
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 02 December 2021
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.790458
This article is part of the Research Topic Quality of Care of Glioma Patients View all 16 articles
 Johannes Kasper1*
Johannes Kasper1* Tim Wende1
Tim Wende1 Michael Karl Fehrenbach1
Michael Karl Fehrenbach1 Florian Wilhelmy1Katja Jähne1Clara Frydrychowicz2Gordian Prasse3Jürgen Meixensberger1Felix Arlt1
Florian Wilhelmy1Katja Jähne1Clara Frydrychowicz2Gordian Prasse3Jürgen Meixensberger1Felix Arlt1Background: IDH-wild-type glioblastoma (GBM) is the most frequent brain-derived malignancy. Despite intense research efforts, it is still associated with a very poor prognosis. Several parameters were identified as prognostic, including general physical performance. In neuro-oncology (NO), special emphasis is put on focal deficits and cognitive (dys-)function. The Neurologic Assessment in Neuro-Oncology (NANO) scale was proposed in order to standardize the assessment of neurological performance in NO. This study evaluated whether NANO scale assessment provides prognostic information in a standardized collective of GBM patients.
Methods: The records of all GBM patients treated between 2014 and 2019 at our facility were retrospectively screened. Inclusion criteria were age over 18 years, at least 3 months postoperative follow-up, and preoperative and postoperative cranial magnetic resonance imaging. The NANO scale was assessed pre- and postoperatively as well as at 3 months follow-up. Univariate and multivariate survival analyses were carried to investigate the prognostic value.
Results: One hundred and thirty-one patients were included. In univariate analysis, poor postoperative neurological performance (HR 1.13, p = 0.004), poor neurological performance at 3 months postsurgery (HR 1.37, p < 0.001), and neurological deterioration during follow-up (HR 1.38, p < 0.001), all assessed via the NANO scale, were associated with shorter survival. In multivariate analysis including other prognostic factors such as the extent of resection, adjuvant treatment regimen, or age, NANO scale assessment at 3 months postoperative follow-up was independently associated with survival prediction (HR 1.36, p < 0.001). The optimal NANO scale cutoff for patient stratification was 3.5 points.
Conclusion: Neurological performance assessment employing the NANO scale might provide prognostic information in patients suffering from GBM.
IDH-wild-type glioblastoma (GBM) is the most common brain-derived malignancy. Due to its high mitotic activity, neoangiogenesis, and highly infiltrative behavior, it is classified as WHO grade four (1). GBM accounts for 14.5% of all primary brain tumors and is more commonly diagnosed in men. Moreover, the median age at first diagnosis is 65 years and the 12-month survival is poor with around 42.8% (2). Standard therapy includes maximum safe resection and adjuvant radiochemotherapy up to 60.0 Gy with concomitant temozolomide, followed by 6 cycles of temozolomide alone (3, 4). Several parameters were identified as influential on patient survival, including tumor location (5), extent of resection (6), age at date of diagnosis (7), O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation (8), and clinical performance (4). Here, the Karnofsky Performance Score (KPS) is commonly used to assess the overall physical status as well as to monitor possible tumor progression via a decrease of clinical performance (9, 10). Moreover, poor or worsened overall neurological performance (11–14) and isolated motor or language deficits might be associated with decreased overall survival (15, 16). In order to address this rising evidence and to standardize the evaluation of neurological performance, the Neurologic Assessment in Neuro-Oncology (NANO) scale was created (17). It was shown to predict overall survival in GBM patients more precisely than comparable performance scales (18, 19). However, previous works are limited by inconsistent therapy regimen within the investigated patient cohorts. Hence, this study was designed to evaluate the independent, prognostic value of neurological performance assessed via the NANO scale at different points of follow-up when the abovementioned clinical and radiological factors are considered within a standardized GBM patient collective.
