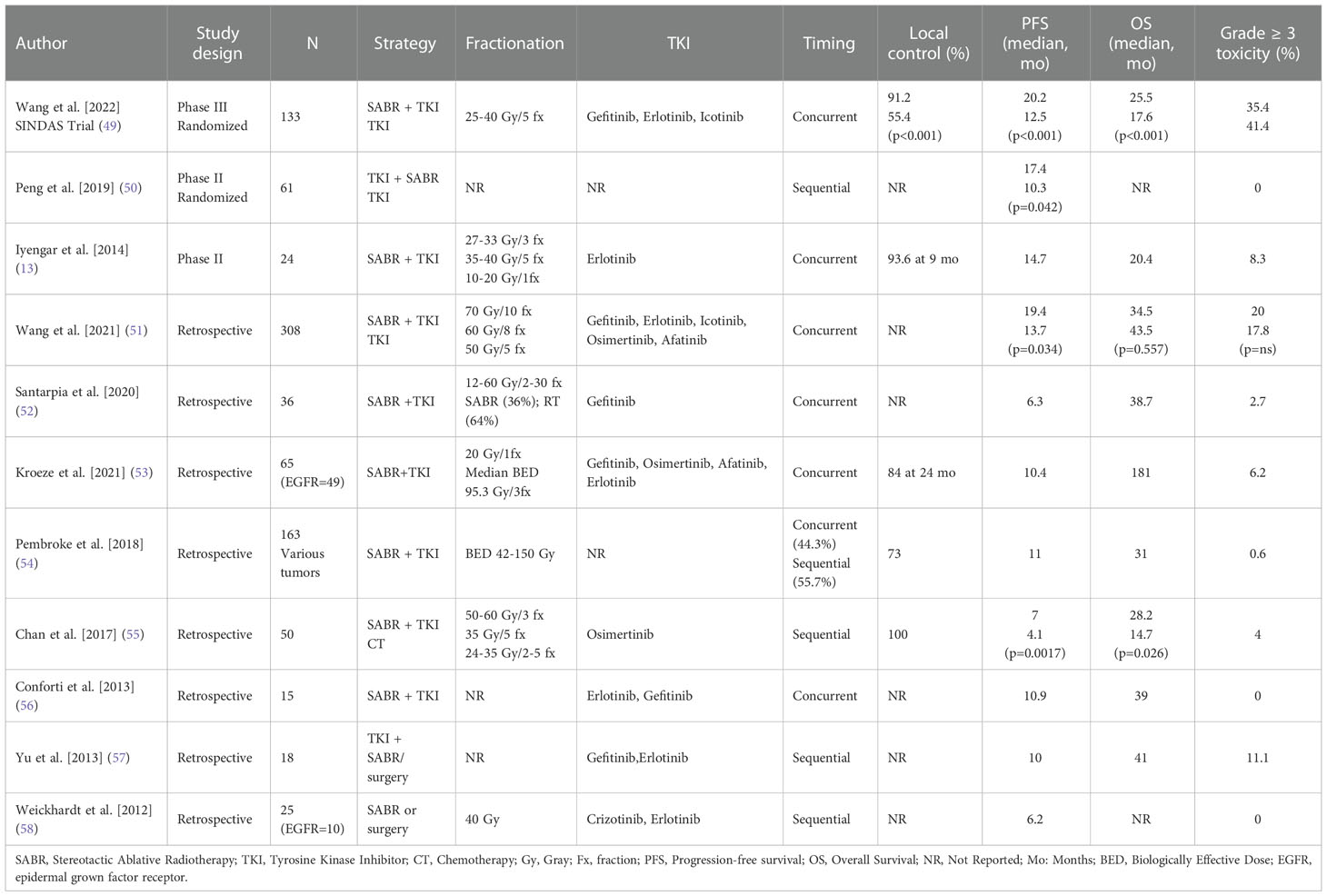
Table 1 Selected studies of SABR and TKIs combination in metastatic NSCLC EGFR-mutated patients.
