
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Oncol., 21 November 2022
Sec. Hematologic Malignancies
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1033413
This article is part of the Research TopicMeasurable Residual Disease in Hematologic MalignanciesView all 12 articles
 Andrea Visentin1,2
Andrea Visentin1,2 Francesca Romana Mauro3
Francesca Romana Mauro3 Gioachino Catania4
Gioachino Catania4 Alberto Fresa5
Alberto Fresa5 Candida Vitale6
Candida Vitale6 Alessandro Sanna7
Alessandro Sanna7 Veronica Mattiello8
Veronica Mattiello8 Francesca Cibien9
Francesca Cibien9 Paolo Sportoletti10
Paolo Sportoletti10 Massimo Gentile11
Massimo Gentile11 Gian Matteo Rigolin12
Gian Matteo Rigolin12 Francesca Maria Quaglia13Roberta Murru14
Francesca Maria Quaglia13Roberta Murru14 Alessandro Gozzetti15
Alessandro Gozzetti15 Stefano Molica16Monia Marchetti4Stefano Pravato1Francesco Angotzi1Alessandro Cellini1
Stefano Molica16Monia Marchetti4Stefano Pravato1Francesco Angotzi1Alessandro Cellini1 Lydia Scarfò17
Lydia Scarfò17 Gianluigi Reda8
Gianluigi Reda8 Marta Coscia6
Marta Coscia6 Luca Laurenti5
Luca Laurenti5 Paolo Ghia17Robin Foà3
Paolo Ghia17Robin Foà3 Antonio Cuneo12Livio Trentin1,2*
Antonio Cuneo12Livio Trentin1,2*One of the main issues in the treatment of patients with chronic lymphocytic leukemia (CLL) deals with the choice between continuous or fixed-duration therapy. Continuous ibrutinib (IB), the first-in-class BTK inhibitor, and obinutuzumab-chlorambucil (G-CHL) are commonly used therapies for elderly and/or comorbid patients. No head-to-head comparison has been carried out. Within the Italian campus CLL network, we performed a retrospective study on CLL patients without TP53 disruption treated with IB or G-CHL as first-line therapy. Patients in the G-CHL arm had a higher CIRS score and the worst renal function. The overall response rates between the G-CHL and IB arms were similar, but more complete remissions (CRs) were achieved with G-CHL (p = 0.0029). After a median follow-up of 30 months, the progression-free survival (PFS, p = 0.0061) and time to next treatment (TTNT, p = 0.0043), but not overall survival (OS, p = 0.6642), were better with IB than with G-CHL. Similar results were found after propensity score matching and multivariate analysis. While PFS and TTNT were longer with IB than with G-CHL in IGHV unmutated patients (p = 0.0190 and 0.0137), they were superimposable for IGHV mutated patients (p = 0.1900 and 0.1380). In the G-CHL arm, the depth of response (79% vs. 68% vs. 38% for CR, PR and SD/PD; p < 0.0001) and measurable residual disease (MRD) influenced PFS (78% vs. 53% for undetectable MRD vs. detectable MRD, p = 0.0203). Hematological toxicities were common in the G-CHL arm, while IB was associated with higher costs. Although continuous IB provides better disease control in CLL, IGHV mutated patients and those achieving an undetectable MRD show a marked clinical and economic benefit from a fixed-duration obinutuzumab-based treatment.
The treatment landscape of chronic lymphocytic leukemia (CLL) has significantly changed in the last few years thanks to the discovery of targeted drugs directed against pivotal kinases, such as BTK [ibrutinib (IB), acalabrutinib, zanubrutinib, and pirtobrutinib] or PI3K (idelalisib and duvelisib), anti-apoptotic protein, such as BCL2 (venetoclax), and new monoclonal antibodies targeting CD19 (tafasitamab) or CD20 (1–3). Among the latter, obinutuzumab (G), a glycoengineered type II humanized anti-CD20 monoclonal antibody, displays increased direct cell death, B-cell depletion, FcγRIIIa binding, and antibody-dependent cell-mediated cytotoxicity, and it has a lower capacity to re-localize CD20 into lipid rafts upon binding and to decrease complement-dependent cytotoxicity (4, 5).
The current frontline therapy of CLL patients can be either a continuous BTK inhibitor or a fixed-duration G-based therapy (1). Choosing between the two approaches remains a challenge, since a continuous treatment might offer better disease control for some aggressive subsets of patients, balanced however by an increased rate of long-term adverse events (AEs) and costs for the health system (6–9). On the other hand, a fixed G-based therapy is administered for a short period, allowing the achievement of deep remission, which is likely to be less prone to the development of resistant clones, but requires an outpatient clinic admission (10–12).
There is no head-to-head comparison between IB and G-chlorambucil (G-CHL) both in clinical trials and in real-life studies. A cross-trial comparison between Resonate-II and CLL11 suggests that overall IB seems to be better than G-CHL (13) in terms of survival analysis and safety profile during the first 6 months of treatment (grade 3 events, 50% vs. 71%). Furthermore, there are only a few retrospective studies that have assessed the efficacy of G-CHL and measurable residual disease (MRD) in the real-life setting (14–18).
In this study, we performed a retrospective study within the Italian Campus CLL network comparing the efficacy, MRD rates, safety, and economic cost of G-CHL vs. IB in treatment-naive CLL patients. We found that IB provides better disease control in most cases, but those patients who were IGHV mutated (M-IGHV) patients and who achieved an undetectable MRD (uMRD) showed a sustained clinical and economic benefit from a fixed-duration G-CHL-based therapy.
This is a retrospective study aimed at collecting and analyzing data of CLL patients treated outside of clinical trials with frontline IB or G-CHL from their reimbursement in Italy up to December 2021. Inclusion criteria were (i) diagnosis of CLL and the need for treatment according to the iwCLL 2018 guidelines (19) and (ii) patients unfit for fludarabine-based therapy (as evaluated by the treating physician). Exclusion criteria were (i) unable to sign the informed consent, (ii) relapsed/refractory patients, and (iii) ECOG >3.
Patients received IB 420 mg daily until progression or unacceptable toxicity, while G was administered at 100 mg on day 1, 900 mg on day 2, and 1,000 mg on days 8 and 15 of the first cycle, then at 1,000 mg of day 1 of cycles 2–6. CHL was used at the dose of 0.5 mg/kg every 2 weeks or according to local policies.
Efficacy and survival analyses were focused in patients without TP53 abnormalities (including FISH 17p13 deletion and/or TP53 mutation). The primary endpoint was progression-free survival (PFS) with G-CHL vs. IB. Secondary endpoints were overall response rate (ORR), which included complete remission (CR) and partial remission with/without lymphocytosis (PR-L and PR), time to next treatment (TTNT), overall survival (OS), subgroup analyses, locally performed flow cytometry to assess measurable residual disease (MRD), AEs, and economic impact of treatments.
