 Fahimeh Attarian1†‡
Fahimeh Attarian1†‡ Farzad Taghizadeh-Hesary2‡
Farzad Taghizadeh-Hesary2‡ Azar Fanipakdel3†
Azar Fanipakdel3† Seyed Alireza Javadinia4*†
Seyed Alireza Javadinia4*† Pejman Porouhan5
Pejman Porouhan5 Babak PeyroShabany6†Danial Fazilat-Panah7†
Babak PeyroShabany6†Danial Fazilat-Panah7†- 1Department of Public Health, School of Health, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran
- 2Department of Radiation Oncology, Shahid Beheshti University of Medical Sciences, Tehran, Iran
- 3Cancer Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
- 4Vasei Clinical Research Development Unit, Sabzevar University of Medical Sciences, Sabzevar, Iran
- 5Department of Radiation Oncology, Sabzevar University of Medical Sciences, Sabzevar, Iran
- 6Department of Internal Medicine, Sabzevar University of Medical Sciences, Sabzevar, Iran
- 7Cancer Research Center, Babol University of Medical Sciences, Babol, Iran
Background: In newly diagnosed glioblastoma, radiation with concurrent and adjuvant (six cycles) temozolomide (TMZ) is the established standard of postsurgical care. However, the benefit of extending adjuvant TMZ therapy beyond six cycles has remained unknown.
Methods: We searched PubMed, Web of Science, Scopus, and Embase up to October 1, 2021. The search keywords were “glioblastoma,” “adjuvant chemotherapy,” and their synonyms. The data of randomized clinical trials were extracted and included in this meta-analysis if they had reported patients’ median overall survival (OS) or median progression-free survival (PFS). The standard and extended chemotherapy regimens were considered as adjuvant TMZ up to six cycles and beyond six cycles (up to a total of 12 cycles), respectively. The median OS and median PFS were pooled and compared.
Results: Four studies consisting of 882 patients (461 patients for the standard chemotherapy group and 421 patients for the extended chemotherapy group) were included in this meta-analysis. The extended TMZ regimen was associated with a nonsignificant improvement in PFS [12.0 months (95% CI 9.0 to 15.0) vs. 10.0 months (95% CI 7.0 to 12.0), P = 0.27] without corresponding improvement in OS [23.0 months (95% CI 19.0 to 27.0) and 24.0 months (95% CI 20.0 to 28.0), P = 0.73].
Conclusions: In newly diagnosed glioblastoma, continuing adjuvant TMZ beyond six cycles did not shown an increase neither in PFS nor OS.
1 Introduction
Glioblastoma is the most common primary brain tumor of glial origin in adults. It is characterized by rapid progression, a high recurrence rate, and a dismal prognosis (1–3). Historically, the management of glioblastoma was maximal safe surgical resection (MSR) followed by radiotherapy. In the early 21st century, a large randomized clinical trial (RCT) converted the standard of care to MSR, adjuvant chemoradiotherapy (CRT) [with concurrent temozolomide (TMZ), an oral alkylating agent], followed by TMZ for six cycles (4). Dismal prognosis of glioblastoma brought up the extended adjuvant TMZ (ext-TMZ) and changed the clinical practice to continue adjuvant TMZ up to 12 cycles or until tumor progression. Since then, numerous studies have attempted to compare the ext-TMZ and the standard Stupp protocol (std-TMZ). However, there is still no consensus on the duration of adjuvant TMZ (5).
In the English literature, there are several studies as case report (6), cohort study (7–18), clinical trial (19–24), and review article (5, 25, 26) assessing the potential benefits of ext-TMZ in patients with glioblastoma. In a pooled analysis of four RCTs (4, 21, 27, 28), the authors concluded that ext-TMZ did not improve the overall survival (OS) of patients with glioblastoma (26). This study did not include three recent RCTs (19, 20, 23). On the other hand, two other meta-analyses noted the improved OS and progression-free survival (PFS) with ext-TMZ (5, 25). These findings might be biased by their search strategy, as well as not including the recent RCTs. The present meta-analysis was therefore designed to compare the survival outcomes of std-TMZ and ext-TMZ in the first-line treatment of patients with glioblastoma.
2 Methods
2.1 Study Design and Types of Included Studies
This meta-analysis was conducted per the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline (29). It included RCTs comparing std-TMZ and ext-TMZ—as the first-line treatment in glioblastoma—in terms of median OS and median PFS.
2.2 Search Strategy
Two authors (S.A.J and F.A) independently searched the English literature for free-text and standard MeSH (Medical Subject Headings) terms in PubMed, Web of Science, Scopus, and Embase up to October 1, 2021. The search keywords were: high-grade glioma OR malignant glioma OR glioblastoma OR glioblastoma multiforme OR grade IV glioma OR grade IV astrocytoma OR GBM, adjuvant chemotherapy OR temozolomide OR temodar, AND extended OR long-term OR prolonged OR maintenance OR cycles OR months. Also, the two review authors handsearched the reference lists of the relevant articles to identify the possible missed RCTs. Thereafter, they downloaded all titles and abstracts retrieved by electronic searching to EndNote™ V.20.0, removed duplicates, and excluded the studies that did not meet the eligibility criteria, clearly (mentioned below). Eventually, they debated on the disagreements to improve the search results.
