
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 01 December 2022
Sec. Gynecological Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1030786
 Angeliki Andrikopoulou
Angeliki Andrikopoulou Eleni Zografos
Eleni Zografos Kleoniki Apostolidou
Kleoniki Apostolidou Anastasios Kyriazoglou
Anastasios Kyriazoglou Alksistis-Maria PapatheodoridiMaria KaparelouKonstantinos KoutsoukosMichalis Liontos
Alksistis-Maria PapatheodoridiMaria KaparelouKonstantinos KoutsoukosMichalis Liontos Meletios-Athanasios Dimopoulos
Meletios-Athanasios Dimopoulos Flora Zagouri*
Flora Zagouri*Background: Germline BRCA1/2 mutations are identified in 13-15% of ovarian cancers, while an additional 5-7% of ovarian cancers harbor somatic BRCA1/2 mutations. Beyond these mutations, germline or somatic aberrations in genes of the homologous recombination (HR) pathway such as RAD51B/C/D, PALB2, ATM, BRIP1 may confer an HR deficiency in up to 50% of ovarian tumors. Next-generation sequencing (NGS) is a high-throughput massive parallel sequencing method that enables the simultaneous detection of several mutations in entire genomes.
Methods: We performed NGS analysis in 86 patients with ovarian cancer treated in the Oncology Department of Alexandra University Hospital in order to identify the molecular landscape of germline and somatic mutations in ovarian cancer.
Results: The genes with the highest number of pathogenic somatic mutations in high grade serous carcinoma (HGSC) patients were TP53 [68%; 34/50] and BRCA1 [22%; 11/50] followed by somatic mutations in RB1 [2%; 1/50], NF1 [2%; 1/50], BRCA2 [2%; 1/50], AKT1 [2%; 1/50], RAD50 [2%; 1/50], PIK3CA [2%; 1/50] genes. Of note, the most common TP53 genetic polymorphism was c.524G>A p.Arg175His in exon 5. Variants of unknown significance (VUS) detected in HGSC included ROS1 [26%; 13/50], RAD50 [6%; 3/50], BRCA2 [6%; 3/50], NOTCH1 [6%; 3/50], TP53 [6%; 3/50], AR [6%; 3/50]. As for germline mutations, BRCA1 [8/30; 27%] and BRCA2 [4/30; 13%] were the most common genes bearing pathogenic alterations in HGSC, while VUS germline mutations commonly affected HRR-related genes, including ATM (c.7816A>G), BRIP (c.2327 C>A), CHEK2 (c.320-5T>A).
Conclusion: Overall, genetic testing should be offered in most patients with ovarian cancer to identify mutations in HRR genes and determine the population that would be susceptible to poly ADP ribose polymerase (PARP) inhibitors.
Ovarian cancer is the eighth leading cause of cancer-related mortality in women accounting for over 200 000 deaths in 2020 (1). Although advances have been made during the last years in ovarian cancer diagnosis and treatment, survival rates have changed modestly for decades. Five-year survival is still as low as 39% and 17% for patients with IIIC/IV disease respectively (2). Ovarian cancer remains a significant burden of morbidity and mortality globally with rising incidence in developing countries and increasing rates in high income countries due to population aging. Histologically, ovarian cancer is classified into two main subtypes: epithelial ovarian cancer (EOC) accounting for more than 95% of the cases and other nonepithelial subtypes, mostly germ cell and sex-cord stromal cancers (3). EOC is further subdivided in high-grade serous ovarian carcinoma (HGSC) which is the most common subtype [75%] and low-grade serous carcinoma (LGSC) [10%], endometrioid (EC) [10%], clear cell carcinoma (OCCC) [5%] and mucinous [2.4%] (3). Debulking surgery either upfront or interval after receiving three cycles of platinum-based chemotherapy remains the cornerstone of ovarian cancer treatment. Platinum-based first line chemotherapy consists the standard treatment for ovarian cancer patients following debulking surgery. After 2018 that GOG-0218 (NCT00262847) Phase III trial published its first results, antivascular agent Bevacizumab has been incorporated in the first-line treatment of patients with stage III/IV EOC (4). Currently, PARP inhibitors have been established as maintenance treatment after primary treatment with platinum-based chemotherapy initially in BRCA1/2 – mutated high-grade serous carcinoma stage III/IV and recently in combination with bevacizumab in homologous-recombination deficient (HRD) HGSC tumors (5, 6).
Molecular testing has been established for the treatment optimization of ovarian cancer but also for primary prevention and genetic counseling. As known, 40% - 60% of BRCA1 and 11% - 27% of BRCA2 germline carriers develop ovarian cancer. PARP inhibitors have been approved for the maintenance treatment of patients with BRCA1/2 somatic mutations. Apart from the well-known BRCA1/2 mutations, other mutations in homologous recombination repair (HRR) genes such as RAD51, ATM, ATR, BRIP1, PALB2, RB1, NF1, CDKN2A confer homologous recombination deficiency and increased susceptibility to PARP inhibitors. HGSC is associated with lower prevalence but recurrent somatic mutations in NF1, BRCA1, BRCA2, RB1, and CDK12 in around 5–8% of tumours (3). Myriad HRD test is a next generation sequencing-based (NGS) test that assesses the qualitative detection and classification of single nucleotide variants, insertions and deletions, and large rearrangement variants in protein coding regions and intron/exon boundaries of the BRCA1 and BRCA2 genes and the determination of Genomic Instability Score (GIS) which is an algorithmic measurement of Loss of Heterozygosity (LOH), Telomeric Allelic Imbalance (TAI), and Large-scale State Transitions (LST) on formalin-fixed paraffin embedded (FFPE) tumor tissue specimens. HR deficiency is estimated to affect nearly 50% of HGSC and confer benefit from the treatment with PARP inhibitors Olaparib and Niraparib that are approved for this population (7). Other frequently identified mutations include mutations in the PI3K/Akt signaling pathway in OCCC [40%] and EC [40%], in AT-rich interaction domain 1A (ARID1A) gene in OCCC [40-67%] and EC [30%] while mutations in TP53 are a nearly universal characteristic of HGSC [97%] (3). It becomes apparent that molecular testing is currently necessary to guide treatment options and personalize treatment.
Next-generation sequencing (NGS) is a massively parallel sequencing technology that captures a broad spectrum of mutations in entire genomes or targeted regions of DNA or RNA. This method enables the simultaneous analysis of several genes or gene regions with a single test compared to traditional methods. Next-generation sequencing could detect quickly and accurately mutations in ovarian cancer patients that could serve as druggable targets. We here performed NGS analysis in patients with ovarian cancer treated in the Oncology Department of Alexandra University Hospital. We aim to identify the molecular landscape of pathogenic germline and somatic mutations as well as mutations of uncertain significance (VUS) in ovarian cancer patients as determined by powerful NGS analysis.
86 women with histologically confirmed ovarian carcinoma that underwent NGS in paraffin blocks and blood samples during the period 10/2019 through 12/2021 were considered eligible for our study. All women were treated at the Oncology Department of “Alexandra” Hospital, Medical School, University of Athens, Greece. Our institution has been certified by the European Society of Gynecologic Oncology (ESGO) as a center of excellence for the treatment of ovarian cancer. Clinicopathological characteristics including age at diagnosis, stage of the disease, histological subtype, grade, performance of PDS or IDS, debulking status, performance status (ECOG), maintenance treatment, progression-free survival and overall survival were collected from the medical records of the patients. This study was approved by the Institutional Review Board of the Alexandra General Hospital of Athens and performed in accordance with the ethical standards described in the Declaration of Helsinki. An informed consent form was obtained from each of the eligible patients.