In order to compare the costs of the drugs, we used the ex-factory prices in Italy in 2021: €16.47 for CHL (os, 2 mg each pill, 25 pills in each box), €2,828.63 for G (ev, 1 bottle, 1,000 mg), and €7,299.59 for IB (os, 140 mg each pill, 90 pills in each box). Costs of outpatient visits (€14.50), emergency room accesses, and days of hospitalization (€530/day) were counted based on the regional prices of reimbursement. Costs of other concomitant therapies were not included.
Cytogenetics by FISH (20, 21), TP53 mutation (22), and IGHV mutational status (23, 24) were performed in all recruited patients in local accredited laboratories, and their protocols are summarized in the supplementary materials. An IGHV gene sequence homology ≥98% was considered as unmutated (U-IGHV), as opposed to mutated (M-IGHV) (25). For MRD assessed by flow cytometry, mononuclear cells were marked according to the ERIC protocol (26) or its update. Briefly, 1,000,000–2,000,000 events were acquired for each sample and analyzed by Infinicyt™. MRD was considered undetectable when <10−4 (uMRD), as opposed to detectable MRD (dMRD) (27). MRD was not performed in patients with progressive disease (PD) at response assessment.
Categorical variables were compared by the Chi-square test or the Fisher exact test, when appropriate. Continuous variables were compared using the Mann–Whitney test. PFS was calculated as start time of treatment to disease relapse or death (event) or last known follow-up (censured). TTNT was calculated according to the start time of G-CHL or IB to the beginning of a new line of therapy (event) or last known follow-up (censured). OS was calculated starting from the start of CLL treatment to death for any cause or last known follow-up. Survival analyses were performed by the Kaplan–Meier method, and the Log-rank test was used to compare survival curves between groups. The prognostic impact for the outcome variables was investigated by univariate and multiple Cox regression analysis. In Cox models, data were expressed as hazard ratios (HRs) and 95% confidence intervals (CIs). All covariates as well as all variables significantly unbalanced between the two study arms were jointly introduced into the same multiple Cox regression model (6). A propensity score matching analysis (1:1) with and without resampling was also carried out with a 0.2 caliper width. A p-value < 0.05 was considered as statistically significant. Correction for multiple comparison was also applied when indicated.
We collected data of 284 patients from 16 Italian hematological centers within the Italian CLL campus network; 104 patients received G-CHL as frontline treatment and 180 patients were treated with IB. As shown in the consort plot, we excluded 101 patients due to the presence TP53 abnormalities: 1 subject in the G-CHL arm, and 100 patients in the IB arm [the latter has been previously published (28)]. For the final analysis, we included patients without TP53 abnormalities: 103 patients treated with G-CHL and 80 patients treated with IB (Figure 1A).
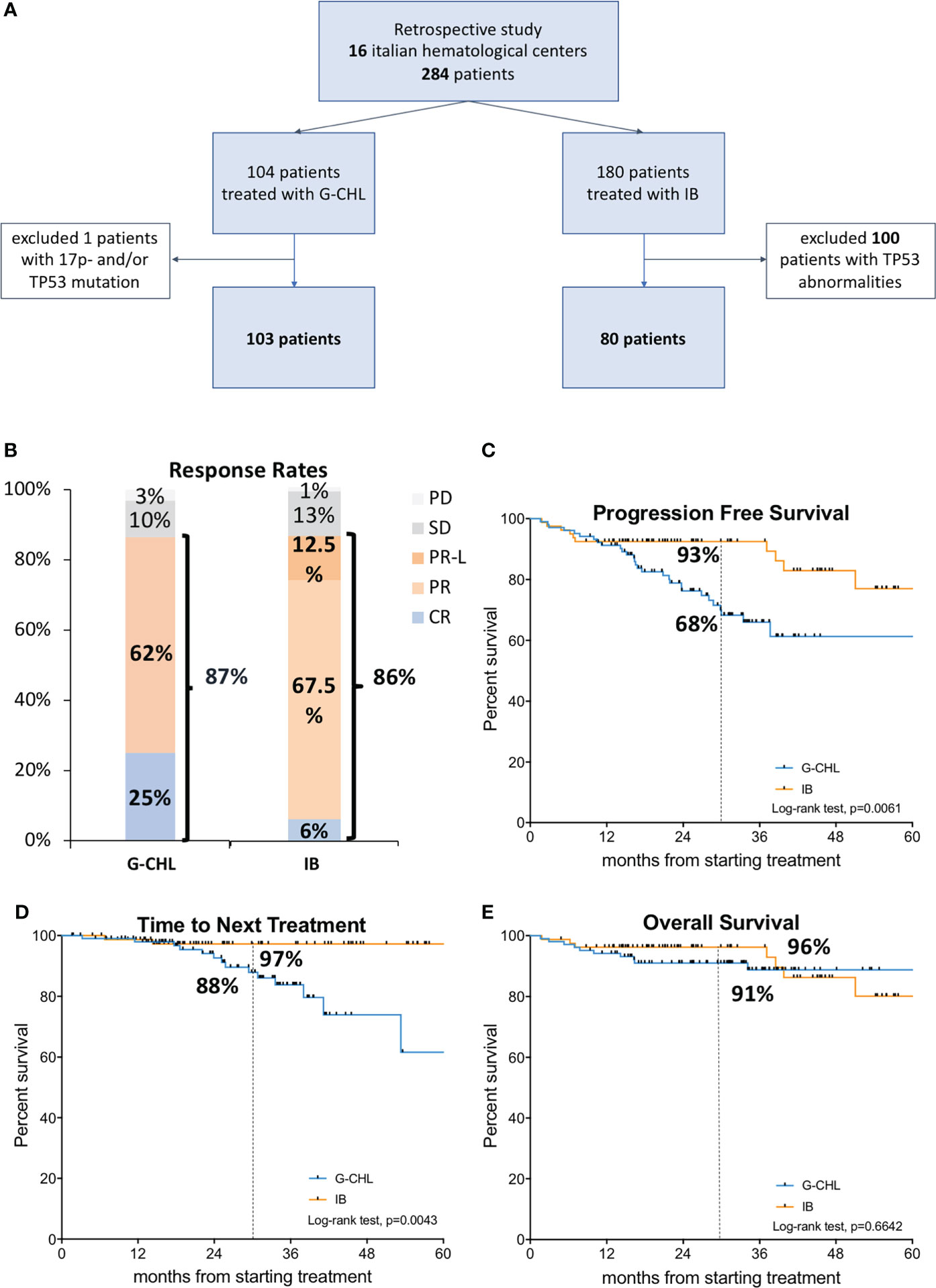
Figure 1 Study design and treatment efficacy. In the upper panel (A), the consort plot of the study is shown. Among the 284 patients recruited within 16 Italian hematological centers, 101 were excluded due to the presence of TP53 abnormalities, including deletion of 17p13 (17p-) and/or TP53 mutation. In the middle panel, on the left (B), the response rates plot for G-CHL (n = 103) and IB treatments are shown, and on the right (C), the Kaplan–Meier curve of progression-free survival of G-CHL (n = 103) vs. IB (n = 80) is displayed. In the lower panel, on the left (D), the Kaplan–Meier curves of time to next treatment is shown, and on the right (E), that of overall survival of G-CHL (n = 103) vs. IB. (n = 80) is displayed.