2.3 Study Screening
2.3.1 Participants
Adult patients with glioblastoma who underwent surgery, radiotherapy (concurrent with TMZ), and adjuvant TMZ as the primary treatment.
2.3.2 Inclusion Criteria
RCTs comparing std-TMZ and ext-TMZ, in which the median OS and/or median PFS were reported.
2.3.3 Exclusion Criteria
Studies if (i) not following the standard treatment sequence of MSR, CRT (with TMZ), and adjuvant TMZ, (ii) submitted only as abstracts or proceedings from scientific meetings, (iii) lacking English full text or summaries, or (iv) including patients with recurrent glioblastoma were excluded. Eligible studies were assessed finally for quality of methodology (30, 31).
2.4 Data Extraction
The following data were extracted from the studies: (i) study information (the first author, year of publication, study country, sample size), (ii) patient baseline characteristics (age, sex ratio), (iii) intervention duration (std-TMZ, ext-TMZ), and (iv) treatment outcomes (median OS, median PFS). Only data from the first-line therapy of both groups were extracted.
The standard chemotherapy regimen (std-TMZ) was defined as ≤ 6 cycles of TMZ following MSR and adjuvant CRT. The extended chemotherapy regimen (ext-TMZ) was defined as > 6 cycles of TMZ (up to 12 cycles) following MSR and adjuvant CRT. The median OS and PFS were extracted directly from the text or the Kaplan-Meier survival curves.
2.5 Quality Assessment
Two investigators (S.A.J. and F.A) assessed the methodological quality and risk of bias of the included studies. All four included studies were assessed using Cochrane’s Risk of bias tool (31). They resolved differences by discussion or appeal to a third review author (F.T) and presented results in a “Risk of bias” table. The risk of bias summary consists of 5 questions (also known as the Oxford quality scoring system), ranging from 0 to 5. Studies with a quality score less than 3 were regarded as poor quality and excluded from the study (Table 1).
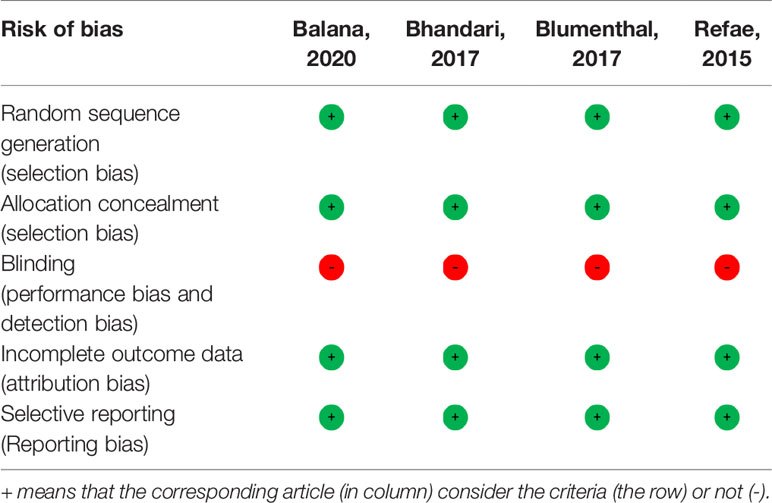
Table 1 Methodological quality summary for the included studies.
2.6 Statistical Analysis
The main objective of this meta-analysis was to compare the median PFS and OS for std-TMZ versus ext-TMZ as the first-line treatment of patients with glioblastoma. The individual patient data (IPD) is essential in the standard approach to pooled survival estimates (26). However, IPD was unavailable in this meta-analysis, and we used the median PFS and OS (weighted by the inverse of variance) to estimate the pooled median and 95% confidence interval (95% CI) of PFS and OS in each group of RCTs. The statistical heterogeneity between studies was evaluated using Cochran’s Q test and quantified by I2 statistics (high heterogeneity was defined as I² > 20% or P-value < 0.1). We applied Stata V.14.0 (Stata Corp, College Station, TX, USA) for the quantitative synthesis. The statistical significance level was set to 0.05.
3 Results
Our databases searching identified 45,060 potentially relevant studies. After deleting duplicates (10,351 records), 22 articles were included in the evaluation through screening titles, abstracts, and full texts. Then, we excluded eighteen studies (4–10, 12–17, 21, 22, 24, 32) on eligibility criteria. Figure 1 details the PRISMA flow diagram.
