 Kota Yoshifuji
Kota Yoshifuji Koji Sasaki
Koji Sasaki
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 06 October 2022
Sec. Hematologic Malignancies
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1021662
This article is part of the Research TopicAdvances in the Treatment of Chronic Myeloid LeukemiaView all 7 articles
The prognosis of chronic myelogenous leukemia (CML-CP) in chronic phase has improved dramatically since the introduction of imatinib. In addition to imatinib, second- and third-generation tyrosine kinase inhibitors (TKIs) and a novel allosteric inhibitor, asciminib, are now available. During long-term TKI therapy, the optimal selection of TKI therapy for individual patients requires the understanding of specific patterns of toxicity profile to minimize chronic toxicity and the risk of adverse events, including pulmonary arterial hypertension, pleural effusion, and cardiovascular events. Given the high efficacy of TKI therapy, dose modifications of TKI therapy reduce the risk of toxicities and improves quality of life during therapy. In this review article, we summarize the characteristics and adverse event profile of each TKI and dose modifications in patients with CML-CP and discuss future perspectives in the treatment of CML-CP.
Chronic myelogenous leukemia (CML) is a clonal myeloproliferative neoplasm derived from pluripotent hematopoietic stem cells (1) and characterized by the presence of Philadelphia chromosome, which is caused by the reciprocal translocation of the ABL1 (Abelson murine leukemia) gene on the long arm of chromosome 9 and the BCR (breakpoint cluster region) gene on the long arm of chromosome 22. The BCR::ABL1 protein constitutively activates downstream signaling pathways such as the Ras, phosphatidylinositol-3 kinase (PI3K)/Akt, and JAK/STAT pathways, which induce tumor growth (2). The incidence of CML varies between 10 and 15 cases/106 people/year without significant regional or racial differences (3); the median age at diagnosis ranges from 55 to 65 years (3–5).
The development of imatinib, a BCR::ABL1 tyrosine kinase inhibitor (TKI), dramatically improved the prognosis of CML (6, 7). Subsequently, second-generation TKIs dasatinib, nilotinib, and bosutinib and third-generation TKI, ponatinib, which shows efficacy in refractory cases with T315I mutation, have been approved by the Food and Drug Administration in the United States. More recently, asciminib, a first-in-class TKI that inhibits BCR::ABL1 by binding to the ABL myristoyl pocket, has been approved for CML treatment (8). These TKI therapy has achieved favorable survival in patients with CML similar to that of general population, particularly in patients who achieved remission (9–15). Therefore, the optimal selection of TKI, the management of TKI toxicity, and the monitoring of response are the key to improve quality of life during long-term TKI therapy and to prevent TKI-related complications given the near-normal life expectancy in patients with CML (16).
Treatment-free remission (TFR) is now an emerging therapeutic goal for patients in sustained deep molecular response (DMR) (17–19). Approximately, half of the patients maintained DMR without TKI therapy (20–22). However, a long-term TKI therapy is required before discontinuation. Therefore, we must remain vigilant for adverse events associated with TKI therapy.
In addition to BCR::ABL1, each TKI has its specific activity against various other kinases (off-target effect) (23). The variation of the inhibition on other kinases lead to a wide range of symptomatic toxicities: Imatinib may cause fluid retention and muscle cramps (24, 25); dasatinib, pulmonary arterial hypertension and pleural effusion (26, 27); nilotinib, hyperglycemia, hyperlipidemia, pancreatitis, and cardiovascular events (28, 29); bosutinib, hepatic impairment and diarrhea (30); and ponatinib, hypertension, pancreatitis, and arterial occlusive events (31). Although the exact cause of dasatinib-related pleural effusion is unknown, it has been hypothesized that this adverse event may be immune-mediated based on reports of elevated lymphocyte counts in pleural fluid and tissue (32). Dasatinib-related pleural effusion may also result from platelet derived growth factor receptor (PDGFR) β inhibition, which lowers interstitial fluid pressure, or from SRC-family kinases inhibition, which alters vascular permeability (33). Several mechanisms have been reported for the pathogenesis of arterial occlusive events. Nilotinib and ponatinib inhibit c-KIT and PDGFR, affecting vascular endothelial cells and perivascular cells, delaying vascular injury recovery and inhibiting angiogenesis (34–36). Nilotinib inhibits discoidin domain receptor 1 (DDR1), which is involved in plague formation, and promotes atherosclerosis (37). Ponatinib causes hypertension via inhibition of the vascular endothelial growth factor receptor (VEGFR) (38). Moreover, in a recent report, in which pro-inflammatory cytokines (IL6 and TNFα) and anti-inflammatory cytokine (IL10) of patients with CML were prospectively measured, nilotinib, not dasatinib and imatinib, induced an imbalance between pro- and anti- inflammatory cytokines. This imbalance led to an excess of inflammation and might help to promote atherothrombotic events (39). To reduce these adverse events, appropriate TKI selection is necessary in light of the patient’s underlying comorbidities. Moreover, the significance of TKI dose modification is also attractive attention (40).
In this review, we first describe the characteristics and adverse event profile of each TKI approved for CML treatment, and then we discuss the latest findings on TKI dose modification in patients with CML to reduce adverse events.
Imatinib, the first TKI, inhibits the tyrosine kinase by targeting the ATP-binding site of BCR::ABL1. Imatinib also inhibits PDGFR and KIT kinase activities. The phase 3 IRIS trial demonstrated that first-line treatment of CML with imatinib, at a dose of 400 mg once daily, was more effective and led to fewer adverse events than combination treatment with interferon alfa and cytarabine (24). The 18-month cumulative complete cytogenetic response (CCyR) rates were 76.2% and 14.5% in the imatinib and the combination of interferon alfa and cytarabine, respectively (P<0.001). A long-term follow-up study of patients in the IRIS trial demonstrated favorable outcome with a 10-year survival of 83.3% in the imatinib group (25).
The STIM study, the first prospective multicenter study of imatinib discontinuation in patients with CML who maintained DMR for at least 2 years, revealed that 41% of patients maintained DMR at 12 months (20). Subsequently, the A-STIM study reported the fluctuations of BCR::ABL1 transcript levels below the major molecular response (MMR) threshold and concluded the loss of MMR is a practical threshold to resume TKI therapy. In the A-STIM study, 64% of patients maintained MMR at 12 months after imatinib discontinuation (41).
Imatinib may affect quality of life through chronic common adverse events, including edema, nausea, muscle spasms, and rash (24). However, serious adverse events were uncommon during the first 12 months of treatment (25). Cardiovascular events have been reported in 7.1% of patients treated with imatinib, and second neoplasms (benign or malignant) have been observed in 11.3% (25).
Dasatinib, a second-generation TKI, has 325 times the potency of imatinib against unmutated BCR::ABL1 in vitro (42). Dasatinib also inhibits Src family kinases, as off-target effects. The open-label, multinational, randomized phase 3 DASISION trail revealed that dasatinib 100 mg/day induced significantly higher and faster CCyR and MMR than imatinib 400 mg/day. The 12-month CCyR and MMR rate was 77% and 46% in the dasatinib group and 66% and 28% in the imatinib group, respectively (26).
