 Yuri Isaka1
Yuri Isaka1 Yayoi Ando
Yayoi Ando Yoshiaki Nakamura
Yoshiaki Nakamura
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 12 January 2023
Sec. Cancer Molecular Targets and Therapeutics
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1064944
This article is part of the Research Topic365 Days of Progress In Cancer Molecular Targets and TherapeuticsView all 23 articles
Patients with advanced duodenal carcinoma usually have a poor prognosis due to limited effective chemotherapy options. The study for genotype-directed therapy in patients with duodenal carcinoma is progressing. However, no clinical data assessing the efficacy of molecularly targeted therapy are presently available. We report the case of a 64-year-old woman who was diagnosed with anaplastic lymphocyte kinase (ALK) fusion-positive advanced duodenal carcinoma. Echinoderm microtubule associated protein like-4 (EML4)-ALK rearrangement was detected by comprehensive genomic profiling after resistance to first-line chemotherapy. The patient received alectinib, an ALK inhibitor, with marked shrinkage in primary tumor and liver metastases. She is currently being treated with alectinib for 6 months or more. This is the first report of the efficacy of alectinib in a patient with duodenal carcinoma harboring ALK fusion. Additionally, this case report suggests that the practical use of next-generation sequencing may expand optimal treatment choices in rare solid tumors, including duodenal carcinoma.
Small intestine cancer is a rare disease with a global incidence of less than 1 per 100,000 people (1). Duodenal carcinoma is the most common subtype of small intestine cancer, constituting more than 50% of small intestine cancers; it has the worst prognosis among small intestine cancers, with a one-year overall survival rate of approximately 20% (2). Although oxaliplatin or irinotecan-based systemic therapy is recommended for the treatment of the cancer in its advanced stages, there is limited evidence supporting the use of systemic therapy (3).
Multigene panel-based comprehensive genomic profiling (CGP) is widely used for the treatment of patients with malignant solid tumors. CGP enables the identification of patients with targetable alterations who may benefit from targeted therapies. A CGP study of small intestine cancer showed potentially targetable genomic alterations in the majority (91%) of cases, such as alterations in KRAS, BRAF, and ERBB2 (4). Nevertheless, no targeted therapies have been established for the treatment of advanced small intestine cancer, excluding tumor-agnostic indications, such as pembrolizumab for microsatellite instability-high or tumor mutational burden-high tumors and TRK inhibitors for NTRK fusion-positive tumors. Therefore, presenting the efficacy of target therapies for patient-specific alterations is necessary for the development of effective targeted therapies for small intestine cancer, even if only one case has been reported.
Herein, we report a patient with anaplastic lymphoma kinase (ALK) fusion-positive duodenal carcinoma who achieved an exceptional response to alectinib. The patient provided informed consent for the presentation of anonymized clinical information.
A 62-year-old female patient presenting with epigastric pain and weight loss for several weeks was referred to the Tokyo Bay Urayasu Ichikawa Medical Center. The patient had a medical history of diabetes mellitus and bronchial asthma. Upper gastrointestinal endoscopy revealed Borrmann type 2 duodenal carcinoma in the descending part of the duodenum (Figure 1A). A biopsy specimen of the primary tumor revealed poorly differentiated adenocarcinoma. Computed tomography (CT) revealed multiple lymph nodes, liver metastases, and lung metastases (Figures 1B, C). The patient was diagnosed with stage IV duodenal carcinoma (clinical stage T3N2M1, according to the TNM classification, 8th edition). She received first-line chemotherapy with modified FOLFOX6 (mFOLFOX6) regimen every 2 weeks: oxaliplatin 85 mg/m2, leucovorin 400 mg/m2, 5-FU bolus 400 mg/m2, and continuous infusion of 5-FU 2400 mg/m2 over 46 h.
