 Huohuan Tian1
Huohuan Tian1 Yu Wu
Yu Wu Dan Liu
Dan Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 13 January 2023
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1032225
This article is part of the Research Topic Case Reports in Thoracic Oncology: 2022 View all 42 articles
Background: The occurrence of acute promyelocytic leukemia (APL) during the management of lung cancer is rare and life-threatening. It was mainly reported to be secondary to chemoradiotherapy. A few studies reported an increased incidence of therapy-related acute promyelocytic leukemia (t-APL) after gefitinib became available.
Case presentation: We reported a patient who developed thrombocytopenia after receiving oral osimertinib in combination with intensity-modulated radiotherapy (IMRT). For half a year, she had an unrecoverable low platelet count, which progressed to concomitant leukopenia and the transient appearance of orthochromatic normoblasts in the peripheral blood test, indicating a dormant myeloid disorder. Due to simultaneous resistance to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKI), pembrolizumab and granulocyte colony-stimulating factor (G-CSF) were administered, revealing prominent signs of hematological malignancy in a peripheral blood test that was later identified as t-APL.
Conclusion: In general, patients undergoing EGFR-TKI combined with local radiotherapy should be concerned about their hematological assessment. If patients exhibit unrecoverable abnormalities in routine blood tests, a secondary nonsolid malignancy other than myelosuppression should be considered, and further lung cancer treatment should be discontinued.
Therapy-related acute myeloid leukemia (t-AML) secondary to the administration of chemotherapy and radiotherapy has been considered an exceptional and serious complication with an antecedent malignancy (1). As a fatal subtype of AML, acute promyelocytic leukemia (APL) is commonly characterized by a balanced chromosomal translocation between chromosomes 15 and 17 t-(15;17) (q24; q21), which leads to promyelocytic leukemia (PML)-retinoic acid receptor-α (RARα) rearrangement (2). Comparatively, t-APL may be favored to harbor additional cytogenetic abnormalities, commonly occurring in chromosomes 5, 7, and 17 (3, 4).
According to a systematic review, therapy-related APL following breast cancer is frequent in clinical practice (5). There are scattered reports of APL secondary to lung cancer and corresponding treatment.
Chemotherapy, radiotherapy, or both for prior neoplasms are demonstrated contributors to the development of t-APL (4, 6, 7). Current therapeutic strategies for lung cancer have flourished due to the emergence of targeted agents, immunotherapy, and the transition from conventional radiotherapy to intensity-modulated radiotherapy (IMRT). However, there is scarce evidence regarding APL in these novel therapies (8, 9).
Herein, we report a case of t-APL with advanced non-small cell lung cancer (NSCLC) after targeted therapy and IMRT followed by granulocyte colony-stimulating factor (G-CSF) and immune checkpoint inhibitor (ICI) treatment. Since t-APL shows a similar remission rate to de novo APL (80%) but a high risk of life-threatening coagulopathy (5, 10), we delineated the details so that clinicians may timely notice and treat the complication during the management of lung cancer.
A 58-year-old woman was diagnosed with lung adenocarcinoma with an EGFR-L858R mutation and thoracic vertebral (T5 and T11) invasion in January 2021. Osimertinib was started in February 2021 at a dose of 80 mg/day. The patient received IMRT at the T5 (3,000 cGy 10 times, 2,100 cGy 7 times) and T11 (3,000 cGy 10 times, 2,100 cGy 7 times) from 3 to 17 June 2021 and 24 June to 5 July 2021, respectively. In June 2021, the patient complained of subtle ostealgia, and her laboratory tests revealed mild thrombocytopenia. While continuing osimertinib, the patient was followed up every 2 months until she achieved partial remission (PR). During that time, her platelet count was consistently 50–90 × 109/L (Table 1), with no signs of hemorrhage.
