
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 05 January 2022
Sec. Cancer Genetics
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.789659
 Van Thuan Tran1Sao Trung Nguyen2Xuan Dung Pham3Thanh Hai Phan4Van Chu Nguyen5Huu Thinh Nguyen6Huu Phuc Nguyen6
Van Thuan Tran1Sao Trung Nguyen2Xuan Dung Pham3Thanh Hai Phan4Van Chu Nguyen5Huu Thinh Nguyen6Huu Phuc Nguyen6 Phuong Thao Thi Doan2Tuan Anh Le7Bao Toan Nguyen4Thanh Xuan Jasmine4
Phuong Thao Thi Doan2Tuan Anh Le7Bao Toan Nguyen4Thanh Xuan Jasmine4 Duy Sinh Nguyen8Hong-Dang Luu Nguyen9,10
Duy Sinh Nguyen8Hong-Dang Luu Nguyen9,10 Ngoc Mai Nguyen9,10Duy Xuan Do9,10Vu Uyen Tran9,10Hue Hanh Thi Nguyen9,10Minh Phong Le9,10Yen Nhi Nguyen9,10Thanh Thuy Thi Do9Dinh Kiet Truong9Hung Sang Tang9,10
Ngoc Mai Nguyen9,10Duy Xuan Do9,10Vu Uyen Tran9,10Hue Hanh Thi Nguyen9,10Minh Phong Le9,10Yen Nhi Nguyen9,10Thanh Thuy Thi Do9Dinh Kiet Truong9Hung Sang Tang9,10 Minh-Duy Phan9,10
Minh-Duy Phan9,10 Hoai-Nghia Nguyen2*
Hoai-Nghia Nguyen2* Hoa Giang9,10*
Hoa Giang9,10* Lan N. Tu9,10*
Lan N. Tu9,10*Background: Hereditary cancer syndromes (HCS) are responsible for 5-10% of cancer cases. Genetic testing to identify pathogenic variants associated with cancer predisposition has not been routinely available in Vietnam. Consequently, the prevalence and genetic landscape of HCS remain unknown.
Methods: 1165 Vietnamese individuals enrolled in genetic testing at our laboratory in 2020. We performed analysis of germline mutations in 17 high- and moderate- penetrance genes associated with HCS by next generation sequencing.
Results: A total of 41 pathogenic variants in 11 genes were detected in 3.2% individuals. The carrier frequency was 4.2% in people with family or personal history of cancer and 2.6% in those without history. The percentage of mutation carriers for hereditary colorectal cancer syndromes was 1.3% and for hereditary breast and ovarian cancer syndrome was 1.6%. BRCA1 and BRCA2 mutations were the most prevalent with the positive rate of 1.3% in the general cohort and 5.1% in breast or ovarian cancer patients. Most of BRCA1 mutations located at the BRCA C-terminus domains and the top recurrent mutation was NM_007294.3:c.5251C>T (p.Arg1751Ter). One novel variant NM_000038.6(APC):c.6665C>A (p.Pro2222His) was found in a breast cancer patient with a strong family history of cancer. A case study of hereditary cancer syndrome was illustrated to highlight the importance of genetic testing.
Conclusion: This is the first largest analysis of carrier frequency and mutation spectrum of HCS in Vietnam. The findings demonstrate the clinical significance of multigene panel testing to identify carriers and their at-risk relatives for better cancer surveillance and management strategies.
Cancer remains the leading cause of death worldwide with 19.3 million new cases and almost 10 million deaths in 2020 (1). In Vietnam, the number of cases is also on the rise with 188 new cases and 126 cancer-related deaths per every 100,000 people (1). About 5-10% of cancer cases are hereditary and result directly from hereditary cancer syndromes (HCS), a genetic predisposition to cancer due to inherited germline mutations in one or more genes (2, 3). The most common HCS include the hereditary breast and ovarian cancer syndrome (HBOC) and hereditary colorectal cancer syndromes (HCCS). HBOC is caused by germline mutations mainly in the BRCA1 and BRCA2 genes; individuals with HBOC tend to have early onset of breast and/or ovarian cancer as well as some other types of cancer (4). HCCS are associated with mutations in various genes and the major types include Lynch syndrome, familial adenomatous polyposis (FAP) and MUTYH-associated adenomatous polypopsis (MAP), all of which predispose affected individuals to both colorectal and extracolonic malignancies at an early age (5). Other HCS such as Li-Fraumeni syndrome, Cowden syndrome and Von Hippel-Lindau syndrome all significantly increase risk for a wide spectrum of tumor types.
Identification of individuals with HCS is highly important as it allows for active surveillance, early cancer detection and tailored management strategies. This can be achieved through genetic counselling and testing, which has been routinely available in Western countries. Particularly, recent advances in next-generation sequencing (NGS) technologies have enabled analysis of multiple genes simultaneously, leading to the widespread adoption of multigene panels for hereditary cancer testing in Western healthcare systems (6). However, in Asia including Vietnam, accessibility to such genetic testing service is far limited due to the high cost and lack of trained laboratories and healthcare professionals (7). Consequently, there is currently no information about the incidence rate of HCS, frequency of pathogenic variant carriers and mutation spectrum of HCS-associated genes in the Vietnamese population. This lack of data further creates barrier for public and healthcare providers’ awareness of the importance of genetic testing and risk management for people carrying germline mutations.
Our laboratory used a panel of 17 high- and moderate- penetrance genes recommended by the National Comprehensive Cancer Network (NCCN) guidelines to screen for germline pathogenic mutations associated with HCS. In this paper, we present the results of mutation profile and prevalence of pathogenic mutations from 1165 Vietnamese participants tested in the year of 2020.
This study included 1165 individuals across Vietnam who were referred by physicians or self-enrolled in genetic testing at our laboratory from January to December 2020. 403 participants met the referral indications for cancer predisposition assessment in the guidelines of American College of Medical Genetics and Genomics (ACMG) and the National Society of Genetic Counselors (NSGC) (8). In brief, people with personal or family history of 1) a rare cancer (e.g., ovarian, triple negative breast, medullary thyroid), 2) an early onset cancer (e.g., colorectal or breast cancer before the age of 50), 3) two or more different cancers affecting multiple organs or separate locations in the same organ (e.g., bilateral breast cancer); 4) people with family history of multiple relatives on the same side of the family getting the same types of cancer; 5) people who had 10 or more colorectal polyps found during colonoscopies; 6) people with family members previously tested positive for cancer-predisposing mutations, were included in the study. 762 individuals without personal or family cancer history but interested in knowing their mutation carrier status were also recruited. These participants either self-enrolled in the study or were referred by their primary care physicians during annual health checkup or other cancer-unrelated examinations. There was no exclusion criteria. After genetic counseling, all participants approved and gave written informed consent to the anonymous reuse of their genomic data for this study. All genomic data were de-identified and aggregated for the genetic analysis of the cohort. Detailed information about personal and family history of cancer was provided by the referring clinicians or by interview with participants.
