 Jiahui Huang
Jiahui Huang Yiwei Tong
Yiwei Tong Xiaosong Chen
Xiaosong Chen Kunwei Shen
Kunwei Shen- Department of General Surgery, Comprehensive Breast Health Center, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China
Purpose: With the application of “less extensive surgery” in breast cancer treatment, the pattern of locoregional recurrence (LRR) has significantly changed. This study aims to evaluate the risk and prognostic factors of LRR in a recent large breast cancer cohort.
Methods: Consecutive early breast cancer patients who received surgery from January 2009 to March 2018 in Shanghai Ruijin Hospital were retrospectively analyzed. LRR was defined as recurrence at the ipsilateral breast (IBTR), chest wall, or regional lymph nodes and without concurrent distant metastasis (DM). Patients’ characteristics and survival were compared among these groups.
Results: Among 5,202 patients included, 87 (1.7%) and 265 (5.1%) experienced LRR and DM as first event after a median 47.0 (3.0–122.5) months’ follow-up. LRR was significantly associated with large tumor size and positive lymph node status (p < 0.05). Forty (46.0%) patients received further salvage surgery after LRR and had a significantly better 3-year post-recurrence overall survival than those who did not (94.7% vs. 60.7%, p = 0.012). Multivariate analysis showed that salvage surgery for LRR was independently associated with better survival (HR = 0.12, 95% CI 0.02–0.93, p = 0.043) along with estrogen receptor (ER) positivity (HR = 0.33, 95% CI 0.12–0.91, p = 0.033).
Conclusion: LRR rate was relatively low in recent era of breast cancer treatment. Tumor size and lymph node status were associated with risk of LRR, and salvage surgery for selected LRR patients achieved an excellent outcome.
Introduction
Breast cancer is the most commonly diagnosed cancer and the leading cause of cancer mortality in females worldwide (1). With a better understanding of tumor biologic behavior, innovations in screening techniques, and the development of comprehensive multidisciplinary treatment strategies, more breast cancers can be diagnosed at early stages. Less extensive surgery, for instance, breast-conserving surgery (BCS) followed by radiotherapy and sentinel lymph node biopsy (SLNB) in selected patients demonstrated equivalence with mastectomy and axillary lymph node dissection (ALND) in terms of survival but with less comorbidities (2, 3).
Locoregional recurrence (LRR) is a clinically relevant, predominant pattern of treatment failure in breast cancer. LRR patterns vary across initial surgical approach and mainly involve recurrence in chest wall post-mastectomy, residual breast after BCS, or regional lymph nodes (LNs). According to previous evidence, factors associated with increased risk of LRR include young age at diagnosis, greater tumor size, involvement of regional LN, high histological grade, triple negative (TN) or human epidermal growth factor receptor 2 (HER2)-positive subtype, lack of endocrine therapy, and omitting indicated adjuvant radiotherapy (4–6). Different from the palliative management of distant metastasis (DM), salvage surgery plays an important role in the comprehensive management of LRR. Patients who received salvage surgery for LRR reported relatively satisfactory 5-year overall survival (OS) ranging from 40.8% to 90.9% (7, 8), suggesting that selective LRR patients would benefit from salvage surgery and quite a number of LRR patients could be cured. However, retrospective series showed that between 15% and 37% patients with LRR had concurrent DM at the time of presentation (9–18). Disease outcomes and treatment strategies of these populations can be very different from those with LRR alone. The management of LRR should be based on systemic evaluation and be discussed in a multidisciplinary setting.
However, studies of LRR were mostly conducted in the late 1990s to early 2000s and in western populations. Following the change of initial surgical procedures from “maximal tolerable treatment” to “minimal effective treatment,” the pattern of LRR has also significantly changed. With an increasing rate of BCS and SLNB, now we meet more patients with ipsilateral breast tumor recurrence (IBTR) and regional LN recurrence in clinical practice. To this end, the objective of this study was to analyze the risk and prognostic factors of LRR in the current “less extensive surgery” era.
Patients and Methods
Patients
We retrospectively included consecutive female patients diagnosed with primary invasive breast cancer and received radical surgical treatment from January 2009 to March 2018 in Comprehensive Breast Health Center, Shanghai Ruijin Hospital. Patients with complete clinicopathological information, with at least 3 months of follow-up, were included in this study. Patient with de novo stage IV disease, with bilateral breast cancer, receiving neoadjuvant therapy for breast cancer, or with previous malignancy history were excluded from this study (Supplementary Figure 1). Patient baseline clinical characteristics were extracted from Shanghai Jiaotong University Breast Cancer Database (SJTU-BCDB).
Pathological Assessment
Histopathological assessment and immunohistochemical (IHC) evaluation were conducted in the Department of Pathology, Ruijin Hospital, by at least two independent experienced pathologists. Estrogen receptor (ER) positivity and progesterone receptor (PR) positivity were defined as 1% or more positive invasive tumor cells with nuclear staining (19). HER2 status was first determined by IHC staining and scored as 0, 1+, 2+, and 3+ according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guideline (20). Samples with HER2 IHC 2+ were further examined by fluorescence in situ hybridization (FISH). HER2 positivity was defined as HER2 IHC 3+ or FISH positive. Five breast cancer molecular subtypes were classified according to the 2013 St. Gallen breast cancer consensus (21): Luminal A (ER+/HER2–, Ki67 < 14%, and PR ≥ 20%), Luminal B HER2− (ER+/HER2−, Ki67 ≥ 14%, or ER+/HER2−, PR < 20%, or ER−/PR+/HER2−), Luminal B HER2+ (ER or PR+/HER2+), TN (ER−/PR−/HER2–), and HER2 enriched (ER−/PR−/HER2+).
Follow-Up and Disease Outcomes
Follow-up was accomplished annually by specialized breast cancer nurses in our center through outpatient medical history and/or phone calls. Recurrences in ipsilateral breast, chest wall, or regional LN (ipsilateral axillary, infra- and/or supraclavicular, or internal mammary LN) were considered LRR. DM included metastases to distant LN, bone, brain, liver, lung (including pleura and lymphangitic carcinomatosis), or others (including peritoneal, other organs not elsewhere classified, and skin not in the breast and chest wall). Patients with concurrent LRR and DM were categorized as DM as first recurrence event.
Recurrence-free interval (RFI) was defined as time from the date of breast cancer surgery to the date of first recurrence event. OS was defined as time from the date of breast cancer surgery to the date of death from any cause. Post-recurrence OS (PR-OS) was defined as the time from the date of first recurrence diagnosis to the time of death from any cause.
Statistical Analysis
Patients were categorized into three groups according to their recurrence status, i.e., recurrence-free, LRR, and DM groups. Descriptive characteristics of categorical variables were tested using chi-squared test or Fisher’s exact test. Binary or multinomial logistic regression analysis was conducted to compare baseline clinicopathological features and adjuvant therapy among groups. Survival curves were plotted using the Kaplan–Meier method and compared between groups by log-rank test. Multivariate Cox proportional-hazards regression analyses were performed to calculate hazard ratios (HRs) and 95% confidence interval (CI) for recurrence and survival. All analyses were performed using IBM SPSS 22.0 (IBM Inc., Armonk, USA). All reported p-values were two-sided, and p < 0.05 was considered statistically significant.