The study by Weickhardt et al. was one of the first to evaluate the use of SABR to mitigate the resistance to TKIs. Of 65 patients included, 27 presented EGFR mutation and were in progression to TKIs. Despite the limited size sample, there was a benefit in PFS for patients who received SABR and maintained the line of TKIs (58). Further retrospective studies have also reported a tendency towards better PFS for patients treated with SABR, ranging from 6.2 to 19.4 months (Table 1). In the context of oligoprogression, maintaining TKIs after SABR has shown better PFS (7 vs 4.1 months) and OS (28.2 vs 14.7 months) compared to CT (55).
Although most studies included oligometastatic patients (up to 5 lesions), Kroeze et al. did actually assess polymetastatic patients. This study in particular found a promising PFS of 10.4 months despite 75% of patients presenting brain metastases (53).
The upfront combination of SABR with TKIs at the start of therapy was evaluated by Iyengar et al. in a phase II trial (13). This study found a PFS of 14.7 months and OS of 20.4 months. A posterior phase II randomized study found a PFS of 17.4 vs 10.3 months in the systemic therapy alone group (50). Finally, the phase III SINDAS trial included 133 oligometastatic EGFR+ patients treated with upfront SABR plus TKI vs TKI alone. A statistically significant benefit was observed in the combination group, with an OS of 25.5 months vs 17.4 months (p<0.001) (49).
Generally, the combination of SABR and TKIs has reported safe outcomes. Randomized studies such as SINDAS found no significant different in grade ≥3 toxicity between the combination and TKI alone (49). Table 1 shows that grade ≥3 side effects are acceptable in most studies. However, liver SABR and treatment with sorafenib has reported a high risk of gastrointestinal toxicity (59). The combination of osimertinib and thoracic radiotherapy has reported a potential increase in pulmonary toxicity. Nonetheless, these data come from retrospective studies with small cohorts, and percentages are similar to those of CRT-induced pneumonitis (60).
In terms of the treatment sequence, there is no clear consensus on whether the combination should be administered concurrently or if TKI should be interrupted during SABR. Studies that have administered this combination concurrently have not reported high grade ≥3 toxicities (0-11%) (13, 47). However, more data are needed to establish the most adequate approach.
The optimal dose and fractionation of SABR when combined with TKIs is still unknown. Although the studies in Table 1 are very heterogeneous, doses have generally followed recommendations for definitive treatments with SABR alone, trying to reach biologically equivalent doses (BED) ≥ 100 Gy.
Ongoing clinical trials are aiming to confirm the data reported up to this point. In oligoprogression to TKIs, the phase II/III HALT trial (NCT03256981) will include an experimental arm in which patients will receive SABR to up to three extracranial sites while continuing TKI. In an earlier scenario, the randomized NORTHSTAR trial (NCT03410043) will evaluate if the combination of SABR plus osimertinib is better than osimetinib alone in stage IIIB/IV EGFR+ NSCLC as first-line therapy.
A pending challenge to overcome is the incorporation of translational aspects into clinical practice through novel biomarkers. Detection of circulating DNA can predict treatment response, but also detect possible resistances (61). The use of these blood biomarkers in clinical trials combining SABR and TKIs could be promising as their implementation into clinical practice would be easily accessible.
SABR is a safe and effective approach for the treatment of oligometastatic NSCLC. Moreover, it can be used in multiple locations and does not require the interruption of systemic therapy. Acquired resistance to TKIs is a challenging scenario in which the use of SABR has reported very promising results at overcoming the resistance mechanisms to TKIs in metastatic NSCLC. Although evidence remains limited, clinical benefit has outweighed the risks mainly in oligoprogresive disease. In this setting, TKIs maintenance after successful SABR has prolonged PFS and, in some cases, OS. The combination has also reported an effective role as first line, although the best strategy is still unknown and warrants further research.