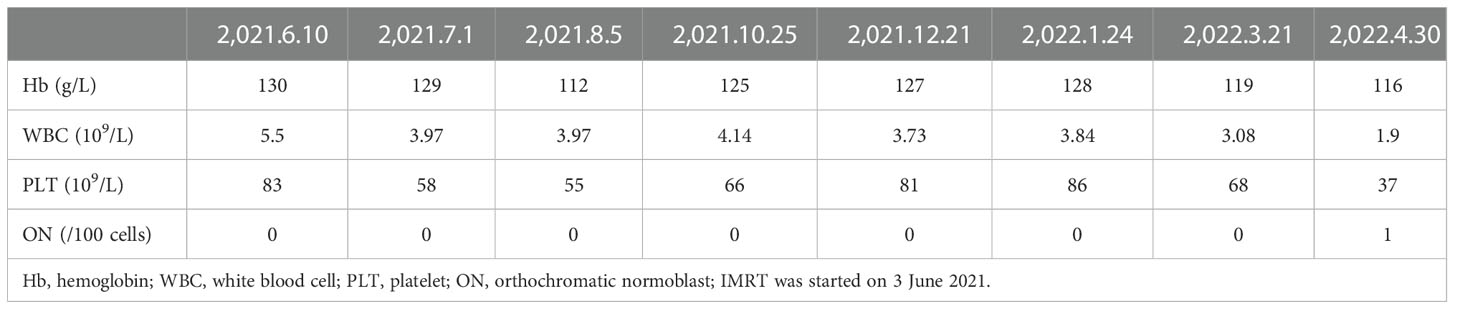
Table 1 Peripheral blood tests during osimertinib and adjuvant IMRT.
In March 2022, the patient reported a mildly aggravated ostealgia. A computed tomography (CT) scan in March 2022 revealed metastasis in the left humerus and sternum. Considering EGFR-TKI resistance, the clinician performed a tissue rebiopsy after withdrawing osimertinib. Peripheral blood test upon admission displayed thrombocytopenia, leukopenia, and orthochromatic normoblast appearance (Table 1), and coagulation parameters are shown in Supplementary Table S1. The pathological result of the rebiopsy is shown in Supplementary Table S2. Because spontaneous thrombocytopenia remission was predicted on 7 June 2022 (Table 2), immunotherapy combined with platinum-based chemotherapy was recommended. On the day when pembrolizumab at 200 mg/dl was administered, the patient experienced severe ostealgia all night. After receiving G-CSF and interleukin (IL)-11, myeloblasts containing Auer’s body appeared in her peripheral blood. Considering the possibility of APL, we monitored her coagulation parameters (Supplementary Table S1). A bone marrow aspiration was performed after stopping G-CSF and IL-11 treatment for 3 days. The bone marrow cytology revealed 68% promyelocytes, indicating t-APL (Supplementary Figure S1). Marrow flow cytometry (FCM) confirmed the finding (Figure 1). The identification of a rare PML/RARα (Bcr 3) fusion gene suggested acute myeloid rearrangement. There was no mutation in any common AML prognostic gene, including FLT3, dupMLL, IDH1, IDH2, NPM1, KIT, NRAS, CEBPA, DNMT3A, PHF6, TET2, ASXL1, RUNX1, TP53, and WT1. Chromosome karyotypic analysis showed 46, XX, add (7, 11), t (15;17) (q24; q21) [6]/46, XX [14] (Figure 2). Subsequently, the patient underwent all-trans retinoic acid and arsenic acid induction therapy. During the induction therapy, fever, hypotension, and pleural effusion occurred. Dexamethasone and vasopressor agents were also administered. She was successfully cured eventually. In September 2022, she received chemotherapy for lung cancer after documenting the complete remission of APL. She is now being followed up by telephone every month.