Several trials of dasatinib discontinuation have been conducted in patients with CML (21, 43–45). The DADI study evaluated the treatment-free remission in patients who received dasatinib as a first-line treatment, and reported that 55.2% of patients maintained DMR at least 1 year since the discontinuation of dasatinib (21).
Dasatinib-related adverse events include pleural effusion, pulmonary arterial hypertension, and bleeding diathesis. In a 5-year follow-up of the DASISION trial, the incidence of pleural effusion was 28% in the dasatinib group (27). The onset of pleural effusion was the highest in the first year with reduced incidence of subsequent years of dasatinib therapy. Patients 65 years and older were more likely to develop pleural effusions than younger patients. In retrospective real-life analysis, 196 out of 852 CML patients (23%) who were treated with dasatinib in 21 Italian hematological centers suffered from pleural effusions, and recurrence occurred in 59.4% of cases after dose reduction of dasatinib (46). In older cases, 15.4 to 28.8% of older patients who received dasatinib suffered from them (47, 48).
The first case of dasatinib-related pulmonary arterial hypertension was reported in 2009 (49). Subsequently, several cases of dasatinib-related pulmonary arterial hypertension were reported in the French pulmonary hypertension registry (50). In the 5-year follow-up of DASISION, the incidence of pulmonary arterial hypertension was 5% after years of therapy in the dasatinib group (27). In many cases, pulmonary arterial hypertension occurred several years after initiation of dasatinib, and particular attention should be paid to patients receiving long-term dasatinib treatment. Dasatinib-related pulmonary arterial hypertension typically appears to be curable if the drug is stopped (51), but sometimes irreversible cases were reported (52).
Nilotinib, a second-generation TKI, has greater potency and selectivity for BCR::ABL1 than imatinib (53). The open-label, multicenter, phase 3, randomized ENESTnd trial demonstrated that nilotinib (600 mg/day or 800 mg/day) was more efficacious than imatinib 400 mg/day. The 12-month cumulative CCyR rates were 80%, 78%, and 65% in the nilotinib 600 mg/day, nilotinib 800 mg/day and imatinib 400 mg/day, respectively (P<0.001); the 12-month cumulative MMR rates were 44%, 43%, and 22% in the nilotinib 600 mg/day, nilotinib 800 mg/day, and imatinib 400 mg/day, respectively (P<0.001) (28).
Several prospective nilotinib discontinuation trials have been conducted (54–56). The ENESTfreedom study, a TKI discontinuation study for patients who received front-line nilotinib for more than 2 years and achieved DMR for at least 1 year, reported that 51.6% of patients maintained MMR at 48 weeks (54).
In a 5-year follow-up of the ENESTnd trial, the rates of ischemic cerebrovascular events, peripheral artery disease, and other cardiovascular events were higher in patients treated with nilotinib than in patients treated with imatinib. A positive linear relationship was observed between the cumulative incidence of cardiovascular events and treatment duration (29). Moreover, in this study, cardiovascular events were more common in patients with higher baseline Framingham general cardiovascular risk scores (57). Therefore, baseline Framingham score was predictive of cardiovascular events during nilotinib therapy (29).
Bosutinib, a second-generation TKI that targets Src and ABL, showed greater activity against BCR::ABL1 in vitro compared with imatinib, with minimal activity against c-KIT or PDGFR (58, 59). The open-label, multinational, phase 3, randomized BELA trial compared bosutinib (500 mg once daily) with imatinib (400 mg once daily) for patients with newly diagnosed CML; the primary endpoint of 12-omonth CCyR was not achieved (bosutinib 70% versus imatinib 68%) (60). The phase 3 BFORE trial compared bosutinib (400 mg once daily) with imatinib (400 mg once daily) for patients with newly diagnosed CML. The 12-month CCyR rates were 77.2% and 66.4% in the bosutinib and imatinib group, respectively; the 12-month MMR rates were 47.2% and 36.9%, respectively (30). The randomized trials confirmed the efficacy of frontline bosutinib at the dose of 400 mg/day compared to standard-dose imatinib.
Gastrointestinal and liver dysfunction and rash were the common adverse events during bosutinib therapy in the 5-year follow-up of BFORE (61). Diarrhea (79.9%), nausea (75%), ALT elevation (33.6%), AST elevation (25.7%), and rash (23.1%) were reported in the bosutinib group; in the bosutinib group, cardiovascular, cerebrovascular, and peripheral vascular adverse events rates were 4.9%, 0.7%, and 2.2%, respectively. Especially, diarrhea is sometimes debilitating. In BFORE trial, grade 3/4 diarrhea rates were 9.0% and 1.1% in the bosutinib and imatinib group, respectively. If diarrhea developed, patients should use antidiarrheal agents, avoid high-fat foods and alcohol, and drink sufficient fluids to avoid dehydration.
Ponatinib, the only third-generation TKI, inhibits mutated BCR::ABL1, including the T315I mutation, which confers resistance to first- and second-generation TKIs. Ponatinib also has activity against VEGFR, SRC, FGFR, and PDGFR (62). Ponatinib is approved for patients with CML who had resistance to or intolerant of previous TKI therapy. The phase 2 PACE trial demonstrated the efficacy of ponatinib at a starting dose of 45 mg once daily in patients with CML who experienced resistance to or could not tolerate dasatinib or nilotinib or had the T315I mutation (31). In a 5-year follow-up of the PACE study, 60% and 40% of the patients achieved major cytogenetic response and MMR, respectively. Moreover, 5-year progression-free and overall survival rates were 53% and 73%, respectively (31).
The prevention of arterial occlusive events, including cardiovascular, cerebrovascular, and peripheral vascular events, are the clinical key during ponatinib therapy through the optimal management of cardiovascular risk factors. In the 5-year follow-up of the PACE study, the cumulative incidence of arterial occlusive events was 31% before the recognition of the optimal prevention during ponatinib therapy. Common adverse events include rash, abdominal pain, thrombocytopenia, headache, dry skin, and constipation (31).
Asciminib is a novel and selective allosteric BCR::ABL1 inhibitor that binds to the ABL myristoyl pocket (63). Asciminib has been approved for patients with CML refractory to or intolerant of previous TKI therapy. The randomized, open-label, multicenter, phase 3 ASCEMBL trial demonstrated the superior efficacy of asciminib (40 mg twice daily) to bosutinib (500 mg once daily) in patients with CML who had been treated with at least two prior TKIs (8). The MMR rates at week 24 were 25.5% and 13.2% in the asciminib and bosutinib group, respectively.
In the ASCEMBL trial, the treatment discontinuation rate was lower in the asciminib group than in the bosutinib group (5.8% versus 21.1%) (8). The incidence of hematological toxicities was higher in the asciminib group than in the bosutinib group; thrombocytopenia was the most common adverse event leading to treatment discontinuation with asciminib. The arterial occlusive event rates were 3.2% and 1.3% in the asciminib and bosutinib group, respectively.
