
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 25 November 2022
Sec. Head and Neck Cancer
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1032471
This article is part of the Research Topic Head and Neck Cancer in the Elderly View all 8 articles
 Elena Colombo1†*
Elena Colombo1†* Charlotte Van Lierde2†
Charlotte Van Lierde2† Alexandra Zlate3
Alexandra Zlate3 Alexandra Jensen4
Alexandra Jensen4 Gemma Gatta5
Gemma Gatta5 Fabio Didonè5
Fabio Didonè5 Lisa F. Licitra1,6
Lisa F. Licitra1,6 Vincent Grégoire3‡
Vincent Grégoire3‡ Vander Vander Poorten2‡
Vander Vander Poorten2‡ Laura D. Locati1‡
Laura D. Locati1‡Salivary gland carcinomas (SGCs) are the most heterogeneous subgroup of head and neck malignant tumors, accounting for more than 20 subtypes. The median age of SGC diagnosis is expected to rise in the following decades, leading to crucial clinical challenges in geriatric oncology. Elderly patients, in comparison with patients aged below 65 years, are generally considered less amenable to receiving state-of-the-art curative treatments for localized disease, such as surgery and radiation/particle therapy. In the advanced setting, chemotherapy regimens are often dampened by the consideration of cardiovascular and renal comorbidities. Nevertheless, the elderly population encompasses a broad spectrum of functionalities. In the last decades, some screening tools (e.g. the G8 questionnaire) have been developed to identify those subjects who should receive a multidimensional geriatric assessment, to answer the question about the feasibility of complex treatments. In the present article, we discuss the most frequent SGC histologies diagnosed in the elderly population and the relative 5-years survival outcomes based on the most recent data from the Surveillance, Epidemiology, and End Results (SEER) Program. Moreover, we review the therapeutic strategies currently available for locoregionally advanced and metastatic disease, taking into account the recent advances in precision oncology. The synergy between the Multidisciplinary Tumor Board and the Geriatrician aims to shape the most appropriate treatment pathway for each elderly patient, focusing on global functionality instead of the sole chronological age.
The global population is ageing at a fast pace. In 2050, the proportion of the world’s population over 60 years is expected to reach 22%, almost doubling the 12% of 2015 (1). The World Health Organization (WHO) defines elderly the subjects aged beyond 65 years (65y+), a highly heterogeneous group of people in terms of performance status, comorbidities and vulnerabilities.
The variability of elderly patients poses significant challenges to the clinical practice of oncology (2, 3), including the context of rare cancers, where few clinical trials are available and study populations are less numerous (4). Clinicians have few tools to estimate the risk/benefit balance of treatments for elderly patients, since an age subgroup-specific analysis is unlikely feasible. However, the differences in survival outcomes from rare cancers in the United States and Europe are more evident for age group rather than for cancer type, with the 65y+ subjects at high risk of poor outcome (5).
The level of clinical challenge is major for patients with rare tumors requiring a multidisciplinary approach, as in the case of head and neck cancers (HNCs). In patients with HNCs, both age and comorbidities influence the overall survival (OS), possibly because of advanced tumor stage, inability to perform multimodal treatments and/or non cancer-related causes of death (6). Moreover, the consideration of chronological age and mild/moderate comorbidities may result in the selection of substandard treatments, which are associated to lower OS and cancer-specific survival, in comparison with the state-of-the-art (7). However, HNCs encompass a heterogeneous group of cancers with different histologies and clinical courses. This review is focused on salivary gland cancers (SGCs) in elderly patients, including the most recent epidemiological findings, the current treatment approaches and the future perspectives.
SGCs are rare cancers, accounting for less than 5% of all malignancies of the cervicofacial region. The WHO Global Cancer Observatory (Globocan) reported 53.583 new cases of SGCs diagnosed in 2020 worldwide, 43% occurring in the elderly, and causing 12.339 cancer-specific deaths, with a male-to-female ratio of 1.3:1. In the next two decades, the new diagnoses in the elderly age group are expected to account for 80% of the total SGCs diagnoses; similarly, SGCs in this group are expected to cause the 88% of all SGC-specific deaths (8). The impact of SGCs in the elderly is going to become a crucial health issue, thus research efforts should be encouraged to identify the main risk factors and the most effective therapeutic strategies for this multifaceted population.
The ICARE study, a multicenter, population-based, case-control study recently conducted in France on 73 SCGs and 3555 controls, reported that the main risk factors for SGCs were related to a previous history of cervicofacial radiation therapy (RT), either for HNCs (odds ratio, OR = 31.74, 95% CI 2.5 – 405.2) or hematological cancers (OR = 5.1, 95% CI 0.6 – 46.2), and professional exposure to chemicals, such as metals in the plumbing industry, electrical equipment and nickel compounds/alloy. In the ICARE study, the mean age at diagnosis was 56.9 years, with 27% of the population aged more than 62 years (9). Another case-control study conducted in Japan showed that heavy smokers were at higher risk of developing SGCs, compared with never smokers (OR = 3.45, 95% CI 2.06-12.87; p < 0.001); 43.7% of the study population was more than 60 years of age (10).
On the basis of the current literature, it is unknown whether the onset of SGCs in the elderly population could be sustained by risk factors that are different from those of younger patients. However, some differences can be observed not only in the survival outcomes, but also in the histotype-specific incidence. The clinical management of elderly patients has improved in the last decades, due to new clinical tools of geriatric assessment. The Comprehensive Geriatric Assessment (CGA) is a method for identifying elderly patients at risk of life-threatening events during oncological therapy by analyzing several domains (functionality, nutrition, cognition, psychological state, social support, comorbidities, medication review, and geriatric syndromes). It can predict functional decline and also be used to adapt cancer treatment, as demonstrated by the ELCAPA study (11). Since CGA is a time-consuming tool, in the last decade various screening instruments were adopted, in order to refine the selection of vulnerable patients who could benefit from a CGA. The G8 questionnaire, based on seven items from the Mini Nutritional Assessment (MNA) and age as the 8th item, uses a scoring system from 0 to 17, where a result below the cut-off value of 14 identifies those patients who should be addressed to CGA. G8 has been validated in multicenter cohort studies (12, 13) and also in a population of elderly HNSCC patients treated with chemo(radio)therapy (14). G8 has high sensitivity, but a proportion of patients with G8 scores ≤14 has no major vulnerabilities detected by the CGA. Moreover, the level of G8 specificity may vary according to the primary tumor sites, as demonstrated by the ELCAPA-02 study, which included few patients with HNC (n=4) (15). An optimized version of the G8 was recently proposed, including six independent predictors for abnormal CGA: weight loss, cognition/mood, performance status, self-rated health status, polypharmacy (≥ 6 medications per day), and history of heart failure/coronary heart disease (16).
Focusing on the treatment of patients with SGCs, the recently released ASCO Guidelines recommend taking clinical decisions in the context of a multidisciplinary tumor board, focusing on histology, disease burden and site of tumor deposits, potential treatment-related toxicities, patient’s overall health, comorbidities and function (17). Comorbidities are the Achilles’ heel of elderly patients with cancer, however, patients with SGCs have less comorbidities compared to those with other HNCs. In a retrospectively analyzed cohort of 666 patients with SGCs, OS – but not disease-free survival (DFS) – was influenced by the Adult Comorbidity Evaluation index (ACE-27). The ACE-27 scoring was affected by age and gender, possibly influenced by lifestyle. In that study, patients with comorbidities were more likely to receive a non-surgical treatment, i.e. exclusive RT, or no treatment at all, achieving a worse outcome. The impact of comorbidities was not related to the histological subtypes, except for the squamous cell histology. Interestingly, DFS was not influenced by comorbidities, indicating that a proper treatment should be delivered as much as possible, even in elderly patients with comorbidities (18).
Another study focused on the influence of age and comorbidities on the outcome using the Age-Adjusted Charlson Comorbidity Index (ACCI) scoring system on a series of 109 patients with a median age of 69 years, treated for major SGCs. Comorbidities, but not age, were an independent prognostic factor for both OS and disease-specific survival (19). A Danish study performed in 871 patients with SGC treated between 1990 and 2005, reported a poorer survival in the population group over 70 years old (n=282), possibly explained by the more advanced disease stages, poorer performance status at the time of diagnosis, more high-grade histological subtypes such as adenocarcinoma not otherwise specified (NOS) and carcinoma ex-pleomorphic adenoma (ca ex-PA). Despite these aggressive clinical features, elderly patients received surgery plus RT only in 45% of cases, while 54% received a suboptimal active treatment, either surgery alone (38%) or exclusive RT (10%), or best supportive care (6%) (20).
Malignant tumors of the major salivary glands (MSG) can be found in 15-32% of parotid, 41-45% of submandibular and 70-90% of sublingual masses. The minor salivary glands (mSG) are located beneath the mucosa of the oral cavity, palate, paranasal sinuses, pharynx, larynx, trachea and bronchi, mostly concentrated in the buccal, labial, palatal, and lingual regions. Almost 50% of the tumors arising from mSG are malignant (21). The staging of MSG is currently based on the 8th edition of the American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) tumor/node/metastasis (TNM) System, while mSGCs are staged according to the AJCC/UICC system for the primary site (22). In patients with a suspicion of SGC, the ASCO Guidelines recommend performing an imaging workup including neck ultrasound, computed tomography (CT) with intravenous contrast, and/or magnetic resonance imaging (MRI) of the neck and primary site (Recommendation 1.1) (17). An MRI with diffusion sequence of the neck and skull base is recommended in case of suspicious perineural spread and/or skull base involvement (R1.3), and an MRI brain scan could be considered in case of high-grade SGCs or if suspected meningeal spread. A CT scan should be performed in case of possible involvement of the adjacent bone (R1.2). An FDG-PET/CT scan from the skull base to mid-thighs may be performed for tumors with high-grade features, while in low-grade histological subtypes it could deliver false negative results (R1.4). For locoregionally advanced cases, a contrast-enhanced chest-abdomen CT scan is recommended to complete the clinical staging. Intracranial metastases are infrequent at diagnosis; however, they may occur especially in case of high-grade SGC (23).
Beside the multiplicity of anatomical subsites, SGCs harbor a wide heterogeneity of histologies, which are associated to different age incidence, clinical behavior, treatments and prognosis. Each glandular segment can be the site of origin of SGCs (Figure 1). The WHO 2017 Classification of Salivary Gland Tumors (4th Edition) classified more than 20 malignant subtypes of epithelial SGCs, including a new entity, the secretory carcinoma (SC), formerly known as mammary analogue SC (MASC) (24, 25). Moreover, the recently released Armed Forces Institute of Pathology (AFIP) Atlas of SGC Tumor Pathology provides an indepth analysis of the morphological and molecular features of both benign and malignant salivary gland tumors (26).
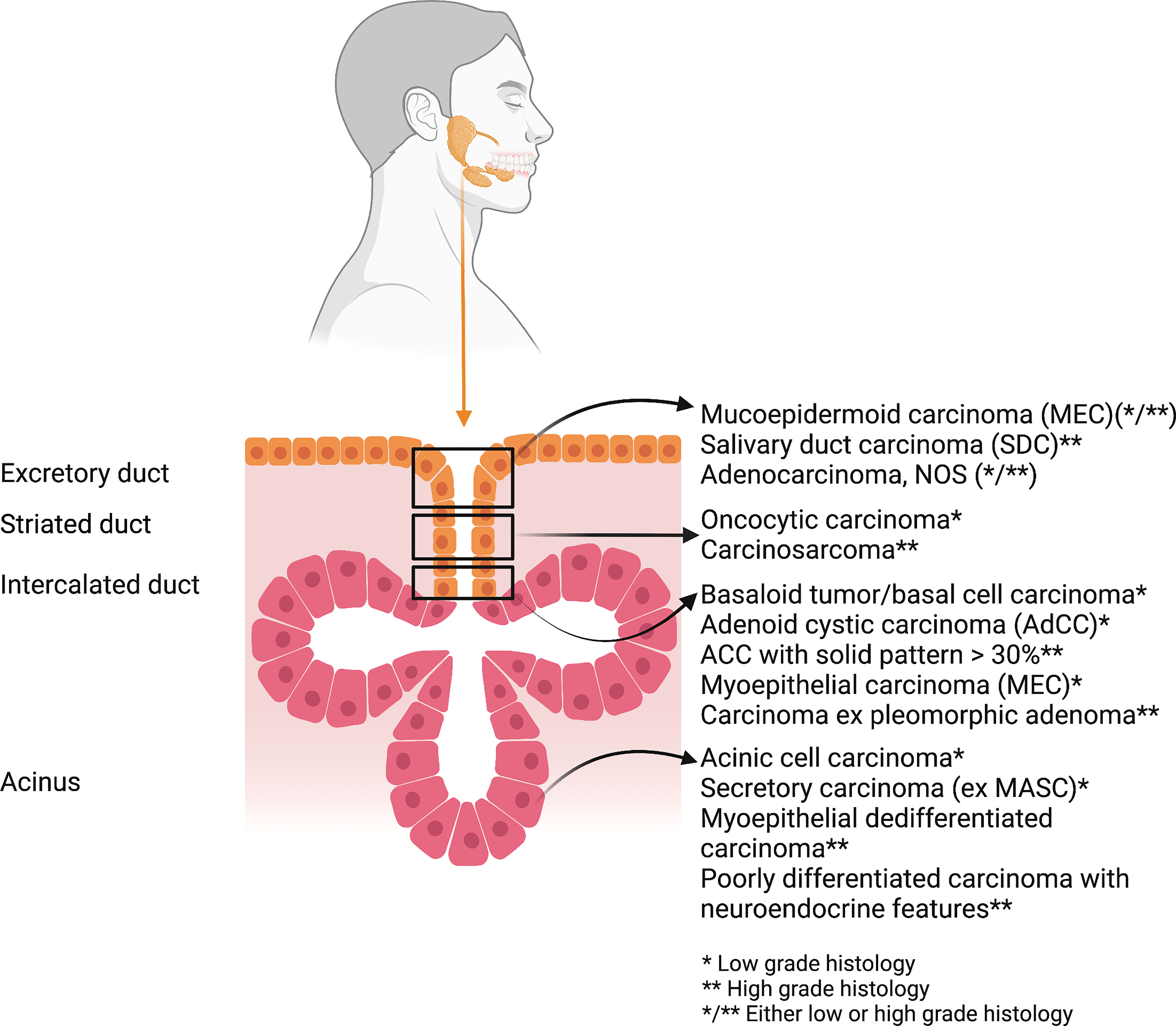
Figure 1 The most frequent histotypes of salivary gland cancers stratified according to the glandular portion of origin and the prevalent grading (*low grade; ** high grade; */** either low- or high-grade histology). Graphic created with BioRender.com.
Recently, the molecular landscape of SGCs has been explored by comprehensive genomic profiling, opening this complex disease to the possibilities of targeted therapy (27, 28). Molecular alterations found in SGCs include amplifications, mutations or rearrangements of transmembrane receptors (ERBB2, FGFR, PDGFR, RET), mTOR pathway (PIK3CA, PTEN) and MAPK pathway (BRAF, HRAS), DNA repair (BRCA1/2), cycle cell regulation (CDKN2A/B, SMARCB1) and activation of androgen-responsive genes by the androgen receptor (AR). Interestingly, the upregulation of ERBB2/PIK3CA pathways is more frequently observed in high-grade than in low-grade SGCs (27). However, certain histotypes can encompass both low-grade and high-grade forms, as in the case of polymorphous adenocarcinoma (PAC), previously known as polymorphous low-grade adenocarcinoma (PLGA); in the last 2017 WHO classification of Head and Neck tumors, both the classic variant of PLGA and aggressive cribriform adenocarcinoma of minor salivary glands (CAMSG), were incorporated under the PAC category. Interestingly, both the variants harbor in the majority of cases an alteration of PRKD genes codifying for Serine/Threonine-Protein Kinase D1, most frequently mutations in the classic PAC variant and rearrangements in CAMSG (29). Certain key rearrangements, such as MYB-NFIB, NR4A3, PLAG1, ETV6-NTRK/RET, CRTC1-MAML2 are typical of certain histotypes, and may help pathologists in the diagnosis of challenging cases (30–36) (Table 1).
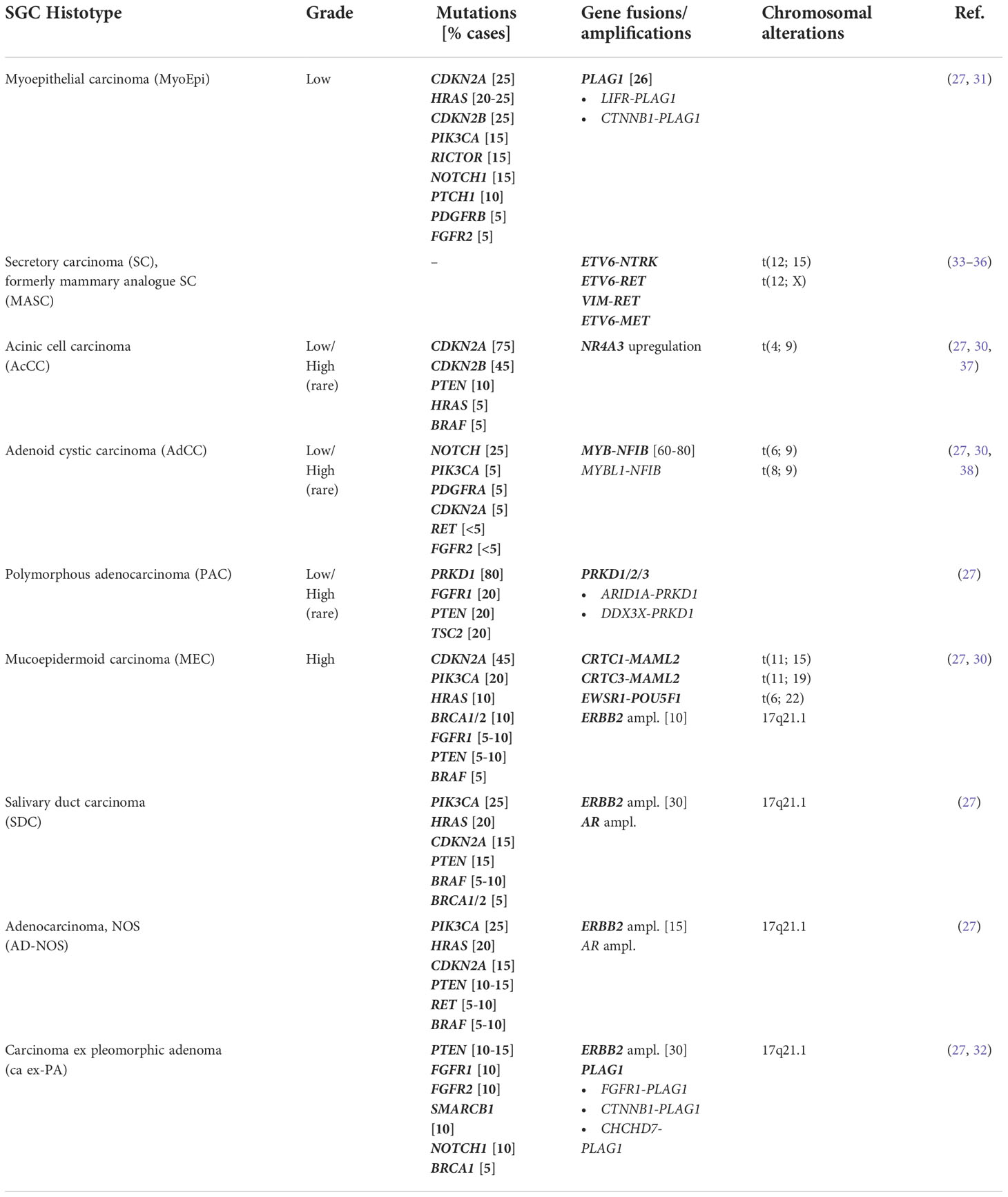
Table 1 Common molecular alterations of the most frequent types of SGCs.
The most frequent high-grade histotypes are mucoepidermoid carcinoma (MEC), salivary duct carcinoma (SDC), adenocarcinoma NOS (AD-NOS) and carcinoma ex-pleomorphic adenoma (ca ex-PA). Low-grade histotypes include adenoid cystic carcinoma (AdCC), acinic cell carcinoma (AcCC), myoepithelial carcinoma (MyoEpi), and SC (previously MASC). However, both AdCC and AcCC may develop a high-grade transformation by dedifferentiation, and this phenomenon has been described also in elderly patients (37, 38) (Table 1).
Tumor grading is directly related to the disease aggressiveness, and it is of utmost interest to capture the age distribution of the commonest types of SGCs. As reported in the AFIP Atlas, certain histotypes are more frequently diagnosed in the 6th decade and beyond, especially SDC, AcCC with high-grade transformation, MyoEpi, basal cell adenocarcinoma, primary squamous cell carcinoma (SCC), large cell undifferentiated carcinoma, epithelial-myoepithelial carcinoma, and carcinosarcoma (26).
For the purpose of this review, we report the age-stratified incidence of epithelial SGCs using the Surveillance, Epidemiology, and End Results (SEER) Program database provided by the U.S.A. National Cancer Institute’s Division of Cancer Control and Population Sciences (39). We selected the cases diagnosed between 2011 and 2018 and retrieved from the updated dataset of the SEER Program based on 18 registries from 13 States (88.816.582 inhabitants). SGCs cases were defined using a combination of the International Classification of Diseases for Oncology (ICD-O) morphology and topography codes (40), as proposed by the RARECAREnet project (5). The SGCs included in the SEER database were divided into two groups:
1 - malignant epithelial tumors of the major salivary glands (MSG);
2 - malignant epithelial salivary glands tumors other than MSG (SGT).