Data collection and analysis were approved by the Ethical Committee of the Medical Faculty, University of Leipzig (No. 144/08-ek). The database of Leipzig University Hospital was searched for all patients with new diagnosis of IDH-wild-type glioblastoma between 2014 and 2019. Inclusion criteria were age over 18 years, at least 3 months postoperative follow-up, and preoperative and postoperative cranial magnetic resonance imaging within 72 h after surgery. Due to the selection criteria, patients with an overall survival less than 3 months or further therapy at another facility were excluded. All cases were discussed in a weekly, interdisciplinary tumor board and therapy regimen was determined based on current EANO guidelines for glioma therapy (20, 21).
Medical records were analyzed for age at date of diagnosis, sex, and adjuvant therapy regimen. The date of diagnosis was set as the date of surgery after neuropathological proof of glioblastoma. Histopathological diagnosis and immunohistochemical status were extracted from neuropathology reports. IDH-mutation status and MGMT promoter methylation of all GBM samples were determined using immunohistochemistry and pyrosequencing or nucleic acid amplification followed by pyrosequencing. According to Quillien et al., the MGMT promoter methylation status was dichotomized into positive (≥12%), negative (<12%), or unknown (22).
Overall survival (OS) was defined as the time between the date of neurosurgery and the date of death. The date of death, if not provided by our hospital database, was collected from the Leipzig Cancer Registry. Dates were assessed on May 31, 2021. If death did not occur by then or if patients were lost to follow-up, the date of last contact to our department was integrated into statistical analysis as censored value.
Tumor location and extent of resection (EOR) were retrospectively determined revising perioperative MRI T1 sequences with and without contrast. Volumetric assessment was manually carried out employing the iPlan Cranial software (version 3.0.5, Brainlab AG, Munich, Germany). If a needle biopsy was performed, EOR was set as 0%.
All patients appointed to our department are examined based on a standardized procedure including general symptoms, cranial nerve status, sensorimotor deficits, and other focal symptoms, such as aphasia or behavior. Findings are routinely documented within a physician report template. The NANO scale was then retrospectively assessed from physician reports at the time of hospital admission, at the time of discharge, and 3 months postsurgery employing the NANO scale as proposed by Nayak et al. (17). Gait, strength, ataxia of upper extremities, sensation, visual fields, facial strength, language, level of consciousness, and behavior sum up to a maximum of 23 points. High-scale values represent impaired neurological performances. NANO scale changes were calculated by subtracting preoperative scale values from postoperative values (NANO difference 1 or time point 1) or postoperative values from values assessed at 3 months postoperative follow-up (NANO difference 2 or time point 2). NANO scale differences below or equal to 0 represent a stable or improved neurological performance and vice versa. In case of missing data, the corresponding neurological deficit was defined as absent and set as 0 points within NANO scale calculation.
Statistical analysis was carried out using SPSS statistics software version 24.0.0.2 (IBM, Armonk, NY, USA). First, the assessed parameters were applied as continuous variables and analyzed via univariate Cox regression. Time-dependent receiver operator characteristic (ROC) analysis was then performed for NANO scale values with p-values below 0.2 from Cox regression, and the optimal cutoff point was defined as the value that maximizes the Youden’s index (parameter value for which sensitivity + specificity − 1 is maximal). After NANO scale values were dichotomized according to cutoff values, a second univariate analysis was carried out employing the Kaplan–Meier estimate. Finally, all continuous variables with p-values below 0.2 in univariate Cox regression were utilized for a multivariate analysis via proportional hazard Cox regression in order to investigate independent statistical relevance. Non-parametric parameters were compared with Mann–Whitney U test.
Survival rates from Kaplan–Meier analysis are given with standard deviation, and statistical significance was calculated via log-rank testing. Hazard ratios (HR) are provided with 95% confidence intervals (95 CI). p-values below 0.05 were considered statistically significant.