Results
Patient Baseline Characteristics
A total of 5,202 women were included in this study. The median age was 55 (range: 22–93) years. Patients’ baseline clinicopathological characteristics at initial diagnosis and treatment for primary breast cancer were summarized in Table 1. Four thousand four hundred fifty-four (85.6%) patients had invasive ductal carcinoma, and 1,723 (33.1%) had node-positive disease. ER positivity were identified in 3,769 (72.5%) patients, and 1,181 (22.7%) had HER2-positive disease. With regard to local and systemic treatment, BCS was performed in 1,597 (30.7%) patients, while others received mastectomy as initial surgery for breast cancer. Two thousand five hundred sixty-three (49.3%) patients received SLNB, 2,598 (49.9%) patients received ALND, and the remaining 41 (0.8%) patients did not receive surgery for the axilla. Adjuvant radiotherapy was performed in 2,539 patients, including 86.4% of patients who underwent BCS and in 32.1% of patients who received mastectomy.
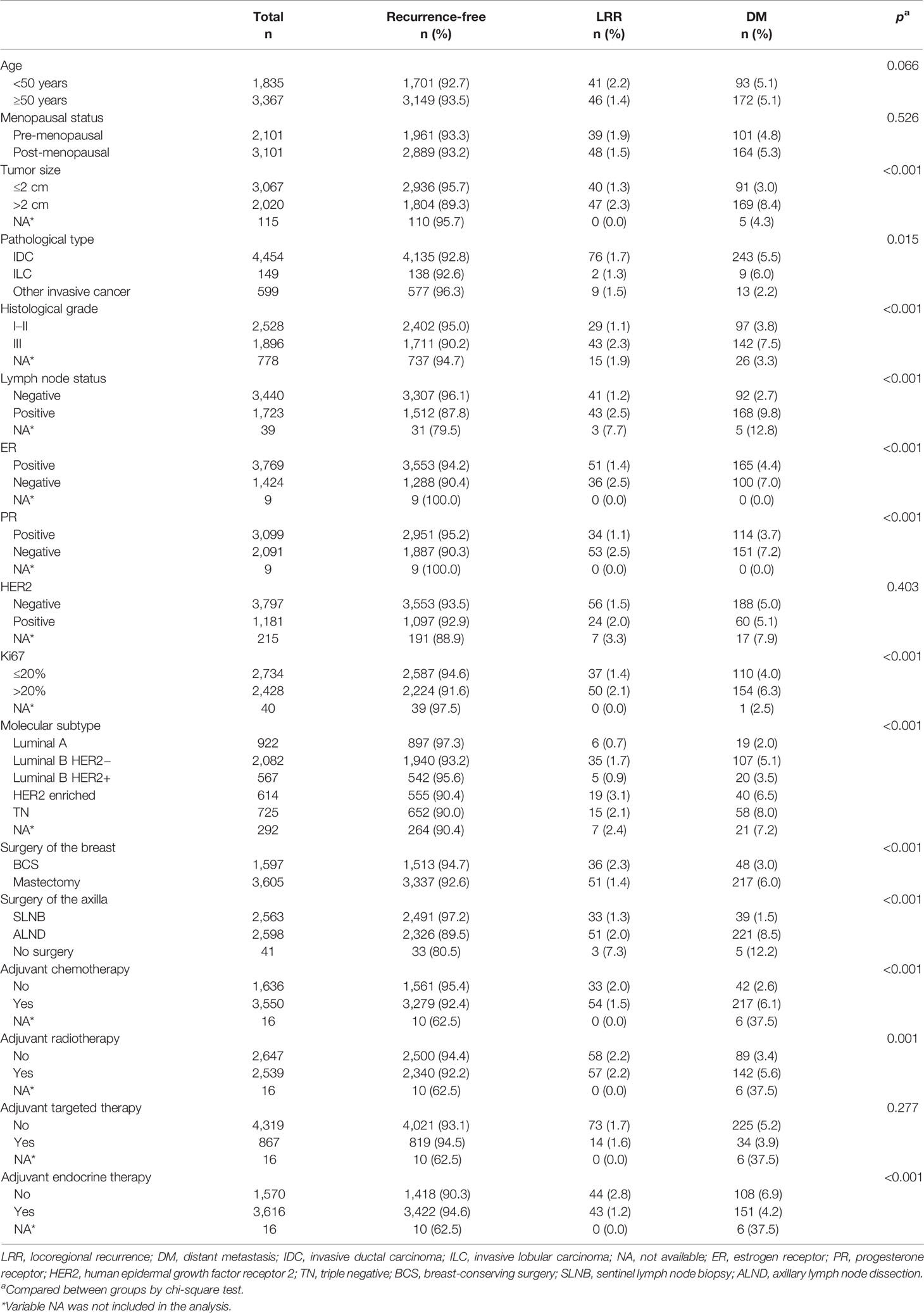
Table 1 Clinicopathological characteristics at initial diagnosis and treatment for primary breast cancer by different first recurrence events.
Patient Characteristics Associated With First Recurrence Event
After a median follow-up of 47.0 (range: 3.0–122.5) months, 352 (6.8%) patients experienced breast cancer recurrence, including 87 (1.7%) LRR and 265 (5.1%) DM as first recurrence event. The 5-year estimated LRR rate was 2.2% in the whole population: 3.3% in patients receiving BCS and 1.7% in patients receiving mastectomy. Tumor size, pathological type, histological grade, LN status, ER status, PR status, Ki67 level, molecular subtype, surgery of the breast, surgery of the axilla, adjuvant chemotherapy, adjuvant radiotherapy, and adjuvant endocrine therapy were differently distributed among patients with no recurrence, LRR, and DM in the univariate model (all p < 0.05; Table 1), while no difference was observed in age, menopausal status, HER2 status, or adjuvant targeted therapy among three groups (p > 0.05).
Multivariate analysis demonstrated that tumor size (p < 0.001; Table 2), histological grade (p < 0.001), lymph node status (p < 0.001), molecular subtype (p = 0.005), surgery of the breast (p < 0.001), surgery of the axilla (p < 0.001), and adjuvant chemotherapy (p = 0.013) were independently associated with first recurrence events. Comparison between patients with LRR and recurrence-free showed that tumor size >2.0 cm (OR = 2.13, 95% CI 1.31–3.48, p = 0.002), positive LNs (OR = 3.24, 95% CI 1.75–6.02, p < 0.001), primary BCS (OR = 3.04, 95% CI 1.73–5.33, p < 0.001), not receiving adjuvant chemotherapy (OR = 2.48, 95% CI 1.37–4.50, p = 0.003), and not receiving adjuvant radiotherapy (OR = 1.91, 95% CI 1.07–3.42, p = 0.030) were independent risk factors for LRR. Regarding patients with DM as first recurrence event, LRR patients had higher rates of BCS (OR = 3.86, 95% CI 1.96–7.58, p < 0.001), SLNB (OR = 2.80, 95% CI 1.37–5.75, p = 0.005), not receiving adjuvant chemotherapy (OR = 2.81, 95% CI 1.37–5.75, p = 0.013), and not receiving adjuvant radiotherapy (OR = 2.52, 95% CI 1.21–5.20, p = 0.042).
