
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 03 January 2022
Sec. Surgical Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.778152
This article is part of the Research Topic Women in Surgical Oncology: 2021 View all 11 articles
 Lin Xiang1,2†
Lin Xiang1,2† Shuai Jin3†Peng Zheng1Ewetse Paul Maswikiti1
Shuai Jin3†Peng Zheng1Ewetse Paul Maswikiti1 Yang Yu1Lei Gao1Jing Zhang1Ying Zhang4*
Yang Yu1Lei Gao1Jing Zhang1Ying Zhang4* Hao Chen1,5,6*
Hao Chen1,5,6*As the most common recurrence pattern after radical gastric cancer resection, peritoneal recurrence is a major cause of mortality, which affects the prognosis of patients to a very large extent. Peritoneal status and risk of peritoneal recurrence can be evaluated by peritoneal lavage cytology, photodynamic diagnosis, imaging examination, and pathologic analysis. Presently, there is no standard approach for preventing peritoneal recurrence after radical surgery; furthermore, controversies exist regarding the effects of some preventive methods. Among the preventive methods, there are high expectations about the potential of preoperative therapy, surgical skill improvement, hyperthermic intraperitoneal chemotherapy, and postoperative treatment to reduce the incidence of peritoneal recurrence after radical gastrectomy. This study aimed to analyze the results of previous studies on the risk assessment and preventive methods of peritoneal recurrence after radical gastrectomy in recent years. We hope to provide references for better approach to clinical diagnosis and treatment strategies for peritoneal recurrence after radical gastrectomy.
As a common malignant tumor of the digestive system, gastric cancer (GC) has the fifth highest incidence among malignant tumors worldwide and the third highest fatality rate, and there has been a significant increase in its incidence in East Asia (1). Currently, radical resection is the only curative treatment strategy for GC. However, many patients have recurrence after radical resection, and the prognosis of these patients is extremely poor. Furthermore, GC is mainly associated with the depth of tumor invasion, lymphatic involvement, and Borrmann type. The recurrence patterns after radical gastrectomy are classified as locoregional, peritoneal, and nonperitoneal distant recurrence. The most common site of first recurrence is the peritoneum (48.8%), then the liver (20.8%), and the locoregional (15.2%) (2). The significant reduction of survival time due to peritoneal recurrence is the leading cause of death (2–4). Therefore, early prevention and detection of recurrence with effective intervention are very important to improve the prognosis of patients with GC after radical resection. Presently, in patients with GC, many therapeutic methods and strategies have been used for the prevention and risk assessment of peritoneal recurrence after radical gastrectomy. To establish a reference value for the formulation of clinical strategies, this study aimed to identify current methods for predicting and preventing peritoneal recurrence after radical resection.
Before surgical operation, it is crucial to evaluate the risk of peritoneal recurrence and identify possible micrometastasis for appropriate treatment modality. Such evaluations can improve the accuracy of diagnoses, to ensure early intervention for high-risk patients, lead to the avoidance of unnecessary additional treatments for low-risk patients, and reduce additional harm from the redundant treatment of patients.
Intraperitoneal free cancer cells (IFCC) play a critical role in the development of peritoneal metastasis of GC (the main cause of failure after radical gastrectomy). Peritoneal lavage cytology, widely regarded as the gold standard for the diagnosis of IFCC, has negative and positive results reported as CY0 and CY1, respectively. Patients with positive peritoneal cytology have poor prognosis; therefore, a positive IFCC is considered an independent adverse prognostic factor. A retrospective review including GC patients with only CY1 status in the absence of obvious peritoneal metastasis reported that all patients had recurrence within 3 years after radical resection, and 92% of these patients had peritoneal metastasis, indicating positive cytology as an important precursor of peritoneal recurrence (5). Several previous studies have demonstrated that serosa infiltration is one of the most important predictors of peritoneal micrometastasis (6, 7). Furthermore, when serosa infiltration or suspected serosa infiltration occurs in GC patients, peritoneal lavage cytology should be implemented to confirm the existence of IFCC. However, GC patients with CY1 status are considered at stage IV, and their prognosis is still poor even after curative surgery for GC (8). Therefore, cytological examinations have a profound influence for GC patients in predicting peritoneal recurrence.
The detection methods of peritoneal cytology mainly include traditional cytology (hematoxylin and eosin staining, HE staining), immunoassay, immunohistochemistry (IHC), and reverse transcription polymerase chain reaction (RT-PCR). The accuracy, sensitivity, and specificity of predicting peritoneal recurrence differ and are 73–91.9, 11.1–80, and 86.4–100%; 72–95, 23–100, and 81–92.9; 54.8–76.7, 22.1–75, and 76.9–97.3%; and 61–89.7, 31–100, and 58.8–95% in traditional cytology, immunoassay, IHC, and RT-PCR, respectively (9). Compared with the remaining three methods, RT-PCR shows some advantages.
The main target of detection by RT-PCR is the carcinoembryonic antigen (CEA). In peritoneal lavage fluid, the sensitivity and diagnostic odds ratio of CEA protein or mRNA to predict peritoneal recurrence are higher than those of traditional cytology; however, traditional cytology has a higher specificity. GC CEA-positive patients are more likely to have peritoneal recurrence after radical resection, with significantly reduced overall survival (OS) (10). A meta-analysis of 117 cases with GC also had a similar conclusion (11). The peritoneal recurrence rate among patients with positive CEA was higher than that among negative-CEA patients. Furthermore, the expression of CEA in peritoneal lavage fluid was closely related to peritoneal recurrence after radical gastrectomy; this is considered the most important prognostic factor for recurrence after curative resection. Some scholars have suggested that the results of traditional cytology are so unstable that the detection of IFCC cannot be guaranteed, and it is necessary to combine them with those of other more sensitive molecular techniques (such as IHC or RT-PCR) to improve the detection rate of IFCC in the abdominal cavity (12).
Although RT-PCR shows advantages in accuracy, sensitivity, and specificity to IFCC detection, its procedure is cumbersome and time-consuming. It is impossible to provide reliable information to the surgeon during operation, which is a great limitation of practicability. The emergence of transcription-reverse transcription concerted reaction (TRC) seems to make up for the deficiency of RT-PCR. As a direct RNA amplification detection method, TRC was developed to detect peritoneal lavage fluid in GC patients (13). Moreover, compared with RT-PCR, TRC has a simpler operation maneuver and a faster detection strategy. The sensitivity (85%) and specificity (100%) of TRC are similar to those of RT-PCR (92 and 100%, respectively), but TRC is significantly faster and can be completed in 1.0–1.5 h (14). A prospective multicenter study of advanced GC (AGC) patients undergoing radical resection revealed that disease-free survival (DFS) and peritoneal recurrence-free survival (RFS) in the positive TRC-CEA group are significantly lower than those in the negative group and that TRC-CEA could be an important prognostic marker to predict survival and peritoneal recurrence in GC with serosal invasion (15). Another study showed that CEA detected by TRC after lymph node resection in radical gastrectomy is an important predictor of prognosis, although it is not closely related to peritoneal recurrence (16).
According to the above-mentioned studies, traditional cytology combined with other detection methods may be the best way to improve the detection rate of peritoneal cancer cells. This can help clinicians to identify the high-risk peritoneal recurrence groups and provide the key basis for the formulation of follow-up therapies.
For GC, 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) combined with computerized tomography (CT) (18F-FDG PET/CT) is often used to evaluate and predict recurrence prior to surgery and to monitor recurrence post-surgery, whereas its clinical significance has always been controversial in peritoneal recurrence prediction. A retrospective study involving 279 AGC patients who underwent 18F-FDG PET/CT before radical resection, with the tumor-to-normal liver uptake ratio (TLR) as the examination parameter, found a remarkably higher 5-year distant metastasis-free survival rate among patients with TLR ≤2.0 compared to that among patients with TLR >2.0 (95.5 vs. 68.8%, respectively, P < 0.0001); however, TLR had no significant correlation with peritoneal RFS (P = 0.7) (17). In addition, the attenuation of 18F-FDG uptake in the visceral adipose tissue (VAT) was found to be significantly associated with peritoneal RFS and OS, whereas in AGC patients with high VAT attenuation and a standardized uptake value (FDG uptake), peritoneal recurrence is more likely to occur after curative resection (18). In summary, depending on some specific parameters, preoperative PET/CT seems to be capable of being used to assess the risk of peritoneal recurrence after radical gastrectomy and may become an important non-invasive evaluation method. Since the sample size of this research was small and the finding was not very convincing, further studies with larger samples of clinical data to support these are still needed.