In both groups we report the incidence and 5-year survival (%) by morphology codes, stage at diagnosis and age groups (0-65y and 65y+) (Tables 2–4). The methods used for the calculation of the frequency (incidence) and outcome (relative survival) were provided by the SEERStat program. The number of new diagnoses made in one year for each specific population of cases (incidence) was expressed in annual rate, defined as the number of cases on 100,000 inhabitants per year. The relative survival is the ratio between life expectancy of the cohort of cases affected by cancer and the life expectancy of the population of cases. It is the closest estimation of cause-specific survival in clinical studies.
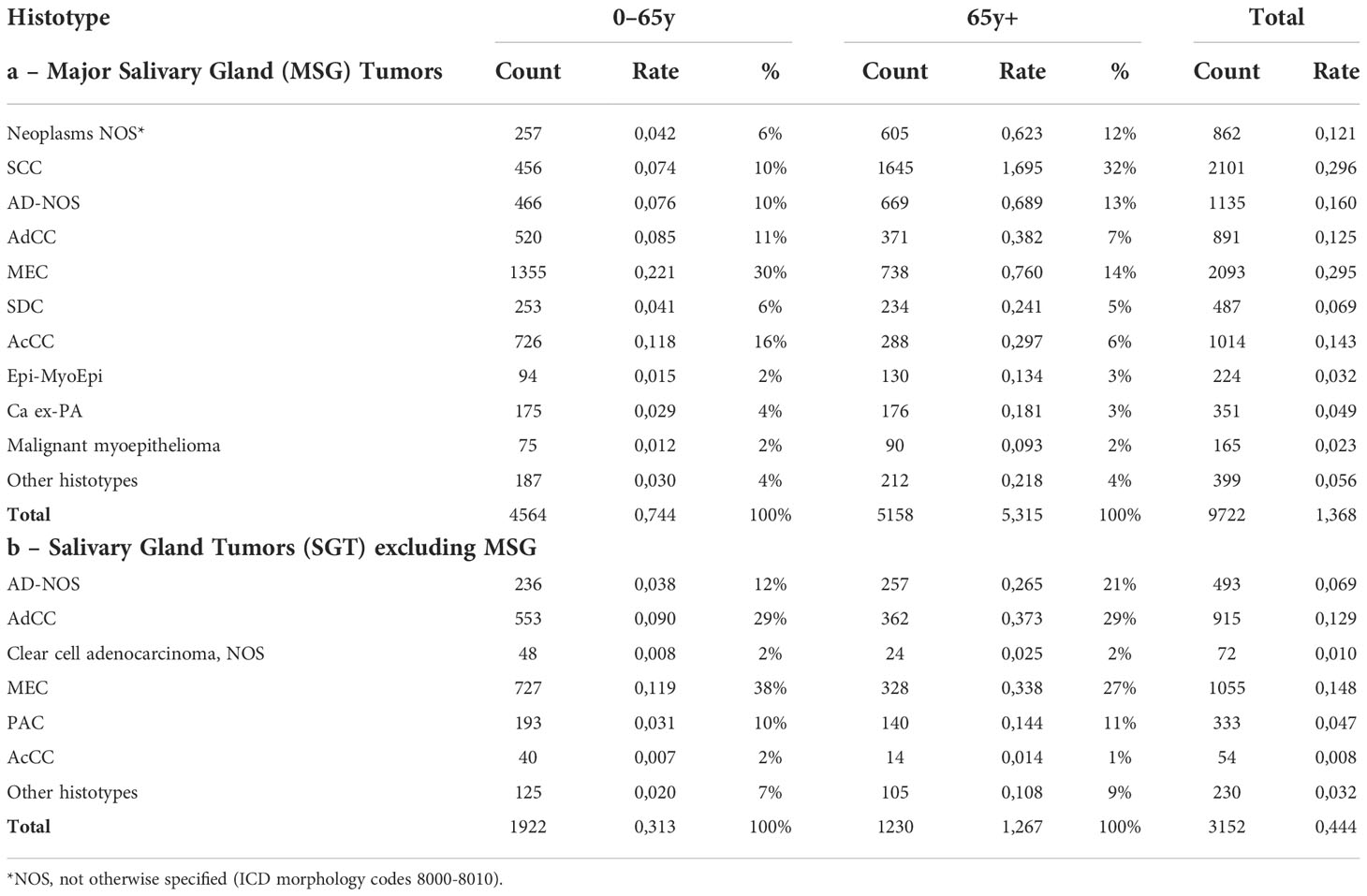
Table 2 Incidence rates of SGCs per 100.000 people, frequency and number by age and histotype. a) Major salivary glands tumors (MSG); b) HN salivary glands tumors (SGT) other than MSG. Period of diagnosis 2011-2018.
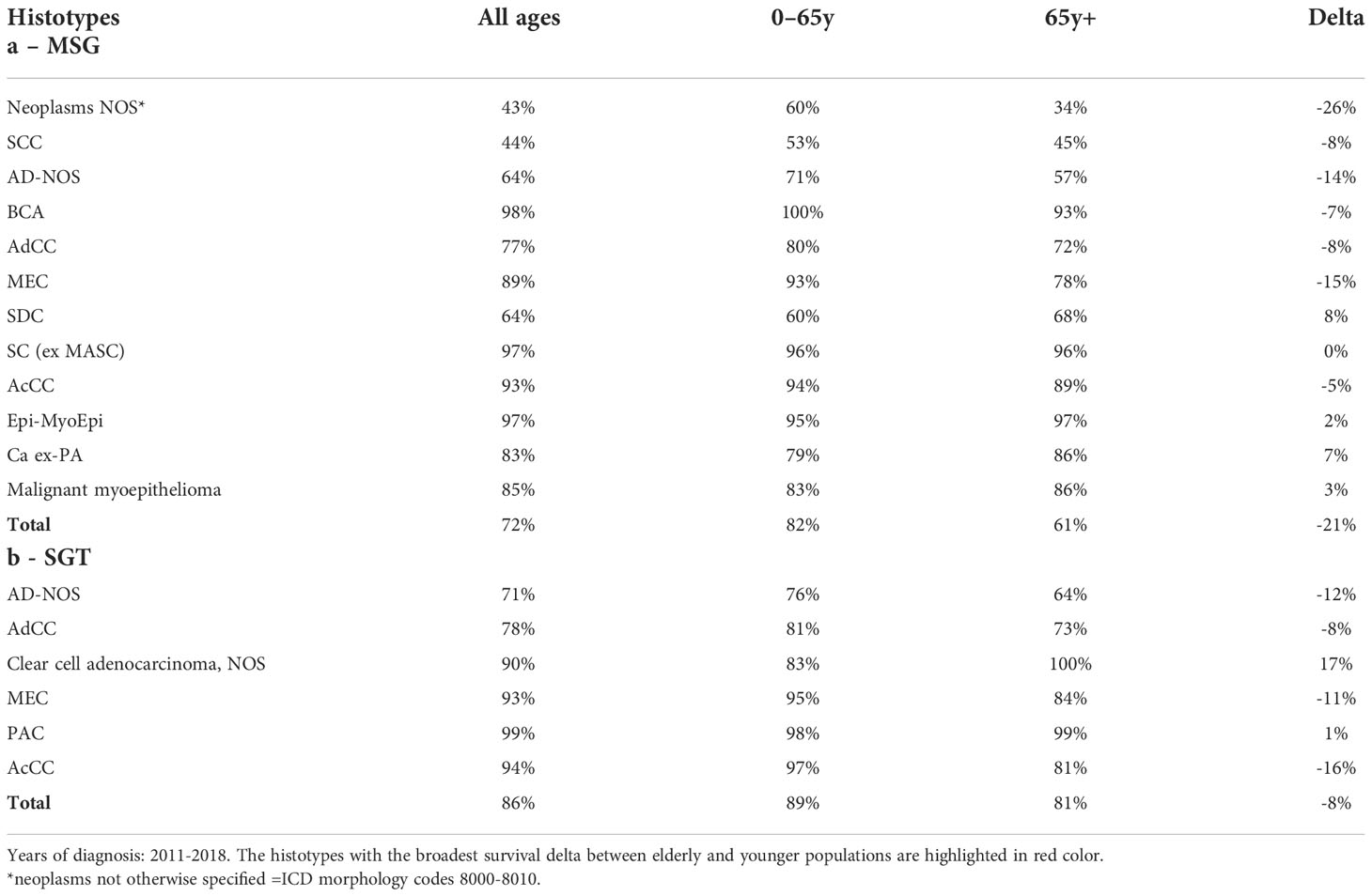
Table 3 Five-years relative survival rates (5y-RS) by age and histotype for a) major salivary glands tumors (MSG), b) Salivary glands type tumors (SGT) other than MSG. .

Table 4 Five-years relative survival (5y-RS) after MSG and SGT diagnoses, stratified by age (0–65y vs 65y+) and extent of disease (localized, locoregional, metastatic, unknown) expressed in raw numbers and in percentage on the total number of cases.
In comparison with 0-65y subgroup, in the 65y+ the incidence rates were 4 and 7 times higher for SGT and MSG, respectively. Focusing on the histotypes, AcCC, MEC and AdCC of SGT were more frequently diagnosed in the 0-64y cohort, while SCC were more common in elderly patients with MSG. Moreover, the neoplasms NOS of MSG and AD-NOS of SGT were more commonly diagnosed in the elderly, compared with younger patients (70% vs 30%) (Table 2).
In the SEER dataset population, the overall 5-years survival rates were significantly better in young than in elderly subjects: the survival rates after MSG and SGT diagnoses were 82% and 89% in the 0-65y group, 61% and 81% in the 65y+ group. Interestingly, the worst outcomes were reported for elderly patients with MSG. The 5-years survival rate was lower for elderly patients in the majority of histotypes, especially in neoplasms NOS (34%), AD-NOS (57%), MEC (78%) of the MSGs and AcCC (81%) of the SGT (Table 3). The differences in survival outcomes observed between the two age groups may be partially explained by a higher proportion of histotypes with favorable prognosis in the 0-65y group, compared to the 65y+ (Table 2).
Almost half of SGC cases from the SEER dataset presented at diagnosis with localised disease, without significant differences between MSG and SGT (Table 4). Elderly patients were diagnosed more frequently at a metastatic stage, and the 5-year survival for each stage was lower in the elderly subgroup. Focusing on the cases with available staging, the greatest difference between age subgroups could be observed for locoregional disease in MSG, where the multidisciplinary team is crucial to define an optimal management.
There is broad consensus that patients with resectable SGCs need surgery as an essential keystone to achieve cure. Depending on the postoperative pathological findings, the majority of patients need postoperative RT to maximize the chance of cure (17, 41–44). Regardless of age, the patients unfit for surgery and those where surgery is not expected to remove all the macroscopic disease are candidate to primary curative or palliative RT.
Independent prognostic factors for survival outcomes following locoregional SGC treatments have been well studied and validated in previous works (45, 46). Independently of the treatment modality, poor outcomes are seen with increasing TNM Stage (reflecting anatomical tumor extension and facial nerve function), higher histological grade, and surgical margins involvement. Increasing age is associated with more advanced stage tumors and more aggressive/high-grade histologies, where free surgical margins are more difficult to obtain. These features occur more frequently in elderly patients, and both biological age and comorbidities are negative prognostic factors (18, 21, 41, 47). Therefore, the most challenging SGCs occur in elderly patients (especially 70y+), who should receive a resection with free margins (R0), but often surgeons and the MDT may hesitate to recommend this important part of the curative treatment because of advanced age, decreased coping mechanisms and comorbidities.
The surgical anatomy of SGs is complex and resection can seriously interfere with vital functions such as speech and swallowing, leading to potentially major functional impact. Thus, it is important to tailor the treatment to the patient (17). Elderly patients, even when apparently still functioning well, are marked by a lower reserve of physiological resources to cope with a surgical treatment and its expected consequences. Frailty is a continuous variable; it reflects the general physical and mental conditions and is directly related to the “biological age” (48–50). For patients affected by HNC, chronological age is not an absolute contraindication for surgery, as it is not strictly associated with major complications. Nevertheless, comorbidities are important predictors of outcome and should be taken into account by the MDT (51). The G8 questionnaire is a valid screening tool to identify elderly patients who need a comprehensive geriatric assessment, leading to an intensified perioperative care (48–50, 52). An impaired G8 score (≤ 14) predicts a prolonged hospital stay, higher risk of delirium and 1-year mortality (53).
Usually, patients with SGC do not present the same risk factors as the population with HNSCC, such as smoke habit and/or alcohol consumption; at equal chronological age, they have lower biological age, they are less frail and have lower ACE-27 scores (18, 48). This translates in a limited role of chronological age in the decision-making process for the elderly patient with SGC, in comparison with the typical HNSCC patient, and less restraint to offer surgery. The feasibility of this approach was proven by a large Dutch cohort where OS, as expected, depended on the ACE-27 score, but DFS did not, meaning that elderly patients with comorbidities received largely the same treatment as the other patients, and had a comparable chance for cure (18). Furthermore, a recent study on the effect of the Age Adjusted Charlson Comorbidity Index (ACCI), incorporating chronological age in the Comorbidity score), in patients with SGCs found that comorbidity did not influence the extent of cancer therapy, and 97% of patients had surgery as initial treatment in this cohort. Patients with a high ACCI score (> 4) in this study had worse oncological and survival outcomes (19).
The following paragraphs provide subsite-dependent state-of-the-art surgical considerations and potential comorbidity-related nuances for operable elderly patients, bearing in mind the limited amount of studies specifically dedicated to elderly patients.
For parotid SGC, a nerve preserving parotidectomy should be performed whenever the facial nerve is preoperatively functioning and detachable from the tumor. If unavoidable, microscopic tumor remnants left on a functioning nerve can be controlled by adjuvant RT. These principles apply also to elderly patients (21, 41, 43). Regarding the extent of parotidectomy, for high-grade T1-T2 tumors localized in the superficial parotid lobe there is still no consensus on the opportunity of removing also the deep lobe (41). Some argue that being more conservative for small high-grade SGC, and removing only the involved part of the superficial lobe, reduces the risk of facial nerve damage without compromising the oncologic outcome (54), while others support total parotidectomy to address the intraparotid lymph nodes both in superficial and deep lobes (55–58). In the absence of high-quality evidence, it is possible to defend a more conservative approach in the 70y+ population, especially if the ACCI score is high (>4). Unfortunately, early-stage high-grade tumors are rarely encountered in this age group: more frequently, elderly patients are diagnosed with advanced-stage high-grade SGC infiltrating the facial nerve or the surrounding structures. Therefore, relatively often, an extended radical parotidectomy with facial nerve, skin, skull base or temporal bone resection is needed (41). As stated previously, chronological age should not impede the surgeon from performing this type of radical intervention, but a G8 geriatric assessment is required to estimate, and eventually increase, the coping capacities of elderly patients. Focusing on the long-term outcomes, the age plays a significant role. A 5-years disease-free survival prognostic model for patients with resected parotid carcinoma was externally validated on a population composed for 35% by 70y+ patients, reporting a significant association between high-grade histology and advanced age, perineural growth, non-radical resection, T classification and N classification. Combined in a prognostic model, all these factors provided more information on the outcome than histology. Therefore, the histology variable was not included in this prognostic index (59).
Patients with T1-T2N0M0 submandibular SGCs are generally treated with surgery alone. Postoperative RT is needed in case of advanced stage, high grade, or pathological risk factors such as perineural invasion and/or positive resection margins (17, 20, 41, 42). Neck dissection of levels I-II-III is the minimal resection for a malignant submandibular SGC without evidence of lymph node involvement at clinical staging (cN0) (41, 47, 60). This should be taken into account especially for elderly patients presenting with high-grade SGCs or AdCC histology, which harbors a clinically occult pN+ rate of 1 out 4 (61). When preoperative MRI scan shows a tumor infiltrating the surrounding structures such as lingual, hypoglossal or marginal mandibular facial nerves, and muscles (digastric, stylohyoid, mylohyoid, hyoglossus), the MDT may deem it not feasible to operate frail elderly patients with comorbidities, while RT can preserve the neural function by achieving locoregional control. Conversely, an extended resection of nerves and mouth floor is usually well tolerated by fit elderly patients (21, 41, 42).
Sublingual SGCs are extremely rare (41). A conservative resection, including Wharton’s duct and the submandibular gland, may be sufficient for small sublingual SGCs confined to the mouth floor (62). For tumors > 2 cm, a more aggressive en-bloc pull-through resection is indicated, due to the high rate of AdCC histology. The resection may need extension to involve the lingual nerve, a marginal mandibulectomy, when the tumor involves the periosteum, or a segmental mandibulectomy, if bone invasion is present. A level I-II-III neck dissection is indicated in these cases (63, 64). Comorbidities and frailty burden are more important than chronological age to assess whether the elderly patient will tolerate this type of surgery.
The primary treatment for resectable mSGC is surgery, most frequently with postoperative RT (44). Often, mSGC are not resectable when diagnosed at an advanced stage, especially if they have nasosinusal/nasopharyngeal origin. The most frequent histotype is AdCC, with a tendency to locally spread along nerves, subperiostal and perichondral planes (41, 44). Especially in elderly and frail patients, RT can achieve a good locoregional control and it should be preferred to complex multidisciplinary surgical efforts that would have profound functional impact, still requiring postoperative RT in the majority of cases. Interestingly, in recent research, postoperative complications were associated with frailty, but RT-associated toxicity was not (52). Moreover, in the context of unresectable mSGCs, particle therapy has presented better locoregional control than photon therapy (65), and this will be extensively discussed further.
Locoregionally advanced disease and high-grade tumors are frequently found in elderly patients (41, 66) and correlate with a high risk of relapse (17, 41, 45). In operable cases, independently of age and salivary gland of origin, the clinical evidence of nodal involvement (cN+) requires an ipsilateral neck dissection of levels I-V. Conversely, the surgical management of cN0 scenario is still debatable (41). For elderly patients, if there is a preoperatively assessed high risk of occult neck disease, valid options are both:
1. elective neck dissection associated with the primary surgery, based on a superselective level II dissection with frozen section (43, 67, 68);
2. elective neck irradiation, especially in frail patients, if adjuvant RT for the primary tumor is foreseen and confirmed by the pathological features of the primary tumor (69, 70).
Since advanced stages and high-grade tumors are frequently observed in the elderly, extended resections are often needed in this population. The resulting defects require a reconstruction to minimize the functional consequences and facilitate adjuvant RT (71). The reconstructing options for major resections of parotid SGCs should match the patients’ medical conditions and comorbidities (41). Especially in the elderly, due to the laxity of the skin of the neck, skin defects resulting from the resection of SGCs with cutaneous invasion can be easily resolved by a local rotation flap (e.g. cervicofacial or cervicodeltopectoral flap) with primary closure of the donor site (41, 71). For large skin defects, in elderly patients unfit for free flaps, an island flap based on occipital and posterior auricular perforators or the supraclavicular artery island flap (SCAIF) are good options (41, 72). Also, deep and supporting tissues often need resection. In patients with vasculopathies, pedicled flaps are often preferred for reconstruction over microvascular free flaps (pectoralis major (myo)cutaneous flap, sternocleidomastoid flap, pedicled latissimus dorsi flap) (41, 73). In elderly patients needing a facial nerve reconstruction, static measures for the upper eyelid (gold implant into the upper tarsal plate, lateral canthopexy), nasolabial groove and angle of the mouth (with a tendinous sling) are primordial (41). In a second procedure ptosis can be restored by a brow lift. For dynamic measures, the general adagium that immediate cable grafting with the greater auricular nerve (GAN) yields the best results, does not hold in the same way in the elderly. More reliable solutions for muscle tone conservation are the hypoglossal-facial-jump anastomosis using the GAN, and the increasingly popular “dual nerve transfer” (masseteric nerve to midface division of facial nerve and ansa hypoglossi branch to lower face division), as these nerves lay in the operative field; however, the long term effects – especially in the elderly – still need evaluation (74). Indeed, a functional re-innervation is more difficult to achieve in the elderly population than in younger patients.
The role of RT in the management of SGCs mainly consists of postoperative radiation therapy (PORT) initiated after the assessment of pathologic risk factors and within 8 weeks post-surgery (Recommendation 3.7) (17), but for patients with medical comorbidities or unresectable tumors, primary RT with curative intent or – more frequently – with palliative intent are also options (Recommendation 3.10) (17). PORT is recommended for tumors with at least one of the following features, according to the ASCO 2021 (Recommendation 3.2) and the National Comprehensive Cancer Network (NCCN) guidelines v.1.2022 (75):
● intermediate/high grade histology (G2-G3)
● large tumor extension (pT3-T4)
● close or positive resection margins
● neural/perineural invasion
● lymphatic or vascular invasion
● lymph node metastases
● adenoid cystic carcinoma histology
Target volume selection and delineation depend on the location of the primary tumors, the histologic subtype and the neck status. For parotid and submandibular gland tumors, PORT for primary tumor should include the tumor bed with a margin to cover all the surrounding normal tissue in which microscopic tumor infiltration could have spread, such as the para-pharyngeal space for deep parotid tumors, or part of the masseter muscle in case of accessory parotid infiltration. There are no guidelines for mSGCs, and the delineation should be done according to the location of the primary tumor. Several authors published guidelines on target volume delineation for parotid and sub-mandibular glands, and readers are referred to these publications for more detailed information (76–79).
