 Karan Seegobin
Karan Seegobin Umair Majeed
Umair Majeed Nathaniel Wiest
Nathaniel Wiest Rami Manochakian
Rami Manochakian Yanyan Lou
Yanyan Lou Yujie Zhao
Yujie Zhao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 01 December 2021
Sec. Thoracic Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.750657
This article is part of the Research Topic Insights in Thoracic Oncology: 2021/2022 View all 16 articles
While first line targeted therapies are the current standard of care treatment for non-small cell lung cancer (NSCLC) with actionable mutations, the cancer cells inevitably acquire resistance to these agents over time. Immune check-point inhibitors (ICIs) have improved the outcomes of metastatic NSCLC, however, its efficacy in those with targetable drivers is largely unknown. In this manuscript, we reviewed the published data on ICI therapies in NSCLC with ALK, ROS1, BRAF, c-MET, RET, NTRK, KRAS, and HER2 (ERBB2) alterations. We found that the objective response rates (ORRs) associated with ICI treatments in lung cancers harboring the BRAF (0–54%), c-MET (12–49%), and KRAS (18.7-66.7%) alterations were comparable to non-mutant NSCLC, whereas the ORRs in RET fusion NSCLC (less than10% in all studies but one) and ALK fusion NSCLC (0%) were relatively low. The ORRs reported in small numbers of patients and studies of ROS1 fusion, NTRK fusion, and HER 2 mutant NSCLC were 0–17%, 50% and 7–23%, respectively, making the efficacy of ICIs in these groups of patients less clear. In most studies, no significant correlation between treatment outcome and PD-L1 expression or tumor mutation burden (TMB) was identified, and how to select patients with NSCLC harboring actionable mutations who will likely benefit from ICI treatment remains unknown.
NSCLC accounts for 85% of all lung cancers, with lung adenocarcinoma being the major subtype (1). Platinum-based combination chemotherapy is the historical first-line standard of care for patients with advanced NSCLC who have no actionable mutations (2). The introduction of ICIs, such as anti-programmed cell death protein ligand 1 (anti-PD-L1) and anti-programmed cell death protein 1 (anti-PD-1) antibodies, as well as the anti-cytotoxic T-lymphocyte-associated protein 4 (anti-CTLA-4) antibody, have revolutionized the treatment of NSCLC, and is typically offered with or without chemotherapy in the front-line setting for incurable NSCLC that does not have any actionable mutations (2). A number of actionable genetic alterations have been identified in NCSLC, including ALK, ROS1, c-MET, RET, NTRK, BRAF V600E, KRAS, and ERBB2 (HER2) (3–11). MET, RET, HER2, ALK, NTRK, and ROS-1 are receptor tyrosine kinases; BRAF is a serine/threonine kinase mediating cellular signal from RAS to MEK1/2; KRAS is a RAS protein which functions as a GDP–GTP-regulated binary on-off switch. While c-MET, BRAF and KRAS altered NSCLC may develop in both smokers and non-smokers, ALK, ROS1, RET, NTRK, and HER2 alerted NSCLC tend to occur in non-smokers. In patients with actionable driver mutations, namely, EGFR, ALK, BRAFV600E, RET, c-MET, NTRK or ROS1 alterations, the standard of care is to treat with a Food and Drug Administration (FDA) approved targeted agent, which typically can achieve ORRs of 60–80% in treatment naive patients (2, 12). After targeted therapies are exhausted in these patients, systemic therapy with chemotherapy is typically available for them. While incorporating immunotherapy in the regimen is a standard of care option for them, the efficacy of immunotherapy in those with actionable mutations remains poorly defined due to the limited numbers of these patients included in the randomized prospective trials. In addition to the genetic alterations for which targeted therapies have been approved by FDA in the first line setting in NSCLC, KRAS G12C has a targeted agent that was approved recently in the beyond first-line setting. Moreover, HER2 mutations have emerged as new therapeutic targets with promising therapeutic agents in development. The efficacy of ICI in the KRAS G12C or HER2 mutant NSCLC is also of great clinical interest.
In this modern era with a booming number of treatment options for NSCLC and continued improvement in survival, further guidance is needed on what to expect from the use of immunotherapy in those with these genetic abnormalities. The goal of this review is to add valuable information on the use of immunotherapy in NSCLC with actionable alterations in genes including ALK, ROS1, BRAF, c-MET, RET, NTRK, KRAS, and HER2. Epidermal growth factor receptor (EGFR) mutations are not included in this review as they are included in another manuscript by our group which was submitted separately. In this review, we showed that the sensitivity to ICIs can be heterogenous and differs according to the driver alteration considered. ALK and RET fusions were found to be associated with low responses to ICI while BRAF, KRAS, and c-MET alterations were associated with responses that were comparable to non-mutant NSCLC, and PD-L1 positive KRAS mutant NSCLC may be associated with better outcome when treated with ICI monotherapy as suggested by two retrospective studies. The responses to ICIs are less clear in HER2, ROS1 or NTRK altered NSCLCs due to low patient numbers. While an association between PD-L1 expression level or TMB and the responses to ICI has not been consistently observed across all driver alterations, the overall lack of response to ICI treatment appeared to be more common among NSCLC with driver alterations that are typically associated with non-smokers, raising the question whether the absence of tobacco exposure may predict the lack of benefit from ICI treatment. Moreover, the emerging data in the role of co-mutations in response to ICI had also shed a light in the potential underlining mechanism of resistance to ICI, and particularly in the presence of KRAS mutation, co-mutations in TP53, STK11, and KEAP1 have been found to modulate the response to ICIs in several studies (13–15).
Anaplastic lymphoma kinase (ALK), a member of the insulin receptor tyrosine kinase family, has been identified as a fusion partner of nearly 30 different proteins in oncogenic signaling in many different cancer types (3). While there are now over 20 ALK fusion partners identified in NSCLC, EML4 represents the most common fusion partner with 29–33% of gene fusions identified to date (16, 17). The fusion of the 5′ end partner EML4 to the coding region of the intracellular tyrosine kinase domain of ALK leads to aberrant expression of the ALK fusions in the cytoplasm. The domains in the partner proteins also promote dimerization and oligomerization of the fusion proteins, leading to constitutive activation of ALK kinase and its downstream signaling pathways including RAS–mitogen-activated protein kinase, phosphoinositide 3-kinase-AKT, and JAK-STAT pathways. This subsequently results in uncontrolled cellular proliferation and promotes survival (3, 18). ALK fusions are seen in 3–5% of NSCLC patients and are more common among the following groups: no prior smoking history, adenocarcinoma histology, younger age, female gender, and tumors with wild type EGFR and KRAS (16, 19–21). Several ALK inhibitors have been approved by the FDA for metastatic NSCLC, including crizotinib, brigatinib, alectinib, lorlatinib and ceritinib (22–29). The data on the efficacy of ICIs in the ALK fusion positive NSCLC has been scarce. It has been postulated that EML4-ALK oncoprotein can upregulate the PD-L1 expression in lung cancer cells. In one report of 100 patients, fifty patients (50.0%) were PD-L1 negative, 34 patients (34.0%) were PD-L1 low expression (tumor proportion score [TPS] 1–50%), and 16 patients (16.0%) had a strong PD-L1 expression (TPS ≥ 50%) (30). Despite the expression of PDL1 in these tumors, the overall response to ICIs in the ALK fusion positive population has been disappointing except in one study (Table 1).

Table 1 Efficacy of ICIs in NSCLS with ALK mutations.
Although small numbers of patients with ALK fusion NSCLC were included in the randomized phase 3 CheckMate 057 and KEYNOTE-010 studies comparing ICI versus docetaxel in previously treated NSCLC patient population, the outcomes in this specific population were not reported (35, 36).
In a retrospective study using the IMMUNOTARGET registry which included 551 patients receiving ICI monotherapy for advanced NSCLC with at least one oncogenic driver alteration, 23 patients with ALK fusion NSCLC were identified (31). The objective response rate to ICI treatment was 0%. The Median PFS was 2.5 (1.5; 3.7) months. The median OS from start of ICI therapy was 17.0 (3.6; NR) months. Among the 10 patients with available PD-L1 status, the median percentage of cells expressing PD-L1 was 7.5% (Table 1).
In a retrospective study conducted at the Massachusetts General Hospital, the ORR to ICI treatment among patients with EGFR mutations or ALK rearrangements was only 1/28 (3.6%) while the ORR among EGFR WT/ALK-negative patients was 7/30 (23.3%) (P = 0.053) (32). Since the lone partial response was seen in an EGFR-mutant patient, it appeared that none of the six ALK fusion NSCLC patients had a response (Table 1).
In the randomized Impower130 study, atezolizumab plus chemotherapy (Nab-Paclitaxel and Carboplatin) did not show improved overall survival versus chemotherapy alone in the subset of 44 patients with EGFR or ALK genomic alterations in the first line setting (37). However, in the Impower150 study, the addition of Atezolizumab to Bevacizumab, Carboplatin, and Paclitaxel improved the median PFS for patients with EGFR or ALK genomic alteration whose diseases had progressed on TKI or who were unable to tolerate TKI (median, 8.3 months vs. 6.8 months; stratified hazard ratio, 0.61; 95% CI, 0.52 to 0.72). Of note, 34 patients with ALK fusion and 80 patients with EGFR mutant nonsquamous metastatic lung cancer were included in this study, and information on the benefit of atezolizumab in ALK fusion NSCLC was not reported separately (38). In another report of 83 patients with ALK mutation treated with ICI, a mPFS of 2.34 months was reported (33).
A recent prospective multicenter trial presented at the World Conference on Lung Cancer evaluated pembrolizumab and chemotherapy in the setting of recurrent EGFR/ALK-positive NSCLC. The study enrolled a total of 33 patients, including 26 EGFR mutant NSCLC and seven ALK fusion positive NSCLC patients. Most of the patients had one prior targeted therapy. No more than one prior line of platinum-based chemotherapy for advanced NSCLC was allowed. In those with ALK-positive tumors, the ORR was seen in 2/7 (28.6%), and the mPFS and mOS were both 2.9 months, suggesting lack of benefit of ICI in this group of patients (34).
BRAF is a serine/threonine kinase mediating cellular signal from RAS to MEK1/2, and BRAF activation can result in phosphorylation and activation of extracellular signal-regulated kinase (ERK)1/2, leading to cell survival and proliferation (4). BRAF mutations are found in 1.5–3.5% of NSCLC with V600E accounting for approximately half of those mutations (39). Besides adenocarcinoma, BRAF mutations have been reported in sarcomatoid carcinomas, large-cell neuroendocrine carcinomas, and squamous cell lung cancer (40, 41). BRAF mutations can occur in both smokers and non-smokers (42). Selective kinase inhibitors have been recommended for the first-line and second-line treatments of BRAF V600E mutant advanced NSCLC with a reported ORR as high as 64% in this group of patients (39). The outcomes associated with ICIs in this population have been studies in multiple retrospective analyses (Table 2). Although the data vary significantly among different studies, responses to ICI have been seen in most of the studies.