Patients’ characteristics are summarized in Table 1. Patients belonging to the two arms were balanced (i.e., p-values > 0.05) for age (74.7 years vs. 69.2 years), male gender (66% vs. 53%), advanced Rai stage (59% vs. 46%), increased β2-microglobulin levels (both 54%), and 11q22–23 deletion by FISH (11% vs. 16%). We observed that more patients treated with G-CHL were octogenarian (20% vs. 5%, p = 0.0038), were comorbid (median CIRS 6 vs. 4, p = 0.0009), and had an impaired kidney function (67% vs. 48%, p = 0.0061). In addition, a higher rate of U-IGHV patients received IB as frontline treatment compared to G-CHL (74% vs. 55%, p = 0.0087).
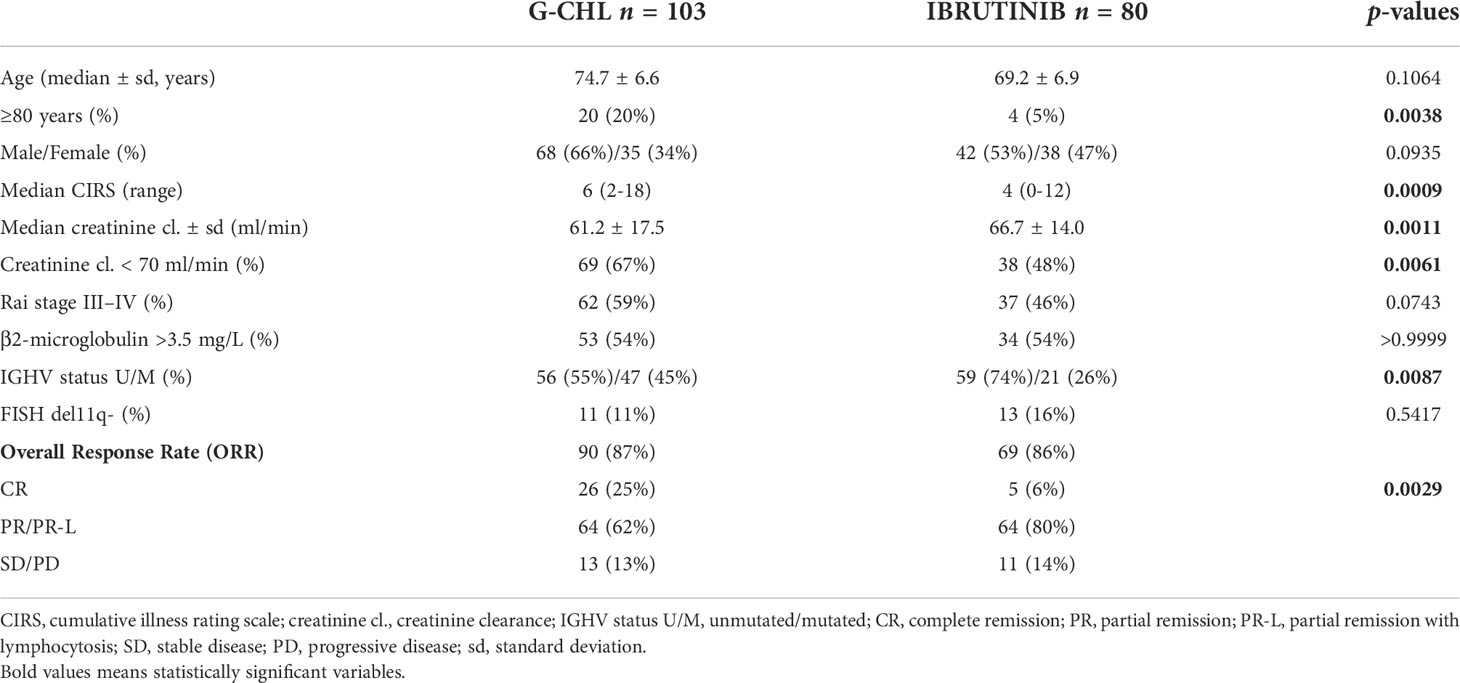
Table 1 Characteristics of recruited patients.
Eighty-three percent of patients received all the eight scheduled doses of G and chlorambucil; treatment was reduced or discontinued by 35% of patients. Forty-four percent of patients decreased the dose of IB and 79% were still under IB treatment at the last follow-up.
After 9 months of treatments (i.e., 2–3 months after the end of the G-CHL), the overall response rate (ORR) according to iwCLL criteria was 87% for G-CHL and 86% for IB (Figure 1B). Despite a similar ORR, a higher rate of patients treated with G-CHL achieved a CR (Table 1, 25% vs. 6%, p = 0.0029) according to the iwCLL criteria (i.e., normalized complete blood count, negative CLL residue in the bone marrow, and lymph node size <1.5 cm). As expected, in the IB arm, there was a higher rate of PR/PR-L (Table 1, 62% vs. 80%). Variables associated with the achievement of a CR were M-IGHV (p = 0.0093), creatinine clearance (p = 0.0271), and G-CHL therapy (p = 0.006) (Table S1).
After a median follow-up of 30 months, 24 patients have relapsed in the G-CHL arm and 3 patients have relapsed in the IB arm; 17 patients required a subsequent treatment in the G-CHL arm (14 BTK inhibitors and 3 venetoclax ± rituximab) and 2 patients in the IB arm (both venetoclax ± rituximab); 10 patients died (4 due to sepsis, 2 due to pneumonia, 2 due to CLL, and 2 due to cardiovascular events) in the G-CHL arm vs. 8 in the IB arm (3 due to cardiovascular events, 1 due to RS, 1 due to pneumonia, 1 due to sepsis, 1 due to lung cancer, and 1 due to unknown cause). None developed a Richter syndrome transformation with G-CHL, but 1 did in the IB arm.
Overall, IB was associated with better PFS and TTNT but not with OS compared to G-CHL (Figures 1C–E). The 30-month PFS was 68% and 98%, and the estimated 5-year PFS was 61% and 82% for G-CHL and IB, respectively (p = 0.0061). Patients who received IB as frontline therapy had a 2.5-fold lower risk of disease progression or death than patients in the G-CHL arm (HR 2.58, 95% CI 1.38–4.84) (Figure 1C).