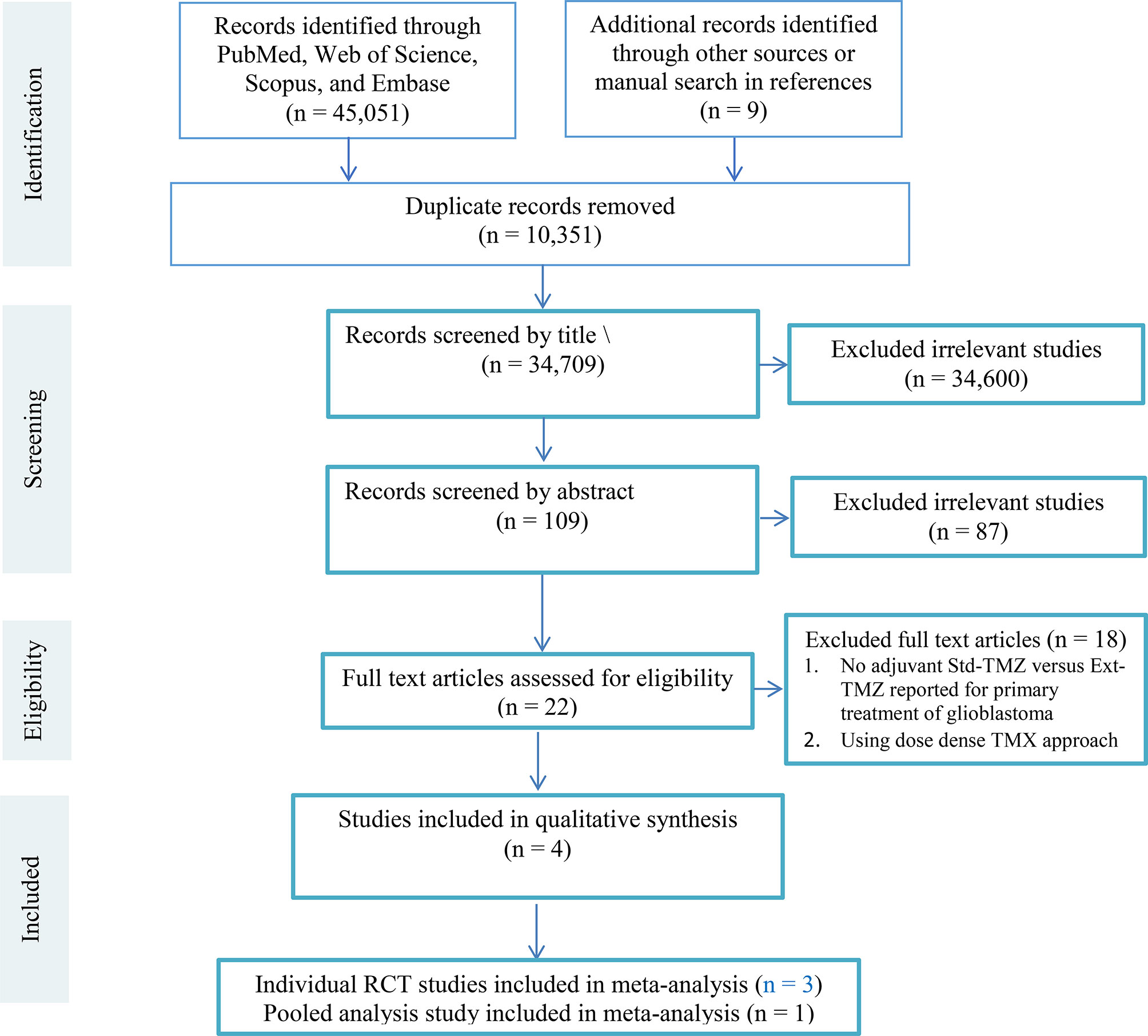
Figure 1 The PRISMA flow diagram. Three out of four eligible studies were randomized comparisons of adjuvant std-TMZ versus ext-TMZ for primary treatment of glioblastoma (19, 20, 23).The remaining study was a pooled analysis of four RCTs (26). The main characteristics of the eligible studies are shown in Table 2.

Table 2 Main characteristics of four studies included in the current meta-analysis.
A total of 882 glioblastoma patients were included in the four studies. Of these, 461 patients were treated by std-TMZ regimen, and 421 patients received ext-TMZ regimen. The median PFS of patients with glioblastoma who were treated by the standard or extended chemotherapy regimens is shown in Figure 2. The overall median PFS was 10.0 months (95% CI 7.0 to 12.0) in the std-TMZ group (TMZ ≤ 6 cycles). The studies had homogeneity in median PFS in this group (P = 0.82). Likewise, in the ext-TMZ group, all studies had homogeneity in the median PFS 12.0 months (95% CI 9.0 to15.0 months) (P = 0.91). The least record of median PFS (10.0 months 95% CI 5.0 to 19.0) in arms with ext-TMZ (TMZ > 6 cycles) was equal to the upper record of median PFS in the std-TMZ group (10.0 months 95% CI 4.0 to 26.0). Comparison between the two groups showed that ext-TMZ was associated with an improved PFS (12.0 months, 95% CI 9.0 to 15.0 vs. 10.0 months, 95% CI 7.0 to 12.0), although this improvement was not statistically significant (P = 0.27) (Figure 2).