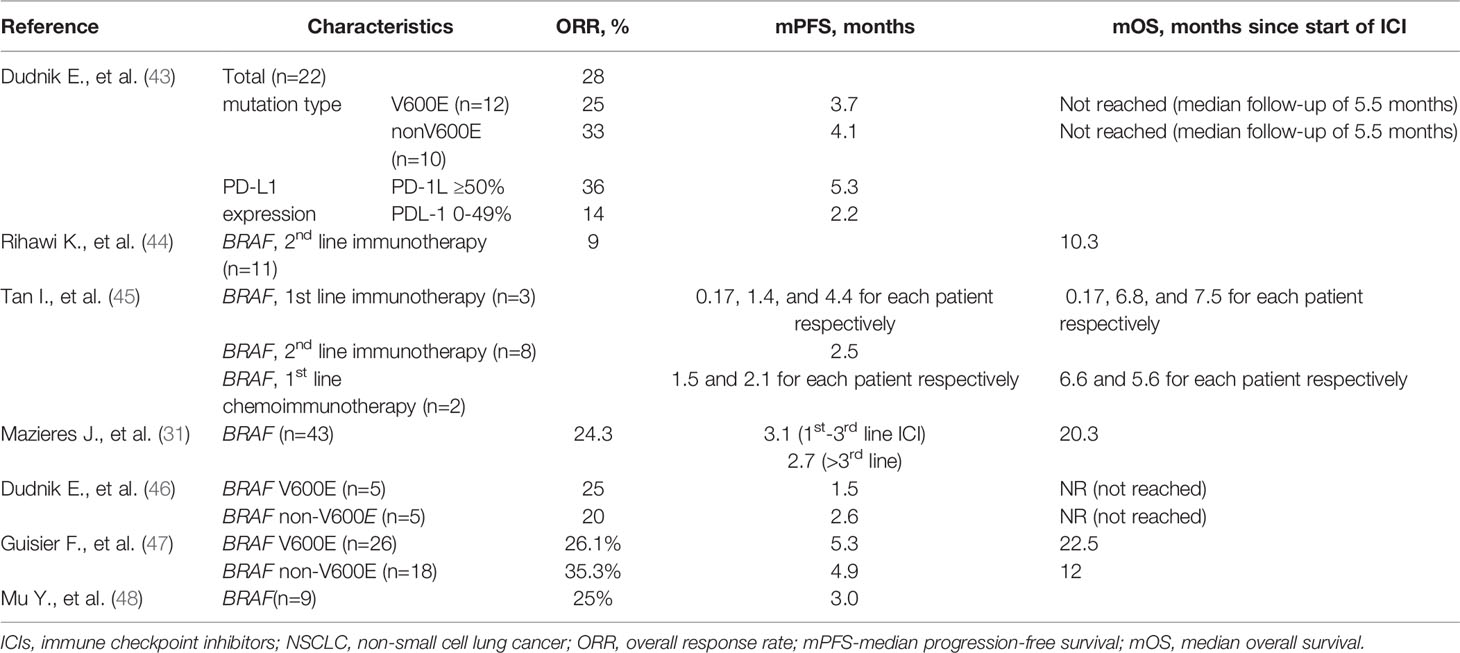
Table 2 Efficacy of ICIs in NSCLS with BRAF mutations.
In a retrospective study including seven participating Israeli cancer centers reported by Dudnik et al., PD-L1 expression level, tumor mutational burden (TMB), and microsatellite instability status were assessed in both BRAF V600E and non-V600E BRAF mutation positive NSCLC, and the outcome with ICI treatment was reported (43). High (≥50%) PD-L1 expression was found to be more common in the non-BRAF V600E mutant group than the V600E BRAF mutant group (50% vs 42%, p = 0.05). No MSI-H was found in both groups, and the median TMB was 5 (1–42) muts/Mb and 11 (7–14) muts/Mb in the BRAF V600E and the non-V600E BRAF mutant groups, respectively. ICI therapy was associated with ORRs of 25 and 33% in the BRAF V600E and the non-V600E BRAF mutant positive groups, respectively (p = 1.0) (Table 2). Among the six patients with high PD-L1 and BRAF V600E mutant NSCLC, two patients had major tumor shrinkage while two other patients had hyperprogression (43).
Among the 1,588 advanced non-squamous NSCLC patients enrolled in the Italian Expanded Access Program of second line nivolumab, 210 patients were assessed for BRAF mutations, and 11 patients (5%) were found to be positive. Median OS was comparable among different groups, and was found to be 11.0 months (range: 9.8 to 12.2 months), 11.2 months (range: 9.2 to 13.2 months) and 10.3 months (range: 2.1 to 18.5 months) in the population with unknown BRAF status, BRAF wild-type subgroup, and BRAF mutated subgroup, respectively (44) (Table 2).
A retrospective study was conducted to evaluate the clinical response to immunotherapy and chemotherapy among 31 patients with BRAF mutant metastatic NSCLC treated at the Duke University Hospital (45). PD-L1 expression information was only available for 11 patients. PD-L1 expression levels ranged from 0 to 90%, with six patients with PD-L1 expression levels greater than 50%. TMB was only available on five patients, ranging from 3 to 18 mutations/Mb. The median PFS in patients who received first-line chemotherapy was 6.4 months (95% CI, 2.3 to 13.0) while the PFS of each of the three patients who received first-line immunotherapy was 0.17, 1.4, and 4.4 months. The median OS in patients who received first-line chemotherapy was 18.4 months (95% CI, 7.4 to 28.6), and the OS of each of the three patients who received first-line immunotherapy was 0.17, 6.8, and 7.5 months (Table 2).
In the retrospective study using the IMMUNOTARGET registry, among the 43 patients with BRAF mutations, PFS was significantly higher in smokers than never smokers (4.1 versus 1.9 months, P = 0.03), however shorter in the V600E subgroup (1.8 months) compared with other BRAF mutations (4.1 months, P = 0.20) (31) (Table 2). The ORR was 24.3%. Among the nine patients with available PD-L1 status, the median percentage of cells expressing PD-L1 was 50%.
In the IMAD2 (GFPC 01-2018), a retrospective study that included 21 centers in France reported by Guisier et al., 44 ICI-treated BRAF mutant (BRAF V600E, n = 26; BRAF non-V600E, n = 18) NSCLC patients were identified (47). Most of the patients received ICI in the beyond-first line setting. Response rates for BRAF-V600E- and BRAF-non-V600E- mutant NSCLC were 26 and 35%, respectively. The median DORs to ICI were NR (95% CI 12.6–NR) and 13.1 months (95% CI 7.6–NR) in the BRAF-V600E- and BRAF-non-V600E groups. The PFS in the BRAF-V600E- and BRAF-non-V600E groups were 5.3 months (95% CI 2.1–NR) and 4.9 months (95% CI 2.3–NR), and the OS in the BRAF-V600E- and BRAF-non-V600E groups were 22.5 months (95% CI 8.3–NR) and 12 months (95% CI 6.8–NR). The 12-month OS in the BRAF-V600E- and BRAF-non-V600E- groups were 53.4 and 44%, respectively (Table 2).
In a cohort of 10 patients with tumors harboring BRAF mutations (BRAF V600E, n−5; BRAF non-V600E, n−5) who received ICI treatment, ORR of 25% (1/4) and 20% (1/5) were seen in patients with BRAF V600E mutation and BRAF non-V600E mutation, respectively (46). Median PFS comprised 1.5 months (95% CI, 1.2–8.3) in patients with BRAF V600E mutation and 2.6 months (95% CI, 2.0–4.2) in patients with BRAF non-V600E mutation. Median OS was not reached in patients with BRAF V600E mutation (95% CI, 1.2–NR) or BRAF non-V600E mutation (95% CI, 2.3–NR) (46) (Table 2). Among patients with known PD-L1 TPS, TPS high (≥50%) was seen in 25 and 60% of the BRAF V600E- and non-BRAF V600E-mutant NSCLC cases, respectively. TMB high (≥10 mut/Mb) was seen in 3 and 1% of the BRAF V600E- and non-BRAF V600E-mutant NSCLC cases, respectively. No MSI-H/I was seen.
In another report of nine patients with BRAF (BRAF V600E, n−6; BRAF non-V600E, n−3) who received ICI with chemotherapy or antiangiogenic treatment, the ORR was 25% and mPFS was three months (95%CI 2.9, 3.1) (48).
MET is a proto-oncogene receptor tyrosine kinase that mediates cell proliferation, survival, and metastasis (5). Recurrent somatic splice site alterations at MET exon 14 (METex14) can result in exon skipping, decreased MET degradation, and MET activation. METex14 is involved in cancer through promoting angiogenesis, cell migration, and invasion (49, 50). METex14 occurs in 3–4% of lung cancers and 8–30% of sarcomatoid lung cancers (51, 52). The occurrence of METex14 appears to be independent of smoking status (53). FDA has granted accelerated approval to capmatinib and tepotinib for adult patients with metastatic NSCLC whose tumors have a mutation that leads to METex14 alterations (54, 55).
In a retrospective study that included 147 patients with METex14 lung cancers, PD-L1 expression of ≥50% was identified in 41% of 111 evaluable tumor samples. The median TMB of METex14 lung cancers was lower than that of unselected non-small-cell lung cancers (NSCLCs). In 24 response-evaluable patients, the ORR was 17% (95% CI 6 to 36%) and the median PFS was 1.9 months (95% CI 1.7–2.7). Responses were not associated with PD-L1 expression ≥50% or high TMB (12) (Table 3).

Table 3 Efficacy of ICIs in NSCLS with c-MET mutations.
Among the 551 patients in the IMMUNOTARGET registry, 13 patients with MET amplification and 23 patients with METex14 were identified (31). Median OS from ICI initiation of this 36-paitent cohort was 18.4 months (7.0; NR) (31). Progressive disease (PD) was found to be the best response to ICI among 50% of patients, and median PFS was found to be 3.4 months (1.7; 6.2). Long-term responders were seen in 23.4% of patients (Table 3). Among the 15 patients with available PD-L1 status, the median percentage of cells expressing PD-L1 was 30%.
In the French retrospective study IMAD2 (GFPC 01-2018), 30 cases of ICI-treated MET mutant NSCLC were identified (47). Most patient received ICI in the beyond-first line setting. The response rate for MET-altered NSCLC was 36%. The median duration of response (mDOR) was 10.4 months (95% CI 4.6–NR). The mPFS was 4.9 months ((95% CI 2.0–11.4), and the mOS was 13.4 months (95% CI 9.4–NR) (Table 3).