Baseline data are presented in Table 1. Within the study period, 227 patients were newly diagnosed with IDH-wild-type GBM and 131 met the inclusion criteria for the study (a flowchart is shown in Supplementary Figure 1). Concerning average age and sex ratio, the cohort is comparable to larger studies (2). The average preoperative NANO scale value was 3.3 ± 2.5 and slightly increased up to 3.8 ± 2.7 at 3 months postsurgery, but statistical significance was not reached (p = 0.09 by Mann–Whitney U test).
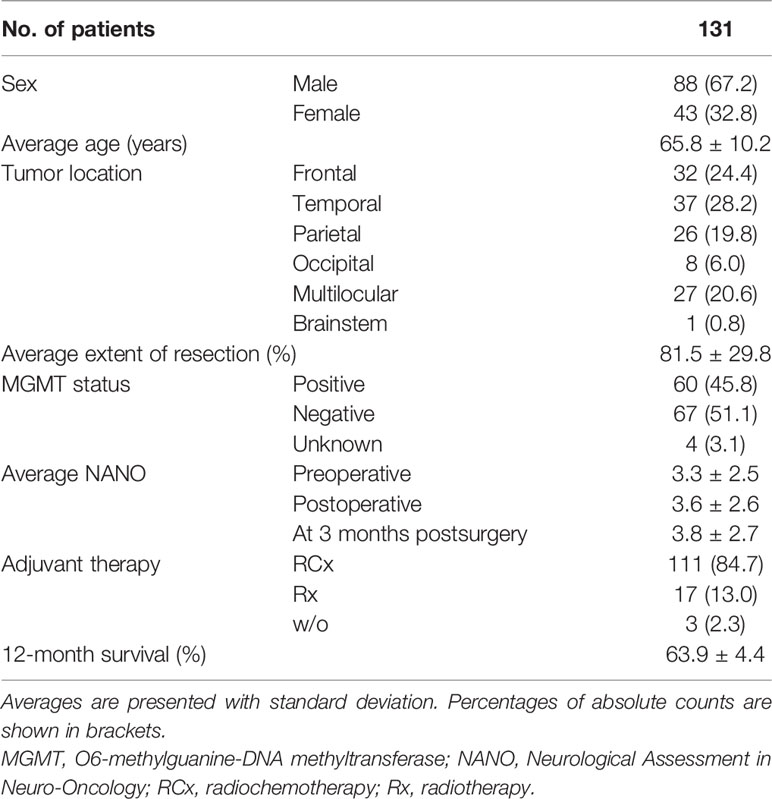
Table 1 Baseline data.
In univariate Cox regression (see Supplementary Table 1), low patient age (HR 1.03, p = 0.028), high extent of resection (HR 0.87, p < 0.001), adjuvant radiochemotherapy (HR 0.27, p < 0.001), positive MGMT promoter methylation status (HR 0.46, p = 0.002), and tumor location (HR 0.42, p = 0.001) were significantly associated with prolonged survival. Also, a low postoperative NANO scale value (HR 1.13, p = 0.004), low NANO scale values at 3 months postsurgery (HR 1.37, p < 0.001), and the difference of NANO scale values after 3 months postoperative follow-up and postoperatively (NANO time point 2, HR 1.38, p < 0.001) had a significant influence on overall survival. Preoperative NANO values and the difference of post- and preoperative NANO scale values were not associated with patient survival.
A further analysis via ROC and Youden’s index calculation revealed 3.5 scale points as the optimal cutoff for both postoperative NANO scale values (AUC 0.706) and NANO scale values at 3 months postoperative follow-up (AUC 0.827). For NANO time point 2, the cutoff was set at 0, with values ≤0 representing stable or increased neurological performance and values >0 representing decreased neurological performance, respectively. Corresponding data were hence dichotomized and employed into Kaplan–Meier analysis, presented in Figure 1. Here, patients with NANO scale values below 3.5 points at 3 months postoperative follow-up (12-month survival 85.0 ± 4.4% vs. 38.7 ± 6.9%, p < 0.001) as well as patients with stable or increased neurological performance (12-month survival 76.2 ± 4.4% vs. 23.1 ± 8.6%, p < 0.001) had a significantly prolonged overall survival. Postoperative NANO scale assessment was associated with prolonged survival but did not reach significance (12-month survival 77.1 ± 5.0% vs. 47.1 ± 7.3%, p = 0.056).