The 30-month TNTT was 88% and 97%, and the estimated 5-year TTNT was 61% vs. 97% for G-CHL and IB, respectively (p = 0.0043). IB was associated with a sixfold decrease in the need of a second line of treatment (HR 6.07, 95% CI 2.39–10.44) (Figure 1D).
The 30-month OS was 91% and 96% for G-CHL and IB, respectively (p = 0.6642), without a significant difference at 5 years (88% vs. 86%) (Figure 1E).
Given that somatic hypermutation of the IGHV gene is one of the most important prognostic and predictive markers in CLL (24, 25, 29, 30), we assessed the impact of the IGHV mutational status in our patients. In U-IGHV patients, the 30-month PFS and TTNT were 72% vs. 90% (p = 0.0199, HR 2.58, 95% CI 1.19–5.57) and 82% vs. 96% (p = 0.0137, HR 5.38, 95% CI 1.73–11.69) for G-CHL and IB, respectively (Figures 2A, B). The median PFS was reached by G-CHL-treated U-IGHV patients at 37.7 months, while it was not reached by patients treated with IB. In M-IGHV patients, the 30-month PFS and TTNT were 82% vs. 96% (p = 0.1900, HR 2.54, 95% CI 0.83–7.84) and 94% vs. 100% (p = 0.1380, HR 3.93, 95% CI 0.93–13.64) for G-CHL and IB, respectively (Figures 2C, D).
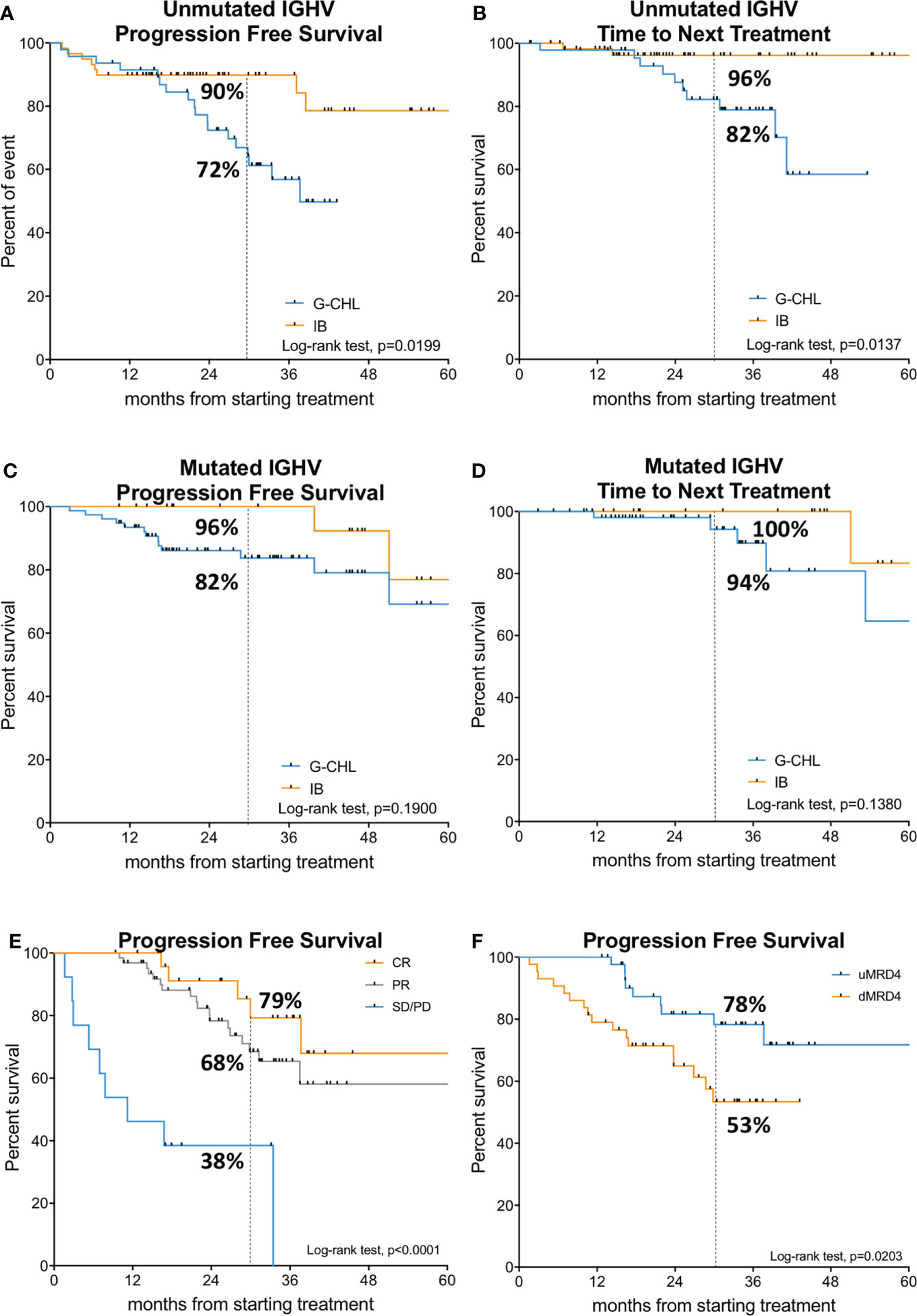
Figure 2 Survival analysis based on IGHV mutational status and deep of response. In the upper and middle panels, the Kaplan–Meier curves of progression-free survival and time to next treatment of IGHV unmutated (A, B); G-CHL, n = 56; IB, n = 59) and mutated patients (C, D); G-CHL, n = 47; IB, n = 21) are shown. In the lower panel, the Kaplan–Meier curves of progression-free survival of the G-CHL arm (n = 103) according to the iwCLL response rate on the left (E) and MRD (measurable residual disease) response on the right (n = 87) (F) are displayed.
Subsequently, we analyzed the impact of depth of clinical response and MRD on the survival of patients in the G-CHL arm. According to iwCLL response rates, the median PFS was not reached for patients in PR and CR, but it was only 11.2 months for patients who did not respond to G-CHL therapy (i.e., classified as SD or PD) (p < 0.001). The 30-month PFS was 79%, 68%, and 38% for patients who achieved CR, PR, and SD/PD, respectively (Figure 2E). TTNT was not impacted by the type of response rate (Figure S1A). Conversely, patients with SD/PD had a shorter OS (median OS, 34.1 months), while it was superimposable for patients who achieved a CR or PR (30-month OS, 95.7% vs. 94.9% vs. 61.5%, p < 0.0001, Figure S1B).