In a retrospective study that included eight cases of NSCLC with METex14 and four cases of NSCLC with MET amplification treated with ICI, median PFS with ICI was 4.0 months (95% CI, 2.4–NR) in patients with METex14 and 4.9 months (95% CI, 2.4–NR) in patients with MET amplification (46). ORR comprised 12% (1/8) and 25% (1/4) in patients with METex14 and MET amplification respectively. Median OS with ICI was not reached in patients with METex14 (95% CI, 4.1–NR) or in patients with MET amplification (95% CI, 3.5–NR) (Table 3). Among patients with known PD-L1 TPS, TPS high (≥50%) was seen in 67% of the cases. TMB high (≥10 mut/Mb) or MSI-H/I was not seen.
In a case series, among 13 patients with METex14 NSCLCs treated with ICI, 46.2% (6/13) patients responded to immunotherapy. Six patients had prolonged duration of responses ranging from 18 months (still ongoing) to 49 months (56).
RET is a proto-oncogene receptor tyrosine kinase that binds with the ligand–co-receptor complex of glial cell line-derived neurotrophic factor (GDNF) family ligands (GFLs) and subsequently activates signaling pathways such as RAS/mitogen activated protein kinase (MAPK), RAS/ERK, phosphatidylinositol 3-kinase (PI3K)/AKT, and c-Jun N-terminal kinase (JNK). Aberrant activation of the RET receptor have been associated with multiple endocrine neoplasia 2 (MEN2), sporadic medullary thyroid cancer, papillary thyroid carcinoma (PTC), and non-small cell lung cancer (NSCLC) (6, 7). RET rearrangements have been identified in 1–3% of NSCLC and were found to have significantly higher frequencies in younger (<60 years of age), female, non-smokers, and adenocarcinoma histology (57–60). RET fusion positive NSCLC is usually associated with low PD-L 1 expression (61). Two potent selective RET inhibitors, selpercatinib and pralsetinib, have been approved by the FDA for RET fusion-positive NSCLC (62, 63). The activity of ICI in RET altered NSCLC has been evaluated in multiple studies, and the benefit of ICI was found to be low in most of the studies (Table 4).

Table 4 Efficacy of ICIs in NSCLS with RET mutations.
In the French retrospective study IMAD2 (GFPC 01-2018), nine patients with RET translocation NSCLC received ICI, all in the beyond-first line setting. The response rate for RET-altered NSCLC was 38%. The mDOR response to ICI was 12.1 months (95% CI 8.4–NR). The median PFS was 7.6 months (2.3–NR), and the median OS was not reached (95% CI 26.8–NR) (47) (Table 4).
In a single center retrospective study conducted in Korea, the median progression-free survival for ICI among 13 patients with RET fusion-positive NSCLC treated with ICI was 2.1 (95% CI: 1.6–2.6) months, and the ORR was 7.7% (64). The median PFS and OS were 2.1 (95% CI: 1.6–2.6) and 12.4 (95% CI: 2.9–21.8) months, respectively. Among patients with PD-L1 expression 25% and above, 2/5 patients demonstrated stable disease, while the best response in the other three patients was disease progression (Table 4). In contrast, the ORR and DCR among 46 patients treated with pemetrexed-based regimens in this study was 63.0 and 91.3%, respectively, and the median PFS was 9.0 (95% CI: 6.9–11.2) months.
Among the 16 patients with RET fusion-positive NSCLC in the IMMUNOTARGET registry, the median OS from the start of ICI therapy was 21.3 (3.8; 28.0), and the median PFS was only 2.1 (1.3; 4.7) (31). The rate of any partial or complete response was very low and was 6.3% (1/16) (Table 4). Among the six patients with available PD-L1 status, the median percentage of cells expressing PD-L1 was 26%.
In a retrospective study conducted at the Memorial Sloan Kettering Cancer Center, 13 patients with RET-rearranged NSCLC treated with ICI were assessed for clinical and/or radiologic response (30). No response to immunotherapy was observed. The median PFS was 3.4 months (95% CI, 2.1 to 5.6 months). No difference in OS between patients with advanced RET-rearranged lung cancers who received immunotherapy (n = 16) and those who did not receive immunotherapy (n = 46), (hazard ratio, 1.4 [95% CI, 0.7 to 2.9]; log-rank P = .35) (Table 4). Only one patient was found to have PD-L1 expression ≥50%, and the disease of this patient did not respond to ICI. No patient had TMB >10 mut/Mb.
In the single institution retrospective study published by Dudnik et al., four patients with RET fusion NSCLC and one patient with RET mutant NSCLC were treated with ICI (46). No objective response was observed. Median PFS was 3.0 months (95% CI, 1.9–3.1) in patients with RET fusion and 6.9 months in patient with RET mutation. Median OS since start of ICP were 14.9 months (95% CI, 7.2–19.7) in patients with RET fusion and 15.3 months in patient with RET mutation (Table 4). Among patients with known PD-L1 TPS, TPS high (≥50%) was seen in 13 and 0% of the RET fusion and the RET mutant NSCLC cases, respectively. TMB high or MSI-H/I was not seen.
ROS proto-oncogene 1 (ROS1) belongs to the subfamily of tyrosine kinase insulin receptors (65). ROS1 fusion can lead to constitutive activation of kinase activity, resulting in increased cell proliferation, survival, and migration due to the upregulation of JAK/STAT, PI3K/AKT, and MAPK/ERK signaling pathways (8). ROS1 rearrangements account for 1–2% of NSCLC patients (66, 67). This alteration more frequently occurs in adenocarcinoma and in younger patients with no or light smoking history (68, 69).
Seven patients with ROS1 fusion NSCLC treated with ICI were identified in the IMMUNOTARGET registry (31). The objective response rate to ICI treatment was 17% (Table 5).

Table 5 Efficacy of ICIs in NSCLS with ROS-1 mutations.
In the single institution retrospective study published by Dudnik et al., only one patient with ROS1 fusion NSCLC treated with ICI was identified, and the reported PFS and OS were both 0.1 month (46) (Table 5). Among the five patients with available PD-L1 status, the median percentage of cells expressing PD-L1 was 90%.
In the Japanese retrospective study, 15 ROS1 altered NSCLC cases were identified. High expression of PD-L1 (>50% of tumor cells by 22C3) were observed in 53% cases, however, no response to immunotherapy was observed (70).
The NTRK genes (NTRK1, NTRK2 and NTRK3) encode tropomyosin receptor kinases (TRKA, TRKB and TRKC) (9). The TRK fusion protein leads to constitutive activation of various downstream signal transduction pathways including the PI3k/Akt and RAS/RAF/MAPK pathways, and subsequently causes proliferation of cancer cells (9). Rearrangements including NTRK1, NTRK2, and NTRK3 occur in approximately 2–3% of NSCLC patients (10). Selective TRK inhibitors, Entrectinib and Larotrectinib, have been approved for patients with NTRK fusion-positive solid tumors, including NSCLC (71, 72).
In the single institution retrospective study published by Dudnik et al., two patients with NTRK fusion NSCLC were treated with ICI. The objective response rate was 50% (1/2). Median PFS was as not reached (95% CI, 3.2–NR). Median OS since start of ICP not reached (95% CI, NR–NR) (46) (Table 6). One patient had PD-L1 TPS ≥50%. No patient had TMB ≥10 muts/Mb.
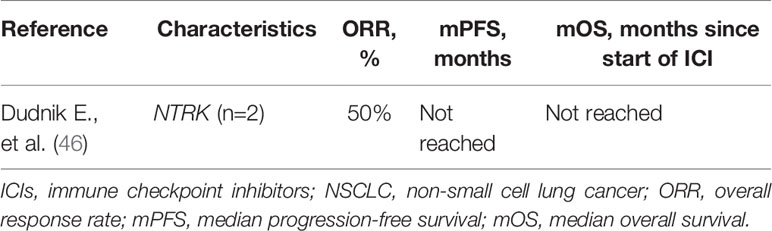
Table 6 Efficacy of ICIs in NSCLS with NTRK mutations.
KRAS is one of the RAS proteins (KRAS4A, KRAS4B, NRAS, and HRAS) which function as GDP–GTP-regulated binary on-off switches and regulate cell survival, cell cycle progression, cell polarity, movement, and nuclear transport by transducing signals from transmembrane receptors to cytoplasmic signaling pathways such as the MAPK pathway (10, 11). It is the most common proto-oncogene identified in NSCLC. KRAS mutations occur in 15–25% of lung adenocarcinomas and are more prevalent in smokers than nonsmokers (73, 74). Majority of the KRAS mutations in NSCLC occur on exon 2 or 3 (G12, G13, and Q61), with the most frequent being the G12C followed by G12V and G12D (75, 76). Sotorasib has been approved by the FDA for patients with KRAS G12C mutant locally advanced or metastatic NSCLC in the beyond the first line setting (72). It is associated with an objective response rate of 37.1% in this group of patients (77). The efficacy of ICIs in KRAS mutant NSCLC has been studied in several retrospective studies, and most of the data support the benefit on ICIs in KRAS mutant NSCLC (Table 7).
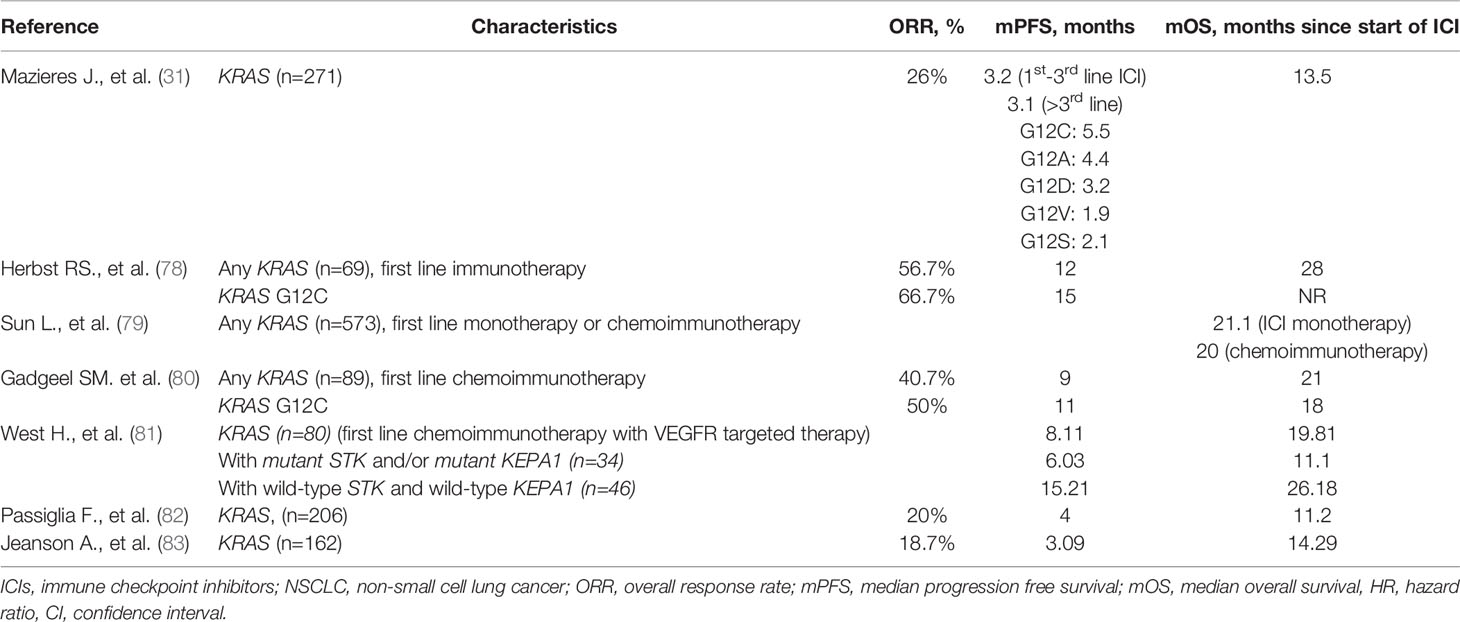
Table 7 Efficacy of ICIs in NSCLS with KRAS mutations.