Previous studies examined the efficacy of a higher dose of imatinib (64, 65). Compared with imatinib 400 mg/day, the overall MMR rate was higher in patients receiving imatinib at the dose of 800 mg/day; grade 3 to 4 adverse events were more common in patients receiving imatinib 800 mg/day. Michel et al., in a study of Chronic Myeloid Leukemia-Study IV patients who had achieved at least a stable MMR, found that 90% of patients whose daily imatinib dose was reduced from 800 mg/day to 400 mg/day maintained MMR, with the benefit of less adverse events (66). Cervantes et al. reported that, in patients with sustained DMR to imatinib at a dose of 400 mg daily, reducing the dose to 300 mg daily significantly improved tolerability and preserved efficacy (67). Further, Russo et al. revealed that, in a study of INTERIM study patients who had received imatinib for more than 2 years and achieved MMR, stopping imatinib every 1 month allowed subjects not only to maintain MMR in 69% of patients, and no patients experienced new or more serous adverse events (68).
Dasatinib-related pleural effusion is treated via treatment interruption, dose reduction, diuretics, corticosteroids, or therapeutic thoracentesis. Dasatinib-related pulmonary arterial hypertension is a rare complication with possible poor prognosis when untreated (69). Therefore, the dose reduction of dasatinib may prevent the incidence of pleural effusion and pulmonary arterial hypertension. Naqvi et al. evaluated the efficacy and safety of dasatinib 50 mg/day in patients with newly diagnosed CML (70). The 6-month CCyR rate was 86%; the 12-month MMR rate was 79%. These results compared favorably with historical data from similar patients treated with dasatinib at a dose of 100 mg daily. The incidence of pleural effusion was 6%, which was significantly lower than that in the DASISION trial. Murai et al. examined very low-dose dasatinib 20 mg/day for patients older than 70 years with newly diagnosed CML (71). The 12-month MMR rate was 60%; the adverse event profile was tolerable with an incidence of pleural effusion at 8%. Other strategy to prevent dasatinib-related adverse events is “on/off” treatment. Rosee et al. retrospectively investigated on/off dasatinib regimen (3 to 5 days on, 2 to 4 days off) for CML patients with imatinib intolerance or resistance. This regimen significantly reduced adverse events such as pleural effusion and hematologic toxicity, and 58% achieved disease control (72). Moreover, therapeutic drug monitoring (TDM) is also a strategy to prevent adverse events. In the OPTIM-dasatinib study, CML patients considered overdosed after initiation of dasatinib were randomized between dose-reduction arm and standard dose arm, and dose-reduction reduced the incidence of pleural effusions (73). Now, Phase II trial evaluating TDM of dasatinib in older CML patients is ongoing (CML 12 study).
The ENESTnd study compared the efficacy and safety of nilotinib at 600 mg/day or 800 mg/day and imatinib 400 mg/day. In a 10-year follow-up of the ENESTnd study, the cardiovascular event rates were 16.5%, 23.5%, and 3.6% in the nilotinib 600 mg/day, nilotinib 800 mg/day, and imatinib 400 mg/day, respectively (74). Therefore, nilotinib 300 mg twice daily is recommended as the initial dose of nilotinib for patients with newly diagnosed CML. Rea et al. examined reducing the nilotinib dose after achieving MMR (75). In the NILO-RED study, nilotinib was reduced to only once daily after patients achieved MMR during nilotinib therapy; only two of 81 patients lost MMR after the dose reduction from twice daily to once daily; these two patients re-achieved MMR while continuing the same once-daily dose of nilotinib without TKI switch or dose escalation. Therefore, the dose reduction of nilotinib from twice daily to once daily can be considered in patients with CML after achieving MMR, though there have been no obvious reports of nilotinib dose reduction reducing the risk of cardiovascular events. In the second-line setting, 20 CML-CP patients intolerant to imatinib or dasatinib switched to nilotinib 300mg twice daily in the ENESTswift study, and 74% resolved non-hematological adverse events within 12 weeks (76).
The results of BELA and BFORE trials suggest bosutinib 400 mg daily is the optimal dose of frontline bosutinib therapy (30, 60). Though the BFORE trial had more patients 65 years or older, the treatment discontinuation rates were 22% and 29% in the BFORE and BELA trials. Therefore, the tolerability of bosutinib therapy at the lower dose led to higher rates of CCyR and MMR. Latagliata et al. retrospectively evaluated 101 patients older than 65 years who received bosutinib after resistant to or intolerant of previous TKI therapies. The starting dose of bosutinib was 500 mg/day in 25% of the patients, 400 mg/day in 7%, 300 mg/day in 33%, 200 mg/day in 24%, and 100 mg/day in 2%. Sixty seven percent of patients achieved MMR or deeper with a discontinuation rate of 26.4%. Therefore, lower dose of bosutinib can be considered in frail patients with severe comorbidities who failed multiple TKI therapies (77).
Second- and third-generation TKI therapy has increased the risk of cardiovascular events during TKI therapy. The dose reduction of potent third-generation TKI, ponatinib, can reduce the cardiovascular risk while maintaining its efficacy. Dorer et al. studied the effect of ponatinib dose intensity on arterial occlusive events using pooled data from three clinical trials of ponatinib. Ponatinib dose intensity was a strong independent predictor of increased risk of arterial occlusive events; each dose reduction by 15 mg/day reduced the risk of arterial occlusive events by 33% (78). The phase 2 OPTIC trial evaluated the efficacy and safety of ponatinib dose reduction in patients with CML-CP who had resistance to or intolerance of at least two prior TKI therapy or had T315I mutation. Patients were randomly assigned to three starting-dose ponatinib groups: ponatinib 45 mg/day, 30 mg/day, and 15 mg/day (79). The ponatinib dose was mandatory reduced to 15 mg when BCR::ABL1 transcript levels of 1% or lower on the International Scale (IS). The cumulative rates of BCR::ABL1 1% or lower (IS) were 44.1%, 29%, and 23.1% in the 45 mg/day, 30 mg/day and 15 mg/day, respectively. The arterial occlusive events of any grade were observed in 9.6%, 5.3%, and 3.2% in the 45 mg/day, 30 mg/day, and 15 mg/day, respectively. The consideration of risk/benefit balance is required to decide on the dose of ponatinib; the low-dose ponatinib 15 mg/day should be considered once patients achieved BCR::ABL1 of 1% or lower (IS). Several real-life analysis data also evaluated low-dose ponatinib regimens or full-dose induction followed by dose reduction in patients intolerant to prior TKIs, and showed its effectiveness (80–84).
TKI therapy has normalized survival in patients with CML-CP similar to that of general population, particularly once patients achieved CCyR or deeper. Given the optimal survival during long-term TKI therapy, the monitoring of response, the prevention of adverse events, and the treatment-free remission is the clinical key in practice. Long-term follow-up of multiple randomized clinical trials clarified specific toxicities of each TKI therapy (Table 1). Therefore, the optimal selection of TKI therapy required the consideration of patient’s medical history and comorbidities for long-term TKI therapy.