The diagnosis of peritoneal metastasis in patients with GC has a profound impact on treatment strategies. Currently, staging laparoscopy is routine in clinical settings; however, because some micrometastasis that are invisible to the naked eyes may be missed, eventually, this may lead to inappropriate radical resection in these GC patients. As a new technique for fluorescence imaging of lesions using photosensitive drugs, photodynamic diagnosis (PDD) shows great potential in the discovery of micrometastatic foci, with the commonly used drug being 5-aminolevulinic acid (ALA). ALA-PDD is more sensitive than white light laparoscopy in the detection of peritoneal dissemination, with an increased detection rate of peritoneal metastasis by 21–34% with ALA-PDD (19–21). If only white light observation is used without ALA-PDD detection, about 11% of patients with peritoneal dissemination will be missed, and most of these patients (76.9%) identified by ALA-PDD and confirmed to have peritoneal metastasis had negative cytological results (22). Although ALA-PDD shows obvious advantages in detecting peritoneal metastases that are not visible to the naked eye, its false positive rate is higher (32.3%) (23). ALA-PDD can improve the visualization of the invisible peritoneal metastases, and this helps to determine the peritoneal status of patients with AGC, resulting in GC staging accuracy. However, more large-sample randomized controlled clinical trials (RCTs) are needed to assess the applicability of PDD.
Neoadjuvant therapy could induce tumor downstaging and improve the rate of R0 resection for resectable GC (24). The neoadjuvant therapy methods are categorized as neoadjuvant chemotherapy (NAC), neoadjuvant radiotherapy, and neoadjuvant chemoradiotherapy. Radiotherapy is mostly used for esophagogastric junction cancer, while chemotherapy is mainly for GC. A meta-analysis involving 15 RCTs showed that neoadjuvant therapy could significantly reduce the overall mortality of AGC patients at 3 (relative risk, RR = 0.74, P = 0.005) and 5 (RR = 0.82, P = 0.009) years after radical surgery (25). Nonetheless, the postoperative recurrence pattern of patients who received NAC did not seem to have changed compared with the results of earlier studies, and the peritoneum was still the most common relapse site after radical gastrectomy in these patients (2, 26). Moreover, different types of NAC had no effect on 5-year RFS (P = 0.236). A retrospective study also reported no statistical difference in overall recurrence and peritoneal recurrence between NAC and surgery-only groups before or after a propensity score matching (27). Recently, the PRODIGY trial published the results indicating that adding NAC (docetaxel, oxaliplatin, and S-1) to the basic treatment of radical surgery plus S-1 adjuvant chemotherapy could notably improve progression-free survival in patients with resectable localized AGC (hazard ratio, HR = 0.70, P = 0.023), although there was no statistical difference in the OS (HR = 0.84, P = 0.338) (28). The detailed data related to recurrence were not reported. Surprisingly, some retrospective studies showed that neoadjuvant therapy before radical operation was an adverse factor for the long-term survival of AGC patients (HR = 1.631, P = 0.006) (2, 29). In terms of peritoneal recurrence, the proportion of patients receiving neoadjuvant therapy was even higher than that of untreated ones (37.1 vs. 32.1%). The above-mentioned conditions may occur because patients who receive neoadjuvant therapy tend to have relatively more advanced stage or high-grade tumors, which may explain the difference between pTNM stage and ypTNM stage (post-neoadjuvant pTNM).
Although many studies have concluded that neoadjuvant therapy has no effect on peritoneal recurrence in GC patients after radical resection (2, 26, 27, 29, 30), the recent findings by Xu et al. seem to have reinforced the confidence in neoadjuvant therapy to reduce peritoneal recurrence (31). By propensity score-matched analysis, Xu et al. found that, for local AGC with serosal invasion, the OS and DFS in NAC-treated patients were significantly better than that in the untreated ones (P < 0.0001), and patients who received NAC had fewer postoperative complications (P = 0.037). It is exciting to note that the overall recurrence in the NAC group was less than that in the non-NAC group (29.9 vs. 63.3%), and peritoneal recurrence significantly decreased (19.0 vs. 48.4%). According to the above-mentioned studies, NAC appears to have the potential to improve prognosis and prevent recurrence, especially for patients who are at a high risk of peritoneal recurrence, including serosa-positive patients. Neoadjuvant therapy is recommended for T ≥3 and/or with node-positive GC, according to The Italian Research Group for Gastric Cancer (32). A multicenter randomized phase II trial (NCT02931890) is underway to explore different neoadjuvant therapy regimens (chemotherapy, chemotherapy followed by chemoradiotherapy, and chemoradiotherapy) for the purpose of identifying a comprehensive and objective clinical evaluation (33). At present, the populations among whom neoadjuvant therapy is being implemented differ between Eastern and Western countries, and no consensus has been reached yet. However, most studies set the treatment range to patients with T ≥3 tumor and N+ tumor.
After diagnosis and staging by routine endoscopy examination, endoscopic biopsy, and contrast-enhanced CT, laparoscopy with/without peritoneal lavage cytology is recommended for patients with stage I B or higher GC or with suspected peritoneal metastasis (32, 34, 35). For GC patients with positive peritoneal cytology or macroscopic peritoneal metastases, it is necessary to change the treatment strategy instead of direct radical operation. Preoperative chemotherapy is needed to improve the possibility of R0 resection to avoid incomplete resection and reduce the risk of cell peritoneal seeding during surgery.
In addition to the serosa infiltration of gastric tumors which increases the risk of peritoneal dissemination, surgical procedures may also cause cancer cells to enter and penetrate the abdominal cavity from the resection margin, blood, or lymphatic vessels and eventually lead to peritoneal metastasis. Radical gastrectomy includes open surgery, laparoscopic surgery, robotic surgery, and endoscopic procedure; among these, endoscopic procedure is mainly aimed at local early-stage GC. According to the cytological analysis of peritoneal lavage in GC patients undergoing radical resection, the diffusion of tumor cells into the peritoneal cavity after operation is higher than that when the abdominal cavity has just been opened and explored, which suggest that the operation could directly promote the iatrogenic dissemination of tumor cells and increase the possibility of peritoneal metastasis (36). Therefore, surgical methods and related precautions for GC have become important concerns for clinicians to reduce postoperative peritoneal recurrence.
Due to extensive trauma, poor postoperative recovery, and other complications, the traditional open radical resection of GC is rapidly giving way to minimally invasive surgery (MIS). Furthermore, a large number of studies have shown that laparoscopic radical gastrectomy has comparable short- and long-term outcomes compared to traditional open radical gastrectomy and is suitable at all stages for GC curative purposes (37–42). According to these literatures, there is no consensus on whether MIS is superior to open surgery in the short- and long-term outcomes, but MIS is, at least, not inferior to traditional open surgery. A propensity score−matched analysis from an eastern center concluded that the postoperative complications (35.2 vs. 40.7%, P = 0.69) and 90-day mortality (1.9 vs. 3.7%, P=1.00) in the laparoscopic gastrectomy (LG) group were comparable to those in the open gastrectomy (OG) group (42). Although there was no significant difference between the two groups in 3-year OS and DFS (P = 0.34; P = 0.51), the LG group had markedly fewer peritoneal recurrences than the OG group (3.7 vs. 27.8, P < 0.01). Another recent propensity score−matched analysis from a western center also reported similar results of no statistical difference in OS, DFS, postoperative complications, and mortality between LG and OG groups (43).
Compared with open resection, the postoperative overall recurrence of laparoscopic gastrectomy has limited demerits, and its peritoneal recurrence rate is not higher than that of traditional open surgery (39, 41, 44). KLASS-01, a large RCT, showed that, for patients with clinical stage I GC, the long-term oncological outcomes of laparoscopic distal gastrectomy (LDG) and open distal gastrectomy (ODG) are similar, with no significant difference in peritoneal recurrence between them (1.2 vs. 1.0%) (45). Furthermore, the other two RCTs (CLASS-01 and KLASS-02) for locally AGC also achieved similar results with similar 3-year DFS in the LDG and ODG groups and no significant difference between the two groups in peritoneal recurrence (46, 47). Shi et al. studied the long-term tumor outcomes of patients with locally AGC after radical resection and found that the 5-year OS and DFS do not notably differ between the LG and OG groups, with no statistical difference in peritoneal recurrence (LG: 28.6% vs. OG: 26.0%, P = 0.705) and other types of recurrence, between the two groups (48). Based on the above-mentioned research, laparoscopic radical gastrectomy could achieve short- and long-term outcomes comparable to open surgery while not increasing the probability of peritoneal recurrence but showing significant and more prominent advantages in other aspects, such as reduced intraoperative blood loss and early postoperative recovery. Compared with laparoscopic surgery, robotic surgery, another MIS, has prominent advantages, such as fatigue reduction, high stability, and three-dimensional vision, and has been gradually applied in the treatment of GC. In addition, many studies have also reported better minimally invasive advantages with robotic surgery than laparoscopic surgery in radical gastrectomy, and these two operative methods have similar short- and long-term outcomes as well as postoperative peritoneal recurrence rates (49–53). Regarding the high expense of robotic surgery, its application in the treatment of GC is still not yet popularized. Therefore, laparoscopic resection has gradually replaced traditional open resection to become the mainstream method of radical gastrectomy.
