
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 06 January 2023
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1091816
 Sheng Deng1†Zhihua Xuan1†
Sheng Deng1†Zhihua Xuan1† Junlong Feng2†
Junlong Feng2† Haisong Li2Bin Wang2Zhen Yang1Lihua Xuan1Fanchao Meng3
Haisong Li2Bin Wang2Zhen Yang1Lihua Xuan1Fanchao Meng3 Lu Wang4Yangchun Xiao5*
Lu Wang4Yangchun Xiao5* Jisheng Wang2*
Jisheng Wang2*Background: Penile cancer is a malignant tumor of the genitourinary system that mostly occurs in middle-aged and elderly men aged 50–70 years, which can seriously affect physical, psychological, and sexual health. Hundreds of original articles and reviews on penile cancer are published each year. However, a bibliometric analysis of these publications has not been performed.
Objective: This study aimed to systematically analyze and visualize penile cancer-related publications through bibliometrics and reveal identified topics, hotspots, and knowledge gaps in related fields.
Methods: Based on the Web of Science core collection database, we first analyzed the quantity and quality of publications in the field of penile cancer. Second, we profiled the publishing groups in terms of country, institution, author’s publication, and cooperation network. Then, we systematized and summarized the hot topics of research.
Results: This bibliometric analysis was conducted from 2001 to 2022. The analysis identified 1,687 articles and reviews, which were published in 432 journals. The number of publications and citations on penile cancer-related research has steadily increased over the last two decades. Furthermore, academic institutions in Europe and the United States play a leading role in penile cancer research. The country, institution, journal, and author with the most publications were the United States (507), H Lee Moffitt Cancer Research Center (96), Journal of Urology (83), and Spiess P (87), respectively. The most frequently used keywords were penile cancer (743), squamous-cell carcinoma (717), cancer (380), carcinoma (232), lymphadenectomy (229). 16 keyword clustering information was obtained, including #0 male circumcision, #1 lichen sclerosus, #2 chemotherapy, #3 penile neoplasms, #4 targeted therapy, #5 resection margin, #6 cervical cancer, #7 lymph node dissection, #8 prognostic factor, #9 prostate cancer, #10 inguinal lymph node dissection, #11 human papillomavirus DNA, #12 gene, #13 penile intraepithelial neoplasia, #14 male sexual function, and #15 penile cancer.
Conclusion: More and more scholars are devoted to the research on penile cancer. This bibliometric analysis revealed that the main research topics and hotspots in penile cancer included risk factors and surgical treatment plans.
Penile cancer is a malignant tumor of the genitourinary system that mostly occurs in middle-aged and elderly men aged 50–70 years, which can seriously affect physical, psychological, and sexual health. Due to different countries, ethnic groups, religious beliefs, and health habits, the incidence of penile cancer has obvious regional differences. Penile cancer accounts for 0.4%–0.6% of all male malignancies in Europe and the United States (USA) (1, 2). Penile cancer is a serious public health problem in economically underdeveloped parts of Asia, Africa, and South America, where it can account for up to 10% of cases (3).
Penile cancer is classified using the tumor, node, metastases (TNM) staging system. Because the penis consists of different types of cells, different types of cancer can occur (4). The majority of tumors (over 95%) are squamous cell carcinomas (SCC), of which there are several recognized subtypes: warty, papillary, basaloid, verrucous, and sarcomatoid. Other non-SCC cancer types include sarcomatoid tumors, malignant melanoma, extramammary Paget’s disease, and malignant lymphomas (5).
The etiology and pathogenesis of penile cancer remain unclear, and its possible risk factors include phimosis, smoking, human immunodeficiency virus (HIV), human papillomavirus (HPV), chronic penile inflammation, and a history of impurity (6–8). Surgery is the main treatment for penile cancer, but there is no consensus on the proportion of lesion removal and penile loss. Early penile cancer without metastasis can be completely cured by surgical resection of the lesion, with a 5-year survival rate of up to 90%. However, once the tumor progresses to inguinal lymph node metastasis, the 5-year survival rate decreases to 50% (9). Additionally, radiotherapy, chemotherapy, and targeted therapy are alternative treatment options for penile cancer, but there is still a risk of local recurrence (10). Doctors must closely monitor these patients through follow-up.
Bibliometrics is the quantitative analysis of literature, which is widely used for evaluating research trends and hotspots in various fields (11). VOSviewer and CiteSpace software is commonly used in bibliometrics for co-word analysis, co-citation analysis, and literature coupling analysis, being able to visually display the outcomes. This software has the advantage of clustering technology and map presentation. It can rapidly analyze research trends in a certain field and exhibit them in the form of multivariate integrated visual knowledge maps (12, 13).
Hundreds of original articles and reviews on penile cancer are published each year. However, so far, there has been no systematic analysis of penile cancer-related publications. Therefore, this study aimed to systematically analyze and visualize penile cancer publications over the past 20 years using related bibliometric software, such as VOSviewer and CiteSpace. Furthermore, the study aimed to summarize the achievements attained in this field, understand the research direction and hotspot areas, and provide a reference for future studies.
The present study did not involve any human subject participation, and it was entirely performed using the bibliometric data retrieved from the Web of Science database (WOS, https://www.webofscience.com/wos/woscc/basic-search). Hence, it was deemed to be exempted from the Institutional Review Board approval.
The WOS database is the most commonly used and widely accepted database in scientific or bibliometric research. It contains nearly 9,000 high-impact journals and more than 12,000 academic conference proceedings, which provide a comprehensive overview of research in the scientific, technological, and medical research fields (14, 15).
Publications on penile cancer were retrieved on October 02, 2022. The time span was set between January 01, 2001, and October 01, 2022. First, the “WOS Core Collection” was selected on the search page. Article types were refined into “article” and “review.” “Plain text” was chosen for the file format, while “Full Record and Cited References” was chosen for the record content.
The search query string was described as follows: “penis cancer” (topic), “penis tumor” (topic), or “penis tumor” (topic) and “penis oncology” (topic), “penis neoplasm” (topic), “penis carcinoma” (topic), “penile cancer” (topic), “penile tumor” (topic), “penile tumor” (topic), “penile oncology” (topic), “penile neoplasm” (topic), or “penile carcinoma” (topic) and article or review article (document types).
The data were downloaded and analyzed by two researchers to ensure the accuracy of the data and the repeatability of the research. Microsoft Excel 2019 and GraphPad Prism 7 were applied to analyze the targeted files and exported the line charts and tables of top-cited or productive countries/regions, institutions, authors, journals, references, and keywords.
The test of fit (R2) was used to predict the relationship between publication year and publication output to compare the degree of agreement between the predicted results and the actual occurrence. The closer R2 is to 1, the better the fitting degree of the regression line to the observed value is; otherwise, the worse it is. The quantity and quality of academic production were evaluated by H-index proposed by Hirsch. Total link strength (TLS) was defined as the total number of co-occurrences. At the same time, the 2021 version of the Impact factor (IF) and Journal impact factor (JIF) quartile, as important indicators to measure the scientific value of research, were also included in the analysis. To characterize the nature of a cluster, CiteSpace was based on three special algorithms, namely log likelihood ratio (LLR), late semantic indexing (LSI), and mutual information (MI). Of the three, LLR generally gives the best results in terms of the uniqueness and coverage of cluster-related topics. Therefore, LLR was used for keyword clustering in this study.
CiteSpace (https://citespace.podia.com/download, R6.1.3) is a visual analysis software widely used in scientific papers. It is based on scientometric data and information visualization technology. Further, it presents the knowledge structure by analyzing the underlying knowledge, patterns, and distribution of the literature. In this study, CiteSpace was used for keyword clustering and burst word analysis (16).
VOSviewer (https://www.vosviewer.com/, R1.6.18) is a bibliometric analysis software for mapping knowledge. It can be used for co-word analysis, co-citation analysis, coupling analysis of documents, and result visualization. In this study, VOSviewer was used to visualize countries, authors, institutional collaborations, cited journals, and keyword co-occurrences and construct density maps (17).
The FoamTree function of Carrot2 (https://search.carrot2.org, R3.10.3) is used to visually display the topic categories. In this study, Carrot2 was utilized to extract keywords of significance and give relative impact to each keyword (18).
Analysis of the annual number of published papers is important as it reflects the growth of knowledge in a certain field. In this study, 1,687 articles and reviews on penile cancer research were selected out of the 2,578 records retrieved from the Web of Science database. A total of 891 conference abstracts, letters, news, book chapters, and editorial materials were excluded (Figure 1).
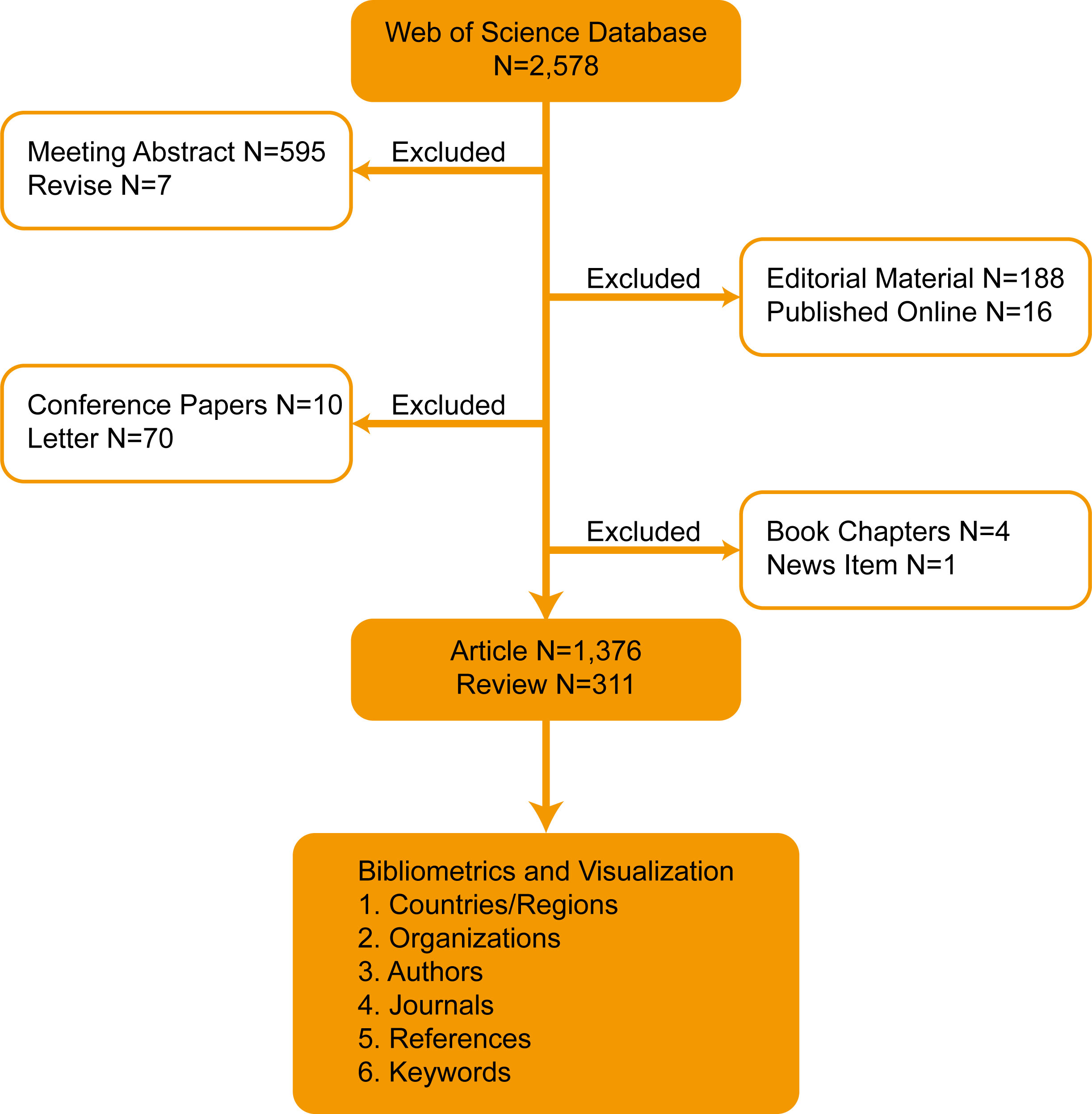
Figure 1 Flowchart of the search strategy.