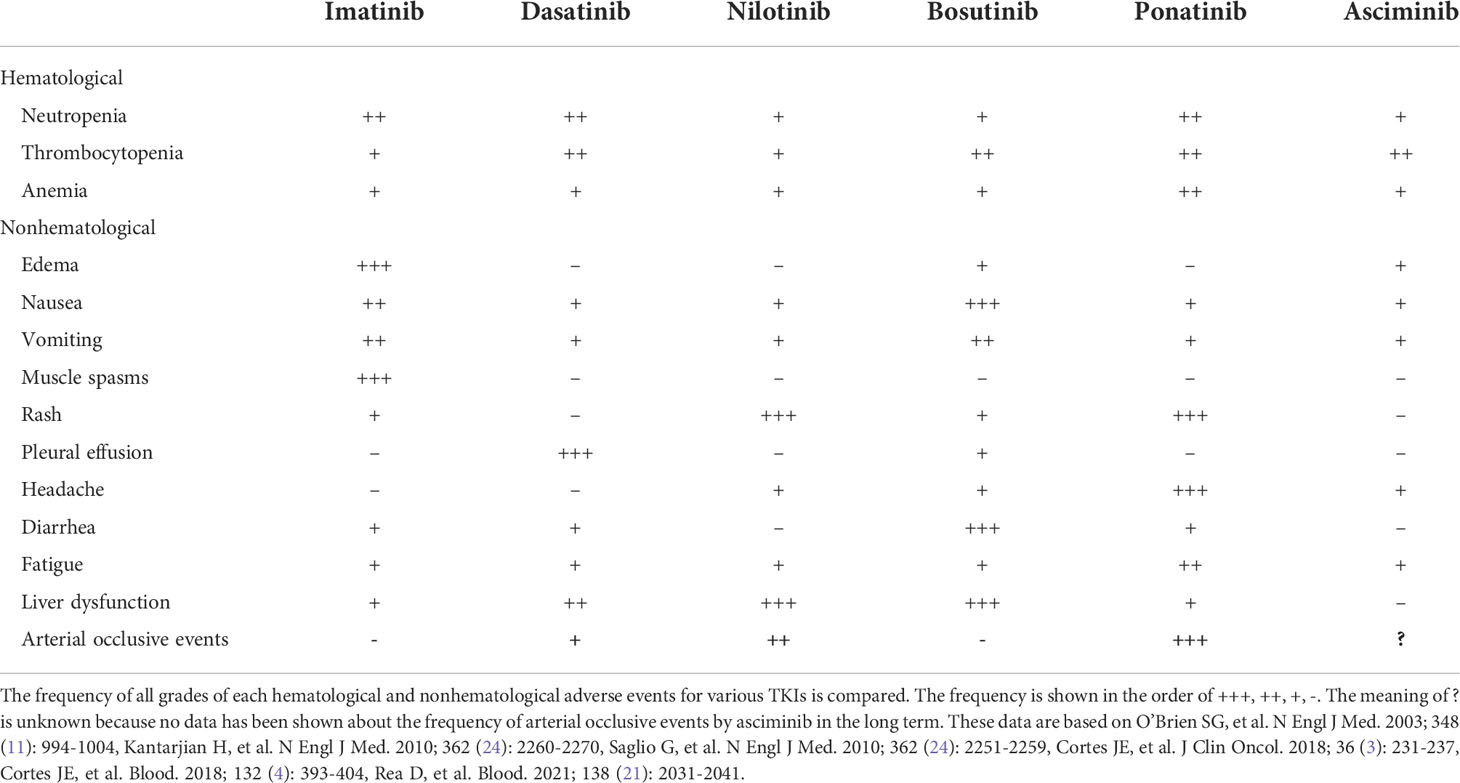
Table 1 Adverse event profiles of tyrosine kinase inhibitors.
Dose reduction of TKI therapy after achieving remission can be considered to minimize the risk of adverse event and to improve quality of life during therapy. Dose reduction can be considered in the frontline therapy, particularly in low-risk patient and older patients. Optimal treatment strategies will be developed for each TKI to minimize the incidence and severity of adverse events. Treatment-free remission is now standard-of-care in patients who maintained DMR over years (22). However, TKI discontinuation is currently limited to a part of patients who have achieved deep molecular response. A novel strategy is required for the optimal selection of TKI therapies during long-term therapy (85). After achieving treatment-free remission, monitoring of BCR::ABL1 transcript levels is still requiredto detect loss of MMR early and restart TKI therapy even with novel therapies (86–91). Eltrombopag can be considered in managing TKI-related thrombocytopenia during TKI therapy (92).
Finally, the prevention and monitoring of anticipated TKI-related adverse events are required after the initiation of TKI therapy. The detection and pre-emptive therapy for cardiovascular risk factors prevents arterial occlusive events during TKI therapy (93). Though the relation of second neoplasm to TKI therapy or the underlying features of CML, the age-appropriate cancer screening should be considered given the 5-year cumulative incidence rate of second neoplasms at 4.4% (94–96).
KY performed a literature search and wrote the initial draft. KS revised and amended the draft. All authors contributed to the article and approved the submitted version.
This study is supported in part by the MD Anderson Cancer Center Leukemia SPORE CA100632, the Cancer Center Support Grant (CCSG) P30CA016672, and the Charif Souki Cancer Research Grant.