In case of AdCC of the parotid gland, owing to the neurotropism of this histology, delineation of the VII cranial nerve should be done, including the skull base for nerve infiltration close to the mastoid; as AdCC cells may spread along the auriculotemporal nerve sheath, the 3rd branch of trigeminal nerve (mandibular nerve, V3) could also be at risk of infiltration, especially for parotid tumors invading the masticator space. For submandibular gland tumors, the branches of the XII nerve and the lingual nerve (a branch of V3) should be delineated. All patients should be treated with IMRT or VMAT, and a dose of 60 Gy should be delivered in 30 daily fractions of 2 Gy (80, 81). There are no data to justify a higher radiation dose in case of positive resection margins (R1), and the benefit of concomitant chemo-radiotherapy is still unknown. The only randomized controlled trial designed to answer this issue (RTOG 1008) has closed to participant accrual and currently is in the phase of data analysis (NCT01220583). Retrospective data do not support RT implementation with chemotherapy on a routine basis (82), and the most recent ASCO Guidelines do not recommend this strategy (17).
After elective neck dissection, PORT is not recommended for pN0 cases and for patients with a single positive node without extra-nodal spread (ENE-). In cN0 patients who did not undergo neck dissection, a watchful policy is recommended for low-grade and low-stage tumors. Conversely, a prophylactic irradiation of level Ib to IV is advised for high grade tumors, SDC, SCC, adenocarcinoma NOS, and undifferentiated histologies. For patients with multiple positive lymph nodes (N+) and/or for those presenting with extra-nodal extension (ENE+), irrespective of the number of positive nodes, PORT of levels Ib to V is recommended (70, 83).
Guidelines on target volume delineation in the neck have been published (84, 85). Typically, elective dose is delivered in the range of 50 Gy in 2 Gy equivalent, whereas a dose of 60 Gy in 30 daily fractions is recommended for pN+ neck (70). Current data do not justify a higher radiation dose in ENE+ cases, and the benefit of concomitant chemotherapy is unknown. As for the primary tumor bed, intensity-modulated RT (IMRT) or volumetric modulated arc therapy (VMAT) should be used as standard irradiation techniques (86–88). When two different dose levels are used, it is recommended to use a Simultaneous Integrated Boost (SIB) approach.
In patients with unresectable or inoperable tumors due to comorbidities, exclusive RT – either with photons or heavy particles – should be considered as a treatment option. For patients who may not be able to receive curative treatment, palliative RT can improve the quality of life by controlling major loco-regional symptoms such as pain, dysphagia, dyspnea, and bleeding. There is no specific protocol for SGCs, and different RT regimens may be administered, such as 30 Gy in 10 fractions, 20-25 Gy in 5 fractions, or 40-50 Gy in 16 fractions (89). Studies focused on target volume selection, delineation, and dose level as a function of patient age/comorbidities are currently lacking. A study compared a small cohort of 29 elderly patients with major SGCs treated with chemo-radiotherapy or PORT with a matched-pair group of younger patients, without finding any difference in acute or late toxicities (90). In RT for mucosal SCC, age was not reported as a prognostic factor for the development of acute or late toxicity, therefore it is recommended to follow similar guidelines for SGCs RT in elderly as in younger patients (91), also considering that irradiated volumes are typically smaller for SGCs in comparison to other HNCs.
SGCs of the head and neck are frequently found in proximity to critical structures, such as the paranasal sinuses and the base of skull, and their local control following RT is dose-dependent. Especially in SGCs, the progress of RT techniques throughout the past decades has been achieved by increasing accuracy, and the dose escalation facilitated by high-precision technologies. As opposed to photon RT, proton and heavy ion (carbon) beams exhibit a finite penetration depth within tissue and deposit most of the energy at the end of their path (Bragg Peak), with only minimal dose deposition beyond the Bragg peak. This allows the generation of extremely steep dose gradients resulting in improved sparing of the normal tissue surrounding the target volume. In addition, carbon ions beams generate more complex DNA damage, leading to increased biological effectiveness as compared to either photon or proton RT, and making this technique ideal for SGCs treatment.
High linear energy transfer (LET) RT for SGCs has been explored early on (92, 93). Despite long-term toxicity was significant, the treatment with neutrons achieved a higher local control of disease compared with photons RT, and these early studies led to the investigation of charged particle therapy for SGCs.
In 2004, the Chiba group investigators shared their initial experience with carbon ions in HNC. In a prospective pilot trial, patients with various advanced HN malignancies (44% T4) were treated with either an RBE-weighted dose of 52.8-64 Gy of C12 in 16 fractions (4 weeks) or 70.2 GyRBE of C12 in 18 fractions (6 weeks). Despite their unfavorable risk profiles, in patients with AdCC histology carbon ions led to local control rates of 50% at 5 years, with a mild toxicity profile (no G3 toxicity or higher) (94). A follow-up protocol confirmed these results, showing a local control rate of 73% at a median follow-up of 54 months and an OS rate of 47% at 5 years (95). Pooled data of the J-CROS consortium representing four Japanese carbon ion institutions have recently been published (96–101). Koto and colleagues reported outcomes of 458 patients with rare HNC, 27% with AdCC and 4,6% with adenocarcinoma of the nasal and paranasal sinuses, treated with carbon ions between 2003 and 2014. Patients received treatment mostly for advanced disease (overall, 65% Stage cT4) with a variety of C12 treatment protocols with RBE-weighted dose between 57,6 – 60,8Gy in 16 fractions to 65 – 70,2Gy in 26 fractions and normofractionated RBE weighted dose of 70,4Gy. At a median follow-up of 25 months, local control in 122 AdCC patients was 86,5% at 2 years and 77,9% at 2 years in 21 patients with adenocarcinoma (96). In a recent update on 289 patients with AdCC (69% T4), the JCROS working group achieved at 2 years a locoregional control (LRC) rate of 88%, median progression free survival (mPFS) of 68% and a CTCAE G3 late toxicity rate of 15% (98).
The combined treatment of IMRT plus carbon ion boost in active beam application achieved comparable results. An initial analysis based on 29 patients with advanced tumors and gross residual disease, treated either with IMRT+C12 boost (mixed beam) or IMRT (photons only), showed a 4-years LRC of 77.5% and 24.6%, respectively. The OS showed a trend in favor of the mixed beam regimen, but differences at the time were not statistically significant (102). Updated results on 95 patients (94% Stage cT4) confirmed the initial findings: at a median follow-up of 63 months, the 5-years LRC was 60% for mixed beam vs 40% of photons only, and the 5-years OS was 79% vs 60%, respectively. Higher-grade late toxicities remained consistently low (5% G3, no G4-G5 toxicities). No significant LRC differences could be detected between patients following radical resection with gross residual tumor and patients with inoperable disease (103).
The phase II COSMIC trial explored the combination of IMRT and dose escalated carbon ion boost, achieving durable LRC and low toxicity profile (104). Moreover, the comparison of patients treated with this modality following surgical resection and those who had received biopsy only, suggested a more favorable toxicity profile in the latter group, without significant differences in terms of LRC. A retrospective analysis of more than 300 patients with AdCC treated with IMRT plus carbon ion boost from the same institution also confirmed those findings (105). The results were updated and analyzed according to the anatomical site, including a study with 24 patients treated for mixed SGCs of the lacrimal gland and another with 59 patients with nasopharyngeal AdCC (106, 107). In the former study, the LRC was 93% at 2 years; in the latter, focused on inoperable (72%) or incompletely resected AdCC, the LRC was 83% at 2 years, similar to the overall analysis (105). Local recurrence occurred mainly within the gradient to adjacent critical structures; potentially, a harder trade-off may improve results, but also significantly increase high-grade late toxicities (8% G3 AEs).
Carbon ion facilities are still few, while proton therapy is more accessible. Proton beams have a finite range and Bragg peak, similarly to carbon ions, although their RBE remains similar to photons. Pommier and Linton reported the outcomes of 23 and 26 patients with AdCC treated with standard fractionated protons at 76 Gy (Boston, U.S.A.) (108) and 72 Gy (Indianapolis, U.S.A.) (109). In the former study, 87% of cases had gross residual disease and the 5-years LRC was 95%; in the latter, the 77% of patients had cT4 disease and the 2-years LRC was 92%. Nevertheless, there is a caveat: in the study of Pommier et al., G3 CNS toxicity rate was 43% and two patients developed fatal late effects (9% G5). However, passive beam shaping was used at the time. Gentile et al. treated 14 patients with AdCC of the nasopharynx with 73,8 Gy protons in spot-scanning technique. The cohort included very advanced tumors (90% cT4, 21% with residual disease following debulking and 79% inoperable). Local failures were detected within the high-dose volume, and 5-years OS rate was 59% at a median follow-up of 69 months (110).
The Orsay group reported a series of 13 patients with incompletely resected or inoperable sinonasal AdCC treated with a combination of photons and protons to a median dose of 73,8Gy: the 3-years LRC was 60% and 2-years OS rate 75% at a median follow-up 34 months; 46% of patients experienced G3 ipsilateral hearing loss, due to proximity of tumor to the ear structures (111). The Paul Scherrer Institute group recently shared the outcomes of 35 patients with AdCC treated with protons at a median RBE-weighted dose of 75,6Gy (definitive RT) and 70Gy (post-operative RT): 2-years LRC was 92.2% and OS 88.8% at a median follow-up of 30 months (112).
Local relapse following initial RT remains a therapeutic challenge. When salvage surgery is not an option, current systemic treatments only achieve modest response rates and rarely alleviate local symptoms. Re-irradiation is used with caution, however data regarding re-irradiation with carbon ions are emerging. Three groups reported their experience with scanned C12 in HN SGCs:
● In CNAO Pavia (Italy) 51 patients with mixed SGC histologies (74.5% AdCC) were treated within a dose escalation protocol ranging from 15-22 x 3 Gy (RBE weighted dose) to 12 x 5 Gy (RBE weighted dose), with a median RBE-weighted dose of 60 Gy reirradiation dose. At a median follow-up of 19 months, the 1-2 years PFS and OS were 72%-52% and 90%-64%, respectively. No G4 or G5 late toxicities were observed, G3 late toxicities (visual deficits, neuropathy, trismus) was detected in 23% of cases (113).
● In Heidelberg (Germany) 52 patients with AdCC received a median RBE weighted dose of 51Gy and cumulative RBE weighted dose of 128 Gy (3 Gy per fraction) after a median RT-interval of 61 months; with a median follow-up of 14 months, 1-year LRC was 70% and OS rate 88%. Overall response was 54%, while toxicity was moderate (< 7% G3-G4). Following re-irradiation, approximately 35% developed another local relapse within the high-dose area (114); updated results of the Heidelberg group in a mixed cohort of recurrent HNC further support those findings (115).
● In Chiba (Japan) 48 patients with mixed histologies of the HN district (35.4% AdCC) were re-irradiated for local recurrence with a median RBE weighted re-RT dose of 54 Gy (C12) following a median initial RBE weighted dose of 57,6 Gy (C12). At a median follow-up of 27 months, 2-years LRC and OS rate were 41% and 60%, respectively. However, G3 and higher late toxicities reached 38% (116).
Considering the reported results, re-irradiation is feasible, but further dose escalation should be explored with utmost caution. Median age in all the aforementioned cohorts ranged between 43 and 63 years (Table 5), and elderly patients constituted a significant percentage of treated patients. Nevertheless, age has been infrequently assessed as a predictor for control and survival rates. Only the large J-CROS series was able to demonstrate a negative impact of higher age on OS (96, 98). Furthermore, radiation therapy on specific subsites may yield a high toxicity impact on elderly patients; Weber et al. showed that age predicted increased visual/ocular toxicity on univariate analysis in a cohort of 36 patients with sinonasal malignancies treated with photons/protons (117).
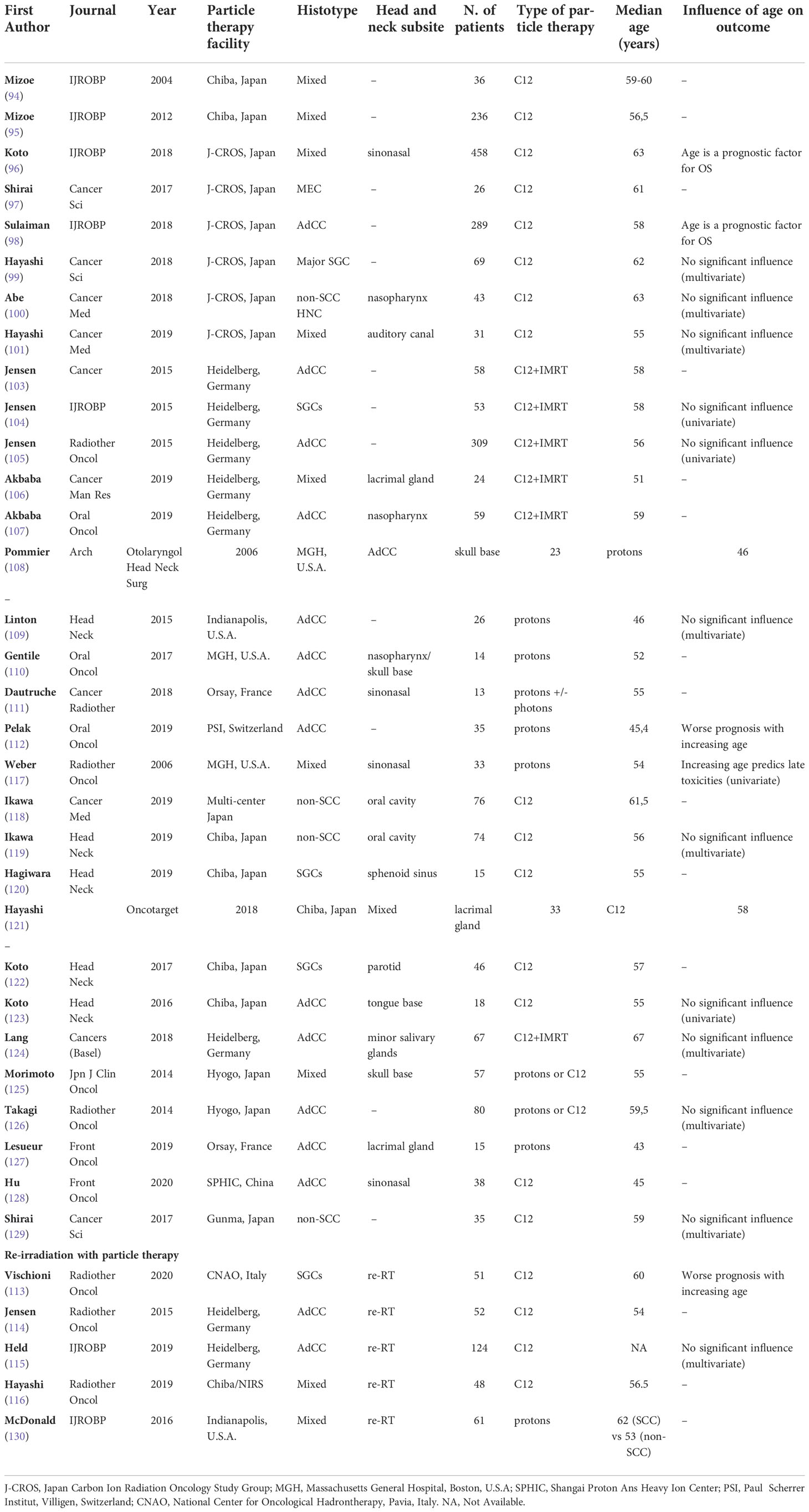
Table 5 Available studies on particle therapy in SGCs and median age of each study population.
Despite the treatment of elderly patients is an important issue to address, indicators such as age, quality of life, performance status and comorbidity scores have not been studied in detail so far. Therefore, in this context data are extremely limited. A pooled data analysis of 288 elderly patients with SGCs treated at 3 institutions between 2005 and 2020 was recently performed: 207/288 subjects (72%) were treated with IMRT plus C12 boost, which was correlated with a high LRC (90.6% at 2 years), but the OS was not improved; 70/288 subjects (24.3%) experienced higher grade (G3) acute toxicities, most commonly mucositis, dysphagia and dermatitis. However, toxicities were not reported separately for particle and photon RT, and no structured evaluation of comorbidities was performed (131).
Adjuvant systemic treatments are not recommended by the ASCO Guidelines outside of clinical trials, despite the fact that two retrospective studies described a potential benefit of androgen deprivation therapy (ADT) and HER2-blockade in SGCs harboring high-risk pathological features of relapse and overexpression of androgen receptor (AR+) and HER2 receptor, respectively (132, 133). Both studies reported a median age at diagnosis of 60 years (range 29–84 years in the study with ADT; 18–87 years in the study with HER2-blockade) and a prevalence of high-risk histologies, such as SDC. In the former study, 22 patients with stage IVA AR+ SDC received bicalutamide alone or bicalutamide plus LHRHa as adjuvant treatment. At a median follow-up of 20 months, the 3-years disease free survival (DFS) of ADT-treated patients and control group was 48% and 27.7% respectively, with a hazard ratio (HR) of 0.14 (95% CI 0.025 – 0.75, p=0.02). In the latter study on adjuvant HER2-blockade, 34 patients were HER2 positive (1-3+) by immunostaining (41% 3+, 38.2% 2+ and 20.6% 1+). A statistically significant survival benefit of adjuvant trastuzumab versus standard follow-up was observed only in the subgroup with high expression of HER2/neu at immunohistochemistry (IHC 3+ score), showing a DFS of 117 vs 9 months (p = 0.02) and an OS of 74 vs 43 months (p = 0.02). A trial with the antibody-drug conjugate (ADC) ado-trastuzumab emtansine (T-DM1) in the adjuvant setting of HER2-positive SGCs is ongoing (NCT04620187).
Currently, the setting of systemic treatments for SGCs is recurrent/metastatic (R/M) disease without either surgical or (re-)irradiation options. Common sites of distant metastases in SGC are the lung (49–91%), bones (40%), liver (19%), soft tissue (9%), distant nodal basins (8%), brain (7%), kidney (2%), orbit (2%), pancreas (2%) (134).
As specified in the last 2021 ASCO Guidelines, therapy initiation should be considered in the following situations (Recommendation 6.3) (17):
1. symptomatic metastatic deposits not amenable to palliative local therapy;
2. if the growth has the potential to compromise organ function;
3. if lesions have grown more than 20% in the preceding 6 months.
Notably, patients with oligometastatic AdCC and low-grade SGCs with a limited metastatic burden (i.e. ≤ 5 lesions) can be considered amenable to palliative local treatments, either by surgery (e.g. lung metastasectomy) or stereotactic body radiation therapy (SBRT) (Recommendation 6.2) (17). SBRT would be the most suitable option to fragile patients facing a high surgical risk for advanced age and/or comorbidities.
Two single-center studies focused on the setting of advanced AdCC showed that increasing age was related to worse OS: in one study of 105 patients with median age 57.3y (range 19 – 87), the hazard ratio per decade for OS was 1.2 (CI 1.1 – 1.6) (135). In another study of 88 patients with a median age of 58y (26 – 79), the group aged > 60y had worse OS compared with the < 40y group (p=.028) (136). Recently, a prognostic nomogram was proposed as a tool which may help clinicians in recognizing patients with metastatic AdCC who could benefit from a watchful waiting strategy vs active treatment (137). The study included 298 patients with a median age of 51y (range 42 – 60) in the testing cohort (n=259) and 59y (range 48 – 68) in the validation cohort (n=39). The nomogram is based on five independent prognostic factors (gender, disease-free interval and presence of lung, liver or bone metastases) that can predict the overall survival at 3, 5 and 7 years. Therefore, age was not confirmed as an independent prognostic factor for OS in this group of R/M AdCC patients.
Few clinical trials investigated the efficacy of cytotoxic chemotherapies in patients with R/M SGCs. In most of the studies, the population number was less than 40 patients and included a variety of histotypes, both AdCC and non-AdCC (Table 6). Consequently, there is not a standard-of-care regimen for SGCs, and the choice of treatment is often directed by the toxicity profile of drugs that proved an activity in this setting.
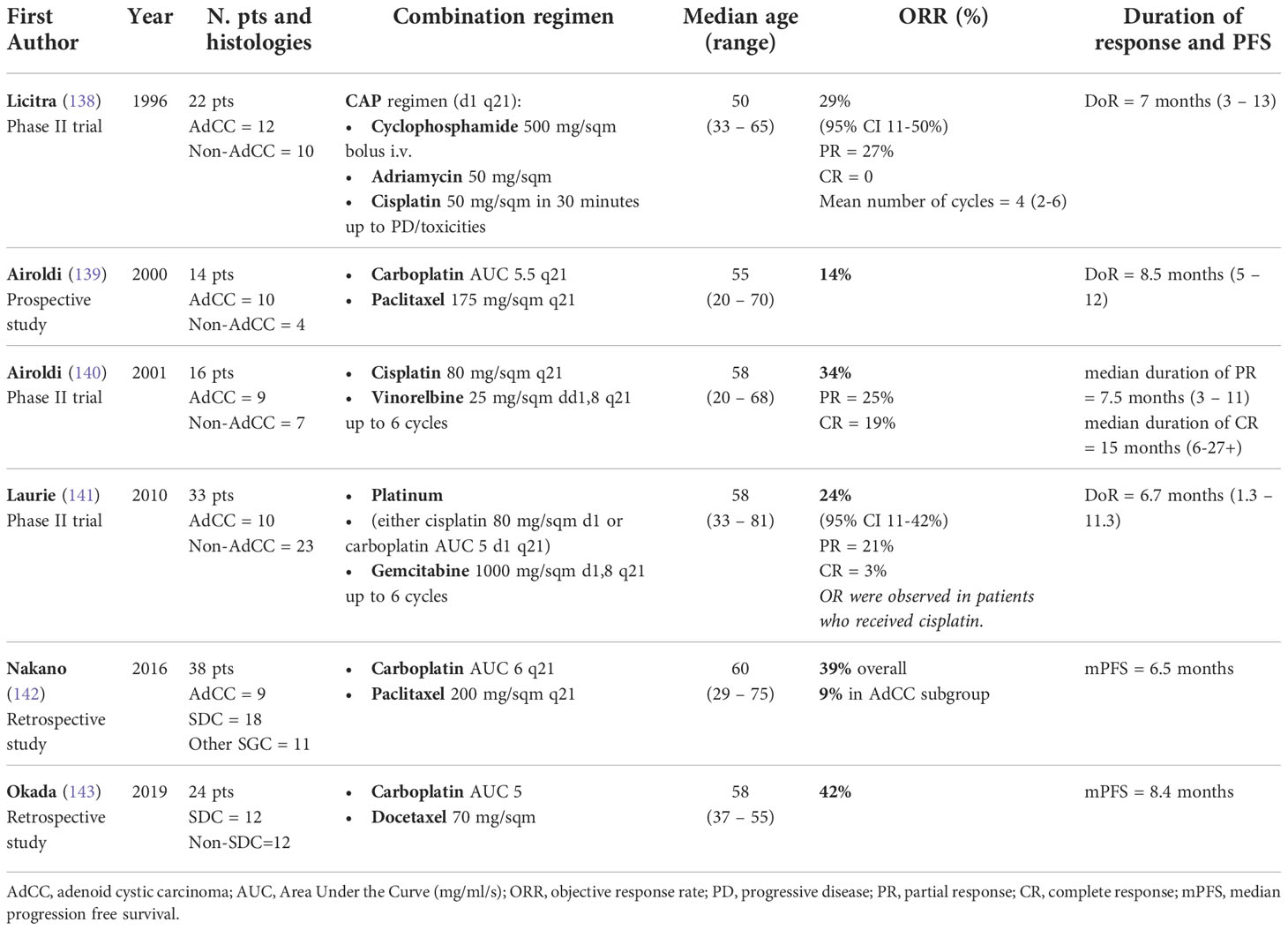
Table 6 Poli-chemotherapy regimens for SGCs and median age of study populations.