Our hereditary cancer gene panel consists of 17 high- and moderate- penetrance genes associated with cancer and hereditary cancer syndromes as recommended by the NCCN guidelines (9, 10): BRCA1, BRCA2, PALB2, PTEN, TP53, CDH1, MLH1, MSH2, MSH6, PMS2, EPCAM, APC, MUTYH, STK11, VHL, RB1, RET. The list of genes and their association with different types of cancer is provided in Table S1.
Each participant provided either 2 mL of peripheral blood or a buccal swab sample. Genomic DNA was extracted from blood samples by the GeneJet whole blood genomic DNA purification minikit (ThermoFisher, USA), or from buccal swab samples by the QIAamp DNA minikit (Qiagen, Germany). DNA fragmentation and library preparation were performed using the NEBNext Ultra II FS DNA library prep kit (New England Biolabs, USA) following the manufacturer’s instructions. Libraries were pooled together and hybridized with predesigned probes for 17 targeted genes (Integrated DNA Technologies, USA). Massive parallel sequencing was performed using NextSeq 500/550 High output kits v2 (150 cycles) on the Illumina NextSeq 550 system (Illumina, USA) with the minimum target coverage of 100x.
Quality control and data processing were performed as previously described (11). Briefly, the paired-end reads were aligned to human reference genome (GRCh38) using Burrows Wheeler Aligner (BWA) (12). The aligned output was used to compute coverage depth of targeted regions and variant calling was performed using GATK 3.8 (13). Variants were annotated against dbSNP (14), ClinVar (15) and LOVD (16) databases and were analyzed for their molecular consequences using the Ensemble Variant Effect Predictor (17).
Variants were classified according to the classification in the guidelines of The American College of Medical Genetics and Genomics (ACMG) (18). In short, ACMG recommends a five-tier system (“pathogenic”, “likely pathogenic”, variant of uncertain significance”, “likely benign”, “benign”) to determine the pathogenicity using known literature/database and computational predictive programs as main criteria. In this study, we reported both pathogenic and likely pathogenic variants as “pathogenic variants”.
Sanger sequencing was performed to confirm all pathogenic variants identified by NGS. First, primers were designed flanking the mutation location using Primer3Plus (19) and synthesized by Integrated DNA Technologies, USA. PCR amplification was prepared using the same genomic DNA samples as above and Q5 High-Fidelity 2X mastermix (New England Biolabs, USA) following the manufacturer’s instructions. PCR products were purified and sequenced by the Genetic Analyzer 3500xl (Applied Biosystems, USA).
From January to December of 2020, 1165 Vietnamese participants enrolled under two cancer screening programs: a female-oriented screening program (Pinkcare) that had 815 women and a general screening program that had 350 people (244 female, 106 male). The participants either were referred by physcians (77.0%) or self-enrolled (23.0%) in the screening programs. The mean age was 38.8 years old with 95.6% of the participants were between 15 to 64 years old. 403 participants (34.6%) reported to have either family history or personal medical history of cancer. The main type of cancer in those with medical history was breast and/or ovarian cancer. Among 762 participants (65.4%) reported not to have any history of cancer, 595 had their history information provided by the referring physicians, 167 people self-reported their history, which could not be verified. Majority of the participants (96.9%) were unrelated. Participant demographics is provided in Table 1.
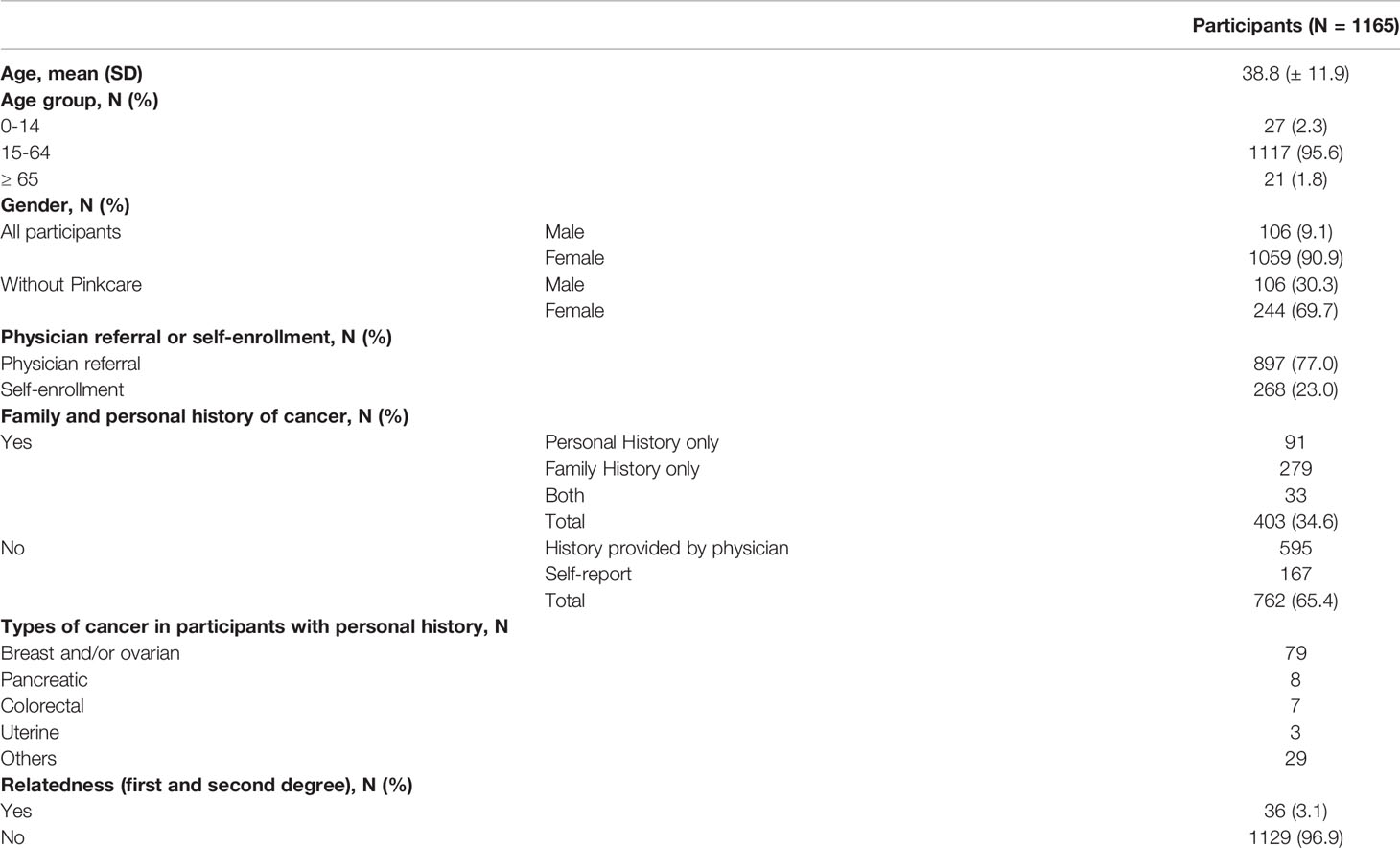
Table 1 Demographics of participants in the study.