Lymph node dissection is an important part of radical gastrectomy and usually classified as D1, D2, and D3 lymphadenectomy according to the extent of dissection. For resectable GC, D2 lymphatic dissection is mainly recommended (54). Currently, there is insufficient and effective evidence for the relationship between the extent of lymph node dissection and peritoneal recurrence after radical gastrectomy. In the Dutch D1D2 trial, despite the absence of noticeable differences in 15-year OS, DFS, and relapse rate between D1 and D2 groups, the cancer-related mortality rate in D1 group was higher than that in D2 group (48 vs. 37%, P = 0.01) (55). The patients who received D1 lymphadenectomy showed higher rates of locoregional and liver recurrences than those undergoing D2 lymphadenectomy, but the data related to peritoneal recurrence were not reported in this publication. In another research, Nakanishi et al. found no significant difference in 5-year cumulative peritoneal recurrence rates between D2 minus and D2 groups for AGC patients with CY0 (29 vs. 33%, P = 0.595) (56). A retrospective study involving 568 AGC patients reported that the overall recurrences of D2 and D3 patients are comparable (57). Furthermore, there was no statistical difference in peritoneal recurrence rates (14.6 vs. 11.6%, P = 0.319) and other types of recurrence between the two groups. Similarly, a recently published retrospective cohort analysis reported comparable rates of peritoneal recurrence in the D1 plus and D2 groups (4.4 vs. 5.0%, P = 0.743) (58). According to the above-mentioned studies, the extent of lymph node dissection during radical resection of GC seems to have no correlation with postoperative peritoneal recurrence. Nevertheless, the propensity score-matched analysis by Hayashi et al. provides some interesting results (59). They reported that the number of retrieved lymph nodes (RLN) is related to the long-term outcome of AGC patients after radical surgery. The RLN ≥40 group had notably longer OS and RFS than the RLN <40 group (HR = 2.11, P = 0.0057; HR = 2.35, P = 0.0001). Furthermore, compared with the RLN ≥40 group, the peritoneal recurrence rate in the RLN <40 group increased significantly (P = 0.0007).
As treatment strategies to prevent peritoneal metastasis after radical gastrectomy, the use of either omentectomy or bursectomy has always been controversial. A multicenter prospective cohort study showed that the incidence of omentum metastasis in curable GC is lower and is only related to later clinical stage and non-curable features, and it suggested that omentum resection is not necessary in radical gastrectomy (60). Sakimura et al. reported that, for patients with AGC who underwent radical resection, there was no significant difference between the omentectomy and non-omentectomy groups in 3-year OS and RFS as well as in overall and peritoneal recurrence rates, which suggest that omentectomy could not improve the survival benefits of AGC patients (61). According to some data from an earlier RCT, the peritoneal recurrence in patients who underwent radical gastrectomy plus bursectomy was less than that of those without bursectomy (8.7 vs. 13.2%). Although the 3-year OS in the bursectomy group was better than that in the non-bursectomy group, there was no statistically significant difference between groups (62). A subsequent large retrospective study found that, for AGC patients that underwent radical surgery, additional bursectomy had no significant effect on the OS rate (P = 0.978), and there was no significant difference in peritoneal recurrence between the bursectomy and non-bursectomy groups (P = 0.623) (63). In 2018, a phase 3, open-label RCT (JCOG1001) that explored the survival benefit of bursectomy for resectable GC was published. The 5-year OS in the non-bursectomy group (omentectomy alone) was 76.7%, compared with 76.9% in the bursectomy group (one-sided P = 0.65), with no extra survival benefit from bursectomy. Moreover, based on the JCOG1001 data, the peritoneal recurrence rate in the bursectomy group was also the same as that in the non-bursectomy group (44%), suggesting that bursectomy could not improve peritoneal recurrence (64). In the light of the above-mentioned studies, omentectomy and bursectomy not only failed to prevent peritoneal metastasis or to improve the long-term survival but also increased the operation time, intraoperative blood loss, and complications. Therefore, it seems meaningless to add omentectomy or bursectomy to the radical resection of GC. Although many studies have reported that omentectomy does not improve survival benefits to patients, it is still part of the standard gastrectomy guidelines (32, 35, 65). This may be because it is easier to perform omentectomy than preserve the omentum in GC resection, and omentectomy is beneficial for lymph node dissection. Bursectomy is mainly used in Japan and included in Japanese GC treatment guidelines (65). The fifth edition of the Japanese guidelines refers to the conclusion of the JCOG1001 trial, but bursectomy has not been revised yet (64, 65). The sixth edition of the Japanese guidelines may reinterpret the application of omentectomy and bursectomy.
In the process of radical surgery for GC, blood from intraoperative bleeding easily accumulates in the abdominal cavity, which brings the peritoneal surface directly in contact with blood components, thus activating the extravascular blood cells to produce a variety of cytokines and thereby providing a favorable survival microenvironment for tumor cells that leak into the abdominal cavity. A retrospective study of 540 patients with AGC who underwent radical resection found that large intraoperative bleeding is associated with a high risk of peritoneal metastasis, whereas small bleeding is not, and patients with large intraoperative hemorrhages are more likely to develop peritoneal recurrence (66). Another retrospective research showed a significantly higher peritoneal recurrence rate in patients who received allogeneic blood transfusion during the perioperative period of radical resection for GC than that in patients without allogeneic blood transfusion (22.8 vs. 9.3%); however, the rates of metastasis to the liver, lung, and lymph nodes did not change (67). Therefore, surgeons should avoid the higher risks of postoperative peritoneal recurrence related to the development of intraoperative bleeding by minimizing intraoperative blood loss to avoid allogeneic blood transfusion.
The mechanism of extensive intra-operative peritoneal lavage (EIPL), a simple adjunctive surgical method, is based on limited dilution to reduce the risk of cancer cell dissemination resulting from surgery. Previous studies have shown that EIPL could effectively reduce the level of cancer cells spreading in the peritoneal cavity during radical resection for GC, and the use of distilled water is as effective as normal saline (36). However, the CCOG1102 trial showed the opposite results of no significant difference in peritoneal relapse-free survival rate (P = 0.676) and DFS and OS between the EIPL and non-EIPL groups after radical gastrectomy. In this trial, EIPL could neither reduce postoperative peritoneal dissemination nor improve the prognosis of patients, but it seemed to ameliorate DFS for patients with higher intraoperative blood loss or postoperative abdominal infection (68). In this study, most patients had negative peritoneal cytology results, so, even if there were undetected free tumor cells, washing the abdominal cavity with less saline is sufficient to remove them in the non-EIPL group, which may be the reason why there was no significant difference between the EIPL and non-EIPL groups. In the latest phase 3, multicenter, large-sample RCT (NCT02140034), the 3-year OS rates in the EIPL and surgery-alone groups were 77.0 and 76.7% (P = 0.62), respectively, while the 3-year cumulative incidences in peritoneal recurrence were 7.9 and 6.6% (P = 0.35), respectively. On the contrary, EIPL not only failed to reduce peritoneal recurrence and improve patient survival but also significantly increased the incidence of adverse events (69). Wound infections and liver function abnormalities were more common in patients receiving EIPL than in patients undergoing surgery alone (2.0 vs. 0.3% and 1.7 vs. 0.3%, respectively). Furthermore, the incidence of death due to adverse events in the EIPL group (2.3%) was also higher than that in the surgery-alone group (0.6%). However, another large-scale, multicenter (11 centers) RCT (NCT02745509) in China showed that the postoperative adverse events and mortality in the EIPL group are lower than those of the surgery-alone group (11.1 vs. 17.0%, P = 0.04; 0 vs. 1.9%, P = 0.02) (70). In this trial, the long-term results have not been released yet.
Hyperthermic intraperitoneal chemotherapy (HIPEC), a combination therapy with precise temperature control for circulating intraperitoneal perfusion of chemotherapeutic agents, has been widely used in the prevention and treatment of peritoneal metastatic tumors. For patients with serosal invasion in GC, compared with the non-HIPEC group, the survival of HIPEC patients significantly improved (P < 0.00001), with a remarkably reduced peritoneal recurrence rate (P = 0.001) (71). A retrospective study involving 38 GC patients with serosal invasion showed that the peritoneal recurrence in the HIPEC group is dramatically lower than that in the radical-surgery-alone group (11.1 vs. 73.7%, respectively, P < 0.001) (72). In another RCT of resectable AGC, the results were similar to the previous RCT results, with much higher peritoneal recurrence in the non-HIPEC group (30%) than that in the HIPEC group (5%) (73). Taken together, HIPEC is an effective method for preventing postoperative peritoneal metastasis in high-risk patients. Presently, the use of HIPEC in most countries is mainly confined to the treatment of peritoneal metastatic carcinoma, which has not been included as a standard practice for the preventive therapy of peritoneal recurrence. Firstly, there may be few medical institutions with equipment and conditions for such treatment. Secondly, the pros and cons of whether the conditions of the patients would still be conducive to accepting HIPEC after severe trauma from radical surgery need to be weighed. Most importantly, there is still a lack of valid evidence from large-sample-size RCTs to support the survival benefits of HIPEC.
