 Anna Collins
Anna Collins Lorna Gurren1
Lorna Gurren1 Jennifer Philip
Jennifer Philip
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 09 December 2022
Sec. Cancer Epidemiology and Prevention
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1003357
This article is part of the Research TopicEarly Palliative Care for Cancer PatientsView all 11 articles
Background: Despite robust evidence for the integration of early palliative care for patients with advanced cancer, many patients still access this approach to care late. Communication about the introduction of Early Palliative Care is an important skill of healthcare providers working in this setting. In the context of limited community understanding about palliative care, patients and their families may express fear or negative reactions to its early introduction. Health professionals may lack the confidence or skill to describe the role and benefits of early palliative care.
Aim: This study sought to explore clinicians’ perspectives on communication about referral to early palliative care, specifically identifying facilitators in undertaking this communication task.
Methods: An exploratory qualitative study set within a tertiary oncology service in Victoria, Australia. Semi-structured interviews were conducted with purposively sampled oncology clinicians exploring their perspectives on communication about referral to early palliative care. A reflexive thematic analysis was undertaken by two researchers, including both latent and semantic coding relevant to the research question. Reporting of the research was guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.
Results: Twelve oncology clinicians (58% female, with 67% > 15 years clinical experience) from medical oncology, surgical oncology, and haematology participated. The artful navigation of communication about early palliative care was characterised by the need for a ‘spiel’ involving the adoption of a series of strategies or ‘tactics’ when introducing this service. These themes included: 1) Using carefully selected and rehearsed language; 2) Framing in terms of symptom control; 3) Framing as additive to patient care; 4) Selling the service benefits of early palliative care; 5) Framing acceptance of referral as an altruistic act; and 6) Adopting a phased approach to delivering information about palliative care.
Implications: This study highlights the wide ranging and innovative communication strategies and skills required by health professionals to facilitate referral to early palliative care for cancer patients and their families. Future focus on upskilling clinicians around communication of this topic will be important to ensure successful implementation of models of early palliative care in routine cancer care.
Palliative care, concerned with the relief of physical, psychological, social, and spiritual suffering (1), is associated with improved clinical outcomes for patients and their families. Several meta-analyses demonstrate benefits for patients including greater health-related quality of life, reduced symptom burden, improved mood, and even prolonged survival (2–4). As such, there is growing impetus to integrate palliative care earlier in the cancer care pathway (5), reflected in the ASCO guideline that patients with advanced cancer receive dedicated palliative care services concurrent with anticancer treatment (6). Yet, late referral of cancer patients to palliative care specialists continues to be identified across international settings (7–9).
The realisation of early integration of palliative care is hampered, in part, by the unique communication barriers in this context (10, 11). Communication between patients and clinicians is a relational process underpinning all oncology and palliative care (11). Communication is broadly considered a core determinant of quality end-of-life care (12), and has ensuing implications for the health of the caregiver in bereavement (13). Despite population-level preferences of >70% who want to be informed about options regarding palliative care in the event of serious illness such as cancer (14), patients and their caregivers report inadequate communication about palliative care, including a tendency to use euphemistic or technical language that is difficult to understand (15, 16). Underlying such challenges in care are the clinician-perceived communication barriers related to the introduction of palliative care (17).
Among these clinician-reported communication barriers are a fear of diminishing patients’ morale (18), prognostic uncertainty (19, 20), perceived lack of adequate training for such discussions (21, 22), language and cultural factors (17), and difficulty judging the appropriate time for these discussions (23). These factors are compounded by variable levels of community understanding about palliative care (24), with perceptions of relevance only for those imminently dying (25), meaning patients may also be fearful or avoidant of discussing early palliative care (15). Thus the communication landscape in the setting of early palliative care is fraught, with communication paradoxically representing both a core component of and barrier to early integration with oncology (26).
While the introduction of ‘Early Palliative Care’ is an important skill of clinicians working in the advanced cancer setting, there has been limited empirical focus on communication facilitators or strategies to navigate this specific task (27). This task is one largely reliant on professionals who are not routinely trained in this specific aspect of care and whose core focus is a different specialty (22). In short, the referral communication task occurs ‘outside’ the field of palliative care where many have the training and skill sets to undertake such complex conversations.
While communication skills training for cancer care clinicians appears effective in improving support for patients in consultations such as when “difficult news” is delivered, uptake of such training is not yet widespread (26, 28–31). As such, the informal, self-adopted strategies of clinicians therefore remain particularly relevant. This study sought to explore oncology healthcare professionals’ perspectives on communication about referral to early palliative care, specifically identifying facilitators when undertaking this communication task.
This study employed an exploratory, qualitative, cross-sectional design using semi-structured interviews to elucidate oncology clinicians’ perspectives on communication of a palliative care referral. The epistemological position adopted by the researchers reflects social constructionism in which positivist notions of mapping reality in a decontextualized sense were rejected in favour of a view of knowledge that is circumscribed, in part, by social context (32). Methodological rigour was conceptualized in line with Lincoln and Guba favouring trustworthiness (transferability, dependability, credibility, confirmability) (33) over quantitative notions of reliability and validity (34). Activities to enhance trustworthiness included the following: AC and LG (both researchers in palliative care, and experienced in qualitative analysis) engaged in an ongoing process of reflexivity through co-analytic sessions during which varying interpretations of the data were questioned and challenged; an audit trail of the data analytic process was kept; and diverse participant perspectives were triangulated via a purposive sampling framework. The reporting of this research is consistent with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (35).