Genetic testing by NGS identified 42 pathogenic variants, 41 of which were confirmed by Sanger sequencing in each individual, demonstrating the accuracy of NGS at 97.6%. 37 out of 1165 participants (3.2%) were positive for at least 1 pathogenic mutation in the gene panel. This frequency among people with family or personal history (Hx) of cancer was 4.2% (17/403) and among those without history was 2.6% (20/762) (Figure 1A). Excluding the relatives, the carrier frequency among unrelated people was 2.9% (33/1129).
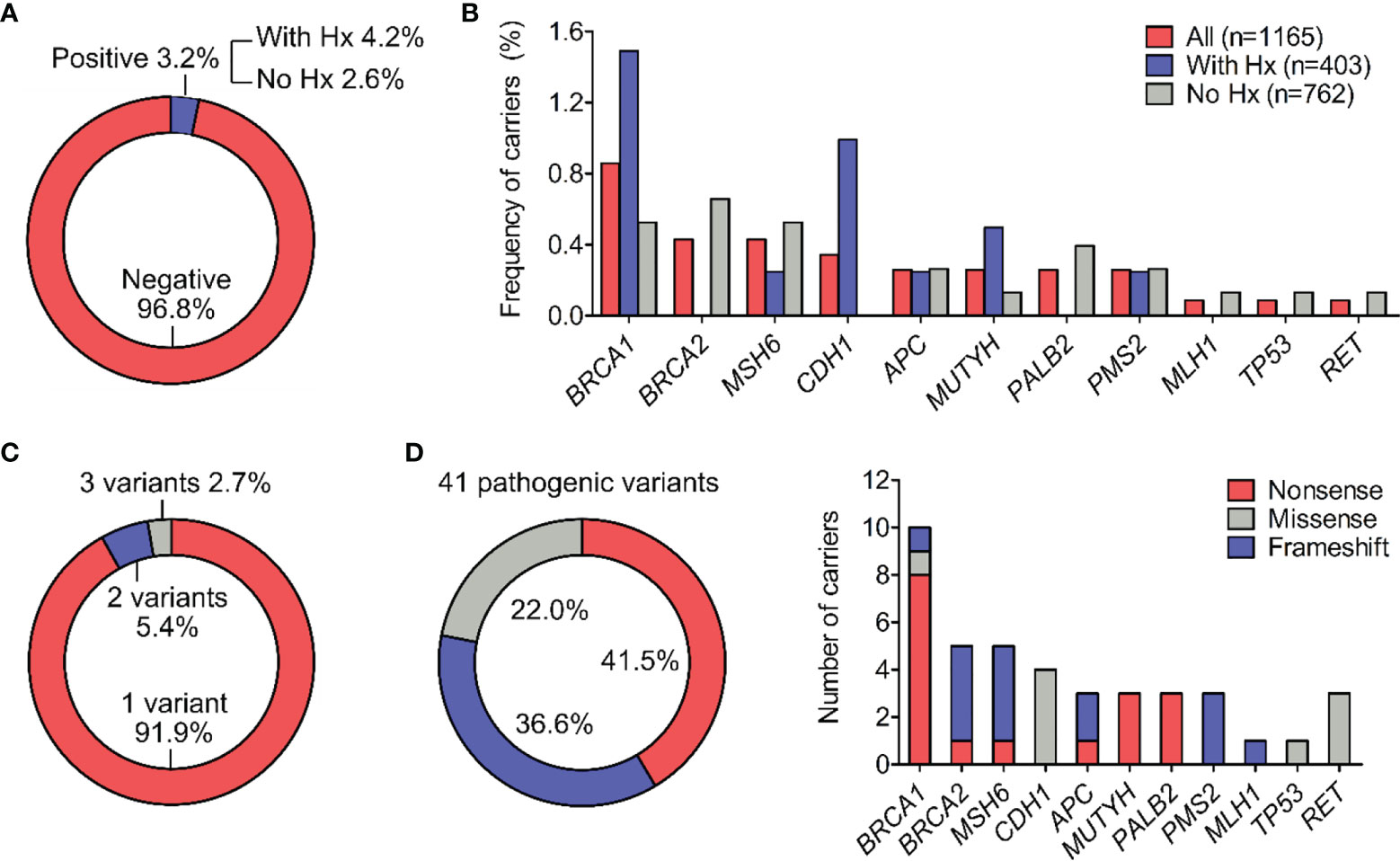
Figure 1 Types and frequency of all pathogenic variants. (A) Percentage of participants positive for at least one pathogenic variant in the general cohort and in subgroups with or without history (Hx) of cancer. (B) Percentage of pathogenic variant carriers for individual gene. (C) Percentage of carriers (n=37) harboring 1, 2 or 3 pathogenic variants. (D) Distribution of molecular consequences (nonsense, missense and frameshift) among the 41 pathogenic variants. The frequency of different molecular consequences for each gene was illustrated.
Out of 17 genes tested, 11 genes had at least 1 mutation while 6 genes: PTEN, MSH2, EPCAM, STK11, VHL, RB1 showed no mutations. BRCA1, BRCA2 and MSH6 were the top mutated genes with the carrier frequency of 0.9%, 0.4%, 0.4% respectively among all participants (Figure 1B and Table 2). The carrier frequency for each gene in the subgroups of people with and without family or personal history is provided in Table 2. For example, the percentage of carriers for BRCA1 mutations was 1.5% in people with history, and 0.5% in those without history (Figure 1B and Table 2).
