 Noa G. Holtzman1,2
Noa G. Holtzman1,2 Michael S. Lebowitz3
Michael S. Lebowitz3 Rima Koka4Maria R. Baer1,5Kanam Malhotra3Amir Shahlaee3Hossein A. Ghanbari3Søren M. Bentzen1,6
Rima Koka4Maria R. Baer1,5Kanam Malhotra3Amir Shahlaee3Hossein A. Ghanbari3Søren M. Bentzen1,6 Ashkan Emadi1,5,7*
Ashkan Emadi1,5,7*- 1Marlene and Stewart Greenebaum Comprehensive Cancer Center, University of Maryland School of Medicine, Baltimore, MD, United States
- 2Immune Deficiency Cellular Therapy Program, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, United States
- 3Sensei Biotherapeutics Inc., Gaithersburg, MD, United States
- 4Department of Pathology, University of Maryland School of Medicine, Baltimore, MD, United States
- 5Department of Medicine, University of Maryland School of Medicine, Baltimore, MD, United States
- 6Department of Epidemiology and Biostatistics, University of Maryland School of Medicine, Baltimore, MD, United States
- 7Department of Pharmacology, University of Maryland School of Medicine, Baltimore, MD, United States
Background: Aspartate β-hydroxylase (ASPH) is an embryonic transmembrane protein aberrantly upregulated in cancer cells, associated with malignant transformation and, in some reports, with poor clinical prognosis.
Objective: To report the expression patterns of ASPH in acute myeloid leukemia (AML).
Methods: Cell surface expression of ASPH was measured via 8-color multiparameter flow cytometry in 41 AML patient samples (31 bone marrow, 10 blood) using fluorescein isothiocyanate (FITC)-conjugated anti-ASPH antibody, SNS-622. A mean fluorescent intensity (MFI) of 10 was used as a cutoff for ASPH surface expression positivity. Data regarding patient and disease characteristics were collected.
Results: ASPH surface expression was found on AML blasts in 16 samples (39%). Higher ASPH expression was seen in myeloblasts of African American patients (p=0.02), but no correlation was found between ASPH expression and other patient or disease characteristics. No association was found between ASPH status and CR rate (p=0.53), EFS (p=0.87), or OS (p=0.17).
Conclusions: ASPH is expressed on blasts in approximately 40% of AML cases, and may serve as a new therapeutically targetable leukemia-associated antigen.
Introduction
Aspartate β-hydroxylase (ASPH) is an α-ketoglutarate-dependent dioxygenase that promotes cellular growth, motility and adhesion by post-translational hydroxylation of aspartyl and asparaginyl residues in epidermal growth factor-like protein domains, including Notch, Notch homologs, Jagged and extracellular matrix molecules such as laminin and tenascin (1, 2). ASPH is encoded by the aspartate beta-hydroxylase (ASPH) gene on chromosome 8 and is upregulated by insulin and insulin growth factor 1 (IGF1) through the MAPK/ERK and PI3K/AKT pathways (2, 3). ASPH can lead to carcinogenesis by inducing decreased cleavage of caspase-3, causing inhibition of apoptosis (4), and may also promote tumor immune escape via inhibition of natural killer (NK)-cell activity (5).
ASPH is highly expressed during fetal development and is aberrantly upregulated in cancer cells (6). ASPH is overexpressed in over 20 different solid neoplasms, including liver (7–10), breast (11), lung (12), brain (13), pancreatic (14), gastric (15) and colorectal cancers (16), in which it propagates a malignant phenotype, associated with increased cell proliferation, invasiveness, metastasis, and also with poor clinical prognosis (7, 8, 17–19).
ASPH has been shown to be immunogenic in preclinical studies exploring its role as a target for vaccination (20, 21) and for dendritic cell therapy (22), making it a promising immunotherapeutic target (23–25). ASPH is currently being targeted with an anti-ASPH nanoparticle vaccine, SNS-301, in a clinical trial in prostate cancer (26).
Despite the established role of ASPH in solid neoplasms, little is known about its role in hematologic malignancies. Acute myeloid leukemia (AML) is a heterogeneous hematologic malignancy with an incidence of 4.3 per 100,000 in the US and a 5-year survival rate of only 24% (27). New treatment options are needed for AML and much interest has shifted toward immunotherapeutic strategies in treatment of AML, necessitating identification of leukemia-associated antigens. Studies have demonstrated overexpression of ASPH in the AML cell line MOLM-14 in vitro, and successful targeting of myeloblasts with anti-ASPH radiolabeled or cytotoxin-linked antibody drug-conjugates (ADCs) (28, 29).
ASPH may have the potential to serve as a tumor- or leukemia-associated antigen for immunotherapy. In an effort to further characterize ASPH as a therapeutic target in AML, we report here the first study of ASPH expression in AML patient samples.
Materials and Methods
Patient Samples
Bone marrow (BM) aspirate and peripheral blood (PB) samples were collected from AML patients treated at the University of Maryland Greenebaum Comprehensive Cancer Center (2014-2018) on a University of Maryland School of Medicine (UMSOM) Institutional Review Board (IRB)-approved institutional tissue procurement protocol. Mononuclear cells isolated by density centrifugation were viably cryopreserved at -80°C in RPMI 1640 with 20% fetal calf serum and 5% dimethyl sulfoxide (DMSO). The study was approved by the UMSOM IRB and was conducted in accordance with the principles of the Declaration of Helsinki.
ASPH Expression
AML BM and PB samples were analyzed for cell surface expression of ASPH with the fluorescein isothiocyanate (FITC)-conjugated anti-ASPH antibody SNS-622 using 8-color flow cytometry on a MACSQuant® Analyzer 10 flow cytometer (Miltenyi Biotec GmbH, Germany). Two panels of 8 antibodies were used. Panel 1: FITC-SNS-622, VioBlue-CD45, VioGreen-CD33, PE-CD34, PEVio770-CD19, APC-CD13 or APC-CD38, APCVio770-CD117. Panel 2: FITC-SNS-622, VioBlue-CD45, VioGreen-CD20, PE-CD34, PEVio770-HLA-DR, APC-CD3, APCVio770-CD64 (Miltenyi Biotec GmbH, Germany). PE-CD14 and APCVio770-CD64 were substituted in Panel 2 for AMLs with monocytic lineage. Propidium iodide (PI) PerCP770 (Miltenyi Biotec GmbH, Germany) was used in both panels to assess cell viability. The original immunophenotype of the blast population as determined by hematopathologist review in the University of Maryland Pathology Laboratory [certified by Clinical Laboratory Improvement Amendments (CLIA) and accredited by the College of American Pathologists (CAP)] using CD45, CD34, CD13, CD33, CD117, HLA-DR, CD14, CD64 antibodies to define the blast population in each case. Expression of ASPH was analyzed by two independent reviewers using FlowLogic™ software (Inivai Technologies, Melbourne, Australia).