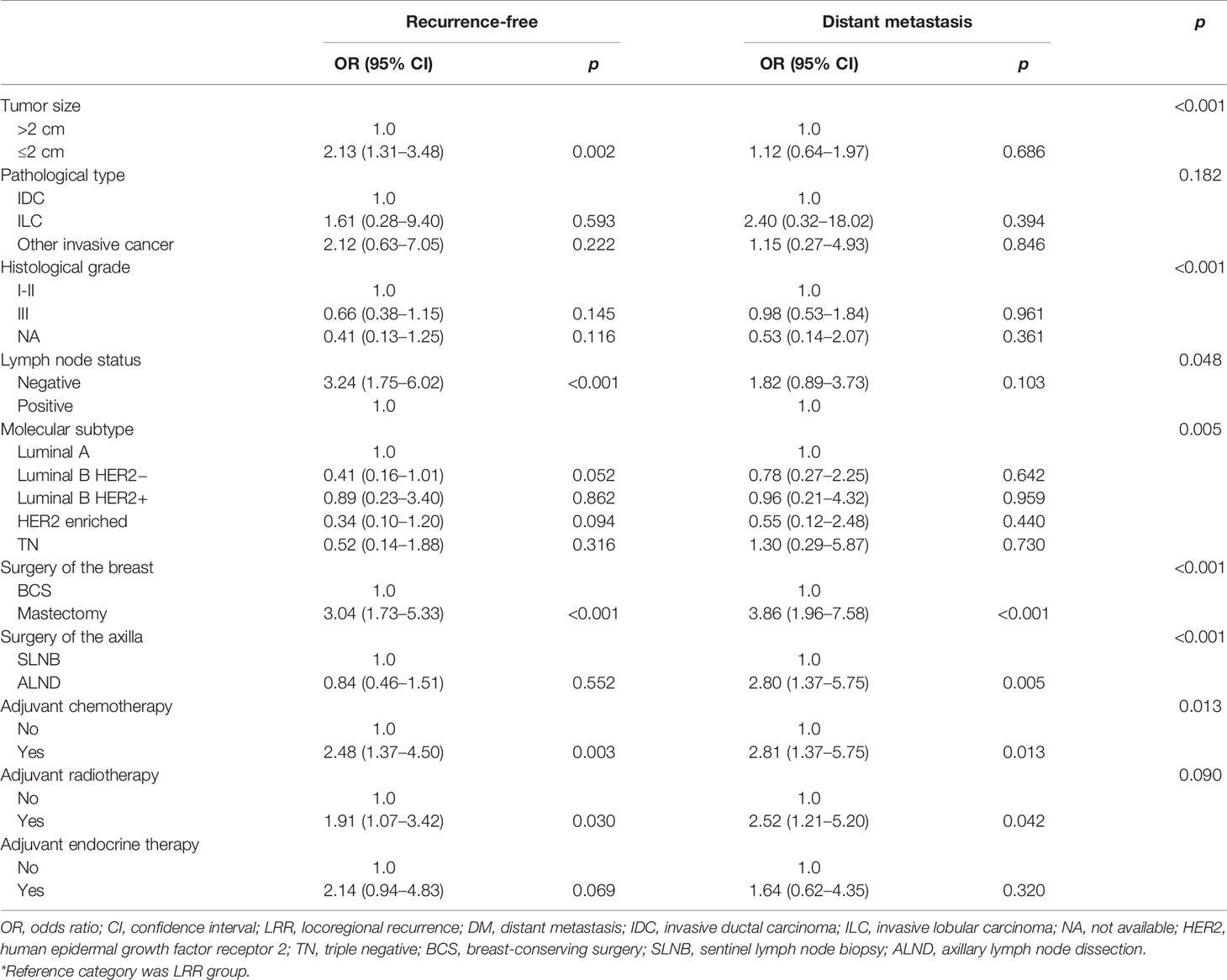
Table 2 Multivariate logistic regression of predictors for disease recurrence type*.
Factors Influencing Salvage Surgery for Locoregional Recurrence Patients
Forty out of 87 (46.0%) LRR patients received further salvage surgery. Table 3 summarizes the clinicopathological features associated with the reception of salvage surgery in LRR patients. Age at recurrence, primary tumor size, primary lymph node status, primary surgery of the breast and axilla, and LRR type significantly influenced the choice of surgery for LRR (p < 0.05; Table 3). Patients with IBTR received more salvage surgery as compared with LRR patients with chest wall recurrence or reginal LN recurrence (p < 0.001). Twenty-one out of 26 (80.8%) patients with IBTR received salvage surgery, all of whom received mastectomy with or without ALND. Only five patients with isolated IBTR did not receive surgery for LRR, including two patients refusing further treatment, two treated with endocrine therapy but not surgery due to advanced age, and one participating in a clinical trial of a new drug. Twelve out of 27 (44.4%) patients with chest wall recurrence received extended tumor excision, while seven out of 34 (20.6%) patients with regional LN recurrence received LN dissection surgery. Among 27 patients who did not receive surgery for regional LN recurrence, nine, 17, and one patients were with ALN recurrence, supraclavicular/infraclavicular LN recurrence, and internal mammary LN recurrence.