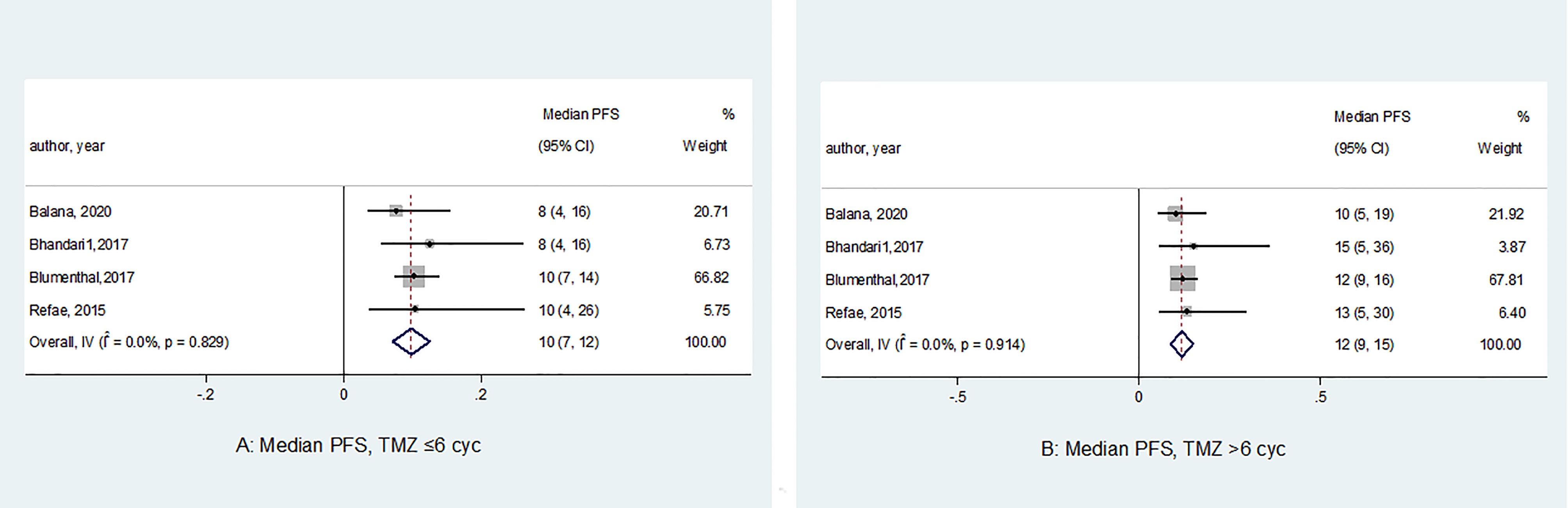
Figure 2 Forest plots of the median progression-free survival (PFS) according to the number of adjuvant temozolomide cycles. The horizontal line of the diamond summary represents the average 95% CI. The statistical heterogeneity between studies was assessed using the I2 test, which revealed a homogeneity in the results (PFS in the std-TMZ, I2 = 0.0%, P = 0.82; and PFS in the exd-TMZ, I2 = 0.0%, P = 0.91).
The median OS of the analyzed studies ranged from 14.0 to 25.0 months for the std-TMZ group (n = 461) versus 19.0 to 27.0 months for the ext-TMZ group (n = 421) (Figure 3). Three out of four studies reported superior median OS in the ext-TMZ group; however, Balana et al. found the contrast results (median OS: 19.0 months in ext-TMZ vs. 23.0 months in std-TMZ). The pooled estimated median OS of patients in the std-TMZ and ext-TMZ were statistically consistent [23.0 months (95% CI 19.0 to 27.0) and 24.0 months (95% CI 20.0 to 28.0), respectively, P = 0.73].
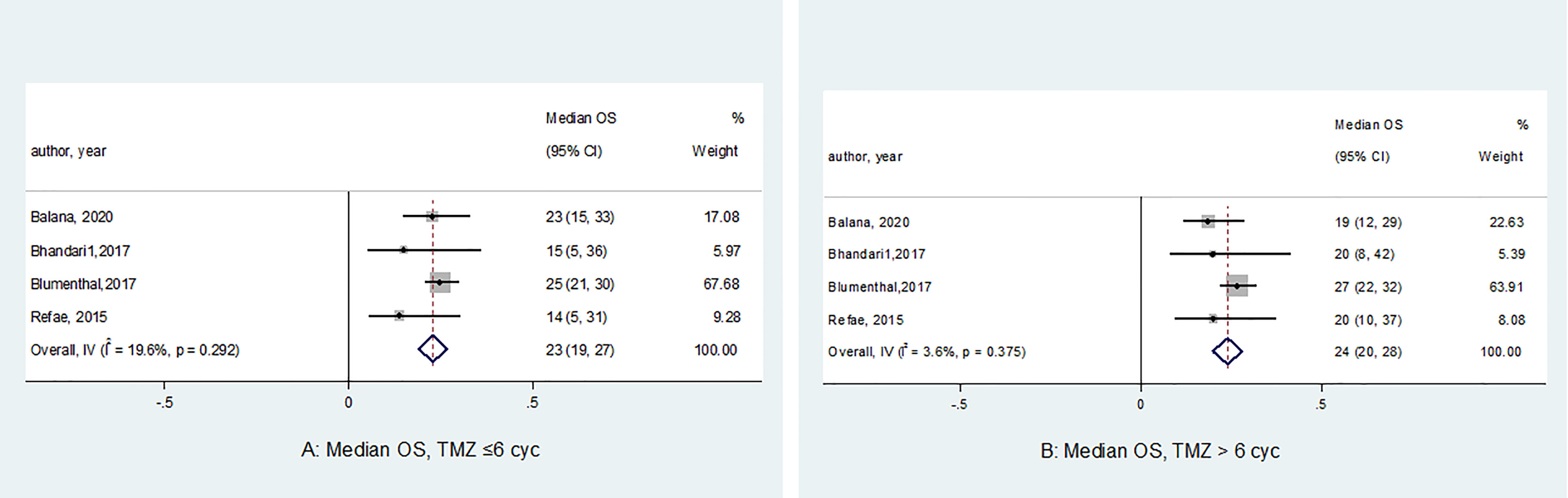
Figure 3 Forest plots of the median overall survival (OS) according to the number of cycles of adjuvant temozolomide (P = 0.99). The horizontal line of the diamond summary represents the average 95% CI. The statistical heterogeneity between studies was assessed using the I2 test, which revealed homogeneity in the results (OS in the std-TMZ, I2 = 19.6%, P = 0.29;and OS in the ext-TMZ, I2 = 3.6%, P = 0.37).