RC-S- Conception and design, collection of data, data analysis and interpretation, manuscript writing, final approval of manuscript JCM- Conception and design, collection of data, manuscript writing, final approval of manuscript JZ- Conception and design, data analysis and interpretation, manuscript writing, final approval of manuscript AH- Conception and design, collection of data, manuscript writing, final approval of manuscript JP-P - Conception and design, collection of data, manuscript writing, final approval of manuscript. All authors contributed to the article and approved the submitted version.
The present work was supported by ASCIRES GRUPO BIOMEDICO.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Besse B, Adjei A, Baas P, Meldgaard P, Nicolson M, Paz-Ares L, et al. 2nd ESMO consensus conference on lung cancer: non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann Oncol (2014) 25(8):1475–84. doi: 10.1093/annonc/mdu123
2. Chan BA, Hughes BG. Targeted therapy for non-small cell lung cancer: Current standards and the promise of the future. Transl Lung Cancer Res (2015) 4(1):36–54. doi: 10.3978/j.issn.2218-6751.2014.05.01
3. Dogan S, Shen R, Ang DC, Johnson ML, D'Angelo SP, Paik PK, et al. Molecular epidemiology of EGFR and KRAS mutations in 3,026 lung adenocarcinomas: higher susceptibility of women to smoking-related KRAS-mutant cancers. Clin Cancer Res (2012) 18(22):6169–77. doi: 10.1158/1078-0432.CCR-11-3265
4. Girard N, Sima CS, Jackman DM, Sequist LV, Chen H, Yang JC, et al. Nomogram to predict the presence of EGFR activating mutation in lung adenocarcinoma. Eur Respir J (2012) 39(2):366–72. doi: 10.1183/09031936.00010111
5. Munfus-McCray D, Harada S, Adams C, Askin F, Clark D, Gabrielson E, et al. EGFR and KRAS mutations in metastatic lung adenocarcinomas. Hum Pathol (2011) 42(10):1447–53. doi: 10.1016/j.humpath.2010.12.011
6. Leonetti A, Sharma S, Minari R, Perego P, Giovannetti E, Tiseo M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br J Cancer. (2019) 121(9):725–37. doi: 10.1038/s41416-019-0573-8
7. Johnson M, Garassino MC, Mok T, Mitsudomi T. Treatment strategies and outcomes for patients with EGFR-mutant non-small cell lung cancer resistant to EGFR tyrosine kinase inhibitors: Focus on novel therapies. Lung Cancer. (2022) 170:41–51. doi: 10.1016/j.lungcan.2022.05.011
8. O'Kane GM, Barnes TA, Leighl NB. Resistance to epidermal growth factor receptor tyrosine kinase inhibitors, T790M, and clinical trials. Curr Oncol (2018) 25(Suppl 1):S28–37. doi: 10.3747/co.25.3796
9. Chen JA, Riess JW. Advances in targeting acquired resistance mechanisms to epidermal growth factor receptor tyrosine kinase inhibitors. J Thorac Dis (2020) 12(5):2859–76. doi: 10.21037/jtd.2019.08.32
10. Palma DA, Olson R, Harrow S, Gaede S, Louie AV, Haasbeek C, et al. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: Long-term results of the SABR-COMET phase II randomized trial. J Clin Oncol (2020) 38(25):2830–8. doi: 10.1200/JCO.20.00818
11. Chicas-Sett R, Zafra J, Rodriguez-Abreu D, Castilla-Martinez J, Benitez G, Salas B, et al. Combination of SABR with anti-PD-1 in oligoprogressive non-small cell lung cancer and melanoma: Results of a prospective multicenter observational study. Int J Radiat Oncol Biol Phys (2022) 114(4):655–65. doi: 10.1016/j.ijrobp.2022.05.013
12. Gomez DR, Tang C, Zhang J, Blumenschein GR Jr., Hernandez M, Lee JJ, et al. Local consolidative therapy vs. maintenance therapy or observation for patients with oligometastatic non-Small-Cell lung cancer: Long-term results of a multi-institutional, phase II, randomized study. J Clin Oncol (2019) 37(18):1558–65. doi: 10.1200/JCO.19.00201
13. Iyengar P, Wardak Z, Gerber DE, Tumati V, Ahn C, Hughes RS, et al. Consolidative radiotherapy for limited metastatic non-Small-Cell lung cancer: A phase 2 randomized clinical trial. JAMA Oncol (2018) 4(1):e173501. doi: 10.1001/jamaoncol.2017.3501
14. Planchard D, Popat S, Kerr K, Novello S, Smit EF, Faivre-Finn C, et al. Metastatic non-small cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29(Suppl 4):iv192–237. doi: 10.1093/annonc/mdy275
15. Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am J Cancer Res (2015) 5(9):2892–911.