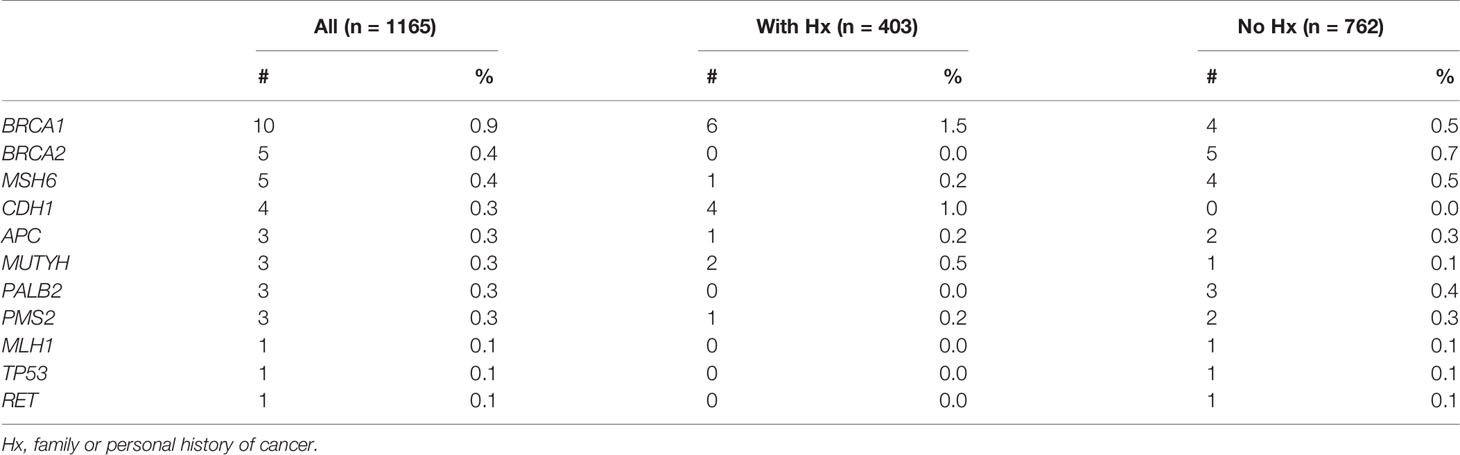
Table 2 The number and percentage of all pathogenic variant carriers.
Most of the carriers (91.9%) had one pathogenic variant while 1 person carried 3 pathogenic variants in the RET gene and 2 people carried 2 pathogenic variants, one of each in the CDH1 and MUTYH genes (Figure 1C). All the variants were found heterozygous.
Nonsense mutations were the most prevalent type, accounting for 41.5% (17/41) of the 41 variants identified in the cohort, followed by frameshift mutations and missense mutations with the frequency of 36.6% (15/41) and 22.0% (9/41) respectively (Figure 1D). No insertion/deletion or rearrangement variants were detected. The type of molecular consequences observed was unique to the genes: BRCA1, MUTYH and PALB2 mainly had nonsense mutations, BRCA2, MSH6, PMS2, MLH1 predominantly had frameshift mutations, while CDH1, TP53 had missense mutations (Figure 1D). Out of 41 pathogenic variants, 27 of them were unique. The full list of variants, their frequency and molecular consequences is provided in Table S2.
The 3 major types of HCCS include Lynch syndrome (genes: MLH1, MSH2, MSH6, PMS2, EPCAM), FAP (gene: APC), and MAP (gene: MUTYH). Frequency of carriers harboring at least one pathogenic variants in the HCCS-associated genes was 1.3% (15/1165). Specifically, the carrier frequency for genes associated with Lynch syndrome, FAP and MAP in the general cohort were 0.8%, 0.3% and 0.3% respectively (Figure 2A). The carrier frequency for subgroups of people with and without history is provided in Table 3. Majority of the carriers were male (73.3%) and positive for only 1 pathogenic variant (85.7%) (Figure 2A). 2 people carried the same 2 pathogenic variants: NM_001048171.1(MUYTH):c.425G>A (p.Trp142Ter) and NM_004360.5(CDH1):c.2195G>A (p.Arg732Gln).
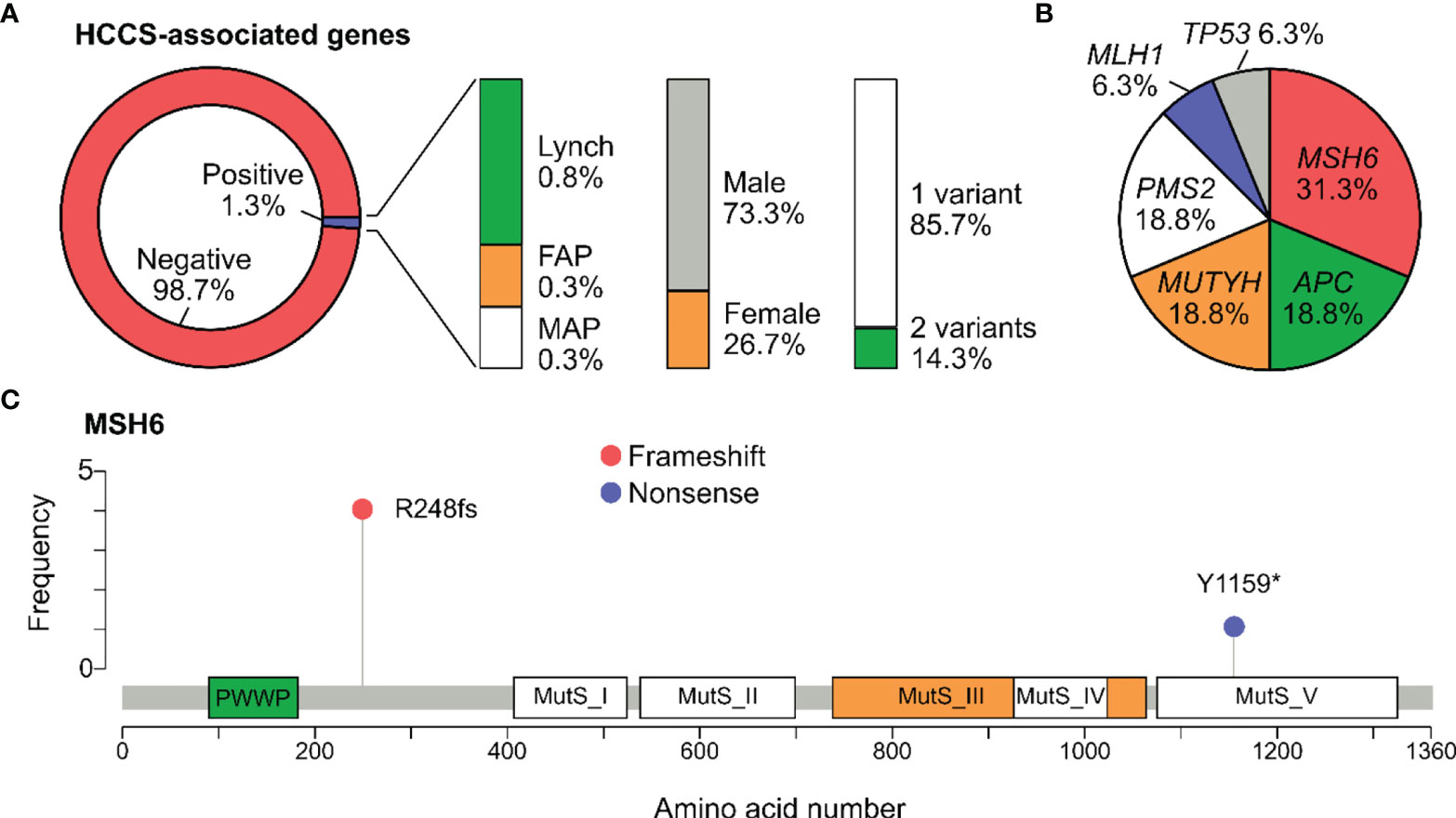
Figure 2 Pathogenic variants associated with Hereditary Colorectal Cancer syndromes. (A) Percentage of participants positive for at least one pathogenic variant in the genes associated with Hereditary Colorectal Cancer Syndromes (HCCS): Lynch syndrome (MLH1, MSH2, MSH6, PMS2, EPCAM), familial adenomatous polyposis (FAP) (APC), MUTYH-associated adenomatous polypopsis (MAP) (MUTYH). The percentage of carriers by gender and number of variants was also illustrated. (B) Pie chart showing the distribution of pathogenic variants among the HCCS-associated genes. No variant was found in EPCAM and MSH2. (C) Lollipop plot reporting distribution of all pathogenic variants identified in MSH6. Protein domains shown include PWWP (Pro-Trp-Trp-Pro) and all Mutator S (MutS) domains.