According to 2021 ASCO Guidelines, symptomatic patients with R/M SGCs requiring a rapid objective response may be offered platinum-based chemotherapy combinations. Solid data on the tolerability of these regimens by the elderly population are lacking, therefore they should be offered only to fit patients. In the aforementioned studies, the median age of the population was below 65, and the majority employed cisplatin as backbone agent. However, cisplatin is rarely an option for elderly patients, due to the frequent comorbidities (e.g. renal function impairment) and the drug-related risk of nephrotoxicity and ototoxicity, which may impact on the quality of life. The replacement of cisplatin with carboplatin is generally considered less effective (141). The only regimens that proved a long-term clinical benefit with carboplatin were the associations with taxanes (139, 142). In the latter study by Nakano et al., 38 SGCs patients (median age 60y) received carboplatin (AUC 6 q21) and paclitaxel (200 mg/sqm q21), reporting G3/4 neutropenia (53%), anemia (13%) and thrombocytopenia (13%). In another study, the association of carboplatin (AUC 5) and docetaxel (70 mg/sqm) provided an ORR of 42%, with a manageable safety profile (G3/4 neutropenia and anemia observed in 20-30% of the patients) (143).
Single-agent cisplatin 100 mg/sqm q21 for 4 cycles (144), vinorelbine (VNB) 30 mg/sqm i.v. weekly (140), and paclitaxel 200 mg/sqm q21 (ECOG 1394 study) (145) provided an objective response rate (ORR) of 18%, 20% and 16%, respectively.
The choice of chemotherapy should be based on the patient’s characteristics (e.g. performace status, comorbidities, biological age) and tumor histotype. Before starting any chemotherapeutic agent, it is recommended to perform:
● a detailed clinical history in order to investigate the comorbidities that would impact on the choice of chemotherapy (e.g. doxorubicin is discouraged in case of cardiac dysfunction, taxanes in case of diabetic neuropathy or chronic liver disease, cisplatin in case of kidney impairment);
● a G8 questionnaire, in order to identify the frail patients who would benefit from a comprehensive geriatric assessment and a de-escalated treatment;
● a complete blood test including blood count, renal and liver function;
● a baseline electrocardiogram with QTc interval.
Carboplatin and taxane combinations may be offered to fit elderly patients with non-AdCC histotypes (e.g. adenocarcinoma, NOS; SDC) requiring a tumor shrinkage. However, a careful monitoring of the complete blood count should be carried out to check the risk of treatment-related leukopenia or thrombocytopenia. Conversely, elderly patients at risk of renal insufficiency and/or taxane-related peripheral sensory neuropathy, due to concomitant comorbidities (e.g. diabetes, vasculopathy) (146), should receive less neurotoxic chemotherapy combinations, or single-agent vinorelbine.
The androgen receptor (AR) is a steroid hormone receptor activated by testosterone and the more potent dihydrotestosterone (DHT) ligands. The receptor-ligand engagement in the cytoplasm induces the AR homodimerization and translocation of the complex in the nucleus, where it acts as a transcription factor. AR is not expressed in normal salivary glands, but it is overexpressed most frequently in SDC (86%) and carcinoma ex-PA (90%). It has been found less commonly in adenocarcinoma NOS (26%), AcCC (15%), MEC (5%) and AdCC (5%). AR positivity in epithelial-myoepithelial carcinoma is anecdotal, mostly reported in the apocrine variant (147). AR-expressing (AR+) SDC, adenocarcinoma NOS and carcinoma ex-PA are mostly found in elderly male patients, supporting the hypothesis of a hormonal-dependence pathogenesis of these tumors. Of note, these histotypes harbor a significant quote of overlapping cases, as almost 40-50% of SDCs arise from carcinomas ex-PA (148).
As shown in prostate cancers, the androgen axis can be targeted at different levels:
1. Pituitary gland: gonadotropin-releasing hormone (GnRH) receptor agonists, specifically LHRH analogs, that are the backbone of androgen-deprivation therapy (ADT) since they inhibit the synthesis of androgens;
2. Adrenal glands: abiraterone inhibits the conversion of testosterone to DHT by blocking the steroid 5α-reductase 1 membrane-bound enzyme;
3. Intracellular: bicalutamide and enzalutamide compete with androgens for the binding to AR, inactivating the receptor.
The association of bicalutamide and LHRH analog is known as combined androgen blockade and ADT. ADT is included by the 2021 ASCO Guidelines among the options for first- or subsequent-line setting in non-AdCC AR+ SGCs (Recommendation 6.5), on the basis of a single-arm phase II trial of leuprorelin and bicalutamide in 36 patients with AR+ R/M SGCs showing an objective response rate (ORR) of 42% (11% CR) and a median PFS of 8.8 months (149). The median age of this study population was 67 years (range 46–90), 22% with > 75 years, and only 14% had received ChT in the first line. Therefore, ADT could be a feasible chemo-free first-line therapy for elderly patients with AR+ SGCs. A single institution retrospective cohort study on 58 pts with SDC or high-grade adenocarcinoma NOS treated in the first line either with ADT or ChT, reported that OS was comparable in the two groups, but response rates to first-line ADT were higher than those with ChT (150). However, the results of the currently ongoing EORTC 1206 randomized clinical trial are expected to answer the question whether ADT is better than ChT as first-line therapy for AR+ SGCs (NCT01969578).
A phase II trial of the second-generation antiandrogen enzalutamide administered as single-agent in a cohort of previously treated and ADT–naive AR+ SGC patients, reported an ORR of 4% (151). Recently, a phase II study tested the efficacy of abiraterone plus ADT in 24 patients with AR+ R/M SGCs who progressed on ADT, reporting an ORR of 21% with a mPFS of 3.65 months (95% CI, 1.94 to 5.89). Fatigue was the most frequent G3 treatment-related adverse event (AE), reported by 8% of patients (152). The median age of this study population was 65.8 years (range 44 – 77). This trial paves the way to a possible anti-androgen treatment sequence in AR+ SGCs.
The clinical benefit from ADT seems to be higher for those cases with AR immunostaining showing strong intensity and diffusion (≥ 70% of positive nuclei) (153), and with high AR pathway activity (154). However, different mechanisms of resistance have been described, from crosstalk with other pathways (HER2, glucocorticoid receptors) to alternative isoforms of AR lacking the ligand-binding domain, and AR-independent activation of the proliferative transcription program (155). Of note, almost 35–50% of SDCs present the ARv7 isoform, detected by IHC also in 15% of ADT-naïve patients (156). In future studies, liquid biopsies could help to investigate the role of AR-v7 as primary/secondary resistance mechanism to ADT in AR+ SGCs, as previously done in prostate cancer (157, 158). Some cases with chemo-hormonal combinations have been reported (159), but it is still to be defined whether there is an extra benefit of the combination over the single components.
The ERBB2 gene codifies for the human epidermal growth factor receptor 2/neu (HER2/neu). HER2 expression can be detected by IHC, with a scoring reported as negative (0/1+), equivocal (2+) or positive (3+), and/or by in situ hybridization (ISH). It is overexpressed (IHC 3+ or IHC 2+ with positive ISH) in almost 8% of SGC cases (160), with the highest prevalence in high-grade subtypes, as it can be found in 43% of SDCs, 39% of carcinoma ex-PA, 17% of SCC and 13% of adenocarcinomas, NOS (161). Conversely, AdCCs express low levels of HER2, as described in a phase II study of 20 patients where 30% had HER2 IHC 1+, 5% IHC 2+ and 0% IHC 3+ score (162).
According to the 2021 ASCO Guidelines, patients with HER2-positive SGCs may receive HER2-blockade as first- or subsequent-line therapy (Recommendation 6.5). Many agents have been tested in the last years and are already approved for the treatment of R/M HER2-positive breast cancer. In Table 7 are summarized the studies that explored HER2-blockade in SGCs.
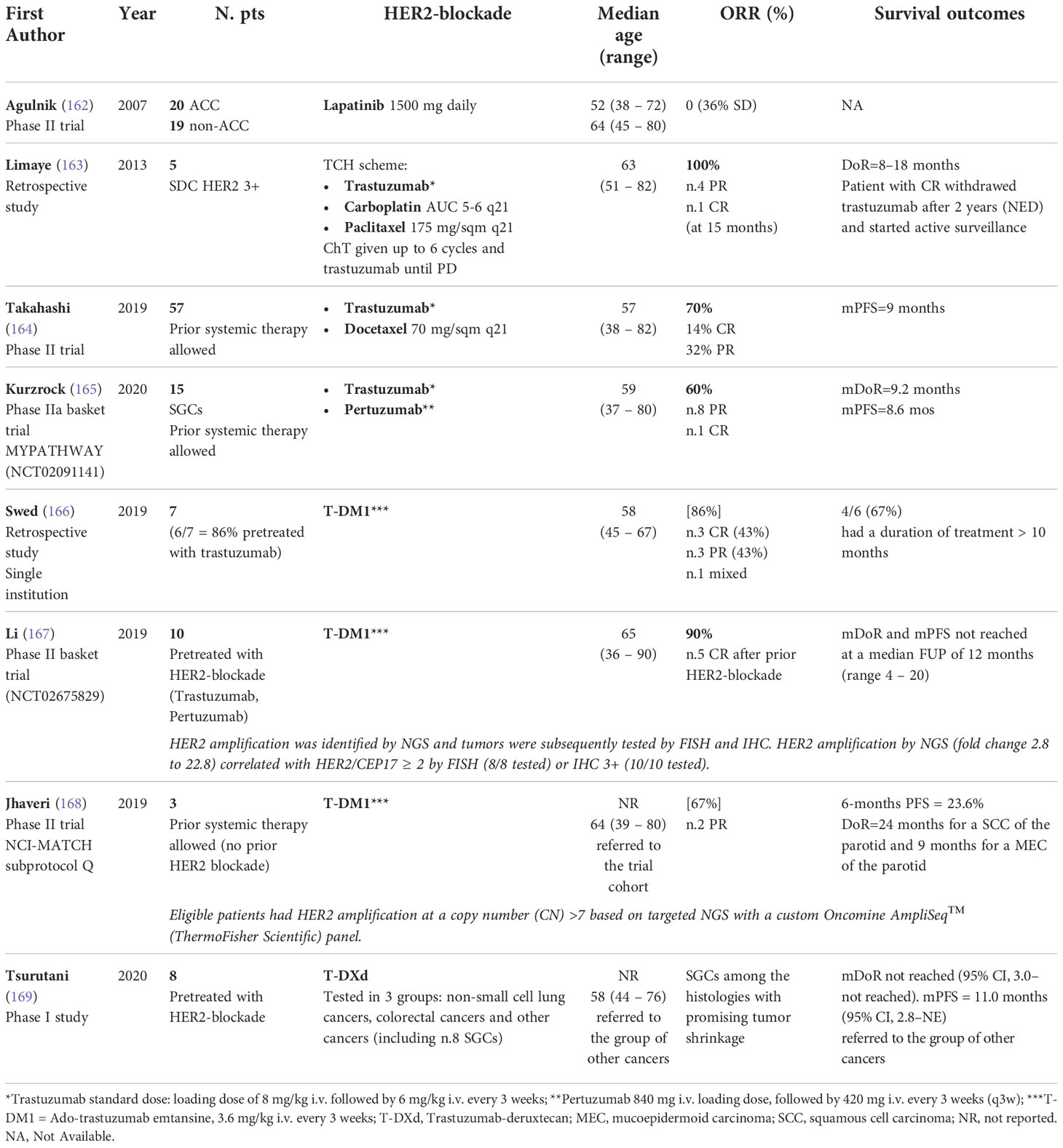
Table 7 Studies that explored HER2-blockade in SGCs and median age of study populations.
In a trial with docetaxel-trastuzumab (164) the median age of study population was 57 years (range 38-82), with 14% of patients older than 75 years; 14% of patients reported G3 febrile neutropenia, and 60% have at least one episode of G4 neutropenia, making this regimen feasible only for selected elderly patients. In a retrospective trial with the triplet of carboplatin-paclitaxel-trastuzumab, G3 fatigue and thrombocytopenia were seen in one patient each, no G4-G5 toxicities occurred and no cardiac dysfunction was seen as a result of trastuzumab-based therapy. In this small retrospective study two elderly patients were included (72 and 82 years), and both managed to receive at least 8 months of trastuzumab-taxane scheme (163).
Dual blockade with trastuzumab and pertuzumab (anti-HER2-HER3 dimerization) was tested in a phase II basket trial with 15 patients that had been previously treated with chemotherapy (patients with active brain metastases were excluded) and showed an ORR 60% with durable responses (165).
The antibody drug conjugate (ADC) Ado-trastuzumab emtansine (T-DM1) is formed by a molecule of trastuzumab linked to 3–4 molecules of the maytansine derivative DM1, a tubuline inhibitor. T-DM1 was investigated in two basket trials where the SGC subgroup showed high objective response rates, up to 90% in the most successful one, that also included patients pretreated with HER2-blockade who achieved 50% of complete responses after prior trastuzumab, pertuzumab and androgen-deprivation therapy (167). The NCI-MATCH trial-subprotocol Q did not meet its primary endpoint of ORR > 16% in a heavily pretreated population composed by various histologies; nevertheless, the authors warranted further studies of T-DM1 in SGCs, as 2 out 3 patients with SGCs enrolled in this trial achieved durable responses (168).
The ADC trastuzumab deruxtecan (T-DXd or DS-8201a) is formed by a molecule of trastuzumab conjugated with a topoisomerase I inhibitor payload (deruxtecan). It is currently approved in HER2-positive R/M metastatic breast cancer, pretreated with HER2-blockade. In a phase I study, HER2-amplified SDCs were among the histologies with the most pronounced tumor shrinkage, although topoisomerase inhibitors are not part of the cytotoxic agents commonly used in SGCs (169).
Globally, anti-HER2 agents provide objective and durable responses in HER2-overexpressing SGCs. Also, no specific adverse events have been related with advanced age, therefore they are potential chemo-free option for elderly patients. Despite the recently observed increase in anti-HER2 agents, there is still a therapeutic void for patients with HER2-positive SGCs. Trials are urgently needed to select the best sequencing of anti-HER2 strategies, as done in breast cancer, and also to define the optimal strategy for the patients with AR and HER2 co-expression, which display a short overall survival (170).
AdCC is associated with low responses to chemotherapy. However, AdCC may harbor hyperactivation of the angiogenic pathway, as demonstrated by recent in-depth analysis of the mutational landscape of recurrent or metastatic (R/M) AdCC (171). According to the 2021 ASCO guidelines, patients who are candidate to start systemic therapy, can receive multikinase inhibitors (MKIs) instead of ChT, on the basis of phase II trials proving the efficacy of lenvatinib and sorafenib (Recommendation 6.4) (17); the median age of study populations was 57y (range 38–73) and 50y (range 21–70), respectively (172, 173). Currently, lenvatinib is the most frequently used MKI for R/M AdCC; it is a second-generation MKI directed to the targets of vascular endothelial growth factor 1-3 (VEGF1–3), fibroblast growth factor receptors 1-2 (FGFR1–4), RET, c-KIT, stem cell growth factor receptor (SCGFR) and platelet-derived growth factor receptor α (PDGFRα). However, up to 50% of patients treated with lenvatinib may experience G3 adverse events, global functioning impairment and increasing fatigue, especially across the first 6 months of treatment (174). Recently, a randomized phase II trial in R/M AdCC showed that the selective VEGFR1–3 inhibitor axitinib, as compared with observation, with a median follow-up of 25.4 months significantly improved the 6-month PFS (73% vs 23%). Even though the ORR of axitinib was 0%, median OS was not reached with axitinib vs 27.2 months in the observation arm (p = 0.226). The cohort treated with axitinib included 30 patients with a median age of 57y (range 28 – 77), and the most frequently reported adverse events for axitinib were oral mucositis and fatigue (175). Recently, at the ASCO 2022 Annual Meeting, a phase II study evaluated the efficacy and safety of the selective VEGFR2-inhibitor rivoceranib (700 mg once daily) in R/M AdCC (Kang H et al., abstract 6020 – NCT04119453). The study was conducted on a population of 80 patients with median age of 54.5y (range 28-76). At a median follow-up of 15 months, ORR was 13.9% in patients pretreated with VEGFR-TKI and 16.9% in VEGFR-TKI naïve; median PFS was 9.2 months regardless of prior anti-VEGFR treatment. 80% of the population experienced at least one G3 AE, mostly hypertension, stomatitis, anemia and fatigue. In the clinical practice, special attention should be addressed to elderly patients with comorbidities such as hypertension and impaired kidney function treated with antiangiogenic agents, as they require a full basal cardiological evaluation with echocardiogram and strict monitoring of blood pressure and proteinuria throughout the treatment.
AdCCs may harbor mutations in genes encoding chromatin-state regulators, TERT promoter, fibroblast growth factor (FGF)–insulin-like growth factor (IGF)–PI3K pathway and RET (4%) (171, 176). The MYB-NFIB fusion is the diagnostic hallmark of AdCC, being present in 65 – 80% of cases, but it is not currently actionable by approved drugs. However, the ionophoric antibiotic monensin has been recently identified as a potent MYB inhibitor in preclinical studies (177), and a phase I trial with TetMYB vaccine and immunotherapy (anti-PD1 agent BGB-A317) has recently completed the accrual (NCT03287427). NOTCH mutation is found in 10-22% of AdCC and identifies a subgroup of AdCCs prone to develop liver and bone metastases, leading to a dismal prognosis (178) especially when the MYB fusion is co-present (171). The phase II trial ACCURACY showed the clinical activity of pan-Notch inhibitor AL101 at 4 mg once weekly (QW), achieving a disease control rate of 68% (15% partial responses) in a cohort of 45 patients with median age of 50 years (179). At the ESMO 2021 Congress, the results of 6 mg QW cohort were presented, showing good tolerability of AL101 in a study population of 37 patients with median age of 59 years (180).
In non-AdCC SGCs, the use of MKIs is not recommended (181). However, in certain cases, single molecular targets can be addressed. NTRK gene fusions, codifying for oncogenic forms of tropomyosin receptor kinase (TRK), occur in an estimated 5% of cases of SGCs, including more than 90% of secretory carcinomas (SC). In the majority of cases, SC presents as an indolent nodule arising from the parotid and harbors the chromosomal translocation t(12,15) between the ETV6 gene on chromosome 12 with NTRK3 on chromosome 15, generating the fusion product ETV6–NTRK3 (33). The nuclear pattern of pan-TRK IHC staining has good sensitivity to detect the ETV6–NTRK3 fusion, helping in the differential diagnosis. From the histological prospective, secretory carcinoma could be misdiagnosed most frequently with AcCC, but also with AdCC, cystadenocarcinoma, MEC and low-grade carcinoma NOS. Recently, the efficacy of TRK-inhibitor larotrectinib for R/M SGCs has been analyzed in a study where the investigators focused on the population of two clinical trials: the phase 2 NAVIGATE basket trial (NCT02576431) and a phase 1 trial (NCT02122913). Overall, 24 patients were treated with 100 mg larotrectinib twice daily and 1 patient received 150 mg twice daily. The median age of study population was 58.5 years (range 28 – 78). Tumor histology was SC in 54%, adenocarcinoma in 21%, and MEC in 13%, followed by AdCC, glandular sarcomatoid carcinoma, and adenocarcinoma NOS. All patients had an ETV6-NTRK3 gene fusion. The ORR to larotrectinib was 92% (95% CI, 73% – 99%), with 79% PR and 13% CR. The median time to response was 1.84 months (range 0.99 – 5.98) and the duration of treatment ranged from 0.95 to > 60.4 months, with a 36-months PFS rate of 66% and OS rate 91% (182). From the integrated analysis of three phase I and II clinical trials on entrectinib (ALKA-372-001, STARTRK-1, and STARTRK-2), a response to this drug was seen also in 6 out 7 patients with SC, with an ORR of 86% (183). Both larotrectinib and entrectinib received FDA and EMA tissue-agnostic approval, and ASCO 2021 Guidelines on SGCs recommend the use of TRK-inhibitors in first or subsequent-line, rather than chemotherapy (Recommendation 6.5) (17). However, different mechanisms of acquired resistance to TRK-inhibitors have been described, either on-target mutations in the drug-binding site, or off-target activation of the mitogen-activated protein kinase (MAPK) pathway (184–186). Currently, clinical trials with next-generation TRK-inhibitors selitrectinib (NCT03215511) and repotrectinib (NCT03093116) are ongoing (187). Of note, a case of entrectinib-resistant SC that achieved a durable response to selitrectinib also on leptomeningeal metastases was recently reported (188).