Formalin-fixed paraffin-embedded (FFPE) ovarian cancer tissues derived from hysterectomy/bilateral salpingo - oophorectomy were analyzed. Paraffin-embedded ovarian specimens were cut at slices of 10μm diameter. DNA was extracted from paraffinized tissue using the QIAamp Tissue kit (Qiagen, Germantown, MD, USA)and libraries were constructed using an Ion AmpliSeq Custom Next Generation Sequencing (NGS) DNA panel (Thermo Fisher Scientific, Waltham, MA, USA)., for the 58 targeted genes that are presented in Supplementary Table 1. The genotyping was performed using the Ion Torrent platform (Ion S5) since the automated amplicon-based library is prepared rapidly, enabling a fast turnaround time and a high degree of sample multiplexing, obtaining an average amplicon coverage of 500x for 91.39% of the targeted regions. We evaluated predicted pathogenic mutations, based on combined variant characterization by IonReporter (v5.12) (Thermo Fisher Scientific, Waltham, MA, USA).An additional manual inspection was performed using data from OncomineReporter (v4.4) and relevant databases (ClinVar, dbSNP, Ensemble, COSMIC, CIVIC, PharmGKB, OMIM, My Cancer Genome, VarSome etc).
Plasma blood samples were collected in Vacutainer tubes. Subsequently, genomic DNA was isolated from whole blood using the QIAsymphony DSP DNA Mini Kit (Qiagen, Germantown, MD, USA) and used to prepare indexed libraries using the Trusight Cancer Panel – Nextera DNA Flex Pre-Enrichment Library Prep (Illumina, San Diego, USA). Libraries were sequenced on a MiSeq genetic analyzer (Illumina, Inc., San Diego, CA), according to the manufacturer’s protocols. Annotation was performed against the human reference genome GRCh38 using VariantStudio V.3 (Illumina, Inc., San Diego, CA). Based on the data generated from this software, alterations were identified as pathogenic when classified as disease causing or as variants of unknown significance (VUS) when evidence regarding their pathogenicity was either conflicting or limited. The validation of results was performed according to criteria of American College of Medical Genetics – ACMG (8) and National Comprehensive Cancer Network (NCCN) guidelines.
Continuous variables were summarized with the use of descriptive statistical measures [median and percentiles (25th,75th)] and categorical variables were displayed as frequency tables (N, %). The outcome of the debulking surgery was classified as optimal (residual disease below 1cm) or suboptimal. Overall Survival (OS) was defined as the time between the start of chemotherapy and the date of death from any cause. Progression-free Survival (PFS) was defined as the time between the start of chemotherapy and the date of disease progression. Alive patients were censored at the date of last contact. Kaplan-Meier estimates were used to describe and visualize the effect of categorical variables on OS and PFS. All statistical analyses were performed using the STATA/SE 16.0 software (Copyright 1985-2019 StataCorp LP).
Overall, 86 ovarian cancer patients underwent somatic and/or germline NGS analysis. Among them, there were 66 cases [76.7%] of high-grade serous carcinoma [HGSC], 7 cases [8.1%] of low grade serous carcinoma [LGSC], 7 cases [8.1%] of endometrioid carcinoma [EC], 4 cases [4.7%] of clear cell carcinoma [OCCC] and two cases [2.3%] of mucinous carcinoma.
Mean age at diagnosis was 58.67 (SD; 11) years for HGSC, 54.43 (SD; 11.73) years for LGSC and 51.29 (SD; 8.46) years for EC. Most patients were diagnosed at an advanced stage: IIIB [5; 5.8%], IIIC [36; 41.9%] and IV [20; 23.3%]. Primary debulking surgery was performed in 67 [77.9%] of cases, while 19 [22.1%] could not be upfront debulked and performed an interval debulking surgery. Debulking was optimal in the majority of cases [66; 76.7%] while it was suboptimal in [18; 20.9%]. 76 [88.4%] patients had performance status ECOG 0. Most of the patients received first line maintenance treatment with bevacizumab either alone [27; 31.4%] or in combination with PARP inhibitors [5; 5.8%], immune checkpoint inhibitors [4; 4.7%] or both of them [4; 4.7%].
Median PFS was 22 months for HGSC [95% CI; 18.57 – 25.42]. Figure 1 illustrates median PFS in HGSC patients. For the remaining population, median PFS was 28 months [95% CI;14.52 – 41.47] for LGSC (Figure 3) and 44 months for EC. Median OS was 112 months [95% CI; 72.28 – 151.71] for patients with HGSC (Figure 2).
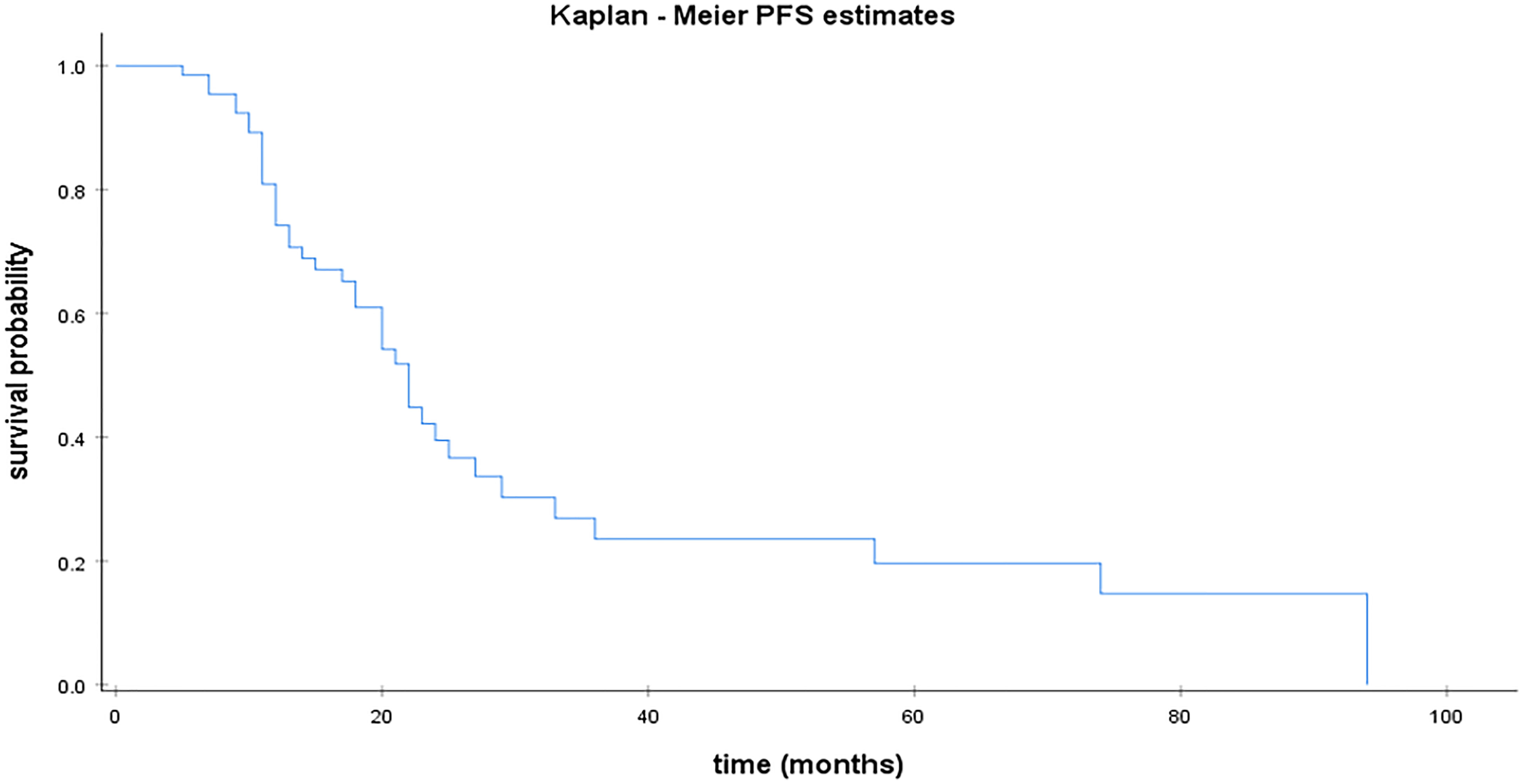
Figure 1 Kaplan Meier curve for PFS in HGSC.