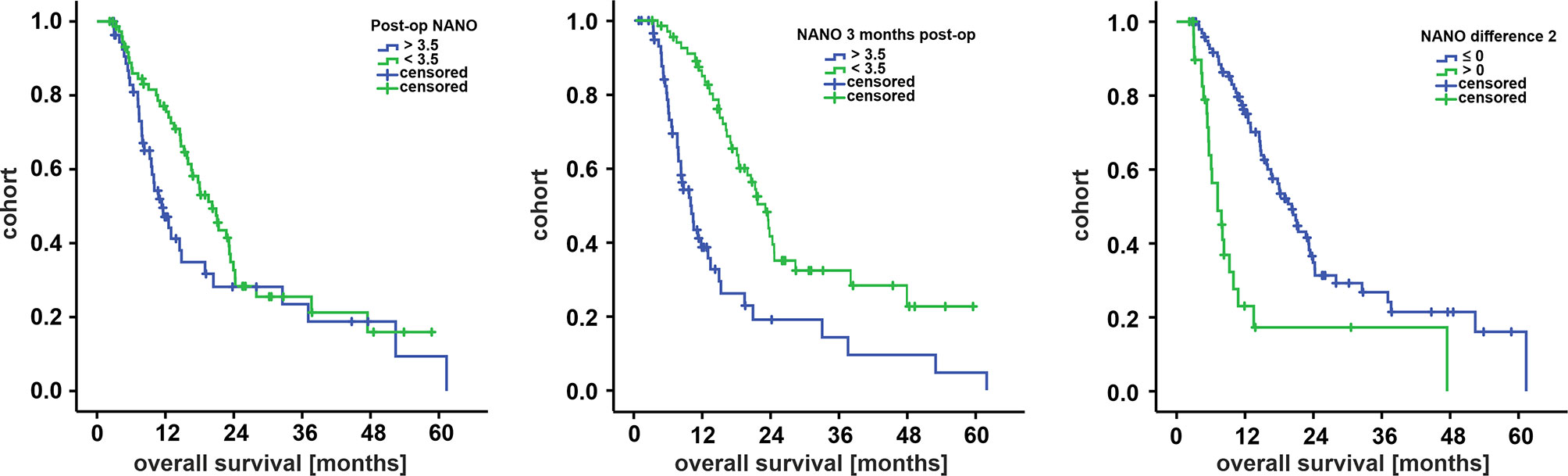
Figure 1 Survival curves for subcohorts by Kaplan–Meier analysis for postoperative NANO scale (left), NANO scale at 3 months follow-up (middle), and NANO scale difference of postoperative values and values at 3 months follow-up (right). Cutoffs for the first two diagrams were determined via ROC analysis. NANO difference 2 was dichotomized in stable/increased (≤0) or worsened (>0) neurological performance at 3 months follow-up compared with postoperative values. NANO, Neurologic Assessment in Neuro-Oncology.
Finally, a multivariate Cox regression (Table 2) revealed that the extent of resection, adjuvant therapy regimen, MGMT promoter methylation status, and NANO scale assessment at 3 months postoperative follow-up (HR 1.36, p < 0.001) were independently associated with increased overall survival.