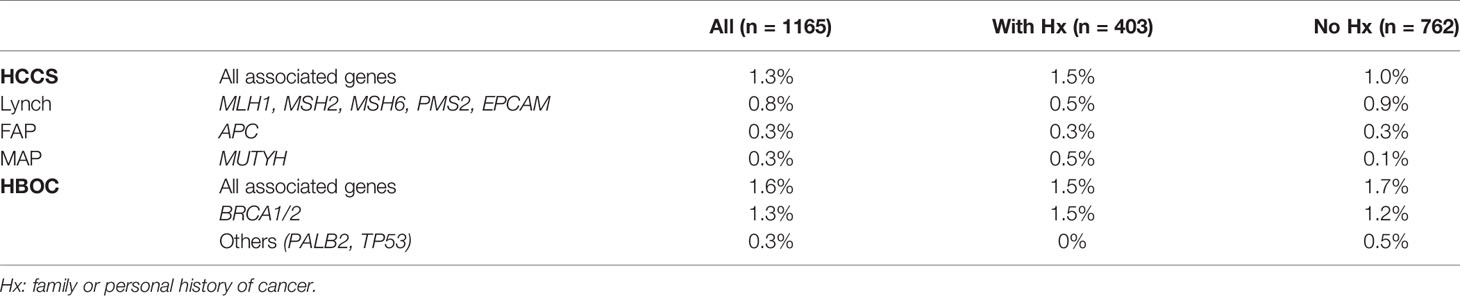
Table 3 The percentage of carriers for pathogenic variants associated with specific hereditary cancer syndromes.
In total, 16 pathogenic variants were detected in all the HCCS-associated genes except EPCAM. MSH6 was the most frequently mutated gene, accounting for 0.4% of the cases and 31.3% of the HCCS-associated genes (Figure 2B). Lollipop plot illustrated the distribution of pathogenic variants along the MSH6 protein sequence, showing that NM_000179.2:c.742del (p.Arg248fs) was the most common mutation and not located in any of the MutS domains of MSH6 (Figure 2C).
The carrier frequency for BRCA1/2 mutations was 1.4% (15/1059) in women and 1.3% (15/1165) in all participants (Figure 3A). Apart from BRCA1/2, pathogenic mutations were also identified in other genes associated with HBOC (PALB2 and TP53), increasing the prevalence of total carriers to 1.6% (19/1165) (Figure 3A). The carrier frequency for subgroups of people with and without history is provided in Table 3.

Figure 3 Pathogenic variants associated with Hereditary Breast and Ovarian Cancer syndrome. (A) Percentage of participants positive for at least one pathogenic variant in the genes associated with the Hereditary Breast and Ovarian Cancer (HBOC) syndrome: BRCA1/2 and others: PALB2, TP53. No variant was identified in CDH1, STK11 and PTEN. (B) Percentage of participants with breast or ovarian cancer that harbored pathogenic variants in HBOC-associated genes. Apart from pathogenic variants, variants of uncertain significance (VUS) and a novel variant were identified in these patients. (C) Lollipop plot reporting distribution of all pathogenic variants identified in the BRCA1 and BRCA2 genes. Protein domains shown in BRCA1 include Zinc finger (ZF), Ethylene insensitive 3 (EIN3), BRCA1 C-Terminus domain 1 (CT1) and domain 2 (CT2). Protein domains shown in BRCA2 include BRC repeats (orange), helical domain, oligonucleotide/oligosaccharide-binding domain 1 (OB1) and domain 3 (OB3).