16. Wu YL, Tsuboi M, He J, John T, Grohe C, Majem M, et al. Osimertinib in resected EGFR-mutated non-Small-Cell lung cancer. N Engl J Med (2020) 383(18):1711–23. doi: 10.1056/NEJMoa2027071
17. Kawashima Y, Fukuhara T, Saito H, Furuya N, Watanabe K, Sugawara S, et al. Bevacizumab plus erlotinib versus erlotinib alone in Japanese patients with advanced, metastatic, EGFR-mutant non-small-cell lung cancer (NEJ026): overall survival analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Respir Med (2022) 10(1):72–82. doi: 10.1016/S2213-2600(21)00166-1
18. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med (2009) 361(10):947–57. doi: 10.1056/NEJMoa0810699
19. Nakagawa K, Garon EB, Seto T, Nishio M, Ponce Aix S, Paz-Ares L, et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol (2019) 20(12):1655–69. doi: 10.1016/S1470-2045(19)30634-5
20. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol (2012) 13(3):239–46. doi: 10.1016/S1470-2045(11)70393-X
21. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non-Small-Cell lung cancer. N Engl J Med (2018) 378(2):113–25. doi: 10.1056/NEJMoa1713137
22. Wu YL, Cheng Y, Zhou X, Lee KH, Nakagawa K, Niho S, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol (2017) 18(11):1454–66. doi: 10.1016/S1470-2045(17)30608-3
23. Yang JC, Wu YL, Schuler M, Sebastian M, Popat S, Yamamoto N, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-lung 3 and LUX-lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol (2015) 16(2):141–51. doi: 10.1016/S1470-2045(14)71173-8
24. Cho JH, Lim SH, An HJ, Kim KH, Park KU, Kang EJ, et al. Osimertinib for patients with non-Small-Cell lung cancer harboring uncommon EGFR mutations: A multicenter, open-label, phase II trial (KCSG-LU15-09). J Clin Oncol (2020) 38(5):488–95. doi: 10.1200/JCO.19.00931
25. Bar J, Waleed K, Wolner M, Derijcke S, Girard N, Rottenberg Y, et al. 1206P uncommon EGFR mutations: International case series on efficacy of osimertinib in real-life practice in first-liNe setting (UNICORN). Ann Oncol (2021). doi: 10.1016/j.annonc.2021.08.1811
26. Park K, Haura EB, Leighl NB, Mitchell P, Shu CA, Girard N, et al. Amivantamab in EGFR exon 20 insertion-mutated non-Small-Cell lung cancer progressing on platinum chemotherapy: Initial results from the CHRYSALIS phase I study. J Clin Oncol (2021) 39(30):3391–402. doi: 10.1200/JCO.21.00662
27. Zhou C, Ramalingam SS, Kim TM, Kim SW, Yang JC, Riely GJ, et al. Treatment outcomes and safety of mobocertinib in platinum-pretreated patients with EGFR exon 20 insertion-positive metastatic non-small cell lung cancer: A phase 1/2 open-label nonrandomized clinical trial. JAMA Oncol (2021) 7(12):e214761. doi: 10.1001/jamaoncol.2021.4761
28. Westover D, Zugazagoitia J, Cho BC, Lovly CM, Paz-Ares L. Mechanisms of acquired resistance to first- and second-generation EGFR tyrosine kinase inhibitors. Ann Oncol (2018) 29(suppl_1):i10–i9. doi: 10.1093/annonc/mdx703