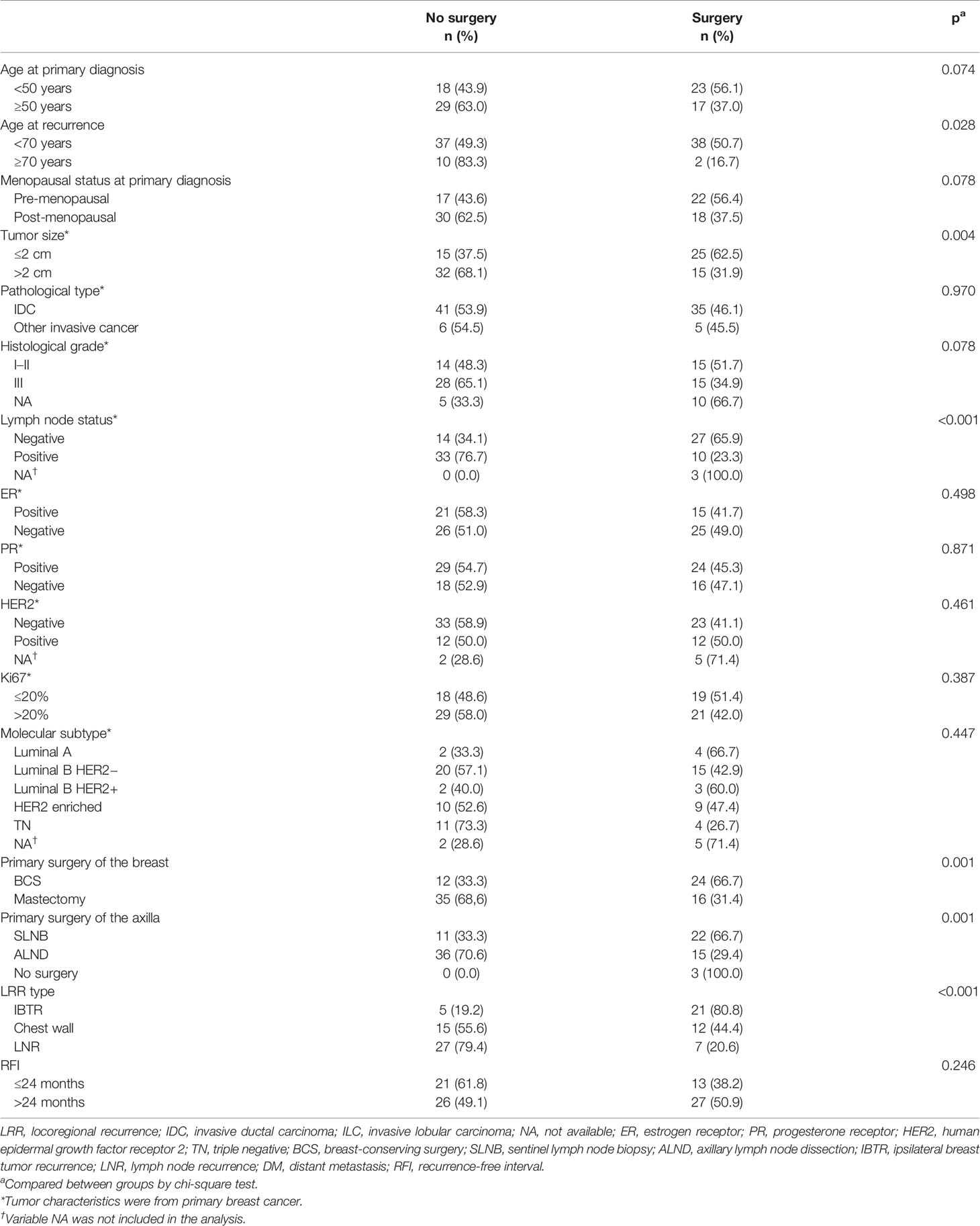
Table 3 Univariate analysis for clinicopathological features related to salvage surgery decision for LRR patients.
Multivariate analysis showed that primary tumor size (p = 0.039), primary surgery of the axilla (p = 0.006), and LRR type (p < 0.001) were factors that independently influenced the choice of surgery for LRR (Table 4). Patients with smaller primary tumor size, primary SLNB, and IBTR had significantly higher probability to receive surgical treatment for LRR. Patients with regional LN recurrence were less likely to receive surgery for LRR than were patients with IBTR only (OR = 0.07, 95% CI 0.02–0.30, p < 0.001), while the probability of surgery for LRR was comparable between patients with chest wall recurrence and IBTR (OR = 0.36, 95% CI 0.09–1.47, p = 0.155).
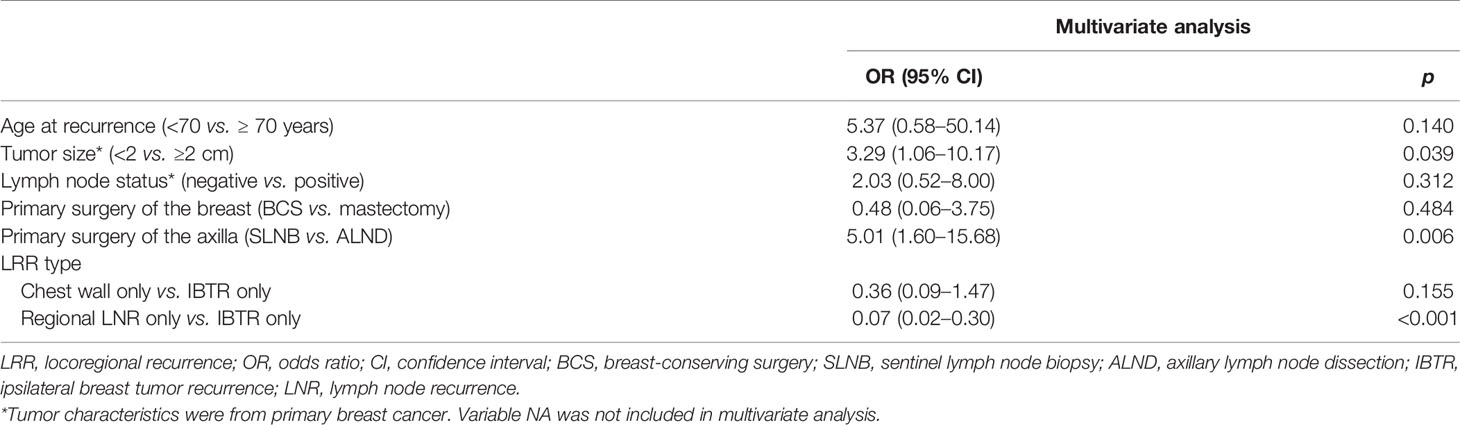
Table 4 Multivariate analysis for clinicopathological features related to salvage surgery decision for LRR patients.
Survival Outcome With Different Recurrence Events
The estimated 5-year OS was 80.7%, 50.3%, and 98.8% for patients with LRR, patients with DM, and recurrence-free patients, respectively (p < 0.001, Figure 1). Among the 87 patients with LRR, 26, 27, and 34 patients had IBTR, chest wall recurrence, and LN recurrence, respectively. During a median post-recurrence follow-up time of 21.3 (range: 1.0–77.5) months, 30 deaths were recorded. PR-OS curve is shown in Figure 2A. Patients with LRR as first event had a significantly better PR-OS than those with DM (3-year PR-OS 75.0% vs. 37.1%; p < 0.001, Figure 2A).