Eighty-seven (75%) patients of the G-CHL arm were studied locally for MRD by flow cytometry in the peripheral blood. No patient with PD was studied for MRD. Considering all the 103 patients treated with G-CHL at disease evaluation (i.e., month +8 or +9), 43% of patients were able to achieve a uMRD in the peripheral blood, 43% had a dMRD, and 16% were not assessed (Figure S1A). Forty-nine patients were assessed for MRD in the bone marrow, 10% achieved uMRD, 38% had detectable MRD, and 52% were not studied. Ten patients (20%) had uMRD both in the peripheral blood and in the bone marrow, 8 (16%) had uMRD in the peripheral blood but a dMRD in the bone marrow, and 31 (63%) had a dMRD both in the peripheral blood and in the bone marrow. The concordance rate between peripheral blood and bone marrow assessment was 83%. Variables associated with uMRD in the peripheral blood were an M-IGHV status (p = 0.0219) and creatinine clearance (p = 0.0311).
The 30-month PFS was significantly higher for patients achieving uMRD4, which was 78% vs. 53% for uMRD patients and dMRD patients, respectively (p = 0.0203) (Figure 2F). The median PFS was not reached. Patients with dMRD at the end of the G-CHL treatment had a 2.5-fold greater risk of progression than those with uMRD (HR 2.49, 95% CI 1.15–5.43).
TTNT was also influenced by the MRD response with an estimated median TTNT of 43.2 months for patients with dMRD, while it was not reached for those with uMRD (Figure S2D). The 30-month TTNT was 96.7% vs. 74.2% for uMRD and dMRD patients (p = 0.0211) (Figure S1G). Patients with dMRD were at threefold greater risk of starting a new treatment than those with uMRD (HR 3.4, 95% CI 1.19–9.92).
An unadjusted Cox analysis performed joining all the patients of both arms (n = 183 patients) showed that IB was significantly more effective than G-CHL in decreasing the risk of disease progression (HR 0.37, p = 0.0078) or next line of therapy (HR 0.14, p = 0.0086) in treatment-naïve patients with CLL (Table S2). To minimize the confounding effect, we adjusted the relationship between treatment arms (IB vs. G-CHL), PFS, and TTNT for all the variables skewed between arms (Table 1), as well as for all variables significantly associated with PFS and TTNT in the Cox univariate analysis (Table S2). After introducing these covariates into a multiple Cox regression model, the protective effect of IB vs. G-CHL in terms of risk of disease progression (HR 0.32, 95% CI 0.13–0.81, p = 0.0163) or next treatment (HR 0.12, 95% CI 0.03–0.61, p = 0.0102) was confirmed independently of potential confounders (Table S3).
Given the relevant differences of comorbidities and IGHV status between G-CHL and IB arms, we also performed a propensity score matched analysis (1:1). New arms were created, either with (n = 79) or without (n = 50) replacement balancing differences among treatment groups (Tables S4, S5). Even after this matched analysis, PFS and TTNT, but not OS, were longer in the IB arm than in the G-CHL arm (Figures S2A, B).
Overall, patients treated with G-CHL had more AEs than those receiving IB (2.98 vs. 1.68 AE/month of treatment/person), and less ambulatory outpatient visits (RR 0.17, 95% CI 0.15–0.20) and hospitalizations (RR 0.42, 95% CI 0.17–1.10). However, only the number of outpatient visits was statistically significant.
Ninety-eight percent of patients received premedication (paracetamol 1 g iv, anti-H1 iv, and methyl-prednisolone iv) before G infusion. Infusion-related reactions (IRRs) were recorded in 36.9% of patients, the majority being grade 1 or grade 2 and only 4.9% being grade 3. Given the retrospective nature of the study, we focus only on severe (grade ≥3) AEs. The most relevant G ≥ 3 AEs were neutropenia (35% vs. 9%, p < 0.0001), infections (13% vs. 16%, p = 0.3188), thrombocytopenia (12% vs. 1%, p = 0.0004), anemia (6% vs. 0%, p = 0.0002), and atrial fibrillation (2% vs. 9%, p = 0.0813) for G-CHL and IB, respectively. No tumor lysis syndrome occurred.
An economic analysis was carried out on 92 patients, 69 patients from the G-CHL arm and 23 patients from the IB arm. The characteristics of the economic cohort is reported in Table S6. As shown in Figure S2C, IB was associated with higher monthly costs, mainly related to the costs of the drug rather than the management of AEs. The mean total monthly cost per patient was €1,545 with G-CHL and €5,587 with IB, resulting in a mean savings per month of €4,074 (95% CI 3,267–4,881). This difference is mainly due to the savings in first-line drug cost (€1,029 vs. €5,297) and slightly to the decrease in hospitalization and/or outpatient visits (€95 vs. €290) (Figure S2C).
We gathered data from 183 CLL patients without TP53 abnormalities who were treated with continuous IB or with 6 months of G-CHL therapy as first-line therapy in the real-life setting. We found that (i) a remarkable number of patients were able to achieve a uMRD with G-CHL, and (ii) PFS and TTNT, but not OS, were better with IB than with G-CHL. The similar OS is likely due to the fact that all patients received targeted therapies with either a BTK or a BCL2 inhibitor as second-line therapy.
Furthermore, recent studies found that a high number of comorbidities, assessed by the CIRS score, have a detrimental impact of target therapies’ efficacy (31–33). In our study, despite a relevant number of comorbid patients, they showed a remarkable outcome with G-CHL.
The IGHV mutational status is one of the most important prognostic and predicted markers in CLL, being able to identify patients who might benefit most from a fixed-duration therapy (6, 10, 30, 34). When PFS and TTNT curves were stratified for the IGHV status, we found that IB improvement was significant only for the U-IGHV patients. Conversely, among M-IGHV patients after a median follow-up of 30 months, the PFS and TTNT curves of the G-CHL and IB almost overlapped, thus suggesting that fixed-duration therapy might be a key strategy in M-IGHV CLL patients in clinical practice.
G-CHL treatment was approved based on the results of the CLL11 trial, where G-CHL was compared with rituximab-CHL and CHL alone (35). The median age was 73 years (range, 39–90 years); 61% were U-IGHV, 8% harbored a del17p-, and 16% harbored a del11q-. All patients had a CIRS score >6 and/or a creatinine clearance <70 ml/min. G-CHL led to a better PFS, TTNT, and OS than the other arms. A uMRD in the peripheral blood at the end of treatment was significantly more common in patients receiving G-CHL compared to those who received rituximab-CHL (35.8% vs. 3.3%, p < 0.001). Patients with uMRD had a median PFS of 56.4 months compared to 23.9 months for patients categorized as MRD intermediate (MRD events between 10−4 and 10−2) and 13.9 months for dMRD patients (p < 0.001). MRD response was also significantly associated with a better OS (35). In our study data, we excluded patients with TP53 abnormalities (deletion or mutation) and fewer patients harbored U-IGHV and/or del11q- by FISH. The presence of fewer patients with unfavorable markers in our study might explain the higher uMRD rate (43% vs. 35.8%) and the longer PFS. Furthermore, G premedication significantly decreased IRR (66% in the CLL11 trial vs. 36.9% in our study, G3 21% in the CLL1 trial vs. 4.9% in our study).