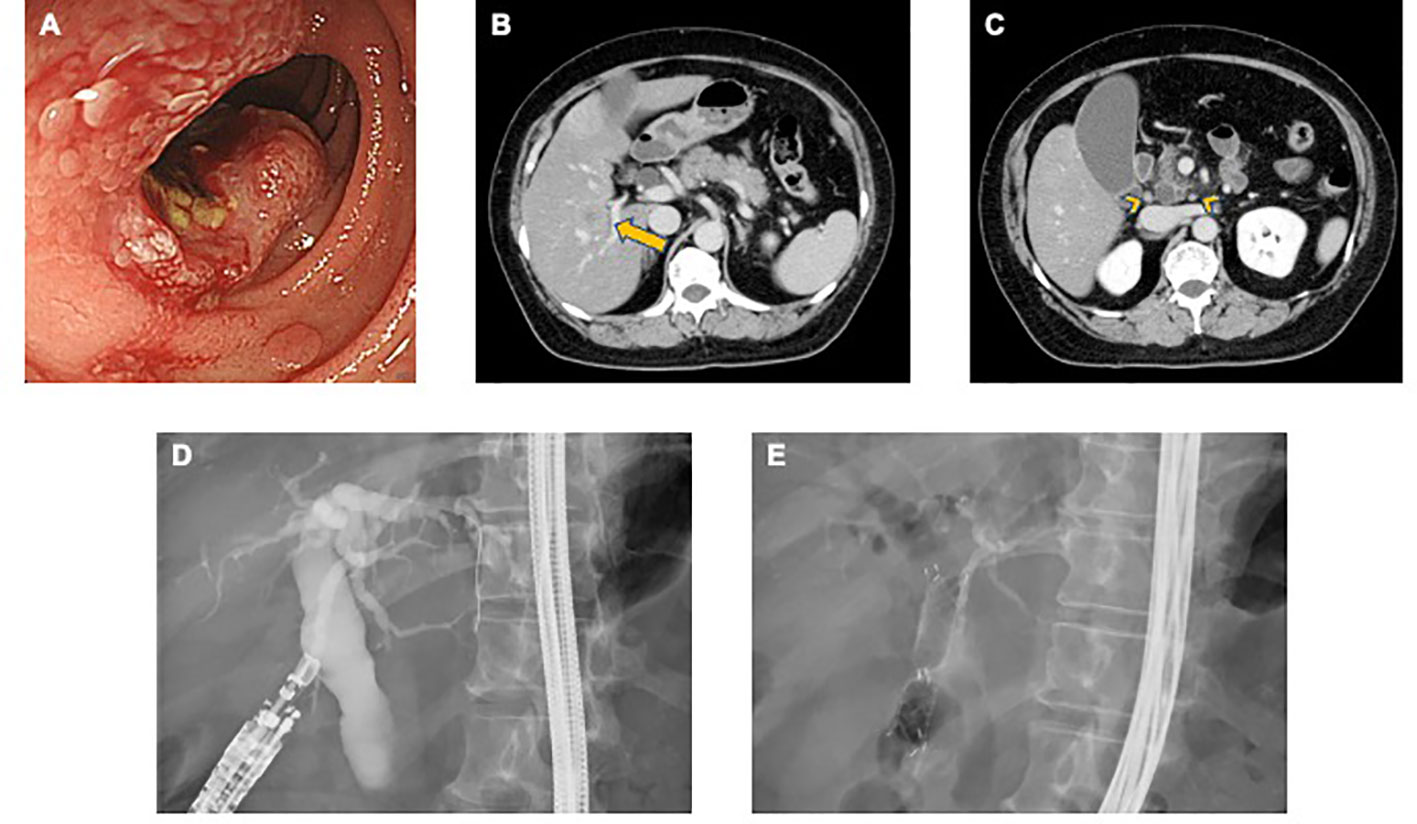
Figure 1 (A) Endoscopic findings of the duodenum reveal a type 2 tumor on the descending part. (B, C) Abdominal computed tomography shows multiple liver metastases (long arrow) and lymph nodes (arrowhead). (D) After EUS-guided puncture, contrast agent was injected into the common bile duct for cholangiogram. (E) Choledochoduodenostomy was accomplished with a fully covered metallic stent through the duodenal bulb.