Although the time span of our search was from January 1, 2001, to October 1, 2022, no papers that meet both the search term and the article type could be included before 2004. This study showed that from 2004 to 2011, the number of publications on penile cancer increased slowly. The turning point occurred in 2012. Since then, the number of papers published has increased rapidly. The number of papers published each year exceeded 100, reaching a record high (140) in 2020. This bibliometric analysis generally showed a linear growth trend (R2 = 0.8898) in penile cancer-related research, reflecting the increasing interest in this research field (Figure 2).
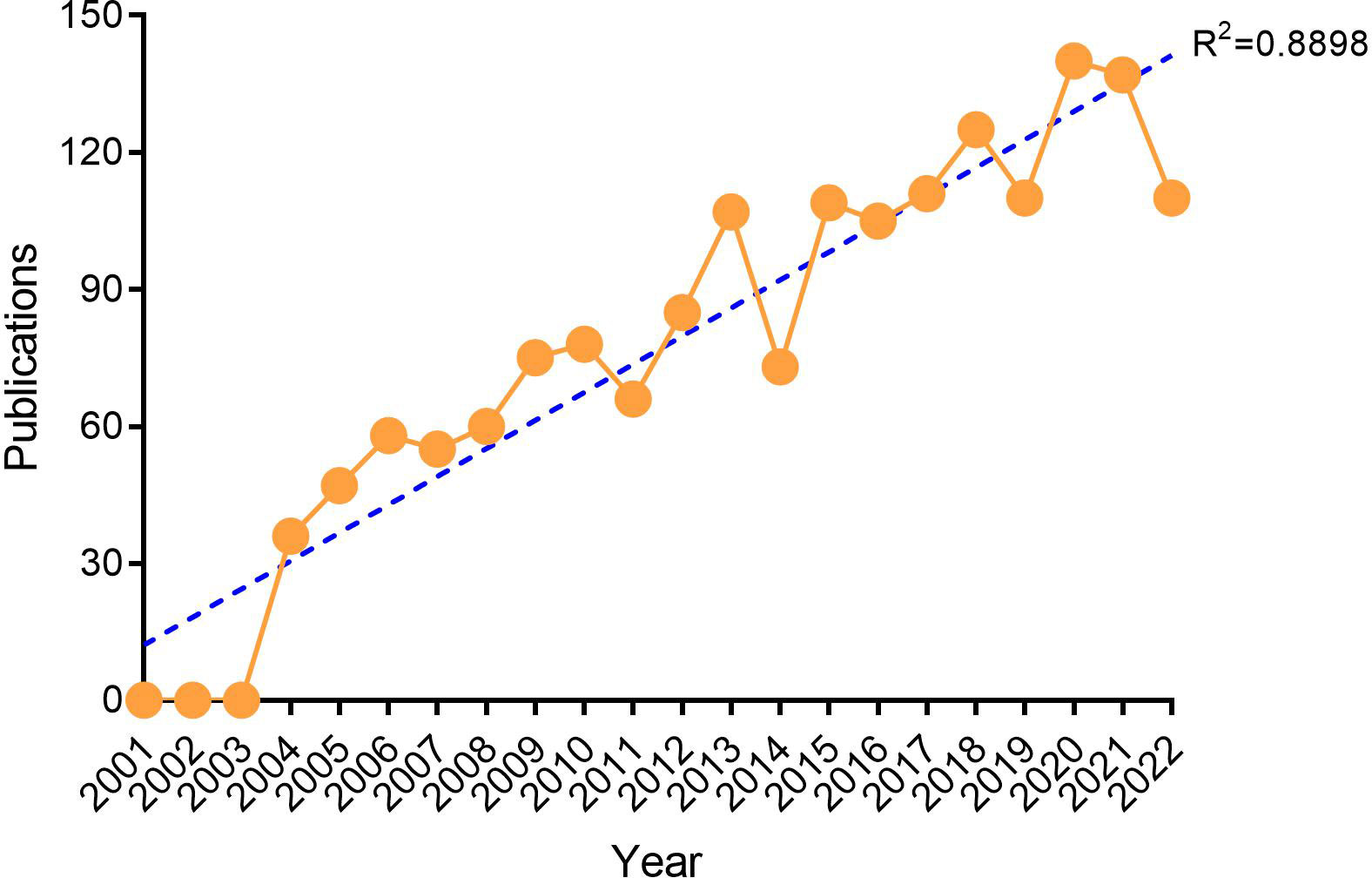
Figure 2 Annual trends of global publications.
A total of 84 countries/regions published papers on penile cancer. The USA had the largest number of publications (507, 30.05%), followed by Germany (241, 14.29%), England (199, 11.80%), China (188, 11.14%), and Italy (158, 9.37%) (Table 1, Figure 3). Additionally, the H index (52) and total citations (11954) of the USA ranked first, followed by England (44, 8170), Netherlands (48, 6478), Germany (30, 4691), and Italy (33, 4106) (Table 1). The results showed that the above-mentioned countries were more interested in the related research of penile cancer.
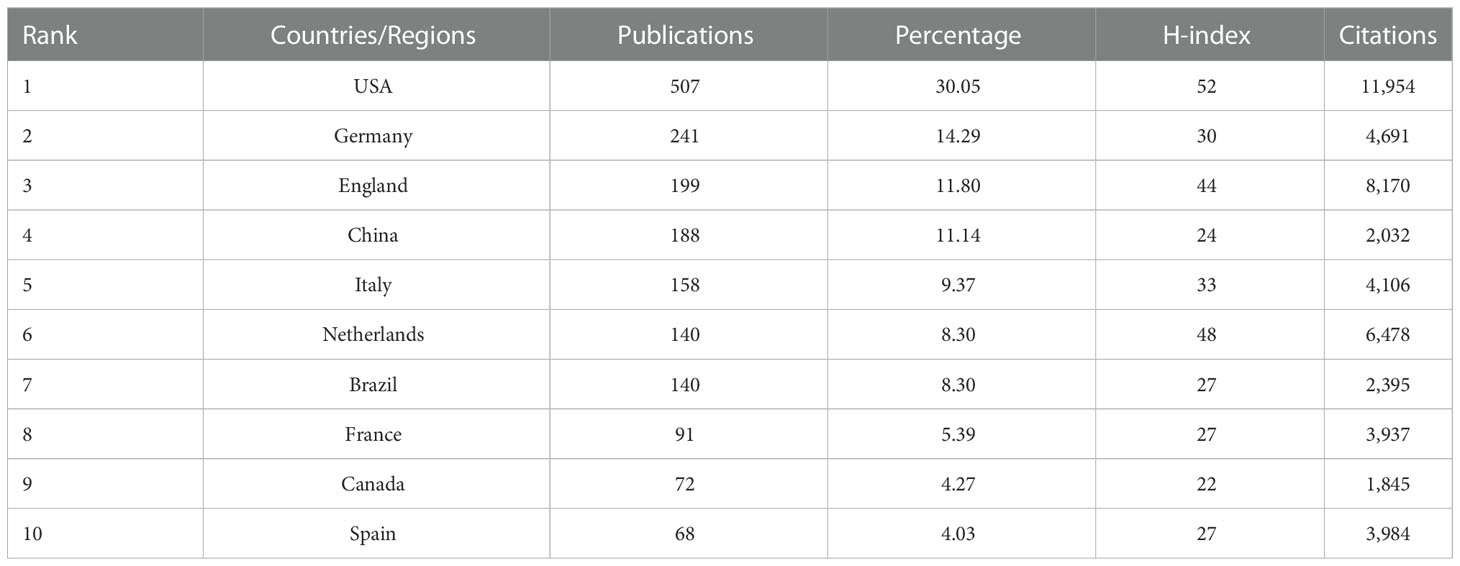
Table 1 Top 10 productive countries/regions.
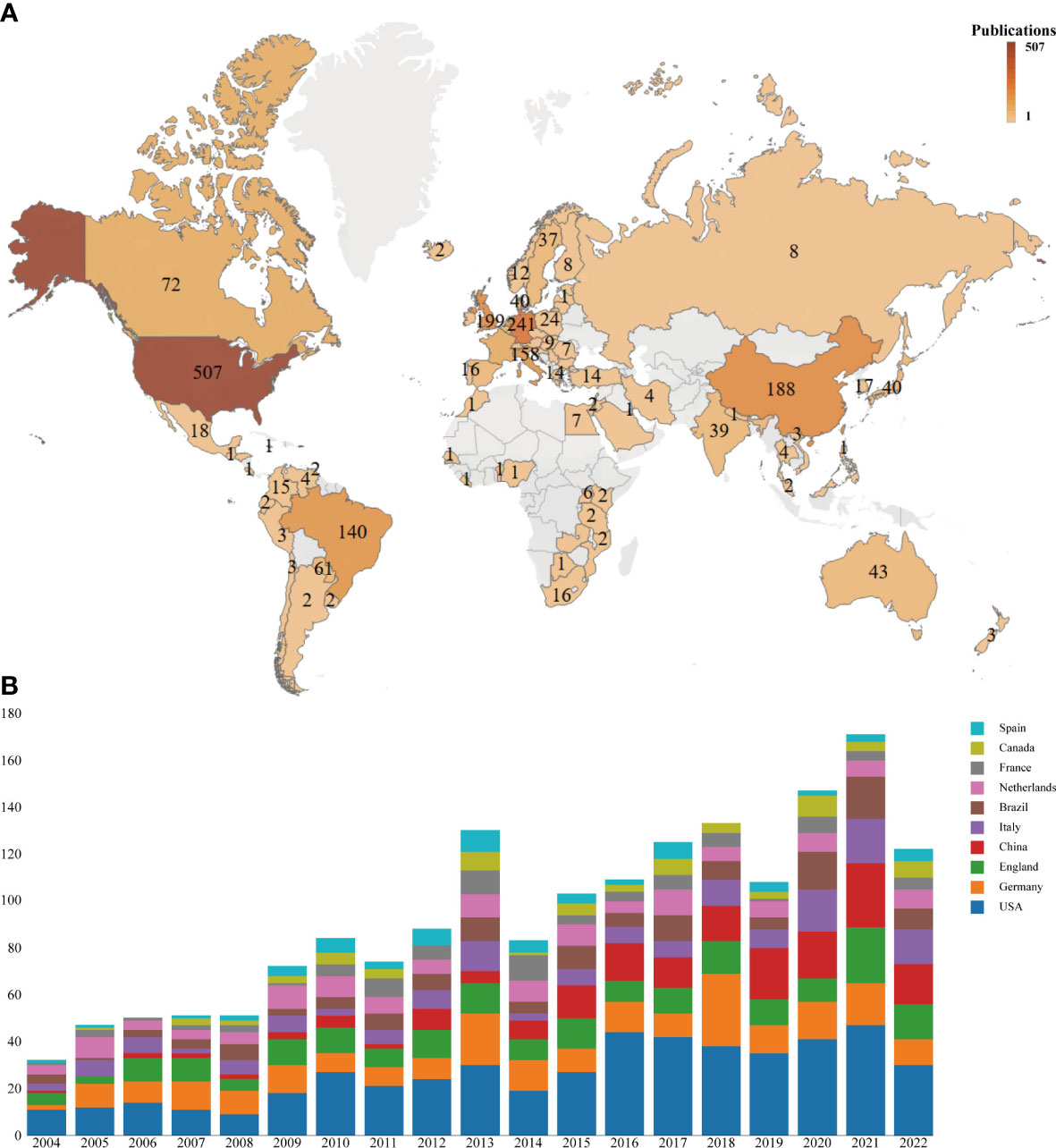
Figure 3 Global analysis of the research trends in penile cancer. (A) World map based on the total publications of different countries/regions. (B) The changing trend of the annual publication quantity in the top 10 countries/regions from 2004 to 2022.