79 participants in our cohort had personal medical history of breast and/or ovarian cancer. The frequency of pathogenic variant carriers among these cancer patients were 6.3%, with BRCA1/2 carriers accounted for 5.1% (Figure 3B). All BRCA mutations were identified in the BRCA1 gene only, not BRCA2 (Table S3). In addition to pathogenic variants, we identified 9 variants of uncertain significance (VUS) in 7 genes and 1 novel missense variant in the APC gene in additional 10 cancer patients (Table S3). The novel variant: NM_000038.6(APC):c.6665C>A (p.Pro2222His) was the only variant found in a breast cancer patient who had two family members diagnosed with breast cancer and liver cancer. This variant had not been reported in any databases. Analysis by SIFT and Polyphen predicted it to be “deleterious” and “Probably_Damaging” respectively.
Since BRCA1 and BRCA2 were the most frequently mutated genes in HBOC, we illustrated the distribution of their pathogenic mutations along the corresponding protein sequences (Figure 3C). The most common variant in BRCA1 was NM_007294.3:c.5251C>T (p.Arg1751Ter) followed by NM_007294.3:c.4997dup (p.Tyr1666Ter). Majority of the variants located at the BRCA C-terminus domains 1 and 2 (CT1 and CT2) of BRCA1. No hotspot was identified for BRCA2.
The proband III.2 was diagnosed with gastric cancer at the age of 31 years old. He described a strong family history of cancer, including his father who died of gastric cancer at 48, a paternal aunt who died of gastric cancer at 37 and a paternal first cousin who also died of gatric cancer at 30 (Figure 4). Based on his family and medical history of early onset gastric cancer, he was referred to our laboratory for genetic testing for potential hereditary cancer syndrome. Genetic testing using our 17-gene panel revealed 2 pathogenic variants: NM_004360.5(CDH1):c.2195G>A (p.Arg732Gln) and NM_001048171.1(MUTYH):c.425G>A (p.Trp142Ter). His at-risk family members and relatives were then offered genetic counselling and testing for the above mutations by Sanger sequencing. His sister III.1 and the first cousin’s son IV.2 were found positive for the mutation NM_004360.5(CDH1):c.2195G>A (p.Arg732Gln) while his brother III.4 carried the same 2 pathogenic mutations above (Figure 4). The mutations were found transmitted through both paternal and maternal lineages and affected several generations, a classic feature of hereditary cancer syndrome. All the affected members received genetic counselling to understand their testing results and got referred to oncologist for cancer risk assessment and management.

Figure 4 A cancer family pedigree with multiple affected members indicating hereditary cancer syndrome. The proband III.2 was diagnosed with gastric cancer at the age of 31 years old. Genetic testing revealed 2 pathogenic variants in the CDH1 and MUTYH genes. Other family members and relatives were labeled for the presence of cancer and mutation status.
Our study used NGS technology to examine the prevalence of carriers for germline HCS-associated variants in 1165 Vietnamese participants. The study cohort was predominantly female (90.9%) because most of them enrolled through our female-oriented screening program Pinkcare. Besides people that met criteria for cancer predisposition assessment (34.6%), majority of the participants (65.4%) did not have any history or risk factors but were interested in knowing their carrier status. The rationale for a mixed cohort was to be able to estimate the frequency of HCS carriers in a more general population, which was found to be 3.2%. This frequency is likely overestimated and not truly reflective of the carrier frequency in the Vietnamese population since the study cohort was still enriched with high-risk individuals and the participants recruited at our laboratory were not representative of the overall Vietnamese population. However, this initial finding helps to raise awareness of HCS in the Vietnamese and serves as a reference for future studies.
BRCA1 and BRCA2 were found the most frequently mutated genes with the total prevalence of BRCA1/2 mutation carriers at 1.3%, or 1 in 78. We compared this finding to a large exome sequencing study from a diverse population-based biobank of 30,223 people. Their subpopulation analysis showed the highest prevalence of carriers in the Ashkenazi Jewish (2%, 1 in 49), followed by the Filipino and other Southeast Asians (1.2%, 1 in 81) (20). Our percentage of BRCA1/2 mutation carriers at 1.3% in the Vietnamese is similar to other Southeast Asian countries and also to the Han Chinese (1.1%, 1 in 91) (21).
Among 79 participants that had breast and/or ovarian cancer, the total carrier frequency was 6.3% (1 in 16) and for BRCA1 only was 5.1% (1 in 20); no mutation was identified in BRCA2. This frequency of BRCA mutation carriers is relatively low compared to 12.6% in Greece, Romania and Turkey (22) and 27.0% in India (23) but comparable to 5.5% in the Han Chinese (21) and 4.7% in the Malaysian (24). However, BRCA2 mutations were readily reported in all of those populations, suggesting that BRCA2 mutations might be less prevalent in the Vietnamese patients with breast or ovarian cancers. Interestingly, this conclusion agrees with the observations by Vu et al. who used NGS to characterize all BRCA mutations in 101 Vietnamese patients with ovarian cancer. Their data showed that 6.9% (7/101) patients carried pathogenic mutations in BRCA1 and similar to our study, no BRCA2 mutation was identified (25). Another study in Vietnam involving 259 breast cancer patients reported only 2 carriers of BRCA mutations (0.8%) (26). This extremely low frequency was likely an underestimation because only 17 BRCA mutations were tested by Sanger sequencing in their study. It has been demonstrated in several studies that NGS technology allows simultaneous detection of all mutations in multiple genes, hence enabling more accurate estimation of the population incident rate than Sanger sequencing (22, 23, 27).
Majority of BRCA1 mutations (7/10) located in the BRCA C-Terminus domains, the highly conserved repeats responsible for BRCA1 function. Frameshift or nonsense mutations that disrupt or eliminate the BRCT domains were often reported to increase cancer predisposition (28). Moreover, the mutation landscape of BRCA1 seems to be unique in our cohort as those reported in the US (29), Greece (22), India (23) and China (30) did not concentrate in any protein domains. This conclusion, however, needs to be corroborated with a larger number of BRCA1 mutations in future studies. The most prevalent BRCA1 mutation was NM_007294.3:c.5251C>T (p.Arg1751Ter) as identified in 3 unrelated individuals. This mutation was previously proposed to be a founder mutation in the Vietnamese when it was identified in 4% (4/101) patients with ovarian cancer in Vietnam (25). However, it has also been reported as a founder or recurrent mutation in the Greek (31) and Polish (32), making it a recurrent rather than founder mutation in the Vietnamese.