In a retrospective analysis in patients enrolled in the KEYNOTE-042 evaluating pembrolizumab monotherapy vs platinum-based chemotherapy as the first-line therapy among patients with PD-L1-positive (TPS ≥1%) advanced non-squamous histology NSCLC, 301 patients were evaluable by whole-exome sequencing (WES). KRAS mutations were found in 69 (23%) patients, among which, 29 (10%) patients were found to have KRAS G12C (78). PD-L1 TPS and TMB were found to be higher in patients with KRAS mutations than without KRAS mutations, although the differences were not significant. The OS associated with pembrolizumab was better than chemotherapy in both the KRAS mutant group and KRAS G12C subgroup, with the HRs being 0.42 (0.22–0.81) and 0.28 (0.09–0.86), respectively. Conversely, there was no significant OS difference seen between pembrolizumab and chemotherapy in the KRAS wild-type patients, and HR was 0.86 (0.63–1.18). A superior PFS was also observed when pembrolizumab was compared with chemotherapy in the KRAS mutant patients. The data supported the benefit of single agent pembrolizumab in the PD-1 TPS >1% KRAS mutant (including KRAS G12C) NSCLC patients, underlining the important role of ICI in the treatment of this group of patients.
The efficacy of ICIs in the first line setting in PD-L1 TPS ≥50% advanced NSCLC was also investigated in a retrospective analysis using the Flatiron Health database (79). Among the1,127 patients with PD-L1 expression of 50% or greater who were treated with either ICI monotherapy or chemoimmunotherapy, 573 (50.8%) had KRAS alterations and 554 (49.2%) had wild type KRAS. Among the patients treated with ICI monotherapy, a better mOS was seen in the KRAS mutant group when compared with the wild-type group (mOS, 21.1 vs 13.6 months; P = .03). Interestingly, this OS advantage was not observed among patients treated with chemoimmunotherapy, and the mOS was 20.0 vs 19.3 months; P = .93 in the KRAS mutant and wild type patients. Furthermore, no mOS difference was seen between ICI monotherapy and chemoimmunotherapy in the KRAS mutant NSCLC patients (mOS, 21.1 vs 20.0 months; P = .78), suggesting that the use of ICI monotherapy in the PD-L1 TPS ≥50% is an acceptable option in the KRAS mutant advanced NSCLC.
The efficacy of chemoimmunotherapy in KRAS mutant NSCLC was also analyzed retrospectively in the participants of another randomized trial, the KEYNOTE-189 study of pembrolizumab plus pemetrexed and platinum chemotherapy vs placebo plus chemotherapy as first-line therapy for metastatic non-squamous NSCLC (80). Among the 289 patients who had evaluable WES data, 89 (31%) patients were found to have KRAS mutations including KRAS G12C, which was found in 37 (13%) patients. As observed in the KEYNOTE-042 study, the higher PD-L1 TPS and TMB tended to be seen with KRAS mutant patients. Although unlike the observation in the KEYNOTE-042, the OS benefit associated with the addition of ICI was only detected in the KRAS wild-type patients. PFS improvement associated with the additional of ICI was seen in both the KRAS mutant and wild type group but not in the KRAS G12C subgroup, which could be related to the small sample number.
In addition to ICI monotherapy and chemoimmunotherapy, the combination of VEGF receptor targeted agent and chemoimmunotherapy represents another first-line treatment option for advanced NSCLC based on the IMpower150 study (84). A post hoc analysis evaluated the efficacy outcomes in patients with KRAS, STK11(LKB1), and KEAP1 mutations (81). Among 920 patients included, KRAS mutations were found in 80 patients (24.5%), with 39 patients found to have co-occurring mutations in STK11 and/or KEAP1. The addition of ICI improved mOS and PFS in the KRAS mutant patients regardless of STK11 and KEAP1 status (Table 7), supporting the use of this regimen in KRAS mutant NSCLC.
The correlation between STK11/LKB1 genomic alterations and the efficacy of ICI treatment in KRAS mutant NSCLC was also evaluated using the Stand Up To Cancer (SU2C) dataset (13). Unlike the post hoc analysis of the IMpower150 study, this study showed that the concurrent STK11/LKB1 mutation in KRAS mutant NSCLC was associated with an inferior ORR to PD-1 blockade when compared with KRAS mutation without STK11/LKB1 mutation and KRAS mutation with P53 mutations groups (7.4, 28.6 and 35.7% (P <0.001)). The details of the ICI therapy in this dataset were not available, and it is unclear whether this group of patients also received angiogenesis targeted agent treatment.
In a systemic review and metanalysis aiming to investigate the predictive clinicopathological characteristics for the relative efficacy of ICIs vs docetaxel in the second-line setting in NSCLCs, the authors analyzed data from five randomized clinical trials involving 3,025 patients (85). ICIs were associated with prolonged overall survival (HR, 0.69; 95% CI, 0.63–0.75; P < .001). The survival benefit was also seen among the 148 KRAS mutant patients (HR, 0.65; 95% CI, 0.44–0.97; P = .03) but not in the 371 KRAS wild-type patients (HR, 0.86; 95% CI, 0.67–1.11; P = .24; interaction, P = .24) (85).
The efficacy of ICI in KRAS mutant non-squamous NSCLC in the beyond first-line setting was also investigated in patients who received nivolumab in an Italian expanded access program (EAP) study (82). Among the 530 patients evaluated, 206 (39%) had KRAS mutations. No significant differences in OS, PFS or ORR were seen between KRAS mutant and KRAS wild- type patients in this study, supporting that nivolumab should be considered for patients regardless of KRAS mutation status. Interestingly, any significantly higher grade and grade 3–4 treatment related adverse events were seen in the KRAS mutant group than the wild-type group, although the underlining mechanism for the finding is unknown.
KRAS mutant NSCLC was also evaluated in the IMMUNOTARGET study. Two hundred and seventy-one patients treated with ICIs were found to have KRAS mutations. An encouraging ORR of 26% was found, and the mPFS and mOS were 3.2 and 13.5months, respectively (31).
In a single instituation retrospective study conducted in France, a total of 162 KRAS-mutant advanced NSCLC were identified among the 282 subjects analyzed. No significant difference was seen in ORR, mPFS or mOS between the KRAS mutant and the KRAS wild-type groups. The ORR, mPFS, and mOS associated with ICI of KRAS mutant NSCLC were 18.7%, 3.09 months and 14.29 months. No significant difference in treamtent outcomes was seen among the KRAS mutation subtypes including G12A, G12C, G12D, G12V, and G13C (83).
Human epidermal growth factor 2 (HER2 erbB-2/neu) is one of the four receptor tyrosine kinase members of the human epidermal growth factor receptor family. Upon forming homo- or hetero-dimers with other family members, HER2 becomes activated and signal through the PI3K-AKT and MEK-ERK downstream pathways to activate proliferation (86). In NSCLC, activating HER2 mutations occur in 2–4% of cases, most commonly in adenocarcinoma histology and never smokers (87). Patients with HER2 mutant NSCLC have worse OS if treated without HER2 targeted therapy (88). Although there has not been any HER 2 targeted agent approved by NSCLC by the FDA, several agents have showed promising activity. Ado-trastuzumab emtansine, a HER2-targeted antibody-drug conjugate was found to be associated with an ORR of 44% in NSCLC with HER2 exon 20 insertions and point mutations (89), and another HER2-targeted antibody-drug conjugate, trastuzumab deruxtecan, also showed an encouraging ORR of 55% in patients with metastatic HER2-overexpressing or HER2-mutant NSCLC whose disease had relapsed during standard treatment or was refractory to standard treatment (90). Both agents are included as novel therapeutic options for HER2 mutant NSCLC in the current NCCN guidelines (2). Poziotinib, a tyrosine kinase inhibitor targeting EGFR/HER2 exon 20 insertion mutation, was found to have an ORR of 27% in HER2 exon 20 mutant NSCLC, gaining fast track designation by FDA (91, 92).
The efficacy of immunotherapy in patients whose cancer harbors HER2 mutation is largely unknown. The ORR associated with ICI among the 29 patients with exon 20 activating mutations in the IMMUNOTARGET study was only 7%. PFS was 2.5 months, and the 12-month PFS was 13.6 months. The OS was 20.3 months (31). The ORR among the 23 patients with exon 20 insertions included in the IMAD2 study by the French Lung Cancer Group was 27.3%. PFS was similar to the findings in the IMMUNOTARGET study and was 2.2 months, and the 12-month PFS was 22.9%. The mOS was an encouraging 20.4 months (47) (Table 8).

Table 8 Efficacy of ICIs in NSCLS with HER2 mutations.
To delineate the benefit of ICI treatment in NSCLC harboring actional mutations other than EGFR alterations, we reviewed the current available data in this area. We found that the ORR, median PFS, and OS with ICPi varied significantly across genetic alteration subgroups. While the ORR observed in the BRAF, c-MET, and KRAS altered NSCLC appeared to be similar to what had been observed in the non-selected NSCLC groups, the ORRs in the ALK and RET altered NSCLC groups were much lower (2).
Unlike ALK and RET fusions, BRAF, MET, and KRAS mutations can be seen in both smokers and non-smokers. The higher prevalence of smoking history in these patients could be a potential reason of the higher response rates since smoking has been found to be associated with the benefit derived from ICI treatment in some of the literatures (93, 94), although not confirmed by other studies (95). Other known predictive biomarkers for ICI treatment include PD-L1 expression level, microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR), and TMB (96–98). A higher percentage of PD-L1 TPS high (67%) was reported in BRAF non V600E mutant and MET mutant NSCLC in some of the reports (46), and a relatively higher response was seen in patients with PD-L1 TPS high BRAF mutant NSCLC (43), albeit the sample numbers was too small to draw any firm conclusion.