In addition to the previously mentioned methods for evaluating the risk of preoperative peritoneal recurrence, pathological analysis of the resected tumor specimens also has considerable value. In AGC patients undergoing radical gastrectomy, the depth of tumor invasion was the only risk factor significantly associated with peritoneal recurrence (74). Yoo et al. analyzed the prospective data of 655 patients that underwent radical resection for GC. The time to peritoneal relapse in patients with macroscopic serosal lesions was considerably shorter than that in patients without serosal lesions (P < 0.001), and the 5-year peritoneal recurrence rates were 32.8 and 8.7%, respectively. These results suggest that the macroscopic assessment of serosal lesions may be a useful index to predict the risk of peritoneal recurrence after radical resection (75). In accordance with the Japanese Classification of Gastric Carcinoma, tumor infiltrative pattern (INF) is classified into INFa (expanding growth with a distinct border from the surrounding tissue), INFb (an intermediate pattern between INFa and INFc), and INFc (infiltrative growth with no distinct border with the surrounding tissue) (76). Compared with INFa and INFb, INFc patients had significantly more peritoneal metastases; furthermore, INF was found to be an independent risk factor for peritoneal recurrence after radical gastrectomy (77–80). A previous study found that adjuvant chemotherapy could not improve the peritoneal recurrence rate in INFc group but reduced the rate in the INFa/b group (78). In a recent study, Chen et al. employed multiphoton imaging technology to quantitatively analyze the collagen characteristics in the tumor microenvironment from the tissue specimens infiltrating the gastric serosa. They revealed that the features of collagen are related to postoperative peritoneal metastasis in GC with serosal invasion. Furthermore, a collagen nomogram that they constructed to predict the risk of peritoneal recurrence with serosa-positive GC after radical gastrectomy displayed a stronger predictive power than the clinicopathological model (81).
To eliminate the microscopic peritoneal lesions after resection of GC, early postoperative intraperitoneal chemotherapy (EPIC) is administered using mitomycin C and 5-fluorouracil (5-FU) or taxanes through inflow and outflow catheters. This is usually performed 1–5 days after surgery and then repeated subsequently every 24 h. As reported in another study, although the safety of EPIC after radical gastrectomy was acceptable, there was no difference in postoperative survival between patients who received EPIC and those who did not, implying that EPIC could not provide survival benefits to patients undergoing curative resection for GC (82). However, the small sample size of 46 patients was a limitation of that study. A retrospective study based on 245 serosa-positive GC patients who underwent radical surgery found that the 5-year OS- and GC-specific survival rates in the EPIC group were significantly better than those in the non-EPIC group. Moreover, the rate of peritoneal recurrence in the EPIC group is notably lower than in the non-EPIC group (18.5 vs. 32.2%, P = 0.038) (83). Therefore, EPIC appears to be an effective method for GC patients at a high risk of peritoneal recurrence by improving their survival through reducing peritoneal metastases.
Systemic adjuvant chemotherapy for GC patients after surgery has always been important in clinical studies, and clinicians pay great attention to the formulation of a therapeutic regimen and the effects of different schemes on postoperative recurrence. Adjuvant chemotherapy regimens generally include oral 5-FU as monotherapy (including S-1 and capecitabine) or combined with oxaliplatin. In a phase 2 clinical trial (CCOG0301), the 2-year survival rate was higher among GC patients with positive peritoneal lavage cytology treated with oral S-1 after radical resection than among historical controls (84). All the cases included in this trial had positive peritoneal cytology. Sasako et al. conducted a randomized phase 3 clinical trial to evaluate the effect of S-1 as adjuvant chemotherapy for GC patients after radical resection. They found that the 5-year survival outcomes in the S-1 group are better than that in the surgery-only group. In terms of recurrence, the overall relapse rate in the S-1 group is lower than that in the surgery-only group; in particular, the lymph nodes and peritoneum recurrence rates decreased significantly, and postoperative adjuvant therapy with S-1 could reduce the risk of recurrence by 34.7% (85). The patients enrolled in the study had pathological stage II or IIIA/B with CY0, and the chemotherapy regimen was still S-1 monotherapy. In another phase 3 clinical trial, JCOG9206-2, cisplatin combined with UFT could not improve the overall and relapse-free survival in patients with serosal invasive GC after radical resection (86). According to the data in this trial, adding adjuvant chemotherapy, compared with surgery alone, could not reduce peritoneal metastasis. The patients who participated in the trial had GC with macroscopic serosa-invasive, negative peritoneal lavage cytology without distant metastasis. The postoperative treatment plan was intraperitoneal chemotherapy with cisplatin before abdominal closure, followed by intravenous chemotherapy (cisplatin + 5-FU + UFT). A meta-analysis including 3,897 patients undergoing radical resection of GC showed that the addition of adjuvant chemotherapy significantly reduced the rate of peritoneal recurrence compared with surgery alone (P = 0.001) (87). However, the above-mentioned research only analyzed all the regimens together and did not classify the specific adjuvant chemotherapy schemes in the analyses. Recently, a randomized, controlled phase 3 trial of S-l plus docetaxel adjuvant chemotherapy in patients after radical gastrectomy reported that the 3-year RFS in the S-l plus docetaxel group was better than that in the S-1 monotherapy group (P < 0.001). Although the hematogenous site and node recurrence rates in the combination group are significantly lower than that in the S-1-alone group, there was no statistically significant difference between these two groups in peritoneal relapse (9.3 vs. 12.9%, P = 0.092). This suggests that S-1, combined with docetaxel adjuvant chemotherapy regimen, does not improve peritoneal metastasis after radical resection of GC compared with S-1 monotherapy (88).
In accordance with previous studies, there is yet no definite conclusion on the effects of postoperative adjuvant chemotherapy in the prevention of peritoneal metastasis after radical gastrectomy of GC. Drug selection and therapeutic regimen are crucial for the appropriate method, and this still needs to be supported with a large number of clinical studies.
The occurrence of peritoneal metastasis after radical gastrectomy seriously affects the prognosis of patients to a great extent, and how to identify patients at a high risk of peritoneal recurrence and develop preventive treatment approaches quickly is vital for the reduction of postoperative peritoneal metastasis. The progression degree of GC is significantly correlated with the resection effect of radical gastrectomy. The greater the progression degree, the lower the possibility of R0 resection that is accompanied by patients at a high risk of peritoneal metastasis. Even if patients with AGC could receive curative surgery and other related treatments, their long-term survival is still relatively poor. Undoubtedly, early detection of tumors cannot only improve the effect of radical resection but also greatly reduce the risk of spread of tumor cells in the peritoneal cavity during operation. Therefore, cancer screening has a more practical significance than any other therapeutic method to avoid postoperative peritoneal metastasis. Presently, many countries with a high incidence of GC, such as Japan and South Korea, have established and formulated their own guidelines for GC screening. There are certain effects on preventing peritoneal metastasis after radical resection of GC through accurate judgment of determining peritoneal status, improvement of surgical procedure, peritoneal lavage, intraperitoneal chemotherapy, and adjuvant chemotherapy (Tables 1, 2). Despite all these findings, several prospective multicenter studies are essential to elucidate clinical evidence, promoting the criteria for the prevention of peritoneal recurrence after radical resection in the management of GC.
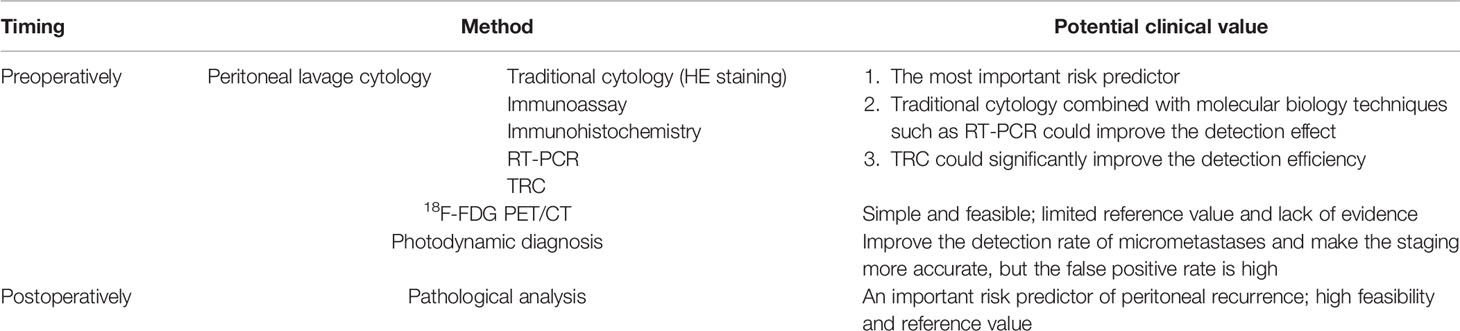
Table 1 Predictive methods of peritoneal recurrence.