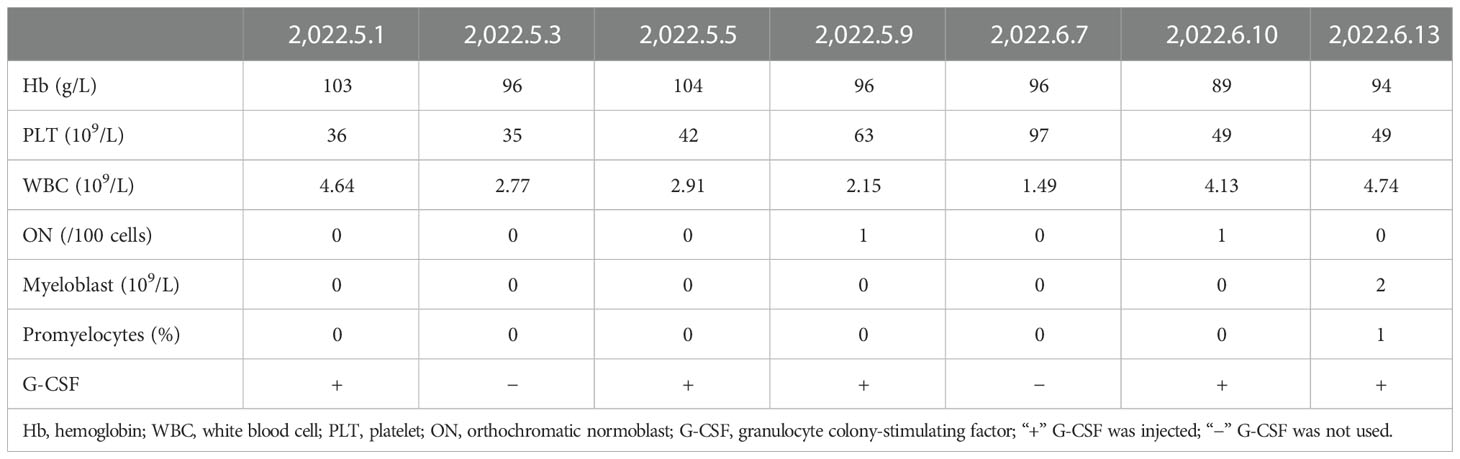
Table 2 Peripheral blood tests during usage of G-CSF and pembrolizumab.
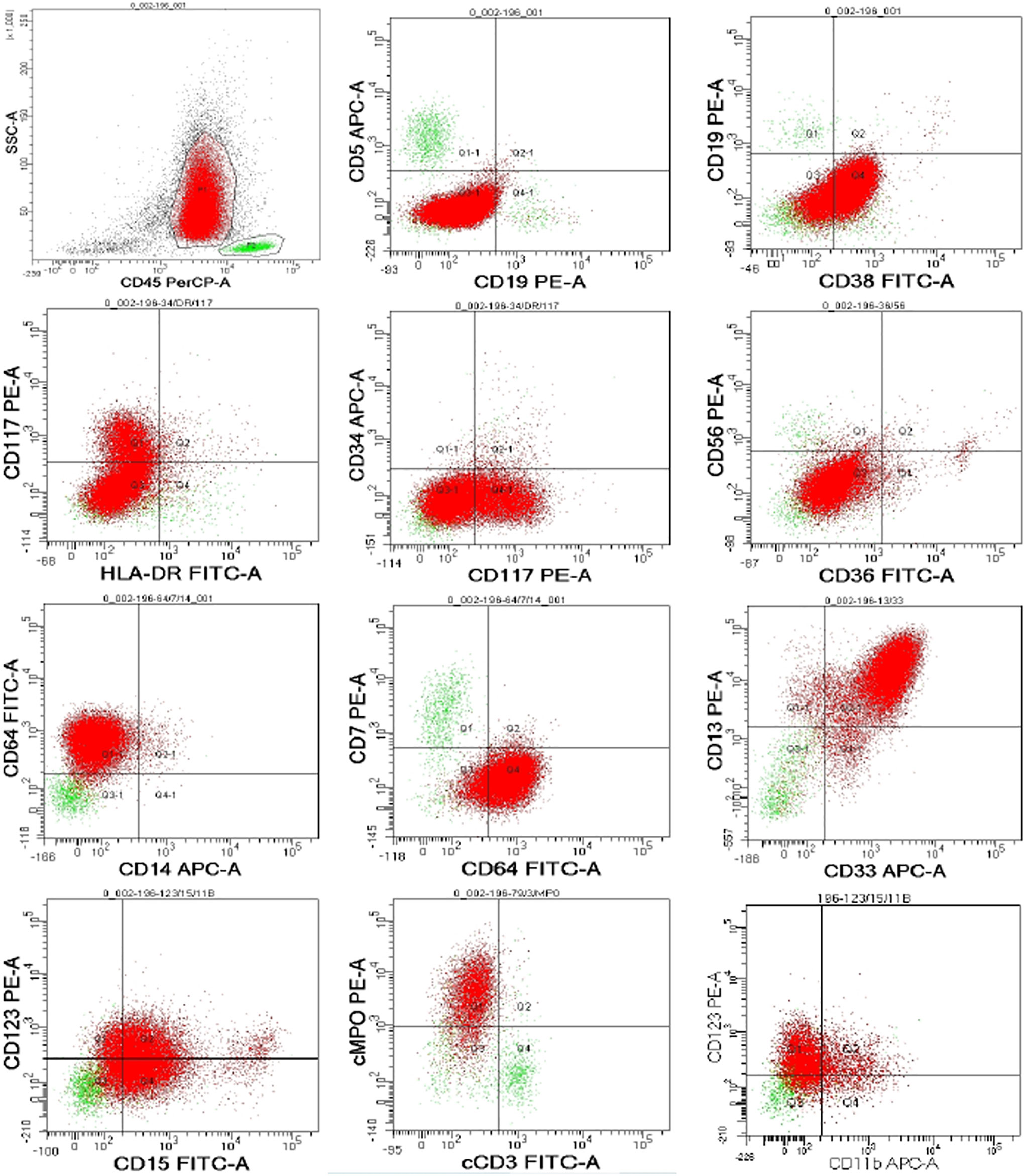
Figure 1 Bone marrow flow cytometry.

Figure 2 Marrow chromosomal analysis.
The patient had no history of any hematological disease that could lead to acute leukemia, such as lymphoma, myelodysplastic syndromes (MDS), multiple myeloma, and so on. She denied any hematological disease history in her family members.
EGFR-TKI ± radiotherapy is the first-line treatment for advanced NSCLC patients with EGFR mutation and oligometastasis (12). Studies demonstrated that radiation was the inciting factor for myeloid neoplasms, including all AML categories and MDS (5, 7, 13). Lung cancer treated with radiation showed an increased relative risk of AML/MDS over the next 1–12 years (14). Ionizing radiation may prompt reactive oxygen species, causing DNA double-strand breaks (15). However, the radiotherapy modality research involved mainly encompassed external beam therapy (EBRT) and brachytherapy. The use of IMRT increased in the past few years because of its superior safety and fewer side effects. Modulated radiation beams and sculpted radiation doses ensure precise coherence with geometric targets and enhanced therapeutic effects (16). A study revealed that secondary MDS/AML could be provoked by IMRT in prostate cancer patients (17). Hematological toxicity, such as thrombocytopenia, was also observed in malignant pleural mesothelioma patients treated with IMRT (18). However, it has not been reported as a factor for hematological malignancy or toxicity in lung cancer patients.