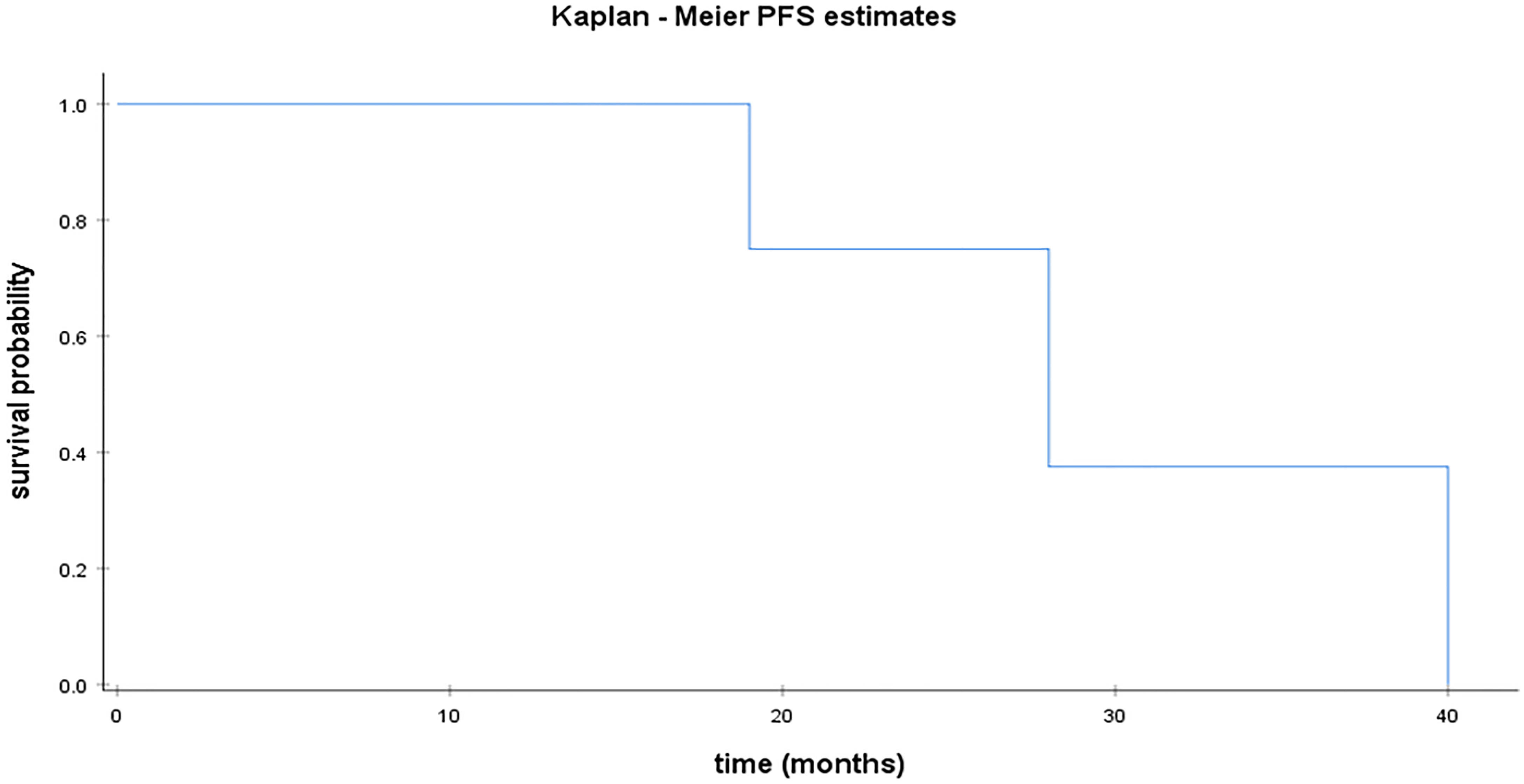
Figure 2 Kaplan Meier curve for OS in HGSC.
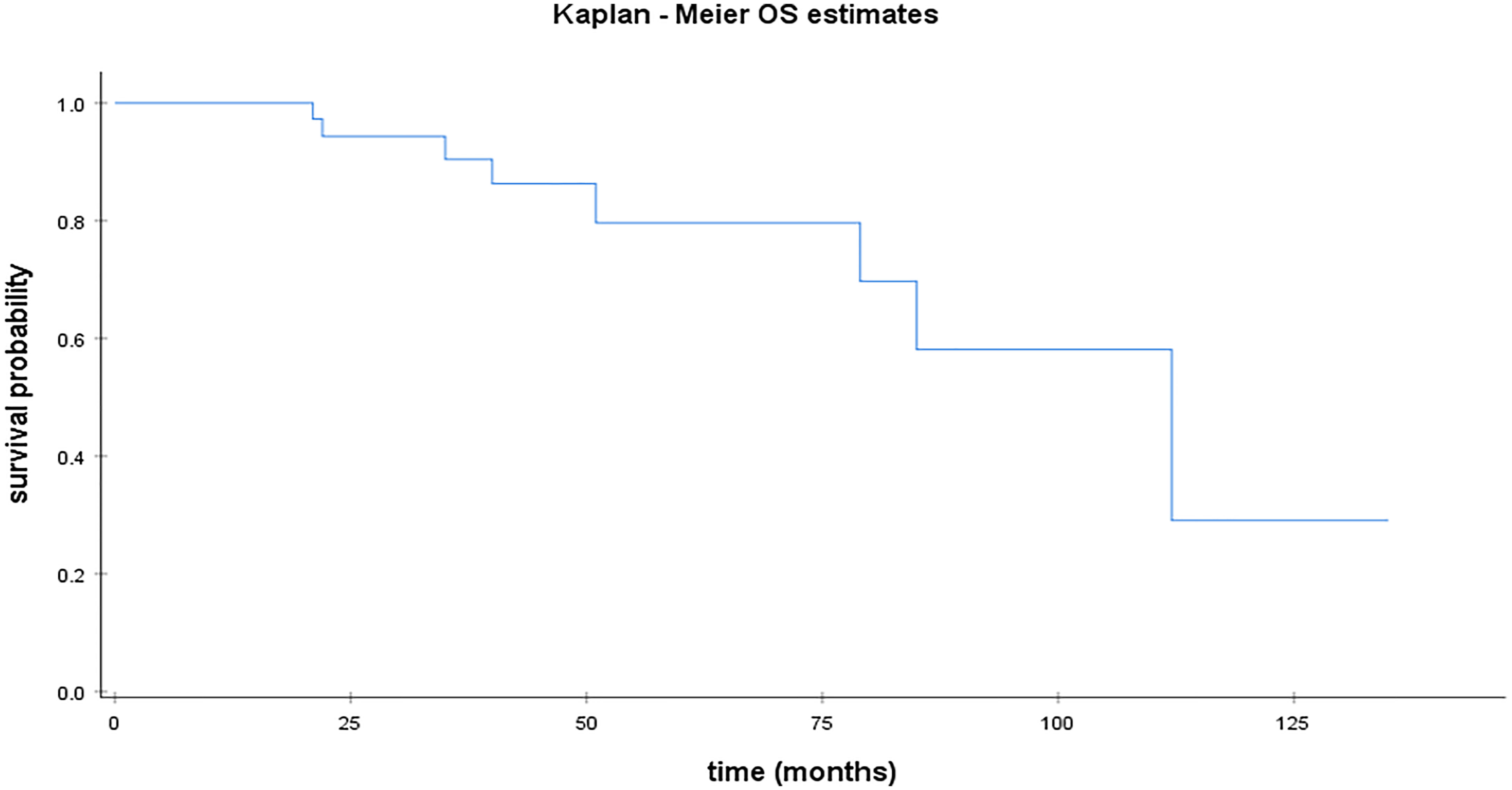
Figure 3 Kaplan Meier curve for PFS in LGSC.