VOSviewer was used to analyze the cooperation of different countries. The line between nodes indicates the co-authorship between countries; the thicker the line, the stronger the cooperative relationship. The results showed that the USA, Germany, Italy, and England had more cooperation with other countries. However, cooperation between other countries was weaker (Figure 4).

Figure 4 Co-occurrence map of countries/regions. (A) The size of the nodes represents the number of articles; the thickness of the curve represents the strength of the collaboration; the colors represent different collaboration groups. (B) The thickness of the line between countries reflects the frequency of the cooperation.
A total of 2,266 institutions were involved in publishing penile cancer-related papers. The top five institutions with the highest number of publications were H Lee Moffitt Cancer Research Center (96), Antoni Van Leeuwenhoek Hospital (60), Fudan University (45), Netherlands Cancer Institute (44), and University Texas Md Anderson Cancer Center (43) (Table 2). The top five institutions with the highest number of total citations were Antoni Van Leeuwenhoek Hospital (3,454), H Lee Moffitt Cancer Research Center (1,526), Harvard University (1,397), University Texas Md Anderson Cancer Center (1,196), and Netherlands Cancer Institute (1,163) (Table 2).
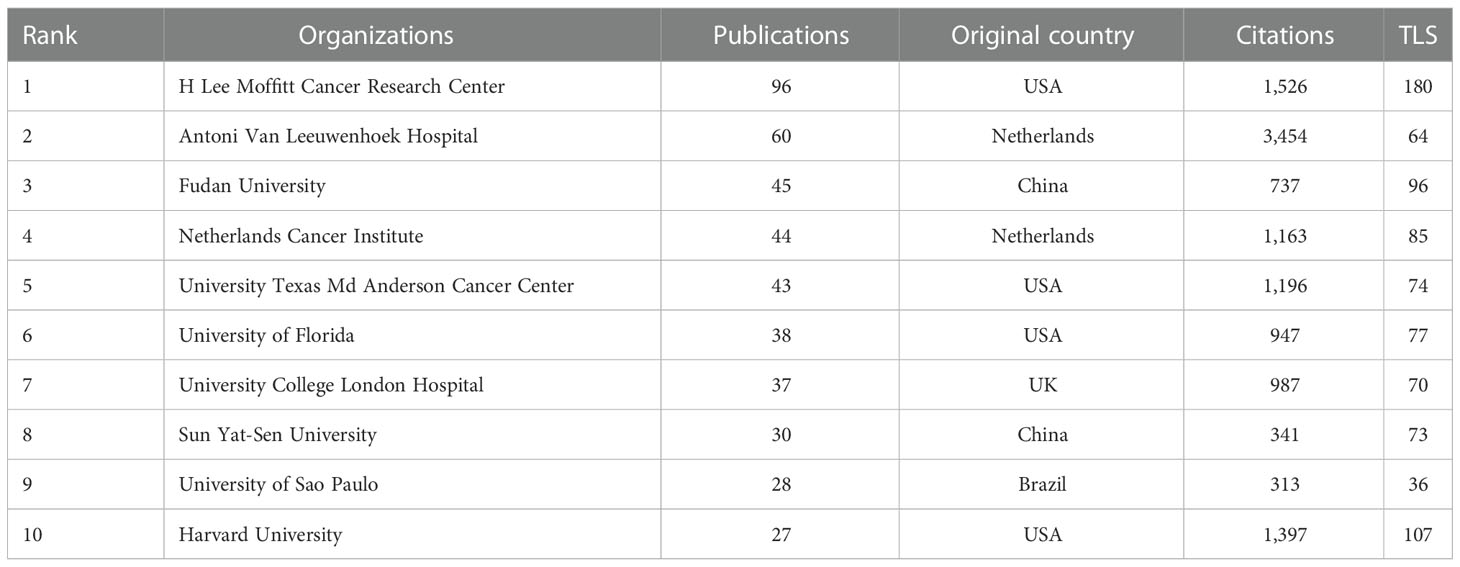
Table 2 Top 10 productive institutions.
Antoni Van Leeuwenhoek Hospital, H Lee Moffitt Cancer Research Center, and University Texas Md Anderson Cancer Center were at the center of the partnerships. However, most institutions were fragmented and lacked cooperation. The overall network density was low (density = 0.0078) (Figure 5).
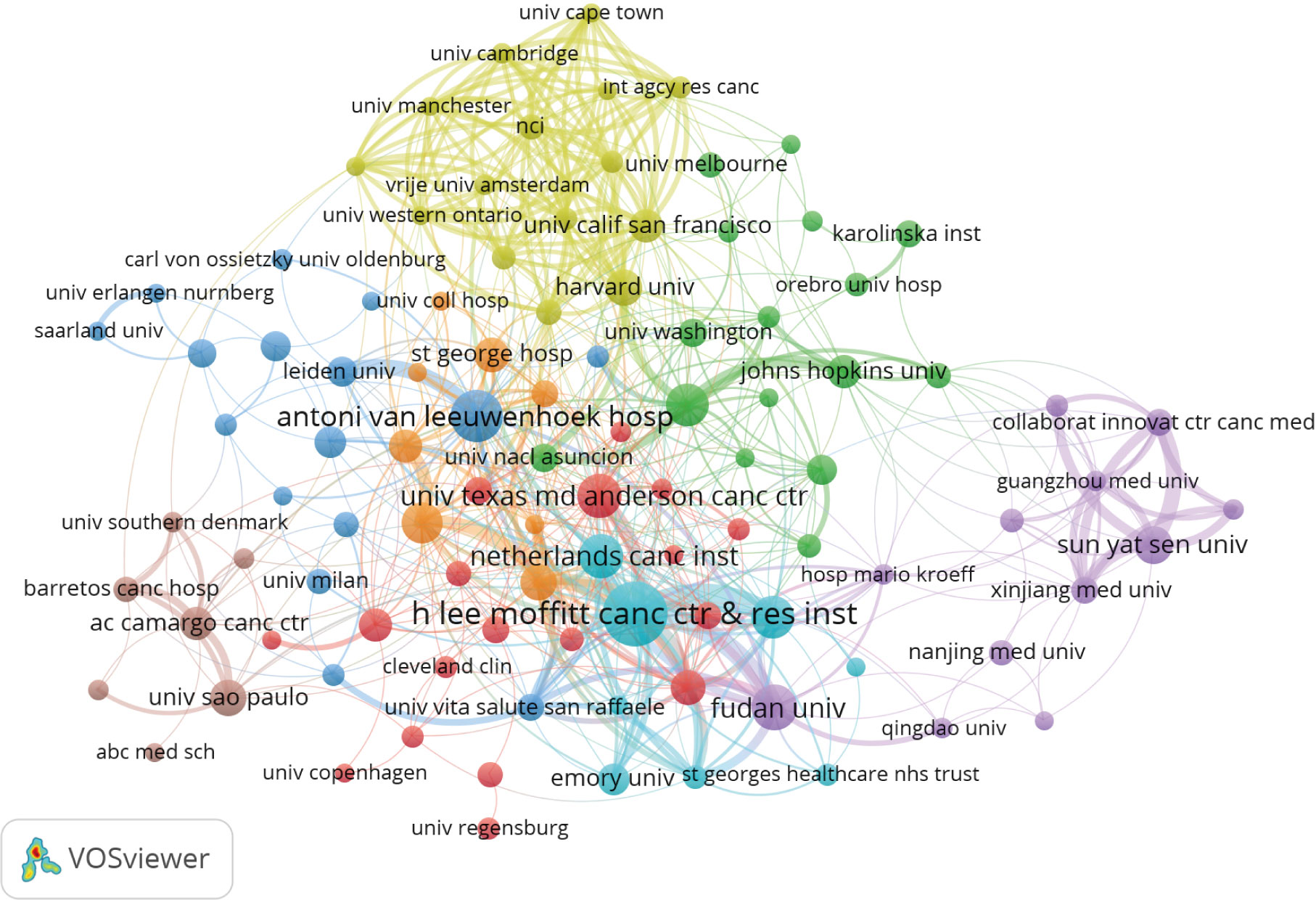
Figure 5 Co-occurrence map of institutions. The size of the nodes represents the number of articles; the thickness of the curve represents the strength of the collaboration; the colors represent different collaboration groups.
The author co-occurrence analysis identified the core authors in penile cancer-related research and the strength of collaboration between authors. Co-cited analysis means that when two authors or papers are cited by a third author or paper at the same time, the two authors or papers have a co-cited relationship.
This analysis revealed a total of 7,290 authors and 19,136 co-cited authors. Among them, Spiess P (87), Horenblas S (71), Cubilla A (46), Zhu Y (40), and Chaux A (37) had the highest number of publications (Table 3 and Figure 6A). The author’s cooperation represents teamwork, but the cooperation among teams is less, and the research is relatively fragmented. The co-citation analysis showed that Leijte J (611), Cubilla A (553), Horenblas S (507), Kroon B (484), and Chaux A (427) had the most co-citations (Table 3 and Figure 6B). The results showed that the above-mentioned authors were more interested in the related research of penile cancer.
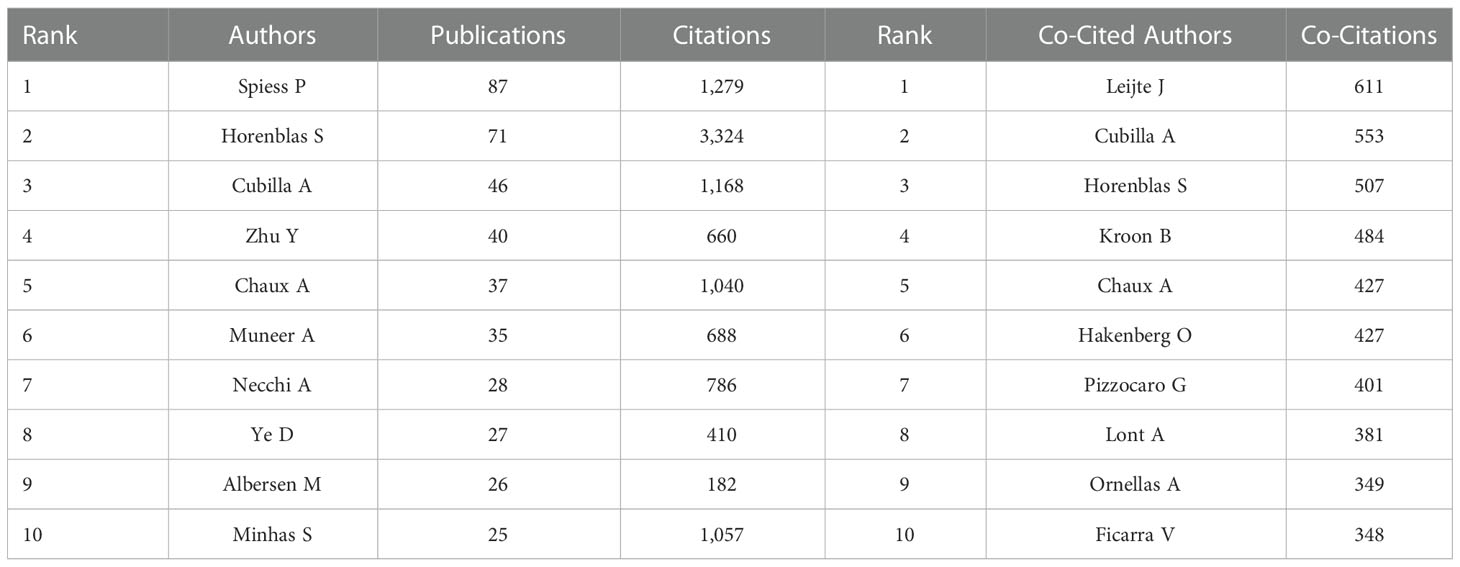
Table 3 Top 10 productive authors and co-cited authors.