29. Mok TS, Wu YL, Ahn MJ, Garassino MC, Kim HR, Ramalingam SS, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med (2017) 376(7):629–40. doi: 10.1056/NEJMoa1612674
30. Li BT, Shen R, Buonocore D, Olah ZT, Ni A, Ginsberg MS, et al. Ado-trastuzumab emtansine for patients with HER2-mutant lung cancers: Results from a phase II basket trial. J Clin Oncol (2018) 36(24):2532–7. doi: 10.1200/JCO.2018.77.9777
31. Li BT, Smit EF, Goto Y, Nakagawa K, Udagawa H, Mazieres J, et al. Trastuzumab deruxtecan in HER2-mutant non-Small-Cell lung cancer. N Engl J Med (2022) 386(3):241–51. doi: 10.1056/NEJMoa2112431
32. Skoulidis F, Li BT, Dy GK, Price TJ, Falchook GS, Wolf J, et al. Sotorasib for lung cancers with KRAS p.G12C mutation. N Engl J Med (2021) 384(25):2371–81. doi: 10.1056/NEJMoa2103695
33. Wolf J, Seto T, Han JY, Reguart N, Garon EB, Groen HJM, et al. Capmatinib in MET exon 14-mutated or MET-amplified non-Small-Cell lung cancer. N Engl J Med (2020) 383(10):944–57. doi: 10.1056/NEJMoa2002787
34. Horrow S, Palma D, Olson R, Gaede S, Louie AV, Haasbeek C, et al. Stereotactic radiation for the comprehensive treatment of oligometastases (SABR-COMET): Extended long-term outcomes. Int J Radiat Oncol Biol Phys (2022) 114(4):611–6. doi: 10.1016/j.ijrobp.2022.05.004
35. Ettinger DS, Wood D, Chair V, Aisner DL, Akerley W, Bauman JR, et al. . NCCN guidelines version 3.2022 non-small cell lung cancer continue NCCN guidelines panel disclosures [Internet] (2022). Available at: https://wwwnccnorg/home/member.
36. Ashworth AB, Senan S, Palma DA, Riquet M, Ahn YC, Ricardi U, et al. An individual patient data metaanalysis of outcomes and prognostic factors after treatment of oligometastatic non-small-cell lung cancer. Clin Lung Cancer. (2014) 15(5):346–55. doi: 10.1016/j.cllc.2014.04.003
37. Wu Y, Verma V, Liang F, Lin Q, Zhou Z, Wang Z, et al. Local consolidative therapy versus systemic therapy alone for metastatic non-small cell lung cancer: A systematic review and meta-analysis. Int J Radiat Oncol Biol Phys (2022) 114(4):635–44. doi: 10.1016/j.ijrobp.2022.02.023
38. Collen C, Christian N, Schallier D, Meysman M, Duchateau M, Storme G, et al. Phase II study of stereotactic body radiotherapy to primary tumor and metastatic locations in oligometastatic nonsmall-cell lung cancer patients. Ann Oncol (2014) 25(10):1954–9. doi: 10.1093/annonc/mdu370
39. Gomez DR, Blumenschein GR Jr., Lee JJ, Hernandez M, Ye R, Camidge DR, et al. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: a multicentre, randomised, controlled, phase 2 study. Lancet Oncol (2016) 17(12):1672–82. doi: 10.1016/S1470-2045(16)30532-0
40. Jasper K, Stiles B, McDonald F, Palma DA. Practical management of oligometastatic non-Small-Cell lung cancer. J Clin Oncol (2022) 40(6):635–41. doi: 10.1200/JCO.21.01719
41. Dohopolski M, Iyengar P. Oligometastatic non-small cell lung cancer: A narrative review of stereotactic ablative radiotherapy. Ann Palliat Med (2021) 10(5):5944–53. doi: 10.21037/apm-20-1409