From 66 patients with HGSC, NGS analysis for somatic mutations was performed in 50 patients. All somatic mutations identified are presented in Supplemental Table 3. Overall, TP53 [68%; 34/50] and BRCA1 [22%; 11/50] were the genes with the highest number of pathogenic somatic mutations (Table 1) as expected. Of note, the most common TP53 genetic polymorphism was c.524G>A p.Arg175His in exon 5. Other genes bearing pathogenic somatic mutations were RB1 [2%; 1/50], NF1 [2%; 1/50], BRCA2 [2%; 1/50], AKT1 [2%; 1/50], RAD50 [2%; 1/50], PIK3CA [2%; 1/50]. Additional analysis was performed to explore the prognostic value of BRCA1/2 mutations (Figure 4). There was a trend for longer PFS in patients with BRCA1/2 mutations (27 months [95% CI; 13.89 – 40.10] vs 23 months [95% CI; 14.68 – 31.31]) although this association was not statistically significant (p=0.65).
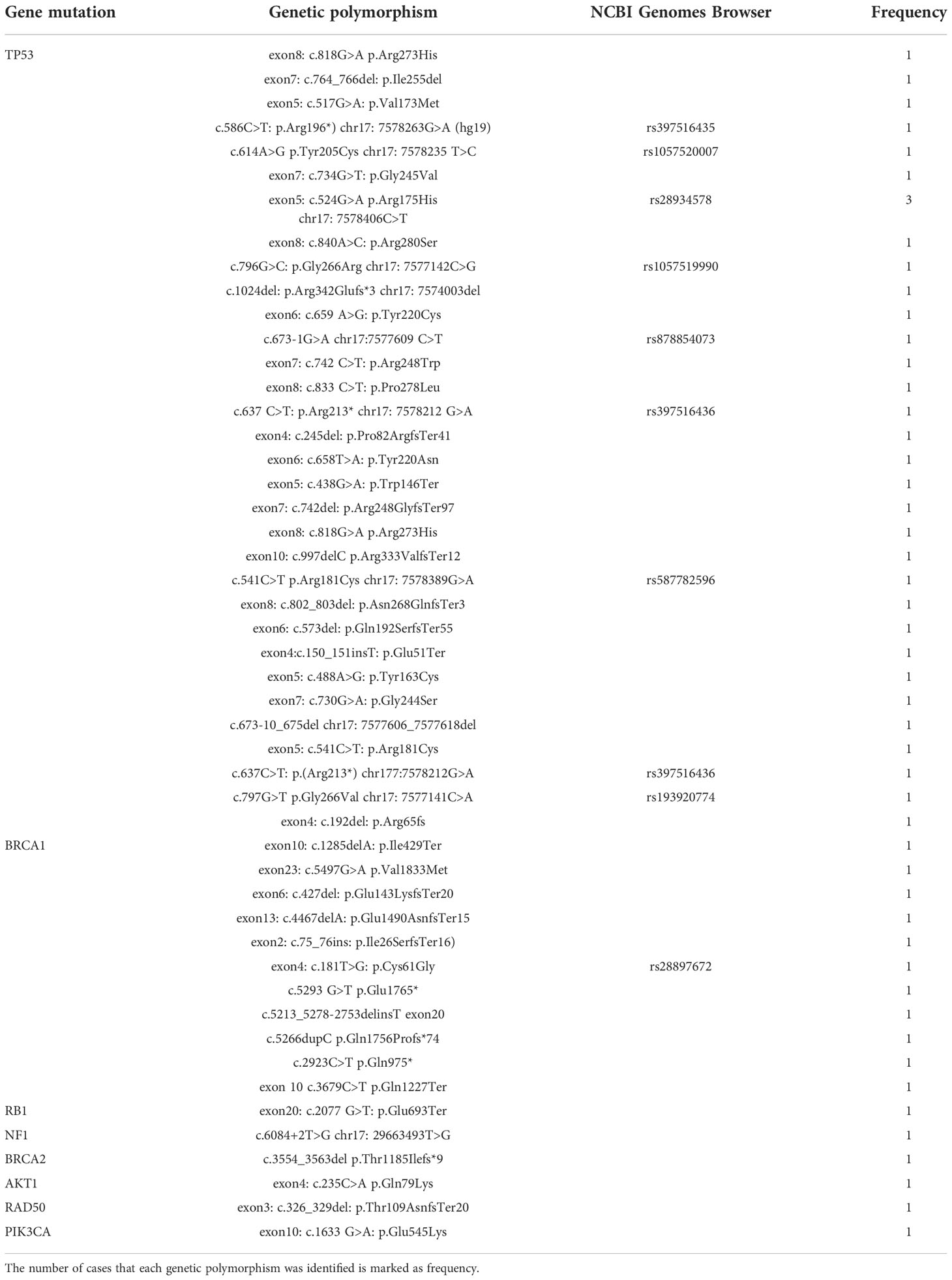
Table 1 Pathogenic somatic mutations identified in patients with HGSC.