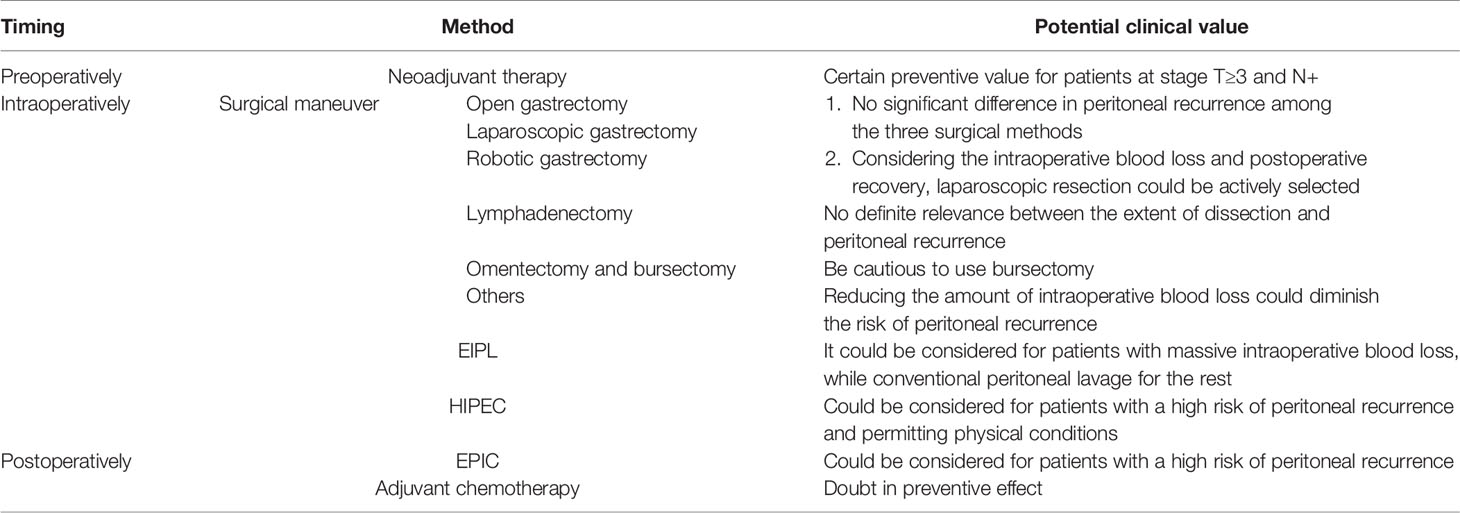
Table 2 Preventive methods of peritoneal recurrence.
LX and HC contributed to the conception and design of the review. LX and SJ collected the related paper and drafted the manuscript. YZ, PZ and EM revised the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by fund from the National Key Research and Development Program of China (2017YFC1601502); Key Talents Project of Gansu Province (2019RCXM020); Key Project of Science and Technology in Gansu Province (19ZD2WA001); Science and Technology Project of Chengguan District of Lanzhou City (2019RCCX0034); Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2017-ZD01); and Project supported by the Science-Technology Foundation for Young Scientist of Gansu Province (21JR1RA163).
Author SJ was employed by company Beijing Weitai’an Pharmaceutical Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Ikoma N, Chen HC, Wang X, Blum M, Estrella JS, Fournier K, et al. Patterns of Initial Recurrence in Gastric Adenocarcinoma in the Era of Preoperative Therapy. Ann Surg Oncol (2017) 24(9):2679–87. doi: 10.1245/s10434-017-5838-y
3. Yoo CH, Noh SH, Shin DW, Choi SH, Min JS. Recurrence Following Curative Resection for Gastric Carcinoma. Br J Surg (2000) 87(2):236–42. doi: 10.1046/j.1365-2168.2000.01360.x
4. Nashimoto A, Akazawa K, Isobe Y, Miyashiro I, Katai H, Kodera Y, et al. Gastric Cancer Treated in 2002 in Japan: 2009 Annual Report of the JGCA Nationwide Registry. Gastric Cancer (2013) 16(1):1–27. doi: 10.1007/s10120-012-0163-4
5. Oh CA, Bae JM, Oh SJ, Choi MG, Noh JH, Sohn TS, et al. Long-Term Results and Prognostic Factors of Gastric Cancer Patients With Only Positive Peritoneal Lavage Cytology. J Surg Oncol (2012) 105(4):393–9. doi: 10.1002/jso.22091
6. Nakamura K, Ueyama T, Yao T, Xuan ZX, Ambe K, Adachi Y, et al. Pathology and Prognosis of Gastric Carcinoma. Findings in 10,000 Patients Who Underwent Primary Gastrectomy. Cancer (1992) 70(5):1030–7. doi: 10.1002/1097-0142(19920901)70:5<1030::aid-cncr2820700504>3.0.co;2-c
7. Boku T, Nakane Y, Minoura T, Takada H, Yamamura M, Hioki K, et al. Prognostic Significance of Serosal Invasion and Free Intraperitoneal Cancer Cells in Gastric Cancer. Br J Surg (1990) 77(4):436–9. doi: 10.1002/bjs.1800770425
8. Griniatsos J, Michail O, Dimitriou N, Karavokyros I. Lymph Node, Peritoneal and Bone Marrow Micrometastases in Gastric Cancer: Their Clinical Significance. World J Gastrointest Oncol (2012) 4(2):16–21. doi: 10.4251/wjgo.v4.i2.16
9. Leake PA, Cardoso R, Seevaratnam R, Lourenco L, Helyer L, Mahar A, et al. A Systematic Review of the Accuracy and Utility of Peritoneal Cytology in Patients With Gastric Cancer. Gastric Cancer (2012) 15(1):011–0071. doi: 10.1007/s10120-011-0071-z
10. Xiao Y, Zhang J, He X, Ji J, Wang G. Diagnostic Values of Carcinoembryonic Antigen in Predicting Peritoneal Recurrence After Curative Resection of Gastric Cancer: A Meta-Analysis. Ir J Med Sci (2014) 183(4):557–64. doi: 10.1007/s11845-013-1051-6
11. Chae HD, Kim IH. Prognostic Significance of CEA Expression by RT-PCR in Peritoneal Wash From Patients With Gastric Cancer: Result of a 5-Year Follow-Up After Curative Resection. Scand J Gastroenterol (2016) 51(8):956–60. doi: 10.3109/00365521.2016.1172339
12. Hasbahceci M, Akcakaya A, Guler B, Kunduz E, Malya FU, Muslumanoglu M. Use of Peritoneal Washing Cytology for the Detection of Free Peritoneal Cancer Cells Before and After Surgical Treatment of Gastric Adenocarcinoma. J Cancer Res Ther (2018) 14(6):1225–9. doi: 10.4103/0973-1482.184518
13. Ishii T, Fujiwara Y, Ohnaka S, Hayashi T, Taniguchi H, Takiguchi S, et al. Rapid Genetic Diagnosis With the Transcription-Reverse Transcription Concerted Reaction System for Cancer Micrometastasis. Ann Surg Oncol (2004) 11(8):778–85. doi: 10.1245/ASO.2004.12.043
14. Ohashi N, Nakanishi H, Kodera Y, Ito S, Mochizuki Y, Koike M, et al. Intraoperative Quantitative Detection of CEA mRNA in the Peritoneal Lavage of Gastric Cancer Patients With Transcription Reverse-Transcription Concerted (TRC) Method. A Comparative Study With Real-Time Quantitative RT-PCR. Anticancer Res (2007) 27(4C):2769–77.