Clinical Data
Data regarding patient and disease characteristics, including karyotype and myeloid mutations, treatment and outcomes were collected (Table 1). Risk category was classified as favorable, intermediate, or unfavorable based on European LeukemiaNet (ELN) 2017 criteria (30).
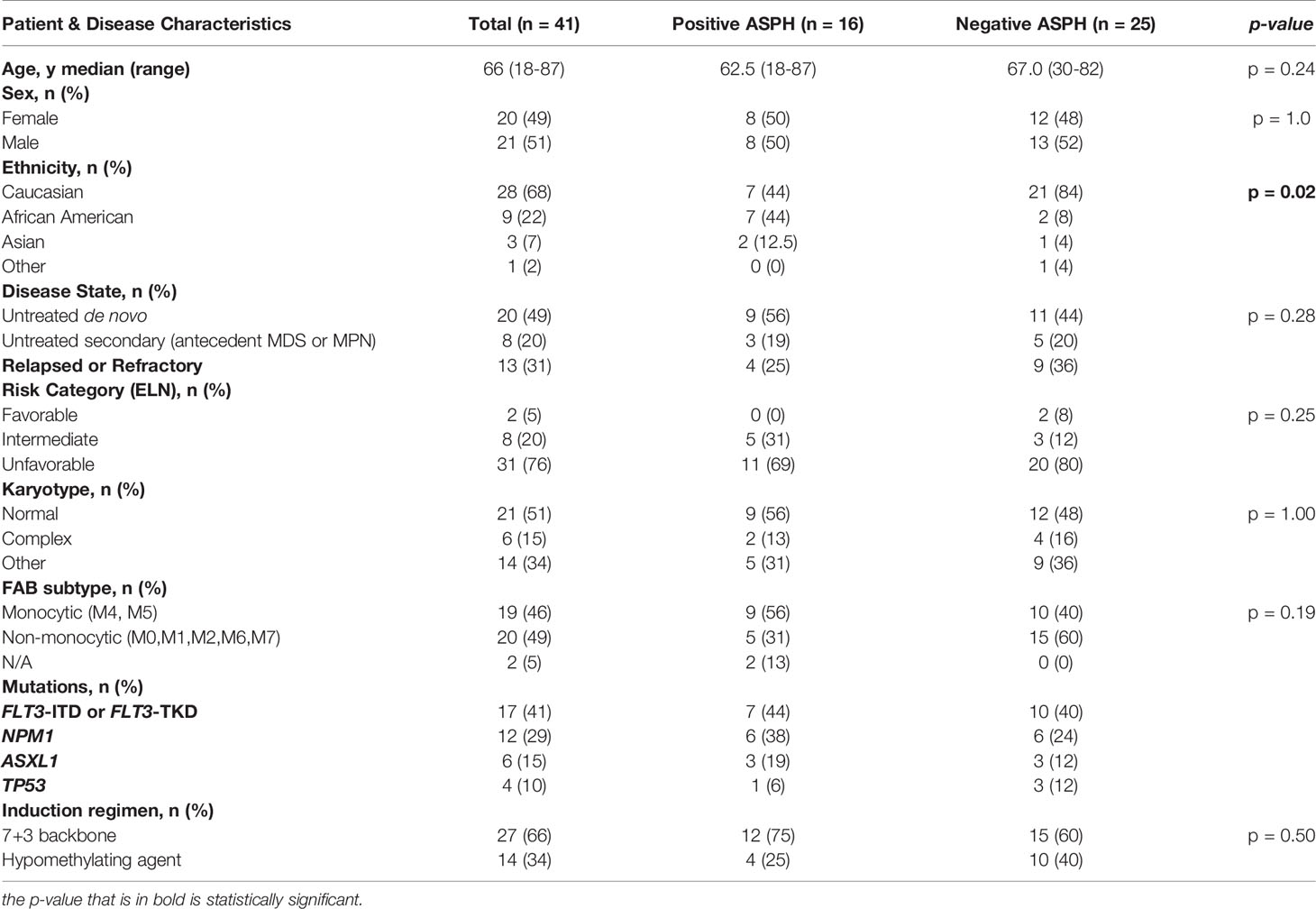
Table 1 Patient and disease haracteristics.
Treatment outcomes included (1) complete remission (CR) - defined as less than 5% bone marrow blasts (as detected by immunohistochemistry on core biopsy) and no evidence of disease elsewhere with packed red blood cell transfusion independence, absolute neutrophil count (ANC) ≥1x109/L and platelet count ≥100x109/L; (2) CRi – fulfills criteria for CR but with incomplete count recovery, or (3) induction failure. Overall survival (OS) was calculated from the time of diagnosis to the time of death or censored at the time of last contact in patients still alive. Event-free survival (EFS) was calculated from the time of AML diagnosis until induction failure, relapse, or death from any cause; patients alive without disease were censored at the time of last follow-up.
Statistical Analysis
Statistical analysis was conducted using IBM® SPSS® Statistics for Windows, release 25.0.0 (IBM Corp., Armonk, N.Y., USA). Visual inspection of the distribution of ASPH expression data on myeloblast or monoblast surface within the whole cell population was used to identify a robust cut-point separating high (i.e., positive) from low (i.e., negative) ASPH expression. Cohen’s kappa (k) was used to quantify the agreement between two independent observers on classification into ASPH-positive vs. -negative disease. The distribution of ASPH positivity in various subgroups of patients was analyzed using Pearson’s chi-square test or, for 2x2 tables, Fisher’s exact test. OS and EFS were estimated using the Kaplan-Meier estimator and compared between ASPH-positive and -negative groups using the Mantel-Cox log-rank test.