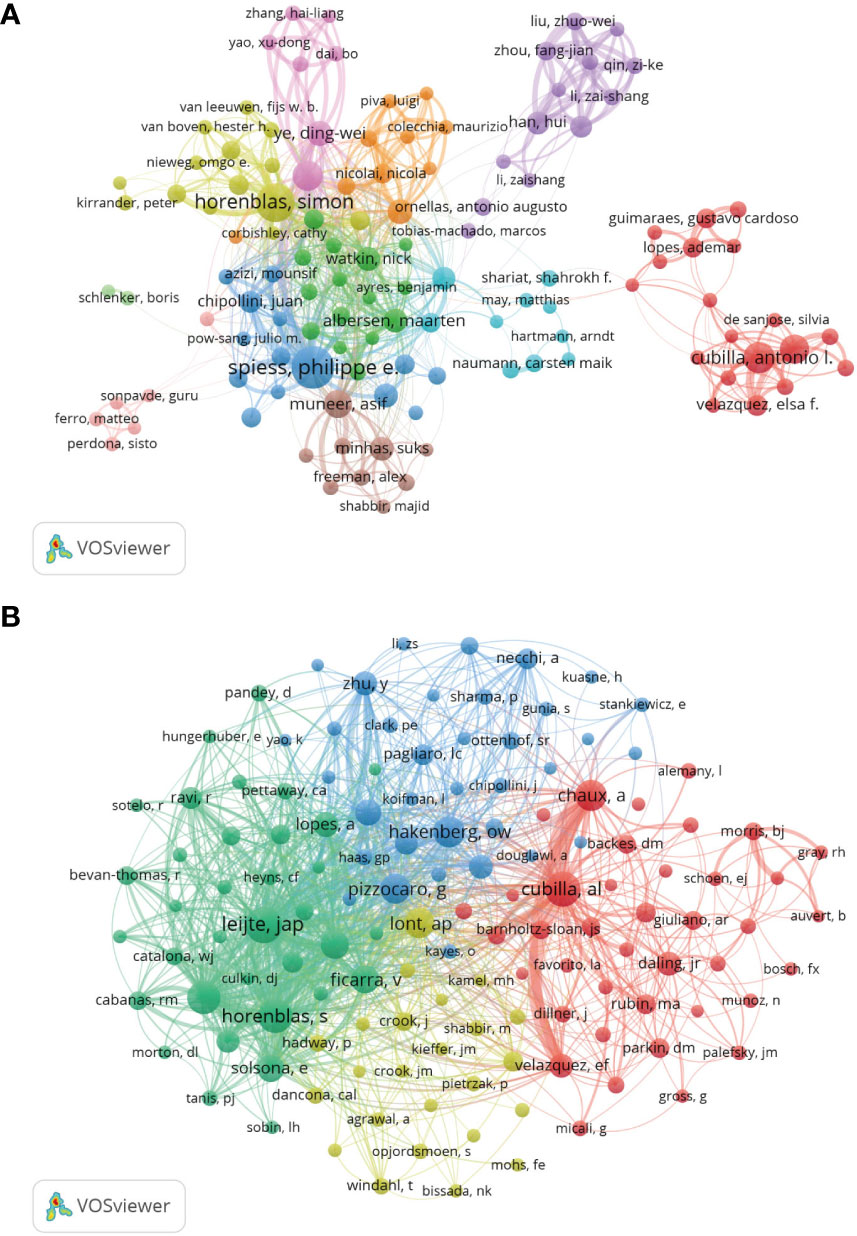
Figure 6 Analysis of authors and co-cited authors. (A) Co-occurrence map of Authors. The size of the nodes represents the number of articles. (B) Co-cited authors analysis map. The size of the nodes represents the number of co-citations.
All the selected papers were published in 432 journals. The top five high-yield journals were the Journal of Urology (83), BJU International (82), Urologic Oncology-Seminars and Original Investigations (81), Urology (58), and Urologe (50). The most cited journals were the Journal of Urology (3,534), European Urology (3,372), BJU International (2,308), Urology (1,305), and World Journal of Urology (960) (Table 4).
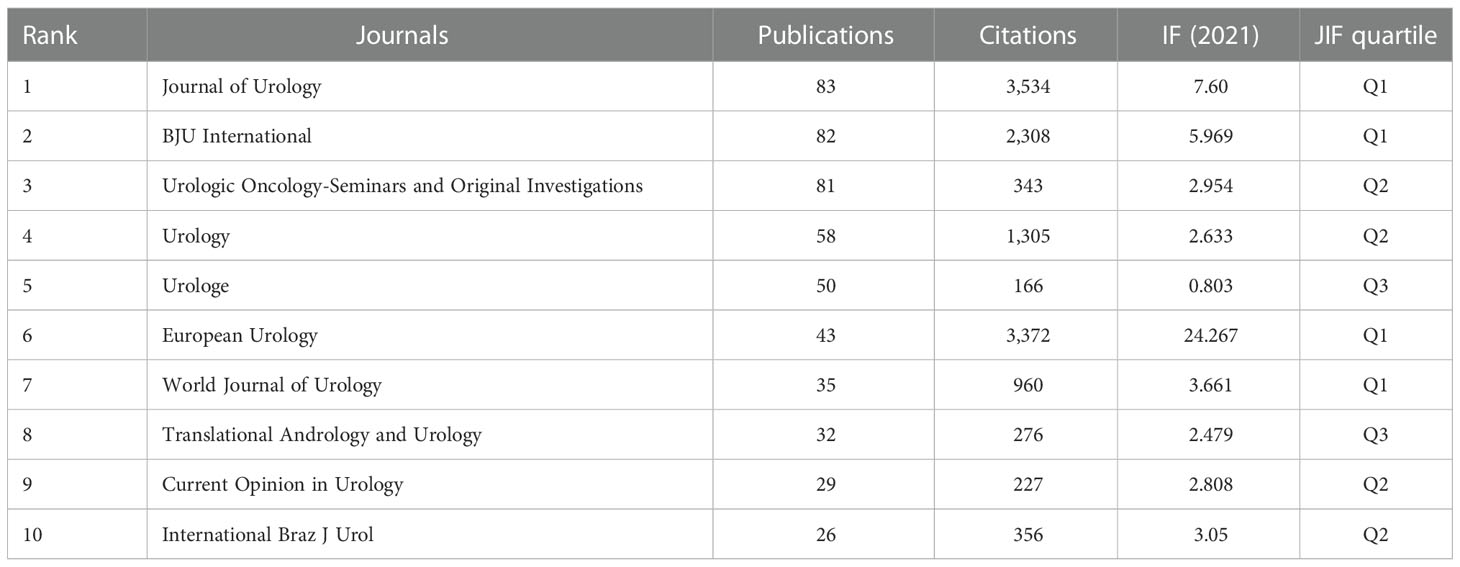
Table 4 Top 10 productive journals.
Analysis of the co-cited journals showed that 4,804 journals were co-cited. The top five co-cited journals were the Journal of Urology (6,476), European Urology (3,257), BJU International (2,446), Urology (1,879), and International Journal of Cancer (1,162) (Table 5). Most of the top ten productive and co-cited journals are divided into Q1 and Q2, reflecting the outstanding academic contributions of penile cancer-related research.
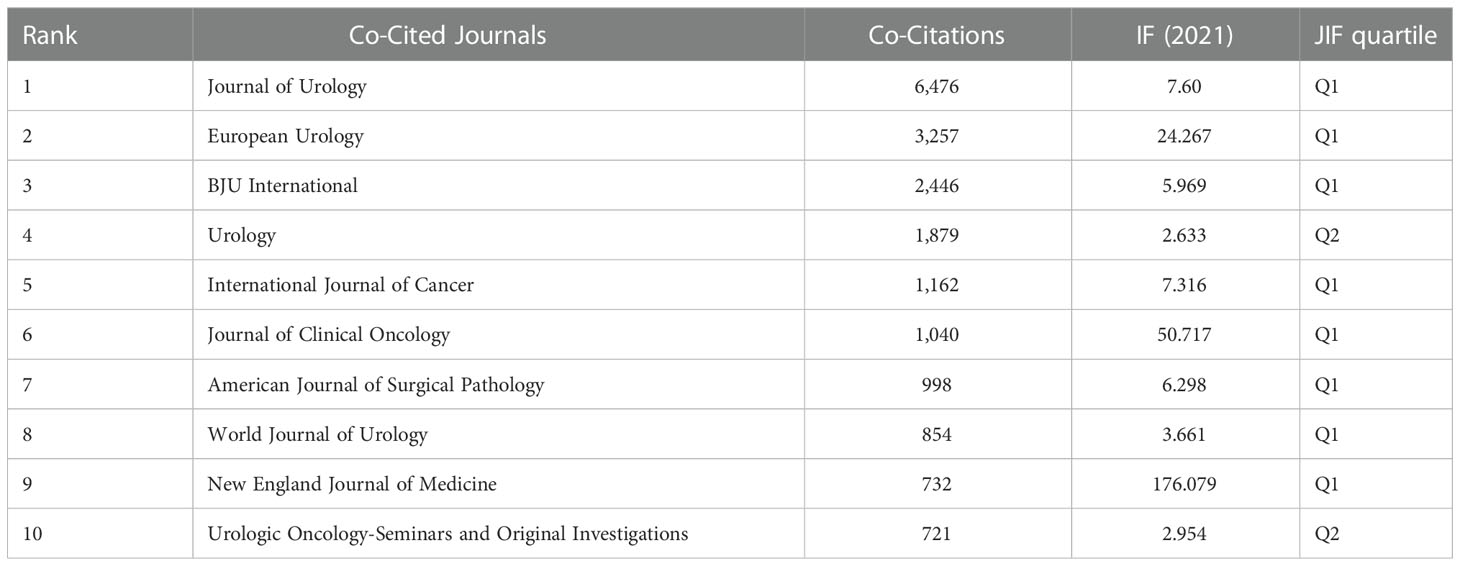
Table 5 Top 10 co-cited journals.
Knowledge flow analysis is used to explore the evolutionary relationship of knowledge citations and co-citations between citing and cited journals. The dual-map overlay of journals can intuitively show the distribution of journals in various disciplines, the evolution of citation trajectories, and the drift of scientific research centers. The citing map is on the left and the cited map is on the right. In Figure 7, the two green citation paths indicate that the research of molecular, biology, genetics, or health, nursing, medicine journals is often cited by medicine, medical, clinical journals.