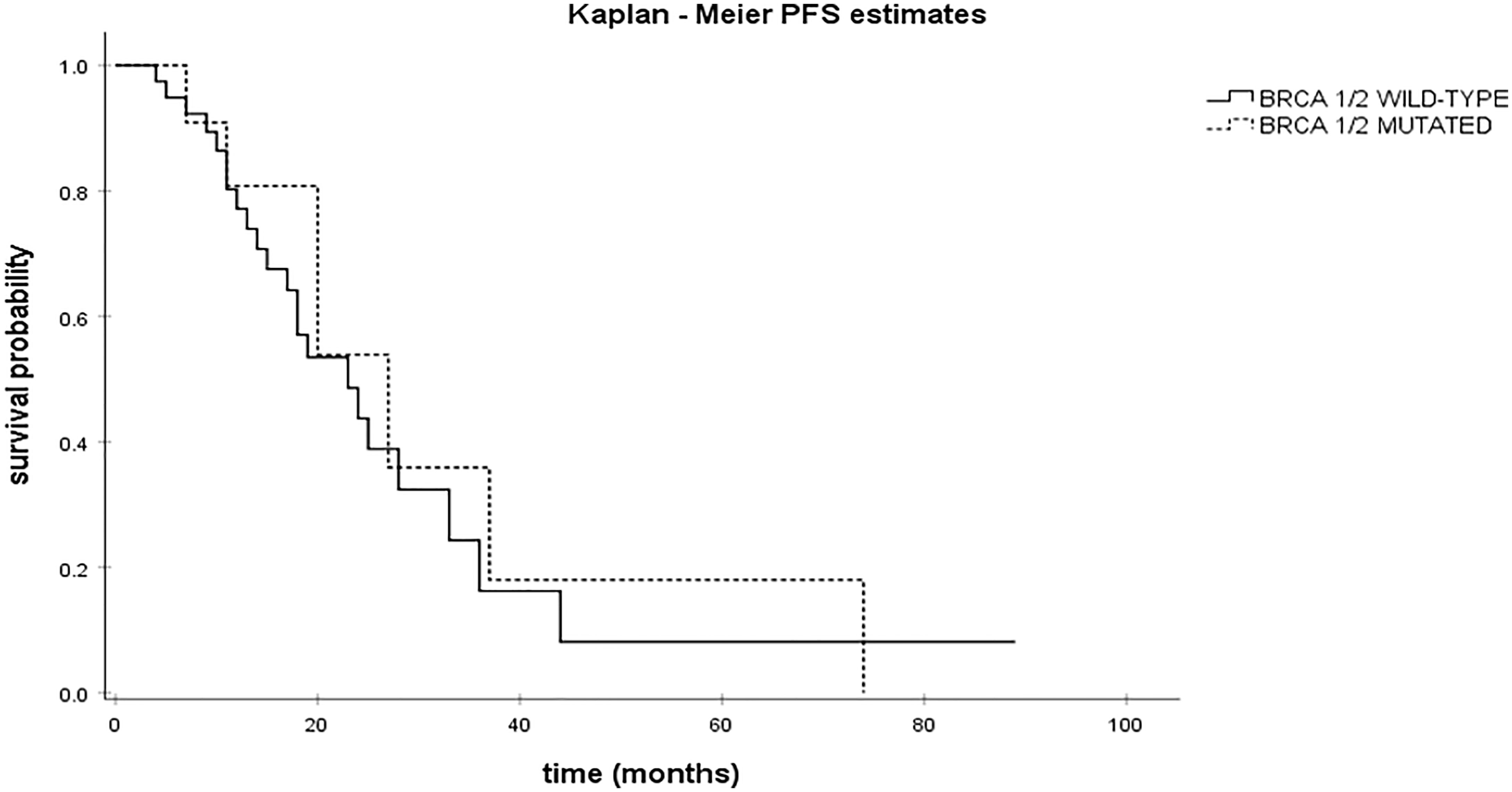
Figure 4 Kaplan Meier curves for PFS in BRCA1/2-mutated vs BRCA1/2 wild-type HGSC.
Variants of unknown significance (VUS) somatic mutations are presented in Table 2. The most common genes with VUS somatic mutations in HGSC were ROS1 [26%; 13/50], RAD50 [6%; 3/50], BRCA2 [6%; 3/50], NOTCH1 [6%; 3/50], TP53 [6%; 3/50], AR [6%; 3/50]. Other genes with VUS mutations identified include CCNE1, MEN1, TP53, PTEN, ATM, FGFR3, MSH2, MYC, IDH1, KMT2C, RAD51, CHEK2, JAK2, KDR, PALB2, BCL2, CHECK1, MSH6, CTNNB1, PDGFRA STK11, BRCA1.
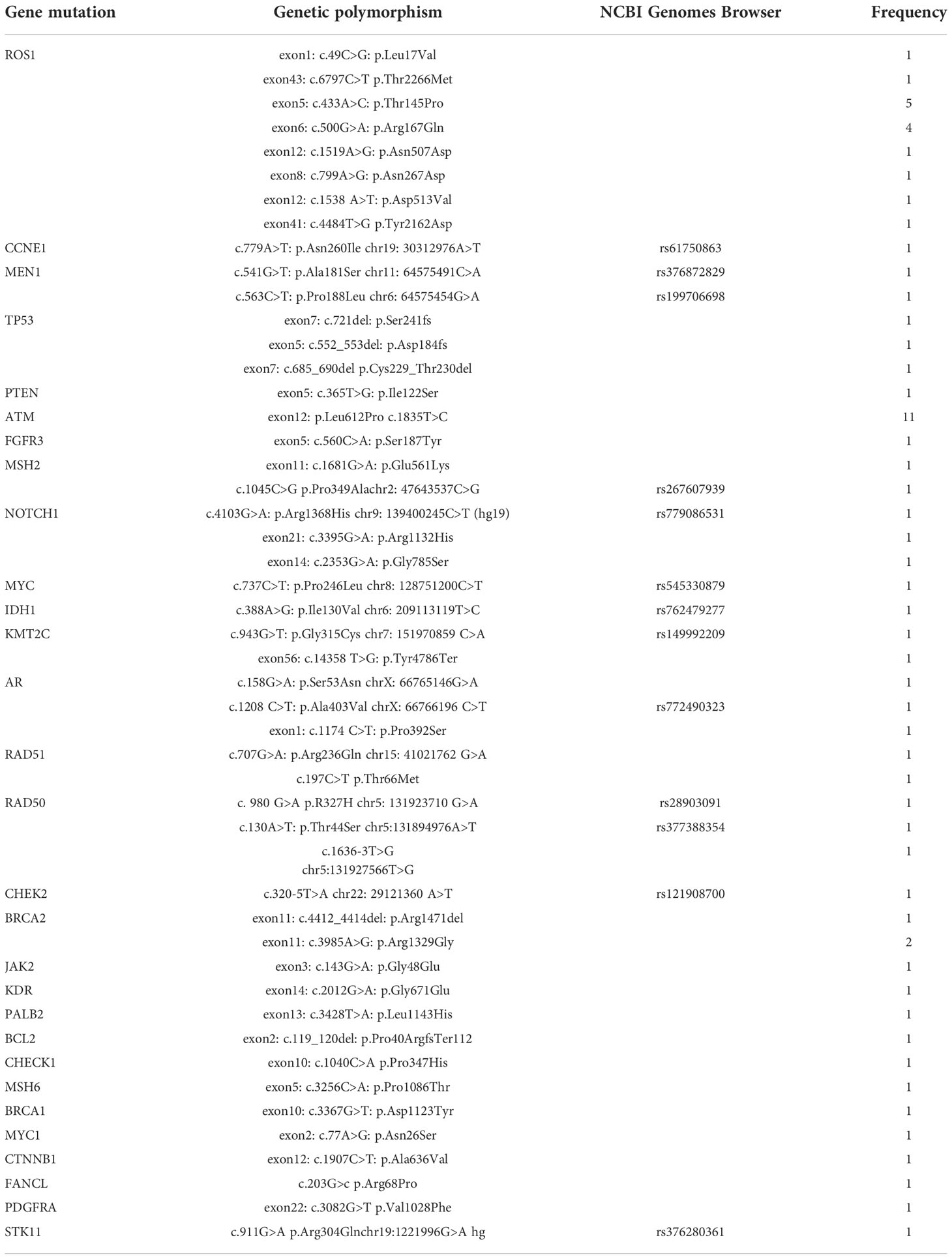
Table 2 Somatic mutations of uncertain significance (VUS) identified in patients with HGSC.
Germline NGS analysis was performed in 30 patients with HGSC (Supplemental Table 2). All germline mutations are presented in Table 3. The most frequent mutated genes identified were BRCA1 [8/30; 27%] and BRCA2 [4/30; 13%] as expected. Other pathogenic germline mutations were identified in APC (c.3920T>A) and MUTYH (c.452A>G) genes. Of note, the most common VUS mutations were identified in HRR-related genes, including ATM (c.7816A>G), BRIP (c.2327 C>A), CHEK2 (c.320-5T>A).