The current NCCN guidelines support the use of targeted therapy in the first line setting for advanced NSCLC with actionable genomic alterations involving EGFR, ALK, ROS1, BRAF, NTRK1/2/3, METex14 skipping, and RET. After disease progression, chemoimmunotherapy is recommended for this population based on the guidelines (2). Although most of the chemoimmunotherapy trials excluded the EGFR and ALK altered NSCLC patients, these groups of patients were evaluated in the IMpower150 study if they have had progression with or unacceptable side effects from treatment with at least one approved tyrosine kinase inhibitor. The data showed improved PFS associated with the additional of atezolizumab to the bevacizumab, carboplatin, and paclitaxel combination in EGFR and ALK altered NSCLC (9.7 months vs. 6.1 months), providing direct evidence supporting the use of the regimen in this population (38). In our review, while not robust, we see that ICI’s do have activity in patients with NSCLC harbouring actionable mutations, and that a response can be seen after progression on targeted therapy, supporting offering chemoimmunotherapy in the post-targeted therapy setting. For KRAS G12C NSCLC, ICI monotherapy or chemoimmunotherapy is the current standard of care first line treatment. The data included in this review did confirm the benefits of ICI in the KRAS mutant NSCLC, supporting the current treatment approach. The benefit of ICI monotherapy in PD-L1 positive KRAS mutant NSLCL was suggested in retrospective studies, warranting further investigation on the selection of ICI monotherapy vs chemoimmunotherapy in this population (78, 79). Furthermore, data from prospective studies will be helpful to identify the best treatment sequence among targeted therapy, ICI, and chemotherapy.
Even in the subgroups where the benefits of ICIs were observed, the ORRs tended to be low. Therefore, developing predictive biomarkers for ICI therapy would be of great importance.
Co-occurring genomic alterations have been reported to be related to responses to immunotherapy through altering the microenvironment. For example, LKB1/STK11 genomic alterations, a frequent co-occurring mutation in of KRAS mutant NSCLC, have been found to be associates with “immune-inert” state (99). This was supported by several studies including a retrospective study conducted in 103 NSCLC patients receiving ICIs. In this study, among the patient with KRAS mutations, the presence of concurrent STK11 mutation or STK11/TP53 mutations were associated with worse survival with ICI therapy. This association was not observed with chemotherapy, supporting the predictive roles of these co-mutations for ICI therapy in KRAS mutant NSCLC (15). The data from a retrospective analysis suggested that co-occurring LKB1/STK11 mutations in KRAS mutant NSCLC may predict lower ORR, while data from another group showed no PFS or OS differences with or without concurrent mutant LKB1/STK11 and/or mutant KEPA1 in patients receiving combined chemoimmunotherapy and angiogenesis targeted agent (13, 81), raising the question whether angiogenesis targeted agent may help to overcome the challenge of the immune-inert state. Other co-occurring genomic alterations such as P53, KEAP1, ATM, PTEN, CDKN2A are common among KRAS-mutant NSCLC, and may play a role in determining response to ICI (100). Furthermore, a recent study showed that co-occurring mutations such as NOTCH and HR pathways were also found to be associated with increased efficacy of immunotherapy in advanced NSCLC (101). Therefore, identifying co-occurring mutations that are responsible for ICI response or resistance could potentially help to identify the candidate for ICI treatments and warrants further investigation in this group of patients.
How to overcome the resistance to ICI therapy is another great challenge. The mechanism of resistance is complex and is a combination of tumor-intrinsic and extrinsic factors. Many factors such as immune contexture and tumor microenvironment, expression of PD-L1 and LAG3, TMB, genetic and epigenetic alterations, antigen-presenting molecules (MHC, HLA) and microbiota may all contribute to the resistance to immunotherapy (102). The tumors with higher initial mutational burdens have been found to be associated with higher sensitivity to ICIs in some studies, although this association may be negated by other factors such as intratumoral heterogeneity and mutations (103). RET fusion positive NSCLC was found to have poor response to ICIs, and the alterations appears to be associated with lower TMB. In the analysis by Offin M. et al., the median TMB of RET altered NSCLC was significantly lower than that of the RET wild-type NSCLCs (1.75 versus 5.27 mutations/Mb, P <.0001) (61). The best outcome in patients in this study was stable disease which only lasted 5.6 months. In the report by Dudnik E. et al, the TBM was low in all 13 patients except one patient who had intermediate TMB, and the ORR in this report was also 0% (46). Nevertheless, an ORR of 37.5% was found among the nine evaluable patients reported by Guisier F. et al. Unfortunately, the TMB information was not available in this study, and it was unclear if the treatments were ICI monotherapy or chemoimmunotherapy. A prospective study to allow uniform treatment and collection of information on biomarkers such as TMB, PD-L1, MSI/MMR, tumor-infiltrating lymphocytes, whole-exome sequencing analysis on tumor samples and intestinal microbiome composition may be helpful to identify the resistance mechanisms.
ALK fusion positive NSCLC showed poor response to ICI in retrospective studies. However, this group of patients did benefit from ICI in the IMpower 150 trial, raising the question if the inhibition of angiogenesis could sensitize cancer cells to ICI therapy. Tumor angiogenesis can lead to immunosuppression through various mechanisms including maintaining an acidic/hypoxic and immunosuppressive environment, development of dysfunctional blood vessels which limits T cell trafficking, and suppression of dendritic cell maturation. Moreover, the angiogenic factors such as VEGF are also immunosuppressive (104). Therefore, further investigation is warranted in co-inhibition of angiogenic factors in NSCLC harboring actionable driver mutations undergoing ICI treatment.
With regard to the combination of ICIs and targeted therapies, a number of studies had evaluated the combiantion of ALK TKIs and different ICIs in NSCLC, including the combination of nivolumab with ceritinib or crizotinib and the combiantion of alectinib plus atezolizumab (105–107). However, significant toxicities were observed without survival benefit. In addition, there has been some concerning safety signals where ICI treatment is followed with targeted therapy (108). Reports showed risk of hepatotoxicity in a series of patients with ALK, ROS1, or MET exon 14 alterations who received ICI before crizotinib. Among the eleven patients treated with crizotinib following ICI, five patients (45.5%) developed grade 3 or 4 hepatotoxicity, whereas only 8% of those patients who received crizotinib alone experienced hepatotoxicity. The increased hepatotoxicity in sequentially treated patients led to permanent discontinuation of crizotinib in four of the five patients (108), highlighting the importance of establishing the presence of actionable mutations prior to initiating ICI therapy in patients with advanced NSCLC. The frequency and severity of toxicities associates with sequential use of ICI followed by targeted therapy may vary among different therapeutic agents. In the CodeBreaK100 phase II study evaluating Sotorasib in the beyond first-line setting, even though 91.3% patients had received ICI treatment prior to Sotorasib, the tolerability remained acceptable. Ongoing clinical trials DESTINY-Lung03 (NCT04686305) and the HUDSON trial (NCT03334617) are investigating the combination of T-DXd with immunotherapy, chemotherapy, novel anticancer agents and will hence shed more light on the approach in HER2 mutant subgroup NSCLC patients.
Our review certainly has limitations. We were unable to comment on the response of HER2, ROS1 and NTRK altered NSCLC to ICI as there were few reports in the literature, and the patient numbers in these reports were often very small. The challenges are obviously associated with the low incidences of these alterations. A recent report from Negrao et al. showed that RET, ROS1 and ALK alterations were associated with low sensitivity to ICIs. However, there were only three ROS1 fusion NSCLC patients included in the study, and the outcome of all three alterations were reported collectively (15). Furthermore, we were also unable to compare the responses to ICIs among different alterations which can be better investigated in prospective studies. Moreover, many studies included in this reivew did not have the biomarker information on all the evaluable patients. The ICI treatments and the number of lines of treament received previously by the patients also varied significantly. Additionally, it was not always clear whether the ICI treament was given as a monotherapy or in combination with cytotoxic chemotherapy. Randomized prospective studies would undoubtly provide more definitive information on this topic.
In conclusion, we see low responses to ICI in ALK and RET altered NSCLCs whereas BRAF, KRAS and c-MET alterations were associated with benefit from ICIs, and PD-L1 positive KRAS mutant NSCLCs may be more responsive to ICI monotherapy. Furthermore, the response to ICIs in KRAS mutant NSCLCs may vary depending on co-existing mutations, and responses to ICIs in HER2, ROS1 and NTRK altered NSCLCs are less clear and varies significantly across a small number of studies. Ultimately, immunotherapy in the second line after progression on targeted agents can be considered as a treatment option at the discretion of treating physicians, following a mutual discussion with patients about the pros and cons of this approach.
All authors contributed equally to the writing, development, editing, and information gathering of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel R, Naishadham D, Jemal A. Cancer Statistics, 2013. CA Cancer J Clin (2013) 63(1):11–30. doi: 10.3322/caac.21166
2. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Non-Small Cell Lung Cancer.Version 5.2021. Available at: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.