15. Fujiwara Y, Okada K, Hanada H, Tamura S, Kimura Y, Fujita J, et al. The Clinical Importance of a Transcription Reverse-Transcription Concerted (TRC) Diagnosis Using Peritoneal Lavage Fluids in Gastric Cancer With Clinical Serosal Invasion: A Prospective, Multicenter Study. Surgery (2014) 155(3):417–23. doi: 10.1016/j.surg.2013.10.004
16. Sugimura K, Fujiwara Y, Omori T, Motoori M, Miyoshi N, Akita H, et al. Clinical Importance of a Transcription Reverse-Transcription Concerted (TRC) Diagnosis Using Peritoneal Lavage Fluids Obtained Pre- and Post-Lymphadenectomy From Gastric Cancer Patients. Surg Today (2016) 46(6):654–60. doi: 10.1007/s00595-015-1235-y
17. Lee JW, Jo K, Cho A, Noh SH, Lee JD, Yun M. Relationship Between 18f-FDG Uptake on PET and Recurrence Patterns After Curative Surgical Resection in Patients With Advanced Gastric Cancer. J Nucl Med (2015) 56(10):1494–500. doi: 10.2967/jnumed.115.160580
18. Lee JW, Son MW, Chung IK, Cho YS, Lee MS, Lee SM. Significance of CT Attenuation and F-18 Fluorodeoxyglucose Uptake of Visceral Adipose Tissue for Predicting Survival in Gastric Cancer Patients After Curative Surgical Resection. Gastric Cancer (2020) 23(2):273–84. doi: 10.1007/s10120-019-01001-2
19. Murayama Y, Ichikawa D, Koizumi N, Komatsu S, Shiozaki A, Kuriu Y, et al. Staging Fluorescence Laparoscopy for Gastric Cancer by Using 5-Aminolevulinic Acid. Anticancer Res (2012) 32(12):5421–7.
20. Kishi K, Fujiwara Y, Yano M, Inoue M, Miyashiro I, Motoori M, et al. Staging Laparoscopy Using ALA-Mediated Photodynamic Diagnosis Improves the Detection of Peritoneal Metastases in Advanced Gastric Cancer. J Surg Oncol (2012) 106(3):294–8. doi: 10.1002/jso.23075
21. Koizumi N, Harada Y, Minamikawa T, Tanaka H, Otsuji E, Takamatsu T. Recent Advances in Photodynamic Diagnosis of Gastric Cancer Using 5-Aminolevulinic Acid. World J Gastroenterol (2016) 22(3):1289–96. doi: 10.3748/wjg.v22.i3.1289
22. Ushimaru Y, Fujiwara Y, Kishi K, Sugimura K, Omori T, Moon JH, et al. Prognostic Significance of Basing Treatment Strategy on the Results of Photodynamic Diagnosis in Advanced Gastric Cancer. Ann Surg Oncol (2017) 24(4):983–9. doi: 10.1245/s10434-016-5660-y
23. Kishi K, Fujiwara Y, Yano M, Motoori M, Sugimura K, Ohue M, et al. Diagnostic Laparoscopy With 5-Aminolevulinic-Acid-Mediated Photodynamic Diagnosis Enhances the Detection of Peritoneal Micrometastases in Advanced Gastric Cancer. Oncology (2014) 87(5):257–65. doi: 10.1159/000365356
24. Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, et al. Perioperative Chemotherapy Versus Surgery Alone for Resectable Gastroesophageal Cancer. N Engl J Med (2006) 355(1):11–20. doi: 10.1056/NEJMoa055531
25. Coccolini F, Nardi M, Montori G, Ceresoli M, Celotti A, Cascinu S, et al. Neoadjuvant Chemotherapy in Advanced Gastric and Esophago-Gastric Cancer. Meta-Analysis of Randomized Trials. Int J Surg (2018) 51:120–7. doi: 10.1016/j.ijsu.2018.01.008
26. Mokadem I, Dijksterhuis WPM, van Putten M, Heuthorst L, de Vos-Geelen JM, Haj Mohammad N, et al. Recurrence After Preoperative Chemotherapy and Surgery for Gastric Adenocarcinoma: A Multicenter Study. Gastric Cancer (2019) 22(6):1263–73. doi: 10.1007/s10120-019-00956-6
27. Agnes A, Biondi A, Laurino A, Strippoli A, Ricci R, Pozzo C, et al. A Detailed Analysis of the Recurrence Timing and Pattern After Curative Surgery in Patients Undergoing Neoadjuvant Therapy or Upfront Surgery for Gastric Cancer. J Surg Oncol (2020) 122(2):293–305. doi: 10.1002/jso.25959
28. Kang YK, Yook JH, Park YK, Lee JS, Kim YW, Kim JY, et al. PRODIGY: A Phase III Study of Neoadjuvant Docetaxel, Oxaliplatin, and S-1 Plus Surgery and Adjuvant S-1 Versus Surgery and Adjuvant S-1 for Resectable Advanced Gastric Cancer. J Clin Oncol (2021) 39(26):2903–13. doi: 10.1200/JCO.20.02914
29. Pachaury A, Chaudhari V, Batra S, Ramaswamy A, Ostwal V, Engineer R, et al. Pathological N3 Stage (Pn3/Ypn3) Gastric Cancer: Outcomes, Prognostic Factors and Pattern of Recurrences After Curative Treatment. Ann Surg Oncol (2021) 20(10):021–10405. doi: 10.1245/s10434-021-10405-3
30. Nakauchi M, Vos E, Tang LH, Gonen M, Janjigian YY, Ku GY, et al. Outcomes of Neoadjuvant Chemotherapy for Clinical Stages 2 and 3 Gastric Cancer Patients: Analysis of Timing and Site of Recurrence. Ann Surg Oncol (2021) 28(9):4829–38. doi: 10.1245/s10434-021-09624-5
31. Xu W, Wang L, Yan C, He C, Lu S, Ni Z, et al. Neoadjuvant Chemotherapy Versus Direct Surgery for Locally Advanced Gastric Cancer With Serosal Invasion (cT4NxM0): A Propensity Score-Matched Analysis. Front Oncol (2021) 11:718556. doi: 10.3389/fonc.2021.718556
32. De Manzoni G, Marrelli D, Baiocchi GL, Morgagni P, Saragoni L, Degiuli M, et al. The Italian Research Group for Gastric Cancer (GIRCG) Guidelines for Gastric Cancer Staging and Treatment: 2015. Gastric Cancer (2017) 20(1):20–30. doi: 10.1007/s10120-016-0615-3
33. Slagter AE, Jansen EPM, van Laarhoven HWM, van Sandick JW, van Grieken NCT, Sikorska K, et al. CRITICS-II: A Multicentre Randomised Phase II Trial of Neo-Adjuvant Chemotherapy Followed by Surgery Versus Neo-Adjuvant Chemotherapy and Subsequent Chemoradiotherapy Followed by Surgery Versus Neo-Adjuvant Chemoradiotherapy Followed by Surgery in Resectable Gastric Cancer. BMC Cancer (2018) 18(1):018–4770. doi: 10.1186/s12885-018-4770-2
34. Smyth EC, Verheij M, Allum W, Cunningham D, Cervantes A, Arnold D. Gastric Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol (2016) 27(suppl 5):v38–49. doi: 10.1093/annonc/mdw350
35. Wang FH, Zhang XT, Li YF, Tang L, Qu XJ, Ying JE, et al. The Chinese Society of Clinical Oncology (CSCO): Clinical Guidelines for the Diagnosis and Treatment of Gastric Cancer, 2021. Cancer Commun (2021) 41(8):747–95. doi: 10.1002/cac2.12193
36. Yu XF, Ren ZG, Xue YW, Song HT, Wei YZ, Li CM. D2 Lymphadenectomy can Disseminate Tumor Cells Into Peritoneal Cavity in Patients With Advanced Gastric Cancer. Neoplasma (2013) 60(2):174–81. doi: 10.4149/neo_2013_023
37. Pak KH, Hyung WJ, Son T, Obama K, Woo Y, Kim HI, et al. Long-Term Oncologic Outcomes of 714 Consecutive Laparoscopic Gastrectomies for Gastric Cancer: Results From the 7-Year Experience of a Single Institute. Surg Endosc (2012) 26(1):130–6. doi: 10.1007/s00464-011-1838-3
38. Nakagawa M, Kojima K, Inokuchi M, Kato K, Sugita H, Kawano T, et al. Patterns, Timing and Risk Factors of Recurrence of Gastric Cancer After Laparoscopic Gastrectomy: Reliable Results Following Long-Term Follow-Up. Eur J Surg Oncol (2014) 40(10):1376–82. doi: 10.1016/j.ejso.2014.04.015
39. Lee JH, Nam BH, Ryu KW, Ryu SY, Kim YW, Park YK, et al. Comparison of the Long-Term Results of Patients Who Underwent Laparoscopy Versus Open Distal Gastrectomy. Surg Endosc (2016) 30(2):430–6. doi: 10.1007/s00464-015-4215-9
40. Hu Y, Huang C, Sun Y, Su X, Cao H, Hu J, et al. Morbidity and Mortality of Laparoscopic Versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: A Randomized Controlled Trial. J Clin Oncol (2016) 34(12):1350–7. doi: 10.1200/JCO.2015.63.7215
41. Zhang X, Sun F, Li S, Gao W, Wang Y, Hu SY. A Propensity Score-Matched Case-Control Comparative Study of Laparoscopic and Open Gastrectomy for Locally Advanced Gastric Carcinoma. J Buon (2016) 21(1):118–24.