42. Lievens Y, Guckenberger M, Gomez D, Hoyer M, Iyengar P, Kindts I, et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother Oncol (2020) 148:157–66. doi: 10.1016/j.radonc.2020.04.003
43. Balagamwala EH, Chao ST, Suh JH. Principles of radiobiology of stereotactic radiosurgery and clinical applications in the central nervous system. Technol Cancer Res Treat (2012) 11(1):3–13. doi: 10.7785/tcrt.2012.500229
44. Nakamura M, Kageyama SI, Niho S, Okumura M, Hojo H, Motegi A, et al. Impact of EGFR mutation and ALK translocation on recurrence pattern after definitive chemoradiotherapy for inoperable stage III non-squamous non-small-cell lung cancer. Clin Lung Cancer. (2019) 20(3):e256–e64. doi: 10.1016/j.cllc.2019.02.021
45. Chinnaiyan P, Huang S, Vallabhaneni G, Armstrong E, Varambally S, Tomlins SA, et al. Mechanisms of enhanced radiation response following epidermal growth factor receptor signaling inhibition by erlotinib (Tarceva). Cancer Res (2005) 65(8):3328–35. doi: 10.1158/0008-5472.CAN-04-3547
46. Li J, Wu X, Wang Z, Shen Z, Sun N, Zhu X. [Ionizing radiation reduces TKI resistance caused by T790M mutation in NSCLC cell lines]. Zhongguo Fei Ai Za Zhi. (2015) 18(8):475–80. doi: 10.3779/j.issn.1009-3419.2015.08.02
47. Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res (2013) 19(8):2240–7. doi: 10.1158/1078-0432.CCR-12-2246
48. Guo T, Ni J, Yang X, Li Y, Li Y, Zou L, et al. Pattern of recurrence analysis in metastatic EGFR-mutant NSCLC treated with osimertinib: Implications for consolidative stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys (2020) 107(1):62–71. doi: 10.1016/j.ijrobp.2019.12.042
49. Wang XS, Bai YF, Verma V, Yu RL, Tian W, Ao R, et al. Randomized trial of first-line tyrosine kinase inhibitor with or without radiotherapy for synchronous oligometastatic EGFR-mutated NSCLC. J Natl Cancer Inst (2022). doi: 10.1093/jnci/djac015
50. Peng P, Chen Y, Han G, Meng R, Zhang S, Liao Z, et al. Concomitant SBRT and EGFR-TKI versus EGFR-TKI alone for oligometastatic NSCLC: A multicenter, randomized phase II study. J Thorac Oncol (2019) 10:S250–1. doi: 10.1016/j.jtho.2019.08.499
51. Wang X, Zeng Z, Cai J, Xu P, Liang P, Luo Y, et al. Efficacy and acquired resistance for EGFR-TKI plus thoracic SBRT in patients with advanced EGFR-mutant non-small-cell lung cancer: a propensity-matched retrospective study. BMC Cancer. (2021) 21(1):482. doi: 10.1186/s12885-021-08228-2
52. Santarpia M, Altavilla G, Borsellino N, Girlando A, Mancuso G, Pergolizzi S, et al. High-dose radiotherapy for oligo-progressive NSCLC receiving EGFR tyrosine kinase inhibitors: Real world data. In Vivo. (2020) 34(4):2009–14. doi: 10.21873/invivo.11999
53. Kroeze SGC, Schaule J, Fritz C, Kaul D, Blanck O, Kahl KH, et al. Metastasis directed stereotactic radiotherapy in NSCLC patients progressing under targeted- or immunotherapy: efficacy and safety reporting from the 'TOaSTT' database. Radiat Oncol (2021) 16(1):4. doi: 10.1186/s13014-020-01730-0