KS reported honoraria from Otsuka; research funding and advisory boards from Novartis; advisory boards from Pfizer, outside the submitted work.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rowley JD. Letter: A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and giemsa staining. Nature (1973) 243(5405):290–3. doi: 10.1038/243290a0
2. Kantarjian HM, Talpaz M, Giles F, O'Brien S, Cortes J. New insights into the pathophysiology of chronic myeloid leukemia and imatinib resistance. Ann Intern Med (2006) 145(12):913–23. doi: 10.7326/0003-4819-145-12-200612190-00008
3. Hochhaus A, Saussele S, Rosti G, Mahon FX, Janssen J, Hjorth-Hansen H, et al. Chronic myeloid leukaemia: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29(Suppl 4):iv261. doi: 10.1093/annonc/mdy159
4. Hoffmann VS, Baccarani M, Hasford J, Lindoerfer D, Burgstaller S, Sertic D, et al. The EUTOS population-based registry: incidence and clinical characteristics of 2904 CML patients in 20 European countries. Leukemia (2015) 29(6):1336–43. doi: 10.1038/leu.2015.73
5. Kizaki M, Takahashi N, Iriyama N, Okamoto S, Ono T, Usui N, et al. Efficacy and safety of tyrosine kinase inhibitors for newly diagnosed chronic-phase chronic myeloid leukemia over a 5-year period: results from the Japanese registry obtained by the new TARGET system. Int J Hematol (2019) 109(4):426–39. doi: 10.1007/s12185-019-02613-1
6. Druker BJ, Talpaz M, Resta DJ, Peng B, Buchdunger E, Ford JM, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med (2001) 344(14):1031–7. doi: 10.1056/NEJM200104053441401
7. Jain P, Kantarjian H, Alattar ML, Jabbour E, Sasaki K, Nogueras Gonzalez G, et al. Long-term molecular and cytogenetic response and survival outcomes with imatinib 400 mg, imatinib 800 mg, dasatinib, and nilotinib in patients with chronic-phase chronic myeloid leukaemia: retrospective analysis of patient data from five clinical trials. Lancet Haematol (2015) 2(3):e118–28. doi: 10.1016/S2352-3026(15)00021-6
8. Réa D, Mauro MJ, Boquimpani C, Minami Y, Lomaia E, Voloshin S, et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood (2021) 138(21):2031–41. doi: 10.1182/blood.2020009984
9. Sasaki K, Strom SS, O'Brien S, Jabbour E, Ravandi F, Konopleva M, et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: analysis of patient data from six prospective clinical trials. Lancet Haematol (2015) 2(5):e186–93. doi: 10.1016/S2352-3026(15)00048-4
10. Bower H, Björkholm M, Dickman PW, Höglund M, Lambert PC, Andersson TM. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J Clin Oncol (2016) 34(24):2851–7. doi: 10.1200/JCO.2015.66.2866
11. Sasaki K, Lahoti A, Jabbour E, Jain P, Pierce S, Borthakur G, et al. Clinical safety and efficacy of nilotinib or dasatinib in patients with newly diagnosed chronic-phase chronic myelogenous leukemia and pre-existing liver and/or renal dysfunction. Clin Lymphoma Myeloma Leuk (2016) 16(3):152–62. doi: 10.1016/j.clml.2015.12.003
12. Jain P, Kantarjian H, Patel KP, Gonzalez GN, Luthra R, Kanagal Shamanna R, et al. Impact of BCR-ABL transcript type on outcome in patients with chronic-phase CML treated with tyrosine kinase inhibitors. Blood (2016) 127(10):1269–75. doi: 10.1182/blood-2015-10-674242
13. Sasaki K, Kantarjian HM, Jain P, Jabbour EJ, Ravandi F, Konopleva M, et al. Conditional survival in patients with chronic myeloid leukemia in chronic phase in the era of tyrosine kinase inhibitors. Cancer (2016) 122(2):238–48. doi: 10.1002/cncr.29745
14. Jain P, Kantarjian H, Sasaki K, Jabbour E, Dasarathula J, Nogueras Gonzalez G, et al. Analysis of 2013 European LeukaemiaNet (ELN) responses in chronic phase CML across four frontline TKI modalities and impact on clinical outcomes. Br J Haematol (2016) 173(1):114–26. doi: 10.1111/bjh.13936
15. Takahashi K, Kantarjian HM, Yang Y, Sasaki K, Jain P, DellaSala S, et al. A propensity score matching analysis of dasatinib and nilotinib as a frontline therapy for patients with chronic myeloid leukemia in chronic phase. Cancer (2016) 122(21):3336–43. doi: 10.1002/cncr.30197
16. Issa GC, Kantarjian HM, Gonzalez GN, Borthakur G, Tang G, Wierda W, et al. Clonal chromosomal abnormalities appearing in Philadelphia chromosome-negative metaphases during CML treatment. Blood (2017) 130(19):2084–91. doi: 10.1182/blood-2017-07-792143
17. Morita K, Sasaki K. Current status and novel strategy of CML. Int J Hematol (2021) 113(5):624–31. doi: 10.1007/s12185-021-03127-5
18. Sasaki K. Chronic myeloid leukemia: update on treatment and survival prediction. Rinsho Ketsueki (2020) 61(9):1179–86. doi: 10.11406/rinketsu.61.1179
19. Iurlo A, Cattaneo D, Artuso S, Consonni D, Abruzzese E, Binotto G, et al. Treatment-free remission in chronic myeloid leukemia patients treated with low-dose TKIs: A feasible option also in the real-life. A Campus CML Study Front Oncol (2022) 12:839915. doi: 10.3389/fonc.2022.839915
20. Mahon FX, Réa D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre stop imatinib (STIM) trial. Lancet Oncol (2010) 11(11):1029–35. doi: 10.1016/S1470-2045(10)70233-3
21. Kimura S, Imagawa J, Murai K, Hino M, Kitawaki T, Okada M, et al. Treatment-free remission after first-line dasatinib discontinuation in patients with chronic myeloid leukaemia (first-line DADI trial): a single-arm, multicentre, phase 2 trial. Lancet Haematol (2020) 7(3):e218–e25. doi: 10.1016/S2352-3026(19)30235-2
22. Haddad FG, Sasaki K, Issa GC, Garcia-Manero G, Ravandi F, Kadia T, et al. Treatment-free remission in patients with chronic myeloid leukemia following the discontinuation of tyrosine kinase inhibitors. Am J Hematol (2022) 97(7):856–64. doi: 10.1002/ajh.26550
23. Greuber EK, Smith-Pearson P, Wang J, Pendergast AM. Role of ABL family kinases in cancer: from leukaemia to solid tumours. Nat Rev Cancer (2013) 13(8):559–71. doi: 10.1038/nrc3563
24. O'Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med (2003) 348(11):994–1004. doi: 10.1056/NEJMoa022457
25. Hochhaus A, Larson RA, Guilhot F, Radich JP, Branford S, Hughes TP, et al. Long-term outcomes of imatinib treatment for chronic myeloid leukemia. N Engl J Med (2017) 376(10):917–27. doi: 10.1056/NEJMoa1609324
26. Kantarjian H, Shah NP, Hochhaus A, Cortes J, Shah S, Ayala M, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med (2010) 362(24):2260–70. doi: 10.1056/NEJMoa1002315
27. Cortes JE, Saglio G, Kantarjian HM, Baccarani M, Mayer J, Boqué C, et al. Final 5-year study results of DASISION: The dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J Clin Oncol (2016) 34(20):2333–40. doi: 10.1200/JCO.2015.64.8899
28. Saglio G, Kim DW, Issaragrisil S, le Coutre P, Etienne G, Lobo C, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med (2010) 362(24):2251–9. doi: 10.1056/NEJMoa0912614
29. Hochhaus A, Saglio G, Hughes TP, Larson RA, Kim DW, Issaragrisil S, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia (2016) 30(5):1044–54. doi: 10.1038/leu.2016.5
30. Cortes JE, Gambacorti-Passerini C, Deininger MW, Mauro MJ, Chuah C, Kim DW, et al. Bosutinib versus imatinib for newly diagnosed chronic myeloid leukemia: Results from the randomized BFORE trial. J Clin Oncol (2018) 36(3):231–7. doi: 10.1200/JCO.2017.74.7162
31. Cortes JE, Kim DW, Pinilla-Ibarz J, le Coutre PD, Paquette R, Chuah C, et al. Ponatinib efficacy and safety in Philadelphia chromosome-positive leukemia: final 5-year results of the phase 2 PACE trial. Blood (2018) 132(4):393–404. doi: 10.1182/blood-2016-09-739086