42. Li B, Yu-Hong Wong I, Siu-Yin Chan F, Chan KK, Lai-Yin Wong C, Law TT, et al. Comparison of Laparoscopic Versus Open Gastrectomy for Gastric Cancer. Surg Oncol (2020) 35:14–21. doi: 10.1016/j.suronc.2020.06.008
43. Ramos M, Pereira MA, Dias AR, Ribeiro U Jr, Zilberstein B, Nahas SC. Laparoscopic Gastrectomy for Early and Advanced Gastric Cancer in a Western Center: A Propensity Score-Matched Analysis. Updates Surg (2021) 73(5):1867–77. doi: 10.1007/s13304-021-01097-1
44. Lu J, Wu D, Xu BB, Xue Z, Zheng HL, Xie JW, et al. A Matched Cohort Study of the Failure Pattern After Laparoscopic and Open Gastrectomy for Locally Advanced Gastric Cancer: Does the Operative Approach Matter? Surg Endosc (2021) 16(10):021–08337. doi: 10.1007/s00464-021-08337-w
45. Kim HH, Han SU, Kim MC, Kim W, Lee HJ, Ryu SW, et al. Effect of Laparoscopic Distal Gastrectomy vs Open Distal Gastrectomy on Long-Term Survival Among Patients With Stage I Gastric Cancer: The KLASS-01 Randomized Clinical Trial. JAMA Oncol (2019) 5(4):506–13. doi: 10.1001/jamaoncol.2018.6727
46. Yu J, Huang C, Sun Y, Su X, Cao H, Hu J, et al. Effect of Laparoscopic vs Open Distal Gastrectomy on 3-Year Disease-Free Survival in Patients With Locally Advanced Gastric Cancer: The CLASS-01 Randomized Clinical Trial. Jama (2019) 321(20):1983–92. doi: 10.1001/jama.2019.5359
47. Hyung WJ, Yang HK, Park YK, Lee HJ, An JY, Kim W, et al. Long-Term Outcomes of Laparoscopic Distal Gastrectomy for Locally Advanced Gastric Cancer: The KLASS-02-RCT Randomized Clinical Trial. J Clin Oncol (2020) 38(28):3304–13. doi: 10.1200/JCO.20.01210
48. Shi Y, Xu X, Zhao Y, Qian F, Tang B, Hao Y, et al. Long-Term Oncologic Outcomes of a Randomized Controlled Trial Comparing Laparoscopic Versus Open Gastrectomy With D2 Lymph Node Dissection for Advanced Gastric Cancer. Surgery (2019) 165(6):1211–6. doi: 10.1016/j.surg.2019.01.003
49. Jiang Y, Zhao Y, Qian F, Shi Y, Hao Y, Chen J, et al. The Long-Term Clinical Outcomes of Robotic Gastrectomy for Gastric Cancer: A Large-Scale Single Institutional Retrospective Study. Am J Transl Res (2018) 10(10):3233–42.
50. Guerrini GP, Esposito G, Magistri P, Serra V, Guidetti C, Olivieri T, et al. Robotic Versus Laparoscopic Gastrectomy for Gastric Cancer: The Largest Meta-Analysis. Int J Surg (2020) 82:210–28. doi: 10.1016/j.ijsu.2020.07.053
51. Nakauchi M, Vos E, Janjigian YY, Ku GY, Schattner MA, Nishimura M, et al. Comparison of Long- and Short-Term Outcomes in 845 Open and Minimally Invasive Gastrectomies for Gastric Cancer in the United States. Ann Surg Oncol (2021) 28(7):3532–44. doi: 10.1245/s10434-021-09798-y
52. Aiolfi A, Lombardo F, Matsushima K, Sozzi A, Cavalli M, Panizzo V, et al. Systematic Review and Updated Network Meta-Analysis of Randomized Controlled Trials Comparing Open, Laparoscopic-Assisted, and Robotic Distal Gastrectomy for Early and Locally Advanced Gastric Cancer. Surgery (2021) 170(3):942–51. doi: 10.1016/j.surg.2021.04.014
53. Marano L, Fusario D, Savelli V, Marrelli D, Roviello F. Robotic Versus Laparoscopic Gastrectomy for Gastric Cancer: An Umbrella Review of Systematic Reviews and Meta-Analyses. Updates Surg (2021) 25(10):021–01059. doi: 10.1007/s13304-021-01059-7
54. Mocellin S. The Effect of Lymph Node Dissection on the Survival of Patients With Operable Gastric Carcinoma. JAMA Oncol (2016) 2(10):1363–4. doi: 10.1001/jamaoncol.2016.2044
55. Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical Treatment of Gastric Cancer: 15-Year Follow-Up Results of the Randomised Nationwide Dutch D1D2 Trial. Lancet Oncol (2010) 11(5):439–49. doi: 10.1016/S1470-2045(10)70070-X
56. Nakanishi Y, Ohara M, Domen H, Shichinohe T, Hirano S, Ishizaka M. Differences in Risk Factors Between Patterns of Recurrence in Patients After Curative Resection for Advanced Gastric Carcinoma. World J Surg Oncol (2013) 11(98):1477–7819. doi: 10.1186/1477-7819-11-98
57. de Manzoni G, Verlato G, Bencivenga M, Marrelli D, Di Leo A, Giacopuzzi S, et al. Impact of Super-Extended Lymphadenectomy on Relapse in Advanced Gastric Cancer. Eur J Surg Oncol (2015) 41(4):534–40. doi: 10.1016/j.ejso.2015.01.023
58. Kota I, Makoto H, Satoshi K, Yutaka T, Etsuro B, Masanori T. Oncologic Feasibility of D1+ Gastrectomy for Patients With cT1N1, cT2N0-1, or cT3N0 Gastric Cancer. Eur J Surg Oncol (2021) 47(2):456–62. doi: 10.1016/j.ejso.2020.07.031
59. Hayashi S, Kanda M, Ito S, Mochizuki Y, Teramoto H, Ishigure K, et al. Number of Retrieved Lymph Nodes Is an Independent Prognostic Factor After Total Gastrectomy for Patients With Stage III Gastric Cancer: Propensity Score Matching Analysis of a Multi-Institution Dataset. Gastric Cancer (2019) 22(4):853–63. doi: 10.1007/s10120-018-0902-2
60. Jongerius EJ, Boerma D, Seldenrijk KA, Meijer SL, Scheepers JJ, Smedts F, et al. Role of Omentectomy as Part of Radical Surgery for Gastric Cancer. Br J Surg (2016) 103(11):1497–503. doi: 10.1002/bjs.10149
61. Sakimura Y, Inaki N, Tsuji T, Kadoya S, Bando H. Long-Term Outcomes of Omentum-Preserving Versus Resecting Gastrectomy for Locally Advanced Gastric Cancer With Propensity Score Analysis. Sci Rep (2020) 10(1):020–73367. doi: 10.1038/s41598-020-73367-8
62. Fujita J, Kurokawa Y, Sugimoto T, Miyashiro I, Iijima S, Kimura Y, et al. Survival Benefit of Bursectomy in Patients With Resectable Gastric Cancer: Interim Analysis Results of a Randomized Controlled Trial. Gastric Cancer (2012) 15(1):42–8. doi: 10.1007/s10120-011-0058-9
63. Eom BW, Joo J, Kim YW, Bae JM, Park KB, Lee JH, et al. Role of Bursectomy for Advanced Gastric Cancer: Result of a Case-Control Study From a Large Volume Hospital. Eur J Surg Oncol (2013) 39(12):1407–14. doi: 10.1016/j.ejso.2013.09.013
64. Kurokawa Y, Doki Y, Mizusawa J, Terashima M, Katai H, Yoshikawa T, et al. Bursectomy Versus Omentectomy Alone for Resectable Gastric Cancer (JCOG1001): A Phase 3, Open-Label, Randomised Controlled Trial. Lancet Gastroenterol Hepatol (2018) 3(7):460–8. doi: 10.1016/S2468-1253(18)30090-6
65. Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2018 (5th Edition). Gastric Cancer (2021) 24(1):1–21. doi: 10.1007/s10120-020-01042-y
66. Arita T, Ichikawa D, Konishi H, Komatsu S, Shiozaki A, Hiramoto H, et al. Increase in Peritoneal Recurrence Induced by Intraoperative Hemorrhage in Gastrectomy. Ann Surg Oncol (2015) 22(3):758–64. doi: 10.1245/s10434-014-4060-4
67. Kanda M, Kobayashi D, Tanaka C, Iwata N, Yamada S, Fujii T, et al. Adverse Prognostic Impact of Perioperative Allogeneic Transfusion on Patients With Stage II/III Gastric Cancer. Gastric Cancer (2016) 19(1):255–63. doi: 10.1007/s10120-014-0456-x