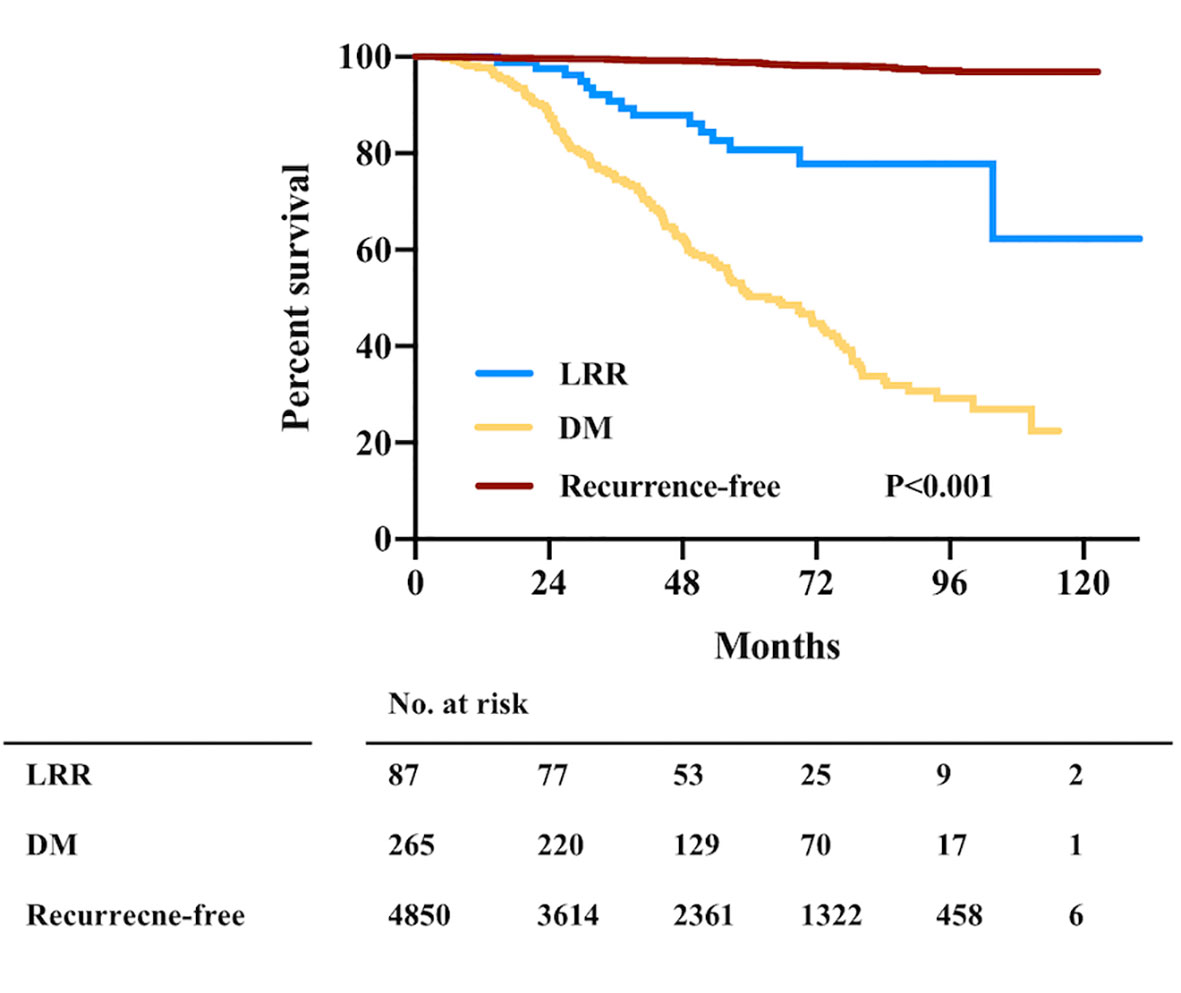
Figure 1 Overall survival by first recurrence event in the whole population. LRR, locoregional recurrence; DM, distant metastasis; No., number.
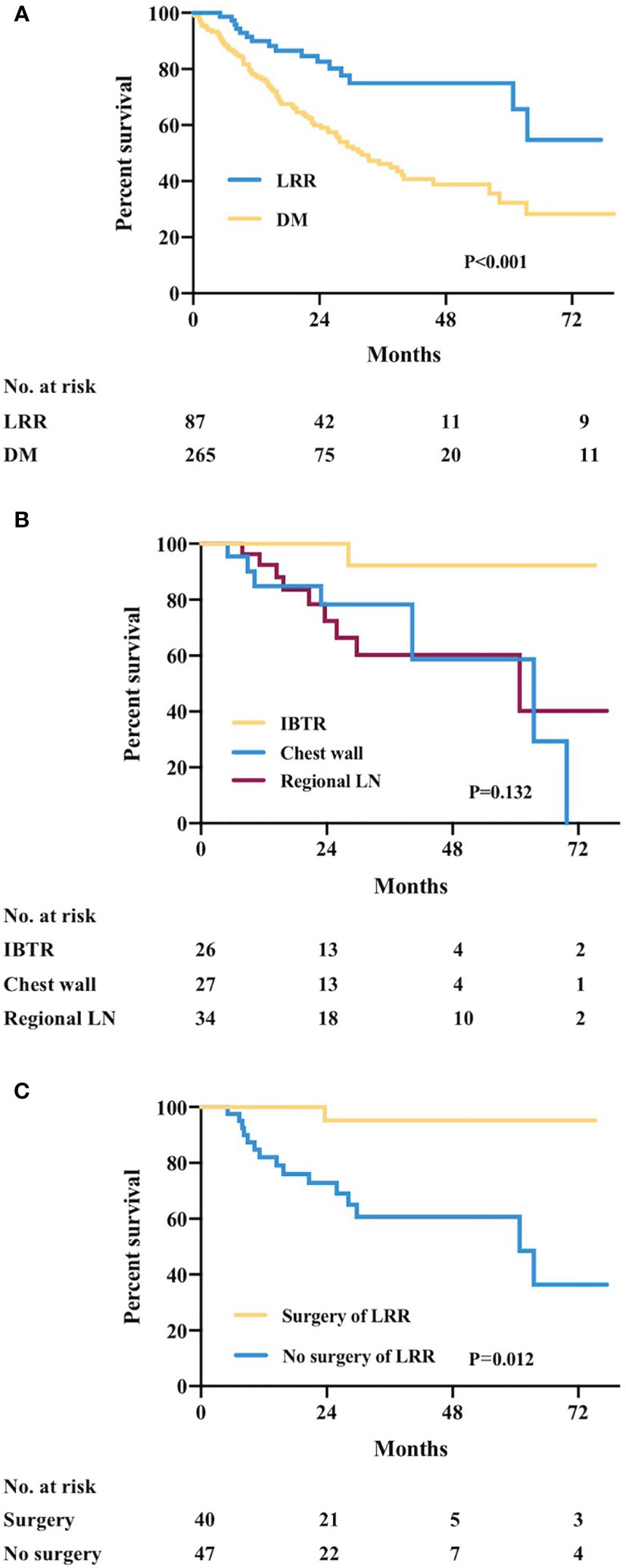
Figure 2 Post-recurrence overall survival (PR-OS) by recurrence type. (A) PR-OS in recurrent patients by first recurrence event. (B) PR-OS in LRR patients by LRR type. (C) PR-OS in LRR patients receiving or not salvage surgery for LRR. LRR, locoregional recurrence; DM, distant metastasis; No., number; IBTR, ipsilateral breast tumor recurrence; LN, lymph node.