Results
Patient Characteristics
AML patients were evaluated, including 31 BM and 10 PB (Table 1). Median patient age was 66 years (range, 18-87 years), 49% (n=20) were female, 68% (n=28) Caucasian and 22% (n=9) African American. Disease status was untreated de novo in 49%, untreated secondary from an antecedent myelodysplastic syndrome (MDS) or myeloproliferative neoplasm (MPN) in 20%, and relapsed/refractory in 31%. Samples were cytogenetically and molecularly diverse, including 51% with normal karyotype and 15% with complex karyotype; 41% had FMS-like tyrosine kinase 3 internal tandem duplication (FLT3-ITD) or FLT3 tyrosine kinase domain (TKD) mutations, 29% nucleophosmin 1 (NPM1), and 10% TP53 mutations. Most patients (76%) had unfavorable risk disease per ELN-2017 risk criteria. Induction therapy for 66% of patients included a 7 + 3 cytarabine plus anthracycline backbone, and the remainder (34%) were treated with hypomethylating agents (HMAs; azacitidine or decitabine). Fourteen patients (34%) underwent consolidative allogeneic hematopoietic stem cell transplant (HSCT) (Table 2).

Table 2 Treatment response and clinical outcomes.
ASPH Expression
ASPH was expressed on AML blasts in 39% of samples (n=16; 13 BM, 3 PB). Expression data for the whole patient population showed a ‘mixed population’, i.e. a clustering of patients with low or zero expression mixed with patients with stronger expression, which determined a mean fluorescent intensity (MFI) of 10 as the cutoff for ASPH surface expression positivity, identifying a robust cut-point separating high (i.e., positive) from low (i.e., negative) ASPH expression (Figure 1). Blinded independent review of the data produced a Cohen’s κ of 0.74 (SE of +/- 0.11).
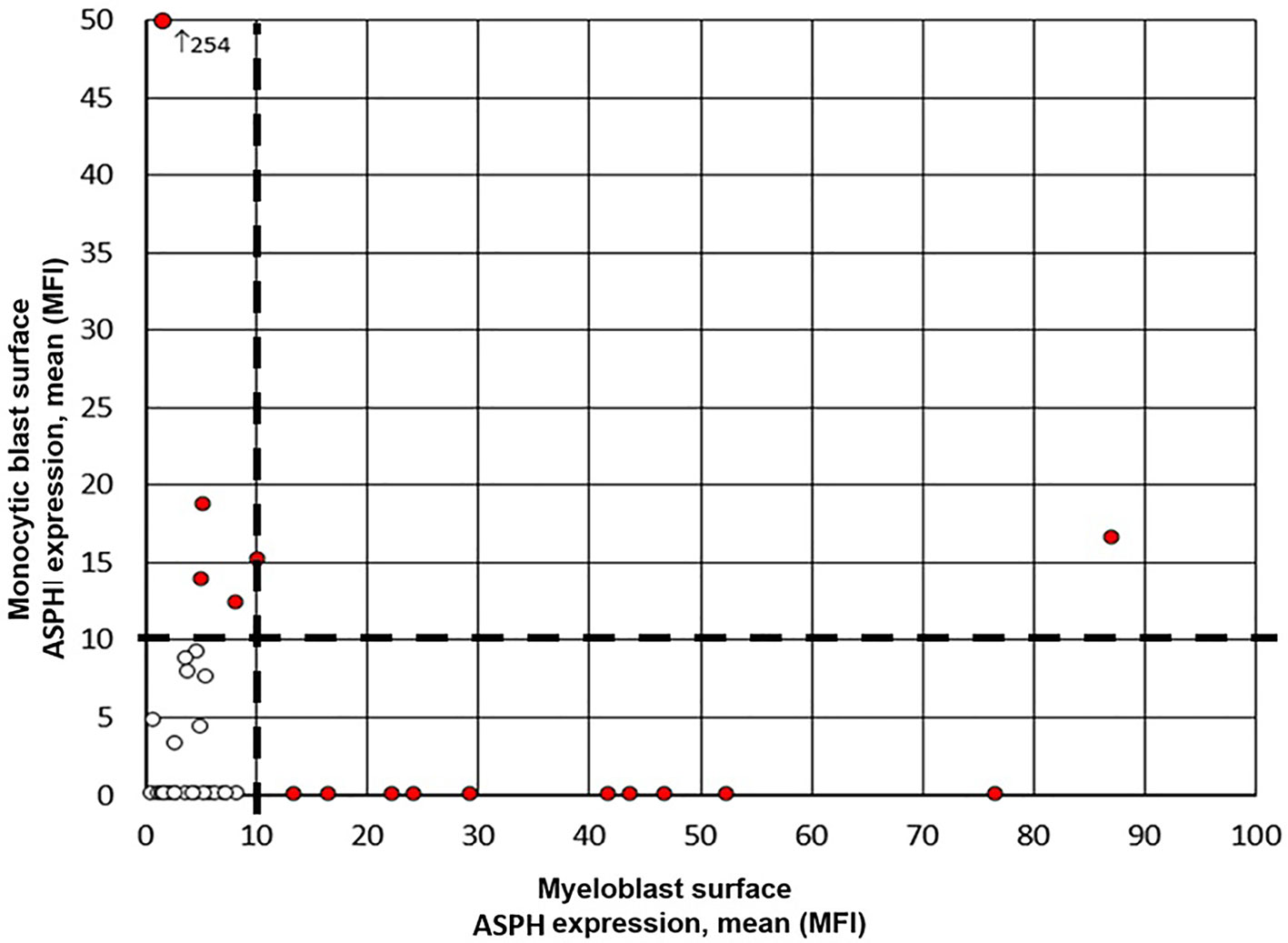
Figure 1 ASPH surface expression on myeloblasts and monoblasts. Expression data for the whole patient population showed a ‘mixed population’, i.e. a clustering of patients with low or zero expression mixed with patients with stronger expression, which was used to identify a robust cut-point of 10 MFI (black dashed line) separating high (i.e., positive, red circles) from low (i.e., negative, white circles) mean ASPH expression on myeloblast (x-axis) or monoblast (y-axis) surface.
ASPH expression was seen only on the surface of blasts, and not on any other cells. Thirteen patients had two populations of blasts as a characteristic of their disease, both myelo- and monoblasts. ASPH expression was higher in monoblasts than in myeloblasts in 11 of these paired values. This difference was statistically significant (p=0.03, Wilcoxon Signed Rank Test). The mean expression per MFI was 27.3 in monoblasts vs 14.1 in myeloblasts in these 13 cases. Patients with AML with ASPH expression were clinically heterogeneous. Higher ASPH expression was seen in myeloblasts of African American patients in our cohort (p=0.02). No correlation was found between ASPH expression and the following variables: sex, ELN risk category, cytogenetics, de novo versus secondary AML classification, monocytic FAB status, and type of induction therapy (Table 1).