Patients with radiation-induced secondary malignancies tend to experience a long latency period (19, 20). Paradoxically, the intervals between initial radiotherapy and our patient’s thrombocytopenia and t-APL diagnosis were 7 days and 12 months, respectively. In 2006, Keitaro et al. observed a clustered incidence of acute promyelocytic leukemia in NSCLC cases treated with first-generation EGFR-TKI gefitinib (8, 21). Notably, all the observed cases reported cytopenia, especially thrombocytopenia in the beginning. The authors suggested that the t-APL inducibility of gefitinib should be further elucidated. In 2016, clinicians from Japan found a chronic myelomonocytic leukemia blast crisis when synchronous lung adenocarcinoma was treated by EGFR-TKI (22). Another study in 2021 reported a case of thrombocytopenia with immature cells in the peripheral blood during receiving erlotinib, which turned out to be t-AML (11). To date, no report has identified hematological malignancies while the patient was receiving osimertinib treatment. We identified transient orthochromatic normoblasts in our patient’s peripheral blood on 30 April 2022, during osimertinib treatment in our case. Furthermore, subsequent G-CSF and IL-11 after TKI cessation did not ameliorate her thrombocytopenia and emerging leukopenia from 30 April 2022 to 9 May 2022 (Table 2), signifying a hematopoiesis disorder such as MDS and acute myeloid leukemia. Hence, we speculated that continuous usage of third-generation EGFR-TKI osimertinib may hasten the secondary APL. Regrettably, bone marrow aspiration was not performed when cytopenia occurred during continuous EGFR-TKI and regional radiotherapy treatment.