The percentage of carriers for mutations associated with HCS was 1.3% (1 in 78), specifically with Lynch syndrome: 0.8% (1 in 129), FAP: 0.3% (1 in 388) and MAP: 0.3% (1 in 388). Surprisingly, most of the carriers were male (73.3%) despite the fact that our cohort was female dominant. Most of the studies in the US reported that MLH1 and MSH2 mutations were detected in 80-90% cases of Lynch syndrome while MSH6 and PMS2 mutations were less than 10% (5, 33). On the contrary, our study found the most mutations in MSH6 and PMS2, only 1 mutation in MLH1 and no mutation in MSH2, similar to a population genetic study in Iceland (34). The variant NM_000179.2(MSH6):c.742del (p.Arg248fs) detected in 4 unrelated individuals is a recurrent mutation in the Vietnamese cohort.
The limitation of this study is that 167 participants who self-enrolled in our screening programs could not have their family or medical history verified. As a result, the subgroup analysis of carrier frequency for people with and without history might be less accurate. Furthermore, our analysis mainly focused on pathogenic variants since they have clear recommendations from the clinical management guidelines. VUS and novel variants that could be specific to the Vietnamese or have clinical relevance are not reported in this study and should be included in more comprehensive mutation profiling in future studies.
In conclusion, our study provides the first insights into the prevalence and mutation spectrum of hereditary cancer syndromes in a large Vietnamese cohort. These findings and the case study of HCS serve as the knowledge base to raise awareness for both the public and healthcare professionals about hereditary cancer syndromes and the importance of genetic counselling and NGS-based genetic testing in Vietnam. The molecular genetic information enables physicians to tailor management plans for inherited cancer patients and engage active surveillance for their at-risk relatives. We anticipate that with the increasing adoption of multigene testing, more comprehensive population-based genetic data and epidemiological information would be available to delineate the role of more genes and variants in cancer predisposition.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the institutional ethics committee of the University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam (approval number 164/HDDD). Written informed consent to participate in this study was provided by the participants or the participants’ legal guardian.
VTT, SN, XP, TP, VN, HTN, HPN, PD, TL, BN, TJ, and DN recruited patients and performed clinical analysis. H-DN, NN, DD, VUT, HHN, ML, YN, TD, DT, HT, and M-DP processed samples and analyzed data. HNN, HG, and LT designed experiments, analyzed data and wrote the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by Gene Solutions, Vietnam. The funder did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
H-DN, NN, DD, VUT, HHN, ML, YN, HT, M-DP, HG, and LT are current employees of Gene Solutions, Vietnam.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.789659/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
2. Rahner N, Steinke V. Hereditary Cancer Syndromes. Dtsch Arztebl Int (2008) 105:706–14. doi: 10.3238/arztebl.2008.0706
3. Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, et al. Environmental and Heritable Factors in the Causation of Cancer–Analyses of Cohorts of Twins From Sweden, Denmark, and Finland. N Engl J Med (2000) 343:78–85. doi: 10.1056/NEJM200007133430201
4. Yoshida R. Hereditary Breast and Ovarian Cancer (HBOC): Review of Its Molecular Characteristics, Screening, Treatment, and Prognosis. Breast Cancer (2021) 28:1167–80. doi: 10.1007/s12282-020-01148-2
5. Jasperson KW, Tuohy TM, Neklason DW, Burt RW. Hereditary and Familial Colon Cancer. Gastroenterology (2010) 138:2044–58. doi: 10.1053/j.gastro.2010.01.054
6. Okur V, Chung WK. The Impact of Hereditary Cancer Gene Panels on Clinical Care and Lessons Learned. Cold Spring Harb Mol Case Stud (2017) 3(6):a002154. doi: 10.1101/mcs.a002154
7. Nakamura S, Kwong A, Kim SW, Iau P, Patmasiriwat P, Dofitas R, et al. Current Status of the Management of Hereditary Breast and Ovarian Cancer in Asia: First Report by the Asian BRCA Consortium. Public Health Genomics (2016) 19:53–60. doi: 10.1159/000441714
8. Hampel H, Bennett RL, Buchanan A, Pearlman R, Wiesner GL. A Practice Guideline From the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: Referral Indications for Cancer Predisposition Assessment. Genet Med (2015) 17:70–87. doi: 10.1038/gim.2014.147
9. Daly MB, Pilarski R, Yurgelun MB, Berry MP, Buys SS, Dickson P, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 1. 2020 J Natl Compr Canc Netw (2020) 18:380–91. doi: 10.6004/jnccn.2020.0017
10. Gupta S, Provenzale D, Llor X, Halverson AL, Grady W, Chung DC, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Colorectal, Version 2. 2019 J Natl Compr Canc Netw (2019) 17:1032–41. doi: 10.6004/jnccn.2019.0044
11. Tran NH, Nguyen Thi TH, Tang HS, Hoang LP, Nguyen TL, Tran NT, et al. Genetic Landscape of Recessive Diseases in the Vietnamese Population From Large-Scale Clinical Exome Sequencing. Hum Mutat (2021) 42(10):1229–38. doi: 10.1101/2020.10.27.358358
12. Li H. Aligning Sequence Reads, Clone Sequences and Assembly Contigs With BWA-MEM. arXiv (2013). 1303.3997v2 [q-bio.GN].