Since CHL is a weak partner, G has been combined with continuous IB [iLLUMINATE trial (36)], continuous acalabrutinib [ELEVATE TN (37)], or the 12-month venetoclax [CLL14 (10)] and compared with G-CHL. In all these trials, the combination of G plus an oral targeted drug led to higher uMRD rates, particularly for G-venetoclax, and sustained longer PFS than G-CHL. Remarkably, IRRs were lower when G was given in combination with BTK inhibitors (36, 37).
Recently, G-CHL has been compared with the fixed-duration oral therapy IB-venetoclax (38). The GLOW trial included patients ≥65 years old or those with CIRS score ≥6 or creatinine clearance <70 ml/min. The uMRD rate in the bone marrow by next-generation sequencing was significantly higher for IB-venetoclax than for G-CHL (56% vs. 21%, p < 0.001), which led to a significantly longer PFS. The improvement in PFS with IB-venetoclax was consistent across patients ≥65 years and/or with a CIRS ≥ 6.
A041202 is a phase 3 clinical trial comparing IB ± rituximab with another chemoimmunotherapy schedule used in elderly patients, i.e., bendamustine-rituximab (BR) (39). With a median follow-up of 55 months, the median PFS was 44 months with BR and was not reached in the IB arms. An economic analysis showed that costs (associated with protocol-specified resource use) were significantly higher for patients receiving IB ± rituximab (mean $189,335 or $219,908; p < 0.0001) compared to BR (mean $51,345), driven by the higher costs for IB (40). Quality-adjusted life years were also similar between arms. In line with our data, IB provides better disease control in patients with del11q by FISH and U-IGHV, counteracted by a much higher cost of the drug. IB plus rituximab was also tested against FCR in CLL patients aged ≤70 years in the E1912 trial (41). With a median follow-up of 5.8 years, the median PFS was superior for IB-rituximab (p < 0.001). Notably, only in the E1912 trial did IB-rituximab improve not only PFS compared to FCR in patients with IGHV mutated and unmutated gene (HR 0.27, p < 0.001) but also OS (HR 0.47, p = 0.018).
The main limitation of our study is its retrospective structure and the sample size. To minimize selection and attrition biases as well as imprecise reporting of data inherent to observational studies, we asked the treating physician to report all CLL patients treated frontline with G-CHL. We analyzed the reported data, excluded cases with TP53 abnormalities, and performed computerized manual consistency checks on each case report form. Furthermore, given the differences in the clinical characteristics of patients (Table 1), particularly age and comorbidities, we applied a propensity score matched analysis with (n = 79) and without (n = 50) replacement balancing (Tables S4, S5). The small size of the samples affects the conclusions of the study. In addition, the median follow-up of 30 months does not allow us to reach conclusions about the OS.
The Italian CLL campus experience with G-CHL confirms the effectiveness of this treatment, particularly for M-IGHV patients capable of reaching a CR or a uMRD. Although MRD assessment is still not recommended by current guidelines, an increasing number of centers utilize this analysis (42). Continuous treatment with IB provides longer remission in elderly CLL patients unfit for fludarabine-based therapy (31). However, it is noteworthy that some patients can achieve long-term disease control with a less expensive fixed-duration obinutuzumab-based therapy, which may represent an option for first-line treatment in countries with economic constraints (8, 9).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Azienda Ospedale Università Paadova. The patients/participants provided their written informed consent to participate in this study.
AV designed the study, performed statistical analysis, visited patients, and wrote the article. GC, AF, CV, AS, FC, PS, MG, GR, FQ, VM, AG, MM, LS, GR, SP, FA, and ACe provided intellectual inputs and visited patients. FM, ACu, RF, SM, MC, LL, PG, and LT visited patients, provided intellectual inputs, and reviewed the article. All authors contributed to the article and approved the submitted version.
This work was supported by funds to LT from Associazione Italiana per la Ricerca sul Cancro (A.I.R.C.) projects (IG-25024), “Ricerca per Credere nella Vita” RCV odv to SP, and Roche spa to LT. Roche sponsored a fellowship to the University of Padova for collecting and analyzing the data, which was won by SP.
AV received honoraria from Janssen, Abbvie, CSL Behring, and Italfarmaco. LT received research funding from Gilead, Roche, Janssen, and Takeda, and is on the advisory board for Roche, Takeda, Abbvie, and AstraZeneca. GR received research funding from Gilead. FM is on the advisory board for Janssen, Takeda, and Abbvie. ACu is on the advisory board and speaker bureau for Roche, Abbvie, Gilead, and Janssen. RF is on the advisory board or speaker bureau for Incyte, Amgen, AstraZeneca, Janssen, Gilead, and Novartis. LL received honoraria from Abbvie, Janssen, Astra Zeneca, and Beigene. FQ plays an advisor role for AstraZeneca and Janssen, is a speaker for Janssen, and is a consultant for Sandoz. LS received honoraria from AbbVie, AstraZeneca, and Janssen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.1033413/full#supplementary-material