Ethics approval was provided by the Institutional Human Research Ethics Committee in St. Vincent’s Hospital Melbourne (LRR 070/15). Informed consent was obtained from each participant prior to study participation.
Participants were recruited through the oncology service of a tertiary hospital in the metropolitan centre of Melbourne, Victoria, Australia. A purposive sampling strategy was utilised to identify a group of clinicians currently providing care to patients with advanced cancer who routinely required referral to palliative care. Purposive sampling ensured that both male and female perspectives were included in the sample, in addition to representation across oncological specialties, and a range of clinical experience. No participants who were invited declined participation.
Data from participants were collected by one researcher (AC) using semi-structured interviews (n = 4) and focus groups (n = 8) of 40-65 minutes duration. These were conducted face-to-face in the hospital setting during 2018. Interviews were included to allow broader participation where purposively sampled participants were unavailable at the focus group times. Demographic information on participants was collected via a brief survey including gender, profession, and number of years’ clinical experience. The interview guide (Table 1) used for all data collection included an initial open exploration of clinicians’ experiences with referring patients to palliative care. Subsequent questions related to views of the timing of palliative care referral, communication about palliative care, and barriers and enablers relating palliative care referral. Supportive affirmations and direct probes were used to encourage dialogue and prompt further discussion around these topics of interest. In the present research, data on communication about palliative care were analysed and are presented herein, with other procedural and systemic barriers to palliative care referral to be published elsewhere.
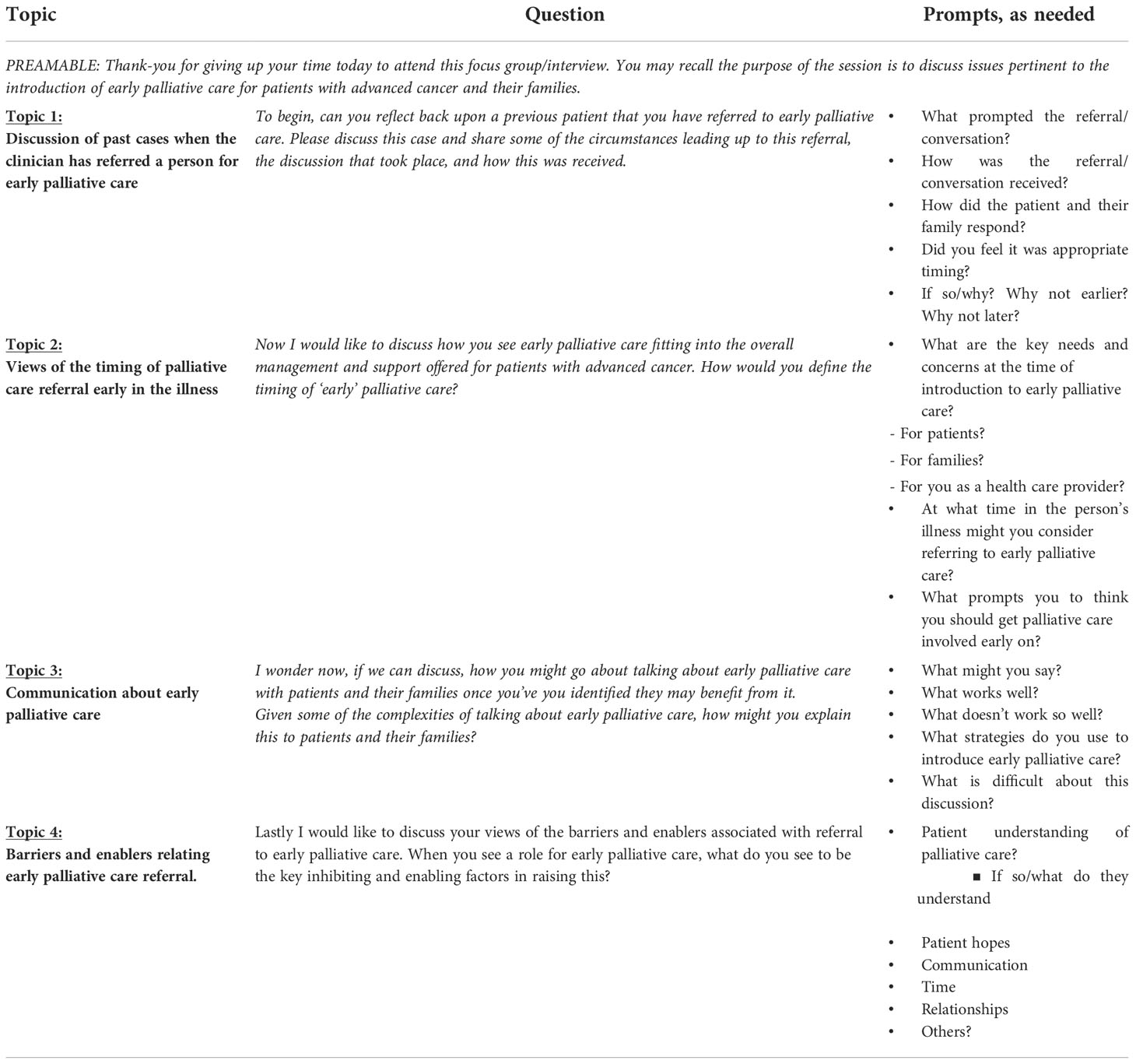
Table 1 Interview guide.