T-APL was not confirmed until the administration of a second-line therapy comprising pembrolizumab and chemotherapy. G-CSF is a hematopoietic glycoprotein produced by monocytes, macrophages, fibroblasts, and endothelial cells (23). It is used to accelerate neutrophil recovery after chemotherapy by regulating cell cycle activation, proliferation, and terminal maturation (23). Researchers revealed that congenital neutropenia patients on G-CSF are more susceptible to developing MDS/AML over time (24). Granulocyte colony-stimulating factor has also been shown to be a risk factor for AML/MDS in breast and lung cancer populations (25). Promyelocytes containing Auer’s body indeed emerged in our patient’s peripheral blood after G-CSF usage. Nevertheless, progressive thrombocytopenia, leukopenia, and orthochromatic normoblast were virtually presented in her peripheral blood before G-CSF usage, when she was still undergoing osimertinib treatment. Considering that t-APL typically occurs without the prodromal, preleukemic, and myelodysplastic phases (5), we speculated a likelihood of t-APL existence prior to the use of G-CSF.
Immunotherapy plays a critical role in NSCLC. PD-1-binding pembrolizumab disrupted its anchoring to PD-L1, impeding the inhibition of T cells and mounting its recognition to tumor cells (26). There is only one case report to date about t-APL involving the history of pembrolizumab treatment (9). According to our observation, the intravenous infusion of pembrolizumab aggravated the patient’s chronic ostealgia acutely. The association between pembrolizumab and t-APL remained occult. Of interest, the refractory leukopenia was alleviated but the thrombocytopenia was exacerbated following pembrolizumab and G-CSF (Table 2). This phenomenon resembled Paola’s study, which found that G-CSF injection worsened anemia in breast cancer patients receiving chemotherapy (27), and it is hypothesized that granulopoietic lineages competed with erythropoietic lineages for differentiating hematopoietic cell stems.
Altogether, our patient had been exposed to a series of predisposing factors to t-APL, making it difficult to ascertain that the third-generation EGFR-TKI osimertinib was the sole and determining cause of the complication. However, it is reasonable to conclude that the myeloid disease developed during IMRT plus continuous osimertinib. Further evaluation based on a larger sample size is warranted. Regardless, a widespread matter of osimertinib resistance gives rise to novel therapy exploration (28). KEYNOTE-789 is an ongoing trial assessing platinum-based chemotherapy combined with pembrolizumab for this entity. EGFR-TKI, radiation, G-CSF, and chemotherapy agents are all widely used, increasing the risk of a secondary hematological disease and even malignancy. Given the positive response of t-APL to all-trans retinoic acid therapy, a key problem now is determining whether we can identify those nearly asymptomatic patients early and withhold APL-facilitating interventions. Thus, after the patients achieved hematological remission, should the treatment strategy for lung cancer be persisted?
We first reported the identification of t-APL when the patient acquired resistance to osimertinib. Chemotherapy, radiotherapy, or both have been demonstrated to be risk factors for t-APL. Previous reports and our case supported positive concern for such complications, given the widespread usage of EGFR TKI and resistance to targeted therapy
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Sichuan University Ethics Review Board. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
HT, LY, and WH: writing—original draft. YW, YD, and JY: writing original draft preparation. DL: administrative support and supervision. All the authors contributed to the article and approved the submitted version.
This work was supported by National Natural Science Foundation of China (Grant Number 82173182).