4 Discussion
This meta-analysis assessed the survival benefit of adjuvant ext-TMZ (7-12 cycles) against the standard 6-cycle regimen for patients with newly diagnosed glioblastoma. The literature search yielded four studies (three RCTs and one pooled analysis) that met our eligibility criteria, including 461 patients in the std-TMZ group and 421 patients in the ext-TMZ group. The quantitative analysis showed trend, although nonsignificant, towards improved PFS with the ext-TMZ regimen [12.0 months (95% CI 9.0 to 15.0) vs. 10.0 months (95% CI 7.0 to 12.0), P > 0.05]. However, the OS of patients who were treated by the ext-TMZ and the std-TMZ remained almost identical [23.0 months (95% CI 19.0 to 27.0) vs. 24.0 months (95% CI 20.0 to 28.0), P > 0.05, respectively]. These findings are inconsistent with the previous meta-analyses by Alimohammadi et al. and Xu et al., stating that extended adjuvant TMZ improves both PFS and OS in patients with newly diagnosed GBM (5, 25). However, these findings might be affected by the included retrospective records, which constituted 28.9% and all of the analyzed cases in the Alimohammadi et al.’s and Xu et al.’s studies, respectively. In our analysis, we excluded all retrospective studies to enhance the power of the results.
In summary, the current meta-analysis did not demonstrate the survival benefit of prolonged adjuvant TMZ in newly diagnosed glioblastoma. This might be explained by adaptive resistance. To better understand this issue, we need to recognize the mechanism of action of TMZ. As an alkylating agent, TMZ acts as a prodrug and induces cell cycle arrest at G2/M through methylation of DNA or RNA. The methylated sites can remain mutated by DNA mismatch repair (MMR) proteins, dealkylated by the action of O6-methylguanine methyltransferase (MGMT), or be removed by the base excision repair (BER) enzymes [such as alkylpurine-DNA-N-glycosylase (APNG)]. Cells are TMZ sensitive when MMR is overexpressed and active. On the other hand, MGMT or BER proteins overexpression increases the resistance of glioblastoma cells to TMZ. In vitro studies have delineated several mechanisms of adaptive resistance to TMZ in glioblastoma cell lines. For example, increased MGMT protein expression (33), decreased Tumor Necrosis Factor-Alpha-Induced Protein 3 (TNFAIP3) expression (34), upregulation of Signal Transducer and Activator of Transcription 3 (STAT3) (35), loss of MSH6 MMR gene (36), or upregulation of NTL1 (a BER enzyme) (37). Therefore, prolonged adjuvant TMZ can promote the development of tumor-resistant clones with more aggressive features. This issue can contribute to a dismal prognosis in salvage therapy of tumor recurrence. A multicenter, phase II trial—evaluating the efficacy of continuous dose-intense TMZ for recurrent glioblastoma—concluded that patients who had received adjuvant std-TMZ got more benefit from therapy in comparison with ext-TMZ group (38).
In addition to the idiosyncratic adverse effects of TMZ (such as aplastic anemia, cholestatic hepatitis, and myelosuppression), clinicians must consider the numerous intrinsic adverse effects of TMZ that might affect the quality and quantity of life of the patients with glioblastoma. In this regard, different retrospective studies have reported different rates of toxicities, as follows: lymphopenia (30-50%), nausea (28-44.3%), vomiting (20-37%), fatigue (10-33%), anorexia (14%), thrombocytopenia (12-13.7%), anemia (1-11%), neutropenia (6.3-7%), leukopenia (1.3-7%), myelodysplasia, or leukemia. The diverse rates of TMZ adverse effects might be due to different distribution of basic characteristics (vomiting and thrombocytopenia are more common in females), stage of treatment (hematological toxicities are more common in the concurrent chemoradiation phase), and the numbers of adjuvant TMZ cycles. In the context of lymphopenia, TMZ can increase the risk of opportunistic infections (such as pneumocystis jiroveci pneumonia, herpes zoster, candida) through selective CD4+ T-cell depletion (39, 40). The intrinsic adverse effect of TMZ is another evidences to avoid prolonged adjuvant TMZ. In an RCT, patients in the ext-TMZ arm experienced more grade ≥ 3 hematological toxicities (5% vs. none), vomiting (15% vs. 10%), and insomnia (10% vs. 5%) in comparison to the std-TMZ regimen. However, the rates of fatigue and headache were more prevalent in the std-TMZ arm (50% vs. 45% and 15% vs. 10%, respectively) (20).