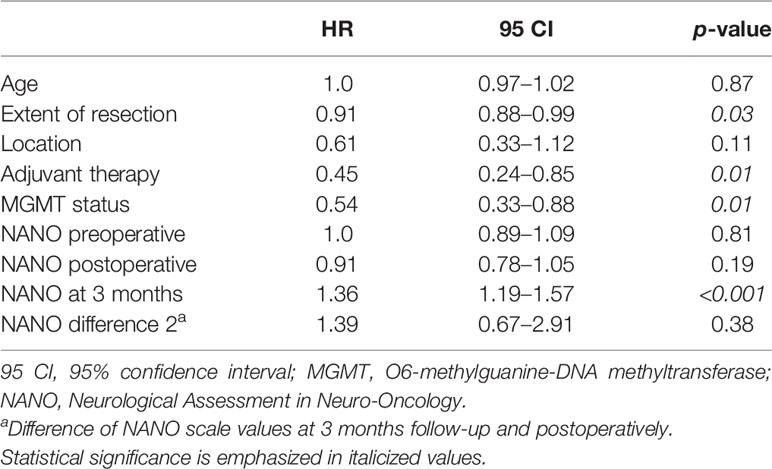
Table 2 Multivariate Cox regression.
In this retrospective study with 131 IDH-wild-type glioblastoma patients, neurological performance, assessed using the NANO scale, was significantly associated with overall survival in univariate analysis (postoperative, at 3 months postoperative follow-up) and in multivariate survival prediction (at 3 months postoperative follow-up). The optimal NANO scale cutoff for cohort stratification in our series was defined with ROC analysis at 3.5 points. Moreover, patients with NANO scale progression (worsened neurological performance) at 3 months postsurgery suffered from significant shorter OS compared with the corresponding subgroup. It is important to note that due to inclusion criteria (only patients with more than 3 months postoperative follow-up), our cohort mainly consists of “good performers,” reflected by prolonged survival when compared with larger studies. The issue is discussed in detail in the succeeding paragraphs.
The influence of general fitness on the prognosis of cancer patients is universally accepted. KPS and the Eastern Co-operative Oncology Group score/WHO performance scale are universally employed to evaluate the general functional status and are recognized for cancer treatment stratification, including glioma treatment guidelines (21, 23). Commonly, cancer-associated cachexia, chemotherapy toxicity and cancer-associated organ dysfunction are the main causes for an impaired general status. The toxicity of temozolomide is relatively low when compared with other anticancer drugs with thrombocytopenia, neutropenia, fatigue, nausea, and vomiting as the main adverse effects (24, 25). Concerning patients suffering from high-grade glioma on the other hand, neurological deterioration, including focal deficits and cognitive impairment, is pivotal for general performance (26). A decreased preoperative (27, 28) or postoperative (12) neurological performance was shown to be associated with poor prognosis in GBM patients; especially, (newly acquired) aphasia and motoric deficits were found to impair overall survival (15, 29). Moreover, a postoperative decrease of neurological performance has been shown to abrogate the beneficial survival effects gained through an increased extent of GBM resection (11, 13).
All the abovementioned studies employed a non-standardized evaluation of neurological deficits, so the NANO scale was created to objectify clinical assessment in neuro-oncology (17). For glioblastoma patients and in compliance with our results, it was previously shown that NANO scale assessment is significantly associated with patient survival in multivariate survival prediction (19) and might predict overall survival or tumor recurrence more specifically when compared with KPS or ECOG (18). However, there are several limitations to both studies. First, Ung et al. did not evaluate additional clinical and radiological parameters such as the extent of resection, adjuvant radiochemotherapy regimen, or patient age. A NANO scale cutoff is not provided. Second, Lee et al. included patients outside the Stupp regimen defining the present first-line therapy algorithm for glioblastoma. The calculated NANO scale cutoff was 7 points, probably due to an overall reduced neurological performance at initial screening when compared with our data (7.3 ± 3.8 vs. 3.3 ± 2.5 in our cohort). Last, both groups did not screen for IDH-mutations and the number of eligible patients did not exceed 80 in either study. In comparison, our data are derived from a larger, homogeneous collective, screened for clinical, radiological, and molecular parameters that are considered essential by current glioma therapy guidelines and classification of CNS tumors (1, 21). This allowed a more coherent interpretation of results and might represent a more reliable database for further projects evaluating the feasibility and prognostic value of neurological performance assessment via the NANO scale.