Audio recordings were transcribed verbatim, de-identified, before being subjected to analysis. The researchers adopted an inductive, reflexive approach to thematic analysis, using a combination of latent and semantic codes (36, 37). This reflexive process first involved initial data immersion and familiarization through repeated reading of the transcript and initial coding to identify latent content within the data. Subsequently, these codes were further abstracted to identify conceptual similarities and differences between codes with related codes then clustered together. Codes that were not coherent in the context of the meaningfulness across the dataset or irrelevant to the research aims were removed. Themes were constructed with the remaining related codes, and themes were then defined and refined to ensure appropriate wording. The write-up process then ensued with the use of illustrative quotations accompanying the themes presented. Trustworthiness in the analytic process was ensured through ongoing meetings between L.G and A.C, to discuss and justify the phrasing and content of codes, and the conceptual relations and organization between codes, themes, and subthemes. This process reflected peer debriefing, which can enhance the credibility of the analysis (33).
Twelve oncology clinicians (58% female) from medical oncology (n = 8), surgical oncology (n = 3) and haematology (n = 1) participated (Table 2). Eight (67%) of the participants reported over 15 years in practice, with 4 (33%) who reported less than 15 years’ experience.
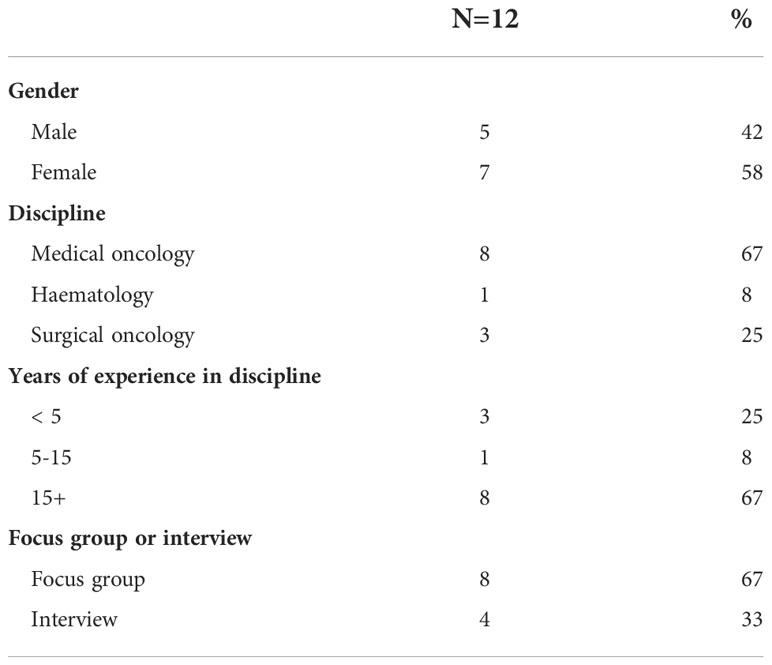
Table 2 Characteristics of participating health care professionals.
The artful navigation of communication about early palliative care was characterised by the need for a ‘spiel’ involving the adoption of a series of strategies or ‘tactics’ when introducing this service. Healthcare Professionals (HCPs) described the various techniques they carefully executed to skillfully introduce the concept of ‘early palliative care’ to patients with advanced cancer. These strategies reflected clinicians’ attention to the timing of the introduction, the quantity of information presented, and the specific content or framing of the message itself.
Six constructed themes represented healthcare professionals’ perspectives on these key strategies for navigating the communication landscape in palliative care referral, namely: Using Carefully Selected and Rehearsed Language; Framing Palliative Care in Terms of Symptom Control; Framing Palliative Care as Additive to patient care; Selling Service Benefits of Adding Palliative Care to Standard Oncology; Framing Palliative Care Referral Acceptance as an Altruistic Act; and Adopting a phased approach to delivering information about palliative care. Each theme is described in turn, with illustrative examples from the clinicians’ data.
HCPs in this study described their carefully selected and rehearsed language in consultations where they sought to introduce early palliative care to patients with advanced cancer. In particular, this related to clinicians’ perceived need to avoid the term ‘palliative care’ when discussing referral with patients:
“Mention the ‘palliative care’ word and you can see the face drop”.
The need to avoid the use of this term was described in relation to negative, patient-held connotations of this name, and specifically end-of-life connotations:
“As soon as you mention ‘palliative care’, people think you’re talking about end of life”.
A variety of strategies were proposed by HCPs for managing or circumventing this anticipated issue in the referral process. Commonly, clinicians described the strategy of first dispelling patient-held negative connotations before using the term. One HCP noted that they preface the use of this term with an instruction for the patient to disregard any end-of-life preconceptions they have about this service:
“I’ve been prefacing it by saying ‘I want you to ignore the terminal connotations of this referral’”
Another HCP described the strategy of delaying the use of the ‘palliative care’ term until late during the referral discussion, owing to the fact that patients’ families do not engage with the remainder of what the clinician has to say, once they hear the word:
“Often I don’t mention the word ‘palliative’ until … late … because I think that once a patient’s family hears the word ‘palliative’ they have an immediate impression. And [I find] they almost don’t hear the conversation, if you’re introducing it.”