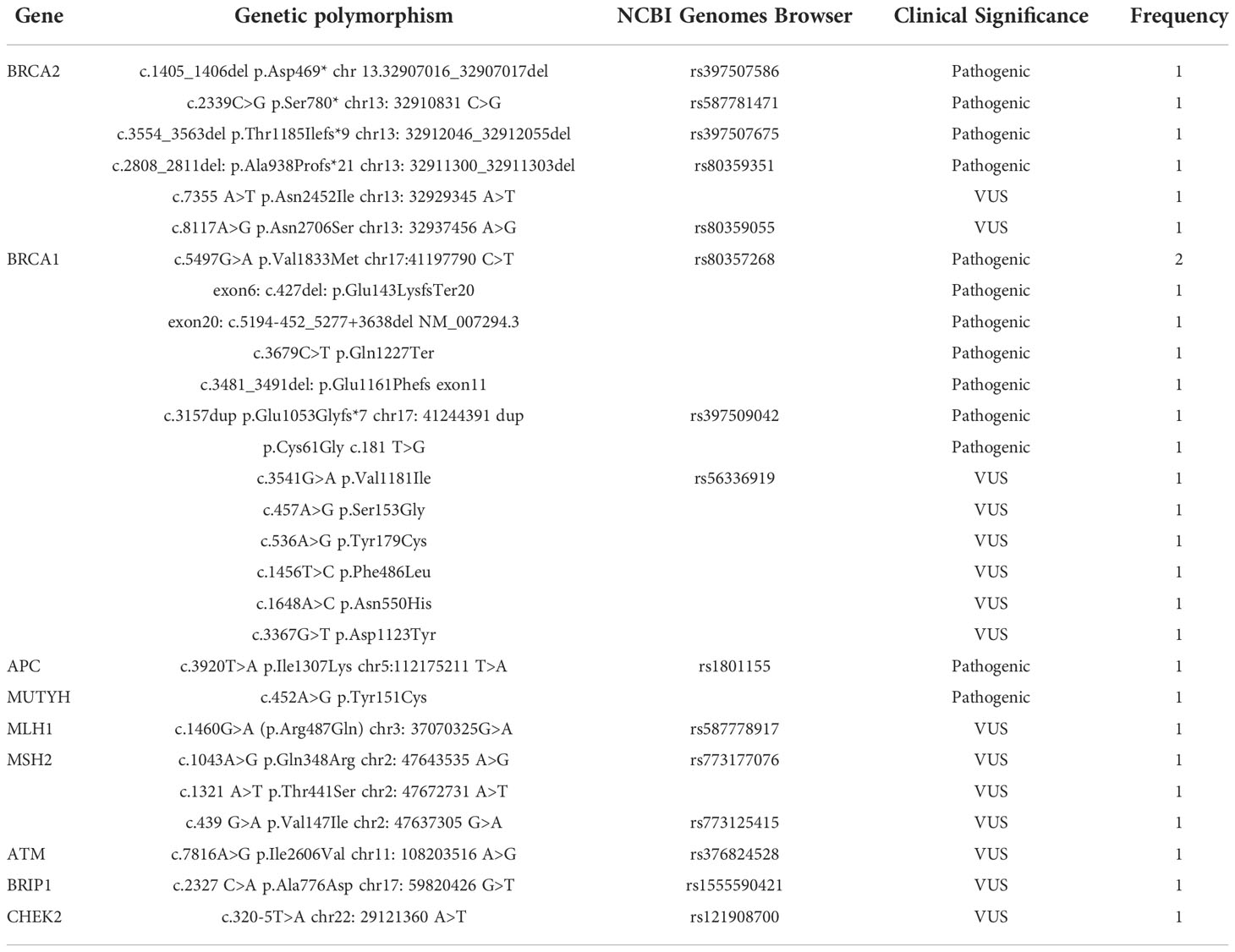
Table 3 Germline mutations in patients with HGSC.
All variants identified in patients with LGSC are summarized in Table 4. Somatic mutations in BRCA1(c.5497G>A) and NRAS (c.182A>G) genes were detected. Although very uncommon, one patient with LGSC harbored a TP53 gene mutation (c.818G>A). In endometrioid carcinoma [EC], PTEN [3/7; 43%] was the most common gene with pathogenic mutations (Table 5). Pathogenic mutations in other genes include ATM (c.3539_3540del), PIK3CA (c.1633G>A), MSH6 (c.2342del), KMT2C (c.5053G>T) and KRAS (c.37G>T). In OCCC, PIK3CA (c.1637A>G) and KRAS (c.35G>T) (Table 6) were the two genes with pathogenic mutations. Two patients with mucinous carcinomas were analyzed. TP53 (c.818G>A) pathogenic variant and somatic VUS in IDH1 (c.548A>G), STK11 (c.901C>T) and ROS1 (c.6344A>G, c.6098A>C, c.1094G>C) genes were identified in these patients.
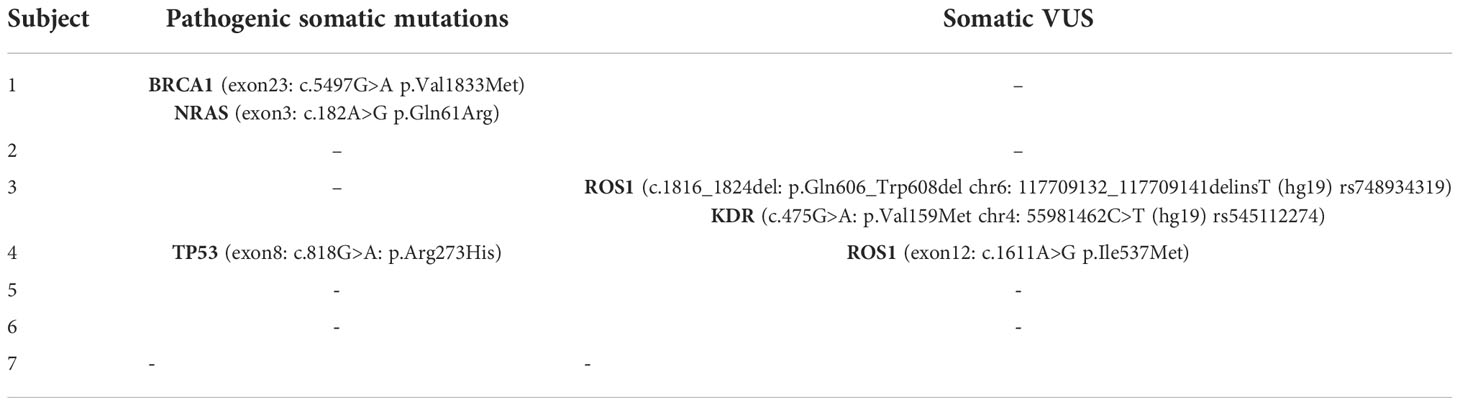
Table 4 Somatic mutations in patients with LGSC.