The authors thank the patient and her family for their persistence in comprehensive treatment and granting permission to present her medical history here. We also thank all our colleagues for the management of such an infrequent patient.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.1032225/full#supplementary-material
1. Leone G, Fianchi L, Pagano L, Voso MT. Incidence and susceptibility to therapy-related myeloid neoplasms. Chemico-biological Interact (2010) 184(1-2):39–45. doi: 10.1016/j.cbi.2009.12.013
2. Jimenez JJ, Chale RS, Abad AC, Schally AV. Acute promyelocytic leukemia (APL): a review of the literature. Oncotarget (2020) 11(11):992–1003. doi: 10.18632/oncotarget.27513
3. Yin CC, Glassman AB, Lin P, Valbuena JR, Jones D, Luthra R, et al. Morphologic, cytogenetic, and molecular abnormalities in therapy-related acute promyelocytic leukemia. Am J Clin Pathol (2005) 123(6):840–8. doi: 10.1309/tjff-k819-rpcl-fkj0
4. Beaumont M, Sanz M, Carli PM, Maloisel F, Thomas X, Detourmignies L, et al. Therapy-related acute promyelocytic leukemia. J Clin Oncol Off J Am Soc Clin Oncol (2003) 21(11):2123–37. doi: 10.1200/jco.2003.09.072
5. Rashidi A, Fisher SI. Therapy-related acute promyelocytic leukemia: a systematic review. Med Oncol (2013) 30(3):625. doi: 10.1007/s12032-013-0625-5
6. Wang H, Yin Y, Wang R, Huang J, Xue H, Cheng Y, et al. Clinicopathological features, risk and survival in lung cancer survivors with therapy-related acute myeloid leukaemia. BMC Cancer. (2020) 20(1):1081. doi: 10.1186/s12885-020-07603-9
7. Le Deley MC, Suzan F, Cutuli B, Delaloge S, Shamsaldin A, Linassier C, et al. Anthracyclines, mitoxantrone, radiotherapy, and granulocyte colony-stimulating factor: risk factors for leukemia and myelodysplastic syndrome after breast cancer. J Clin Oncol Off J Am Soc Clin Oncol (2007) 25(3):292–300. doi: 10.1200/JCO.2006.05.9048
8. Matsuo K, Kiura K, Tabata M, Uchida A, Hotta K, Niiya D, et al. Clustered incidence of acute promyelocytic leukemia during gefitinib treatment for non-small-cell lung cancer: experience at a single institution. Am J Hematol (2006) 81(5):349–54. doi: 10.1002/ajh.20569
9. Suzuki R, Kawai H, Furuya D, Akashi H, Ogawa Y, Kawada H, et al. Successful treatment of therapy-related acute promyelocytic leukemia:with all-trans-retinoic acid following. Tokai J Exp Clin Med (2020) 45(2):92–6.
10. Tallman MS. The thrombophilic state in acute promyelocytic leukemia. Semin Thromb hemostasis. (1999) 25(2):209–15. doi: 10.1055/s-2007-994922
11. Koo SM, Kim KU, Kim YK, Uh ST. Therapy-related myeloid leukemia during erlotinib treatment in a non-small cell lung cancer patient: A case report. World J Clin Cases. (2021) 9(24):7205–11. doi: 10.12998/wjcc.v9.i24.7205
12. Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman JR, Bharat A, et al. Non-small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2022) 20(5):497–530. doi: 10.6004/jnccn.2022.0025
13. Teepen JC, Curtis RE, Dores GM, Berrington de Gonzalez A, van den Heuvel-Eibrink MM, Kremer LCM, et al. Risk of subsequent myeloid neoplasms after radiotherapy treatment for a solid cancer among adults in the united states, 2000-2014. Leukemia (2018) 32(12):2580–9. doi: 10.1038/s41375-018-0149-2
14. Radivoyevitch T, Sachs RK, Gale RP, Molenaar RJ, Brenner DJ, Hill BT, et al. Defining AML and MDS second cancer risk dynamics after diagnoses of first cancers treated or not with radiation. Leukemia (2016) 30(2):285–94. doi: 10.1038/leu.2015.258
15. Sill H, Olipitz W, Zebisch A, Schulz E, Wölfler A. Therapy-related myeloid neoplasms: pathobiology and clinical characteristics. Br J Pharmacol (2011) 162(4):792–805. doi: 10.1111/j.1476-5381.2010.01100.x
16. Chun SG, Hu C, Choy H, Komaki RU, Timmerman RD, Schild SE, et al. Impact of intensity-modulated radiation therapy technique for locally advanced non-Small-Cell lung cancer: A secondary analysis of the NRG oncology RTOG 0617 randomized clinical trial. J Clin Oncol Off J Am Soc Clin Oncol (2017) 35(1):56–62. doi: 10.1200/JCO.2016.69.1378
17. Wang R, Zeidan AM, Yu JB, Soulos PR, Davidoff AJ, Gore SD, et al. Myelodysplastic syndromes and acute myeloid leukemia after radiotherapy for prostate cancer: A population-based study. Prostate (2017) 77(5):437–45. doi: 10.1002/pros.23281
18. Matsuo Y, Shibuya K, Okubo K, Ueki N, Aoyama A, Sonobe M, et al. Long-term outcomes of intensity-modulated radiotherapy following extra-pleural pneumonectomy for malignant pleural mesothelioma. Acta Oncologica (2017) 56(7):957–62. doi: 10.1080/0284186x.2017.1279749
19. Hall EJ, Wuu C-S. Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat OncologyBiologyPhysics. (2003) 56(1):83–8. doi: 10.1016/s0360-3016(03)00073-7
20. Amadori S, Papa G, Anselmo AP, Fidani P, Mandelli F, Biagini C. Acute promyelocytic leukemia following ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) and radiotherapy for hodgkin's disease. Cancer Treat Rep (1983) 67(6):603–4.