68. Misawa K, Mochizuki Y, Sakai M, Teramoto H, Morimoto D, Nakayama H, et al. Randomized Clinical Trial of Extensive Intraoperative Peritoneal Lavage Versus Standard Treatment for Resectable Advanced Gastric Cancer (CCOG 1102 Trial). Br J Surg (2019) 106(12):1602–10. doi: 10.1002/bjs.11303
69. Yang HK, Ji J, Han SU, Terashima M, Li G, Kim HH, et al. Extensive Peritoneal Lavage With Saline After Curative Gastrectomy for Gastric Cancer (EXPEL): A Multicentre Randomised Controlled Trial. Lancet Gastroenterol Hepatol (2021) 6(2):120–7. doi: 10.1016/S2468-1253(20)30315-0
70. Guo J, Xu A, Sun X, Zhao X, Xia Y, Rao H, et al. Combined Surgery and Extensive Intraoperative Peritoneal Lavage vs Surgery Alone for Treatment of Locally Advanced Gastric Cancer: The SEIPLUS Randomized Clinical Trial. JAMA Surg (2019) 154(7):610–6. doi: 10.1001/jamasurg.2019.0153
71. Sun J, Song Y, Wang Z, Gao P, Chen X, Xu Y, et al. Benefits of Hyperthermic Intraperitoneal Chemotherapy for Patients With Serosal Invasion in Gastric Cancer: A Meta-Analysis of the Randomized Controlled Trials. BMC Cancer (2012) 12(526):1471–2407. doi: 10.1186/1471-2407-12-526
72. Yarema RR, Ohorchak MA, Zubarev GP, Mylyan YP, Oliynyk YY, Zubarev MG, et al. Hyperthermic Intraperitoneal Chemoperfusion in Combined Treatment of Locally Advanced and Disseminated Gastric Cancer: Results of a Single-Centre Retrospective Study. Int J Hyperthermia (2014) 30(3):159–65. doi: 10.3109/02656736.2014.893451
73. Beeharry MK, Zhu ZL, Liu WT, Yao XX, Yan M, Zhu ZG. Correction to: Prophylactic HIPEC With Radical D2 Gastrectomy Improves Survival and Peritoneal Recurrence Rates for Locally Advanced Gastric Cancer: Personal Experience From a Randomized Case Control Study. BMC Cancer (2019) 19(1):019–6411. doi: 10.1186/s12885-019-6411-9
74. Chou HH, Kuo CJ, Hsu JT, Chen TH, Lin CJ, Tseng JH, et al. Clinicopathologic Study of Node-Negative Advanced Gastric Cancer and Analysis of Factors Predicting Its Recurrence and Prognosis. Am J Surg (2013) 205(6):623–30. doi: 10.1016/j.amjsurg.2012.04.014
75. Yoo C, Ryu MH, Park YS, Yoo MW, Park SR, Ryoo BY, et al. Intraoperatively Assessed Macroscopic Serosal Changes in Patients With Curatively Resected Advanced Gastric Cancer: Clinical Implications for Prognosis and Peritoneal Recurrence. Ann Surg Oncol (2015) 22(9):2940–7. doi: 10.1245/s10434-014-4352-8
76. Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma: 3rd English Edition. Gastric Cancer (2011) 14(2):101–12. doi: 10.1007/s10120-011-0041-5
77. Huang B, Sun Z, Wang Z, Lu C, Xing C, Zhao B, et al. Factors Associated With Peritoneal Metastasis in Non-Serosa-Invasive Gastric Cancer: A Retrospective Study of a Prospectively-Collected Database. BMC Cancer (2013) 13(57):1471–2407. doi: 10.1186/1471-2407-13-57
78. Kanda M, Mizuno A, Fujii T, Shimoyama Y, Yamada S, Tanaka C, et al. Tumor Infiltrative Pattern Predicts Sites of Recurrence After Curative Gastrectomy for Stages 2 and 3 Gastric Cancer. Ann Surg Oncol (2016) 23(6):1934–40. doi: 10.1245/s10434-016-5102-x
79. Nakagawa N, Kanda M, Ito S, Mochizuki Y, Teramoto H, Ishigure K, et al. Pathological Tumor Infiltrative Pattern and Sites of Initial Recurrence in Stage II/III Gastric Cancer: Propensity Score Matching Analysis of a Multi-Institutional Dataset. Cancer Med (2018) 7(12):6020–9. doi: 10.1002/cam4.1868
80. Zhao B, Zhang J, Mei D, Huang X, Zou S, Luo R, et al. Prognostic Significance of Tumour Infiltration Growth Pattern in Patients With Advanced Gastric Cancer. J Clin Pathol (2019) 72(2):165–71. doi: 10.1136/jclinpath-2018-205403
81. Chen D, Liu Z, Liu W, Fu M, Jiang W, Xu S, et al. Predicting Postoperative Peritoneal Metastasis in Gastric Cancer With Serosal Invasion Using a Collagen Nomogram. Nat Commun (2021) 12(1):020–20429. doi: 10.1038/s41467-020-20429-0
82. Markelis R, Endzinas Z, Grižas S, Pundzius J, Saladžinskas Z, Juozaitytė E, et al. Early Postoperative Intraperitoneal Chemotherapy for the Treatment of Advanced Gastric Cancer. Medicina (2011) 47(1):63–9.
83. Kwon OK, Chung HY, Yu W. Early Postoperative Intraperitoneal Chemotherapy for Macroscopically Serosa-Invading Gastric Cancer Patients. Cancer Res Treat (2014) 46(3):270–9. doi: 10.4143/crt.2014.46.3.270
84. Kodera Y, Ito S, Mochizuki Y, Kondo K, Koshikawa K, Suzuki N, et al. A Phase II Study of Radical Surgery Followed by Postoperative Chemotherapy With S-1 for Gastric Carcinoma With Free Cancer Cells in the Peritoneal Cavity (CCOG0301 Study). Eur J Surg Oncol (2009) 35(11):1158–63. doi: 10.1016/j.ejso.2009.03.003
85. Sasako M, Sakuramoto S, Katai H, Kinoshita T, Furukawa H, Yamaguchi T, et al. Five-Year Outcomes of a Randomized Phase III Trial Comparing Adjuvant Chemotherapy With S-1 Versus Surgery Alone in Stage II or III Gastric Cancer. J Clin Oncol (2011) 29(33):4387–93. doi: 10.1200/JCO.2011.36.5908
86. Miyashiro I, Furukawa H, Sasako M, Yamamoto S, Nashimoto A, Nakajima T, et al. Randomized Clinical Trial of Adjuvant Chemotherapy With Intraperitoneal and Intravenous Cisplatin Followed by Oral Fluorouracil (UFT) in Serosa-Positive Gastric Cancer Versus Curative Resection Alone: Final Results of the Japan Clinical Oncology Group Trial JCOG9206-2. Gastric Cancer (2011) 14(3):212–8. doi: 10.1007/s10120-011-0027-3
87. Cao J, Qi F, Liu T. Adjuvant Chemotherapy After Curative Resection for Gastric Cancer: A Meta-Analysis. Scand J Gastroenterol (2014) 49(6):690–704. doi: 10.3109/00365521.2014.907337
88. Yoshida K, Kodera Y, Kochi M, Ichikawa W, Kakeji Y, Sano T, et al. Addition of Docetaxel to Oral Fluoropyrimidine Improves Efficacy in Patients With Stage III Gastric Cancer: Interim Analysis of JACCRO GC-07, a Randomized Controlled Trial. J Clin Oncol (2019) 37(15):1296–304. doi: 10.1200/JCO.18.01138
Keywords: gastric cancer, radical resection, peritoneal recurrence, risk assessment, preventive treatment
Citation: Xiang L, Jin S, Zheng P, Maswikiti EP, Yu Y, Gao L, Zhang J, Zhang Y and Chen H (2022) Risk Assessment and Preventive Treatment for Peritoneal Recurrence Following Radical Resection for Gastric Cancer. Front. Oncol. 11:778152. doi: 10.3389/fonc.2021.778152
Received: 17 September 2021; Accepted: 29 November 2021;
Published: 03 January 2022.
Edited by:
Luigi Bonavina, University of Milan, ItalyReviewed by:
Andrea Laurenzi, University Hospital of Bologna Policlinico S. Orsola-Malpighi, ItalyCopyright © 2022 Xiang, Jin, Zheng, Maswikiti, Yu, Gao, Zhang, Zhang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Zhang, Y2hlcnJ5emp1QGFsaXl1bi5jb20=; Hao Chen, ZXJ5X2NoZW5oQGx6dS5lZHUuY24=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.