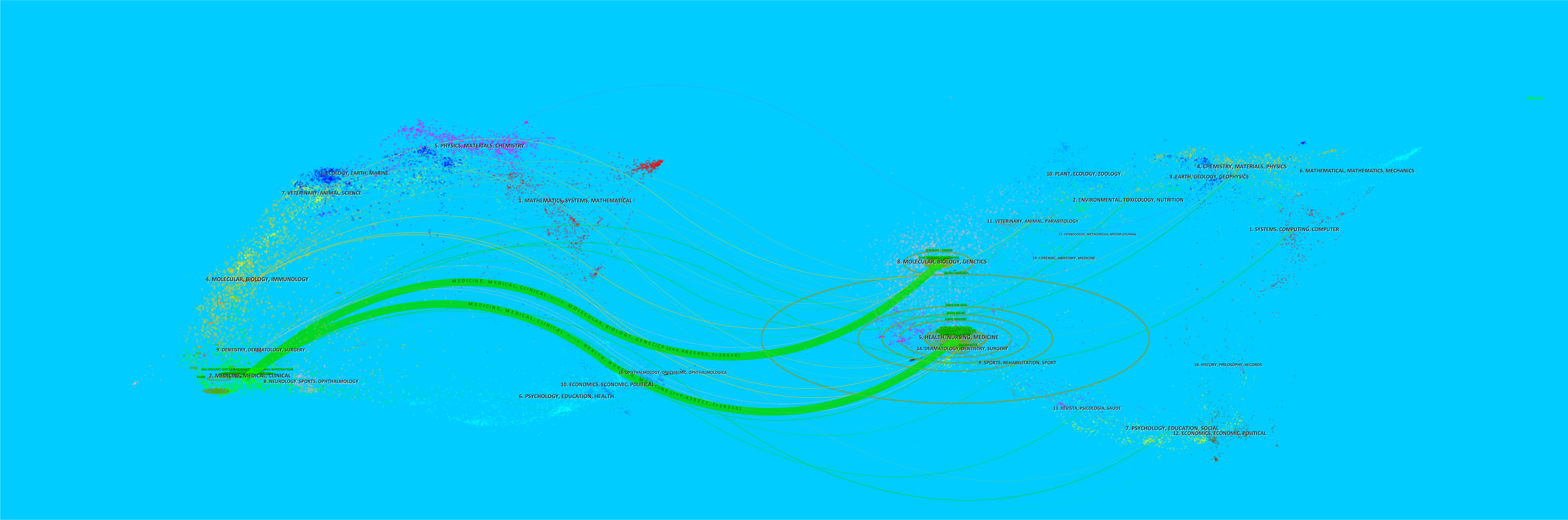
Figure 7 The dual-map overlay of journals in penile cancer. The more papers the journal publishes, the longer the vertical axis of the ellipse, and the greater the number of authors, the longer the horizontal axis of the ellipse.
A total of 1,687 references were obtained, of which three references Forman (2012), zur Hausen (2009), and Parkin (2006) were cited more than 900 times (Table 6). Additionally, a total of 20 references had the strongest citation bursts. The three references with the highest strength were Hakenberg O, 2015 (66.72), Pizzocaro G, 2010 (49.48), and Solsona E, 2004 (31.92). The first reference that triggered a citation burst appeared in 2004 (Bevan-Thomas R, 2002) (Figure 8).
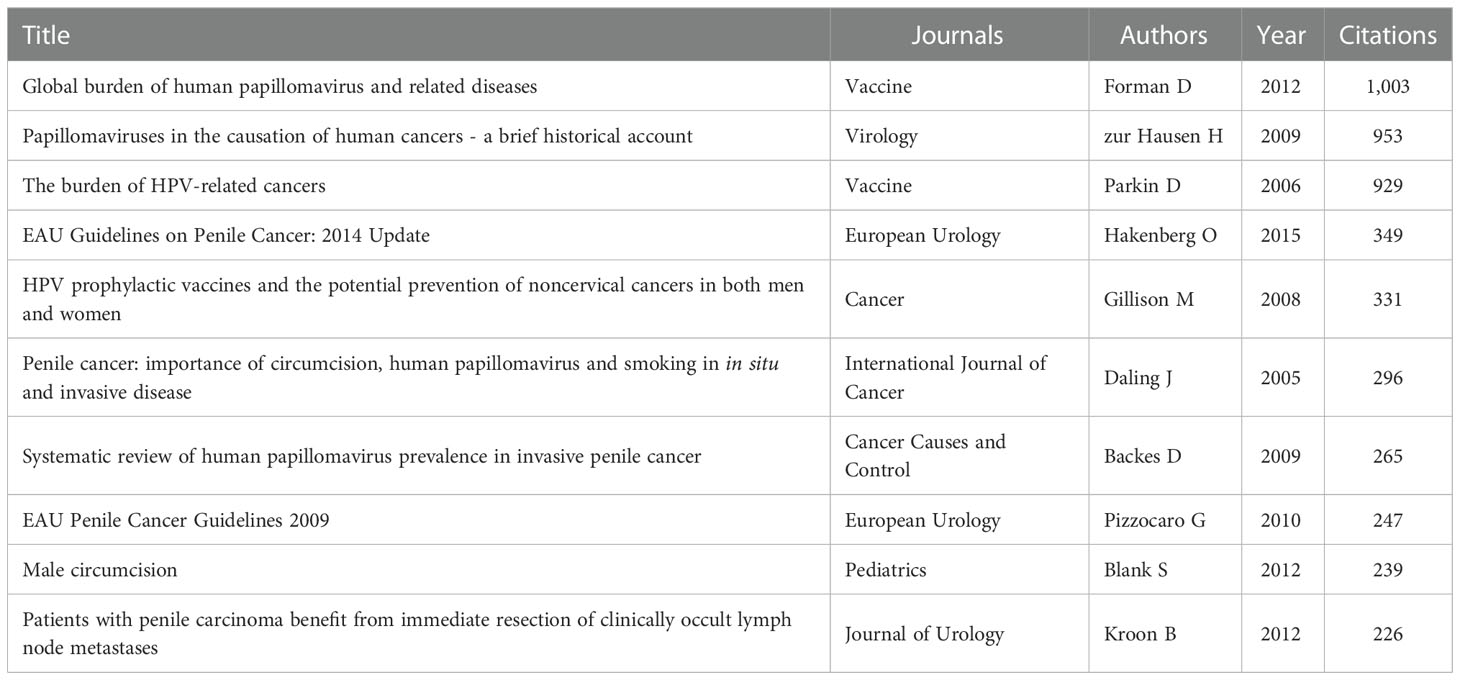
Table 6 Top 10 cited references.
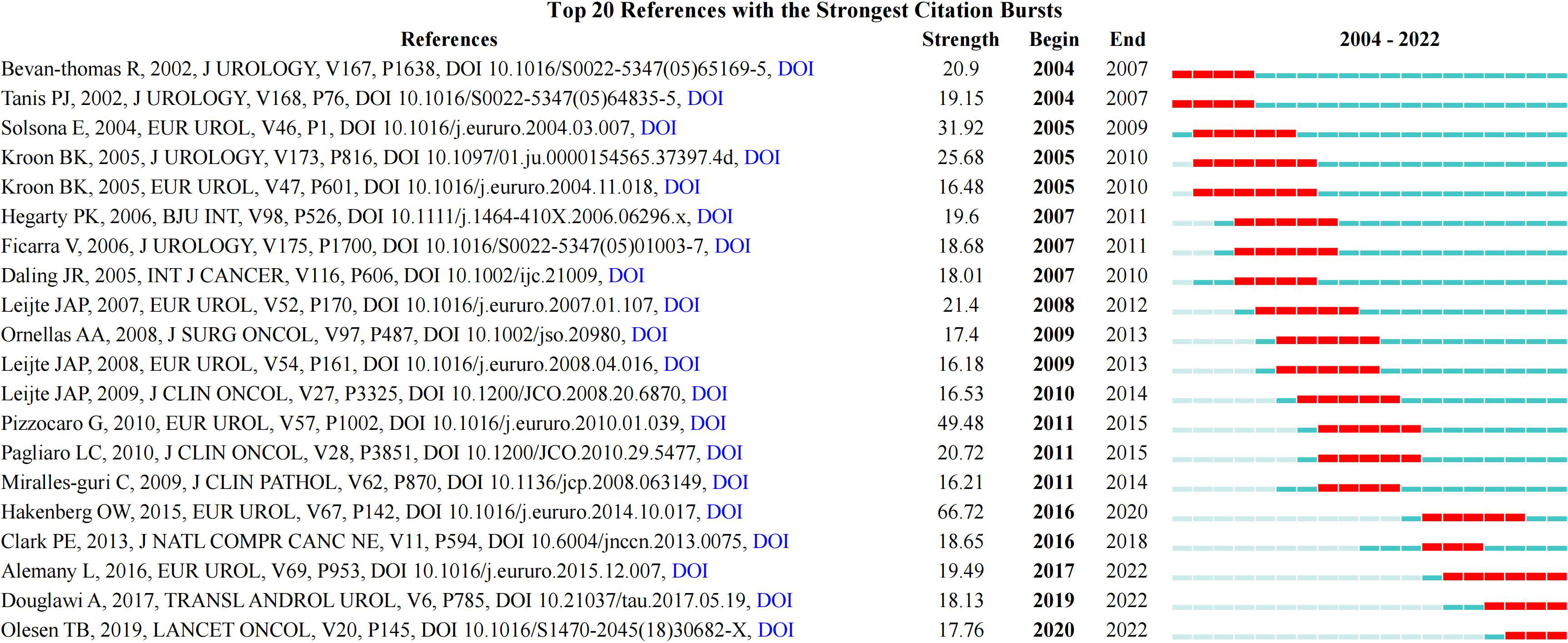
Figure 8 References burst analysis by CiteSpace.
Keywords frequently reflect an article core and the main content. The cluster map reflects research hotspots effectively. A total of 4,149 keywords were obtained. The top ten keywords obtained were penile cancer (743), squamous-cell carcinoma (717), cancer (380), carcinoma (232), lymphadenectomy (229), survival (206), management (206), penile carcinoma (191), prognostic-factor (160), and human papillomavirus (160) (Figures 9A, B). After clustering through CiteSpace software, a total of 16 clustering words were obtained, namely: #0 male circumcision, #1 lichen sclerosus, #2 chemotherapy, #3 penile neoplasms, #4 targeted therapy, #5 resection margin, #6 cervical cancer, #7 lymph node dissection, #8 prognostic factor, #9 prostate cancer, #10 inguinal lymph node dissection, #11 human papillomavirus DNA, #12 gene, #13 penile intraepithelial neoplasia, #14 male sexual function, and #15 penile cancer (Figure 9C).