Clinical Outcomes
Twenty patients (49%) achieved CR or CRi, including 9 (56%) with ASPH expression. No association was found between ASPH status and achievement of CR (p = 0.53). Sixteen patients (39%) had primary refractory disease, including 6 (38%) with ASPH expression (Table 2). Median EFS was 7.3 months, with no difference based on ASPH status (median EFS for ASPH-positive vs. ASPH-negative patients, 6.5 vs. 7.3 months, p=0.87) (Figure 2). When stratified by disease state at diagnosis, among the 13 patients with relapsed/refractory (R/R) disease, 31% (n=4) were ASPH positive (Table 1). ASPH positivity was not significantly associated with OS (p=0.71) or EFS (p=0.85) among the R/R cohort. Among 28 patients with newly diagnosed or secondary AML, 43% (n=12) were ASPH positive. Again, in this subgroup analysis, ASPH status was also not significantly associated with OS (p=0.16) or EFS (p=0.39).
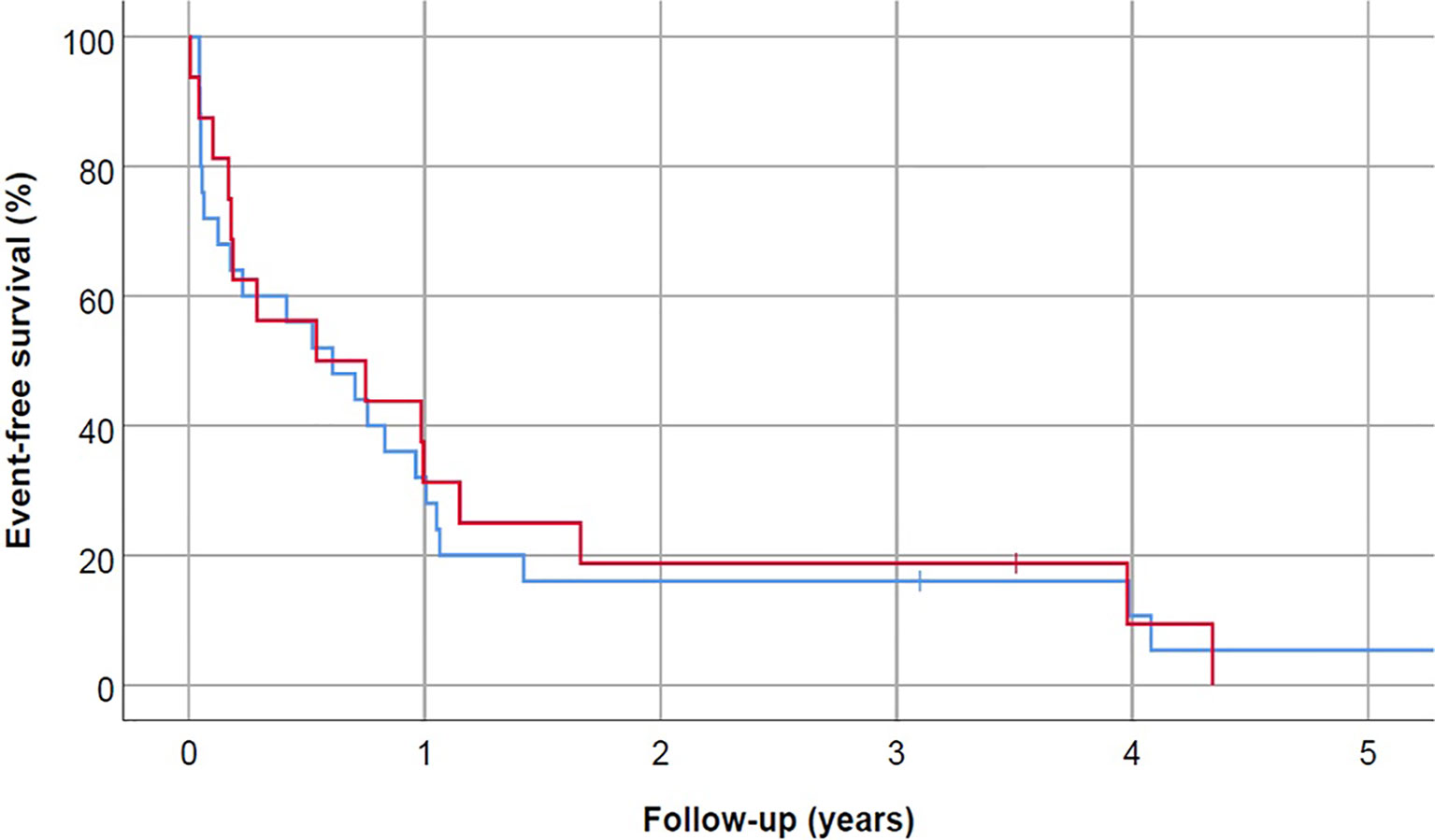
Figure 2 Event-free survival did not correlate with ASPH status (p=0.87). Blue line represents ASPH- negative AML patients and red line is ASPH-positive AML patients.
Median OS for our cohort was 13.1 months, with no difference based on ASPH expression (median OS for ASPH-positive vs. ASPH-negative, 18.5 vs. 12.0 months, p=0.169) (Figure 3). At the time of analysis, 9 patients (22%) were alive, including 6 (67%) who underwent HSCT.