Univariate analysis showed that primary tumor size (p = 0.033; Supplementary Table 1), primary ER status (p = 0.033), primary surgery of the axilla (p = 0.034), LRR type (regional LN vs. IBTR only, p = 0.045), and surgery of LRR (p = 0.012) were factors associated with PR-OS. The estimated 3-year PR-OS was 90.9%, 77.3%, and 60.3% in patients with recurrence type of IBTR, chest wall, and regional LN, respectively (p = 0.132, Figure 2B). The estimated 3-year PR-OS was 94.7% in patients receiving surgery after LRR, which was significantly higher than that not receiving surgery (60.7%, p = 0.012, Figure 2C). In multivariate analysis, ER positivity (HR = 0.33, 95% CI 0.12–0.91, p = 0.033) and salvage surgery of LRR (HR = 0.11, 95% CI 0.02–0.93, p = 0.043) were independently associated with better PR-OS for LRR patients (Table 5).
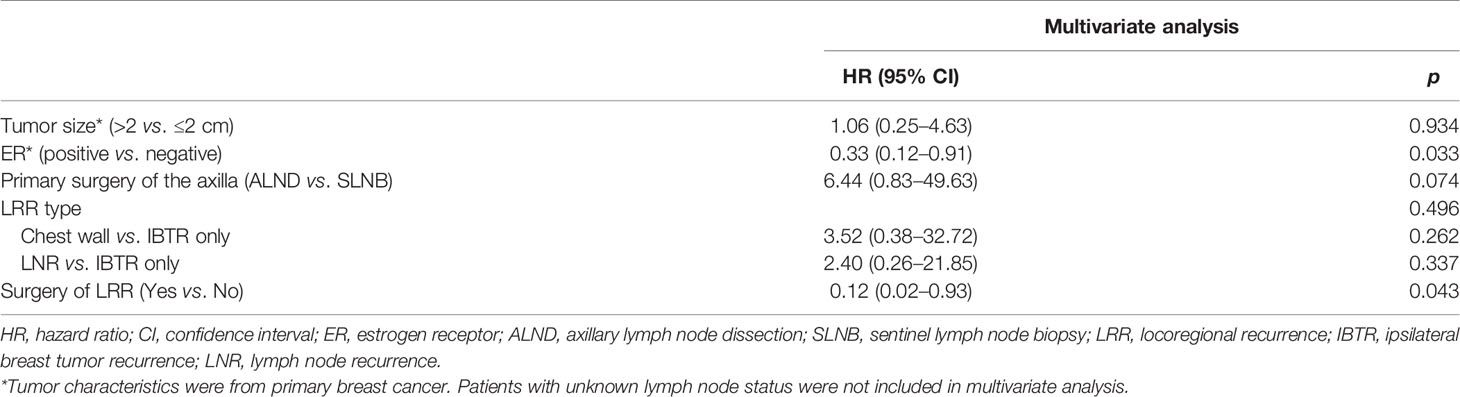
Table 5 Multivariate analysis of factors associated with post-recurrence overall survival in patients with locoregional recurrence.
Discussion
In this cohort of 5,202 consecutive breast cancer patients, we showed that LRR after radical surgery in the modern era is relatively low. Clinicopathological factors, including large tumor size, positive lymph node status, and molecular subtype, were significantly associated with increased risk of LRR. Primary surgical treatment for breast or adjuvant chemotherapy or radiotherapy also influenced the risk of LRR. Moreover, LRR patients had higher rates of receiving BCS or SLNB and not receiving adjuvant chemotherapy or radiotherapy compared with DM patients. Furthermore, we found that LRR types were related with salvage surgery choice after LRR. For patients receiving surgery after LRR, they could achieve an excellent outcome after recurrence.
According to the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) overview, which included trials up to year 2000 evaluating the effects of radiotherapy, the 5-year LRR rate was 7% in patients after BCS and radiotherapy and 6% in patients after mastectomy (22). A reduction of LRR has been seen in the recent years with the improvement in imaging, earlier diagnosis, surgical planning, and adjuvant therapy for breast cancer patients (5). In our study, the 5-year LRR rate was 2.8% in the whole population: 3.8% in patients receiving BCS and 2.5% in patients receiving mastectomy, which were quite low compared with the established evidence. The low LRR rate highlights the effect of multiple changes in breast cancer management over the past two decades.
Several clinicopathological factors as well as treatment patterns were associated with LRR after surgery in early breast cancer patients. Not surprisingly, in our study, we found that large tumor size, positive LN status, and primary BCS were identified as independent risk factors for LRR, which was consistent with previous studies (23, 24). Meanwhile, adjuvant chemotherapy and radiotherapy can effectively reduce the risk of LRR. Neoadjuvant chemotherapy was one of risk factors for local recurrence as reported by the EBCTCG meta-analysis (25), but neoadjuvant population was not included in our study. There was controversy in grouping patients when analyzing the two populations together, since there is discordance of molecular biomarkers before and after neoadjuvant therapy, and the staging of patients will change after neoadjuvant therapy. Also, in neoadjuvant study, we usually use event-free survival to evaluate patients’ outcome, which includes more information than recurrence-free interval that we evaluated in adjuvant studies. By reason of the foregoing, we excluded patients who received neoadjuvant therapy in this study, to make the evaluation standardized in the whole study population.
We also found that LRR was a less common recurrence event, as either first recurrence event or subsequent recurrence event comparing with DM. Few studies directly compared the difference between patients with different first recurrence events. Our study demonstrated that LRR patients had higher rate of receiving primary BCS, primary SLNB, and lower rate of receiving adjuvant chemotherapy or radiotherapy, indicating that more effective systemic and local treatment should be evaluated to further reduce the rate of LRR.
In the modern era of breast cancer treatment, management of LRR breast cancer patients remained a big challenge due to lower LRR events, fewer high quality clinical evidence, and relatively hard to follow-up patients. For patients who developed IBTR after BCS, the current standard of care is further salvage surgery, including salvage mastectomy or repeat BCS (26), which can achieve 59% to 90.9% 5-year OS after salvage surgery (11, 27–30). There is also another special consideration for patients with IBTR that whether it is “true recurrence” or “new primary,” since new primaries should theoretically have a prognosis independent of the primary breast cancer. The rate of new primary breast cancer in patients with IBTR was 18%–58.9% in published studies (31–34), also strengthening the reason for surgery of IBTR. For patients with isolated chest wall recurrence, full-thickness chest wall resection can be performed with excellent survival and low morbidity. In a recent systematic meta-analysis of 48 studies accounting for 1,305 patients who received full-thickness resection for chest wall recurrence, the mortality was consistently low (<1%), and 5-year OS was 40.8% (8). Axillary recurrence rates are rare, ranging of 1% to 3% after adequate management of primary disease (35, 36). Salvage ALND was the first choice for selected patients and can be performed in 45.5% to 69.5% patients (37, 38). Surgery of LRR might be encouraged in patients who can achieve R0 resection. In our study, salvage surgery was performed in 46.0% of LRR patients: 80.8% for IBTR, 44.4% for chest wall recurrence, and 20.6% for regional LN recurrence. Patients with smaller primary tumor, receiving primary SLNB, and LRR type were related with the choice of surgery after LRR. Although the post-LRR follow-up period is short, and there was selective bias in patients receiving salvage surgery, we do observe that patients receiving surgery for LRR achieved a better PR-OS, which emphasized the importance of surgery as part of multidisciplinary management of LRR patients.