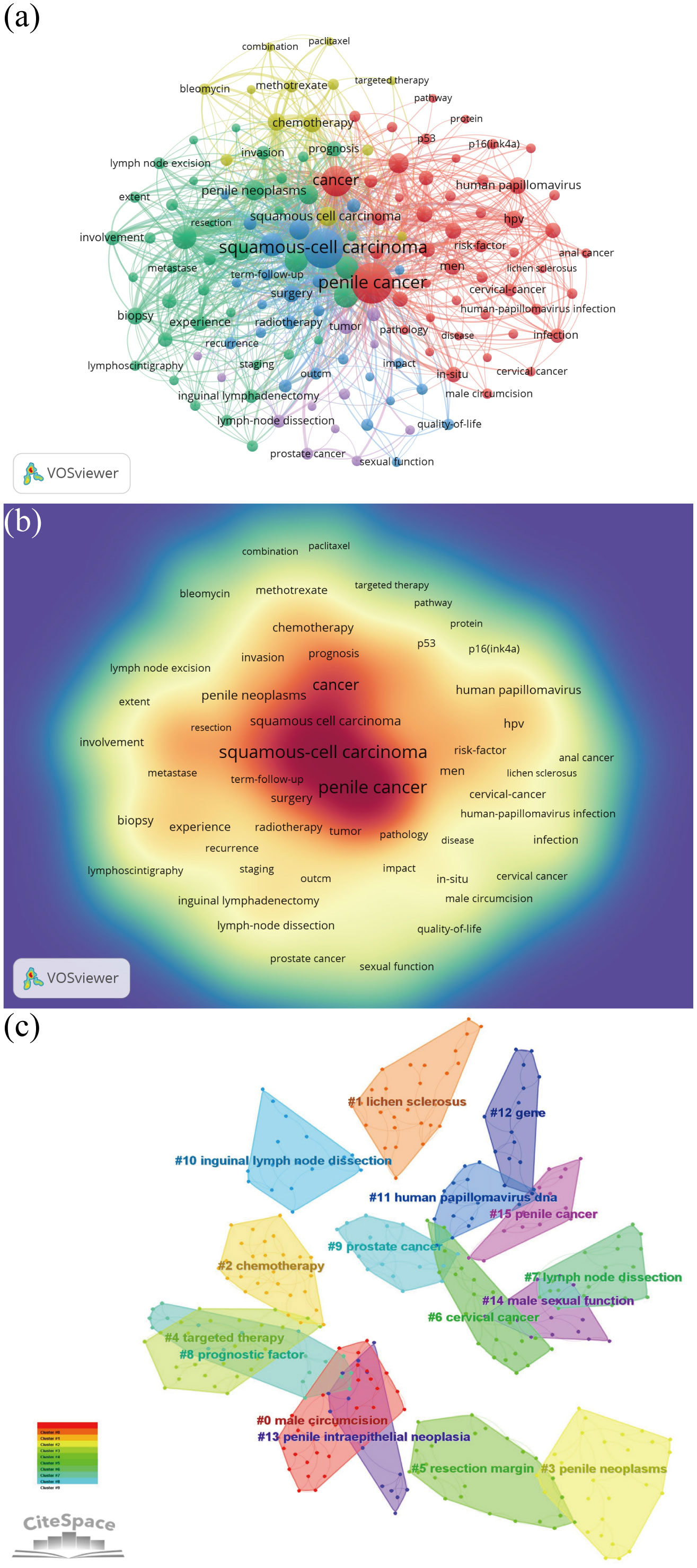
Figure 9 Keyword analysis. (A) Keyword co-occurrence analysis map obtained using VOSviewer. The size of the nodes represents the number of occurrences; the thickness of the curve represents the strength of collaboration; the different colors represent the different clusters. (B) Keyword density visualization analysis. The higher the intensity of the red color node, the higher the number of keywords. (C) Keyword clustering map analysis through CiteSpace. A total of 16 categories of keywords were obtained. The different color blocks represent different keyword clusters.
Using the FoamTrees function of Carrot2 and taking keywords as the data source, 100 clustering results were obtained (Figure 10). The larger the area of foam, the higher the heat of the study. It can be seen that “carcinoma is a ray disease,” “disease and its treatment,” “tumors are squamous cell carcinomas,” “treatment of penile tumor,” “treatment and survival,” “lymphadenectomy for penile cancer,” and “human papillomavirus HPV” were the main topics related to penile cancer.
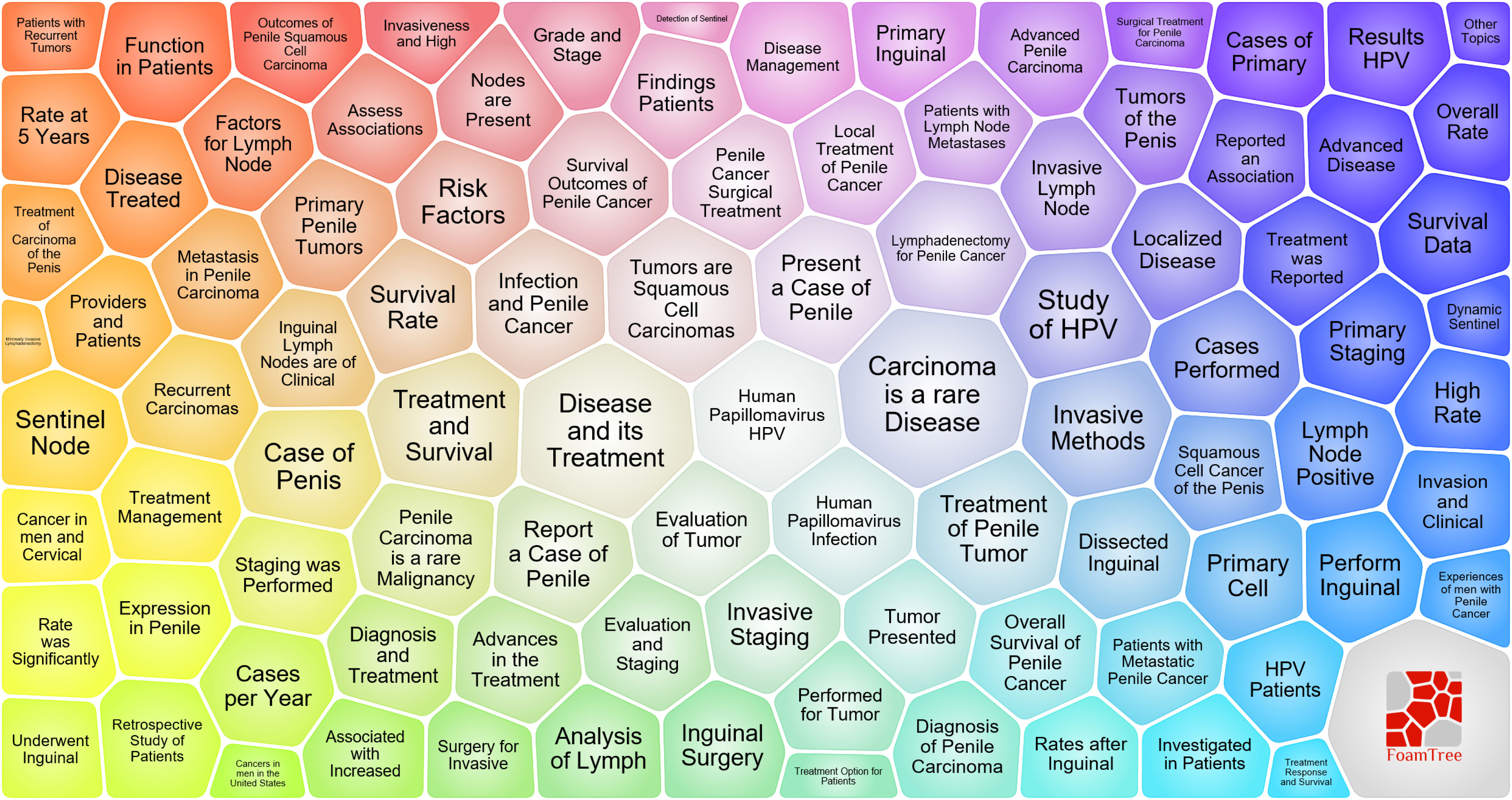
Figure 10 Topic categories survey for penile cancer based on the carrot 2.
Furthermore, a total of 20 keyword burst term analysis results were obtained. From 2004 to 2008, research on penile cancer focused on tumor staging, invasion, and surgical classification. From 2010 to 2017, the research related to penile cancer in this stage was transformed into research on human papillomavirus infection, male circulation, and other etiology and prevention measures. Since 2017, research on penile cancer has begun to explore the development of neoadjuvants on the basis of previous studies. The three burst words with the highest strength were tumor stage (15.88), invasion (10.23), and grade (9.66), Figure 11.
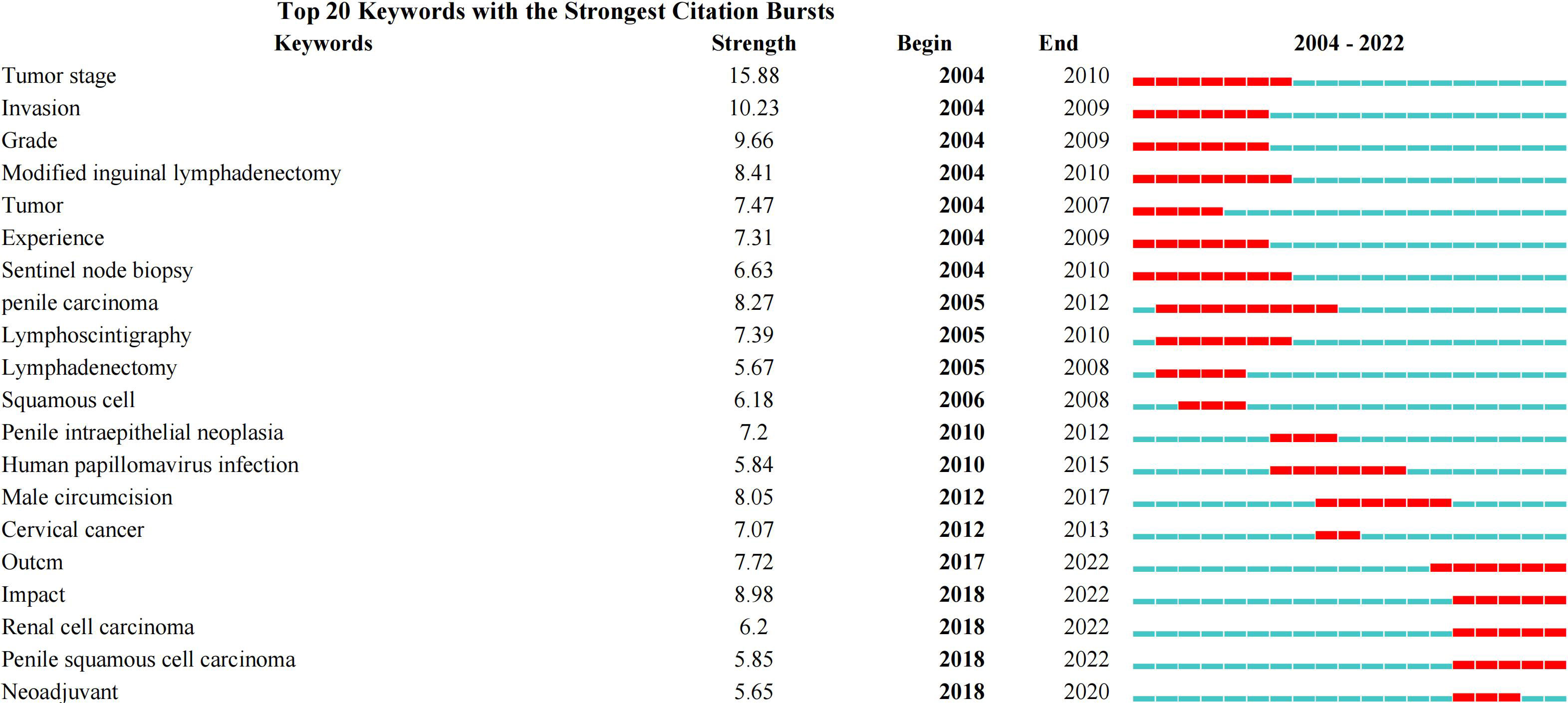
Figure 11 Keywords burst analysis by CiteSpace.
With the advent of big data, researchers need to understand the developments within penile cancer-related research. The bibliometric analysis uses visualization software, such as VOSviewer and CiteSpace, to comprehensively analyze the existing literature, understand the research trends, and predict future research hotspots (19). This study was the first bibliometric analysis of the related publications on penile cancer in the past 20 years.
In the past 20 years, the number of papers published in the research related to penile cancer has shown a linear upward trend (R2 = 0.8898). Especially in the past five years, the number of papers published each year exceeded 110, indicating that researchers in various countries are more interested in the field of penile cancer. It can be predicted that more countries and researchers will participate in penile cancer research in the future. Additionally, most studies were funded by the National Science Foundation and large pharmaceutical enterprises, showing that, at the national scientific and technological levels, more attention has been paid to research in this field.
Compared with other countries, the USA ranked first in the number of publications, citations, and H-index, being the major contributor in this field. It was followed by Germany, England, China, and Italy. It can be seen that the top five countries in terms of productivity were mainly concentrated in Europe and the USA. Although the incidence rate of penile cancer in some Asian, African, and South American countries is significantly higher than that in European and American countries, only China and Brazil ranked in the top 10, and the H-index of both countries was low, indicating that the quality of published papers was not high. The possible reason is the lack of international cooperation, subject support, and language barriers between researchers. Among the top 10 institutions that published papers, only Fudan University, Sun Yat Sen University, and University of Sao Paulo came from Asia and South America, and the rest came from Europe and the USA. Most institutions showed little cooperation, and the network density was only 0.0078. Therefore, it is necessary to strengthen exchanges and cooperation between research institutions and countries, especially in Asia and South America.