Few cases of SC with high-grade histology and aggressive behavior have been described in association with ETV6-MET, ETV6-RET and VIM-RET fusions, which are not detectable by pan-TRK IHC and could be actionable by other targeted therapies, especially RET inhibitors in the case of ETV6-RET fusions (34–36). Therefore, all tumors with morphological features resembling secretory carcinoma should undergo Next Generation Sequencing in order to detect the specific fusion transcripts, as recommended by the ESMO guidelines on molecular profiling of solid tumors (189, 190).
In the last decade several studies reported single-gene potential targets with different incidence, stratified by histotypes and grade, and uncovered novel therapeutic targets by comprehensive molecular profiling (27, 191–193). For patients who may be potential candidates for systemic therapy and have SGC histologies with unknown driver mutation status, the ASCO 2021 Guidelines on SGCs recommend performing a comprehensive panel for driver mutations by NGS profiling (Recommendation 6.9) (17). Currently, mutations in RET, BRAF, HRAS, FGFR, PIK3CA, BRCA1/2, PTCH1 genes are actionable by oral drugs already approved for other cancer types, and basket clinical trials/managed access programs are currently ongoing. This is a promising area of research also for elderly patients, usually more fragile and difficult to treat with standard chemotherapy.
The microenvironment of SGCs is highly heterogeneous, ranging from the immune-exclusion of AdCC to the high immune-infiltration and high PD-L1 expression of high-grade histologies, such as carcinoma ex-PA (75%), MEC (57.1%) and SDC (50%) (194–196).
Currently, the role of immune checkpoint inhibitors (ICI) in SGCs is a subject of active research (Table 8). According to the ASCO 2021 Guidelines (17), ICI should be offered for patients with high tumor mutational burden (TMB) or high microsatellite instability (MSI-H). Also, the NCCN guidelines (v.1 2022) limit the use of pembrolizumab to the cases with TMB-high, on the basis of the KEYNOTE-158 study that proved the agnostic efficacy of pembrolizumab in solid tumors with TMB ≥ 10 mutations identified per megabase (202). Of note, the cohort J of KEYNOTE-158 dedicated to SGCs histology included 3 patients with TMB-high and 79 patients with TMB-low; one SGC tumor was found MSI-high. Objective responses to pembrolizumab were reported in 1/3 cases of TMB-high and in 3/79 of TMB-low. Therefore, TMB-high did not show a high sensitivity as predictive biomarker of response to anti-PD1 inhibition in SGCs. Currently, the tumor-agnostic approval of pembrolizumab upon TMB-high status has not been endorsed by the European Medical Agency.
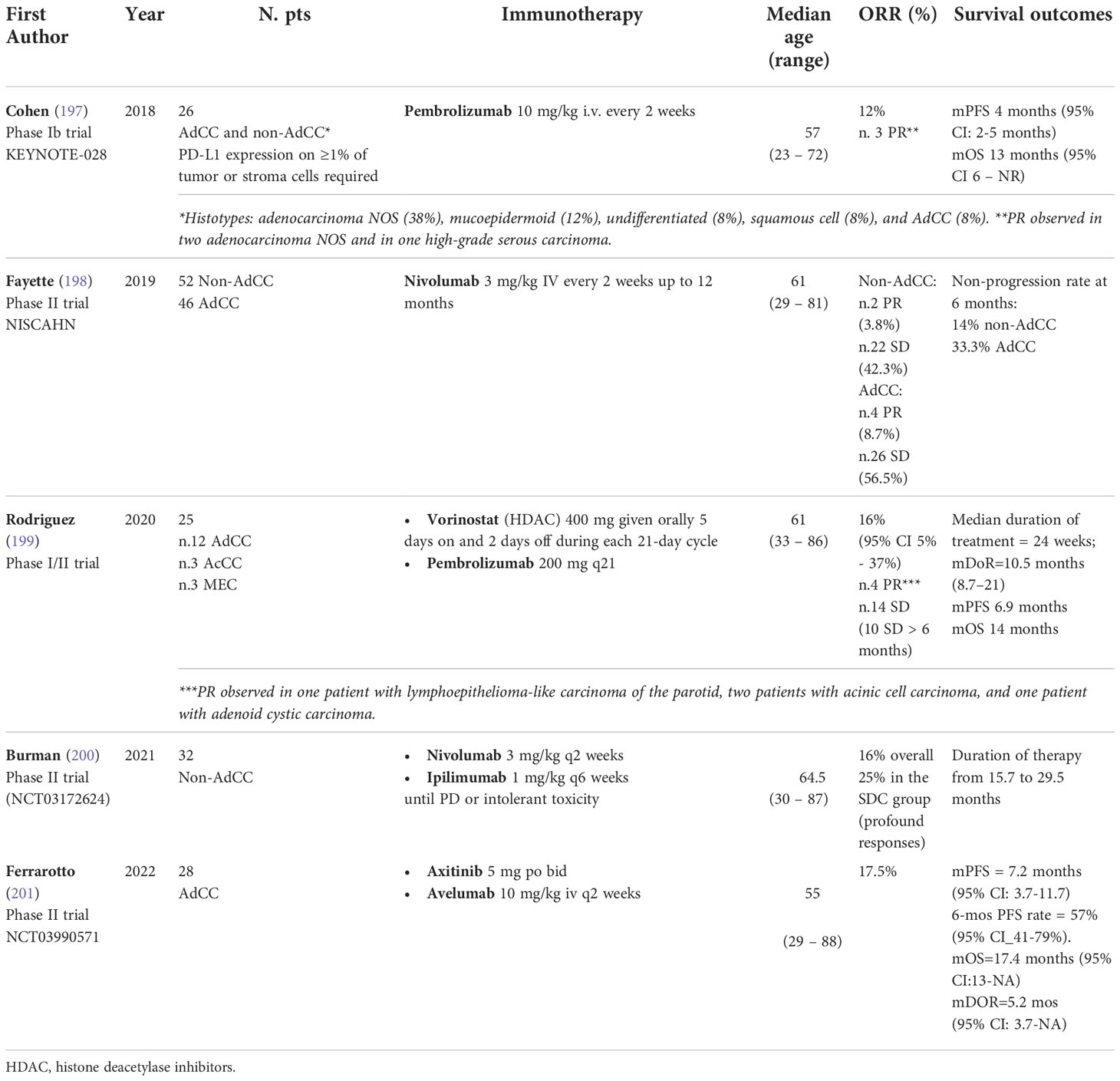
Table 8 Studies that explored the efficacy of immunotherapy in SGCs and median age of study populations.
At the 2021 ASCO Annual Meeting, the results of Cohort 2 of NCT03172624 study were reported (200). This phase II trial included 32 patients affected by R/M non-AdCC SGCs, who received anti-PD1 nivolumab plus anti-CTLA4 ipilimumab. The majority of patients were diagnosed with SDC (38%) and AcCC (22%) histotypes. Median age was 64.5 (range 30 – 87); 69% of the total population had received a prior chemotherapy, 22% androgen-deprivation therapy and 25% other targeted therapies (no ICI). The study met the primary endpoint of best overall response with 5 responses (16%) in the overall population, while the SDC subgroup showed a PR rate of 25% (3/12). The 5 confirmed responders had regressions ranging from -66% to -100% in target lesions, with a duration of therapy ranging from 15.7 to 29.5 months. Of note, the RNAseq analysis highlighted a correlation between baseline immune infiltration and benefit from ICI. In a recent case series of Chinese patients with R/M AdCC treated with immunotherapy, the response to PD-1 checkpoint inhibitors (camrelizumab or pembrolizumab) was related to elevated T-cell infiltration score and antigen-presenting machinery score (203). Recently, the immunomodulatory role of antiangiogenic drugs has been explored. At the 2022 ASCO Annual Meeting, the results of a phase II clinical trial of VEGFR1-3 inhibitor axitinib (5 mg BID) associated with PD-L1 inhibitor avelumab (10 mg/kg every 2 weeks) in patients with R/M AdCC were presented: of 28 patients with evaluable treatment efficacy, 16 had received the treatment in first line. Median age of study population was 58y (range 29 – 88), 39% had AdCC with solid component, 36% with cribriform/tubular histology. The ORR was 14.3% (4/28, 95%CI: 4-32.7%) and responses were independent from NOTCH1 activating mutation; 6-months PFS rate was 57%. The most common treatment-related adverse events were fatigue, hypertension and diarrhea (Ferrarotto R et al., Abstract #6019 - NCT03990571).
The most relevant trials that explored the activity of immunotherapy in SGCs are resumed in Table 8. Overall, the efficacy of immunotherapy is still under investigation in SGCs, but in a subset of patients it provides profound and durable responses. Reliable predictive biomarkers beyond TMB are needed, in order to select the population of patients who could benefit the most from this type of therapy usually well-tolerated also by elderly patients.
Elderly patients with SGC carry a poor prognosis compared to younger patients. We have reported the incidence and the 5-years survival outcomes of the most common histotypes in the U.S. population, in order to assess whether a different distribution of histotypes in the two main age subgroups (< 65y and 65y+) could explain part of this survival disparity. Good prognosis histotypes and early stage at diagnosis were more common in younger patients. Conversely, advanced stage at diagnosis and unspecified (NOS) histotypes presented more frequently in the elderly. These characteristics are possibly related to the aggressiveness of disease, poor attention to early symptoms, and difficulty in accessing referral hospitals to receive an accurate diagnosis and appropriate treatment. Such features, typically found in elderly, have been recognized as independent poor prognostic factors in SGC patients, regardless of the type of treatment (17, 18). Also, the high proportion of “carcinoma, NOS” in the elderly group could be an indirect sign of suboptimal pathological diagnosis in this population.
Since a correct pathological diagnosis is the prerequisite for an appropriate treatment planning, proper pathological and molecular analyses should be carried out, both for diagnostic and therapeutic purposes, in order to avoid the generic diagnosis of “carcinoma, NOS”. As assessed in the ASCO 2021 Guidelines (Recommendation 1.6), the use of ultrasound-guided core needle biopsy (CNB) has an estimated sensitivity of 94% and specificity of 98% (204). Moreover, CNB has a lower inadequacy rate (1.2%) than FNAB (8%) and yields adequate material for ancillary molecular testing (205, 206).
In Europe, the centralization for HNCs cases is feasible and active (207). However, existing differences among countries have been reported (208). In consideration of the multiple and challenging clinical variables (e.g. comorbidities, high-grade tumors, advanced stage), an optimal care of elderly patients with a diagnosis of SGC should start with a multidisciplinary tumor board evaluation, together with a G8 questionnaire, and a comprehensive geriatric assessment should be offered whenever needed (Figure 2).
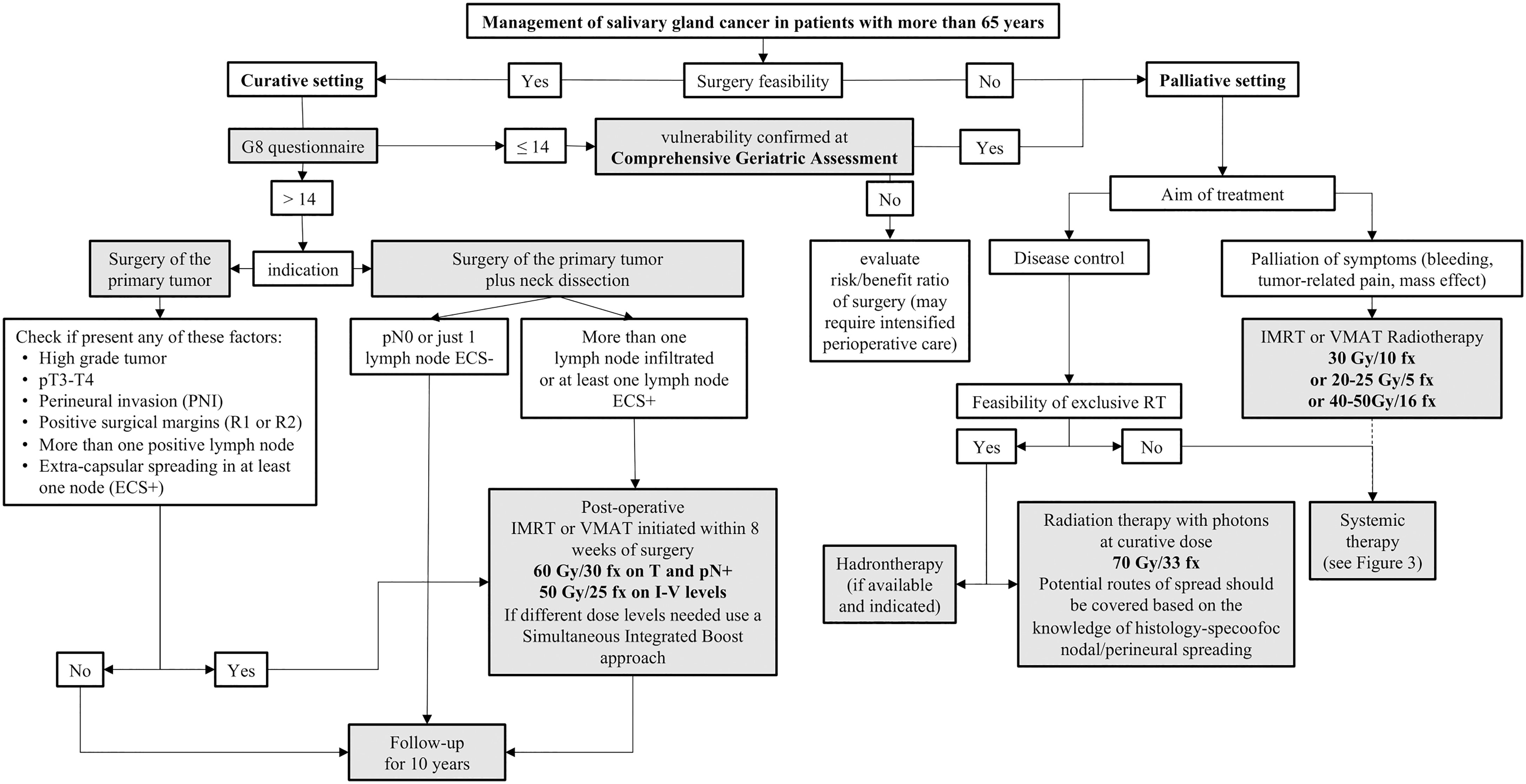
Figure 2 Algorithm proposal for the clinical assessment and treatment strategies of elderly patients with SGCs. G-8,; PNI, perineural invasion; R1, microscopic residual tumor; R2, macroscopic residual tumor; ECS, extra-capsular spreading (+ present, - absent); Gy gray; fx fractions; T, tumor; N, lymph nodes; IMRT Intensity-modulated radiation therapy; V-MAT, Volumetric modulated arc therapy; IHC, immunohistochemistry; SC, secretory carcinoma; NGS, next generation sequencing; TMB, tumor mutational burden; BSC, best supportive care.
Surgery is the hinge of curative pathway in SGC patients, and not less so in the elderly population. An advanced chronological age is not an absolute contraindication for surgery. The tumor resectability, the extent of surgery and the expected outcomes should be discussed. In addition, screening tools such as the Age Adjusted Charlson Comorbidity Index and G8 questionnaire have to be assessed also in this setting, in order to identify frail patients and their special needs.
Postoperative RT is generally delivered in advanced stage, high-grade or in case of high-risk pathological features. The choice of radiation type – by photons or heavy particles – should be based on clinicopathological characteristics, resection margins, and facilities availability. Toxicities should be closely monitored and early managed, with a careful and continuous supportive care during the whole treatment period. For those patients not amenable to surgery, either due to the extent of disease or comorbidities, exclusive RT with radical or palliative aim would be most reasonable choice. Based on the available data, there is no evidence to support that elderly patients undergoing particle therapy should be treated differently than younger subjects. In fact, toxicity profiles and control rates favor particle therapy over photon RT. There is a general lack of information on structured quality of life assessments in the particle therapy literature throughout all age groups, and this subject should be addressed alongside future prospective clinical trials. Until further data are available, no recommendations can be made on differential treatments with particle therapy in elderly patients with SGCs.
The use of systemic chemotherapy, especially cisplatin-based combinations, might face some barriers in elderly patients. The choice of systemic therapy should be independent from the chronological age, but based on performance status, comorbidities and also caregivers’ support. In the last years, as a comprehensive molecular characterization of SGCs has been developed, the therapeutic options have potentially expanded, following the principles of precision oncology. However, differently from the patients affected by high-incidence malignancies harboring analogous molecular alterations, patients with molecularly targetable SGCs are penalized by the scarcity of clinical trials specifically dedicated to these rare cancers, and they can access to innovative cancer drugs mostly through basket clinical trials, managed access programs or off-label. The type of primary tumor has to be considered in the algorithm choice; for instance, taxane and gemcitabine are not recommended in AdCC due to the lack of activity. Personalized approaches are feasible, especially for some histotypes as SDC, adenocarcinoma NOS and ca ex-PA. The search for known molecular alterations (e.g. AR and HER2 in SDC and ca ex-PA) is recommended to offer an effective therapeutic alternative to chemotherapy (e.g. ADT in case of AR overexpression; HER2-blockade in case of HER2 overexpression; NTRK inhibitors in case of NTRK fusions).
Next Generation Sequencing is the most cost-effective approach to find further actionable targets, and this technology can be available in referral cancer centers and/or by prescreening of innovative targeted therapy-oriented clinical trials. The availability of new drugs may change among countries, and the participation of fit elderly patients into clinical trials is encouraged (Figure 3). Overall, the management of elderly patients with SGCs is extremely challenging and requires a complex multidisciplinary know-how. The referral to experienced facilities is recommended also for elderly patients, in order to guarantee the most accurate diagnosis and therapeutic opportunities.
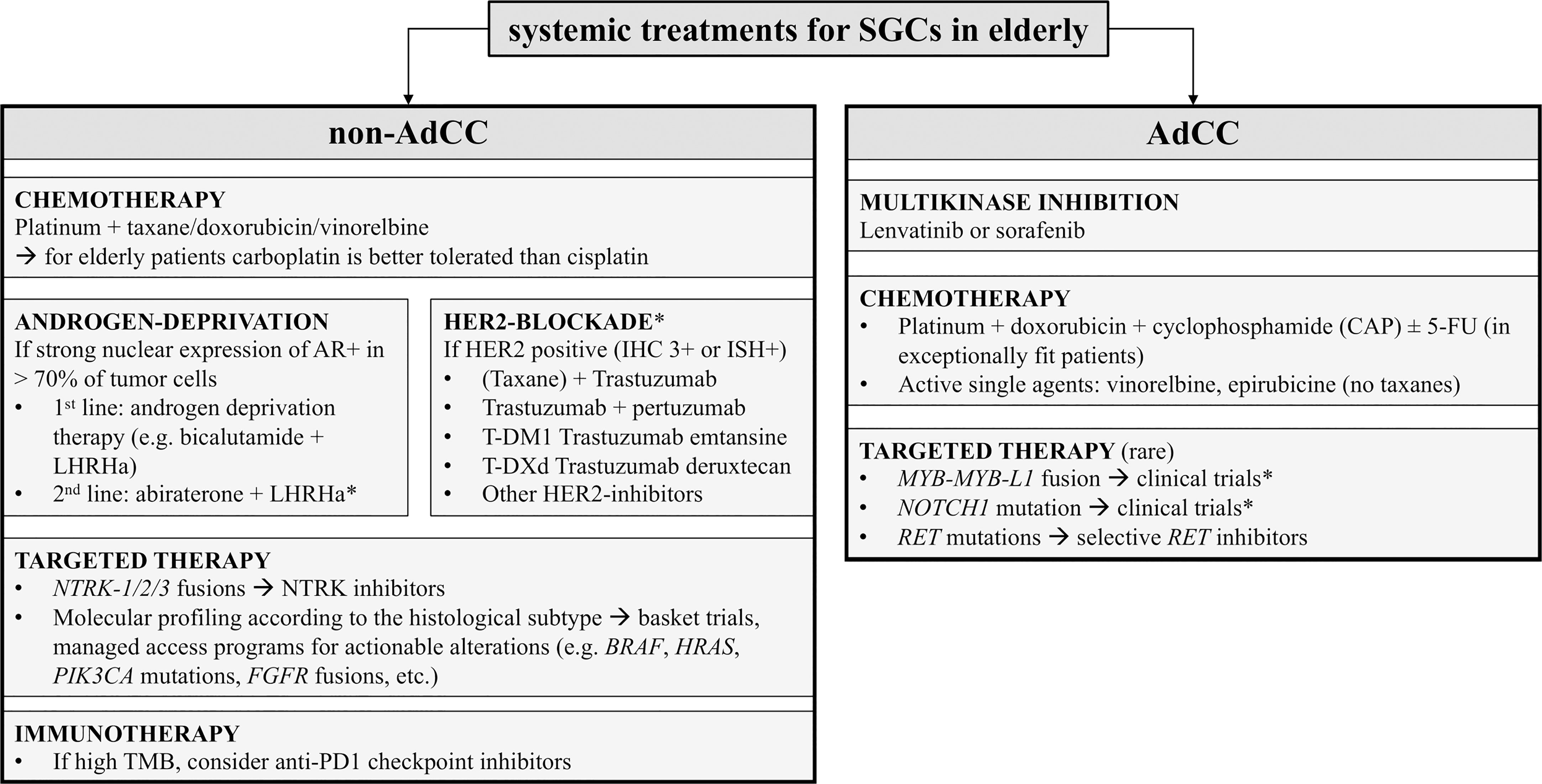
Figure 3 The main strategies for the treatment of patients with salivary gland cancers (AdCC and non-AdCC histotypes) readapted to the elderly population. Therapies marked with (*) have shown activity in clinical trials but are not currently licensed for R/M SGC indication. AR, androgen receptors; LHRH, luteinizing hormone-releasing hormone analogue; HER2, human epidermal growth factor receptor 2, T-DM1, trastuzumab emtansine; NTRK, neurotrophic tyrosine receptor kinase.