However, after four cycles of mFOLFOX6, the patient was admitted to the hospital for fever and abdominal pain. Laboratory findings showed elevated C-reactive protein (CRP) (4.34 mg/dL) and liver enzyme levels (aspartate aminotransferase [AST], 284 IU/L; alanine aminotransferase [ALT], 133 IU/L; total bilirubin, 5.67 mg/dL). Abdominal CT revealed biliary tract obstruction due to the progression of duodenal carcinoma and enlargement of liver metastases. The patient was diagnosed with acute cholangitis and administered antibiotics (4/0.5g of piperacillin-tazobactam 4 times daily). Thereafter, she underwent endoscopic ultrasonography-guided choledochoduodenostomy (EUS-CDS) for biliary drainage. Guide wire was inserted through the duodenal bulb into the common bile duct and a metallic biliary stent (fully covered metallic stent 6cm) was placed using EUS-CDS (Figures 1D, E). The patient’s fever went down, and her general condition gradually improved after the drainage procedure. The laboratory data, such as CRP and liver enzyme levels, were normalized (CRP, 0.24 IU/L; AST, 31 IU/L; ALT, 15 IU/L; total bilirubin, 0.84 mg/dL).
The patient was considered to be refractory to mFOLFOX6 treatment. Subsequently, multigene panel-based CGP using FoundationOne CDx (Foundation Medicine, Cambridge, MA) was performed on the tumor tissue from the primary duodenal carcinoma. ALK fusion and echinoderm microtubule-associated protein-like 4 (EML4)-ALK rearrangement intron 19 were detected as actionable genomic alterations. Alterations in CDKN2A/B and TP53 P151R were also detected; however, both were of unknown clinical significance. Immunohistochemistry analysis showed strong ALK expression in over 80% of tumor cells (Figure 2).
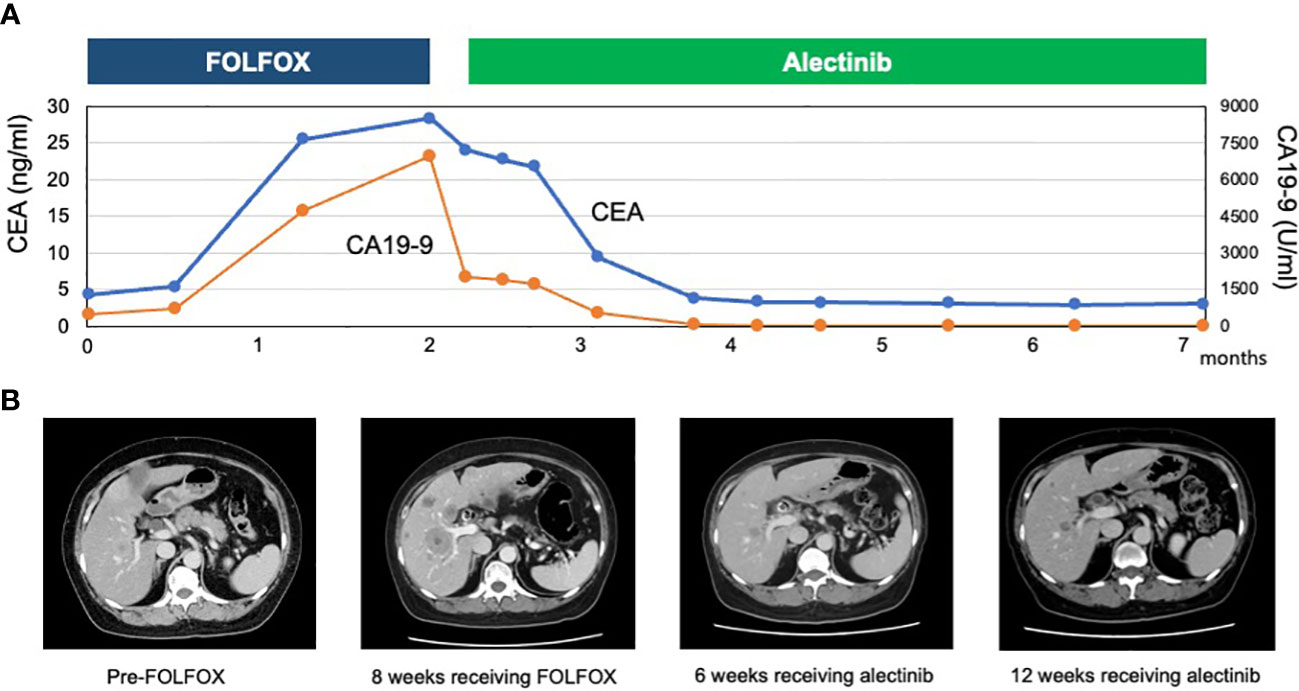
Figure 2 (A) Hematoxylin and eosin-stained biopsy specimen of the primary tumor. (B) Immunohistochemistry analysis showing strong ALK-positive staining.