In the absence of a different name for palliative care, some clinicians described favouring an approach to ‘get them in the door’ by introducing the concept of early palliative care using different terms. Some clinicians adopted the strategy of simply avoiding the term ‘palliative care’ completely:
“I don’t even mention palliative care.”
Related to this, several HCPs in this study raised the suggestion of changing the name of ‘palliative care’ in general:
“They should just change the name of ‘palliative care’ anyway.”
HCPs in the study described framing Palliative Care in terms of symptom control when introducing early palliative care with patients. The approach of directly aligning palliative care with symptom control involved characterizing this service as the best approach to manage the symptoms that the person is presently experiencing:
“I say, ‘Look, you’ve got symptoms. The best people to manage symptoms are the palliative care service.’ And I actually … frame it in the symptom management kind of way.”
Similarly, two participants noted that they specifically frame the palliative care service in terms of being the “pain team” or as specialists in pain control:
“I think I found it easy to introduce palliative care as the pain specialists.”
HCPs noted that they opt for the term ‘symptom control’ specifically due to the stigma associated with the term palliative care:
“I think you have to frame it [palliative care] as symptom control. I think it’s like a stigma.
The approach of framing palliative care as symptom control was therefore perceived by HCPs as an effective strategy, describing that it was helpful to avoid negative patient-held reactions:
“Because I frame it a bit differently, maybe I don’t see so many people reacting [negatively] so much now.”
However, one HCP in the sample noted that, when patients are asymptomatic, this makes it difficult to discuss PC:
“I guess I would have difficulty broaching, or more difficulty broaching pall(iative) care when a patient has no symptoms whatsoever from their cancer.”
Indeed, one HCP expressed skepticism with respect to the effectiveness of symptom control framing, noting that irrespective of the framing used, palliative care will hold different connotations for some patients:
“It’s easy to say ‘it’s just how you sell it’ but that’s not really true. I mean, yes, it’s how we’re going to get a group of people who can help us see if we can … to remove the pain or whatever it is. But it still sends a slightly different message to a lot of people.”
In introducing early palliative care, HCPs in the study described representing this concept as an additional layer of support to their care. One HCP described explaining to patients that it involves adding elements to their care, as opposed to withdrawing care:
“I sort of emphasize that [palliative care] is about adding extra things in. It’s not about taking things away”
In this context, this participant also noted a perceived obligation to reassure their patients that a referral for early palliative care does not mean discontinuation of their oncologic care:
“I feel I’m obliged to say ‘Just because you go to palliative care doesn’t mean I’m going to stop seeing you.’”
Moreover, HCPs raised their strategy of explicitly offering the patient a choice of which professionals are involved in their care, in this way framing the addition of palliative care to the team of professionals to work with the oncologist:
“I say, ‘Look, do you want me to be involved? Would you prefer me to involve somebody fresh and new who specializes in this area? Would you prefer us to work as a team?”
One HCP also noted that they frame palliative care professionals as ‘experts’ who are even ‘better’ than the referring clinician, being an added pair of eyes who can make better recommendations for care:
“I’ve found it’s good to sell it as them being experts even better than me. I’ll say ‘They are a lot better than me at this. I could prescribe something, but an extra pair of eyes, they can find key things, or suggest something better.’”
HCPs noted how they inform patients of the specific service benefits of adding palliative care to their standard oncologic care. One HCP described framing palliative care in terms of necessary services which could solve existing anxieties or concerns of patients and their family members:
“Usually what I’m talking about is services, and trying to identify things that family might already be worried is going to be a problem.”
Another HCP enumerated several specific service benefits of palliative care including the role to facilitate patients staying at home or out of the hospital, or if admitted, to align with a person’s desire to go home:
“I sort of sell the role of palliative care in discharge planning. The importance of not just going home, but being comfortable at home, being able to stay home for a significant amount of time.”
The availability of advice or care 24 hours a day and seven days a week was another specific service benefit described by HCPs as a strategy when describing early palliative care to patients. Palliative care was framed as the point of contact for patients and their family if they found themselves at home with concerns and needing help, in this away avoiding the emergency department:
“Another selling point I’ve used is, let’s say you’re at home and your symptoms get worse. It’s nice to have someone to call, people who can visit, rather than coming back to ED waiting for hours.”
The ‘pace’ of palliative care was also described by one HCP as a selling point used when discussing palliative care with patients, whereby they note that the service affords more time for care:
“I sell the pace. I say you won’t be rushed on the pall care ward.”
Several HCPs described framing early palliative care as a service needed by family members or even by themselves as their health professional when attempting to convince patients to accept an early referral to palliative care. Two HCPs noted that family members are eager to avail themselves for support:
“I think the partner is desperate for help…”
This HCP notes that such help for a patient’s partner may be provided by palliative care:
“[palliative care] is support for the partner.”
Similarly, HCPs on occasion noted that they inform patients that, by accepting an early referral to palliative care, they would help them as their doctor, knowing that they have support in the community who can contact them when needed:
“I often say that ‘it will be helpful for me if we organize this.’ I say it makes my life much easier if I know you’ve got this support in the community and they can contact me when they need to. And it would be helpful for me.”