Our study is limited by well-known factors inherent to all retrospective analyses. Selection bias cannot be fully ruled out, especially as all patients with less than 3 months postoperative follow-up are excluded by selection criteria. The time frame was set based on the clinical routine at our center and to allow monitoring neurological performance via NANO scale assessment. After receiving the histopathological diagnosis of GBM, patients are directly admitted to adjuvant therapy, followed by 4 to 6 weeks of neurorehabilitation, or vice versa. Hence, the first readmission appointment to our outpatient clinic for initiating maintenance chemotherapy is averagely set 3 months after surgery. Naturally, patients with an extreme short survival period or the wish for palliative care are not recognized by the presented data (55 patients within the study period, see Supplementary Figure 1), explaining the prolonged 12-month survival rate shown in Table 1 when compared with epidemiological analyses (2). This also might have led to a false-negative non-significance of NANO time point 1 (difference of postoperative and preoperative NANO scale values) as patients with an initial extremely poor clinical performance were likely to be ruled out by the study design. Neuro-oncologists should be aware of this especially vulnerable group of patients that is commonly ruled out in projects evaluating new treatment options.
Monitoring neurological performance via the NANO scale might provide prognostic information independently from other well-established clinical, radiological, or pathological factors. Special attention should be paid when worsened neurological performance occurs at the first outpatient appointment after radiochemotherapy and neurorehabilitation. Prospective and multicenter data are needed to further investigate NANO scale assessment in glioblastoma patients, also including a comparison to other performance scales such as KPS or ECOG.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethical Committee of the Medical Faculty, University of Leipzig. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization: FA, JK, and JM. Data curation: JK, GP, and CF. Formal analysis: JK, MF, TW, and FW. Methodology: JK, MF, TW, and FW. Project administration: JM and FA. Software: GP. Supervision: KJ, FA, and JM. Validation: JM, FA, and KJ. Writing—original draft: JK. Writing—review and editing: all authors. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors acknowledge the support from the German Research Foundation (DFG) and Universität Leipzig within the program of Open Access Publishing.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.790458/full#supplementary-material
95 CI, 95% confidence interval; AUC, area under the curve; EOR, extent of resection; GBM, IDH-wild-type glioblastoma; HR, hazard ratio; MGMT, O6-methylguanine-DNA methyltransferase; NANO, Neurological Assessment in Neuro-Oncology; NO, neuro-oncology; RCx, radiochemotherapy; Rx, radiotherapy; ROC, receiver operator characteristic.
1. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol (2016) 131:803–20. doi: 10.1007/s00401-016-1545-1
2. Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro-Oncology (2020) 22:iv1–iv96. doi: 10.1093/neuonc/noaa200
3. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy Plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl J Med (2005) 352:987–96. doi: 10.1056/NEJMoa043330
4. Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat Rev Clin Oncol (2021) 18:170–86. doi: 10.1038/s41571-020-00447-z
5. Awad A-W, Karsy M, Sanai N, Spetzler R, Zhang Y, Xu Y, et al. Impact of Removed Tumor Volume and Location on Patient Outcome in Glioblastoma. J Neurooncol (2017) 135:161–71. doi: 10.1007/s11060-017-2562-1
6. Brown TJ, Brennan MC, Li M, Church EW, Brandmeir NJ, Rakszawski KL, et al. Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-Analysis. JAMA Oncol (2016) 2:1460–9. doi: 10.1001/jamaoncol.2016.1373
7. Okada M, Miyake K, Tamiya T. Glioblastoma Treatment in the Elderly. Neurol Medico-Chirurgica (2017) 57:667–76. doi: 10.2176/nmc.ra.2017-0009
8. Hegi ME, Diserens A-C, Gorlia T, Hamou M-F, de Tribolet N, Weller M, et al. MGMT Gene Silencing and Benefit From Temozolomide in Glioblastoma. N Engl J Med (2005) 352:997–1003. doi: 10.1056/NEJMoa043331
9. Chambless LB, Kistka HM, Parker SL, Hassam-Malani L, McGirt MJ, Thompson RC. The Relative Value of Postoperative Versus Preoperative Karnofsky Performance Scale Scores as a Predictor of Survival After Surgical Resection of Glioblastoma Multiforme. J Neurooncol (2015) 121:359–64. doi: 10.1007/s11060-014-1640-x
10. Marina O, Suh JH, Reddy CA, Barnett GH, Vogelbaum MA, Peereboom DM, et al. Treatment Outcomes for Patients With Glioblastoma Multiforme and a Low Karnofsky Performance Scale Score on Presentation to a Tertiary Care Institution. J Neurosurg (2011) 115:220–9. doi: 10.3171/2011.3.JNS10495
11. Dietterle J, Wende T, Wilhelmy F, Eisenlöffel C, Jähne K, Taubenheim S, et al. The Prognostic Value of Peri-Operative Neurological Performance in Glioblastoma Patients. Acta Neurochir (Wien) (2020) 162:417–25. doi: 10.1007/s00701-019-04136-4
12. Bleehen NM, Stenning SP. A Medical Research Council Trial of Two Radiotherapy Doses in the Treatment of Grades 3 and 4 Astrocytoma. The Medical Research Council Brain Tumour Working Party. Br J Cancer (1991) 64:769–74. doi: 10.1038/bjc.1991.396
13. Rahman M, Abbatematteo J, de Leo EK, Kubilis PS, Vaziri S, Bova F, et al. The Effects of New or Worsened Postoperative Neurological Deficits on Survival of Patients With Glioblastoma. J Neurosurg (2017) 127:123–31. doi: 10.3171/2016.7.JNS16396
14. Verlut C, Mouillet G, Magnin E, Buffet-Miny J, Viennet G, Cattin F, et al. Age, Neurological Status MRC Scale, and Postoperative Morbidity Are Prognostic Factors in Patients With Glioblastoma Treated by Chemoradiotherapy. Clin Med Insights Oncol (2016) 10:77–82. doi: 10.4137/CMO.S38474
15. McGirt MJ, Mukherjee D, Chaichana KL, Than KD, Weingart JD, Quinones-Hinojosa A. Association of Surgically Acquired Motor and Language Deficits on Overall Survival After Resection of Glioblastoma Multiforme. Neurosurgery (2009) 65:463–9; discussion 469-70. doi: 10.1227/01.NEU.0000349763.42238.E9
16. Sanai N, Mirzadeh Z, Berger MS. Functional Outcome After Language Mapping for Glioma Resection. N Engl J Med (2008) 358:18–27. doi: 10.1056/NEJMoa067819
17. Nayak L, DeAngelis LM, Brandes AA, Peereboom DM, Galanis E, Lin NU, et al. The Neurologic Assessment in Neuro-Oncology (NANO) Scale: A Tool to Assess Neurologic Function for Integration Into the Response Assessment in Neuro-Oncology (RANO) Criteria. Neuro-Oncology (2017) 19:625–35. doi: 10.1093/neuonc/nox029