Based on the result of multigene panel-based CGP, the therapeutic strategy was discussed by an intra-institutional molecular tumor board, called an expert panel, and treatment with an ALK inhibitor was recommended. the patient started 300 mg of alectinib twice daily by participating in the BELIEVE trial (NCCH1901, jRCTs031190104) according to the expert panel’s recommendation. Several days after treatment initiation, there was a gradual improvement in the patient’s general condition with an associated reduction in the severity of abdominal pain. In addition, her performance status (PS) score improved from 1 to 0. The patient had grade 1 constipation and dysgeusia due to alectinib but tolerated the dose. A CT scan on day 49 showed a significant tumor reduction of liver lesions and lymph nodes, exhibiting a partial response (57% reduction), according to the Response Evaluation Criteria in Solid Tumors version 1.1 (Figure 3). Furthermore, the patient’s serum carcinoembryonic antigen and carbohydrate antigen 19-9 levels markedly decreased. The 2-month follow-up CT imaging, the second assessment of response to alectinib, showed continuing partial response. The patient returned to her weight before she got duodenal carcinoma. As of December 2022, the patient was still being treated with alectinib without tumor progression.
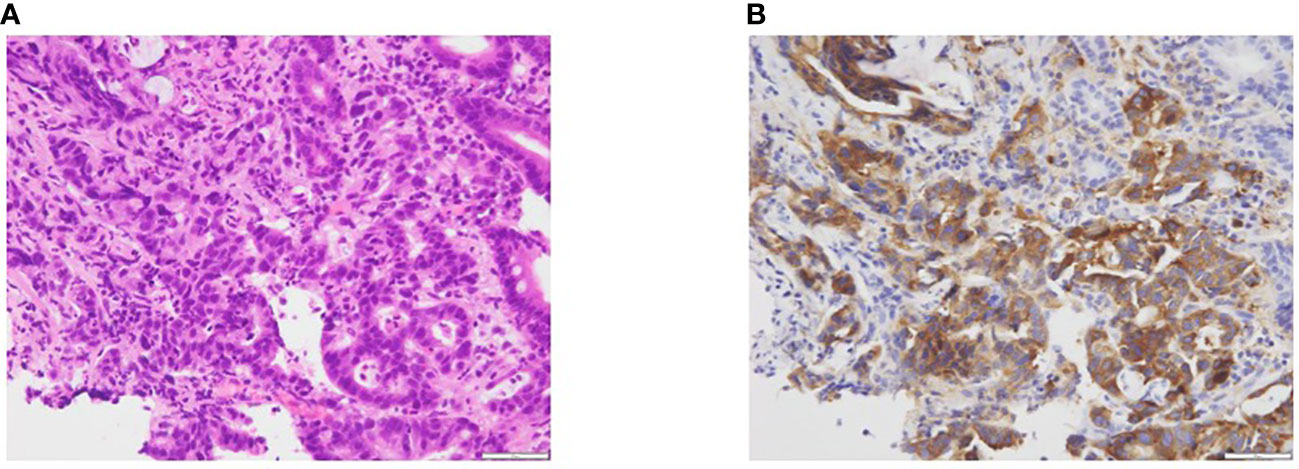
Figure 3 (A) Course of tumor markers (carcinoembryonic antigen [CEA] and carbohydrate antigen 19-9 [CA 19-9]) while receiving treatment with FOLFOX and alectinib. (B) Abdominal computed tomography showing multiple liver metastases pre-FOLFOX therapy, increased tumor volume 4 weeks after the FOLFOX therapy, and reduction of liver metastases 6 weeks after alectinib. the second follow-up CT imaging showed continuing response for liver metastases.