21. Uchida A, Matsuo K, Tanimoto M. APL during gefitinib treatment for non-small-cell lung cancer. N Engl J Med (2005) 352(8):843. doi: 10.1056/NEJM200502243520825
22. Ogata H, Okamoto I, Yoshimoto G, Obara T, Ijichi K, Iwama E, et al. Chronic myelomonocytic leukemia blast crisis in a patient with advanced non-small cell lung cancer treated with EGFR tyrosine kinase inhibitors. Respir Investig (2017) 55(2):181–3. doi: 10.1016/j.resinv.2016.12.002
23. D'Souza A, Jaiyesimi I, Trainor L, Venuturumili P. Granulocyte colony-stimulating factor administration: adverse events. Transfus Med Rev (2008) 22(4):280–90. doi: 10.1016/j.tmrv.2008.05.005
24. Rosenberg PS, Alter BP, Bolyard AA, Bonilla MA, Boxer LA, Cham B, et al. The incidence of leukemia and mortality from sepsis in patients with severe congenital neutropenia receiving long-term G-CSF therapy. Blood. (2006) 107(12):4628–35. doi: 10.1182/blood-2005-11-4370
25. Danese MD, Schenfeld J, Shaw J, Gawade P, Balasubramanian A, Kelsh M, et al. Association between granulocyte colony-stimulating factor (G-CSF) use and myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) among elderly patients with breast, lung, or prostate cancer. Adv Ther (2022) 39(6):2778–95. doi: 10.1007/s12325-022-02141-1
26. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med (2015) 372(21):2018–28. doi: 10.1056/NEJMoa1501824
27. Papaldo P, Ferretti G, Di Cosimo S, Giannarelli D, Marolla P, Lopez M, et al. Does granulocyte colony-stimulating factor worsen anemia in early breast cancer patients treated with epirubicin and cyclophosphamide? J Clin Oncol Off J Am Soc Clin Oncol (2006) 24(19):3048–55. doi: 10.1200/jco.2005.02.9488
Keywords: therapy-related acute promyelocytic leukemia, osimertinib, granulocyte colony-stimulating factor, pembrolizumab, lung cancer
Citation: Tian H, Yang L, Hou W, Wu Y, Dai Y, Yu J and Liu D (2023) Case report: Identification of acute promyelocytic leukemia during osimertinib resistance followed by granulocyte colony-stimulating factor and pembrolizumab. Front. Oncol. 12:1032225. doi: 10.3389/fonc.2022.1032225
Received: 30 August 2022; Accepted: 21 December 2022;
Published: 13 January 2023.
Edited by:
Kohei Fujita, National Hospital Organization Kyoto Medical Center, JapanReviewed by:
Dan Ma, Affiliated Hospital of Guizhou Medical University, ChinaCopyright © 2023 Tian, Yang, Hou, Wu, Dai, Yu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dan Liu, bGl1ZGFuMTA5NjVAd2Noc2N1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.