32. de Lavallade H, Punnialingam S, Milojkovic D, Bua M, Khorashad JS, Gabriel IH, et al. Pleural effusions in patients with chronic myeloid leukaemia treated with dasatinib may have an immune-mediated pathogenesis. Br J Haematol (2008) 141(5):745–7. doi: 10.1111/j.1365-2141.2008.07108.x
33. Quintás-Cardama A, Kantarjian H, O'Brien S, Borthakur G, Bruzzi J, Munden R, et al. Pleural effusion in patients with chronic myelogenous leukemia treated with dasatinib after imatinib failure. J Clin Oncol (2007) 25(25):3908–14. doi: 10.1200/JCO.2007.12.0329
34. Andrae J, Gallini R, Betsholtz C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev (2008) 22(10):1276–312. doi: 10.1101/gad.1653708
35. Rix U, Hantschel O, Dürnberger G, Remsing Rix LL, Planyavsky M, Fernbach NV, et al. Chemical proteomic profiles of the BCR-ABL inhibitors imatinib, nilotinib, and dasatinib reveal novel kinase and nonkinase targets. Blood (2007) 110(12):4055–63. doi: 10.1182/blood-2007-07-102061
36. Karvinen H, Rutanen J, Leppänen O, Lach R, Levonen AL, Eriksson U, et al. PDGF-c and -d and their receptors PDGFR-alpha and PDGFR-beta in atherosclerotic human arteries. Eur J Clin Invest (2009) 39(4):320–7. doi: 10.1111/j.1365-2362.2009.02095.x
37. Sun X, Wu B, Chiang HC, Deng H, Zhang X, Xiong W, et al. Tumour DDR1 promotes collagen fibre alignment to instigate immune exclusion. Nature (2021) 599(7886):673–8. doi: 10.1038/s41586-021-04057-2
38. des Guetz G, Uzzan B, Chouahnia K, Morère JF. Cardiovascular toxicity of anti-angiogenic drugs. Target Oncol (2011) 6(4):197–202. doi: 10.1007/s11523-011-0204-7
39. Sicuranza A, Ferrigno I, Abruzzese E, Iurlo A, Galimberti S, Gozzini A, et al. Pro-inflammatory and pro-oxidative changes during nilotinib treatment in CML patients: Results of a prospective multicenter front-line TKIs study (KIARO study). Front Oncol (2022) 12:835563. doi: 10.3389/fonc.2022.835563
40. Iurlo A, Cattaneo D, Bucelli C, Breccia M. Dose optimization of tyrosine kinase inhibitors in chronic myeloid leukemia: A new therapeutic challenge. J Clin Med (2021) 10(3):515. doi: 10.3390/jcm10030515
41. Rousselot P, Charbonnier A, Cony-Makhoul P, Agape P, Nicolini FE, Varet B, et al. Loss of major molecular response as a trigger for restarting tyrosine kinase inhibitor therapy in patients with chronic-phase chronic myelogenous leukemia who have stopped imatinib after durable undetectable disease. J Clin Oncol (2014) 32(5):424–30. doi: 10.1200/JCO.2012.48.5797
42. Lombardo LJ, Lee FY, Chen P, Norris D, Barrish JC, Behnia K, et al. Discovery of n-(2-chloro-6-methyl- phenyl)-2-(6-(4-(2-hydroxyethyl)- piperazin-1-yl)-2-methylpyrimidin-4- ylamino)thiazole-5-carboxamide (BMS-354825), a dual Src/Abl kinase inhibitor with potent antitumor activity in preclinical assays. J Med Chem (2004) 47(27):6658–61. doi: 10.1021/jm049486a
43. Imagawa J, Tanaka H, Okada M, Nakamae H, Hino M, Murai K, et al. Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): a multicentre phase 2 trial. Lancet Haematol (2015) 2(12):e528–35. doi: 10.1016/S2352-3026(15)00196-9
44. Kumagai T, Nakaseko C, Nishiwaki K, Yoshida C, Ohashi K, Takezako N, et al. Dasatinib cessation after deep molecular response exceeding 2 years and natural killer cell transition during dasatinib consolidation. Cancer Sci (2018) 109(1):182–92. doi: 10.1111/cas.13430
45. Shah NP, García-Gutiérrez V, Jiménez-Velasco A, Larson S, Saussele S, Rea D, et al. Dasatinib discontinuation in patients with chronic-phase chronic myeloid leukemia and stable deep molecular response: the DASFREE study. Leuk Lymphoma (2020) 61(3):650–9. doi: 10.1080/10428194.2019.1675879
46. Iurlo A, Galimberti S, Abruzzese E, Annunziata M, Bonifacio M, Latagliata R, et al. Pleural effusion and molecular response in dasatinib-treated chronic myeloid leukemia patients in a real-life Italian multicenter series. Ann Hematol (2018) 97(1):95–100. doi: 10.1007/s00277-017-3144-1
47. Latagliata R, Stagno F, Annunziata M, Abruzzese E, Iurlo A, Guarini A, et al. Frontline dasatinib treatment in a "Real-life" cohort of patients older than 65 years with chronic myeloid leukemia. Neoplasia (2016) 18(9):536–40. doi: 10.1016/j.neo.2016.07.005
48. Stagno F, Breccia M, Annunziata M, Trawinska MM, Iurlo A, Sgherza N, et al. Long term follow-up of frontline dasatinib in older patients with chronic myeloid leukemia in chronic phase treated outside clinical trials: a real-life cohort observational study. Acta Oncol (2021) 60(11):1527–33. doi: 10.1080/0284186X.2021.1971292
49. Mattei D, Feola M, Orzan F, Mordini N, Rapezzi D, Gallamini A. Reversible dasatinib-induced pulmonary arterial hypertension and right ventricle failure in a previously allografted CML patient. Bone Marrow Transplant (2009) 43(12):967–8. doi: 10.1038/bmt.2008.415
50. Montani D, Bergot E, Günther S, Savale L, Bergeron A, Bourdin A, et al. Pulmonary arterial hypertension in patients treated by dasatinib. Circulation (2012) 125(17):2128–37. doi: 10.1161/CIRCULATIONAHA.111.079921
51. Özgür Yurttaş N, Eşkazan AE. Dasatinib-induced pulmonary arterial hypertension. Br J Clin Pharmacol (2018) 84(5):835–45. doi: 10.1111/bcp.13508
52. Daccord C, Letovanec I, Yerly P, Bloch J, Ogna A, Nicod LP, et al. First histopathological evidence of irreversible pulmonary vascular disease in dasatinib-induced pulmonary arterial hypertension. Eur Respir J (2018) 51(3):1701694. doi: 10.1183/13993003.01694-2017
53. Weisberg E, Manley PW, Breitenstein W, Brüggen J, Cowan-Jacob SW, Ray A, et al. Characterization of AMN107, a selective inhibitor of native and mutant bcr-abl. Cancer Cell (2005) 7(2):129–41. doi: 10.1016/j.ccr.2005.01.007
54. Hochhaus A, Masszi T, Giles FJ, Radich JP, Ross DM, Gómez Casares MT, et al. Treatment-free remission following frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: results from the ENESTfreedom study. Leukemia (2017) 31(7):1525–31. doi: 10.1038/leu.2017.63
55. Hughes TP, Clementino NCD, Fominykh M, Lipton JH, Turkina AG, Moiraghi EB, et al. Long-term treatment-free remission in patients with chronic myeloid leukemia after second-line nilotinib: ENESTop 5-year update. Leukemia (2021) 35(6):1631–42. doi: 10.1038/s41375-021-01260-y
56. Nagafuji K, Matsumura I, Shimose T, Kawaguchi T, Kuroda J, Nakamae H, et al. Cessation of nilotinib in patients with chronic myelogenous leukemia who have maintained deep molecular responses for 2 years: a multicenter phase 2 trial, stop nilotinib (NILSt). Int J Hematol (2019) 110(6):675–82. doi: 10.1007/s12185-019-02736-5
57. D'Agostino RB, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the framingham heart study. Circulation (2008) 117(6):743–53. doi: 10.1161/CIRCULATIONAHA.107.699579
58. Puttini M, Coluccia AM, Boschelli F, Cleris L, Marchesi E, Donella-Deana A, et al. In vitro and in vivo activity of SKI-606, a novel src-abl inhibitor, against imatinib-resistant bcr-abl+ neoplastic cells. Cancer Res (2006) 66(23):11314–22. doi: 10.1158/0008-5472.CAN-06-1199
59. Golas JM, Arndt K, Etienne C, Lucas J, Nardin D, Gibbons J, et al. SKI-606, a 4-anilino-3-quinolinecarbonitrile dual inhibitor of src and abl kinases, is a potent antiproliferative agent against chronic myelogenous leukemia cells in culture and causes regression of K562 xenografts in nude mice. Cancer Res (2003) 63(2):375–81.