EC, CVL, AZ, AJ, GG, FD, LFL, VG, VVP and LDL participated in the concept design of the manuscript. EC and LDL drafted the introduction and discussion sections, developed further by all authors. Each subsection on treatments was written by specialists of the fields: Epidemiology by GG and FD. Surgery by CVL and VVP. Radiation therapy by VG and AZ. Particle therapy by AJ. Systemic therapy by EC, LFL and LDL. All authors contributed to the revision of the final manuscript and approved the submitted version.
VVP and CVL disclosed a financial support for the publication of this article from the Walter Vandeputte Head and Neck Cancer Fund (KU Leuven, Leuven, Belgium). The remaining authors received no financial support for the publication of this article.
Author LFL received occasional conference honoraria/Advisory Board fees from Astrazeneca, Bayer, MSD, Merck-Serono, AccMed, Neutron Therapeutics, Inc. Author LDL received conference honoraria/Advisory Board fees from EISAI, MSD, Merck Serono, McCann Healthcare, Eli Lilly, Sanofi, Sunpharma, IPSEN, Bayer, Roche. Author VVP performed consultancy services for Bristol-Meyers Squibb 2019 and for ATOS medical 2020 and is a surgical trainer for thyroid surgery for Ethicon – J&J. None of these relationships interfere with the intellectual content in the current manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. Ageing and health (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. Marosi C, Köller M. Challenge of cancer in the elderly. ESMO Open (2016) 1(3):e000020. doi: 10.1136/esmoopen-2015-000020
3. Mohile SG, Dale W, Somerfield MR, Schonberg MA, Boyd CM, Burhenn PS, et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO guideline for geriatric oncology. Journal of Clinical Oncology (2018) 36(22):2326–47. doi: 10.1200/JCO.2018.78.8687
4. Haddad RI, Chan ATC, Vermorken JB. Barriers to clinical trial recruitment in head and neck cancer. Oral Oncol (2015) 51(3):203–11. doi: 10.1016/j.oraloncology.2014.12.007
5. Botta L, Gatta G, Trama A, Bernasconi A, Sharon E, Capocaccia R, et al. Incidence and survival of rare cancers in the US and Europe. Cancer Med (2020) 9(15):5632–42. doi: 10.1002/cam4.3137
6. Sanabria A, Carvalho AL, Vartanian JG, Magrin J, Ikeda MK, Kowalski LP. Comorbidity is a prognostic factor in elderly patients with head and neck cancer. Ann Surg Oncol (2007) 14(4):1449–57. doi: 10.1245/s10434-006-9296-1
7. Sanabria A, Carvalho AL, Vartanian JG, Magrin J, Ikeda MK, Kowalski LP. Factors that influence treatment decision in older patients with resectable head and neck cancer. Laryngoscope (2007) 117(5):835–40. doi: 10.1097/MLG.0b013e3180337827
8. WHO Global Cancer Observatory. Salivary glands - source: GLOBOCAN 2020 . Available at: https://gco.iarc.fr/today/data/factsheets/cancers/2-Salivary-glands-fact-sheet.pdf.
9. Radoï L, Barul C, Menvielle G, Carton M, Matrat M, Sanchez M, et al. Risk factors for salivary gland cancers in France: Results from a case-control study, the ICARE study. Oral Oncol (2018) 80:56–63. doi: 10.1016/j.oraloncology.2018.03.019
10. Sawabe M, Ito H, Takahara T, Oze I, Kawakita D, Yatabe Y, et al. Heterogeneous impact of smoking on major salivary gland cancer according to histopathological subtype: A case-control study. Cancer (2018) 124(1):118–24. doi: 10.1002/cncr.30957
11. Caillet P, Canoui-Poitrine F, Vouriot J, Berle M, Reinald N, Krypciak S, et al. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J Clin Oncol (2011) 29(27):3636–42. doi: 10.1200/JCO.2010.31.0664
12. Bellera CA, Rainfray M, Mathoulin-Pélissier S, Mertens C, Delva F, Fonck M, et al. Screening older cancer patients: first evaluation of the G-8 geriatric screening tool. Ann Oncol (2012) 23(8):2166–72. doi: 10.1093/annonc/mdr587
13. Soubeyran P, Bellera C, Goyard J, Heitz D, Curé H, Rousselot H, et al. Screening for vulnerability in older cancer patients: The ONCODAGE prospective multicenter cohort study. PloS One (2014) 9(12):e115060. doi: 10.1371/journal.pone.0115060
14. Pottel L, Boterberg T, Pottel H, Goethals L, Van Den Noortgate N, Duprez F, et al. Determination of an adequate screening tool for identification of vulnerable elderly head and neck cancer patients treated with radio(chemo)therapy. J Geriatric Oncol (2012) 3 (1):24–32. doi: 10.1016/j.jgo.2011.11.006
15. Liuu E, Canouï-Poitrine F, Tournigand C, Laurent M, Caillet P, Le Thuaut A, et al. Accuracy of the G-8 geriatric-oncology screening tool for identifying vulnerable elderly patients with cancer according to tumour site: The ELCAPA-02 study. J Geriatric Oncol (2014) 5(1):11–9. doi: 10.1016/j.jgo.2013.08.003
16. Martinez-Tapia C, Canoui-Poitrine F, Bastuji-Garin S, Soubeyran P, Mathoulin-Pelissier S, Tournigand C, et al. Optimizing the G8 screening tool for older patients with cancer: Diagnostic performance and validation of a six-item version. Oncologist (2016) 21(2):188–95. doi: 10.1634/theoncologist.2015-0326
17. Geiger JL, Ismaila N, Beadle B, Caudell JJ, Chau N, Deschler D, et al. Management of salivary gland malignancy: ASCO guideline. JCO (2021) 39(17):1909–41. doi: 10.1200/JCO.21.00449
18. Terhaard CHJ, van der Schroeff MP, van Schie K, Eerenstein SEJ, Lubsen H, Kaanders JHAM, et al. The prognostic role of comorbidity in salivary gland carcinoma. Cancer (2008) 113(7):1572–9. doi: 10.1002/cncr.23771
19. Becker C, Dahlem KKK, Pfeiffer J. Prognostic value of comorbidities in patients with carcinoma of the major salivary glands. Eur Arch Otorhinolaryngol (2017) 274(3):1651–7. doi: 10.1007/s00405-016-4404-8
20. Bjørndal K, Larsen SR, Therkildsen MH, Kristensen CA, Charabi B, Andersen E, et al. Does age affect prognosis in salivary gland carcinoma patients? a national Danish study. Acta Oncol (2016) 55(sup1):19–22. doi: 10.3109/0284186X.2015.1114671
21. Guzzo M, Locati LD, Prott FJ, Gatta G, McGurk M, Licitra L. Major and minor salivary gland tumors. Crit Rev Oncol Hematol (2010) 74(2):134–48. doi: 10.1016/j.critrevonc.2009.10.004
22. Amin M, Edge S. American Joint committee on cancer: AJCC cancer staging manual. New York: Springer (2017).
23. Venteicher AS, Walcott BP, Sheth SA, Snuderl M, Patel AP, Curry WT, et al. Clinical features of brain metastasis from salivary gland tumors. J Clin Neurosci (2013) 20(11):1533–7. doi: 10.1016/j.jocn.2012.11.024
24. Speight PM, Barrett AW. Salivary gland tumours: diagnostic challenges and an update on the latest WHO classification. Diagn Histopathol (2020) 26(4):147–58. doi: 10.1016/j.mpdhp.2020.01.001
25. Seethala RR, Stenman G. Update from the 4th edition of the world health organization classification of head and neck tumours: Tumors of the salivary gland. Head Neck Pathol (2017) 11 (1):55–67. doi: 10.1007/s12105-017-0795-0
26. AFIP atlas of tumor pathology series 5 | fascicle 5 tumors of the salivary glands . Available at: https://www.arppress.org/product-p/5f05.htm.
27. Ross JS, Gay LM, Wang K, Vergilio JA, Suh J, Ramkissoon S, et al. Comprehensive genomic profiles of metastatic and relapsed salivary gland carcinomas are associated with tumor type and reveal new routes to targeted therapies. Ann Oncol (2017) 28(10):2539–46. doi: 10.1093/annonc/mdx399
28. Di Villeneuve L, Souza IL, Tolentino FDS, Ferrarotto R, Schvartsman G. Salivary gland carcinoma: Novel targets to overcome treatment resistance in advanced disease. Front Oncol (2020) 10:2097. doi: 10.3389/fonc.2020.580141
29. Vander Poorten V, Triantafyllou A, Skálová A, Stenman G, Bishop JA, Hauben E, et al. Polymorphous adenocarcinoma of the salivary glands: reappraisal and update. Eur Arch Otorhinolaryngol (2018) 275(7):1681–95. doi: 10.1007/s00405-018-4985-5
30. Moutasim KA, Thomas GJ. Salivary gland tumours: update on molecular diagnostics. Diagn Histopathol (2020) 26(4):159–64. doi: 10.1016/j.mpdhp.2020.01.002
31. Skálová A, Agaimy A, Vanecek T, Baněčková M, Laco J, Ptáková N, et al. Molecular profiling of clear cell myoepithelial carcinoma of salivary glands with EWSR1 rearrangement identifies frequent PLAG1 gene fusions but no EWSR1 fusion transcripts. Am J Surg Pathol (2021) 45(1):1–13. doi: 10.1097/PAS.0000000000001591
32. Asahina M, Saito T, Hayashi T, Fukumura Y, Mitani K, Yao T. Clinicopathological effect of PLAG1 fusion genes in pleomorphic adenoma and carcinoma ex pleomorphic adenoma with special emphasis on histological features. Histopathology (2019) 74 (3):514–25. doi: 10.1111/his.13759
33. Skálová A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol (2010) 34(5):599–608. doi: 10.1097/PAS.0b013e3181d9efcc
34. Skalova A, Vanecek T, Martinek P, Weinreb I, Stevens TM, Simpson RHW, et al. Molecular profiling of mammary analog secretory carcinoma revealed a subset of tumors harboring a novel ETV6-RET translocation: Report of 10 cases. Am J Surg Pathol (2018) 42 (2):234–46. doi: 10.1097/PAS.0000000000000972
35. Skálová A, Banečkova M, Thompson LDR, Ptáková N, Stevens TM, Brcic L, et al. Expanding the molecular spectrum of secretory carcinoma of salivary glands with a novel VIM-RET fusion. Am J Surg Pathol (2020) 44(10):1295–307. doi: 10.1097/PAS.0000000000001535
36. Rooper LM, Karantanos T, Ning Y, Bishop JA, Gordon SW, Kang H. Salivary secretory carcinoma with a novel ETV6-MET fusion: Expanding the molecular spectrum of a recently described entity. Am J Surg Pathol (2018) 42(8):1121–6. doi: 10.1097/PAS.0000000000001065
37. Skálová A, Sima R, Vanecek T, Muller S, Korabecna M, Nemcova J, et al. Acinic cell carcinoma with high-grade transformation: a report of 9 cases with immunohistochemical study and analysis of TP53 and HER-2/neu genes. Am J Surg Pathol (2009) 33 (8):1137–45. doi: 10.1097/PAS.0b013e3181a38e1c
38. Seethala RR, Hunt JL, Baloch ZW, Livolsi VA, Leon Barnes E. Adenoid cystic carcinoma with high-grade transformation: a report of 11 cases and a review of the literature. Am J Surg Pathol (2007) 31(11):1683–94. doi: 10.1097/PAS.0b013e3180dc928c
39. National cancer institute surveillance, epidemiology, and end results (SEER) program . Available at: https://seer.cancer.gov/.
40. Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin LH, Parkin DM, et al. International classification of diseases for oncology . Available at: https://apps.who.int/iris/handle/10665/42344.
41. Lombardi D, McGurk M, Vander Poorten V, Guzzo M, Accorona R, Rampinelli V, et al. Surgical treatment of salivary malignant tumors. Oral Oncol (2017) 65:102–13. doi: 10.1016/j.oraloncology.2016.12.007
42. Sood S, McGurk M, Vaz F. Management of salivary gland tumours: United kingdom national multidisciplinary guidelines. J Laryngol Otol (2016) 130(S2):S142–9. doi: 10.1017/S0022215116000566
43. Vander Poorten V, Bradley PJ, Takes RP, Rinaldo A, Woolgar JA, Ferlito A. Diagnosis and management of parotid carcinoma with a special focus on recent advances in molecular biology. Head Neck (2012) 34(3):429–40. doi: 10.1002/hed.21706
44. Vander Poorten V, Hunt J, Bradley PJ, Haigentz M, Rinaldo A, Mendenhall WM, et al. Recent trends in the management of minor salivary gland carcinoma. Head Neck (2014) 36(3):444–55. doi: 10.1002/hed.23249
45. Westergaard-Nielsen M, Möller S, Godballe C, Grau Eriksen J, Larsen SR, Kiss K, et al. Prognostic scoring models in parotid gland carcinoma. Head Neck (2021) 43(7):2081–90. doi: 10.1002/hed.26672
46. Peeperkorn S, Meulemans J, Van Lierde C, Laenen A, Valstar MH, Balm AJM, et al. Validated prognostic nomograms for patients with parotid carcinoma predicting 2- and 5-year tumor recurrence-free interval probability. Front Oncol (2020) 10:1535. doi: 10.3389/fonc.2020.01535
47. Vander Poorten VL, Balm AJ, Hilgers FJ, Tan IB, Loftus-Coll BM, Keus RB, et al. Prognostic factors for long term results of the treatment of patients with malignant submandibular gland tumors. Cancer (1999) 85(10):2255–64. doi: 10.1002/(SICI)1097-0142(19990515)85:10<2255::AID-CNCR22>3.0.CO;2-D
48. Lang P-O, Michel J-P, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology (2009) 55(5):539–49. doi: 10.1159/000211949
49. Bakas AT, Sewnaik A, van Straaten J, Baatenburg de Jong RJ, Mattace-Raso FUS, Polinder-Bos HA. The multidimensional prognostic index as a measure of frailty in elderly patients with head and neck cancer. Clin Interv Aging (2021) 16:1679–89. doi: 10.2147/CIA.S323740
50. Thomas CM, Sklar MC, Su J, Xu W, De Almeida JR, Alibhai SMH, et al. Longitudinal assessment of frailty and quality of life in patients undergoing head and neck surgery. Laryngoscope (2021) 131(7):E2232–42. doi: 10.1002/lary.29375
51. Coca-Pelaz A, Halmos GB, Strojan P, de Bree R, Bossi P, Bradford CR, et al. The role of age in treatment-related adverse events in patients with head and neck cancer: A systematic review. Head Neck (2019) 41(7):2410–29. doi: 10.1002/hed.25696
52. Bras L, de Vries J, Festen S, Steenbakkers RJHM, Langendijk JA, Witjes MJH, et al. Frailty and restrictions in geriatric domains are associated with surgical complications but not with radiation-induced acute toxicity in head and neck cancer patients: A prospective study. Oral Oncol (2021) 118:105329. doi: 10.1016/j.oraloncology.2021.105329
53. Bruijnen CP, Heijmer A, van Harten-Krouwel DG, van den Bos F, de Bree R, Witteveen PO, et al. Validation of the G8 screening tool in older patients with cancer considered for surgical treatment. J Geriatr Oncol (2021) 12(5):793–8. doi: 10.1016/j.jgo.2020.10.017
54. McGurk M, Graham Combes J. Controversies in the management of salivary gland disease - Oxford medicine (Oxford: Oxford University Press) (2012). doi: 10.1093/med/9780199578207.001.0001/med-9780199578207.
55. Olsen KD, Moore EJ. Deep lobe parotidectomy: clinical rationale in the management of primary and metastatic cancer. Eur Arch Otorhinolaryngol (2014) 271(5):1181–5. doi: 10.1007/s00405-013-2616-8
56. Olsen KD, Quer M, de Bree R, Vander Poorten V, Rinaldo A, Ferlito A. Deep lobe parotidectomy-why, when, and how? Eur Arch Otorhinolaryngol (2017) 274(12):4073–8. doi: 10.1007/s00405-017-4767-5
57. Stennert E, Kisner D, Jungehuelsing M, Guntinas-Lichius O, Schröder U, Eckel HE, et al. High incidence of lymph node metastasis in major salivary gland cancer. Arch Otolaryngol Head Neck Surg (2003) 129(7):720–3. doi: 10.1001/archotol.129.7.720
58. Klussmann JP, Ponert T, Mueller RP, Dienes HP, Guntinas-Lichius O. Patterns of lymph node spread and its influence on outcome in resectable parotid cancer. Eur J Surg Oncol (2008) 34(8):932–7. doi: 10.1016/j.ejso.2008.02.004
59. Vander Poorten VLM, Hart AAM, van der Laan BFAM, de Jong RJB, Manni JJ, Marres HAM, et al. Prognostic index for patients with parotid carcinoma: External validation using the nationwide 1985-1994 Dutch head and neck oncology cooperative group database. Cancer (2003) 97(6):1453–63. doi: 10.1002/cncr.11254
60. Lombardi D, Accorona R, Lambert A, Mercante G, Coropciuc R, Paderno A, et al. Long-term outcomes and prognosis in submandibular gland malignant tumors: A multicenter study. Laryngoscope (2018) 128(12):2745–50. doi: 10.1002/lary.27236
61. INTERNATIONAL HEAD AND NECK SCIENTIFIC GROUP. Cervical lymph node metastasis in adenoid cystic carcinoma of the major salivary glands. J Laryngol Otol (2017) 131(2):96–105. doi: 10.1017/S0022215116009749
62. Spiro RH. Treating tumors of the sublingual glands, including a useful technique for repair of the floor of the mouth after resection. Am J Surg (1995) 170(5):457–60. doi: 10.1016/S0002-9610(99)80329-8
63. Nishijima W, Tokita N, Takooda S, Tsuchiya S, Watanabe I. Adenocarcinoma of the sublingual gland: case report and 50 year review of the literature. Laryngoscope (1984) 94(1):96–101. doi: 10.1002/lary.5540940118
64. Rinaldo A, Shaha AR, Pellitteri PK, Bradley PJ, Ferlito A. Management of malignant sublingual salivary gland tumors. Oral Oncol (2004) 40(1):2–5. doi: 10.1016/S1368-8375(03)00104-0
65. Orlandi E, Iacovelli NA, Bonora M, Cavallo A, Fossati P. Salivary gland. photon beam and particle radiotherapy: Present and future. Oral Oncol (2016) 60:146–56. doi: 10.1016/j.oraloncology.2016.06.019
66. Frankenthaler RA, Byers RM, Luna MA, Callender DL, Wolf P, Goepfert H. Predicting occult lymph node metastasis in parotid cancer. Arch Otolaryngol Head Neck Surg (1993) 119(5):517–20. doi: 10.1001/archotol.1993.01880170041008
67. Korkmaz H, Yoo GH, Du W, Hocwald E, Otero-Garcia JE, Volkan Adsay N, et al. Predictors of nodal metastasis in salivary gland cancer. J Surg Oncol (2002) 80(4):186–9. doi: 10.1002/jso.10125
68. Nobis C-P, Rohleder NH, Wolff K-D, Wagenpfeil S, Scherer EQ, Kesting MR. Head and neck salivary gland carcinomas–elective neck dissection, yes or no? J Oral Maxillofac Surg (2014) 72(1):205–10. doi: 10.1016/j.joms.2013.05.024
69. Herman MP, Werning JW, Morris CG, Kirwan JM, Amdur RJ, Mendenhall WM. Elective neck management for high-grade salivary gland carcinoma. Am J Otolaryngol (2013) 34(3):205–8. doi: 10.1016/j.amjoto.2012.11.012
70. Terhaard CHJ, Lubsen H, Rasch CRN, Levendag PC, Kaanders HHAM, Tjho-Heslinga RE, et al. The role of radiotherapy in the treatment of malignant salivary gland tumors. Int J Radiat Oncol Biol Phys (2005) 61(1):103–11. doi: 10.1186/1748-717X-6-149
71. Ch’ng S, Ashford BG, Gao K, McGuinness J, Clark JR. Reconstruction of post-radical parotidectomy defects. Plast Reconstr Surg (2012) 129(2):275e–87e. doi: 10.1097/PRS.0b013e318213a11a
72. Emerick KS, Herr MW, Lin DT, Santos F, Deschler DG. Supraclavicular artery island flap for reconstruction of complex parotidectomy, lateral skull base, and total auriculectomy defects. JAMA Otolaryngol Head Neck Surg (2014) 140 (9):861–6. doi: 10.1001/jamaoto.2014.1394
73. Ahmad QG, Navadgi S, Agarwal R, Kanhere H, Shetty KP, Prasad R. Bipaddle pectoralis major myocutaneous flap in reconstructing full thickness defects of cheek: a review of 47 cases. J Plast Reconstr Aesthet Surg (2006) 59(2):166–73. doi: 10.1016/j.bjps.2005.07.008
74. Okland TS, Pepper J-P. Dual nerve transfer for facial reanimation. Facial Plast Surg Clin North Am (2021) 29(3):397–403. doi: 10.1016/j.fsc.2021.03.004
75. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology - head and neck cancers, salivary gland tumors - version 1 (.2022). Available at: https://www.nccn.org.