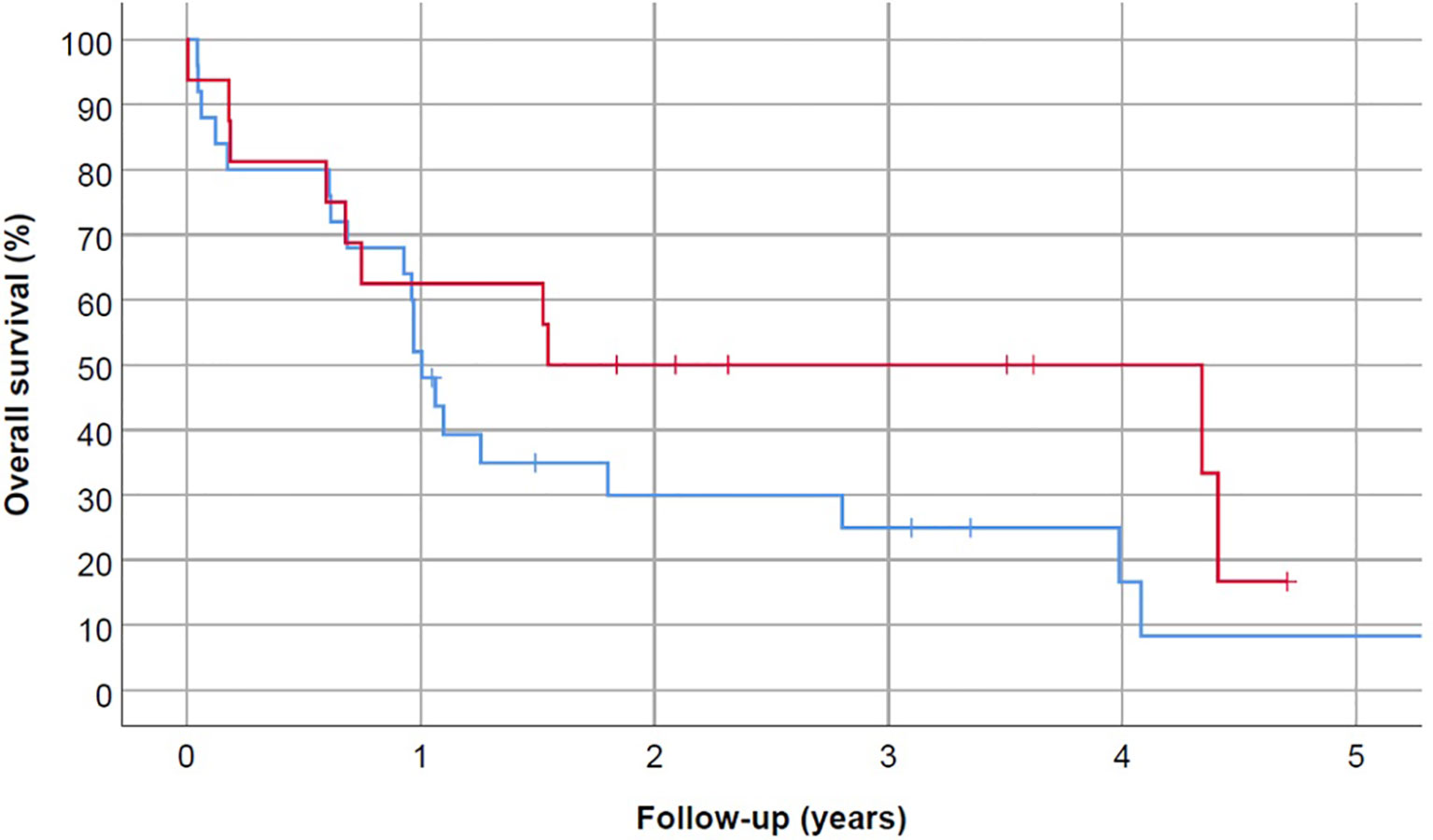
Figure 3 Overall survival did not correlate with ASPH status (p=0.169). Blue line represents ASPH-negative AML patients and red line is ASPH-positive AML patients. Patients were censored at the time of death, loss to follow-up, or HSCT.
Discussion
ASPH was overexpressed on blasts of approximately 40% of AML patients in this series. While not appearing to be associated with any specific disease features or with clinical prognosis, this surface expression serves as a potential new therapeutic target for AML.
Discovery of new therapeutic targets in AML remains imperative. Specifically, new treatments are needed for patients with relapsed/refractory disease or those who are unfit for intensive cytotoxic chemotherapy. Immunotherapeutic strategies using ADCs, bispecific T-cell engagers (BiTEs), and chimeric antigen receptor (CAR) T-cell therapy have shown great success in B-cell lymphoid leukemia and lymphoma due to the consistently expressed, safe and effective targets CD19 and/or CD22 (31–34). However, progress for AML has lagged because of lack of a selective leukemia-associated target. Therefore, much interest has been focused on discovery of new tumor- or leukemia-associated antigens, such as ASPH.
ASPH is a safe therapeutic target due to its inherent embryonic function, which is not required for healthy adult human function (barring its possible role in pregnancy) (35, 36). Mutations in the ASPH gene lead to Traboulsi Syndrome in humans, reported in four families in the literature. This syndrome is characterized by developmental defects including facial dysmorphism and ophthalmologic abnormalities such as lens dislocation and anterior-segment abnormalities. Most importantly, monitoring of these patients has shown that the loss of ASPH function has not been associated with disease later in life (37).
ASPH is further a promising target due to its immunogenicity. When expressed, ASPH is found at high levels on the cell surface plasma membrane, where its N-terminal sequences and the catalytic site located in the C-terminal region have been shown to serve as antigens that are accessible to the immune system (21). In preclinical studies, vaccination is capable of inducing ASPH epitope-specific CD4+ and CD8+ T-cell responses in both animal and human models of hepatocellular carcinoma (26). Dendritic cell vaccination studies in a rodent model of biliary cancer showed successful passive vaccination with naïve dendritic cells that were matured in vivo in the presence of ASPH, leading to tumor regression, along with ASPH-specific T-cell responses (25). ASPH is also thought to lead to immune surveillance escape and promotes tumor growth by direct effects on NK-cells, including reducing NK-cell viability and cytotoxicity (5).
Importantly, unlike data in solid tumors that suggest the role of ASPH as a predictive marker of poor clinical prognosis (17–19), we found that ASPH status was not associated with clinical outcomes (CR, EFS, OS) in AML. Further, there was no association seen between ASPH status and cytogenetic abnormality, mutation status, or ELN risk category, though notably the majority (74%) of our patient cohort fell into the unfavorable risk category. This may reflect the limitations of our study, including the relatively small patient cohort and the retrospective nature of our clinical outcome review, along with the significant heterogeneity of AML as a clinical entity. The heterogeneity of AML as seen by various combinations of cytogenetic and molecular characteristics that define disease subsets and control how aggressive the disease can be, is important to consider, as due to the small cohort in this study, this heterogeneity may explain the lack of association found with any significant outcome and begs for further large scale studies. Also, changes can be perhaps seen longitudinally in serial samples of the same patient after treatment, where AML myeloblasts can exhibit changes to surface antigen expression and clonal evolution at times, which would be another interesting angle to explore in future trials and not represented by our study that only included samples at time of diagnosis. Additionally, a further limitation may be that while CR data was available for all patients, measurable residual disease (MRD) status at time of CR based on molecular next-generation sequencing was not available for all given the time period of sample collection, which was partly in the years prior to increasing standardization of MRD and its currently established influence on clinical outcomes.