1. Hallek M, Al-Sawaf O. Chronic lymphocytic leukemia: 2022 update on diagnostic and therapeutic procedures. Am J Hematol (2021) 96(12):1679–705. doi: 10.1002/ajh.26367
2. Marchetti M, Vitale C, Rigolin GM, Vasile A, Visentin A, Scarfo L, et al. Old and new drugs for chronic lymphocytic leukemia: Lights and shadows of real-world evidence. J Clin Med (2022) 11(8):2076. doi: 10.3390/jcm11082076
3. Visentin A, Frezzato F, Severin F, Imbergamo S, Pravato S, Romano Gargarella L, et al. Lights and shade of next-generation Pi3k inhibitors in chronic lymphocytic leukemia. Onco Targets Ther (2020) 13:9679–88. doi: 10.2147/OTT.S268899
4. Dalla Pieta A, Cappuzzello E, Palmerini P, Ventura A, Visentin A, Astori G, et al. Innovative therapeutic strategy for b-cell malignancies that combines obinutuzumab and cytokine-induced killer cells. J Immunother Cancer (2021) 9(7):e002475. doi: 10.1136/jitc-2021-002475
5. Herter S, Herting F, Mundigl O, Waldhauer I, Weinzierl T, Fauti T, et al. Preclinical activity of the type II CD20 antibody GA101 (obinutuzumab) compared with rituximab and ofatumumab in vitro and in xenograft models. Mol Cancer Ther (2013) 12(10):2031–42. doi: 10.1158/1535-7163.MCT-12-1182
6. Morabito F, Tripepi G, Del Poeta G, Mauro FR, Reda G, Sportoletti P, et al. Effectiveness of ibrutinib as first-line therapy for chronic lymphocytic leukemia patients and indirect comparison with rituximab-bendamustine: Results of study on 486 cases outside clinical trials. Am J Hematol (2021) 96(8):E269–E72. doi: 10.1002/ajh.26201
7. Visentin A, Deodato M, Mauro FR, Autore F, Reda G, Vitale C, et al. A scoring system to predict the risk of atrial fibrillation in chronic lymphocytic leukemia. Hematol Oncol (2019) 37(4):508–12. doi: 10.1002/hon.2655
8. Cuneo A, Cavazzini F, Cavallari M, Foa R, Rigolin GM. Optimal management of chronic lymphocytic leukemia and economic constraints. Cancer J (2021) 27(4):320–7. doi: 10.1097/PPO.0000000000000531
9. Patel KK, Isufi I, Kothari S, Davidoff AJ, Gross CP, Huntington SF. Cost-effectiveness of first-line vs third-line ibrutinib in patients with untreated chronic lymphocytic leukemia. Blood (2020) 136(17):1946–55. doi: 10.1182/blood.2020004922
10. Al-Sawaf O, Zhang C, Lu T, Liao MZ, Panchal A, Robrecht S, et al. Minimal residual disease dynamics after venetoclax-obinutuzumab treatment: Extended off-treatment follow-up from the randomized CLL14 study. J Clin Oncol (2021) 39(36):4049–60. doi: 10.1200/JCO.21.01181
11. Deodato M, Frustaci AM, Sportoletti P, Laurenti L, Murru R, Visentin A, et al. How COVID-19 pandemic changed our attitude to venetoclax-based treatment in chronic lymphocytic leukemia. Leuk Lympho (2022) 63(8):1985–8. doi: 10.1080/10428194.2022.2053532
12. Ferrarini I, Rigo A, Visco C. The mitochondrial anti-apoptotic dependencies of hematologic malignancies: from disease biology to advances in precision medicine. Haematologica (2022) 107(4):790–802. doi: 10.3324/haematol.2021.280201
13. Tedeschi A, Greil R, Demirkan F, Robak T, Moreno C, Barr PM, et al. A cross-trial comparison of single-agent ibrutinib versus chlorambucil-obinutuzumab in previously untreated patients with chronic lymphocytic leukemia or small lymphocytic lymphoma. Haematologica (2020) 105(4):e164–e8. doi: 10.3324/haematol.2019.223743
14. Fresa A, Autore F, Piciocchi A, Catania G, Visentin A, Tomasso A, et al. Relative dose intensity of obinutuzumab-chlorambucil in chronic lymphocytic leukemia: a multicenter Italian study. Blood Adv (2022) 6(13):3875–8. doi: 10.1182/bloodadvances.2022006964
15. Bourrier N, Landego I, Bucher O, Squires M, Streu E, Hibbert I, et al. Real world risk of infusion reactions and effectiveness of front-line obinutuzumab plus chlorambucil compared with other frontline treatments for chronic lymphocytic leukemia. BMC Cancer (2022) 22(1):148. doi: 10.1186/s12885-022-09256-2
16. Panovska A, Nemcova L, Nekvindova L, Spacek M, Simkovic M, Papajik T, et al. Real-world data on efficacy and safety of obinutuzumab plus chlorambucil, rituximab plus chlorambucil, and rituximab plus bendamustine in the frontline treatment of chronic lymphocytic leukemia: The GO-CLLEAR study by the Czech CLL study group. Hematol Oncol (2020) 38(4):509–16. doi: 10.1002/hon.2744
17. Dlugosz-Danecka M, Jurczak W, Latka-Cabala E, Morawska M, Gawronski K, Wisniewska A, et al. Efficacy and safety of the obinutuzumab-chlorambucil combination in the frontline treatment of elderly CLL patients with comorbidities - polish adult leukemia group (PALG) real-life analysis. Pol Arch Intern Med (2018) 128(7-8):421–6. doi: 10.20452/pamw.4294
18. Herishanu Y, Shaulov A, Fineman R, Basic-Kinda S, Aviv A, Wasik-Szczepanek E, et al. Frontline treatment with the combination obinutuzumab +/- chlorambucil for chronic lymphocytic leukemia outside clinical trials: Results of a multinational, multicenter study by ERIC and the Israeli CLL study group. Am J Hematol (2020) 95(6):604–11. doi: 10.1002/ajh.25766
19. Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G, Dohner H, et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood (2018) 131(25):2745–60. doi: 10.1182/blood-2017-09-806398
20. Visentin A, Bonaldi L, Rigolin GM, Mauro FR, Martines A, Frezzato F, et al. The complex karyotype landscape in chronic lymphocytic leukemia allows the refinement of the risk of Richter syndrome transformation. Haematologica (2022) 107(4):868–76.