13. DePristo MA, Banks E, Poplin R, Garimella KV, Maguire JR, Hartl C, et al. A Framework for Variation Discovery and Genotyping Using Next-Generation DNA Sequencing Data. Nat Genet (2011) 43:491–8. doi: 10.1038/ng.806
14. Sherry ST, Ward MH, Kholodov M, Baker J, Phan L, Smigielski EM, et al. dbSNP: The NCBI Database of Genetic Variation. Nucleic Acids Res (2001) 29:308–11. doi: 10.1093/nar/29.1.308
15. Landrum MJ, Lee JM, Riley GR, Jang W, Rubinstein WS, Church DM, et al. ClinVar: Public Archive of Relationships Among Sequence Variation and Human Phenotype. Nucleic Acids Res (2014) 42:D980–5. doi: 10.1093/nar/gkt1113
16. Fokkema IF, Taschner PE, Schaafsma GC, Celli J, Laros JF, den Dunnen JT. LOVD V.2.0: The Next Generation in Gene Variant Databases. Hum Mutat (2011) 32:557–63. doi: 10.1002/humu.21438
17. McLaren W, Gil L, Hunt SE, Riat HS, Ritchie GR, Thormann A, et al. The Ensembl Variant Effect Predictor. Genome Biol (2016) 17:122. doi: 10.1186/s13059-016-0974-4
18. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med (2015) 17:405–24. doi: 10.1038/gim.2015.30
19. Untergasser A, Cutcutache I, Koressaar T, Ye J, Faircloth BC, Remm M, et al. Primer3–New Capabilities and Interfaces. Nucleic Acids Res (2012) 40:e115. doi: 10.1093/nar/gks596
20. Abul-Husn NS, Soper ER, Odgis JA, Cullina S, Bobo D, Moscati A, et al. Exome Sequencing Reveals a High Prevalence of BRCA1 and BRCA2 Founder Variants in a Diverse Population-Based Biobank. Genome Med (2019) 12:2. doi: 10.1186/s13073-019-0691-1
21. Liu Y, Wang H, Wang X, Liu J, Li J, Wang X, et al. Prevalence and Reclassification of BRCA1 and BRCA2 Variants in a Large, Unselected Chinese Han Breast Cancer Cohort. J Hematol Oncol (2021) 14:18. doi: 10.1186/s13045-020-01010-0
22. Tsaousis GN, Papadopoulou E, Apessos A, Agiannitopoulos K, Pepe G, Kampouri S, et al. Analysis of Hereditary Cancer Syndromes by Using a Panel of Genes: Novel and Multiple Pathogenic Mutations. BMC Cancer (2019) 19:535. doi: 10.1186/s12885-019-5756-4
23. Kadri MSN, Patel KM, Bhargava PA, Shah FD, Badgujar NV, Tarapara BV, et al. Mutational Landscape for Indian Hereditary Breast and Ovarian Cancer Cohort Suggests Need for Identifying Population Specific Genes and Biomarkers for Screening. Front Oncol (2020) 10:568786. doi: 10.3389/fonc.2020.568786
24. Wen WX, Allen J, Lai KN, Mariapun S, Hasan SN, Ng PS, et al. Inherited Mutations in BRCA1 and BRCA2 in an Unselected Multiethnic Cohort of Asian Patients With Breast Cancer and Healthy Controls From Malaysia. J Med Genet (2018) 55:97–103. doi: 10.1136/jmedgenet-2017-104947
25. Vu HA, Phu ND, Khuong LT, Hoa PH, Nhu BTH, Nhan VT, et al. Recurrent BRCA1 Mutation, But No BRCA2 Mutation, in Vietnamese Patients With Ovarian Carcinoma Detected With Next Generation Sequencing. Asian Pac J Cancer Prev (2020) 21:2331–5. doi: 10.31557/APJCP.2020.21.8.2331
26. Ginsburg OM, Dinh NV, To TV, Quang LH, Linh ND, Duong BT, et al. Family History, BRCA Mutations and Breast Cancer in Vietnamese Women. Clin Genet (2011) 80:89–92. doi: 10.1111/j.1399-0004.2010.01545.x
27. Sung PL, Wen KC, Chen YJ, Chao TC, Tsai YF, Tseng LM, et al. The Frequency of Cancer Predisposition Gene Mutations in Hereditary Breast and Ovarian Cancer Patients in Taiwan: From BRCA1/2 to Multi-Gene Panels. PloS One (2017) 12:e0185615. doi: 10.1371/journal.pone.0185615
28. di Masi A, Gullotta F, Cappadonna V, Leboffe L, Ascenzi P. Cancer Predisposing Mutations in BRCT Domains. IUBMB Life (2011) 63:503–12. doi: 10.1002/iub.472
29. Rosenthal SH, Sun W, Zhang K, Liu Y, Nguyen Q, Gerasimova A, et al. Development and Validation of a 34-Gene Inherited Cancer Predisposition Panel Using Next-Generation Sequencing. BioMed Res Int (2020) 2020:3289023. doi: 10.1155/2020/3289023
30. Dong H, Chandratre K, Qin Y, Zhang J, Tian X, Rong C, et al. Prevalence of BRCA1/BRCA2 Pathogenic Variation in Chinese Han Population. J Med Genet (2021) 58:565–9. doi: 10.1136/jmedgenet-2020-106970
31. Janavičius R. Founder BRCA1/2 Mutations in the Europe: Implications for Hereditary Breast-Ovarian Cancer Prevention and Control. EPMA J (2010) 1:397–412. doi: 10.1007/s13167-010-0037-y
32. Kowalik A, Siołek M, Kopczyński J, Krawiec K, Kalisz J, Zięba S, et al. BRCA1 Founder Mutations and Beyond in the Polish Population: A Single-Institution BRCA1/2 Next-Generation Sequencing Study. PloS One (2018) 13:e0201086. doi: 10.1371/journal.pone.0201086
33. Hegde M, Ferber M, Mao R, Samowitz W, Ganguly A, Working Group of the American College of Medical Genetics and Genomics (ACMG) Laboratory Quality Assurance. ACMG Technical Standards and Guidelines for Genetic Testing for Inherited Colorectal Cancer (Lynch Syndrome, Familial Adenomatous Polyposis, and MYH-Associated Polyposis). Genet Med (2014) 16:101–16. doi: 10.1038/gim.2013.166
Keywords: hereditary cancer syndrome, pathogenic variant, genetic carrier screening, carrier frequency, BRCA1
Citation: Tran VT, Nguyen ST, Pham XD, Phan TH, Nguyen VC, Nguyen HT, Nguyen HP, Doan PTT, Le TA, Nguyen BT, Jasmine TX, Nguyen DS, Nguyen H-DL, Nguyen NM, Do DX, Tran VU, Nguyen HHT, Le MP, Nguyen YN, Do TTT, Truong DK, Tang HS, Phan M-D, Nguyen H-N, Giang H and Tu LN (2022) Pathogenic Variant Profile of Hereditary Cancer Syndromes in a Vietnamese Cohort. Front. Oncol. 11:789659. doi: 10.3389/fonc.2021.789659
Received: 05 October 2021; Accepted: 09 December 2021;
Published: 05 January 2022.
Edited by:
Daniela Turchetti, University of Bologna, ItalyReviewed by:
Lucas Delmonico, Federal University of Rio de Janeiro, BrazilCopyright © 2022 Tran, Nguyen, Pham, Phan, Nguyen, Nguyen, Nguyen, Doan, Le, Nguyen, Jasmine, Nguyen, Nguyen, Nguyen, Do, Tran, Nguyen, Le, Nguyen, Do, Truong, Tang, Phan, Nguyen, Giang and Tu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lan N. Tu, bGFudHVAZ2VuZXNvbHV0aW9ucy52bg==; Hoa Giang, Z2lhbmdob2FAZ21haWwuY29t; Hoai-Nghia Nguyen, bmhuZ2hpYTgxQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.