One hypothesis is that while ASPH plays an important role in cancer cell metastasis in solid neoplasms, including cellular detachment, migration, and adhesion at a distant site (19), circulating tumor cells such as leukemic blasts do not need a seeding advantage in order to exert their deleterious effects that lead to poor prognosis. Further investigation regarding a possible relationship between ASPH expression and extramedullary disease in AML would be interesting to explore in future studies. While higher expression of ASPH has been reported in some cancer stem cells such as glioma stem cells (38), its expression on leukemia stem cells (LSC) is not well described. Another question of interest in study of ASPH in leukemia, specifically, includes whether ASPH is differentially expressed in leukemia stem cells compared to more differentiated leukemia blasts, and while this study did not address this question – there has been much study into genes that play a role in stemness for AML. One such study pursuing the development of predictive and/or prognostic biomarkers related to stemness, Ng et al. generated a list of genes that are differentially expressed between 138 LSC positive (LSC+) and 89 LSC− cell fractions from 78 AML patients validated by xenotransplantation. They generated a 17-gene LSC score (LSC17). ASPH was not among the 17 signature genes, which were GPR56, AKR1C3, CD34, NGFRAP1, EMP1, SMIM24, SOCS2, CPXM1, CDK6, KIAA0125, DPYSL3, MMRN1, LAPTM4B, ARHGAP22, NYNRIN, ZBTB46, and DNMT3B. Of note, the LSC17 score was highly prognostic in five independent cohorts of approximately 900 AML patients (39).
An additional potentially important finding was the statistically significant higher incidence of ASPH expression on blasts of African American AML patients. It is unknown if this is a pattern seen across other cancers with ASPH expression. Though our relatively small cohort is a limiting factor, this finding should be further explored prospectively and validated. Racial disparities and their effect on clinical outcomes for AML represent an important field of interest that requires more investigation (40, 41).
Lastly, it has been reported that embryonic antigens, such as ASPH, are upregulated by HMAs (42–44). In our patient cohort, approximately one third (34%) of patients who were treated with HMA (alone or in combination with another drug) had ASPH-positive AML at diagnosis. Among these 14 patients, 4 (29%) were secondary AML patients, 4 (21%) were relapsed/refractory AML, and 7 (50%) were newly diagnosed AML. Importantly, for all these patients, the HMA was administered after the collection of the sample that was analyzed for ASPH expression – none received HMA prior. While the decision to use HMAs likely reflects patients’ older age, poor performance status or AML features, such as complex karyotype, HMA use and potential effects on ASPH expression warrant further investigation. Future studies exploring ASPH expression on serial samples in patients who were treated with or without HMAs would be of great interest. Further, there is potential for synergy when using HMAs as they may increase ASPH antigen expression to allow for concurrent targeting of surface ASPH expression with an immunotherapeutic agent.
In summary, ASPH is overexpressed in approximately 40% of AML cases, and can serve as a potential immunotherapeutically targetable tumor-specific antigen. An anti-ASPH nanoparticle vaccine is currently under clinical investigation, having completed Phase 1 testing with encouraging results in solid tumors (29). Additional immunotherapies such as ADCs and CAR T-cells targeting ASPH may be promising potential therapeutic agents for AML.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Maryland School of Medicine (UMSOM) Institutional Review Board (IRB). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Conception: NH, AE, ML, and HG. Interpretation or analysis of data: NH, ML, AE, RK, MB, and SB. Manuscript preparation: NH, AE, ML, RK, MB, KM, AS, HG, and SB. Revision for important intellectual content: NH, AE, ML, RK, MB, and HG. Supervision: AE, ML, RK, and KM. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by funds through the National Cancer Institute–Cancer Center Support Grant (CCSG)–P30CA134274.
Conflict of Interest
Authors ML, KM and AS were employed by company Sensei Biotherapeutics.
ML: Stock ownership in Sensei. AS: Stock ownership in and received consultancy fee from Sensei. HG: Founder and emeritus CSO, Panacea Pharmaceuticals/Sensei Biotherapeutics, Founder/CEO, Athanor Biosciences, MD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lavaissiere L, Jia S, Nishiyama M, de la Monte S, Stern AM, Wands JR, et al. Overexpression of Human Aspartyl(Asparaginyl)Beta-Hydroxylase in Hepatocellular Carcinoma and Cholangiocarcinoma. J Clin Invest (1996) 98(6):1313–23. doi: 10.1172/JCI118918
2. Yang H, Li J, Tang R, Li J, Liu Y, Ye L, et al. The Aspartyl (Asparaginyl) Beta-Hydroxylase in Carcinomas. Front Biosci (Landmark Ed) (2015) 20:902–9. doi: 10.2741/4344
3. Lahousse SA, Carter JJ, Xu XJ, Wands JR, de la Monte SM. Differential Growth Factor Regulation of Aspartyl-(Asparaginyl)-Beta-Hydroxylase Family Genes in SH-Sy5y Human Neuroblastoma Cells. BMC Cell Biol (2006) 7:41. doi: 10.1186/1471-2121-7-41
4. Huang CK, Iwagami Y, Aihara A, Chung W, de la Monte S, Thomas JM, et al. Anti-Tumor Effects of Second Generation β-Hydroxylase Inhibitors on Cholangiocarcinoma Development and Progression. PloS One (2016) 11(3):e0150336. doi: 10.1371/journal.pone.0150336