IF, JIF quartile, and total citation are effective indicators to appraise journal quality. The top 3 journals for productivity were the Journal of Urology (83; 3534; IF = 7.60; Q1), BJU International (82; 2308; IF = 5.969; Q1), and Urologic Oncology-Seminars and Original Investigations (81; 343; IF = 2.954; Q2). Additionally, although the number of papers published by European Urology was low, its total citations and co-citations were higher than that of most journals, indicating the important influence of European Urology in this field. Most of the top 10 journals were divided into Q1 and Q2, reflecting outstanding academic contributions to penile cancer research. It is a new method to show the flow of knowledge at the journal level on the dual-map overlay of journals. All colored curves originating from the citing map and pointing to the ones cited are the citation connection lines, which completely show the ins and outs of the citation. In Figure 7, the two green citation paths indicate that the research of molecular, biology, genetics, or health, nursing, medicine journals is often cited by medicine, medical, clinical journals.
Spiess P had the most publications (87), followed by Horenblas S (71), Cubilla A (46), Zhu Y (40), and Chaux A (37). Furthermore, Horenblas S was cited the most. The main research direction of Spiess P was the surgical treatment of penile cancer and the management of patients with lymphatic metastasis (20, 21). The papers cited most frequently by Horenblas S mainly involved clinical guidelines, epidemiology, pathogenesis, and prevention of penile cancer (22, 23). Forman (2012), zur Hausen (2009), and Parkin (2006) all cited more than 900 times. Interestingly, these three references were about the relationship between HPV and penile cancer. Thus, it can be seen that researchers all over the world have a strong interest in the etiology of penile cancer (24–26).
Through the analysis and comparison of the above-discussed general information, we can see that the most influential authors and references were mostly review articles and clinical guides from internationally renowned institutions and journals. Combined with the co-occurrence, clustering, and burst analysis of keywords, we preliminarily identified the risk factors and surgical treatment plan of penile cancer as the main research topic and hotspot in this field.
In recent years, people have had more knowledge about the risk factors of penile cancer, although the exact cause is still unclear. Penile cancer has two different pathogenic pathways. The first is related to high-risk HPV infection, and the second is related to chronic irritation and inflammation (27). HPV infection is a major risk factor for sexually transmitted infection of penile cancer (24). The HPV subtypes most frequently associated with penile cancer are HPV-16 and HPV-18. Studies have found that the carcinogenic pathogenesis of HPV infection is viral proteins E6 and E7-induced overexpression of cyclin-dependent kinase inhibitor 2A (p16Ink4a), which plays a role in cancer promotion, followed by the induction of malignant cell proliferation and carcinogenesis (28). Ferreux et al. have studied 53 penile cancer samples and found that 20 samples were positive for HPV-DNA. High-risk HPV-16 was the most common type of HPV (15/20). At the same time, the expression of p16Ink4a was significantly increased in 13 of 15 HPV-16 samples (P < 0.01) (29). There was a close relationship between HPV infection and abnormal expression of p16Ink4a, which promotes the use of p16Ink4a immunostaining as HPV detection. Additionally, Barzon et al. have analyzed microRNA (miRNA) of 59 patients with penile squamous cell carcinoma and found that the expression of miR-218 in high-risk HPV infection-positive samples was reduced (30). The decrease in miR-218 expression might be an important factor in HPV-induced carcinogenesis. Therefore, the use of condoms and HPV vaccination are essential. However, recommendations for HPV vaccination may vary from country to country.
Chronic inflammation is considered to be the carcinogenic mechanism of many malignant tumors. A total of 45% of penile cancer patients have a history of balanitis foreskin compared to only 8% of patients in the control group (31). A meta-analysis of 443 patients has found that the odds ratio (OR) of penile cancer with balanitis was 3.82. Similarly, lichen sclerosis (a type of chronic inflammation) and balanitis xerotic organisms (BXO) are also associated with the progression of penile cancer (32). Recent literature has shown that 28%–50% of patients with penile cancer have a history of BXO, and the estimated risk of developing penile squamous cell carcinoma is 2%–15% (33). This risk is mediated by the formation of phimosis, a known risk factor for penile cancer. Therefore, circumcision is necessary to prevent penile cancer, especially for patients with phimosis. The protective mechanism of circumcision is believed to improve hygiene, reduce the risk of transmission of HPV and other viruses, and reduce the occurrence of chronic inflammation. A recent systematic review by Larke et al. has found that early circumcision has a strong protective effect on invasive penile cancer (OR = 0.33) (34). Additionally, smoking, genital warts, age, obesity, metabolism, and social factors might be one of the risk factors for penile cancer.
Surgery is the gold standard for the treatment of penile cancer (35). However, the penis is a male sexual organ. Due to social, psychological, physiological, and other factors, the surgical treatment of penile cancer should follow the principle of removing the focus while minimizing the damage to the penis while maintaining the original shape and function of the penis as much as possible (9). The lesions only limited to the foreskin or penis head or tumors before the T1 stage can be circumcised or locally removed, and close observation and follow-up are required after the operation. Phase T1 tumors limited to the penis and without lymph node metastasis can be partially resected. If the invasive penile cancer or tumor invades more than 1/2 of the length of the whole penis, total penis resection should be performed (36). Compared with the operation of penis preservation, total penis resection can better clear the lesions, but it often leads to the loss of the patient’s sexual function, accompanied by various psychological diseases that affect the patient’s social life, and seriously reduces the quality of life. The main route of metastasis of penile cancer is lymph node metastasis. In 1977, Cabanas first proposed the concept of penile sentinel limp nodes (SLN) (37). SLN is located in the groin region, which is the earliest lymph node of penile cancer metastasis. Therefore, it is very important to determine whether there is tumor cell metastasis in SLN of penis. At present, the evaluation of lymph nodes requires careful physical examination first (38). If the swollen lymph node is not touched, fine needle aspiration cytology (FNAC) is a less invasive and more accurate method to determine suspicious lymph node metastasis, or with CT/MRI and other imaging techniques (39). If it is positive, lymph node dissection should be performed, including open inguinal lymphadenectomy (OIL) and video endoscopic inguinal lymphadenectomy (VEIL). OIL has many complications, mainly including wound infection, skin necrosis, wound dehiscence, lymphedema, etc (40). Compared with OIL, VEIL has fewer postoperative complications and similar efficacy. It may be used as a first-line treatment for inguinal lymph node dissection in the future, but it still needs to be further confirmed by multi-center randomized controlled trials with higher quality and larger samples (41).
At present, in addition to surgical treatment, chemotherapy, radiotherapy, immunotherapy and other systematic therapies for penile cancer are also the focus of research in this field (42). National Comprehensive Cancer Network (NCCN) and European Association of Urology (EAU) guidelines recommend a multimodal first-line approach involving neoadjuvant chemotherapy (NAC) followed by lymph node dissection for the treatment of bulky nodal disease (43). In a prospective study (44), NAC was significantly associated with an improvement in overall survival and time to progression among responders versus non-responders (P < 0.01), and 30% of the cohort remained free of disease recurrence following a median follow-up period of 34 months. Pathologically, 50% of patients responded to NAC and 10% of patients showed a pathological complete response. In the setting of locally advanced penile cancer, current NCCN guidelines recommend adjuvant chemotherapy in the form of either TIP or 5-fluorouracil (5-FU) in patients who did not receive first-line NAC and exhibited ≥2 positive nodes or extranodal extension at the time of inguinal lymph node dissection (45). The debate on whether to use radiotherapy, surgery, or both in penile cancer management has been ongoing for more than 50 years (46). At present, data from randomized controlled trials comparing radiotherapy and surgery are lacking, and thus management is frequently determined by institutional practice patterns and available expertise. In recent years, more new systemic treatment options for penis cancer have been reported, including immune checkpoint inhibitors (ICIs) (47), adaptive and engineered T-cell therapies (48), tyrosine kinase inhibitors (TKIs) and other targeted therapies (49), and HPV targeting vaccines (50). However, most of the relevant types of literature are relatively small, and we will update this study accordingly after the data is enriched in the future.
The significance of our research is as follows. (1) The countries/regions, institutions, authors, journals, references, keywords, and other elements of penile cancer-related literature in the past 20 years were clearly displayed. (2) Through the collation of data sets, readers and experts in relevant fields were helped to understand the development process, research status, and knowledge hotspots of penile cancer. (3) Future research directions for penile cancer were further provided for reference. However, there were still some limitations to our study. 1. Recently published articles might have low citations due to the limited time available for citations; thus, the study might be prone to research bias. 2. This study only included articles and reviews published in English, which might have overlooked some of the literature. 3. With the rapid development of big data, this study might have a short timeframe and needs to be updated regularly.
In the past 20 years, the number of papers published in research related to penile cancer has shown a linear upward trend. Especially in the past five years, the number of papers published each year exceeded 110. The USA and Europe were leading in research on penile cancer. However, there is a need to strengthen collaboration relationships, especially in developing countries. The top 10 cited and co-cited journals were mostly in Q1 and Q2, reflecting that research on penile cancer was of high quality. Furthermore, this bibliometric analysis revealed that the main research topics and hotspots in penile cancer included risk factors and surgical treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
SD and JW designed the study. SD, ZX and JF conducted the literature search. HL, BW, ZY, LX, FM and LW analyzed the data and wrote the paper. YX and JW approved the final manuscript. All authors contributed to the article and approved the submitted version.