76. Leong YH, Scher E, Lee N, Tham IW Major salivary glands. in Lee NY, Riaz N, Lu JJ (eds) Target volume delineation for conformal and intensity-modulated radiation therapy. Medical radiology (Switzerland: Springer, Cham) (2015). doi: 10.1007/174_2014_1013
77. Nutting CM, Morden JP, Beasley M, Bhide S, Cook A, De Winton E, et al. Results of a multicentre randomised controlled trial of cochlear- sparing intensity-modulated radiotherapy versus conventional radiotherapy in patients with parotid cancer (COSTAR; CRUK/08/004). Eur J Cancer (2018) 103:249–58. doi: 10.1016/j.ejca.2018.08.006
78. Piram L, Frédéric-Moreau T, Bellini R, Martin F, Miroir J, Saroul N, et al. Delineation of the primary tumour clinical target volumes and neck node levels selection of parotid cancers. Cancer Radiother (2019) 23(3):255–63. doi: 10.1016/j.canrad.2018.07.141
79. Terhaard CHJ. Postoperative and primary radiotherapy for salivary gland carcinomas: indications, techniques, and results. Int J Radiat Oncol Biol Phys (2007) 69(2 Suppl):S52–55. doi: 10.1016/j.ijrobp.2007.04.079
80. Ko HC, Gupta V, Mourad WF, Hu KS, Harrison LB, Som PM, et al. A contouring guide for head and neck cancers with perineural invasion. Pract Radiat Oncol (2014) 4(6):e247–258. doi: 10.1016/j.prro.2014.02.001
81. Armstrong K, Ward J, Hughes NM, Mihai A, Blayney A, Mascott C, et al. Guidelines for clinical target volume definition for perineural spread of major salivary gland cancers. Clin Oncol (R Coll Radiol) (2018) 30(12):773–9. doi: 10.1016/j.clon.2018.08.018
82. Cerda T, Sun XS, Vignot S, Marcy P-Y, Baujat B, Baglin A-C, et al. A rationale for chemoradiation (vs radiotherapy) in salivary gland cancers? on behalf of the REFCOR (French rare head and neck cancer network). Crit Rev Oncol Hematol (2014) 91 (2):142–58. doi: 10.1016/j.critrevonc.2014.02.002
83. Armstrong JG, Harrison LB, Thaler HT, Friedlander-Klar H, Fass DE, Zelefsky MJ, et al. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer (1992) 69(3):615–9. doi: 10.1002/1097-0142(19920201)69:3<615::AID-CNCR2820690303>3.0.CO;2-9
84. Grégoire V, Coche E, Cosnard G, Hamoir M, Reychler H. Selection and delineation of lymph node target volumes in head and neck conformal radiotherapy. proposal for standardizing terminology and procedure based on the surgical experience. Radiother Oncol (2000) 56(2):135–50. doi: 10.1016/s0167-8140(00)00202-4
85. Grégoire V, Ang K, Budach W, Grau C, Hamoir M, Langendijk JA, et al. Delineation of the neck node levels for head and neck tumors: a 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiother Oncol (2014) 110(1):172–81. doi: 10.1016/j.radonc.2013.10.010
86. Bragg CM, Conway J, Robinson MH. The role of intensity-modulated radiotherapy in the treatment of parotid tumors. Int J Radiat Oncol Biol Phys (2002) 52(3):729–38. doi: 10.1016/S0360-3016(01)02660-8
87. Lamers-Kuijper E, Schwarz M, Rasch C, Mijnheer B. Intensity-modulated vs. conformal radiotherapy of parotid gland tumors: potential impact on hearing loss. Med Dosim (2007) 32(4):237–45. doi: 10.1016/j.meddos.2006.12.004
88. Nutting CM, Rowbottom CG, Cosgrove VP, Henk JM, Dearnaley DP, Robinson MH, et al. Optimisation of radiotherapy for carcinoma of the parotid gland: a comparison of conventional, three-dimensional conformal, and intensity-modulated techniques. Radiother Oncol (2001) 60(2):163–72. doi: 10.1016/S0167-8140(01)00339-5
89. Grewal AS, Jones J, Lin A. Palliative radiation therapy for head and neck cancers. Int J Radiat Oncol Biol Phys (2019) 105(2):254–66. doi: 10.1016/j.ijrobp.2019.05.024
90. Rühle A, Rothhaar S, Haehl E, Kalckreuth T, Sprave T, Stoian R, et al. Radiation-induced toxicities and outcomes after radiotherapy are independent of patient age in elderly salivary gland cancer patients: results from a matched-pair analysis of a rare disease. Eur Arch Otorhinolaryngol (2021) 278(7):2537–48. doi: 10.1007/s00405-020-06393-x
91. Pignon T, Horiot JC, Van den Bogaert W, Van Glabbeke M, Scalliet P. No age limit for radical radiotherapy in head and neck tumours. Eur J Cancer (1996) 32A(12):2075–81. doi: 10.1016/S0959-8049(96)00265-1
92. Griffin TW, Pajak TF, Laramore GE, Duncan W, Richter MP, Hendrickson FR, et al. Neutron vs photon irradiation of inoperable salivary gland tumors: results of an RTOG-MRC cooperative randomized study. Int J Radiat Oncol Biol Phys (1988) 15 (5):1085–90. doi: 10.1016/0360-3016(88)90188-5
93. Laramore GE, Krall JM, Griffin TW, Duncan W, Richter MP, Saroja KR, et al. Neutron versus photon irradiation for unresectable salivary gland tumors: final report of an RTOG-MRC randomized clinical trial. radiation therapy oncology group. medical research council. Int J Radiat Oncol Biol Phys (1993) 27(2):235–40. doi: 10.1016/0360-3016(93)90233-L
94. Mizoe J-E, Tsujii H, Kamada T, Matsuoka Y, Tsuji H, Osaka Y, et al. Dose escalation study of carbon ion radiotherapy for locally advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys (2004) 60(2):358–64. doi: 10.1016/j.ijrobp.2004.02.067
95. Mizoe J-E, Hasegawa A, Jingu K, Takagi R, Bessyo H, Morikawa T, et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother Oncol (2012) 103(1):32–7. doi: 10.1016/j.radonc.2011.12.013
96. Koto M, Demizu Y, Saitoh J-I, Suefuji H, Tsuji H, Okimoto T, et al. Definitive carbon-ion radiation therapy for locally advanced sinonasal malignant tumors: Subgroup analysis of a multicenter study by the Japan carbon-ion radiation oncology study group (J-CROS). Int J Radiat Oncol Biol Phys (2018) 102(2):353–61. doi: 10.1016/j.ijrobp.2018.05.074
97. Shirai K, Koto M, Demizu Y, Suefuji H, Ohno T, Tsuji H, et al. Multi-institutional retrospective study of mucoepidermoid carcinoma treated with carbon-ion radiotherapy. Cancer Sci (2017) 108(7):1447–51. doi: 10.1111/cas.13270
98. Sulaiman NS, Demizu Y, Koto M, Saitoh J-I, Suefuji H, Tsuji H, et al. Multicenter study of carbon-ion radiation therapy for adenoid cystic carcinoma of the head and neck: Subanalysis of the Japan carbon-ion radiation oncology study group (J-CROS) study (1402 HN). Int J Radiat Oncol Biol Phys (2018) 100(3):639–46. doi: 10.1016/j.ijrobp.2017.11.010
99. Hayashi K, Koto M, Demizu Y, Saitoh J-I, Suefuji H, Okimoto T, et al. A retrospective multicenter study of carbon-ion radiotherapy for major salivary gland carcinomas: Subanalysis of J-CROS 1402 HN. Cancer Sci (2018) 109(5):1576–82. doi: 10.1111/cas.13558
100. Abe T, Ohno T, Koto M, Demizu Y, Suefuji H, Tsuji H, et al. A multi-institutional retrospective study of carbon-ion radiotherapy for non-squamous cell malignant tumors of the nasopharynx: Subanalysis of Japan carbon-ion radiation oncology study group study 1402 HN. Cancer Med (2018) 7(12):6077–83. doi: 10.1002/cam4.1884
101. Hayashi K, Koto M, Demizu Y, Saitoh J-I, Suefuji H, Okimoto T, et al. A retrospective multicenter study of carbon-ion radiotherapy for external auditory canal and middle ear carcinomas. Cancer Med (2019) 8(1):51–7. doi: 10.1002/cam4.1830
102. Schulz-Ertner D, Nikoghosyan A, Didinger B, Münter M, Jäkel O, Karger CP, et al. Therapy strategies for locally advanced adenoid cystic carcinomas using modern radiation therapy techniques. Cancer (2005) 104(2):338–44. doi: 10.1002/cncr.21158
103. Jensen AD, Nikoghosyan AV, Poulakis M, Höss A, Haberer T, Jäkel O, et al. Combined intensity-modulated radiotherapy plus raster-scanned carbon ion boost for advanced adenoid cystic carcinoma of the head and neck results in superior locoregional control and overall survival. Cancer (2015) 121(17):3001–9. doi: 10.1002/cncr.29443
104. Jensen AD, Nikoghosyan AV, Lossner K, Haberer T, Jäkel O, Münter MW, et al. COSMIC: A regimen of intensity modulated radiation therapy plus dose-escalated, raster-scanned carbon ion boost for malignant salivary gland tumors: Results of the prospective phase 2 trial. Int J Radiat Oncol Biol Phys (2015) 93(1):37–46. doi: 10.1016/j.ijrobp.2015.05.013
105. Jensen AD, Poulakis M, Nikoghosyan AV, Welzel T, Uhl M, Federspil PA, et al. High-LET radiotherapy for adenoid cystic carcinoma of the head and neck: 15 years’ experience with raster-scanned carbon ion therapy. Radiother Oncol (2016) 118 (2):272–80. doi: 10.1016/j.radonc.2015.05.010
106. Akbaba S, Lang K, Held T, Herfarth K, Rieber J, Plinkert P, et al. Carbon-ion radiotherapy in accelerated hypofractionated active raster-scanning technique for malignant lacrimal gland tumors: feasibility and safety. Cancer Manag Res (2019) 11:1155–66. doi: 10.2147/CMAR.S190051
107. Akbaba S, Ahmed D, Lang K, Held T, Mattke M, Hoerner-Rieber J, et al. Results of a combination treatment with intensity modulated radiotherapy and active raster-scanning carbon ion boost for adenoid cystic carcinoma of the minor salivary glands of the nasopharynx. Oral Oncol (2019) 91:39–46. doi: 10.1016/j.oraloncology.2019.02.019
108. Pommier P, Liebsch NJ, Deschler DG, Lin DT, McIntyre JF, Barker FG, et al. Proton beam radiation therapy for skull base adenoid cystic carcinoma. Arch Otolaryngol Head Neck Surg (2006) 132(11):1242–9. doi: 10.1001/archotol.132.11.1242
109. Linton OR, Moore MG, Brigance JS, Summerlin D-J, McDonald MW. Proton therapy for head and neck adenoid cystic carcinoma: initial clinical outcomes. Head Neck (2015) 37(1):117–24. doi: 10.1002/hed.23573
110. Gentile MS, Yip D, Liebsch NJ, Adams JA, Busse PM, Chan AW. Definitive proton beam therapy for adenoid cystic carcinoma of the nasopharynx involving the base of skull. Oral Oncol (2017) 65:38–44. doi: 10.1016/j.oraloncology.2016.11.016
111. Dautruche A, Bolle S, Feuvret L, Le Tourneau C, Jouffroy T, Goudjil F, et al. Three-year results after radiotherapy for locally advanced sinonasal adenoid cystic carcinoma, using highly conformational radiotherapy techniques proton therapy and/or tomotherapy. Cancer Radiother (2018) 22(5):411–6. doi: 10.1016/j.canrad.2017.11.015
112. Pelak MJ, Walser M, Bachtiary B, Hrbacek J, Lomax AJ, Kliebsch UL, et al. Clinical outcomes of head and neck adenoid cystic carcinoma patients treated with pencil beam-scanning proton therapy. Oral Oncol (2020) 107:104752. doi: 10.1016/j.oraloncology.2020.104752
113. Vischioni B, Dhanireddy B, Severo C, Bonora M, Ronchi S, Vitolo V, et al. Reirradiation of salivary gland tumors with carbon ion radiotherapy at CNAO. Radiother Oncol (2020) 145:172–7. doi: 10.1016/j.radonc.2020.01.004
114. Jensen AD, Poulakis M, Nikoghosyan AV, Chaudhri N, Uhl M, Münter MW, et al. Re-irradiation of adenoid cystic carcinoma: analysis and evaluation of outcome in 52 consecutive patients treated with raster-scanned carbon ion therapy. Radiother Oncol (2015) 114(2):182–8. doi: 10.1016/j.radonc.2015.01.002
115. Held T, Windisch P, Akbaba S, Lang K, El Shafie R, Bernhardt D, et al. Carbon ion reirradiation for recurrent head and neck cancer: A single-institutional experience. Int J Radiat Oncol Biol Phys (2019) 105(4):803–11. doi: 10.1016/j.ijrobp.2019.07.021
116. Hayashi K, Koto M, Ikawa H, Hagiwara Y, Tsuji H, Ogawa K, et al. Feasibility of re-irradiation using carbon ions for recurrent head and neck malignancies after carbon-ion radiotherapy. Radiother Oncol (2019) 136:148–53. doi: 10.1016/j.radonc.2019.04.007
117. Weber DC, Chan AW, Lessell S, McIntyre JF, Goldberg SI, Bussiere MR, et al. Visual outcome of accelerated fractionated radiation for advanced sinonasal malignancies employing photons/protons. Radiother Oncol (2006) 81(3):243–9. doi: 10.1016/j.radonc.2006.09.009
118. Ikawa H, Koto M, Hayashi K, Tonogi M, Takagi R, Nomura T, et al. Feasibility of carbon-ion radiotherapy for oral non-squamous cell carcinomas. Head Neck (2019) 41(6):1795–803. doi: 10.1002/hed.25618
119. Ikawa H, Koto M, Demizu Y, Saitoh J, Suefuji H, Okimoto T, et al. Multicenter study of carbon-ion radiation therapy for nonsquamous cell carcinomas of the oral cavity. Cancer Med (2019) 8(12):5482–91. doi: 10.1002/cam4.2408
120. Hagiwara Y, Koto M, Bhattacharyya T, Hayashi K, Ikawa H, Nemoto K, et al. Long-term outcomes and toxicities of carbon-ion radiotherapy in malignant tumors of the sphenoid sinus. Head Neck (2020) 42(1):50–8. doi: 10.1002/hed.25965
121. Hayashi K, Koto M, Ikawa H, Ogawa K, Kamada T. Efficacy and safety of carbon-ion radiotherapy for lacrimal gland carcinomas with extraorbital extension: a retrospective cohort study. Oncotarget (2018) 9(16):12932–40. doi: 10.18632/oncotarget.24390
122. Koto M, Hasegawa A, Takagi R, Ikawa H, Naganawa K, Mizoe J-E, et al. Definitive carbon-ion radiotherapy for locally advanced parotid gland carcinomas. Head Neck (2017) 39(4):724–9. doi: 10.1002/hed.24671
123. Koto M, Hasegawa A, Takagi R, Ikawa H, Naganawa K, Mizoe J-E, et al. Evaluation of the safety and efficacy of carbon ion radiotherapy for locally advanced adenoid cystic carcinoma of the tongue base. Head Neck (2016) 38 Suppl 1:E2122–2126. doi: 10.1002/hed.24397
124. Lang K, Baur M, Akbaba S, Held T, Kargus S, Bougatf N, et al. Intensity modulated radiotherapy (IMRT) + carbon ion boost for adenoid cystic carcinoma of the minor salivary glands in the oral cavity. Cancers (Basel) (2018) 10 (12):E488. doi: 10.3390/cancers10120488
125. Morimoto K, Demizu Y, Hashimoto N, Mima M, Terashima K, Fujii O, et al. Particle radiotherapy using protons or carbon ions for unresectable locally advanced head and neck cancers with skull base invasion. Jpn J Clin Oncol (2014) 44(5):428–34. doi: 10.1093/jjco/hyu010
126. Takagi M, Demizu Y, Hashimoto N, Mima M, Terashima K, Fujii O, et al. Treatment outcomes of particle radiotherapy using protons or carbon ions as a single-modality therapy for adenoid cystic carcinoma of the head and neck. Radiother Oncol (2014) 113 (3):364–70. doi: 10.1016/j.radonc.2014.11.031
127. Lesueur P, Rapeaud E, De Marzi L, Goudjil F, Levy C, Galatoire O, et al. Adenoid cystic carcinoma of the lacrimal gland: High dose adjuvant proton therapy to improve patients outcomes. Front Oncol (2020) 10:135. doi: 10.3389/fonc.2020.00135
128. Hu W, Hu J, Huang Q, Gao J, Yang J, Qiu X, et al. Particle beam radiation therapy for adenoid cystic carcinoma of the nasal cavity and paranasal sinuses. Front Oncol (2020) 10:572493. doi: 10.3389/fonc.2020.572493
129. Shirai K, Saitoh J-I, Musha A, Abe T, Kobayashi D, Takahashi T, et al. Prospective observational study of carbon-ion radiotherapy for non-squamous cell carcinoma of the head and neck. Cancer Sci (2017) 108(10):2039–44. doi: 10.1111/cas.13325
130. McDonald MW, Zolali-Meybodi O, Lehnert SJ, Estabrook NC, Liu Y, Cohen-Gadol AA, et al. Reirradiation of recurrent and second primary head and neck cancer with proton therapy. Int J Radiat Oncol Biol Phys (2016) 96(4):808–19. doi: 10.1016/j.ijrobp.2016.07.037
131. Akbaba S, Rühle A, Rothhaar S, Zamboglou C, Gkika E, Foerster R, et al. Treatment outcomes of elderly salivary gland cancer patients undergoing radiotherapy – results from a large multicenter analysis. Radiother Oncol (2021) 156:266–74. doi: 10.1016/j.radonc.2020.12.024
132. van Boxtel W, Locati LD, van Engen-van Grunsven ACH, Bergamini C, Jonker MA, Fiets E, et al. Adjuvant androgen deprivation therapy for poor-risk, androgen receptor–positive salivary duct carcinoma. Eur J Cancer (2019) 110:62–70. doi: 10.1016/j.ejca.2018.12.035
133. Hanna GJ, Bae JE, Lorch JH, Haddad RI, Jo VY, Schoenfeld JD, et al. The benefits of adjuvant trastuzumab for HER-2-Positive salivary gland cancers. Oncologist (2020) 25(7):598–608. doi: 10.1634/theoncologist.2019-0841
134. Glazer TA, Shuman AG. Distant metastases and palliative care. Adv Oto Rhino Laryngol (2016) 78:182–8. doi: 10.1159/000442139
135. van Weert S, Bloemena E, van der Waal I, de Bree R, Rietveld DHF, Kuik JD, et al. Adenoid cystic carcinoma of the head and neck: A single-center analysis of 105 consecutive cases over a 30-year period. Oral Oncol (2013) 49(8):824–9. doi: 10.1016/j.oraloncology.2013.05.004
136. Choi Y, Kim S-B, Yoon DH, Kim JY, Lee S, Cho K-J. Clinical characteristics and prognostic factors of adenoid cystic carcinoma of the head and neck. Laryngoscope (2013) 123(6):1430–8. doi: 10.1002/lary.23976
137. Cavalieri S, Mariani L, Vander Poorten V, Van Breda L, Cau MC, Lo Vullo S, et al. Prognostic nomogram in patients with metastatic adenoid cystic carcinoma of the salivary glands. Eur J Cancer (2020) 136:35–42. doi: 10.1016/j.ejca.2020.05.013
138. Licitra L, Cavina R, Grandi C, Palma SD, Guzzo M, Demicheli R, et al. Cisplatin, doxorubicin and cyclophosphamide in advanced salivary gland carcinoma. A phase II trial of 22 patients. Ann Oncol (1996) 7(6):640–2. doi: 10.1093/oxfordjournals.annonc.a010684
139. Airoldi M, Fornari G, Pedani F, Marchionatti S, Gabriele P, Succo G, et al. Paclitaxel and carboplatin for recurrent salivary gland malignancies. Anticancer Res (2000) 20(5C):3781–3.