5. Huyan T, Li Q, Ye LJ, Yang H, Xue XP, Zhang MJ, et al. Inhibition of Human Natural Killer Cell Functional Activity by Human Aspartyl β-Hydroxylase. Int Immunopharmacol (2014) 23(2):452–9. doi: 10.1016/j.intimp.2014.09.018
6. Yang H, Song K, Xue T, Xue XP, Huyan T, Wang W, et al. The Distribution and Expression Profiles of Human Aspartyl/Asparaginyl Beta-Hydroxylase in Tumor Cell Lines and Human Tissues. Oncol Rep (2010) 24(5):1257–64. doi: 10.3892/or_00000980
7. Maeda T, Taguchi K, Aishima S, Shimada M, Hintz D, Larusso N, et al. Clinicopathological Correlates of Aspartyl (Asparaginyl) Beta-Hydroxylase Over-Expression in Cholangiocarcinoma. Cancer Detect Prev (2004) 28(5):313–8. doi: 10.1016/j.cdp.2004.06.001
8. de la Monte SM, Tamaki S, Cantarini MC, Ince N, Wiedmann M, Carter JJ, et al. Aspartyl-(Asparaginyl)-Beta-Hydroxylase Regulates Hepatocellular Carcinoma Invasiveness. J Hepatol (2006) 44(5):971–83. doi: 10.1016/j.jhep.2006.01.038
9. Iwagami Y, Huang CK, Olsen MJ, Thomas JM, Jang G, Kim M, et al. Aspartate β-Hydroxylase Modulates Cellular Senescence Through Glycogen Synthase Kinase 3β in Hepatocellular Carcinoma. Hepatology (2016) 63(4):1213–26. doi: 10.1002/hep.28411
10. Xue T, Su J, Li H, Xue X. Evaluation of HAAH/humbug Quantitative Detection in the Diagnosis of Hepatocellular Carcinoma. Oncol Rep (2015) 33(1):329–37. doi: 10.3892/or.2014.3606
11. Shimoda M, Hori A, Wands JR, Tsunashima R, Naoi Y, Miyake T, et al. Endocrine Sensitivity of Estrogen Receptor-Positive Breast Cancer is Negatively Correlated With Aspartate-β-Hydroxylase Expression. Cancer Sci (2017) 108(12):2454–61. doi: 10.1111/cas.13416
12. Luu M, Sabo E, de la Monte SM, Greaves W, Wang J, Tavares R, et al. Prognostic Value of Aspartyl (Asparaginyl)-Beta-Hydroxylase/Humbug Expression in non-Small Cell Lung Carcinoma. Hum Pathol (2009) 40(5):639–44. doi: 10.1016/j.humpath.2008.11.001
13. Sturla LM, Tong M, Hebda N, Gao J, Thomas JM, Olsen M, et al. Aspartate-β-Hydroxylase (ASPH): A Potential Therapeutic Target in Human Malignant Gliomas. Heliyon (2016) 2(12):e00203. doi: 10.1016/j.heliyon.2016.e00203
14. Hou G, Xu B, Bi Y, Wu C, Ru B, Sun B, et al. Recent Advances in Research on Aspartate β-Hydroxylase (ASPH) in Pancreatic Cancer: A Brief Update. Bosn J Basic Med Sci (2018) 18(4):297–304. doi: 10.17305/bjbms.2018.3539
15. Lee JH. Overexpression of Humbug Promotes Malignant Progression in Human Gastric Cancer Cells. Oncol Rep (2008) 19(3):795–800. doi: 10.3892/or.19.3.795
16. Wang J, de la Monte SM, Sabo E, Kethu S, Tavares R, Branda M, et al. Prognostic Value of Humbug Gene Overexpression in Stage II Colon Cancer. Hum Pathol (2007) 38(1):17–25. doi: 10.1016/j.humpath.2006.07.009
17. Ince N, de la Monte SM, Wands JR. Overexpression of Human Aspartyl (Asparaginyl) Beta-Hydroxylase is Associated With Malignant Transformation. Cancer Res (2000) 60(5):1261–6.
18. Wang K, Liu J, Yan ZL, Li J, Shi LH, Cong WM, et al. Overexpression of Aspartyl-(Asparaginyl)-Beta-Hydroxylase in Hepatocellular Carcinoma is Associated With Worse Surgical Outcome. Hepatology (2010) 52(1):164–73. doi: 10.1002/hep.23650
19. Zou Q, Hou Y, Wang H, Wang K, Xing X, Xia Y, et al. Hydroxylase Activity of ASPH Promotes Hepatocellular Carcinoma Metastasis Through Epithelial-To-Mesenchymal Transition Pathway. EBioMedicine (2018) 31:287–98. doi: 10.1016/j.ebiom.2018.05.004
20. Biswas B, Stewart S, Malhotra K, Lebowitz M, Fuller S, Merril C, et al. Design, Development and Production of Nano-Particle-Based Anticancer Vaccine Targeting Human Aspartyl (Asparaginyl) B-Hydroxylase (HAAH). J Immunother Cancer (2013) 1(Suppl 1):P201. doi: 10.1186/2051-1426-1-S1-P201
21. Iwagami Y, Casulli S, Nagaoka K, Kim M, Carlson RI, Ogawa K, et al. Lambda Phage-Based Vaccine Induces Antitumor Immunity in Hepatocellular Carcinoma. Heliyon (2017) 3(9):e00407. doi: 10.1016/j.heliyon.2017.e00407
22. Noda T, Shimoda M, Ortiz V, Sirica AE, Wands JR. Immunization With Aspartate-β-Hydroxylase-Loaded Dendritic Cells Produces Antitumor Effects in a Rat Model of Intrahepatic Cholangiocarcinoma. Hepatology (2012) 55(1):86–97. doi: 10.1002/hep.24629
23. Tomimaru Y, Mishra S, Safran H, Charpentier KP, Martin W, De Groot AS, et al. Aspartate-β-Hydroxylase Induces Epitope-Specific T Cell Responses in Hepatocellular Carcinoma. Vaccine (2015) 33(10):1256–66. doi: 10.1016/j.vaccine.2015.01.037
24. Yeung YA, Finney AH, Koyrakh IA, Lebowitz MS, Ghanbari HA, Wands JR, et al. Isolation and Characterization of Human Antibodies Targeting Human Aspartyl (Asparaginyl) Beta-Hydroxylase. Hum Antibodies (2007) 16(3-4):163–76. doi: 10.3233/HAB-2007-163-410
25. Shimoda M, Tomimaru Y, Charpentier KP, Safran H, Carlson RI, Wands J. Tumor Progression-Related Transmembrane Protein Aspartate-β-Hydroxylase is a Target for Immunotherapy of Hepatocellular Carcinoma. J Hepatol (2012) 56(5):1129–35. doi: 10.1016/j.jhep.2011.12.016
26. Nordquist LT, Ghanbari H, Elist JJ, Oliver JC, Gannon W, Shahlaee A, et al. Final Results From a Phase I Clinical Trial Evaluating the Safety, Immunogenicity, and Anti-Tumor Activity of SNS-301 in Men With Biochemically Relapsed Prostate Cancer. Ann Oncol (2018) 29(Supplement 8):viii136. doi: 10.1093/annonc/mdy279.404
27. Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM. Epidemiology of Acute Myeloid Leukemia: Recent Progress and Enduring Challenges. Blood Rev (2019) 36:70–87. doi: 10.1016/j.blre.2019.04.005
28. Lebowitz MS, Revskaya E, Malhotra K, Shahlaee A, Fuller S, Baer MR, et al. Radioimmunotherapy for Acute Myeloid Leukemia Targeting Human Aspartyl (Asparaginyl) β-Hydroxylase [Abstract]. In: Proceedings of the American Association for Cancer Research Annual Meeting 2017, vol. 77. Washington, DC. Philadelphia (PA: AACR; Cancer Res (2017). p. Abstract nr 2650.