HCPs discussed the benefits of raising palliative care early, when it is ‘not needed’, giving an opportunity to address misperceptions. At the same time, HCPs also perceived that patients with advanced cancer are presented with copious amounts of information at diagnosis. In this context, HCPs described difficulty in introducing the discussion of palliative care early following diagnosis, owing to the perception that it may be overwhelming for the patient:
“I personally find I just explained the cancer alone, even without getting treatment, that might be too overwhelming at first consultation. No doubt they need pal care, but personally I feel like maybe it might be too early [to discuss]”
One HCP noted that this is particularly true of younger cancer patients as, in their perspective, these patients find palliative care particularly difficult to understand at this initial stage:
“We’re increasingly seeing these younger patients with metastatic cancer … I just find bringing up pal care at [the initial] stage is even harder for them to comprehend.”
Related to this, another HCP described not introducing the topic of palliative care at diagnosis, but wait for the consultations that follow:
“Maybe within a time frame so get over the period where they’re just taking cancer as a word, digesting the treatment. And just have a person say within two or three weeks to find them”.
When introducing the conversation about early referral to palliative care, HCPs described the careful balancing act of the need for providing the patient with information about the service, while at the same time recognising that too much detail may also lead the patient to close the conversation. In response, some HCPs adopted the strategy of introducing the concept of palliative care in broad terms only:
“I start to maybe outline some of the things that pall care can offer, but maybe not in a lot of nitty-gritty details”.
Responding to this tension, some HCPs also described the strategy of delivering the introduction to palliative care in a piecemeal or ‘drip feed’ approach, involving a brief mention in one consultation and then following up at a later visit:
“I find it’s good just to sort of plant the seed [of palliative care] one time, follow it up the next time. And it might actually be two or three visits before you actually get them to say ‘yes’”.
With the implementation of early palliative care far from being standard of care across many international settings, communication around the task of referral is one key issue that requires further attention. This study sought to explore oncology clinicians’ perspectives on communication about palliative care, highlighting some key strategies adopted to underpin the content, framing, and timing of the communication about early referral. The ‘artful’ navigation of introducing early palliative care, characterised by the need to employ various strategies executed overtime to enable referral, point to the complexity of this clinical communication task. To ensure the successful implementation of models of early palliative care in routine cancer care, further empirical studies to distill the effectiveness of these strategies, and interventions to support clinicians around communication of this topic are needed.
This study has revealed strategies adopted by oncology clinicians who must frequently broach referral to early palliative care. These strategies were largely focused around referring clinicians’ perceived need for a rehearsed ‘spiel’ to introduce this concept in a manner perceived to be ‘gentler’, ‘easier’ or more palatable for patients. This involved carefully selected words and framing of palliative care: for symptom control; as experts – mostly in pain management; to help loved ones; to help the treating clinician; to add to the care team; to access specific services or tasks; to support patient hopes to go home; to support a focus on quality of life. Interestingly, some of this framing is also consistent with the palliative care discourse which has seen messaging used by palliative care professionals focused on actions (e.g. availability, family care, wellbeing), values (e.g. individualized care – ‘you matter’) or alignment with immediate needs (e.g. support to go home), rather than identity (11, 38).
The approach used by clinicians also involved considered timing as to when to optimally raise this discussion – timing not necessarily defined based upon the best evidence but instead framed around enhancing patient acceptability through a phased, ‘drip-fed’ approach. This has resonance with a stepwise questioning strategy observed in other studies, allowing opportunities for the person to engage in difficult talk without explicitly inviting such talk or placing patients in this potentially delicate position (39).
The finding that clinicians avoid using the term ‘palliative care’ is consistent with prior literature indicating stigma associated with this term (10, 15, 16, 40) and that many referring clinicians and patients dislike and opt to avoid this term (15), frequently in favour of re-branding as ‘supportive care’ (41–45). In this study some clinicians also broadly suggested that the name of the discipline should be changed. The extant debate in the literature regarding the need to re-name ‘palliative care’ has seen a spectrum of perspectives. This includes proponents, often from referring specialities, who argue that a name change is necessary due to the stigma associated with the name.
Conversely, opponents, often from palliative care, point to the risk of a ‘euphemistic treadmill’ (46), citing the limited (or short-term) increase in palliative care referral following a name change in a given setting (47) or arguing that the limitations of the term are a cultural artefact and hence would not be readily ameliorated by a name change (48, 49). Indeed surveys of palliative care clinicians suggest that although many recognise patients perceive the term “palliative care” negatively, few believe a name change to supportive care would encourage early referral, and <21% support renaming the specialty (7, 50). Others point to the opportunities for a re-branding of message which conveys the benefits, re-focuses the message, and builds the service accordingly, while still maintaining the name, palliative care (51–53). In any case, the results of this study highlight the complexity of palliative care discourse and potential for mixed messaging underpinning ‘early palliative care’ (38, 49, 51). Further, the results support the need for greater clarity of message within the communication underpinning referral to early palliative care, explaining the intended role and service offerings to health professionals and patients (10).