Some limitations of this study exist. The data were collected retrospectively, which may have led to selection bias. The follow-up time is relatively short, and only a small number of LRR events were recorded, given that LRR was less common in clinical practice. The actual site of recurrence may influence the possibility of surgery for LRR lesions and were not analyzed in this study. Details of the recurrence including site and pathologic features of the recurrent lesion are not completely collected, and we cannot distinguish whether there is true recurrence or new primary breast cancer in patients with IBTR. Treatments of LRR out of surgery such as systemic therapy or radiotherapy and their impact on survival were not recorded or analyzed in this study. More comprehensive treatment data as well as longer follow-up are warranted to find the best management for LRR patients.
Conclusion
LRR rate was relatively low in the modern era of breast cancer treatment cohort. Large tumor size, positive lymph node status, and treatment strategies were associated with LRR. Moreover, LRR patients had a higher rate of receiving primary BCS or SLNB, and not receiving adjuvant chemotherapy or radiotherapy compared with DM patients. LRR patients treated with salvage surgery experienced excellent survival, indicating salvage surgery should play an important role in multidisciplinary treatment of LRR patients.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical Committees of Ruijin Hospital, Shanghai Jiaotong University School of Medicine. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This study was funded by the National Natural Science Foundation of China (81772797, 82072937); Shanghai Municipal Education Commission—Gaofeng Clinical Medicine Grant Support (20172007); Shanghai Jiao Tong University Yi Gong Jiao Cha Funding (YG2019QNA30); and Ruijin Hospital, Shanghai Jiao Tong University School of Medicine—”Guangci Excellent Youth Training Program” (GCQN-2019-B07). All these financial sponsors had no role in the study design, data collection, analysis, or interpretation.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Ms. Yidong Du for her assistance in inputting SJTU-BCDB.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.763119/full#supplementary-material
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-Year Follow-Up of a Randomized Trial Comparing Total Mastectomy, Lumpectomy, and Lumpectomy Plus Irradiation for the Treatment of Invasive Breast Cancer. N Engl J Med (2002) 347(16):1233–41. doi: 10.1056/NEJMoa022152
3. Rao R, Euhus D, Mayo HG, Balch C. Axillary Node Interventions in Breast Cancer: A Systematic Review. JAMA (2013) 310(13):1385–94. doi: 10.1001/jama.2013.277804
4. Wallgren A, Bonetti M, Gelber RD, Goldhirsch A, Castiglione-Gertsch M, Holmberg SB, et al. Risk Factors for Locoregional Recurrence Among Breast Cancer Patients: Results From International Breast Cancer Study Group Trials I Through VII. J Clin Oncol (2003) 21(7):1205–13. doi: 10.1200/JCO.2003.03.130
5. McGuire A, Lowery AJ, Kell MR, Kerin MJ, Sweeney KJ. Locoregional Recurrence Following Breast Cancer Surgery in the Trastuzumab Era: A Systematic Review by Subtype. Ann Surg Oncol (2017) 24(11):3124–32. doi: 10.1245/s10434-017-6021-1
6. Holleczek B, Stegmaier C, Radosa JC, Solomayer EF, Brenner H. Risk of Loco-Regional Recurrence and Distant Metastases of Patients With Invasive Breast Cancer Up to Ten Years After Diagnosis - Results From a Registry-Based Study From Germany. BMC Cancer (2019) 19(1):520. doi: 10.1186/s12885-019-5710-5
7. Wadasadawala T, Vadgaonkar R, Bajpai J. Management of Isolated Locoregional Recurrences in Breast Cancer: A Review of Local and Systemic Modalities. Clin Breast Cancer (2017) 17(7):493–502. doi: 10.1016/j.clbc.2017.03.008
8. Wakeam E, Acuna SA, Keshavjee S. Chest Wall Resection for Recurrent Breast Cancer in the Modern Era: A Systematic Review and Meta-Analysis. Ann Surg (2018) 267(4):646–55. doi: 10.1097/SLA.0000000000002310
9. Schmoor C, Sauerbrei W, Bastert G, Schumacher M. Role of Isolated Locoregional Recurrence of Breast Cancer: Results of Four Prospective Studies. J Clin Oncol (2000) 18(8):1696–708. doi: 10.1200/JCO.2000.18.8.1696
10. Buchanan CL, Dorn PL, Fey J, Giron G, Naik A, Mendez J, et al. Locoregional Recurrence After Mastectomy: Incidence and Outcomes. J Am Coll Surg (2006) 203(4):469–74. doi: 10.1016/j.jamcollsurg.2006.06.015
11. Haffty BG, Fischer D, Beinfield M, McKhann C. Prognosis Following Local Recurrence in the Conservatively Treated Breast Cancer Patient. Int J Radiat Oncol Biol Phys (1991) 21(2):293–8. doi: 10.1016/0360-3016(91)90774-X
12. Harris EE, Hwang WT, Seyednejad F, Solin LJ. Prognosis After Regional Lymph Node Recurrence in Patients With Stage I-II Breast Carcinoma Treated With Breast Conservation Therapy. Cancer (2003) 98(10):2144–51. doi: 10.1002/cncr.11767
13. Tennant S, Evans A, Macmillan D, Lee A, Cornford E, James J, et al. CT Staging of Loco-Regional Breast Cancer Recurrence. A Worthwhile Practice? Clin Radiol (2009) 64(9):885–90. doi: 10.1016/j.crad.2009.05.006
14. Touboul E, Buffat L, Belkacemi Y, Lefranc JP, Uzan S, Lhuillier P, et al. Local Recurrences and Distant Metastases After Breast-Conserving Surgery and Radiation Therapy for Early Breast Cancer. Int J Radiat Oncol Biol Phys (1999) 43(1):25–38. doi: 10.1016/s0360-3016(98)00365-4
15. van Oost FJ, van der Hoeven JJ, Hoekstra OS, Voogd AC, Coebergh JW, van de Poll-Franse LV. Staging in Patients With Locoregionally Recurrent Breast Cancer: Current Practice and Prospects for Positron Emission Tomography. Eur J Cancer (2004) 40(10):1545–53. doi: 10.1016/j.ejca.2004.03.012
16. Yi M, Kronowitz SJ, Meric-Bernstam F, Feig BW, Symmans WF, Lucci A, et al. Local, Regional, and Systemic Recurrence Rates in Patients Undergoing Skin-Sparing Mastectomy Compared With Conventional Mastectomy. Cancer (2011) 117(5):916–24. doi: 10.1002/cncr.25505