Our study harbors several limitations. Lack of access to IPD and not reporting the hazard ratio in most of the studies are among the main ones. Besides, the current evidence on the role of MGMT methylation in the value of prolonged TMZ therapy beyond six months is either not addressed properly in the clinical trials (20, 23), or is assessed retrospectively (26). Therefore, prospective data on the predictive value of MGMT methylation is lacking, and our analysis cannot provide any comment in this regard. Among the included studies, only Balana et al. evaluated the role of MGMT on the survival of patients with glioblastoma receiving first-line adjuvant TMZ. By multivariate analysis, they showed that MGMT methylation was an independent factor for longer PFS and OS. However, this finding was not translated into the survival benefit of extended TMZ in patients with MGMT methylation (19).
In conclusion, prolonged adjuvant TMZ (beyond six cycles) did not provide OS and PFS benefits in patients with newly diagnosed glioblastoma. Considering this finding, along with the adverse effects of TMZ, the economic burden and psychosocial impacts of prolonged treatment can underscore the rationality of the current practice, which is 6 cycles of adjuvant TMZ. Further studies are needed to determine the predictive value of MGMT status on the long-term TMZ maintenance therapy. Moreover, the role of surgically validated results of dynamic imaging such as O-(2-[18F] fluoroethyl-)-L-tyrosine positron emission tomography (18F-FET PET) on the extending of TMZ should be assessed in future studies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
SJ, FT-H, and FA designed the meta-analysis, screened the studies and wrote the manuscript. FA analyzed data. AF, PP, and BP helped designed the study. All authors reviewed the manuscript finally. DF-P and AF wrote the initial draft. SJ, FA, PP, and BP approved the final submission of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to express our gratitude to Vasei Clinical Research Development Unit in Sabzevar University of Medical Sciences for their sincere cooperation.
References
1. Khurana R, Rath S, Singh HB, Rastogi M, Nanda SS, Chauhan A, et al. Correlation of Molecular Markers in High Grade Gliomas With Response to Chemo-Radiation. Asian Pacific J Cancer Prev: APJCP (2020) 21(3):755. doi: 10.31557/APJCP.2020.21.3.755
2. Fitzmaurice. Global, Regional, and National Burden of Brain and Other CNS Cancer, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol (2019) 18(4):376–93. doi: 10.1016/s1474-4422(18)30468-x
3. Houshyari M, Hajalikhani F, Rakhsha A, Hajian P. A Comparative Study of Survival Rate in High Grade Glioma Tumors Being Treated by Radiotherapy Alone Versus Chemoradiation With Nitrosourea. Global J Health Sci (2015) 7(6):33. doi: 10.5539/gjhs.v7n6p33
4. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy Plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl J Med (2005) 352(10):987–96. doi: 10.1056/NEJMoa043330
5. Alimohammadi E, Bagheri SR, Taheri S, Dayani M, Abdi A. The Impact of Extended Adjuvant Temozolomide in Newly Diagnosed Glioblastoma Multiforme: A Meta-Analysis and Systematic Review. Oncol Rev (2020) 14(1):461. doi: 10.4081/oncol.2020.461
6. Liu Y, Hao S, Yu L, Gao Z. Long-Term Temozolomide Might be an Optimal Choice for Patient With Multifocal Glioblastoma, Especially With Deep-Seated Structure Involvement: A Case Report and Literature Review. World J Surg Oncol (2015) 13:142. doi: 10.1186/s12957-015-0558-x
7. Barbagallo GM, Paratore S, Caltabiano R, Palmucci S, Parra HS, Privitera G, et al. Long-Term Therapy With Temozolomide is a Feasible Option for Newly Diagnosed Glioblastoma: A Single-Institution Experience With as Many as 101 Temozolomide Cycles. Neurosurg Focus (2014) 37(6):E4. doi: 10.3171/2014.9.Focus14502
8. Choi JW, Lee MM, Kim IA, Kim JH, Choe G, Kim CY. The Outcomes of Concomitant Chemoradiotherapy Followed by Adjuvant Chemotherapy With Temozolomide for Newly Diagnosed High Grade Gliomas: The Preliminary Results of Single Center Prospective Study. J Korean Neurosurg Soc (2008) 44(4):222–7. doi: 10.3340/jkns.2008.44.4.222
9. Darlix A, Baumann C, Lorgis V, Ghiringhelli F, Blonski M, Chauffert B, et al. Prolonged Administration of Adjuvant Temozolomide Improves Survival in Adult Patients With Glioblastoma. Anticancer Res (2013) 33(8):3467–74.
10. Freyschlag CF, Smolczyk DR, Janzen E, Schmieder K, Thomé C, Lohr F, et al. Prolonged Administration of Temozolomide in Adult Patients With Anaplastic Glioma. Anticancer Res (2011) 31(11):3873–7.