29. Malhotra K, Walker S, Fang C, Birthare K, Lebowitz MS, Fuller S, et al. Antibody-Drug Conjugates Targeted at Human Aspartyl (Asparaginyl) β-Hydroxylase [Abstract]. In: Proceedings of the AACR-NCI-EORTC International Conference: Molecular Targets and Cancer Therapeutics; 2017 Oct 26-30; Philadelphia, PA. Philadelphia (PA): AACR; Mol Cancer Ther (2018) 17(1 Suppl):Abstract nr B106.
30. Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, Büchner T, et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations From an International Expert Panel. Blood (2017) 129(4):424–47. doi: 10.1182/blood-2016-08-733196
31. Kantarjian HM, DeAngelo DJ, Stelljes M, Liedtke M, Stock W, Gökbuget N, et al. Inotuzumab Ozogamicin Versus Standard of Care in Relapsed or Refractory Acute Lymphoblastic Leukemia: Final Report and Long-Term Survival Follow-Up From the Randomized, Phase 3 INO-VATE Study. Cancer (2019) 125(14):2474–87. doi: 10.1002/cncr.32116
32. Kantarjian H, Stein A, Gökbuget N, Fielding AK, Schuh AC, Ribera JM, et al. Blinatumomab Versus Chemotherapy for Advanced Acute Lymphoblastic Leukemia. N Engl J Med (2017) 376:836–47. doi: 10.1056/NEJMoa1609783
33. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in Children and Young Adults With B-Cell Lymphoblastic Leukemia. N Engl J Med (2018) 378(5):439–48. doi: 10.1056/NEJMoa1709866
34. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med (2017) 377(26):2531–44. doi: 10.1056/NEJMoa1707447
35. Gundogan F, Elwood G, Greco D, Rubin LP, Pinar H, Carlson RI, et al. Role of Aspartyl-(Asparaginyl) Beta-Hydroxylase in Placental Implantation: Relevance to Early Pregnancy Loss. Hum Pathol (2007) 38(1):50–9. doi: 10.1016/j.humpath.2006.06.005
36. Dinchuk JE, Focht RJ, Kelley JA, Henderson NL, Zolotarjova NI, Wynn R, et al. Absence of Post-Translational Aspartyl Beta-Hydroxylation of Epidermal Growth Factor Domains in Mice Leads to Developmental Defects and an Increased Incidence of Intestinal Neoplasia. J Biol Chem (2002) 277(15):12970–7. doi: 10.1074/jbc.M110389200
37. Patel N, Khan AO, Mansour A, Mohamed JY, Al-Assiri A, Haddad R, et al. Mutations in ASPH Cause Facial Dysmorphism, Lens Dislocation, Anterior-Segment Abnormalities, and Spontaneous Filtering Blebs, or Traboulsi Syndrome. Am J Hum Genet (2014) 94(5):755–9. doi: 10.1016/j.ajhg.2014.04.002
38. Sturla LM, Tong M, Hebda N, Gao J, Thomas JM, Olsen M, et al. Aspartate-β-Hydroxylase (ASPH): A Potential Therapeutic Target in Human Malignant Gliomas. Heliyon (2016) 2(12):e00203. doi: 10.1016/j.heliyon.2016.e00203
39. Ng SW, Mitchell A, Kennedy JA, Chen WC, McLeod J, Ibrahimova N, et al. A 17-Gene Stemness Score for Rapid Determination of Risk in Acute Leukaemia. Nature (2016) 540(7633):433–7. doi: 10.1038/nature20598
40. Utuama O, Mukhtar F, Pham YT, Dabo B, Manani P, Moser J, et al. Racial/ethnic, Age and Sex Disparities in Leukemia Survival Among Adults in the United States During 1973-2014 Period. PloS One (2019) 14(8):e0220864. doi: 10.1371/journal.pone.0220864
41. Bhatnagar B, Kohlschmidt J, Mrózek K, Zhao Q, Fisher JL, Nicolet D, et al. Poor Survival and Differential Impact of Genetic Features of Black Patients With Acute Myeloid Leukemia. Cancer Discov (2021) 11(3):626–37. doi: 10.1158/2159-8290.CD-20-1579
42. Almstedt M, Blagitko-Dorfs N, Duque-Afonso J, Karbach J, Pfeifer D, Jäger E, et al. The DNA Demethylating Agent 5-Aza-2’-Deoxycytidine Induces Expression of NY-ESO-1 and Other Cancer/Testis Antigens in Myeloid Leukemia Cells. Leuk Res (2010) 34(7):899–905. doi: 10.1016/j.leukres.2010.02.004
43. Ortmann CA, Eisele L, Nückel H, Klein-Hitpass L, Führer A, Dührsen U, et al. Aberrant Hypomethylation of the Cancer-Testis Antigen PRAME Correlates With PRAME Expression in Acute Myeloid Leukemia. Ann Hematol (2008) 87(10):809–18. doi: 10.1007/s00277-008-0514-8
Keywords: leukemia, myeloid, myeloblasts, ASPH, leukemia-associated antigen
Citation: Holtzman NG, Lebowitz MS, Koka R, Baer MR, Malhotra K, Shahlaee A, Ghanbari HA, Bentzen SM and Emadi A (2021) Aspartate β-Hydroxylase (ASPH) Expression in Acute Myeloid Leukemia: A Potential Novel Therapeutic Target. Front. Oncol. 11:783744. doi: 10.3389/fonc.2021.783744
Received: 26 September 2021; Accepted: 01 December 2021;
Published: 22 December 2021.
Edited by:
Joshua Zeidner, University of North Carolina at Chapel Hill, United StatesReviewed by:
Maria Helena Ornellas, Universidade Estadual do Rio de Janeiro, BrazilMichael Richard Grunwald, Levine Cancer Institute, United States
Matthew Foster, University of North Carolina at Chapel Hill, United States
Copyright © 2021 Holtzman, Lebowitz, Koka, Baer, Malhotra, Shahlaee, Ghanbari, Bentzen and Emadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashkan Emadi, YWVtYWRpQHVtbS5lZHU=