China Postdoctoral Innovative Talent Support Program (BX20220047); Young Talent Support Project of Beijing Association of Science and Technology (BYESS2022182); Young Talent Support Project of Chinese Association of Chinese Medicine (CACM-2021-QNRC2-B04).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kakies CH, Lopez-Beltran A, Comperat E, Erbersdobler A, Grobholz R, Hakenberg OW, et al. Reproducibility of histopathologic tumor grading in penile cancer–results of a European project. Virchows Arch (2014) 464(4):453–61. doi: 10.1007/s00428-014-1548-z
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin (2018) 68(1):7–30. doi: 10.3322/caac.21442
3. Turner B, Drudge-Coates L, Henderson S. Penile cancer: diagnosis, clinical features and management. Nurs Stand (2013) 27(29):50–7. doi: 10.7748/ns2013.03.27.29.50.e6135
4. Sanchez DF, Fernandez-Nestosa MJ, Cañete-Portillo S, Cubilla AL. Evolving insights into penile cancer pathology and the eighth edition of the AJCC TNM staging system. Urol Oncol (2022) 40(6):215–22. doi: 10.1016/j.urolonc.2020.09.010
5. Thomas A, Necchi A, Muneer A, Tobias-Machado M, Tran ATH, Van Rompuy AS, et al. Penile cancer. Nat Rev Dis Primers (2021) 7(1):11. doi: 10.1038/s41572-021-00246-5
6. Schlenker B, Schneede P. The role of human papilloma virus in penile cancer prevention and new therapeutic agents. Eur Urol Focus (2019) 5(1):42–5. doi: 10.1016/j.euf.2018.09.010
7. Yuan T, Fitzpatrick T, Ko NY, Cai Y, Chen Y, Zhao J, et al. Circumcision to prevent HIV and other sexually transmitted infections in men who have sex with men: A systematic review and meta-analysis of global data. Lancet Glob Health (2019) 7(4):e436–47. doi: 10.1016/S2214-109X(18)30567-9
8. Bada M, Berardinelli F, Nyiràdy P, Varga J, Ditonno P, Battaglia M, et al. Adherence to the EAU guidelines on penile cancer treatment: European, multicentre, retrospective study. J Cancer Res Clin Oncol (2019) 145(4):921–6. doi: 10.1007/s00432-019-02864-9
9. Akers C, Holden F. An overview of the diagnoses and treatments for penile cancer. Br J Nurs (2020) 29(9):S6–S14. doi: 10.12968/bjon.2020.29.9.S6
10. Peyraud F, Allenet C, Gross-Goupil M, Domblides C, Lefort F, Daste A, et al. Current management and future perspectives of penile cancer: An updated review. Cancer Treat Rev (2020) 90:102087. doi: 10.1016/j.ctrv.2020.102087
11. Rondanelli M, Perna S, Peroni G, Guido D. A bibliometric study of scientific literature in scopus on botanicals for treatment of androgenetic alopecia. J Cosmet Dermatol (2016) 15(2):120–30. doi: 10.1111/jocd.12198
12. Maula AW, Fuad A, Utarini A. Ten-years trend of dengue research in Indonesia and south-east Asian countries: A bibliometric analysis. Glob Health Action (2018) 11(1):1504398. doi: 10.1080/16549716.2018.1504398
13. Baskaran S, Agarwal A, Leisegang K, Pushparaj PN, Panner Selvam MK, Henkel R. An in-depth bibliometric analysis and current perspective on Male infertility research. World J Mens Health (2021) 39(2):302–14. doi: 10.5534/wjmh.180114
14. Shen Z, Wu H, Chen Z, Hu J, Pan J, Kong J, et al. The global research of artificial intelligence on prostate cancer: A 22-year bibliometric analysis. Front Oncol (2022) 12:843735. doi: 10.3389/fonc.2022.843735
15. Ma C, Su H, Li H. Global research trends on prostate diseases and erectile dysfunction: A bibliometric and visualized study. Front Oncol (2021) 10:627891. doi: 10.3389/fonc.2020.627891
16. Hui J, He S, Liu R, Zeng Q, Zhang H, Wei A. Trends in erectile dysfunction research from 2008 to 2018: A bibliometric analysis. Int J Impot Res (2020) 32(4):409–19. doi: 10.1038/s41443-019-0161-8
17. Ma D, Guan B, Song L, Liu Q, Fan Y, Zhao L, et al. A bibliometric analysis of exosomes in cardiovascular diseases from 2001 to 2021. Front Cardiovasc Med (2021) 8:734514. doi: 10.3389/fcvm.2021.734514
18. Wu LZ, Weng YQ, Ling YX, Zhou SJ, Ding XK, Wu SQ, et al. A web of science-based scientometric analysis about mammalian target of rapamycin signaling pathway in kidney disease from 1986 to 2020. Transl Androl Urol (2021) 10(3):1006–17. doi: 10.21037/tau-20-1469
19. Zhang YD, Zhang X, Wang XY, Han DM, Du JS. Visual analysis of global research output of lymphedema based on bibliometrics. Front Oncol (2022) 12:926237. doi: 10.3389/fonc.2022.926237
20. Bermejo C, Busby JE, Spiess PE, Heller L, Pagliaro LC, Pettaway CA. Neoadjuvant chemotherapy followed by aggressive surgical consolidation for metastatic penile squamous cell carcinoma. J Urol (2007) 177(4):1335–8. doi: 10.1016/j.juro.2006.11.038
21. Spiess PE, Hernandez MS, Pettaway CA. Contemporary inguinal lymph node dissection: Minimizing complications. World J Urol (2009) 27(2):205–12. doi: 10.1007/s00345-008-0324-6
22. Pizzocaro G, Algaba F, Horenblas S, Solsona E, Tana S, van der Poel H, et al. EAU penile cancer guidelines 2009. Eur Urol (2010) 57(6):1002–12. doi: 10.1016/j.eururo.2010.01.039
23. Bleeker MC, Heideman DA, Snijders PJ, Horenblas S, Dillner J, Meijer CJ. Penile cancer: epidemiology, pathogenesis and prevention. World J Urol (2009) 27(2):141–50. doi: 10.1007/s00345-008-0302-z
24. Forman D, de Martel C, Lacey CJ, Soerjomataram I, Lortet-Tieulent J, Bruni L, et al. Global burden of human papillomavirus and related diseases. Vaccine (2012) 30 Suppl 5:F12–23. doi: 10.1016/j.vaccine.2012.07.055
25. zur Hausen H. Papillomaviruses in the causation of human cancers - a brief historical account. Virology (2009) 384(2):260–5. doi: 10.1016/j.virol.2008.11.046
26. Parkin DM, Bray F. Chapter 2: The burden of HPV-related cancers. Vaccine (2006) 24 Suppl 3:S3/11–25. doi: 10.1016/j.vaccine.2006.05.111
27. Hakenberg OW, Dräger DL, Erbersdobler A, Naumann CM, Jünemann KP, Protzel C. The diagnosis and treatment of penile cancer. Dtsch Arztebl Int (2018) 115(39):646–52. doi: 10.3238/arztebl.2018.0646
28. Pereira-Lourenço M, Vieira E Brito D, Eliseu M, Castelo-Branco N, Peralta JP, Godinho R, et al. Prognostic value of p16INK4a overexpression in penile cancer. Arch Ital Urol Androl (2020) 92(1):11–6. doi: 10.4081/aiua.2020.1.11
29. Ferreux E, Lont AP, Horenblas S, Gallee MP, Raaphorst FM, von Knebel Doeberitz M, et al. Evidence for at least three alternative mechanisms targeting the p16INK4A/cyclin D/Rb pathway in penile carcinoma, one of which is mediated by high-risk human papillomavirus. J Pathol (2003) 201(1):109–18. doi: 10.1002/path.1394
30. Barzon L, Cappellesso R, Peta E, Militello V, Sinigaglia A, Fassan M, et al. Profiling of expression of human papillomavirus-related cancer miRNAs in penile squamous cell carcinomas. Am J Pathol (2014) 184(12):3376–83. doi: 10.1016/j.ajpath.2014.08.004
31. Minhas S, Manseck A, Watya S, Hegarty PK. Penile cancer–prevention and premalignant conditions. Urology. (2010) 76(2 Suppl 1):S24–35. doi: 10.1016/j.urology.2010.04.007
32. Morris BJ, Gray RH, Castellsague X, Bosch FX, Halperin DT, Waskett JH, et al. The strong protective effect of circumcision against cancer of the penis. Adv Urol (2011) 2011:812368. doi: 10.1155/2011/812368
33. Pietrzak P, Hadway P, Corbishley CM, Watkin NA. Is the association between balanitis xerotica obliterans and penile carcinoma underestimated? BJU Int (2006) 98(1):74–6. doi: 10.1111/j.1464-410X.2006.06213.x
34. Larke NL, Thomas SL, dos Santos Silva I, Weiss HA. Male Circumcision and penile cancer: A systematic review and meta-analysis. Cancer Causes Control (2011) 22(8):1097–110. doi: 10.1007/s10552-011-9785-9
35. Ahmed ME, Khalil MI, Kamel MH, Karnes RJ, Spiess PE. Progress on management of penile cancer in 2020. Curr Treat Options Oncol (2020) 22(1):4. doi: 10.1007/s11864-020-00802-3
36. Chipollini J, Yan S, Ottenhof SR, Zhu Y, Draeger D, Baumgarten AS, et al. Surgical management of penile carcinoma in situ: Results from an international collaborative study and review of the literature. BJU Int (2018) 121(3):393–8. doi: 10.1111/bju.14037
37. Cabanas RM. An approach for the treatment of penile carcinoma. Cancer. (1977) 39(2):456–66. doi: 10.1002/1097-0142(197702)39
38. Marchioni M, Berardinelli F, De Nunzio C, Spiess P, Porpiglia F, Schips L, et al. New insight in penile cancer. Minerva Urol Nefrol (2018) 70(6):559–69. doi: 10.23736/S0393-2249.18.03215-0
39. Mir MC, Herdiman O, Bolton DM, Lawrentschuk N. The role of lymph node fine-needle aspiration in penile cancer in the sentinel node era. Adv Urol (2011) 2011:383571. doi: 10.1155/2011/383571
40. Correa AF. Technical management of inguinal lymph-nodes in penile cancer: Open versus minimal invasive. Transl Androl Urol (2021) 10(5):2264–71. doi: 10.21037/tau.2020.04.02
41. Chaudhari R, Khant SR, Patel D. Video endoscopic inguinal lymphadenectomy for radical management of inguinal nodes in patients with penile squamous cell carcinoma. Urol Ann (2016) 8(3):281–5. doi: 10.4103/0974-7796.184883
42. Zouhair A, Coucke PA, Jeanneret W, Douglas P, Do HP, Jichlinski P, et al. Radiation therapy alone or combined surgery and radiation therapy in squamous-cell carcinoma of the penis? Eur J Cancer (2001) 37(2):198–203. doi: 10.1016/s0959-8049(00)00368-3
43. Hakenberg OW, Compérat EM, Minhas S, Necchi A, Protzel C, Watkin N. EAU guidelines on penile cancer: 2014 update. Eur Urol (2015) 67(1):142–50. doi: 10.1016/j.eururo.2014.10.017
44. Pagliaro LC, Williams DL, Daliani D, Williams MB, Osai W, Kincaid M, et al. Neoadjuvant paclitaxel, ifosfamide, and cisplatin chemotherapy for metastatic penile cancer: A phase II study. J Clin Oncol (2010) 28(24):3851–7. doi: 10.1200/JCO.2010.29.5477
45. Joshi SS, Handorf E, Strauss D, Correa AF, Kutikov A, Chen DYT, et al. Treatment trends and outcomes for patients with lymph node-positive cancer of the penis. JAMA Oncol (2018) 4(5):643–9. doi: 10.1001/jamaoncol.2017.5608
46. Murrell DS, Williams JL. Radiotherapy in the treatment of carcinoma of the penis. Br J Urol (1965) 37:211–22. doi: 10.1111/j.1464-410x.1965.tb09590.x
47. Huang T, Cheng X, Chahoud J, Sarhan A, Tamboli P, Rao P, et al. Effective combinatorial immunotherapy for penile squamous cell carcinoma. Nat Commun (2020) 11(1):2124. doi: 10.1038/s41467-020-15980-9
48. Aydin AM, Hall M, Bunch BL, Branthoover H, Sannasardo Z, Mackay A, et al. Expansion of tumor-infiltrating lymphocytes (TIL) from penile cancer patients. Int Immunophar (2021) 94:107481. doi: 10.1016/j.intimp.2021.107481
49. Jacob JM, Ferry EK, Gay LM, Elvin JA, Vergilio JA, Ramkissoon S, et al. Comparative genomic profiling of refractory and metastatic penile and nonpenile cutaneous squamous cell carcinoma: Implications for selection of systemic therapy. J Urol (2019) 201(3):541–8. doi: 10.1016/j.juro.2018.09.056
Keywords: penile cancer, bibliometrics, data visualization, research status, hotspots
Citation: Deng S, Xuan Z, Feng J, Li H, Wang B, Yang Z, Xuan L, Meng F, Wang L, Xiao Y and Wang J (2023) Global research trends in penile cancer: Bibliometric and visualized analysis. Front. Oncol. 12:1091816. doi: 10.3389/fonc.2022.1091816
Received: 07 November 2022; Accepted: 12 December 2022;
Published: 06 January 2023.
Edited by:
Alessandro Tafuri, Ospedale Vito Fazzi, ItalyReviewed by:
Reza Nabavizadeh, Mayo Clinic, United StatesCopyright © 2023 Deng, Xuan, Feng, Li, Wang, Yang, Xuan, Meng, Wang, Xiao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jisheng Wang, aG91ZGVqaXNoZW5nQHNpbmEuY29t; Yangchun Xiao, eWFuZ2NodW4xMTN4aWFvQDE2My5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.