60. Cortes JE, Kim DW, Kantarjian HM, Brümmendorf TH, Dyagil I, Griskevicius L, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: results from the BELA trial. J Clin Oncol (2012) 30(28):3486–92. doi: 10.1200/JCO.2011.38.7522
61. Brümmendorf TH, Cortes JE, Milojkovic D, Gambacorti-Passerini C, Clark RE, le Coutre P, et al. Bosutinib versus imatinib for newly diagnosed chronic phase chronic myeloid leukemia: final results from the BFORE trial. Leukemia (2022) 36(7):1825–33. doi: 10.1038/s41375-022-01589-y
62. O'Hare T, Shakespeare WC, Zhu X, Eide CA, Rivera VM, Wang F, et al. AP24534, a pan-BCR-ABL inhibitor for chronic myeloid leukemia, potently inhibits the T315I mutant and overcomes mutation-based resistance. Cancer Cell (2009) 16(5):401–12. doi: 10.1016/j.ccr.2009.09.028
63. Wylie AA, Schoepfer J, Jahnke W, Cowan-Jacob SW, Loo A, Furet P, et al. The allosteric inhibitor ABL001 enables dual targeting of BCR-ABL1. Nature (2017) 543(7647):733–7. doi: 10.1038/nature21702
64. Cortes JE, Kantarjian HM, Goldberg SL, Powell BL, Giles FJ, Wetzler M, et al. High-dose imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: high rates of rapid cytogenetic and molecular responses. J Clin Oncol (2009) 27(28):4754–9. doi: 10.1200/JCO.2008.20.3869
65. Cortes JE, Baccarani M, Guilhot F, Druker BJ, Branford S, Kim DW, et al. Randomized, open-label study of daily imatinib mesylate 400 mg versus 800 mg in patients with newly diagnosed, previously untreated chronic myeloid leukemia in chronic phase using molecular end points: tyrosine kinase inhibitor optimization and selectivity study. J Clin Oncol (2010) 28(3):424–30. doi: 10.1200/JCO.2009.25.3724
66. Michel C, Burchert A, Hochhaus A, Saussele S, Neubauer A, Lauseker M, et al. Imatinib dose reduction in major molecular response of chronic myeloid leukemia: results from the German chronic myeloid leukemia-study IV. Haematologica (2019) 104(5):955–62. doi: 10.3324/haematol.2018.206797
67. Cervantes F, Correa JG, Pérez I, García-Gutiérrez V, Redondo S, Colomer D, et al. Imatinib dose reduction in patients with chronic myeloid leukemia in sustained deep molecular response. Ann Hematol (2017) 96(1):81–5. doi: 10.1007/s00277-016-2839-z
68. Russo D, Martinelli G, Malagola M, Skert C, Soverini S, Iacobucci I, et al. Effects and outcome of a policy of intermittent imatinib treatment in elderly patients with chronic myeloid leukemia. Blood (2013) 121(26):5138–44. doi: 10.1182/blood-2013-01-480194
69. Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol (2013) 62Supp l):D34–41. doi: 10.1016/j.jacc.2013.10.029
70. Naqvi K, Jabbour E, Skinner J, Anderson K, Dellasala S, Yilmaz M, et al. Long-term follow-up of lower dose dasatinib (50 mg daily) as frontline therapy in newly diagnosed chronic-phase chronic myeloid leukemia. Cancer (2020) 126(1):67–75. doi: 10.1002/cncr.32504
71. Murai K, Ureshino H, Kumagai T, Tanaka H, Nishiwaki K, Wakita S, et al. Low-dose dasatinib in older patients with chronic myeloid leukaemia in chronic phase (DAVLEC): a single-arm, multicentre, phase 2 trial. Lancet Haematol (2021) 8(12):e902–e11. doi: 10.1016/S2352-3026(21)00333-1
72. La Rosée P, Martiat P, Leitner A, Klag T, Müller MC, Erben P, et al. Improved tolerability by a modified intermittent treatment schedule of dasatinib for patients with chronic myeloid leukemia resistant or intolerant to imatinib. Ann Hematol (2013) 92(10):1345–50. doi: 10.1007/s00277-013-1769-2
73. Rousselot P, Mollica L, Guilhot J, Guerci A, Nicolini FE, Etienne G, et al. Dasatinib dose optimisation based on therapeutic drug monitoring reduces pleural effusion rates in chronic myeloid leukaemia patients. Br J Haematol (2021) 194(2):393–402. doi: 10.1111/bjh.17654
74. Kantarjian HM, Hughes TP, Larson RA, Kim DW, Issaragrisil S, le Coutre P, et al. Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase: ENESTnd 10-year analysis. Leukemia (2021) 35(2):440–53. doi: 10.1038/s41375-020-01111-2
75. Rea D, Cayuela J-M, Dulucq S, Etienne G. Molecular responses after switching from a standard-dose twice-daily nilotinib regimen to a reduced-dose once-daily schedule in patients with chronic myeloid leukemia: A real life observational study (NILO-RED). Blood (2017) 130(Supplement 1):318. doi: 10.1182/blood.V130.Suppl_1.318.318
76. Hiwase D, Tan P, D'Rozario J, Taper J, Powell A, Irving I, et al. Efficacy and safety of nilotinib 300 mg twice daily in patients with chronic myeloid leukemia in chronic phase who are intolerant to prior tyrosine kinase inhibitors: Results from the phase IIIb ENESTswift study. Leuk Res (2018) 67:109–15. doi: 10.1016/j.leukres.2018.02.013
77. Latagliata R, Attolico I, Trawinska MM, Capodanno I, Annunziata M, Elena C, et al. Bosutinib in the real-life treatment of chronic phase chronic myeloid leukemia (CML) patients aged < 65 years Resistant/Intolerant to frontline tyrosine-kynase inhibitors. Blood (2019) 134(Supplement_1):1649. doi: 10.1182/blood-2019-127029
78. Dorer DJ, Knickerbocker RK, Baccarani M, Cortes JE, Hochhaus A, Talpaz M, et al. Impact of dose intensity of ponatinib on selected adverse events: Multivariate analyses from a pooled population of clinical trial patients. Leuk Res (2016) 48:84–91. doi: 10.1016/j.leukres.2016.07.007