While clinicians spoke of using different terms and strategies to avoid patient distress while enabling palliative care referral, it is possible that they are also seeking to avoid their own discomfort. While there is little literature in the area, the use of euphemisms, different names, and discussion of activities of palliative care such as pain relief enable the patient and the physician to avoid talking of end-of-life care and death (15). It is possible that the use of this avoidant strategy serves to not only protect patients from distress, but also to lessen their own discomfort in discussing palliative care and its implications. Exploring this possibility and undertaking to directly evaluate clinicians’ distress in performing an early referral may provide opportunities for redress. Importantly, these communication aspects, as a seemingly major barrier, will be crucial to address in any future implementation of systematic screening for palliative care referral. The finding in this study of framing palliative care referral acceptance as an altruistic act is consistent with the literature on oncology trial participation. Such research has demonstrated that altruism is a frequent motivation for clinical trial participation (54), with patients demonstrating high agreement for scale items such as ‘contributing to research that can help others in the future’ as a motivation for their participation. However, cancer patients are not monolithic in these altruistic motivations, with patients with a poorer prognosis demonstrating a lesser altruistic motivation for research participation than for those with a better prognosis (55). There is a dearth of literature exploring the role of altruism in palliative care referral acceptance among cancer patients. However, it is conceivable that the framing of referral acceptance in terms of supporting others (e.g., family, primary clinician) may capitalize on altruistic motivations among cancer cohorts and thereby facilitate referral. Further research is necessary to investigate altruism as a motivator of palliative care referral acceptance in this cohort. Potential ethical implications of this framing, for example in terms of coercion, must also be explored.
When exploring the nature of communication in healthcare, observational research methods such as conversation analysis offer an alternative approach which may elucidate different issues. Additionally, triangulation of the findings with a patient sample would further add to the interpretation, which in this analysis, was limited to the clinician’s perspectives of how they communicate about early referral to palliative care. Similarly, other referring clinicians such as General Practitioners working in community settings may provide additional important perspectives around this task. Finally, the prior communication skills training of clinicians participating in this study was not recorded. Such training has been demonstrated to influence cancer care consultations and would likely enhance confidence and practices in this important task of introducing early palliative care. Nonetheless, this well-designed and analysed qualitative study, albeit small, provides new insights into the strategies used by clinicians in this communication task which can form the basis of further study, highlight the role for formal communication skills training, and support other clinicians seeking peer guidance on introducing early palliative care.
This study reveals the complex task of communicating about early referral to palliative care and the communication skills required by health professionals to ‘artfully’ navigate this task. Oncology clinicians conveyed their self-adopted strategies which underpinned their ‘spiel’ to ease the introduction of early palliative care for patients and their families, and perhaps for the clinicians themselves. This was characterised by careful rehearsed language, framing and attention to the timing of the introduction- none of which was necessarily straightforward or overt. While there are apparent opportunities and also limitations of such an approach, the attention given to this clinical task equivalent to a “breaking bad news” conversation gives weight to its importance. The future successful implementation of models of early palliative care integration in oncology will require support for communication skills training specific to introducing early referral to palliative care.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by St Vincent’s Hospital Melbourne Human Research Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
AC was the lead investigator, obtained the study funding, was responsible for the study conduct, had access to the data, and co-authored the first draft. AC, LG, and OW were involved in the data analysis. All authors contributed to the study protocol, interpretation and, contributed to the manuscript. All authors contributed to the article and approved the submitted version.
AC is funded by an Emerging Leadership Grant awarded by the National Health and Medical Research Council (NHMRC GNT1173054).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The contents of the published material are solely the responsibility of the individual authors and do not reflect the views of the NHMRC, who had no role in the study conduct or interpretation of the results.
2. Hoerger M, Wayser GR, Schwing G, Suzuki A, Perry LM. Impact of interdisciplinary outpatient specialty palliative care on survival and quality of life in adults with advanced cancer: a meta-analysis of randomized controlled trials. Ann Behav Med (2019) 53:674–85. doi: 10.1093/abm/kay077