11. Seiz M, Krafft U, Freyschlag CF, Weiss C, Schmieder K, Lohr F, et al. Long-Term Adjuvant Administration of Temozolomide in Patients With Glioblastoma Multiforme: Experience of a Single Institution. J Cancer Res Clin Oncol (2010) 136(11):1691–5. doi: 10.1007/s00432-010-0827-6
12. Hsieh SY, Chan DT, Kam MK, Loong HH, Tsang WK, Poon DM, et al. Feasibility and Safety of Extended Adjuvant Temozolomide Beyond Six Cycles for Patients With Glioblastoma. Hong Kong Med J (2017) 23(6):594–8. doi: 10.12809/hkmj165002
13. Kim BS, Seol HJ, Nam DH, Park CK, Kim IH, Kim TM, et al. Concurrent Chemoradiotherapy With Temozolomide Followed by Adjuvant Temozolomide for Newly Diagnosed Glioblastoma Patients: A Retrospective Multicenter Observation Study in Korea. Cancer Res Treat (2017) 49(1):193–203. doi: 10.4143/crt.2015.473
14. Okumus NO, Gursel B, Meydan D, Ozdemir O, Odabas E, Gonullu G. Prognostic Significance of Concomitant Radiotherapy in Newly Diagnosed Glioblastoma Multiforme: A Multivariate Analysis of 116 Patients. Ann Saudi Med (2012) 32(3):250–5. doi: 10.5144/0256-4947.2012.250
15. Quan R, Zhang H, Li Z, Li X. Survival Analysis of Patients With Glioblastoma Treated by Long-Term Administration of Temozolomide. Med (Baltimore) (2020) 99(2):e18591. doi: 10.1097/md.0000000000018591
16. Rivoirard R, Falk AT, Chargari C, Guy JB, Mery B, Nuti C, et al. Long-Term Results of a Survey of Prolonged Adjuvant Treatment With Temozolomide in Patients With Glioblastoma (SV3 Study). Clin Oncol (R Coll Radiol) (2015) 27(8):486–7. doi: 10.1016/j.clon.2015.04.003
17. Roldán Urgoiti GB, Singh AD, Easaw JC. Extended Adjuvant Temozolomide for Treatment of Newly Diagnosed Glioblastoma Multiforme. J Neurooncol (2012) 108(1):173–7. doi: 10.1007/s11060-012-0826-3
18. Hirono S, Hasegawa Y, Sakaida T, Uchino Y, Hatano K, Iuchi T. Feasibility Study of Finalizing the Extended Adjuvant Temozolomide Based on Methionine Positron Emission Tomography (Met-PET) Findings in Patients With Glioblastoma. Sci Rep (2019) 9(1):17794. doi: 10.1038/s41598-019-54398-2
19. Balana C, Vaz MA, Manuel Sepúlveda J, Mesia C, Del Barco S, Pineda E, et al. A Phase II Randomized, Multicenter, Open-Label Trial of Continuing Adjuvant Temozolomide Beyond 6 Cycles in Patients With Glioblastoma (GEINO 14-01). Neuro-Oncol (2020) 22(12):1851–61. doi: 10.1093/neuonc/noaa107
20. Bhandari M, Gandhi AK, Devnani B, Kumar P, Sharma DN, Julka PK. Comparative Study of Adjuvant Temozolomide Six Cycles Versus Extended 12 Cycles in Newly Diagnosed Glioblastoma Multiforme. J Clin Diagn research: JCDR (2017) 11(5):XC04. doi: 10.7860/JCDR/2017/27611.9945
21. Gilbert MR, Wang M, Aldape KD, Stupp R, Hegi ME, Jaeckle KA, et al. Dose-Dense Temozolomide for Newly Diagnosed Glioblastoma: A Randomized Phase III Clinical Trial. J Clin Oncol (2013) 31(32):4085. doi: 10.1200/JCO.2013.49.6968
22. Hau P, Koch D, Hundsberger T, Marg E, Bauer B, Rudolph R, et al. Safety and Feasibility of Long-Term Temozolomide Treatment in Patients With High-Grade Glioma. Neurol (2007) 68(9):688–90. doi: 10.1212/01.wnl.0000255937.27012.ee
23. Refae AA, Ezzat A, Salem DA, Mahrous M. Protracted Adjuvant Temozolomide in Glioblastoma Multiforme. J Cancer Ther (2015) 6(08):748. doi: 10.4236/jct.2015.68082
24. van Genugten JA, Leffers P, Baumert BG, Tjon AFH, Twijnstra A. Effectiveness of Temozolomide for Primary Glioblastoma Multiforme in Routine Clinical Practice. J Neurooncol (2010) 96(2):249–57. doi: 10.1007/s11060-009-9956-7
25. Xu W, Li T, Gao L, Zheng J, Shao A, Zhang J. Efficacy and Safety of Long-Term Therapy for High-Grade Glioma With Temozolomide: A Meta-Analysis. Oncotarget (2017) 8(31):51758–65. doi: 10.18632/oncotarget.17401
26. Blumenthal DT, Gorlia T, Gilbert MR, Kim MM, Burt Nabors L, Mason WP, et al. Is More Better? The Impact of Extended Adjuvant Temozolomide in Newly Diagnosed Glioblastoma: A Secondary Analysis of EORTC and NRG Oncology/RTOG. Neuro-Oncol (2017) 19(8):1119–26. doi: 10.1093/neuonc/nox025
27. Nabors LB, Fink KL, Mikkelsen T, Grujicic D, Tarnawski R, Nam DH, et al. Two Cilengitide Regimens in Combination With Standard Treatment for Patients With Newly Diagnosed Glioblastoma and Unmethylated MGMT Gene Promoter: Results of the Open-Label, Controlled, Randomized Phase II CORE Study. Neuro Oncol (2015) 17(5):708–17. doi: 10.1093/neuonc/nou356
28. Stupp R, Hegi ME, Gorlia T, Erridge SC, Perry J, Hong YK, et al. Cilengitide Combined With Standard Treatment for Patients With Newly Diagnosed Glioblastoma With Methylated MGMT Promoter (CENTRIC EORTC 26071-22072 Study): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol (2014) 15(10):1100–8. doi: 10.1016/s1470-2045(14)70379-1
29. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst Rev (2015) 4(1):1–9. doi: 10.1186/2046-4053-4-1
30. Khan KS, Daya S, Jadad AR. The Importance of Quality of Primary Studies in Producing Unbiased Systematic Reviews. Arch Internal Med (1996) 156(6):661–6. doi: 10.1001/archinte.1996.00440060089011
31. Higgins J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1. 0 [Updated March 2011]. The Cochrane Collaboration. (2011). www cochrane-handbook org.