17. Neuman HB, Schumacher JR, Francescatti AB, Adesoye T, Edge SB, Vanness DJ, et al. Risk of Synchronous Distant Recurrence at Time of Locoregional Recurrence in Patients With Stage II and III Breast Cancer (AFT-01). J Clin Oncol (2018) 36(10):975–80. doi: 10.1200/JCO.2017.75.5389
18. Elfgen C, Schmid SM, Tausch CJ, Montagna G, Guth U. Radiological Staging for Distant Metastases in Breast Cancer Patients With Confirmed Local and/or Locoregional Recurrence: How Useful are Current Guideline Recommendations? Ann Surg Oncol (2019) 26(11):3455–61. doi: 10.1245/s10434-019-07629-9
19. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College Of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. J Clin Oncol (2010) 28(16):2784–95. doi: 10.1200/JCO.2009.25.6529
20. Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J Clin Oncol (2013) 31(31):3997–4013. doi: 10.1200/JCO.2013.50.9984
21. Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thurlimann B, et al. Personalizing the Treatment of Women With Early Breast Cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol Off J Eur Soc Med Oncol (2013) 24(9):2206–23. doi: 10.1093/annonc/mdt303
22. Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, et al. Effects of Radiotherapy and of Differences in the Extent of Surgery for Early Breast Cancer on Local Recurrence and 15-Year Survival: An Overview of the Randomised Trials. Lancet (2005) 366(9503):2087–106. doi: 10.1016/S0140-6736(05)67887-7
23. Harahap WA, Nindrea RD. Prognostic Factors of Local-Regional Recurrence in Patients With Operable Breast Cancer in Asia: A Meta-Analysis. Open Access Maced J Med Sci (2019) 7(4):690–5. doi: 10.3889/oamjms.2019.151
24. Houvenaeghel G, de Nonneville A, Cohen M, Classe JM, Reyal F, Mazouni C, et al. Isolated Ipsilateral Local Recurrence of Breast Cancer: Predictive Factors and Prognostic Impact. Breast Cancer Res Treat (2019) 173(1):111–22. doi: 10.1007/s10549-018-4944-2
25. Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Long-Term Outcomes for Neoadjuvant Versus Adjuvant Chemotherapy in Early Breast Cancer: Meta-Analysis of Individual Patient Data From Ten Randomised Trials. Lancet Oncol (2018) 19(1):27–39. doi: 10.1016/S1470-2045(17)30777-5
26. Mahvi DA, Liu R, Grinstaff MW, Colson YL, Raut CP. Local Cancer Recurrence: The Realities, Challenges, and Opportunities for New Therapies. CA Cancer J Clin (2018) 68(6):488–505. doi: 10.3322/caac.21498
27. Doyle T, Schultz DJ, Peters C, Harris E, Solin LJ. Long-Term Results of Local Recurrence After Breast Conservation Treatment for Invasive Breast Cancer. Int J Radiat Oncol Biol Phys (2001) 51(1):74–80. doi: 10.1016/S0360-3016(01)01625-X
28. Galper S, Blood E, Gelman R, Abner A, Recht A, Kohli A, et al. Prognosis After Local Recurrence After Conservative Surgery and Radiation for Early-Stage Breast Cancer. Int J Radiat Oncol Biol Phys (2005) 61(2):348–57. doi: 10.1016/j.ijrobp.2004.06.011
29. Voogd AC, van Oost FJ, Rutgers EJ, Elkhuizen PH, van Geel AN, Scheijmans LJ, et al. Long-Term Prognosis of Patients With Local Recurrence After Conservative Surgery and Radiotherapy for Early Breast Cancer. Eur J Cancer (2005) 41(17):2637–44. doi: 10.1016/j.ejca.2005.04.040
30. Abner AL, Recht A, Eberlein T, Come S, Shulman L, Hayes D, et al. Prognosis Following Salvage Mastectomy for Recurrence in the Breast After Conservative Surgery and Radiation Therapy for Early-Stage Breast Cancer. J Clin Oncol (1993) 11(1):44–8. doi: 10.1200/JCO.1993.11.1.44
31. Veronesi U, Marubini E, Del Vecchio M, Manzari A, Andreola S, Greco M, et al. Local Recurrences and Distant Metastases After Conservative Breast Cancer Treatments: Partly Independent Events. J Natl Cancer Inst (1995) 87(1):19–27. doi: 10.1093/jnci/87.1.19
32. Smith TE, Lee D, Turner BC, Carter D, Haffty BG. True Recurrence vs. New Primary Ipsilateral Breast Tumor Relapse: An Analysis of Clinical and Pathologic Differences and Their Implications in Natural History, Prognoses, and Therapeutic Management. Int J Radiat Oncol Biol Phys (2000) 48(5):1281–9. doi: 10.1016/s0360-3016(00)01378-x
33. Alexandrova E, Sergieva S, Kostova P, Mihaylova I, Katzarov D, Milev A. Ipsilateral in-Breast Tumor Recurrence After Breast Conserving Therapy: True Recurrence Versus New Primary Tumor. J BUON (2015) 20(4):1001–8.
34. Gujral DM, Sumo G, Owen JR, Ashton A, Bliss JM, Haviland J, et al. Ipsilateral Breast Tumor Relapse: Local Recurrence Versus New Primary Tumor and the Effect of Whole-Breast Radiotherapy on the Rate of New Primaries. Int J Radiat Oncol Biol Phys (2011) 79(1):19–25. doi: 10.1016/j.ijrobp.2009.10.074
35. Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Costantino JP, et al. Sentinel-Lymph-Node Resection Compared With Conventional Axillary-Lymph-Node Dissection in Clinically Node-Negative Patients With Breast Cancer: Overall Survival Findings From the NSABP B-32 Randomised Phase 3 Trial. Lancet Oncol (2010) 11(10):927–33. doi: 10.1016/S1470-2045(10)70207-2
36. Giuliano AE, Ballman KV, McCall L, Beitsch PD, Brennan MB, Kelemen PR, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA (2017) 318(10):918–26. doi: 10.1001/jama.2017.11470
37. Newman LA, Hunt KK, Buchholz T, Kuerer HM, Vlastos G, Mirza N, et al. Presentation, Management and Outcome of Axillary Recurrence From Breast Cancer. Am J Surg (2000) 180(4):252–6. doi: 10.1016/S0002-9610(00)00456-6
Keywords: breast cancer, risk factors, surgery, survival, locoregional recurrence
Citation: Huang J, Tong Y, Chen X and Shen K (2021) Prognostic Factors and Surgery for Breast Cancer Patients With Locoregional Recurrence: An Analysis of 5,202 Consecutive Patients. Front. Oncol. 11:763119. doi: 10.3389/fonc.2021.763119
Received: 23 August 2021; Accepted: 22 September 2021;
Published: 13 October 2021.
Edited by:
Tadahiko Shien, Okayama University, JapanReviewed by:
Shinsuke Sasada, Hiroshima University, JapanSota Asaga, Kyorin University Hospital, Japan
Copyright © 2021 Huang, Tong, Chen and Shen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaosong Chen, chenxiaosong0156@hotmail.com; Kunwei Shen, kwshen@medmail.com.cn