3. Kavalieratos D, Corbelli J, Zhang D, Dionne-Odom JN, Ernecoff NC, Hanmer J, et al. Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA (2016) 316:2104–14. doi: 10.1001/jama.2016.16840
4. Kassianos AP, Ioannou M, Koutsantoni M, Charalambous H. The impact of specialized palliative care on cancer patients’ health-related quality of life: A systematic review and meta-analysis. Supportive Care Cancer. (2018) 26:61–79. doi: 10.1007/s00520-017-3895-1
5. Hui D, Heung Y, Bruera E. Timely palliative care: Personalizing the process of referral. Cancers (2022) 14:1047. doi: 10.3390/cancers14041047
6. Ferrell BR, Temel JS, Temin S, Alesi ER, Balboni TA, Basch EM, et al. Integration of palliative care into standard oncology care: American society of clinical oncology clinical practice guideline update. J Clin Oncol (2017) 35:96–112. doi: 10.1200/JCO.2016.70.1474
7. Sorensen A, Wentlandt K, Le LW, Swami N, Hannon B, Rodin G, et al. Practices and opinions of specialized palliative care physicians regarding early palliative care in oncology. Support Care Cancer. (2020) 28:877–85. doi: 10.1007/s00520-019-04876-0
8. Jordan RI, Allsop MJ, ElMokhallalati Y, Jackson CE, Edwards HL, Chapman EJ, et al. Duration of palliative care before death in international routine practice: A systematic review and meta-analysis. BMC Med (2020) 18:1–25. doi: 10.1186/s12916-020-01829-x
9. Collins A, Sundararajan V, Burchell J, Millar J, McLachlan S-A, Krishnasamy M, et al. Transition points for the routine integration of palliative care in patients with advanced cancer. J Pain symptom management. (2018) 56:185–94. doi: 10.1016/j.jpainsymman.2018.03.022
10. Sarradon-Eck A, Besle S, Troian J, Capodano G, Mancini J. Understanding the barriers to introducing early palliative care for patients with advanced cancer: a qualitative study. J palliative Med (2019) 22:508–16. doi: 10.1089/jpm.2018.0338
11. Back AL. Patient-clinician communication issues in palliative care for patients with advanced cancer. J Clin Oncol (2020) 38:866–76. doi: 10.1200/JCO.19.00128
12. Trice ED, Prigerson HG. Communication in end-stage cancer: Review of the literature and future research. J Health Communication. (2009) 14:95–108. doi: 10.1080/10810730902806786
13. Wright AA, Zhang B, Ray A, Mack JW, Trice E, Balboni T, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. Jama (2008) 300:1665–73. doi: 10.1001/jama.300.14.1665
14. De Vleminck A, Pardon K, Roelands M, Houttekier D, Van den Block L. Vander stichele r and deliens l. information preferences of the general population when faced with life-limiting illness. Eur J Public Health (2014) 2014:cku158. doi: 10.1093/eurpub/cku158
15. Collins A, McLachlan S-A, Philip J. Communication about palliative care: A phenomenological study exploring patient views and responses to its discussion. Palliative Med (2018) 32:133–42. doi: 10.1177/0269216317735247
16. Collins A, McLachlan S-A, Philip J. How should we talk about palliative care, death and dying? a qualitative study exploring perspectives from caregivers of people with advanced cancer. Palliative Med (2018) 32:861–9. doi: 10.1177/0269216317746584
17. Horlait M, Chambaere K, Pardon K, Deliens L, Van Belle S. What are the barriers faced by medical oncologists in initiating discussion of palliative care? a qualitative study in Flanders, Belgium. J Supportive Care Cancer (2016) 24:3873–81. doi: 10.1007/s00520-016-3211-5
18. Kelly B, Varghese FT, Burnett P, Turner J, Robertson M, Kelly P, et al. General practitioners’ experiences of the psychological aspects in the care of a dying patient. Palliat Support Care (2008) 6:125–31. doi: 10.1017/S1478951508000205
19. Hancock K, Clayton JM, Parker SM, Wal der S, Butow PN, Carrick S, et al. Truth-telling in discussing prognosis in advanced life-limiting illnesses: A systematic review. Palliat Med (2007) 21:507–17. doi: 10.1177/0269216307080823
20. Hancock K, Clayton JM, Parker SM, Walder S, Butow PN, Carrick S, et al. Discrepant perceptions about end-of-life communication: a systematic review. J Pain symptom management. (2007) 34:190–200. doi: 10.1016/j.jpainsymman.2006.11.009
21. Suwanabol PA, Reichstein AC, Suzer-Gurtekin ZT, Forman J, Silveira MJ, Mody L, et al. Surgeons’ perceived barriers to palliative and end-of-Life care: A mixed methods study of a surgical society. J Palliat Med (2018) 21:780–8. doi: 10.1089/jpm.2017.0470
22. Horlait M, Van Belle S, Leys M. Are future medical oncologists sufficiently trained to communicate about palliative care? the medical oncology curriculum in Flanders, Belgium. J Acta Clinica Belgica (2017) 72:18–325. doi: 10.1080/17843286.2016.1275377
23. Almack K, Cox K, Moghaddam N, Pollock K, Seymour J. After you: conversations between patients and healthcare professionals in planning for end of life care. BMC Palliative Care (2012) 11:15. doi: 10.1186/1472-684X-11-15
24. Collins A, McLachlan S-A, Philip J. Community knowledge of and attitudes to palliative care: A descriptive study. Palliative Med (2020) 34:245–52. doi: 10.1177/0269216319888371
25. Collins A, McLachlan S-A, Philip J. Initial perceptions of palliative care: An exploratory qualitative study of patients with advanced cancer and their family caregivers. Palliative Med (2017) 31:825–32. doi: 10.1177/0269216317696420
26. Harnischfeger N, Rath HM, Ullrich A, Alt-Epping B, Letsch A, Thuss-Patience P, et al. Evaluation of a communication skills training to facilitate addressing palliative care related topics in advanced cancer patients: study protocol of a multicenter randomized controlled trial (PALLI-KOM). BMC Palliative Care (2020) 19:1–8. doi: 10.1186/s12904-020-00568-3
27. Beernaert K, Deliens L, De Vleminck A, Devroey D, Pardon K, Van den Block L, et al. Early identification of palliative care needs by family physicians: A qualitative study of barriers and facilitators from the perspective of family physicians, community nurses, and patients. Palliat Med (2014) 28:480–90. doi: 10.1177/0269216314522318