We present the case of a patient with ALK fusion-positive duodenal carcinoma treated with alectinib. Our patient responded remarkably to alectinib treatment. ALK is located on chromosome 2p23 and encodes a transmembrane tyrosine kinase receptor. ALK rearrangements occur in the form of a translocation with another partner gene, leading to ALK activation. This fusion activates downstream signaling pathways, such as PI3K–Akt, MEKK2/3/MEK5/ERK5, RAS-MAPK, CRKL-C3G-RAP1, JAK-STAT, and JUN (5). Most ALK alterations account for EML4-ALK fusion. In addition, other ALK fusion partners include STRN, KCNQ, KLC1, KIF5B, PPM1B, and TGF (6). ALK inhibitors, including alectinib, have shown a significant survival benefit and have been approved for patients with non-small cell lung cancer (NSCLC) harboring ALK fusions. Alectinib is one of the most active ALK inhibitor showing a significant improvement of progression-free survival compared to crizotinib (7).
ALK translocations have been detected in other cancer types such as glioblastoma, non-Hodgkin lymphoma, and breast cancer (8, 9). However, the role of EML4-ALK as a therapeutic target in these non-NSCLC cancers, including gastrointestinal cancers, is not well understood. From our extensive literature search, we summarize in Table 1 the case series of patients with gastrointestinal cancer who were treated with ALK inhibitors (10–17). A total of 23 patients with gastrointestinal cancer and ALK fusion were treated with ALK inhibitors. The median age was 50 years (range 32–87 years), and 13 patients (57%) were male. The cancer types included pancreatic (n = 10), colorectal (n = 8), gallbladder (n = 2), esophageal (n = 1), and gastric (n = 1), and only one patient with duodenal carcinoma was included. Crizotinib and alectinib were administered to 10 and 9 patients, respectively. The objective response rate to ALK inhibitors was 43.5%, and the median PFS was 6 months in patients in this literature review. The efficacy in these patients tended to be inferior to that in clinical trials involving patients with NSCLC harboring ALK fusions (7). One patient switched from crizotinib to ceritinib due to neutropenia, and no other serious adverse events were reported. Similar to our patient, the patient with duodenal carcinoma was treated with alectinib. Although the best response was stable disease, the patient achieved a PFS of 7.8 months.