21. Rigolin GM, Saccenti E, Guardalben E, Cavallari M, Formigaro L, Zagatti B, et al. In chronic lymphocytic leukaemia with complex karyotype, major structural abnormalities identify a subset of patients with inferior outcome and distinct biological characteristics. Br J Haematol (2018) 181(2):229–33. doi: 10.1111/bjh.15174
22. Pospisilova S, Gonzalez D, Malcikova J, Trbusek M, Rossi D, Kater AP, et al. ERIC recommendations on TP53 mutation analysis in chronic lymphocytic leukemia. Leukemia (2012) 26(7):1458–61. doi: 10.1038/leu.2012.25
23. Visentin A, Bonaldi L, Rigolin GM, Mauro FR, Martines A, Frezzato F, et al. The combination of complex karyotype subtypes and IGHV mutational status identifies new prognostic and predictive groups in chronic lymphocytic leukaemia. Br J Cancer (2019) 121(2):150–6. doi: 10.1038/s41416-019-0502-x
24. Agathangelidis A, Chatzidimitriou A, Gemenetzi K, Giudicelli V, Karypidou M, Plevova K, et al. Higher-order connections between stereotyped subsets: implications for improved patient classification in CLL. Blood (2021) 137(10):1365–76. doi: 10.1182/blood.2020007039
25. Agathangelidis A, Chatzidimitriou A, Chatzikonstantinou T, Tresoldi C, Davis Z, Giudicelli V, et al. Immunoglobulin gene sequence analysis in chronic lymphocytic leukemia: the 2022 update of the recommendations by ERIC, the European research initiative on CLL. Leukemia (2022) 36(8):1961–8. doi: 10.1038/s41375-022-01604-2
26. Rawstron AC, Fazi C, Agathangelidis A, Villamor N, Letestu R, Nomdedeu J, et al. A complementary role of multiparameter flow cytometry and high-throughput sequencing for minimal residual disease detection in chronic lymphocytic leukemia: an European research initiative on CLL study. Leukemia (2016) 30(4):929–36. doi: 10.1038/leu.2015.313
27. Wierda WG, Rawstron A, Cymbalista F, Badoux X, Rossi D, Brown JR, et al. Measurable residual disease in chronic lymphocytic leukemia: expert review and consensus recommendations. Leukemia (2021) 35(11):3059–72. doi: 10.1038/s41375-021-01241-1
28. Visentin A, Mauro FR, Cibien F, Vitale C, Reda G, Fresa A, et al. Continuous treatment with ibrutinib in 100 untreated patients with TP53 disrupted chronic lymphocytic leukemia: A real-life campus CLL study. Am J Hematol (2022) 97(3):E95–E9. doi: 10.1002/ajh.26437
29. Visentin A, Facco M, Gurrieri C, Pagnin E, Martini V, Imbergamo S, et al. Prognostic and predictive effect of IGHV mutational status and load in chronic lymphocytic leukemia: Focus on FCR and BR treatments. Clin Lymph Myeloma Leuk (2019) 19(10):678–85 e4. doi: 10.1016/j.clml.2019.03.002
30. Rossi D, Terzi-di-Bergamo L, De Paoli L, Cerri M, Ghilardi G, Chiarenza A, et al. Molecular prediction of durable remission after first-line fludarabine-cyclophosphamide-rituximab in chronic lymphocytic leukemia. Blood (2015) 126(16):1921–4. doi: 10.1182/blood-2015-05-647925
31. Reda G, Mattiello V, Frustaci AM, Visentin A, Mauro FR, Innocenti I, et al. Ibrutinib in patients over 80 with chronic lymphocytic leukemia: a multicenter Italian cohort. Blood Adv (2022). doi: 10.1182/bloodadvances.2022007619
32. Tedeschi A, Frustaci AM, Mauro FR, Chiarenza A, Coscia M, Ciolli S, et al. Do age, fitness, and concomitant medications influence management and outcomes of patients with CLL treated with ibrutinib? Blood Adv (2021) 5(24):5490–500. doi: 10.1182/bloodadvances.2021004824
33. Gordon MJ, Churnetski M, Alqahtani H, Rivera X, Kittai A, Amrock SM, et al. Comorbidities predict inferior outcomes in chronic lymphocytic leukemia treated with ibrutinib. Cancer (2018) 124(15):3192–200. doi: 10.1002/cncr.31554
34. Molica S, Giannarelli D, Visentin A, Reda G, Sportoletti P, Frustaci AM, et al. Prediction of outcomes in chronic lymphocytic leukemia patients treated with ibrutinib: Validation of current prognostic models and development of a simplified three-factor model. Am J Hematol (2022) 97(5):E176–E80. doi: 10.1002/ajh.26502
35. Langerak AW, Ritgen M, Goede V, Robrecht S, Bahlo J, Fischer K, et al. Prognostic value of MRD in CLL patients with comorbidities receiving chlorambucil plus obinutuzumab or rituximab. Blood (2019) 133(5):494–7. doi: 10.1182/blood-2018-03-839688
36. Moreno C, Greil R, Demirkan F, Tedeschi A, Anz B, Larratt L, et al. First-line treatment of chronic lymphocytic leukemia with ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab: final analysis of the randomized, phase 3 iLLUMINATE trial. Haematologica (2022) 107(9):2108–20. doi: 10.3324/haematol.2021.279012
37. Sharman JP, Egyed M, Jurczak W, Skarbnik A, Pagel JM, Flinn IW, et al. Efficacy and safety in a 4-year follow-up of the ELEVATE-TN study comparing acalabrutinib with or without obinutuzumab versus obinutuzumab plus chlorambucil in treatment-naive chronic lymphocytic leukemia. Leukemia (2022) 36(4):1171–5. doi: 10.1038/s41375-021-01485-x
38. Kater AP, Owen C, Moreno C, Follows G, Munir T, Levin M-D, et al. Fixed-Duration ibrutinib-venetoclax in patients with chronic lymphocytic leukemia and comorbidities. NEJM Evidence (2022) 1(7). doi: 10.1056/EVIDoa2200006
39. Woyach JA, Ruppert AS, Heerema NA, Zhao W, Booth AM, Ding W, et al. Long-term results of alliance A041202 show continued advantage of ibrutinib-based regimens compared with bendamustine plus rituximab (BR) chemoimmunotherapy. Blood (2021) 138(Supplement 1):639. doi: 10.1182/blood-2021-153146
40. Cheung MC, Mittmann N, Owen C, Abdel-Samad N, Fraser GAM, Lam S, et al. A prospective economic analysis of early outcome data from the alliance A041202/ CCTG CLC.2 randomized phase III trial of bendamustine-rituximab compared with ibrutinib-based regimens in untreated older patients with chronic lymphocytic leukemia. Clin Lymph Myeloma Leuk (2021) 21(11):766–74.
41. Shanafelt TD, Wang XV, Hanson CA, Paietta EM, O'Brien S, Barrientos J, et al. Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: updated results of the E1912 trial. Blood (2022) 140(2):112–20. doi: 10.1182/blood.2021014960
Keywords: obinutizumab, ibrutinib, treatment-naive, MRD, economic impact
Citation: Visentin A, Mauro FR, Catania G, Fresa A, Vitale C, Sanna A, Mattiello V, Cibien F, Sportoletti P, Gentile M, Rigolin GM, Quaglia FM, Murru R, Gozzetti A, Molica S, Marchetti M, Pravato S, Angotzi F, Cellini A, Scarfò L, Reda G, Coscia M, Laurenti L, Ghia P, Foà R, Cuneo A and Trentin L (2022) Obinutuzumab plus chlorambucil versus ibrutinib in previously untreated chronic lymphocytic leukemia patients without TP53 disruptions: A real-life CLL campus study. Front. Oncol. 12:1033413. doi: 10.3389/fonc.2022.1033413
Received: 31 August 2022; Accepted: 20 October 2022;
Published: 21 November 2022.
Edited by:
Sara Galimberti, University of Pisa, ItalyReviewed by:
Marina Martello, University of Bologna, ItalyCopyright © 2022 Visentin, Mauro, Catania, Fresa, Vitale, Sanna, Mattiello, Cibien, Sportoletti, Gentile, Rigolin, Quaglia, Murru, Gozzetti, Molica, Marchetti, Pravato, Angotzi, Cellini, Scarfò, Reda, Coscia, Laurenti, Ghia, Foà, Cuneo and Trentin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Livio Trentin, bGl2aW8udHJlbnRpbkB1bmlwZC5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.