79. Cortes J, Apperley J, Lomaia E, Moiraghi B, Undurraga Sutton M, Pavlovsky C, et al. Ponatinib dose-ranging study in chronic-phase chronic myeloid leukemia: a randomized, open-label phase 2 clinical trial. Blood (2021) 138(21):2042–50. doi: 10.1182/blood.2021012082
80. Iurlo A, Cattaneo D, Orofino N, Bucelli C, Molica M, Breccia M. Low-dose ponatinib in intolerant chronic myeloid leukemia patients: A safe and effective option. Clin Drug Investig (2018) 38(5):475–6. doi: 10.1007/s40261-018-0623-7
81. Breccia M, Abruzzese E, Castagnetti F, Bonifacio M, Gangemi D, Sorà F, et al. Ponatinib as second-line treatment in chronic phase chronic myeloid leukemia patients in real-life practice. Ann Hematol (2018) 97(9):1577–80. doi: 10.1007/s00277-018-3337-2
82. Tefferi A. Upfront low-dose ponatinib (15 mg/day) for multi-TKI resistant chronic myeloid leukemia. Hematol Oncol (2018) 36(4):718–20. doi: 10.1002/hon.2517
83. Luciano L, Annunziata M, Attolico I, Di Raimondo F, Maggi A, Malato A, et al. The multi-tyrosine kinase inhibitor ponatinib for chronic myeloid leukemia: Real-world data. Eur J Haematol (2020) 105(1):3–15. doi: 10.1111/ejh.13408
84. Iurlo A, Cattaneo D, Malato A, Accurso V, Annunziata M, Gozzini A, et al. Low-dose ponatinib is a good option in chronic myeloid leukemia patients intolerant to previous TKIs. Am J Hematol (2020) 95(10):E260–e3. doi: 10.1002/ajh.25908
85. Sasaki K, Jabbour EJ, Ravandi F, Konopleva M, Borthakur G, Wierda WG, et al. The LEukemia artificial intelligence program (LEAP) in chronic myeloid leukemia in chronic phase: A model to improve patient outcomes. Am J Hematol (2021) 96(2):241–50. doi: 10.1002/ajh.26047
86. Jain P, Kantarjian HM, Ghorab A, Sasaki K, Jabbour EJ, Nogueras Gonzalez G, et al. Prognostic factors and survival outcomes in patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era: Cohort study of 477 patients. Cancer (2017) 123(22):4391–402. doi: 10.1002/cncr.30864
87. Maiti A, Franquiz MJ, Ravandi F, Cortes JE, Jabbour EJ, Sasaki K, et al. Venetoclax and BCR-ABL tyrosine kinase inhibitor combinations: Outcome in patients with Philadelphia chromosome-positive advanced myeloid leukemias. Acta Haematol (2020) 143(6):567–73. doi: 10.1159/000506346
88. Morita K, Kantarjian HM, Sasaki K, Issa GC, Jain N, Konopleva M, et al. Outcome of patients with chronic myeloid leukemia in lymphoid blastic phase and Philadelphia chromosome-positive acute lymphoblastic leukemia treated with hyper-CVAD and dasatinib. Cancer (2021) 127(15):2641–7. doi: 10.1002/cncr.33539
89. Saxena K, Jabbour E, Issa G, Sasaki K, Ravandi F, Maiti A, et al. Impact of frontline treatment approach on outcomes of myeloid blast phase CML. J Hematol Oncol (2021) 14(1):94. doi: 10.1186/s13045-021-01106-1
90. Morita K, Jabbour E, Ravandi F, Borthakur G, Khoury JD, Hu S, et al. Clinical outcomes of patients with chronic myeloid leukemia with concurrent core binding factor rearrangement and Philadelphia chromosome. Clin Lymphoma Myeloma Leuk (2021) 21(5):338–44. doi: 10.1016/j.clml.2020.12.025
91. Alfayez M, Richard-Carpentier G, Jabbour E, Vishnu P, Naqvi K, Sasaki K, et al. Sudden blastic transformation in treatment-free remission chronic myeloid leukaemia. Br J Haematol (2019) 187(4):543–5. doi: 10.1111/bjh.16245
92. Shoukier M, Borthakur G, Jabbour E, Ravandi F, Garcia-Manero G, Kadia T, et al. The effect of eltrombopag in managing thrombocytopenia associated with tyrosine kinase therapy in patients with chronic myeloid leukemia and myelofibrosis. Haematologica (2021) 106(11):2853–8. doi: 10.3324/haematol.2020.260125
93. Jain P, Kantarjian H, Boddu PC, Nogueras-González GM, Verstovsek S, Garcia-Manero G, et al. Analysis of cardiovascular and arteriothrombotic adverse events in chronic-phase CML patients after frontline TKIs. Blood Adv (2019) 3(6):851–61. doi: 10.1182/bloodadvances.2018025874
94. Sasaki K, Kantarjian HM, O'Brien S, Ravandi F, Konopleva M, Borthakur G, et al. Incidence of second malignancies in patients with chronic myeloid leukemia in the era of tyrosine kinase inhibitors. Int J Hematol (2019) 109(5):545–52. doi: 10.1007/s12185-019-02620-2
95. Aitken MJL, Benton CB, Issa GC, Sasaki K, Yilmaz M, Short NJ. Two cases of possible familial chronic myeloid leukemia in a family with extensive history of cancer. Acta Haematol (2021) 144(5):585–90. doi: 10.1159/000513925
Keywords: chronic myelogenous leukemia, imatinib, dasatinib, nilotinib, bosutinib, ponatinib, asciminib, dose modification
Citation: Yoshifuji K and Sasaki K (2022) Adverse events and dose modifications of tyrosine kinase inhibitors in chronic myelogenous leukemia. Front. Oncol. 12:1021662. doi: 10.3389/fonc.2022.1021662
Received: 17 August 2022; Accepted: 21 September 2022;
Published: 06 October 2022.
Edited by:
Chung Hoow Kok, University of Adelaide, AustraliaReviewed by:
Monica Bocchia, University of Siena, ItalyCopyright © 2022 Yoshifuji and Sasaki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Koji Sasaki, a3Nhc2FraTFAbWRhbmRlcnNvbi5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.