140. Airoldi M, Pedani F, Succo G, Gabriele AM, Ragona R, Marchionatti S, et al. Phase II randomized trial comparing vinorelbine versus vinorelbine plus cisplatin in patients with recurrent salivary gland malignancies. Cancer (2001) 91 (3):541–7. doi: 10.1002/1097-0142(20010201)91:3<541::AID-CNCR1032>3.0.CO;2-Y
141. Laurie SA, Siu LL, Winquist E, Maksymiuk A, Harnett EL, Walsh W, et al. A phase 2 study of platinum and gemcitabine in patients with advanced salivary gland cancer: a trial of the NCIC clinical trials group. Cancer (2010) 116(2):362–8. doi: 10.1002/cncr.24745
142. Nakano K, Sato Y, Sasaki T, Shimbashi W, Fukushima H, Yonekawa H, et al. Combination chemotherapy of carboplatin and paclitaxel for advanced/metastatic salivary gland carcinoma patients: differences in responses by different pathological diagnoses. Acta Otolaryngol (2016) 136(9):948–51. doi: 10.3109/00016489.2016.1170876
143. Okada T, Saotome T, Nagao T, Masubuchi T, Fushimi C, Matsuki T, et al. Carboplatin and docetaxel in patients with salivary gland carcinoma: A retrospective study. In Vivo (2019) 33(3):843–53. doi: 10.21873/invivo.11549
144. Licitra L, Marchini S, Spinazzè S, Rossi A, Rocca A, Grandi C, et al. Cisplatin in advanced salivary gland carcinoma. a phase II study of 25 patients. Cancer (1991) 68(9):1874–7. doi: 10.1002/1097-0142(19911101)68:9<1874::aid-cncr2820680904>3.0.co;2-s
145. Gilbert J, Li Y, Pinto HA, Jennings T, Kies MS, Silverman P, et al. Phase II trial of taxol in salivary gland malignancies (E1394): a trial of the Eastern cooperative oncology group. Head Neck (2006) 28 (3):197–204. doi: 10.1002/hed.20327
146. Sempere-Bigorra M, Julián-Rochina I, Cauli O. Chemotherapy-induced neuropathy and diabetes: A scoping review. Curr Oncol (2021) 28(4):3124–38. doi: 10.3390/curroncol28040273
147. Dalin MG, Watson PA, Ho AL, Morris LGT. Androgen receptor signaling in salivary gland cancer. Cancers (Basel) (2017) 9(2):17. doi: 10.3390/cancers9020017
148. D'heygere E, Meulemans J, Vander Poorten V. Salivary duct carcinoma. Curr Opin Otolaryngol Head Neck Surg (2018) 26(2):142–51. doi: 10.1097/MOO.0000000000000436
149. Fushimi C, Tada Y, Takahashi H, Nagao T, Ojiri H, Masubuchi T, et al. A prospective phase II study of combined androgen blockade in patients with androgen receptor-positive metastatic or locally advanced unresectable salivary gland carcinoma. Ann Oncol (2018) 29(4):979–84. doi: 10.1093/annonc/mdx771
150. Viscuse PV, Price KA, Garcia JJ, Schembri-Wismayer DJ, Chintakuntlawar AV. First line androgen deprivation therapy vs. chemotherapy for patients with androgen receptor positive recurrent or metastatic salivary gland carcinoma-a retrospective study. Front Oncol (2019) 9:701. doi: 10.3389/fonc.2019.00701
151. Ho AL, Foster NR, Zoroufy AJ, Worden FP, Price KA, Adkins D, et al Alliance A091404: A phase II study of enzalutamide (NSC# 766085) for patients with androgen receptor-positive salivary cancers. J Clin Oncol (2019) 37(15_suppl):6020. doi: 10.1200/JCO.2019.37.15_suppl.6020
152. Locati LD, Cavalieri S, Bergamini C, Resteghini C, Colombo E, Calareso G, et al. Abiraterone acetate in patients with castration-resistant, androgen receptor–expressing salivary gland cancer: A phase II trial. JCO (2021) 39(36):4061–8. doi: 10.1200/JCO.21.00468
153. Locati LD, Perrone F, Cortelazzi B, Lo Vullo S, Bossi P, Dagrada G, et al. Clinical activity of androgen deprivation therapy in patients with metastatic/relapsed androgen receptor-positive salivary gland cancers. Head Neck (2016) 38 (5):724–31. doi: 10.1002/hed.23940
154. van Boxtel W, Verhaegh GW, van Engen-van Grunsven IA, van Strijp D, Kroeze LI, Ligtenberg MJ, et al. Prediction of clinical benefit from androgen deprivation therapy in salivary duct carcinoma patients. Int J Cancer (2020) 146(11):3196–206. doi: 10.1002/ijc.32795
155. Ho AL. Androgen receptor pathway in salivary gland cancer. J Clin Oncol (2022) 39(36):4069–72. doi: 10.1200/JCO.21.01983
156. Yang RK, Zhao P, Lu C, Luo J, Hu R. Expression pattern of androgen receptor and AR-V7 in androgen-deprivation therapy-naïve salivary duct carcinomas. Hum Pathol (2019) 84:173–82. doi: 10.1016/j.humpath.2018.09.009
157. Cappelletti V, Miodini P, Reduzzi C, Alfieri S, Daidone MG, Licitra L, et al. Tailoring treatment of salivary duct carcinoma (SDC) by liquid biopsy: ARv7 expression in circulating tumor cells. Ann Oncol (2018) 29(7):1599–601. doi: 10.1093/annonc/mdy141
158. Nimir M, Ma Y, Jeffreys SA, Opperman T, Young F, Khan T, et al. Detection of AR-V7 in liquid biopsies of castrate resistant prostate cancer patients: A comparison of AR-V7 analysis in circulating tumor cells, circulating tumor RNA and exosomes. Cells (2019) 8(7):E688. doi: 10.3390/cells8070688
159. Jeong ISD, Moyers J, Thung I, Thinn MM. Combination chemohormonal therapy in metastatic salivary duct carcinoma. Am J Case Rep (2020) 21:e925181. doi: 10.12659/AJCR.925181
160. Can NT, Lingen MW, Mashek H, McElherne J, Briese R, Fitzpatrick C, et al. Expression of hormone receptors and HER-2 in benign and malignant salivary gland tumors. Head Neck Pathol (2018) 12 (1):95–104. doi: 10.1007/s12105-017-0833-y
161. Egebjerg K, Harwood CD, Woller NC, Kristensen CA, Mau-Sørensen M. HER2 positivity in histological subtypes of salivary gland carcinoma: A systematic review and meta-analysis. Front Oncol (2021) 11:2154. doi: 10.3389/fonc.2021.693394
162. Agulnik M, Cohen EWE, Cohen RB, Chen EX, Vokes EE, Hotte SJ, et al. Phase II study of lapatinib in recurrent or metastatic epidermal growth factor receptor and/or erbB2 expressing adenoid cystic carcinoma and non adenoid cystic carcinoma malignant tumors of the salivary glands. J Clin Oncol (2007) 25(25):3978–84. doi: 10.1200/JCO.2007.11.8612
163. Limaye SA, Posner MR, Krane JF, Fonfria M, Lorch JH, Dillon DA, et al. Trastuzumab for the treatment of salivary duct carcinoma. Oncologist (2013) 18(3):294–300. doi: 10.1634/theoncologist.2012-0369
164. Takahashi H, Tada Y, Saotome T, Akazawa K, Ojiri H, Fushimi C, et al. Phase II trial of trastuzumab and docetaxel in patients with human epidermal growth factor receptor 2-positive salivary duct carcinoma. J Clin Oncol (2019) 37 (2):125–34. doi: 10.1200/JCO.18.00545
165. Kurzrock R, Bowles DW, Kang H, Meric-Bernstam F, Hainsworth J, Spigel DR, et al. Targeted therapy for advanced salivary gland carcinoma based on molecular profiling: results from MyPathway, a phase IIa multiple basket study. Ann Oncol (2020) 31 (3):412–21. doi: 10.1016/j.annonc.2019.11.018
166. Swed BL, Cohen RB, Aggarwal C. Targeting HER2/neu oncogene overexpression with ado-trastuzumab emtansine in the treatment of metastatic salivary gland neoplasms: A single-institution experience. JCO Precis Oncol (2019) 3:1–4. doi: 10.1200/PO.18.00351
167. Li BT, Shen R, Offin M, Buonocore DJ, Myers ML, Venkatesh A, et al. Ado-trastuzumab emtansine in patients with HER2 amplified salivary gland cancers (SGCs): Results from a phase II basket trial. JCO (2019) 37 (15_suppl):6001–1. doi: 10.1200/JCO.2019.37.15_suppl.6001
168. Jhaveri KL, Wang XV, Makker V, Luoh S-W, Mitchell EP, Zwiebel JA, et al. Ado-trastuzumab emtansine (T-DM1) in patients with HER2-amplified tumors excluding breast and gastric/gastroesophageal junction (GEJ) adenocarcinomas: results from the NCI-MATCH trial (EAY131) subprotocol q. Ann Oncol (2019) 30(11):1821–30. doi: 10.1093/annonc/mdz291
169. Tsurutani J, Iwata H, Krop I, Jänne PA, Doi T, Takahashi S, et al. Targeting HER2 with trastuzumab deruxtecan: A dose-expansion, phase I study in multiple advanced solid tumors. Cancer Discovery (2020) 10 (5):688–701. doi: 10.1158/2159-8290.CD-19-1014
170. Santana T, Pavel A, Martinek P, Steiner P, Grossmann P, Baněčková M, et al. Biomarker immunoprofile and molecular characteristics in salivary duct carcinoma: clinicopathological and prognostic implications. Hum Pathol (2019) 93:37–47. doi: 10.1016/j.humpath.2019.08.009
171. Ho AS, Ochoa A, Jayakumaran G, Zehir A, Valero Mayor C, Tepe J, et al. Genetic hallmarks of recurrent/metastatic adenoid cystic carcinoma. J Clin Invest (2019) 129(10):4276–89. doi: 10.1172/JCI128227
172. Tchekmedyian V, Sherman EJ, Dunn L, Tran C, Baxi S, Katabi N, et al. Phase II study of lenvatinib in patients with progressive, recurrent or metastatic adenoid cystic carcinoma. JCO (2019) 37(18):1529–37. doi: 10.1200/JCO.18.01859
173. Locati LD, Perrone F, Cortelazzi B, Bergamini C, Bossi P, Civelli E, et al. A phase II study of sorafenib in recurrent and/or metastatic salivary gland carcinomas: Translational analyses and clinical impact. Eur J Cancer (2016) 69:158–65. doi: 10.1016/j.ejca.2016.09.022
174. Locati LD, Galbiati D, Calareso G, Alfieri S, Singer S, Cavalieri S, et al. Patients with adenoid cystic carcinomas of the salivary glands treated with lenvatinib: Activity and quality of life. Cancer (2020) 126(9):1888–94. doi: 10.1002/cncr.32754
175. Kang EJ, Ahn MJ, Ock CY, Lee KW, Kwon JH, Yang Y, et al. Randomized phase II study of axitinib versus observation in patients with recurred or metastatic adenoid cystic carcinoma. Clin Cancer Res (2021) 27(19):5272–9. doi: 10.1158/1078-0432.CCR-21-1061
176. Ho AS, Kannan K, Roy DM, Morris LGT, Ganly I, Katabi N, et al. The mutational landscape of adenoid cystic carcinoma. Nat Genet (2013) 45(7):791–8. doi: 10.1038/ng.2643
177. Yusenko MV, Trentmann A, Andersson MK, Ghani LA, Jakobs A, Arteaga Paz M-F, et al. Monensin, a novel potent MYB inhibitor, suppresses proliferation of acute myeloid leukemia and adenoid cystic carcinoma cells. Cancer Lett (2020) 479:61–70. doi: 10.1016/j.canlet.2020.01.039
178. Ferrarotto R, Mitani Y, Diao L, Guijarro I, Wang J, Zweidler-McKay P, et al. Activating NOTCH1 mutations define a distinct subgroup of patients with adenoid cystic carcinoma who have poor prognosis, propensity to bone and liver metastasis, and potential responsiveness to Notch1 inhibitors. J Clin Oncol (2017) 35(3):352–60. doi: 10.1200/JCO.2016.67.5264
179. Ferrarotto R, Wirth LJ, Muzaffar J, Rodriguez CP, Xia B, Perez CA, et al. ACCURACY a phase II trial of AL101, a selective gamma secretase inhibitor, in subjects with recurrent/metastatic (R/M) adenoid cystic carcinoma (ACC) harboring notch activating mutations (Notchmut). Ann Oncol (2020) 2020:S599–628. doi: 10.1016/j.annonc.2020.08.1034
180. Ho AL, Bowles DW, Even C, Hao D, Kang R, Metcalf R, et al. ACCURACY: A phase II trial of AL101, a selective gamma secretase inhibitor, in subjects with recurrent/metastatic (R/M) adenoid cystic carcinoma (ACC) harboring notch activating mutations (Notchmut): Results of 6-mg cohort. Ann Oncol (2021) 2021:S786–817. doi: 10.1016/j.annonc.2021.08.1314
181. Locati LD, Cavalieri S, Bergamini C, Resteghini C, Alfieri S, Calareso G, et al. Phase II trial with axitinib in recurrent and/or metastatic salivary gland cancers of the upper aerodigestive tract. Head Neck (2019) 41(10):3670–6. doi: 10.1002/hed.25891
182. Le X, Baik C, Bauman J, Gilbert J, Brose MS, Grilley-Olson JE, et al. Efficacy and safety of larotrectinib in patients with advanced TRK fusion salivary gland cancer. The Oncologist (2022) oyac080. doi: 10.1093/oncolo/oyac080
183. Doebele RC, Drilon A, Paz-Ares L, Siena S, Shaw AT, Farago AF, et al. Entrectinib in patients with advanced or metastatic NTRK fusion- positive solid tumours: integrated analysis of three phase 1–2 trials. Lancet Oncol (2020) 21 (2):271–82. doi: 10.1016/S1470-2045(19)30691-6
184. Drilon A, Li G, Dogan S, Gounder M, Shen R, Arcila M, et al. What hides behind the MASC: clinical response and acquired resistance to entrectinib after ETV6-NTRK3 identification in a mammary analogue secretory carcinoma (MASC). Ann Oncol (2016) 27(5):920–6. doi: 10.1093/annonc/mdw042
185. Hemming ML, Nathenson MJ, Lin J-R, Mei S, Du Z, Malik K, et al. Response and mechanisms of resistance to larotrectinib and selitrectinib in metastatic undifferentiated sarcoma harboring oncogenic fusion of NTRK1. JCO Precis Oncol (2020) 4:79–90. doi: 10.1200/PO.19.00287
186. Cocco E, Schram AM, Kulick A, Misale S, Won HH, Yaeger R, et al. Resistance to TRK inhibition mediated by convergent MAPK pathway activation. Nat Med (2019) 25(9):1422–7. doi: 10.1038/s41591-019-0542-z
187. Murray BW, Rogers E, Zhai D, Deng W, Chen X, Sprengeler PA, et al. Molecular characteristics of repotrectinib that enable potent inhibition of TRK fusion proteins and resistant mutations. Mol Cancer Ther (2021) 20(12):2446–56. doi: 10.1158/1535-7163.MCT-21-0632
188. Florou V, Nevala-Plagemann C, Whisenant J, Maeda P, Gilcrease GW, Garrido-Laguna I. Clinical activity of selitrectinib in a patient with mammary analogue secretory carcinoma of the parotid gland with secondary resistance to entrectinib. J Natl Compr Canc Netw (2021) 19(5):478–82. doi: 10.6004/jnccn.2021.7022
189. Mosele F, Remon J, Mateo J, Westphalen CB, Barlesi F, Lolkema MP, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO precision medicine working group. Ann Oncol (2020) 31 (11):1491–505. doi: 10.1016/j.annonc.2020.07.014
190. Belli C, Penault-Llorca F, Ladanyi M, Normanno N, Scoazec J-Y, Lacroix L, et al. ESMO recommendations on the standard methods to detect RET fusions and mutations in daily practice and clinical research. Ann Oncol (2021) 32(3):337–50. doi: 10.1016/j.annonc.2020.11.021
191. Nardi V, Sadow PM, Juric D, Zhao D, Cosper AK, Bergethon K, et al. Detection of novel actionable genetic changes in salivary duct carcinoma helps direct patient treatment. Clin Cancer Res (2013) 19(2):480–90. doi: 10.1158/1078-0432.CCR-12-1842
192. Wang K, Russell JS, McDermott JD, Elvin JA, Khaira D, Johnson A, et al. Profiling of 149 salivary duct carcinomas, carcinoma ex pleomorphic adenomas, and adenocarcinomas, not otherwise specified reveals actionable genomic alterations. Clin Cancer Res (2016) 22(24):6061–8. doi: 10.1158/1078-0432.CCR-15-2568
193. Gargano SM, Senarathne W, Feldman R, Florento E, Stafford P, Swensen J, et al. Novel therapeutic targets in salivary duct carcinoma uncovered by comprehensive molecular profiling. Cancer Med (2019) 8(17):7322–9. doi: 10.1002/cam4.2602
194. Linxweiler M, Kuo F, Katabi N, Lee M, Nadeem Z, Dalin MG, et al. The immune microenvironment and neoantigen landscape of aggressive salivary gland carcinomas differ by subtype. Clin Cancer Res (2020) 26(12):2859–70. doi: 10.1158/1078-0432.CCR-19-3758
195. Mukaigawa T, Hayashi R, Hashimoto K, Ugumori T, Hato N, Fujii S. Programmed death ligand-1 expression is associated with poor disease free survival in salivary gland carcinomas. J Surg Oncol (2016) 114 (1):36–43. doi: 10.1002/jso.24266
196. Nakano T, Takizawa K, Uezato A, Taguchi K, Toh S, Masuda M. Prognostic value of programed death ligand-1 and ligand-2 co-expression in salivary gland carcinomas. Oral Oncol (2019) 90:30–7. doi: 10.1016/j.oraloncology.2019.01.015
197. Cohen RB, Delord J-P, Doi T, Piha-Paul SA, Liu SV, Gilbert J, et al. Pembrolizumab for the treatment of advanced salivary gland carcinoma: Findings of the phase 1b KEYNOTE-028 study. Am J Clin Oncol (2018) 41(11):1083–8. doi: 10.1097/COC.0000000000000429
198. Fayette J, Even C, Digue L, Geoffrois L, Rolland F, Cupissol D, et al. NISCAHN: A phase II, multicenter nonrandomized trial aiming at evaluating nivolumab (N) in two cohorts of patients (pts) with recurrent/metastatic (R/M) salivary gland carcinoma of the head and neck (SGCHN), on behalf of the unicancer head & neck group. JCO (2022) 37(15_suppl):6083–3. doi: 10.3390/cancers14061383
199. Rodriguez CP, Wu QV, Voutsinas J, Fromm JR, Jiang X, Pillarisetty VG, et al. A phase II trial of pembrolizumab and vorinostat in recurrent metastatic head and neck squamous cell carcinomas and salivary gland cancer. Clin Cancer Res (2020) 26 (4):837–45. doi: 10.1158/1078-0432.CCR-19-2214
200. Burman B, Sherman EJ, Dunn L, Fetten JV, Michel LS, Morris LGT, et al. A phase II trial cohort of nivolumab plus ipilimumab in patients (Pts) with recurrent/metastatic salivary gland cancers (R/M SGCs). JCO (2021) 39(15_suppl):6002–2. doi: 10.1200/JCO.2021.39.15_suppl.6002
201. Ferrarotto R, Bell D, Feng L, Li K, Mott F, Blumenschein GR, et al. A phase II clinical trial of axitinib and avelumab in patients with Recurrent/Metastatic adenoid cystic carcinoma. J Clin Oncol (2022) 40(16_suppl):6019. doi: 10.1200/JCO.2022.40.16_suppl.6019
202. Marabelle A, Fakih M, Lopez J, Shah M, Shapira-Frommer R, Nakagawa K, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol (2020) 21(10):1353–65. doi: 10.1016/S1470-2045(20)30445-9
203. Dou S, Li R, He N, Zhang M, Jiang W, Ye L, et al. The immune landscape of Chinese head and neck adenoid cystic carcinoma and clinical implication. Front Immunol (2021) 12:618367. doi: 10.3389/fimmu.2021.618367
204. Kim HJ, Kim JS. Ultrasound-guided core needle biopsy in salivary glands: A meta- analysis. Laryngoscope (2018) 128(1):118–25. doi: 10.1002/lary.26764
205. Schmidt RL, Hall BJ, Layfield LJ. A systematic review and meta-analysis of the diagnostic accuracy of ultrasound-guided core needle biopsy for salivary gland lesions. Am J Clin Pathol (2011) 136 (4):516–26. doi: 10.1309/AJCP5LTQ4RVOQAIT
206. Schmidt RL, Hall BJ, Wilson AR, Layfield LJ. A systematic review and meta-analysis of the diagnostic accuracy of fine-needle aspiration cytology for parotid gland lesions. Am J Clin Pathol (2011) 136 (1):45–59. doi: 10.1309/AJCPOIE0CZNAT6SQ
207. Orlandi E, Alfieri S, Simon C, Trama A, Licitra L. RARECAREnet working group. treatment challenges in and outside a network setting: Head and neck cancers. Eur J Surg Oncol (2019) 45(1):40–5. doi: 10.1016/j.ejso.2018.02.007
Keywords: salivary gland (SG) tumors, geriatric oncology, salivary gland surgery, radiation therapy (radiotherapy), particle therapy, precision oncology, multidisciplinary team (MDT)
Citation: Colombo E, Van Lierde C, Zlate A, Jensen A, Gatta G, Didonè F, Licitra LF, Grégoire V, Vander Poorten V and Locati LD (2022) Salivary gland cancers in elderly patients: challenges and therapeutic strategies. Front. Oncol. 12:1032471. doi: 10.3389/fonc.2022.1032471
Received: 30 August 2022; Accepted: 31 October 2022;
Published: 25 November 2022.
Edited by:
Jan Baptist Vermorken, University of Antwerp, BelgiumReviewed by:
Hitesh Singhavi, Fortis Hospital, IndiaCopyright © 2022 Colombo, Van Lierde, Zlate, Jensen, Gatta, Didonè, Licitra, Grégoire, Vander Poorten and Locati. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Colombo, ZWxlbmEuY29sb21ib0Bpc3RpdHV0b3R1bW9yaS5taS5pdA==
†These authors share first authorship
‡These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.