3. Hallberg B, Palmer RH. The Role of the ALK Receptor in Cancer Biology. Ann Oncol (2016) 27(Suppl 3):iii4–15. doi: 10.1093/annonc/mdw301
4. Marchetti A, Felicioni L, Malatesta S, Grazia Sciarrotta M, Guetti L, Chella A, et al. Clinical Features and Outcome of Patients With Non-Small-Cell Lung Cancer Harboring BRAF Mutations. J Clin Oncol (2011) 29(26):3574–9. doi: 10.1200/JCO.2011.35.9638
5. Maulik G, Shrikhande A, Kijima T, Ma PC, Morrison PT, Salgia R. Role of the Hepatocyte Growth Factor Receptor, C-Met, in Oncogenesis and Potential for Therapeutic Inhibition. Cytokine Growth Factor Rev (2002) 13(1):41–59. doi: 10.1016/S1359-6101(01)00029-6
6. Li AY, McCusker MG, Russo A, Scilla KA, Gittens A, Arensmeyer K, et al. RET Fusions in Solid Tumors. Cancer Treat Rev (2019) 81:101911. doi: 10.1016/j.ctrv.2019.101911
7. Santoro M, Moccia M, Federico G, Carlomagno F. RET Gene Fusions in Malignancies of the Thyroid and Other Tissues. Genes (Basel) (2020) 11(4):424. doi: 10.3390/genes11040424
8. Roskoski R Jr. ROS1 Protein-Tyrosine Kinase Inhibitors in the Treatment of ROS1 Fusion Protein-Driven non-Small Cell Lung Cancers. Pharmacol Res (2017) 121:202–12. doi: 10.1016/j.phrs.2017.04.022
9. Miao Q, Ma K, Chen D, Wu X, Jiang S. Targeting Tropomyosin Receptor Kinase for Cancer Therapy. Eur J Med Chem (2019) 175:129–48. doi: 10.1016/j.ejmech.2019.04.053
10. Stokoe D, Macdonald SG, Cadwallader K, Symons M, Hancock JF. Activation of Raf as a Result of Recruitment to the Plasma Membrane. Science (1994) 264(5164):1463–7. doi: 10.1126/science.7811320
11. Wennerberg K, Rossman KL, Der CJ. The Ras Superfamily at a Glance. J Cell Sci (2005) 118(Pt 5):843–6. doi: 10.1242/jcs.01660
12. Sabari JK, Leonardi GC, Shu CA, Umeton R, Montecalvo J, Ni A, et al. PD-L1 Expression, Tumor Mutational Burden, and Response to Immunotherapy in Patients With MET Exon 14 Altered Lung Cancers. Ann Oncol (2018) 29(10):2085–91. doi: 10.1093/annonc/mdy334
13. Skoulidis F, Goldberg ME, Greenawalt DM, Hellmann MD, Awad MM, Gainor JF, et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov (2018) 8(7):822–35. doi: 10.1158/2159-8290.CD-18-0099
14. Pavan A, Boscolo Bragadin A, Calvetti L, Ferro A, Zulato E, Attili I, et al. Role of Next Generation Sequencing-Based Liquid Biopsy in Advanced Non-Small Cell Lung Cancer Patients Treated With Immune Checkpoint Inhibitors: Impact of STK11, KRAS and TP53 Mutations and Co-Mutations on Outcome. Trans Lung Cancer Res (2020) 10(1):202–20. doi: 10.21037/tlcr-20-674
15. Negrao MV, Skoulidis F, Montesion M, Schulze K, Bara I, Shen V, et al. Oncogene-Specific Differences in Tumor Mutational Burden, PD-L1 Expression, and Outcomes From Immunotherapy in Non-Small Cell Lung Cancer. J ImmunoTherapy Cancer (2021) 9(8):e002891. doi: 10.1136/jitc-2021-002891
16. Wong DW, Leung EL, So KK, Tam IY, Sihoe AD, Cheng LC, et al. The EML4-ALK Fusion Gene is Involved in Various Histologic Types of Lung Cancers From Nonsmokers With Wild-Type EGFR and KRAS. Cancer (2009) 115(8):1723–33. doi: 10.1002/cncr.24181
17. Koivunen JP, Mermel C, Zejnullahu K, Murphy C, Lifshits E, Holmes AJ, et al. EML4-ALK Fusion Gene and Efficacy of an ALK Kinase Inhibitor in Lung Cancer. Clin Cancer Res (2008) 14(13):4275–83. doi: 10.1158/1078-0432.CCR-08-0168
18. Sasaki T, Rodig SJ, Chirieac LR, Janne PA. The Biology and Treatment of EML4-ALK Non-Small Cell Lung Cancer. Eur J Cancer (2010) 46(10):1773–80. doi: 10.1016/j.ejca.2010.04.002
19. Shaw AT, Yeap BY, Mino-Kenudson M, Digumarthy SR, Costa DB, Heist RS, et al. Clinical Features and Outcome of Patients With Non-Small-Cell Lung Cancer Who Harbor EML4-ALK. J Clin Oncol (2009) 27(26):4247–53. doi: 10.1200/JCO.2009.22.6993
20. Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S, et al. Identification of the Transforming EML4-ALK Fusion Gene in Non-Small-Cell Lung Cancer. Nature (2007) 448(7153):561–6. doi: 10.1038/nature05945
21. Chia PL, Mitchell P, Dobrovic A, John T. Prevalence and Natural History of ALK Positive Non-Small-Cell Lung Cancer and the Clinical Impact of Targeted Therapy With ALK Inhibitors. Clin Epidemiol (2014) 6:423–32. doi: 10.2147/CLEP.S69718
22. Cruz BD, Barbosa MM, Torres LL, Azevedo PS, Silva VEA, Godman B, et al. Crizotinib Versus Conventional Chemotherapy in First-Line Treatment for ALK-Positive Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Oncol Ther (2021) 9:505–24. doi: 10.1007/s40487-021-00155-3
23. Chen J, O'Gorman MT, James LP, Klamerus KJ, Mugundu G, Pithavala YK. Pharmacokinetics of Lorlatinib After Single and Multiple Dosing in Patients With Anaplastic Lymphoma Kinase (ALK)-Positive Non-Small Cell Lung Cancer: Results From a Global Phase I/II Study. Clin Pharmacokinet (2021) 60:1313–24. doi: 10.1007/s40262-021-01015-z
24. Camidge DR, Kim HR, Ahn MJ, Yang JCH, Han JY, Hochmair MJ, et al. Brigatinib Versus Crizotinib in Advanced ALK Inhibitor-Naive ALK-Positive Non-Small Cell Lung Cancer: Second Interim Analysis of the Phase III ALTA-1l Trial. J Clin Oncol (2020) 38(31):3592–603. doi: 10.1200/JCO.20.00505
25. Wu YL, Lu S, Lu Y, Zhou J, Shi YK, Sriuranpong V, et al. Results of PROFILE 1029, a Phase III Comparison of First-Line Crizotinib Versus Chemotherapy in East Asian Patients With ALK-Positive Advanced Non-Small Cell Lung Cancer. J Thorac Oncol (2018) 13(10):1539–48. doi: 10.1016/j.jtho.2018.06.012
26. Solomon BJ, Besse B, Bauer TM, Felip E, Soo RA, Camidge DR, et al. Lorlatinib in Patients With ALK-Positive Non-Small-Cell Lung Cancer: Results From a Global Phase 2 Study. Lancet Oncol (2018) 19(12):1654–67. doi: 10.1016/S1470-2045(18)30649-1
27. Camidge DR, Kim HR, Ahn MJ, Yang JC, Han JY, Lee JS, et al. Brigatinib Versus Crizotinib in ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2018) 379(21):2027–39. doi: 10.1056/NEJMoa1810171
28. Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim DW, et al. Alectinib Versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2017) 377(9):829–38. doi: 10.1056/NEJMoa1704795
29. Soria JC, Tan DSW, Chiari R, Wu YL, Paz-Ares L, Wolf J, et al. First-Line Ceritinib Versus Platinum-Based Chemotherapy in Advanced ALK-Rearranged Non-Small-Cell Lung Cancer (ASCEND-4): A Randomised, Open-Label, Phase 3 Study. Lancet (2017) 389(10072):917–29. doi: 10.1016/S0140-6736(17)30123-X
30. Chang G-C, Yang T-Y, Chen K-C, Hsu K-H, Huang Y-H, Su K-Y, et al. ALK Variants, PD-L1 Expression, and Their Association With Outcomes in ALK-Positive NSCLC Patients. Sci Rep (2020) 10(1):21063. doi: 10.1038/s41598-020-78152-1
31. Mazieres J, Drilon A, Lusque A, Mhanna L, Cortot AB, Mezquita L, et al. Immune Checkpoint Inhibitors for Patients With Advanced Lung Cancer and Oncogenic Driver Alterations: Results From the IMMUNOTARGET Registry. Ann Oncol (2019) 30(8):1321–8. doi: 10.1093/annonc/mdz167
32. Gainor JF, Shaw AT, Sequist LV, Fu X, Azzoli CG, Piotrowska Z, et al. EGFR Mutations and ALK Rearrangements Are Associated With Low Response Rates to PD-1 Pathway Blockade in Non-Small Cell Lung Cancer: A Retrospective Analysis. Clin Cancer Res (2016) 22(18):4585–93. doi: 10.1158/1078-0432.CCR-15-3101
33. Jahanzeb M, Lin HM, Pan X, Yin Y, Baumann P, Langer CJ. Immunotherapy Treatment Patterns and Outcomes Among ALK-Positive Patients With Non-Small-Cell Lung Cancer. Clin Lung Cancer (2021) 22(1):49–57. doi: 10.1016/j.cllc.2020.08.003
34. Gadgeel S, Dziubek K, Nagasaka M, Braun T, Hassan K, Cheng H, et al. Pembrolizumab in Combination With Platinum-Based Chemotherapy in Recurrent EGFR/ALK-Positive Non-Small Cell Lung Cancer (NSCLC), in: Abstracts | IASLC 2021 World Conference on Lung Cancer | Worldwide Virtual Event. 2021(WCLC 2021). Journal of Thoracic Oncology. Amsterdam: Elsevier (2021). Available at: Dziubek.
35. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab Versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N Engl J Med (2015) 373(17):1627–39. doi: 10.1056/NEJMoa1507643
36. Herbst RS, Baas P, Kim D-W, Felip E, Pérez-Gracia JL, Han J-Y, et al. Pembrolizumab Versus Docetaxel for Previously Treated, PD-L1-Positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010): A Randomised Controlled Trial. Lancet (2016) 387(10027):1540–50. doi: 10.1016/S0140-6736(15)01281-7
37. West H, McCleod M, Hussein M, Morabito A, Rittmeyer A, Conter HJ, et al. Atezolizumab in Combination With Carboplatin Plus Nab-Paclitaxel Chemotherapy Compared With Chemotherapy Alone as First-Line Treatment for Metastatic Non-Squamous Non-Small-Cell Lung Cancer (IMpower130): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol (2019) 20(7):924–37. doi: 10.1016/S1470-2045(19)30167-6
38. Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N Engl J Med (2018) 378(24):2288–301. doi: 10.1056/NEJMoa1716948
39. Dong J, Li B, Lin D, Zhou Q, Huang D. Advances in Targeted Therapy and Immunotherapy for Non-Small Cell Lung Cancer Based on Accurate Molecular Typing. Front Pharmacol (2019) 10:230–. doi: 10.3389/fphar.2019.00230
40. Leonetti A, Facchinetti F, Rossi G, Minari R, Conti A, Friboulet L, et al. BRAF in Non-Small Cell Lung Cancer (NSCLC): Pickaxing Another Brick in the Wall. Cancer Treat Rev (2018) 66:82–94. doi: 10.1016/j.ctrv.2018.04.006
41. Cancer Genome Atlas Research N. Comprehensive Genomic Characterization of Squamous Cell Lung Cancers. Nature (2012) 489(7417):519–25. doi: 10.1038/nature11404
42. Cui G, Liu D, Li W, Fu X, Liang Y, Li Y, et al. A Meta-Analysis of the Association Between BRAF Mutation and Nonsmall Cell Lung Cancer. Med (Baltimore) (2017) 96(14):e6552. doi: 10.1097/MD.0000000000006552
43. Dudnik E, Peled N, Nechushtan H, Wollner M, Onn A, Agbarya A, et al. BRAF Mutant Lung Cancer: Programmed Death Ligand 1 Expression, Tumor Mutational Burden, Microsatellite Instability Status, and Response to Immune Check-Point Inhibitors. J Thorac Oncol (2018) 13(8):1128–37. doi: 10.1016/j.jtho.2018.04.024
44. Rihawi K, Giannarelli D, Galetta D, Delmonte A, Giavarra M, Turci D, et al. BRAF Mutant NSCLC and Immune Checkpoint Inhibitors: Results From a Real-World Experience. J Thorac Oncol (2019) 14(3):e57–9. doi: 10.1016/j.jtho.2018.11.036
45. Tan I, Stinchcombe TE, Ready NE, Crawford J, Datto MB, Nagy RJ, et al. Therapeutic Outcomes in Non-Small Cell Lung Cancer With BRAF Mutations: A Single Institution, Retrospective Cohort Study. Transl Lung Cancer Res (2019) 8(3):258–67. doi: 10.21037/tlcr.2019.04.03
46. Dudnik E, Bshara E, Grubstein A, Fridel L, Shochat T, Roisman LC, et al. Rare Targetable Drivers (RTDs) in Non-Small Cell Lung Cancer (NSCLC): Outcomes With Immune Check-Point Inhibitors (ICPi). Lung Cancer (2018) 124:117–24. doi: 10.1016/j.lungcan.2018.07.044
47. Guisier F, Dubos-Arvis C, Vinas F, Doubre H, Ricordel C, Ropert S, et al. Efficacy and Safety of Anti-PD-1 Immunotherapy in Patients With Advanced NSCLC With BRAF, HER2, or MET Mutations or RET Translocation: GFPC 01-2018. J Thorac Oncol (2020) 15(4):628–36. doi: 10.1016/j.jtho.2019.12.129
48. Mu Y, Yang K, Hao X, Wang Y, Wang L, Liu Y, et al. Clinical Characteristics and Treatment Outcomes of 65 Patients With BRAF-Mutated Non-Small Cell Lung Cancer. Front Oncol (2020) 10:603–. doi: 10.3389/fonc.2020.00603
49. Ding S, Merkulova-Rainon T, Han ZC, Tobelem G. HGF Receptor Up-Regulation Contributes to the Angiogenic Phenotype of Human Endothelial Cells and Promotes Angiogenesis In Vitro. Blood (2003) 101(12):4816–22. doi: 10.1182/blood-2002-06-1731
50. Bauer TW, Somcio RJ, Fan F, Liu W, Johnson M, Lesslie DP, et al. Regulatory Role of C-Met in Insulin-Like Growth Factor-I Receptor-Mediated Migration and Invasion of Human Pancreatic Carcinoma Cells. Mol Cancer Ther (2006) 5(7):1676–82. doi: 10.1158/1535-7163.MCT-05-0175
51. Frampton GM, Ali SM, Rosenzweig M, Chmielecki J, Lu X, Bauer TM, et al. Activation of MET via Diverse Exon 14 Splicing Alterations Occurs in Multiple Tumor Types and Confers Clinical Sensitivity to MET Inhibitors. Cancer Discov (2015) 5(8):850–9. doi: 10.1158/2159-8290.CD-15-0285
52. Awad MM, Oxnard GR, Jackman DM, Savukoski DO, Hall D, Shivdasani P, et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and C-Met Overexpression. J Clin Oncol (2016) 34(7):721–30. doi: 10.1200/JCO.2015.63.4600
53. Van Der Steen N, Giovannetti E, Pauwels P, Peters GJ, Hong DS, Cappuzzo F, et al. cMET Exon 14 Skipping: From the Structure to the Clinic. J Thorac Oncol (2016) 11(9):1423–32. doi: 10.1016/j.jtho.2016.05.005
54. Wolf J, Seto T, Han JY, Reguart N, Garon EB, Groen HJM, et al. Capmatinib in MET Exon 14-Mutated or MET-Amplified Non-Small-Cell Lung Cancer. N Engl J Med (2020) 383(10):944–57. doi: 10.1056/NEJMoa2002787
55. Paik PK, Felip E, Veillon R, Sakai H, Cortot AB, Garassino MC, et al. Tepotinib in Non-Small-Cell Lung Cancer With MET Exon 14 Skipping Mutations. N Engl J Med (2020) 383(10):931–43. doi: 10.1056/NEJMoa2004407
56. Mayenga M, Assie JB, Monnet I, Massiani MA, Tabeze L, Friard S, et al. Durable Responses to Immunotherapy of Non-Small Cell Lung Cancers Harboring MET Exon-14-Skipping Mutation: A Series of 6 Cases. Lung Cancer (2020) 150:21–5. doi: 10.1016/j.lungcan.2020.09.008
57. Kohno T, Ichikawa H, Totoki Y, Yasuda K, Hiramoto M, Nammo T, et al. KIF5B-RET Fusions in Lung Adenocarcinoma. Nat Med (2012) 18(3):375–7. doi: 10.1038/nm.2644
58. Li F, Feng Y, Fang R, Fang Z, Xia J, Han X, et al. Identification of RET Gene Fusion by Exon Array Analyses in "Pan-Negative" Lung Cancer From Never Smokers. Cell Res (2012) 22(5):928–31. doi: 10.1038/cr.2012.27
59. Kato S, Subbiah V, Marchlik E, Elkin SK, Carter JL, Kurzrock R. RET Aberrations in Diverse Cancers: Next-Generation Sequencing of 4,871 Patients. Clin Cancer Res (2017) 23(8):1988–97. doi: 10.1158/1078-0432.CCR-16-1679
60. Lin C, Wang S, Xie W, Chang J, Gan Y. The RET Fusion Gene and Its Correlation With Demographic and Clinicopathological Features of Non-Small Cell Lung Cancer: A Meta-Analysis. Cancer Biol Ther (2015) 16(7):1019–28. doi: 10.1080/15384047.2015.1046649
61. Offin M, Guo R, Wu SL, Sabari J, Land JD, Ni A, et al. Immunophenotype and Response to Immunotherapy of RET-Rearranged Lung Cancers. JCO Precis Oncol (2019) 3:1–8. doi: 10.1200/PO.18.00386
62. Drilon A, Oxnard GR, Tan DSW, Loong HHF, Johnson M, Gainor J, et al. Efficacy of Selpercatinib in RET Fusion-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2020) 383(9):813–24. doi: 10.1056/NEJMoa2005653
63. Gainor JF, Curigliano G, Kim DW, Lee DH, Besse B, Baik CS, et al. Pralsetinib for RET Fusion-Positive Non-Small-Cell Lung Cancer (ARROW): A Multi-Cohort, Open-Label, Phase 1/2 Study. Lancet Oncol (2021) 22(7):959–69. doi: 10.1016/S1470-2045(21)00247-3
64. Lee J, Ku BM, Shim JH, La Choi Y, Sun JM, Lee SH, et al. Characteristics and Outcomes of RET-Rearranged Korean Non-Small Cell Lung Cancer Patients in Real-World Practice. Jpn J Clin Oncol (2020) 50(5):594–601. doi: 10.1093/jjco/hyaa019
65. Birchmeier C, Sharma S, Wigler M. Expression and Rearrangement of the ROS1 Gene in Human Glioblastoma Cells. Proc Natl Acad Sci U S A (1987) 84(24):9270–4. doi: 10.1073/pnas.84.24.9270
66. Davies KD, Le AT, Theodoro MF, Skokan MC, Aisner DL, Berge EM, et al. Identifying and Targeting ROS1 Gene Fusions in Non-Small Cell Lung Cancer. Clin Cancer Res (2012) 18(17):4570–9. doi: 10.1158/1078-0432.CCR-12-0550
67. Facchinetti F, Rossi G, Bria E, Soria JC, Besse B, Minari R, et al. Oncogene Addiction in non-Small Cell Lung Cancer: Focus on ROS1 Inhibition. Cancer Treat Rev (2017) 55:83–95. doi: 10.1016/j.ctrv.2017.02.010
68. Lin JJ, Shaw AT. Recent Advances in Targeting ROS1 in Lung Cancer. J Thorac Oncol (2017) 12(11):1611–25. doi: 10.1016/j.jtho.2017.08.002
69. Bergethon K, Shaw AT, Ou SH, Katayama R, Lovly CM, McDonald NT, et al. ROS1 Rearrangements Define a Unique Molecular Class of Lung Cancers. J Clin Oncol (2012) 30(8):863–70. doi: 10.1200/JCO.2011.35.6345
70. Yoh K, Matsumoto S, Kunimasa K, Kodani M, Nishi K, Nakagawa T, et al. The Efficacy of Immune Checkpoint Inhibitors and PD-L1 Status in Patients With Advanced Non-Small Cell Lung Cancer Harboring Oncogenic Driver Alterations: Immuno-Oncology Biomarker Study in LC-SCRUM-Japan. J Clin Oncol (2019) 37(15_suppl):9046–. doi: 10.1200/JCO.2019.37.15_suppl.9046
71. Al-Salama ZT, Keam SJ. Entrectinib: First Global Approval. Drugs (2019) 79(13):1477–83. doi: 10.1007/s40265-019-01177-y
72. Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-sotorasib-kras-g12c-mutated-nsclc.