32. Stupp R, Hegi ME, Mason WP, Van Den Bent MJ, Taphoorn MJ, Janzer RC, et al. Effects of Radiotherapy With Concomitant and Adjuvant Temozolomide Versus Radiotherapy Alone on Survival in Glioblastoma in a Randomised Phase III Study: 5-Year Analysis of the EORTC-NCIC Trial. Lancet Oncol (2009) 10(5):459–66. doi: 10.1016/S1470-2045(09)70025-7
33. Happold C, Roth P, Wick W, Schmidt N, Florea AM, Silginer M, et al. Distinct Molecular Mechanisms of Acquired Resistance to Temozolomide in Glioblastoma Cells. J neurochem (2012) 122(2):444–55. doi: 10.1111/j.1471-4159.2012.07781.x
34. Bredel M, Bredel C, Juric D, Duran GE, Yu RX, Harsh GR, et al. Tumor Necrosis Factor-Alpha-Induced Protein 3 as a Putative Regulator of Nuclear factor-kappaB-Mediated Resistance to O6-Alkylating Agents in Human Glioblastomas. J Clin Oncol (2006) 24(2):274–87. doi: 10.1200/jco.2005.02.9405
35. Kohsaka S, Wang L, Yachi K, Mahabir R, Narita T, Itoh T, et al. STAT3 Inhibition Overcomes Temozolomide Resistance in Glioblastoma by Downregulating MGMT Expression. Mol Cancer Ther (2012) 11(6):1289–99. doi: 10.1158/1535-7163.MCT-11-0801
36. Cahill DP, Levine KK, Betensky RA, Codd PJ, Romany CA, Reavie LB, et al. Loss of the Mismatch Repair Protein MSH6 in Human Glioblastomas is Associated With Tumor Progression During Temozolomide Treatment. Clin Cancer Res (2007) 13(7):2038–45. doi: 10.1158/1078-0432.Ccr-06-2149
37. Zhang J, Stevens MF, Laughton CA, Madhusudan S, Bradshaw TD. Acquired Resistance to Temozolomide in Glioma Cell Lines: Molecular Mechanisms and Potential Translational Applications. Oncol (2010) 78(2):103–14. doi: 10.1159/000306139
38. Perry JR, Bélanger K, Mason WP, Fulton D, Kavan P, Easaw J, et al. Phase II Trial of Continuous Dose-Intense Temozolomide in Recurrent Malignant Glioma: RESCUE Study. J Clin Oncol (2010) 28(12):2051–7. doi: 10.1200/jco.2009.26.5520
39. Dixit S, Baker L, Walmsley V, Hingorani M. Temozolomide-Related Idiosyncratic and Other Uncommon Toxicities: A Systematic Review. Anticancer Drugs (2012) 23(10):1099–106. doi: 10.1097/CAD.0b013e328356f5b0
Keywords: adjuvant, extended chemotherapy, glioblastoma, temozolomide, treatment duration, The Stupp protocol, high-grade gliomas
Citation: Attarian F, Taghizadeh-Hesary F, Fanipakdel A, Javadinia SA, Porouhan P, PeyroShabany B and Fazilat-Panah D (2021) A Systematic Review and Meta-Analysis on the Number of Adjuvant Temozolomide Cycles in Newly Diagnosed Glioblastoma. Front. Oncol. 11:779491. doi: 10.3389/fonc.2021.779491
Received: 18 September 2021; Accepted: 29 October 2021;
Published: 23 November 2021.
Edited by:
Luca Ricciardi, Sapienza University of Rome, ItalyReviewed by:
Giovanni Raffa, University of Messina, ItalyNicola Montemurro, Azienda Ospedaliera Universitaria Pisana, Italy
Copyright © 2021 Attarian, Taghizadeh-Hesary, Fanipakdel, Javadinia, Porouhan, PeyroShabany and Fazilat-Panah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seyed Alireza Javadinia, SmF2YWRpbmlhYTk0MUBtdW1zLmFjLmly; SmF2YWRpbmlhLmFsaXJlemFAZ21haWwuY29t
†ORCID: Fahimeh Attarian, orcid.org/0000-0001-9752-0480
Farzad Taghizadeh-Hesary, orcid.org/0000-0002-6195-2203
Azar Fanipakdel, orcid.org/0000-0003-4055-5783
Seyed Alireza Javadinia, orcid.org/0000-0003-2467-837X
Pejman Porouhan, orcid.org/0000-0001-6296-3214
Babak PeyroShabany, orcid.org/0000-0002-4452-2041
Danial Fazilat-Panah, orcid.org/0000-0003-4194-657
‡These authors share first authorship