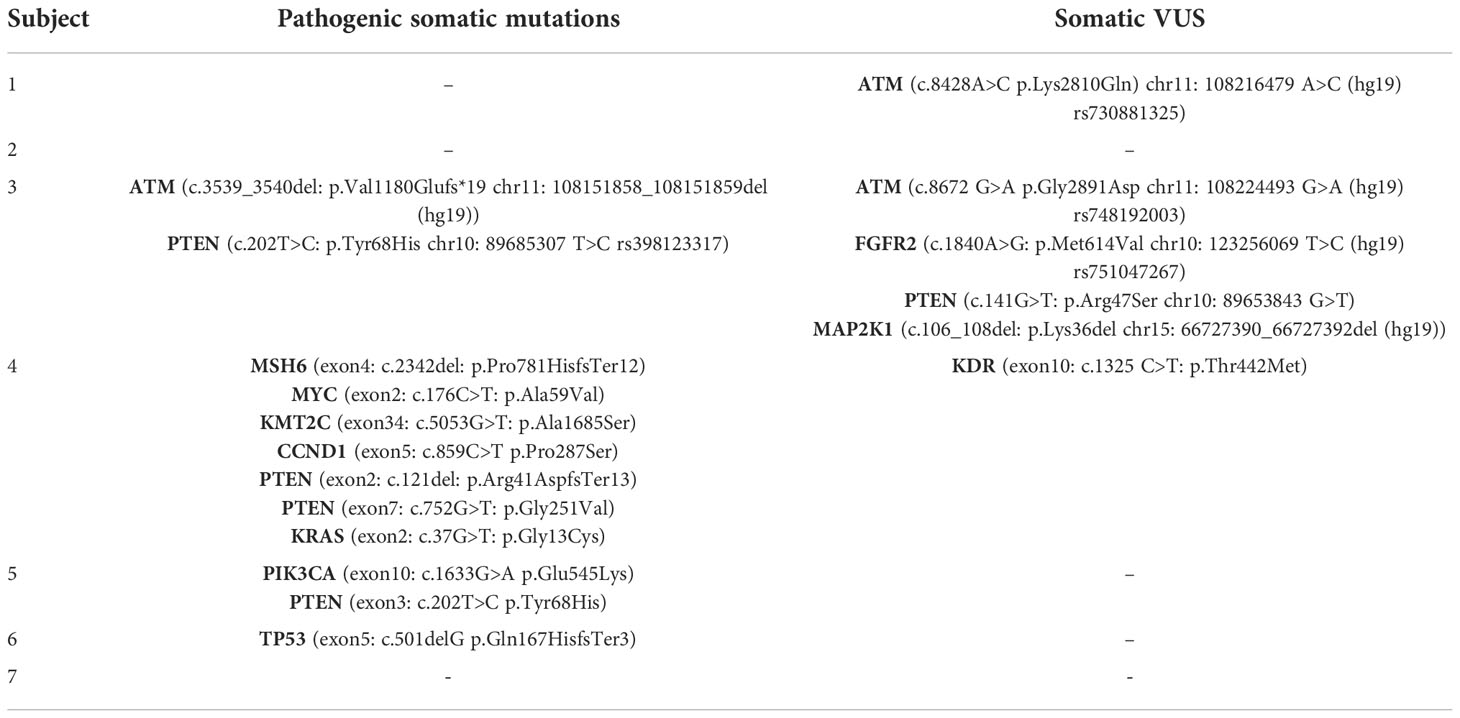
Table 5 Somatic mutations in patients with endometrioid (EC) ovarian carcinoma.

Table 6 Somatic mutations in patients with OCCC.
We here report the mutational landscape of ovarian cancer patients treated in the Oncology Department of Alexandra University Hospital as defined that underwent powerful NGS analysis. In the era of precision medicine, the identification of druggable mutations could help to optimize treatment especially after the introduction of PARP inhibitors in clinical practice. Mutations in HRD genes other than BRCA1/2 that are necessary for successful HR repair (RAD50, RAD51, ATM, PALB2, RAD52, ATM, CHEK2) can lead to genomic instability and HR deficiency. Of note, one in four women with ovarian cancer will have a germline HR deficiency and an additional 5–7% will have a somatic HR deficiency (9).
Patients with HGSC comprise the main population in our analysis. TP53 [68%; 34/50] and BRCA1 [22%; 11/50] ARE the genes with the highest number of pathogenic somatic mutations, as described in previous literature. However, many other genes with pathogenic somatic mutations were also reported (RB1, NF1, BRCA2, AKT1, RAD50, PIK3CA). It has been described that recurrent mutations in NF1 (4-6%), RB1 (2-6%) and PTEN (<1%) are observed in HGSC and when including larger deletions these alterations become even more frequent (NF1: 20%; RB1: 17%; PTEN: 7%) (10). In accordance with these data, pathogenic mutations in RB1 [2%; 1/50] and NF1 [2%; 1/50] were also identified in our study. In addition, pathogenic and VUS mutations involve genes of the homologous recombination (HR) pathway. These genes include ATM, RAD51, CHEK2, PALB2, CHECK1, CTNNB1, BRCA1. As it is known, alterations in HRR pathway genes harbor the 50% of HGSC tumors. HRR alterations involve Fanconi anemia genes (PALB2, FANCA, FANCL, FANCI, FANCC), core RAD genes (RAD50, RAD51, RAD51B, RAD51C) as well as DNA damage response genes (ATM, ATR, CHEK1, CHEK2) (10). The Cancer Genome Atlas (TCGA) analysis reported that HGSC tumors are characterized by mutations in PTEN (7%), RAD51C (3%), ATM/ATR (2%) and Fanconi anemia genes (5%). Of note, Pennington et al. associated the presence of somatic or germline HR mutations with platinum sensitivity and favorable prognosis (P = 0.0006) (11). Overall survival was 59 months for patients with somatic HR mutations in contrast to 41 months of non-carriers (11).
The majority of patients were characterized by BRCA1 [8/30; 27%] and BRCA2 [4/30; 13%] germline mutations, while VUS germline mutations were identified in HRR-related genes, including ATM (c.7816A>G), BRIP (c.2327 C>A), CHEK2 (c.320-5T>A). Another study also reported similar findings (11). Apart from BRCA1/2 germline mutations that predominate in HGSC, other germline mutations were reported in HR genes: (2%) in BARD1, 4 (4.5%) in BRIP1, 1 (1%) in CHEK1, 3 (3%) in CHEK2, 2 (2%) in FAM175A, 1 (1%) in NBN, 2 (2%) in PALB2, 3 (3%) in RAD51C and 4 (4.5%) in RAD51D. Recent literature supports that up to 24% of ovarian cancers are associated with germline mutations, and of these, 29% harbor mutations in genes other than BRCA1/2 (9). Germline mutations in other HRR genes including BRIP1, ATM RAD51C, RAD51D contribute cumulatively to about 2% of HGSC (10). These genetic alterations are both prognostic and predictive biomarkers: HRD tumors are associated with a prolonged survival, sensitivity to platinum chemotherapy and PARP inhibition (10, 11). We also report one case of germline pathogenic APC (c.3920T>A) mutation and another of germline pathogenic MUTYH (c.452A>G) mutation. Heterozygous APC germline mutations predispose to familial adenomatous polyposis (FAP) syndrome and a lifetime risk for colorectal cancer (12). APC germline mutation will lead to the development of more than 100 adenomas at adolescence that will eventually lead to CRC by the age of 40 if left untreated (12). Similarly, MUTYH germline mutations cause an autosomal recessive form of familial adenomatous polyposis known as MYH-associated polyposis (MAP) (13). People with MAP tend to develop multiple adenomatous colon polyps although sometimes at a lesser extent than those with FAP (10-100 adenomas) (13). Approximately 1 to 2 percent of the general population carry a single (monoallelic) germline MUTYH pathogenic variant, whereas biallelic MUTYH pathogenic variants are found in 7 to 13 percent of patients with >100 adenomas and in 14 to 40 percent of patients with 10 to 99 adenomas. Interestingly, MAP is associated with the significant increase in the incidence of ovarian, bladder, and skin cancers and a trend of increased risk of breast cancer (14). There are also reports of APC carriers developing ovarian or endometrial tumors although rarely (15). Our patient had a synchronous BRCA1 germline mutation which explains the development of HGSC ovarian cancer.