73. Wood K, Hensing T, Malik R, Salgia R. Prognostic and Predictive Value in KRAS in Non-Small-Cell Lung Cancer: A Review. JAMA Oncol (2016) 2(6):805–12. doi: 10.1001/jamaoncol.2016.0405
74. Liu C, Zheng S, Jin R, Wang X, Wang F, Zang R, et al. The Superior Efficacy of Anti-PD-1/PD-L1 Immunotherapy in KRAS-Mutant Non-Small Cell Lung Cancer That Correlates With an Inflammatory Phenotype and Increased Immunogenicity. Cancer Lett (2020) 470:95–105. doi: 10.1016/j.canlet.2019.10.027
75. Dogan S, Shen R, Ang DC, Johnson ML, D'Angelo SP, Paik PK, et al. Molecular Epidemiology of EGFR and KRAS Mutations in 3,026 Lung Adenocarcinomas: Higher Susceptibility of Women to Smoking-Related KRAS-Mutant Cancers. Clin Cancer Res (2012) 18(22):6169–77. doi: 10.1158/1078-0432.CCR-11-3265
76. El Osta B, Behera M, Kim S, Berry LD, Sica G, Pillai RN, et al. Characteristics and Outcomes of Patients With Metastatic KRAS-Mutant Lung Adenocarcinomas: The Lung Cancer Mutation Consortium Experience. J Thorac Oncol (2019) 14(5):876–89. doi: 10.1016/j.jtho.2019.01.020
77. Skoulidis F, Li BT, Dy GK, Price TJ, Falchook GS, Wolf J, et al. Sotorasib for Lung Cancers With KRAS P.G12C Mutation. N Engl J Med (2021) 384(25):2371–81. doi: 10.1056/NEJMoa2103695
78. Herbst RS. LBA4 Association of KRAS Mutational Status With Response to Pembrolizumab Monotherapy Given as First-Line Therapy for PD-L1-Positive Advanced Non-Squamous NSCLC in Keynote-042. Ann Oncol (2019) 30(Supplement 11):xi63–xi4. doi: 10.1093/annonc/mdz453.001
79. Sun L, Hsu M, Cohen RB, Langer CJ, Mamtani R, Aggarwal C. Association Between KRAS Variant Status and Outcomes With First-Line Immune Checkpoint Inhibitor-Based Therapy in Patients With Advanced Non-Small-Cell Lung Cancer. JAMA Oncol (2021) 7(6):937–9. doi: 10.1001/jamaoncol.2021.0546
80. Gadgeel S, Rodriguez-Abreu D, Felip E, Esteban E, Speranza G, Reck M, et al. KRAS Mutational Status and Efficacy in KEYNOTE-189: Pembrolizumab (Pembro) Plus Chemotherapy (Chemo) vs Placebo Plus Chemo as First-Line Therapy for Metastatic Non-Squamous NSCLC. Ann Oncol (2019) 30:xi64–xi5. doi: 10.1093/annonc/mdz453.002
81. West H, Cappuzzo F, Reck M, Mok T, Jotte RM, Nishio M, et al. IMpower150: A Post Hoc Analysis of Efficacy Outcomes in Patients With KRAS, STK11 and KEAP1 Mutations. Ann Oncol (2020) 31(10):817–8. doi: 10.1016/j.annonc.2020.08.1579
82. Passiglia F, Cappuzzo F, Alabiso O, Bettini AC, Bidoli P, Chiari R, et al. Efficacy of Nivolumab in Pre-Treated Non-Small-Cell Lung Cancer Patients Harbouring KRAS Mutations. Br J Cancer (2019) 120(1):57–62. doi: 10.1038/s41416-018-0234-3
83. Jeanson A, Tomasini P, Souquet-Bressand M, Brandone N, Boucekine M, Grangeon M, et al. Efficacy of Immune Checkpoint Inhibitors in KRAS-Mutant Non-Small Cell Lung Cancer (NSCLC). J Thorac Oncol (2019) 14(6):1095–101. doi: 10.1016/j.jtho.2019.01.011
84. Remon J, Castro-Henriques M, Esteller L, Vives J. Combination of Atezolizumab, Bevacizumab, and Chemotherapy (IMpower 150) in a Patient With NSCLC Having Leptomeningeal Metastases. JTO Clin Res Rep (2021) 2(1):100096. doi: 10.1016/j.jtocrr.2020.100096
85. Lee CK, Man J, Lord S, Cooper W, Links M, Gebski V, et al. Clinical and Molecular Characteristics Associated With Survival Among Patients Treated With Checkpoint Inhibitors for Advanced Non–Small Cell Lung Carcinoma: A Systematic Review and Meta-Analysis. JAMA Oncol (2018) 4(2):210–6. doi: 10.1001/jamaoncol.2017.4427
86. Lenferink AE, Pinkas-Kramarski R, van de Poll ML, van Vugt MJ, Klapper LN, Tzahar E, et al. Differential Endocytic Routing of Homo- and Hetero-Dimeric ErbB Tyrosine Kinases Confers Signaling Superiority to Receptor Heterodimers. EMBO J (1998) 17(12):3385–97. doi: 10.1093/emboj/17.12.3385
87. Ekman S. HER2: Defining a Neu Target in Non-Small-Cell Lung Cancer. Ann Oncol (2019) 30(3):353–5. doi: 10.1093/annonc/mdz043
88. Pillai RN, Behera M, Berry LD, Rossi MR, Kris MG, Johnson BE, et al. HER2 Mutations in Lung Adenocarcinomas: A Report From the Lung Cancer Mutation Consortium. Cancer (2017) 123(21):4099–105. doi: 10.1002/cncr.30869
89. Li BT, Shen R, Buonocore D, Olah ZT, Ni A, Ginsberg MS, et al. Ado-Trastuzumab Emtansine for Patients With HER2-Mutant Lung Cancers: Results From a Phase II Basket Trial. J Clin Oncol (2018) 36(24):2532–7. doi: 10.1200/JCO.2018.77.9777
90. Li BT, Smit EF, Goto Y, Nakagawa K, Udagawa H, Mazières J, et al. Trastuzumab Deruxtecan in HER2-Mutant Non–Small-Cell Lung Cancer. N Engl J Med (2021). doi: 10.1056/NEJMoa2112431
91. Elamin YY, Robichaux JP, Carter BW, Altan M, Gibbons DL, Fossella FV, et al. Poziotinib for Patients With HER2 Exon 20 Mutant Non–Small-Cell Lung Cancer: Results From a Phase II Trial. J Clin Oncol (2021) 2021:JCO.21.01113. doi: 10.1200/JCO.21.01113
92. Heymach J, Negrao M, Robichaux J, Carter B, Patel A, Altan M, et al. OA02.06 A Phase II Trial of Poziotinib in EGFR and HER2 Exon 20 Mutant Non-Small Cell Lung Cancer (NSCLC). J Thorac Oncol (2018) 13(10):S323–S4. doi: 10.1016/j.jtho.2018.08.243
93. Mo J, Hu X, Gu L, Chen B, Khadaroo PA, Shen Z, et al. Smokers or Non-Smokers: Who Benefits More From Immune Checkpoint Inhibitors in Treatment of Malignancies? An Up-to-Date Meta-Analysis. World J Surg Oncol (2020) 18(1):15. doi: 10.1186/s12957-020-1792-4
94. Wang X, Ricciuti B, Alessi JV, Nguyen T, Awad MM, Lin X, et al. Smoking History as a Potential Predictor of Immune Checkpoint Inhibitor Efficacy in Metastatic Non-Small Cell Lung Cancer. J Natl Cancer Inst (2021). doi: 10.1093/jnci/djab116
95. Chen DL, Li QY, Tan QY. Smoking History and the Efficacy of Immune Checkpoint Inhibitors in Patients With Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. J Thorac Dis (2021) 13(1):220–31. doi: 10.21037/jtd-20-1953
96. Marabelle A, Le DT, Ascierto PA, Di Giacomo AM, De Jesus-Acosta A, Delord JP, et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J Clin Oncol (2020) 38(1):1–10. doi: 10.1200/JCO.19.02105
97. Yu Y, Zeng D, Ou Q, Liu S, Li A, Chen Y, et al. Association of Survival and Immune-Related Biomarkers With Immunotherapy in Patients With Non-Small Cell Lung Cancer: A Meta-Analysis and Individual Patient-Level Analysis. JAMA Netw Open (2019) 2(7):e196879. doi: 10.1001/jamanetworkopen.2019.6879
98. Kim JY, Kronbichler A, Eisenhut M, Hong SH, van der Vliet HJ, Kang J, et al. Tumor Mutational Burden and Efficacy of Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers (Basel) (2019) 11(11):1798. doi: 10.3390/cancers11111798
99. Skoulidis F, Byers LA, Diao L, Papadimitrakopoulou VA, Tong P, Izzo J, et al. Co-Occurring Genomic Alterations Define Major Subsets of KRAS-Mutant Lung Adenocarcinoma With Distinct Biology, Immune Profiles, and Therapeutic Vulnerabilities. Cancer Discov (2015) 5(8):860–77. doi: 10.1158/2159-8290.CD-14-1236
100. Davis AP, Cooper WA, Boyer M, Lee JH, Pavlakis N, Kao SC. Efficacy of Immunotherapy in KRAS-Mutant Non-Small-Cell Lung Cancer With Comutations. Immunotherapy (2021) 13(11):941–52. doi: 10.2217/imt-2021-0090
101. Mazzotta M, Filetti M, Occhipinti M, Marinelli D, Scalera S, Terrenato I, et al. Efficacy of Immunotherapy in Lung Cancer With Co-Occurring Mutations in NOTCH and Homologous Repair Genes. J Immunother Cancer (2020) 8(2):1–6. doi: 10.1136/jitc-2020-000946
102. Perez-Ruiz E, Melero I, Kopecka J, Sarmento-Ribeiro AB, Garcia-Aranda M, De Las Rivas J. Cancer Immunotherapy Resistance Based on Immune Checkpoints Inhibitors: Targets, Biomarkers, and Remedies. Drug Resist Update (2020) 53:100718. doi: 10.1016/j.drup.2020.100718
103. Park YJ, Kuen DS, Chung Y. Future Prospects of Immune Checkpoint Blockade in Cancer: From Response Prediction to Overcoming Resistance. Exp Mol Med (2018) 50(8):1–13. doi: 10.1038/s12276-018-0130-1
104. Kashyap AS, Schmittnaegel M, Rigamonti N, Pais-Ferreira D, Mueller P, Buchi M, et al. Optimized Antiangiogenic Reprogramming of the Tumor Microenvironment Potentiates CD40 Immunotherapy. Proc Natl Acad Sci U S A (2020) 117(1):541–51. doi: 10.1073/pnas.1902145116
105. Felip E, de Braud FG, Maur M, Loong HH, Shaw AT, Vansteenkiste JF, et al. Ceritinib Plus Nivolumab in Patients With Advanced ALK-Rearranged Non-Small Cell Lung Cancer: Results of an Open-Label, Multicenter, Phase 1b Study. J Thorac Oncol (2020) 15(3):392–403. doi: 10.1016/j.jtho.2019.10.006
106. Spigel DR, Reynolds C, Waterhouse D, Garon EB, Chandler J, Babu S, et al. Phase 1/2 Study of the Safety and Tolerability of Nivolumab Plus Crizotinib for the First-Line Treatment of Anaplastic Lymphoma Kinase Translocation - Positive Advanced Non-Small Cell Lung Cancer (CheckMate 370). J Thorac Oncol (2018) 13(5):682–8. doi: 10.1016/j.jtho.2018.02.022
107. Kim D-W, Gadgeel SM, Gettinger SN, Riely GJ, Oxnard GR, Mekhail T, et al. Safety and Clinical Activity Results From a Phase Ib Study of Alectinib Plus Atezolizumab in ALK+ Advanced NSCLC (aNSCLC). J Clin Oncol (2018) 36(15_suppl):9009–. doi: 10.1200/JCO.2018.36.15_suppl.9009
Keywords: targeted mutations, immunotherapy, c-MET, RET, BRAF, ROS-1, ALK, NTRK
Citation: Seegobin K, Majeed U, Wiest N, Manochakian R, Lou Y and Zhao Y (2021) Immunotherapy in Non-Small Cell Lung Cancer With Actionable Mutations Other Than EGFR. Front. Oncol. 11:750657. doi: 10.3389/fonc.2021.750657
Received: 09 August 2021; Accepted: 10 November 2021;
Published: 01 December 2021.
Edited by:
Laura Bonanno, Veneto Institute of Oncology (IRCCS), ItalyReviewed by:
Min Li, Sun Yat-sen University Cancer Center (SYSUCC), ChinaCopyright © 2021 Seegobin, Majeed, Wiest, Manochakian, Lou and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yujie Zhao, Wmhhby5ZdWppZUBtYXlvLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.