18. Ung TH, Ney DE, Damek D, Rusthoven CG, Youssef AS, Lillehei KO, et al. The Neurologic Assessment in Neuro-Oncology (NANO) Scale as an Assessment Tool for Survival in Patients With Primary Glioblastoma. Neurosurgery (2019) 84:687–95. doi: 10.1093/neuros/nyy098
19. Lee J, Park SH, Kim YZ. Prognostic Evaluation of Neurological Assessment of the Neuro-Oncology Scale in Glioblastoma Patients. Brain Tumor Res Treat (2018) 6:22–30. doi: 10.14791/btrt.2018.6.e1
20. Weller M, van den Bent M, Hopkins K, Tonn JC, Stupp R, Falini A, et al. EANO Guideline for the Diagnosis and Treatment of Anaplastic Gliomas and Glioblastoma. Lancet Oncol (2014) 15:e395–403. doi: 10.1016/S1470-2045(14)70011-7
21. Weller M, van den Bent M, Tonn JC, Stupp R, Preusser M, Cohen-Jonathan-Moyal E, et al. European Association for Neuro-Oncology (EANO) Guideline on the Diagnosis and Treatment of Adult Astrocytic and Oligodendroglial Gliomas. Lancet Oncol (2017) 18:e315–29. doi: 10.1016/S1470-2045(17)30194-8
22. Quillien V, Lavenu A, Ducray F, Joly M-O, Chinot O, Fina F, et al. Validation of the High-Performance of Pyrosequencing for Clinical MGMT Testing on a Cohort of Glioblastoma Patients From a Prospective Dedicated Multicentric Trial. Oncotarget (2016) 7:61916–29. doi: 10.18632/oncotarget.11322
23. Wick W, Osswald M, Wick A, Winkler F. Treatment of Glioblastoma in Adults. Ther Adv Neurol Disord (2018) 11:1756286418790452. doi: 10.1177/1756286418790452
24. Bae SH, Park M-J, Lee MM, Kim TM, Lee S-H, Cho SY, et al. Toxicity Profile of Temozolomide in the Treatment of 300 Malignant Glioma Patients in Korea. J Korean Med Sci (2014) 29:980. doi: 10.3346/jkms.2014.29.7.980
25. Scaringi C, de Sanctis V, Minniti G, Enrici RM. Temozolomide-Related Hematologic Toxicity. Onkologie (2013) 36:2. doi: 10.1159/000353752
26. Sizoo EM, Braam L, Postma TJ, Pasman HR, Heimans JJ, Klein M, et al. Symptoms and Problems in the End-of-Life Phase of High-Grade Glioma Patients. Neuro-Oncology (2010) 12:1162–6. doi: 10.1093/neuonc/nop045
27. Chaichana KL, Chaichana KK, Olivi A, Weingart JD, Bennett R, Brem H, et al. Surgical Outcomes for Older Patients With Glioblastoma Multiforme: Preoperative Factors Associated With Decreased Survival. Clinical Article. J Neurosurg (2011) 114:587–94. doi: 10.3171/2010.8.JNS1081
28. Liang H-K, Wang C-W, Tseng H-M, Huang C-Y, Lan K-H, Chen Y-H, et al. Preoperative Prognostic Neurologic Index for Glioblastoma Patients Receiving Tumor Resection. Ann Surg Oncol (2014) 21:3992–8. doi: 10.1245/s10434-014-3793-4
Keywords: GBM, glioblastoma, neuro-oncology, neurological performance, NANO scale
Citation: Kasper J, Wende T, Fehrenbach MK, Wilhelmy F, Jähne K, Frydrychowicz C, Prasse G, Meixensberger J and Arlt F (2021) The Prognostic Value of NANO Scale Assessment in IDH-Wild-Type Glioblastoma Patients. Front. Oncol. 11:790458. doi: 10.3389/fonc.2021.790458
Received: 06 October 2021; Accepted: 09 November 2021;
Published: 02 December 2021.
Edited by:
Marie-Therese Forster, University Hospital Frankfurt, GermanyReviewed by:
John E. Mignano, Tufts University School of Medicine, United StatesCopyright © 2021 Kasper, Wende, Fehrenbach, Wilhelmy, Jähne, Frydrychowicz, Prasse, Meixensberger and Arlt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johannes Kasper, am9oYW5uZXMua2FzcGVyQG1lZGl6aW4udW5pLWxlaXB6aWcuZGU=; orcid.org/0000-0003-2122-2676
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.