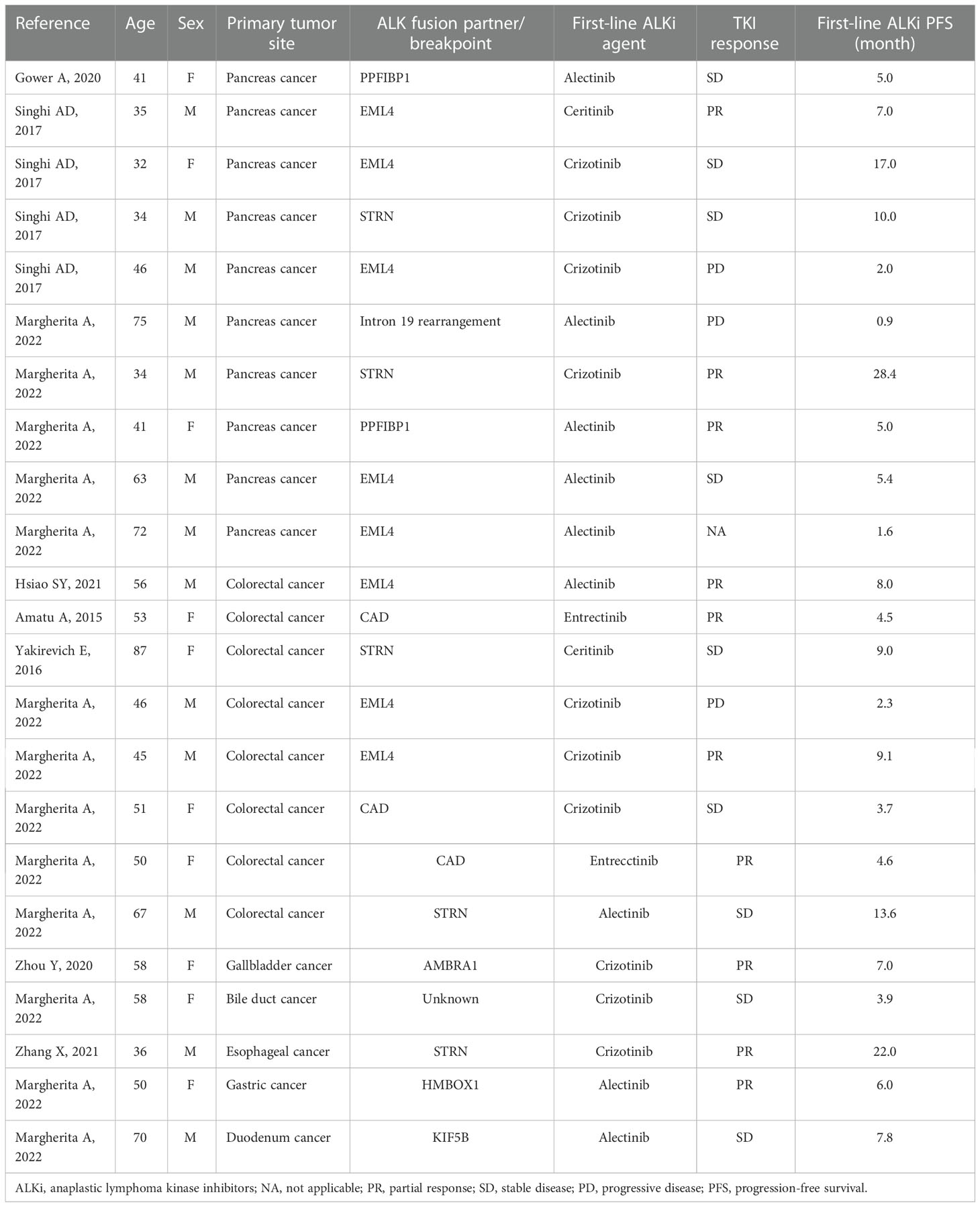
Table 1 Review of ALK inhibitors for patients with gastrointestinal cancers.
CGP studies for rare tumors identified targetable alterations, suggesting that the addition of CGP to management adds a potential line of therapy for tumors that have little or no standard of care (18). In addition, emergence of tumor-agnostic biomarkers, such as microsatellite instability-high, tumor mutational burden-high, and NTRK1/2/3 fusions, supports the use of NGS for rare tumors. Since there is no randomized trial of systemic chemotherapy in patients with duodenal carcinoma due to its rarity, the choice of chemotherapy in duodenal carcinoma is also currently limited in clinical practice. With the development of next-generation sequencing (NGS), several meaningful oncogenic pathways have been found to be altered in duodenal carcinoma. In a CGP study, alterations in ERBB2/HER2 and BRAF, microsatellite instability, and high tumor mutational burden were more frequently enriched in 317 small bowel cancers than that in gastric and colorectal cancers, and EML4-ALK fusion was identified in only one patient (0.3%) (4). Our case report encourages the use of NGS-based CGP for patients with small bowel cancers, including duodenal carcinoma, which potentially provides an opportunity of an appropriate precision medicine for these patients.