28. Back AL, Arnold RM, Baile WF, Fryer-Edwards KA, Alexander SC, Barley GE, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Internal Med (2007) 167:453–60. doi: 10.1001/archinte.167.5.453
29. Goelz T, Wuensch A, Stubenrauch S, Ihorst G, de Figueiredo M, Bertz H, et al. Specific training program improves oncologists’ palliative care communication skills in a randomized controlled trial. J Clin Oncol (2011) 29:3402–7. doi: 10.1200/JCO.2010.31.6372
30. Clayton JM, Butow PN, Waters A, Laidsaar-Powell RC, O’Brien A, Boyle F, et al. Evaluation of a novel individualised communication-skills training intervention to improve doctors’ confidence and skills in end-of-life communication. Palliative Med (2013) 27:236–43. doi: 10.1177/0269216312449683
31. Moore PM, Rivera S, Bravo-Soto GA, Olivares C, Lawrie TA. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev (2018) 7:Cd003751. doi: 10.1002/14651858.CD003751.pub4
32. Gergen KJ. The social constructionist movement in modern psychology. Am Psychol (1985) 40:266–75. doi: 10.1037/0003-066X.40.3.266
34. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: Striving to meet the trustworthiness criteria. Int J Qual Methods (2017) 16:1609406917733847. doi: 10.1177/1609406917733847
35. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
36. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
37. Braun V, Clarke V. Can I use TA? should I use TA? should I not use TA? comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Counselling Psychother Res (2021) 21:37–47. doi: 10.1002/capr.12360
38. Reigada C, Arantzamendi M, Centeno CJ. Palliative care in its own discourse: a focused ethnography of professional messaging in palliative care. BMC Palliative Care. (2020) 19:1–10. Bpc. doi: 10.1186/s12904-020-00582-5
39. Pino M, Parry R. Talking about death and dying: Findings and insights from five conversation analytic studies. J Patient Educ Counseling. (2019) 102:185–7. doi: 10.1016/j.pec.2019.01.011
40. Cherny N. Stigma associated With’’Palliative care”: Getting around it or getting over it. Cancer (2009) 115:3034–4. doi: 10.1002/cncr.24212
41. Dai Y-X, Chen T-J, Lin M-H. Branding palliative care units by avoiding the terms “Palliative” and “Hospice” a nationwide study in Taiwan. INQUIRY: J Health Care Organization Provision Financing. (2017) 54:0046958016686449. doi: 10.1177/0046958016686449
42. Dalal S, Palla S, Hui D, Nguyen L, Chacko R, Li Z, et al. Association between a name change from palliative to supportive care and the timing of patient referrals at a comprehensive cancer center. oncologist. (2011) 16:105–11. doi: 10.1634/theoncologist.2010-0161
43. Fadul N, Elsayem A, Palmer JL, Del Fabbro E, Swint K, Li Z, et al. Supportive versus palliative care: What’s in a name? Cancer (2009) 115:2013–21. doi: 10.1002/cncr.24206
44. Katz NM. The term “supportive care” is preferable to “palliative care” for consults in the cardiothoracic intensive care unit. J Thorac Cardiovasc surgery. (2018) 155(5):2030–2031. doi: 10.1016/j.jtcvs.2017.12.117
45. Maciasz R, Arnold R, Chu E, Park SY, White D, Vater L, et al. Does it matter what you call it? a randomized trial of language used to describe palliative care services. Supportive Care cancer. (2013) 21:3411–9. doi: 10.1007/s00520-013-1919-z
47. Ryan S, Wong J, Chow R, Zimmermann C. Evolving definitions of palliative care: Upstream migration or confusion? Curr Treat options Oncol (2020) 21:20. doi: 10.1007/s11864-020-0716-4
48. Milne D, Jefford M, Schofield P, Aranda S. Appropriate, timely referral to palliative care services: A name change will not help. J Clin Oncol (2013) 31:2055–5. doi: 10.1200/JCO.2012.48.4493
49. Pastrana T, Jünger S, Ostgathe C, Elsner F, Radbruch L. A matter of definition–key elements identified in a discourse analysis of definitions of palliative care. Palliative Med (2008) 22:222–32. doi: 10.1177/0269216308089803
50. Zambrano SC, Centeno C, Larkin PJ, Eychmüller S. Using the term “Palliative care”: International survey of how palliative care researchers and academics perceive the term “Palliative care”. J Palliat Med (2020) 23:184–91. doi: 10.1089/jpm.2019.0068
51. Berry LL, Castellani R, Stuart B. The branding of palliative care. J Oncol Practice. (2016) 12:48–50. doi: 10.1200/JOP.2015.008656
52. Collins A, McLachlan S-A, Philip JJ. Community knowledge of and attitudes to palliative care: A descriptive study. Palliative Medicine (2020) 34:245–52. PM. doi: 10.1177/0269216319888371
53. Boyd K, Moine S, Murray SA, Bowman D, Brun N. Should palliative care be rebranded? BMJ (2019) 364:I881. doi: 10.1136/bmj.l881
54. Godskesen T, Hansson MG, Nygren P, Nordin K, Kihlbom U. Hope for a cure and altruism are the main motives behind participation in phase 3 clinical cancer trials. Eur J Cancer Care (2015) 24:133–41. doi: 10.1111/ecc.12184
Keywords: early palliative care, oncology, referral, communication, qualitative study
Citation: Collins A, Gurren L, McLachlan S-A, Wawryk O and Philip J (2022) Communication about early palliative care: A qualitative study of oncology providers’ perspectives of navigating the artful introduction to the palliative care team. Front. Oncol. 12:1003357. doi: 10.3389/fonc.2022.1003357
Received: 26 July 2022; Accepted: 04 November 2022;
Published: 09 December 2022.
Edited by:
Marco Maltoni, University of Bologna, ItalyReviewed by:
Leonardo Potenza, University of Modena and Reggio Emilia, ItalyCopyright © 2022 Collins, Gurren, McLachlan, Wawryk and Philip. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Collins, YW5uYS5jb2xsaW5zQHN2aGEub3JnLmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.