Focusing on non-high grade histologies, BRCA1(c.5497G>A) and NRAS (c.182A>G pathogenic somatic mutations were detected in LGSC patients. According to literature, LGSC commonly involves mutations in MAPK pathway genes (KRAS [25%], BRAF [8%], NRAS [8%]), whereas BRCA1/2 are rarely detected (10). In EC patients, PTEN [3/7; 43%] was the most common pathogenic mutations identified, along with ATM, PIK3CA, MSH6, KMT2C and KRAS mutations. Similarly, PIK3CA and KRAS were the main pathogenic mutations identified in OCCC. Based on a dualistic model of carcinogenesis, EOC could be divided into two categories: type I tumors that comprise of LGSC, low-grade EC, OCCC and mucinous carcinomas and type II tumors that include HGSC, high-grade EC and undifferentiated carcinomas. Type I tumors are relatively genetically stable and are characterized by specific mutations, including KRAS, BRAF, ERBB2, CTNNB1, PTEN PIK3CA, ARID1A and PPPR1A, but rarely harbor TP53 mutations (16). Indeed, the most common mutations observed in EC are CTNNB1 [30-50%], PIK3CA [15-40%], ARID1A [30-35%], PTEN [20-30%] and KRAS [10-30%] (10). OCCC significantly overlaps with EC in terms of mutational profile harboring ARID1A [50-75%], PIK3CA [40-50%] and KRAS [15%] in the vast majority of cases (10). Both histological subtypes typically arise from endometriosis and are the predominant subtypes observed in patients with endometriosis (60% for EC and 15% for OCCC). These data come in agreement with the mutations identified in our study, although the number of cases is relatively limited.
Concerning the limitations of our study that deserve mention, it is important to advert that we analyzed a small number of tumor samples and blood samples due to the increased cost of sequencing. Despite the small number of samples, NGS is highly accurate and rapidly analyzes the targeted regions of the genome enabling the characterization of both pathogenic and VUS mutations. Given the fact that most ovarian cancer patients undergo either a more targeted genetic testing e.g. BRCA1/2 gene test or an only somatic mutation test, this genome-wide analysis is of high value.
We here report the mutational profile of ovarian cancer patients treated in a single institution. Germline and somatic tumor genetic testing should be offered in most patients with ovarian carcinomas as a prognostic and predictive biomarker. Since the approval of novel therapies including PARP inhibitors in clinical practice, we should identify the population that could be of the utmost benefit from this treatment.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Review Board of Alexandra University Hospital (Ethics code: 513/15-07-2020). The patients/participants provided their written informed consent to participate in this study.
FZ, KK, and M-AD: Conceptualization, KA: validation, KA: formal analysis, AA, A-MP, AK. MK. and EZ; investigation, AA, A-MP, AK, EZ, and MK: data curation, AA; writing—original draft preparation, AA, AK, ML, FZ, and EZ: writing—review and editing, A-MP, FZ, KK, and M-AD: supervision, FZ, M-AD, KK, and ML: project administration. All authors have read and agreed to the published version of the manuscript.
KK has received honoraria by Roche, BMS, MSD and IPSEN. M-AD has received honoraria from participation in advisory boards from Amgen, Bristol-Myers-Squibb, Celgene, Janssen, Takeda. FZ has received honoraria for lectures and has served in an advisory role for Astra-Zeneca, Daiichi, Eli-Lilly, Merck, Novartis, Pfizer, and Roche. ML has received honoraria by Roche, Astra Zeneca, Astellas, MSD, Janssen, BMS and IPSEN.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.1030786/full#supplementary-material
1. Cancer today (2021). Available at: https://gco.iarc.fr/today/home.
2. Ovarian cancer stages, survival rate and prognosis | OCRA (2022). Available at: https://ocrahope.org/patients/about-ovarian-cancer/staging/.
3. Lheureux S, Gourley C, Vergote I, Oza AM. Epithelial ovarian cancer. Lancet (2019) 393:1240–53. doi: 10.1016/S0140-6736(18)32552-2
4. FDA Approves bevacizumab in combination with chemotherapy for ovarian cancer. FDA (2022). Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-bevacizumab-combination-chemotherapy-ovarian-cancer.
5. Moore K, Colombo N, Scambia G, Kim B-G, Oaknin A, Friedlander M, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med (2018) 379:2495–505. doi: 10.1056/NEJMoa1810858
6. Ray-Coquard I, Pautier P, Pignata S, Pérol D, González-Martín A, Berger R, et al. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. N Engl J Med (2019) 381:2416–28. doi: 10.1056/NEJMOA1911361/SUPPL_FILE/NEJMOA1911361_DATA-SHARING.PDF
7. myChoice® CDx - myriad oncology (2022). Available at: https://myriad-oncology.com/mychoice-cdx/.
8. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American college of medical genetics and genomics and the association for molecular pathology. Genet Med (2015) 17:405–24. doi: 10.1038/gim.2015.30
9. Frey MK, Pothuri B. Homologous recombination deficiency (HRD) testing in ovarian cancer clinical practice: A review of the literature. Gynecol Oncol Res Pract (2017) 4:1–11. doi: 10.1186/S40661-017-0039-8
10. Molecular pathology, an issue of surgical pathology clinics, EBook - Bιβλία Google (2022). Available at: https://books.google.gr/books?id=gH49EAAAQBAJ&pg=PA420&lpg=PA420&dq=mutations+lgsc&source=bl&ots=rPYkFhq5WP&sig=ACfU3U2d0i1ZM7hUsNQZZZX0xjMW4aoBiA&hl=el&sa=X&ved=2ahUKEwjDt4OS69f3AhWiSfEDHe_8CJEQ6AF6BAgOEAM#v=onepage&q=mutationslgsc&f=false.
11. Pennington KP, Walsh T, Harrell MI, Lee MK, Pennil CC, Rendi MH, et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin Cancer Res (2014) 20:764–75. doi: 10.1158/1078-0432.CCR-13-2287
12. Preisler L, Habib A, Shapira G, Kuznitsov-Yanovsky L, Mayshar Y, Carmel-Gross I, et al. Heterozygous APC germline mutations impart predisposition to colorectal cancer. Sci Rep (2021) 11(1):5113. doi: 10.1038/S41598-021-84564-4
13. Sieber OM, Lipton L, Crabtree M, Heinimann K, Fidalgo P, Phillips RKS, et al. Multiple colorectal adenomas, classic adenomatous polyposis, and germ-line mutations in MYH. N Engl J Med (2003) 348:791–9. doi: 10.1056/NEJMOA025283
14. Vogt S, Jones N, Christian D, Engel C, Nielsen M, Kaufmann A, et al. Expanded extracolonic tumor spectrum in MUTYH-associated polyposis. Gastroenterology (2009) 137:1976–85. doi: 10.1053/J.GASTRO.2009.08.052
15. Stoffel M, Rysavy MB, Rose SL, Laffin J, Rehrauer WM, Reza Hafez G, et al. Multiple concurrent unusual neoplasms presenting in a patient with familial adenomatous polyposis: A case report and review of the literature. Hum Pathol Case Rep (2018) 14:41–6. doi: 10.1016/J.EHPC.2018.07.004
Keywords: ovarian cancer, next-generation sequencing, NGS, germline mutations, BRCA, HRD
Citation: Andrikopoulou A, Zografos E, Apostolidou K, Kyriazoglou A, Papatheodoridi A-M, Kaparelou M, Koutsoukos K, Liontos M, Dimopoulos M-A and Zagouri F (2022) Germline and somatic variants in ovarian carcinoma: A next-generation sequencing (NGS) analysis. Front. Oncol. 12:1030786. doi: 10.3389/fonc.2022.1030786
Received: 29 August 2022; Accepted: 31 October 2022;
Published: 01 December 2022.
Edited by:
Sarah M. Temkin, National Institutes of Health (NIH), United StatesReviewed by:
Andrea Moreno Manuel, Fundación de Investigación del Hospital General Universitario de Valencia, SpainCopyright © 2022 Andrikopoulou, Zografos, Apostolidou, Kyriazoglou, Papatheodoridi, Kaparelou, Koutsoukos, Liontos, Dimopoulos and Zagouri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Flora Zagouri, ZmxvcmF6YWdvdXJpQHlhaG9vLmNvLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.