In conclusion, to our knowledge, this is the first report of an exceptional response to alectinib treatment in a patient with duodenal carcinoma harboring ALK fusion. The use of NGS to explore potentially actionable mutations in our patient paved the way for administering alectinib, which improved our patient’s quality of life and prolonged her survival after traditional chemotherapy failure. Therefore, NGS should be considered as a treatment option for patients with duodenal carcinoma. Further studies are warranted to evaluate the efficacy and safety of ALK inhibitors in patients with cancers other than NSCLC.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
YI, AkinS, and YN designed the study, collected data, performed data analysis, and wrote the manuscript. YM and YA were involved in data interpretation and critically reviewing the manuscript. AkirS was involved in testing tumor tissue as well as critically reviewing the manuscript. All authors read and approved the final manuscript.
Providing alectinib from the CHUGAI PHARMACEUTICAL CO., LTD is gratefully acknowledged.
YN reports honoraria from Chugai Pharmaceutical, Merck Biopharma, and Guardant Health AMEA and research grants from Taiho Pharmaceutical, Chugai Pharmaceutical, Guardant Health, Genomedia, Daiichi Sankyo, Seagen, and Roche Diagnostics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ALK, anaplastic lymphoma kinase; ALKi, anaplastic lymphoma kinase inhibitors; BRAF, b-Raf proto-oncogene; CGP, comprehensive genomic profiling; EML4, echinoderm microtubule associated protein like-4; ERBB2, epidermal growth factor receptor 2; KRAS, Kirsten rat sarcoma; NA, not applicable; NGS, next-generation sequencing; NSCLC, non-small cell lung cancer; NTRK, Neurotropic tropomyosin receptor kinase; ORR, objective response rate; PD, progressive disease;PFS, progression-free survival; PR, partial response; SD, stable disease; TRK, tropomyosin receptor kinase.
1. Schottenfeld D, Beebe-Dimmer JL, Vigneau FD. The epidemiology and pathogenesis of neoplasia in the small intestine. Ann Epidemiol (2009) 19:58–69. doi: 10.1016/j.annepidem.2008.10.004
2. Bojesen RD, Andersson M, Riis LB, Nielsen OH, Jess T. Incidence of, phenotypes of and survival from small bowel cancer in Denmark, 1994–2010: A population-based study. J Gastroenterol (2016) 51:891–9. doi: 10.1007/s00535-016-1171-7
3. Al BAP, Pederson K, Mahmoud M. NCCN clinical practice guidelines in oncology: Small bowel adenocarcinoma (2022) (Accessed March 9).