54. Pembroke CA, Fortin B, Kopek N. Comparison of survival and prognostic factors in patients treated with stereotactic body radiotherapy for oligometastases or oligoprogression. Radiother Oncol (2018) 127(3):493–500. doi: 10.1016/j.radonc.2018.04.022
55. Chan OSH, Lee VHF, Mok TSK, Mo F, Chang ATY, Yeung RMW. The role of radiotherapy in epidermal growth factor receptor mutation-positive patients with oligoprogression: A matched-cohort analysis. Clin Oncol (R Coll Radiol). (2017) 29(9):568–75. doi: 10.1016/j.clon.2017.04.035
56. Conforti F, Catania C, Toffalorio F, Duca M, Spitaleri G, Barberis M, et al. EGFR tyrosine kinase inhibitors beyond focal progression obtain a prolonged disease control in patients with advanced adenocarcinoma of the lung. Lung Cancer. (2013) 81(3):440–4. doi: 10.1016/j.lungcan.2013.05.019
57. Yu HA, Sima CS, Huang J, Solomon SB, Rimner A, Paik P, et al. Local therapy with continued EGFR tyrosine kinase inhibitor therapy as a treatment strategy in EGFR-mutant advanced lung cancers that have developed acquired resistance to EGFR tyrosine kinase inhibitors. J Thorac Oncol (2013) 8(3):346–51. doi: 10.1097/JTO.0b013e31827e1f83
58. Weickhardt AJ, Scheier B, Burke JM, Gan G, Lu X, Bunn PA Jr., et al. Local ablative therapy of oligoprogressive disease prolongs disease control by tyrosine kinase inhibitors in oncogene-addicted non-small-cell lung cancer. J Thorac Oncol (2012) 7(12):1807–14. doi: 10.1097/JTO.0b013e3182745948
59. Brade AM, Ng S, Brierley J, Kim J, Dinniwell R, Ringash J, et al. Phase 1 trial of sorafenib and stereotactic body radiation therapy for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys (2016) 94(3):580–7. doi: 10.1016/j.ijrobp.2015.11.048
60. Jia W, Guo H, Jing W, Jing X, Li J, Wang M, et al. An especially high rate of radiation pneumonitis observed in patients treated with thoracic radiotherapy and simultaneous osimertinib. Radiother Oncol (2020) 152:96–100. doi: 10.1016/j.radonc.2020.07.051
Keywords: SAbR, EGFR - epidermal growth factor receptor, NSCLC - lung adenocarcinoma - EGFR - ALK - BRAF - KRAS - RET - MET - PD-L1 - ROS1, oligoprogressive disease, targeted therapy, metastatic NSCLC, oligometastatic
Citation: Chicas-Sett R, Castilla Martinez J, Hernández Blanquisett A, Zafra J and Pastor-Peidro J (2023) Stereotactic ablative radiotherapy for acquired resistance to EGFR therapy in metastatic non-small cell lung cancer. Front. Oncol. 12:1092875. doi: 10.3389/fonc.2022.1092875
Received: 08 November 2022; Accepted: 12 December 2022;
Published: 16 January 2023.
Edited by:
Stephanie G.C. Kroeze, Aarau Cantonal Hospital, SwitzerlandReviewed by:
Tobias Finazzi, University Hospital of Basel, SwitzerlandCopyright © 2023 Chicas-Sett, Castilla Martinez, Hernández Blanquisett, Zafra and Pastor-Peidro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodolfo Chicas-Sett, cmNoaWNhc0B1Zm0uZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.