4. Schrock AB, Devoe CE, McWilliams R, Sun J, Aparicio T, Stephens PJ, et al. Genomic profiling of small-bowel adenocarcinoma. JAMA Oncol (2017) 3:1546–53. doi: 10.1001/jamaoncol.2017.1051
5. Hallberg B, Palmer RH. The role of the ALK receptor in cancer biology. Ann Oncol (2016) 27 Suppl 3:iii4–iii15. doi: 10.1093/annonc/mdw301
6. Della Corte CM, Viscardi G, Di Liello R, Fasano M, Martinelli E, Troiani T, et al. Role and targeting of anaplastic lymphoma kinase in cancer. Mol Cancer (2018) 17:30. doi: 10.1186/s12943-018-0776-2
7. Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim DW, et al. Alectinib versus crizotinib in untreated ALK-positive non-small-Cell lung cancer. N Engl J Med (2017) 377:829–38. doi: 10.1056/NEJMoa1704795
8. Morris SW, Kirstein MN, Valentine MB, Dittmer KG, Shapiro DN, Saltman DL, et al. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-hodgkin’s lymphoma. Science (1994) 263:1281–4. doi: 10.1126/science.8122112
9. Lin E, Li L, Guan Y, Soriano R, Rivers CS, Mohan S, et al. Exon array profiling detects EML4-ALK fusion in breast, colorectal, and non-small cell lung cancers. Mol Cancer Res (2009) 7:1466–76. doi: 10.1158/1541-7786.MCR-08-0522
10. Gower A, Golestany B, Gong J, Singhi AD, Hendifar AE. Novel ALK fusion, PPFIBP1-ALK, in pancreatic ductal adenocarcinoma responsive to alectinib and lorlatinib. JCO Precis Oncol (2020) 4:865–870. doi: 10.1200/PO.19.00365
11. Singhi AD, Ali SM, Lacy J, Hendifar A, Nguyen K, Koo J, et al. Identification of targetable ALK rearrangements in pancreatic ductal adenocarcinoma. J Natl Compr Canc Netw (2017) 15:555–62. doi: 10.6004/jnccn.2017.0058
12. Hsiao SY, He HL, Weng TS, Lin CY, Chao CM, Huang WT, et al. Colorectal cancer with EML4-ALK fusion gene response to alectinib: A case report and review of the literature. Case Rep Oncol (2021) 14:232–8. doi: 10.1159/000511069
13. Amatu A, Somaschini A, Cerea G, Bosotti R, Valtorta E, Buonandi P, et al. Novel CAD-ALK gene rearrangement is drugable by entrectinib in colorectal cancer. Br J Cancer (2015) 113:1730–4. doi: 10.1038/bjc.2015.401
14. Yakirevich E, Resnick MB, Mangray S, Wheeler M, Jackson CL, Lombardo KA, et al. Oncogenic ALK fusion in rare and aggressive subtype of colorectal adenocarcinoma as a potential therapeutic target. Clin Cancer Res (2016) 22:3831–40. doi: 10.1158/1078-0432.CCR-15-3000
15. Zhou Y, Lizaso A, Mao X, Yang N, Zhang Y. Novel AMBRA1-ALK fusion identified by next-generation sequencing in advanced gallbladder cancer responds to crizotinib: A case report. Ann Transl Med (2020) 8:1099. doi: 10.21037/atm-20-1007
16. Zhang X, Xiao XC, Zhao K, Zhao W. A case of a rare STRN-ALK fusion in esophagus adenocarcinoma exhibits excellent response to crizotinib. Clin Oncol Case Rep (2021) 4:2.
17. Ambrosini M, Del Re M, Manca P, Hendifar A, Drilon A, Harada G, et al. ALK inhibitors in patients with ALK fusion-positive GI cancers: An international data set and a molecular case series. JCO Precis Oncol (2022) 6:e2200015. doi: 10.1200/PO.22.00015
Keywords: duodenal cancer, EML4-ALK rearrangement, alectinib, next-generation sequencing, gastrointestinal cancer
Citation: Isaka Y, Sasaki A, Saito A, Motomura Y, Ando Y and Nakamura Y (2023) Exceptional response to alectinib for duodenal carcinoma with ALK fusion: A case report and literature review. Front. Oncol. 12:1064944. doi: 10.3389/fonc.2022.1064944
Received: 09 October 2022; Accepted: 20 December 2022;
Published: 12 January 2023.
Edited by:
Massimo Broggini, Mario Negri Institute for Pharmacological Research (IRCCS), ItalyReviewed by:
Ingrid Garajova, University Hospital of Parma, ItalyCopyright © 2023 Isaka, Sasaki, Saito, Motomura, Ando and Nakamura. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yoshiaki Nakamura, eW9zaGluYWtAZWFzdC5uY2MuZ28uanA=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.